Early Postoperative Circulating miR-483-5p Is a Prognosis Marker for Adrenocortical Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
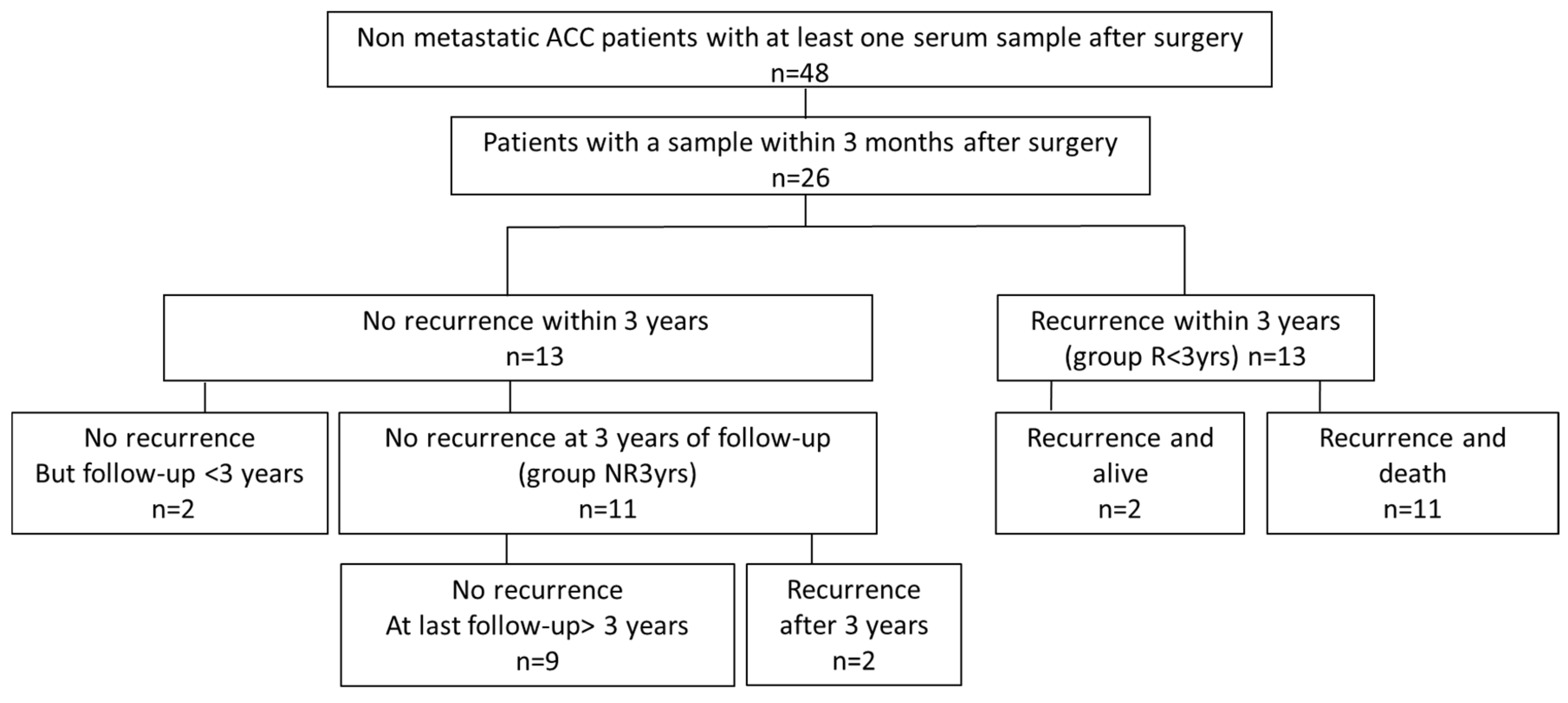
2.1. Patients
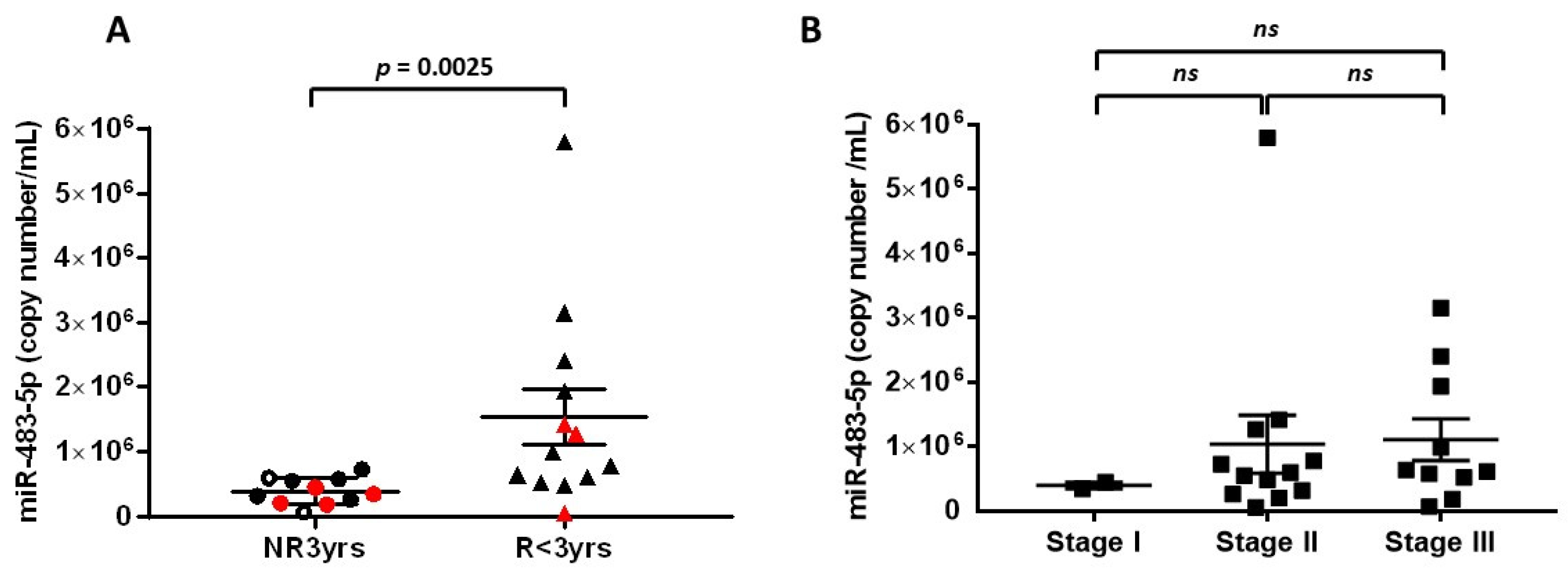
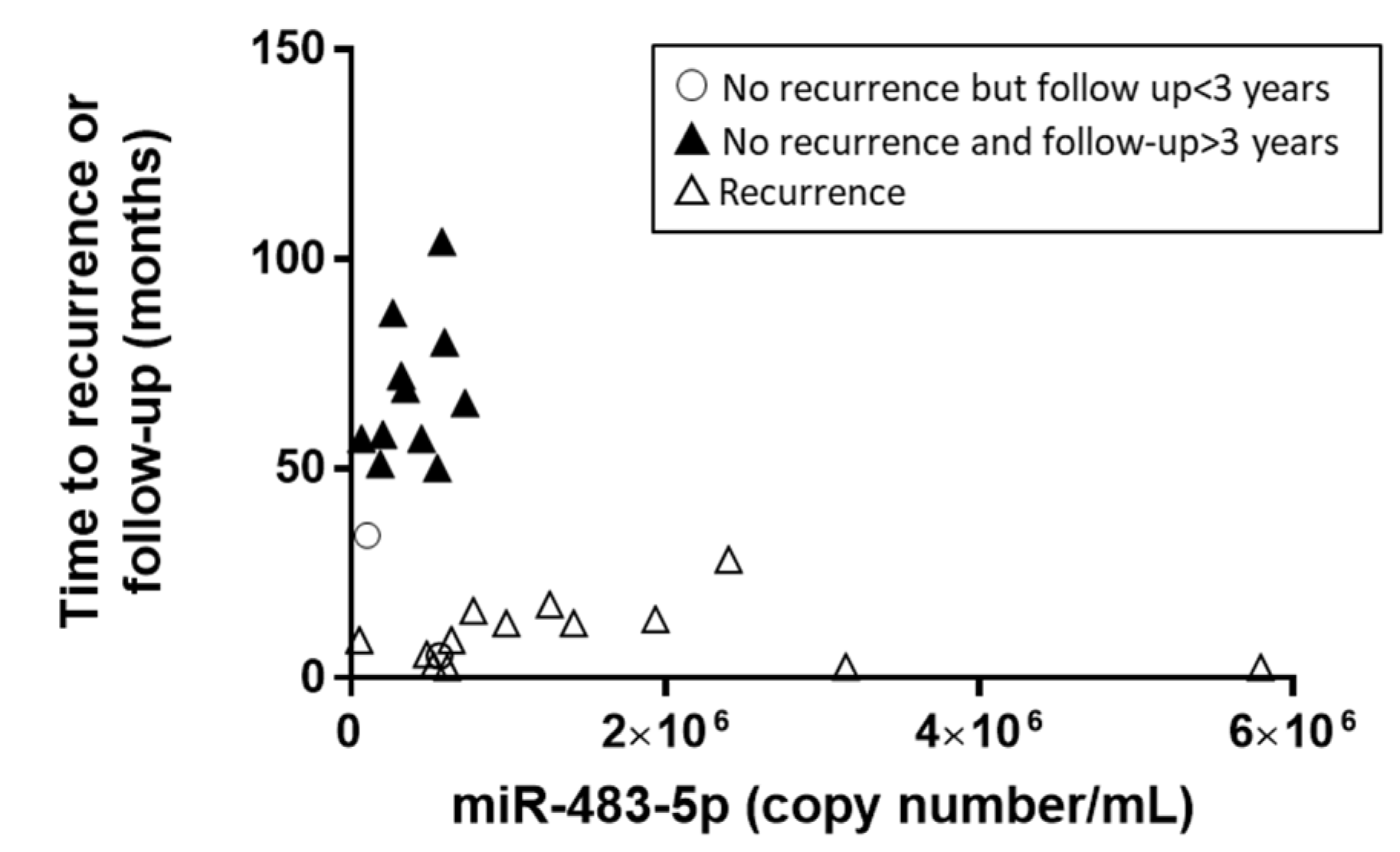
2.2. MiR-483-5p Levels and Recurrence-Risk Within 3 Years: Analysis of the Group R < 3yrs vs. the Group NR3yrs
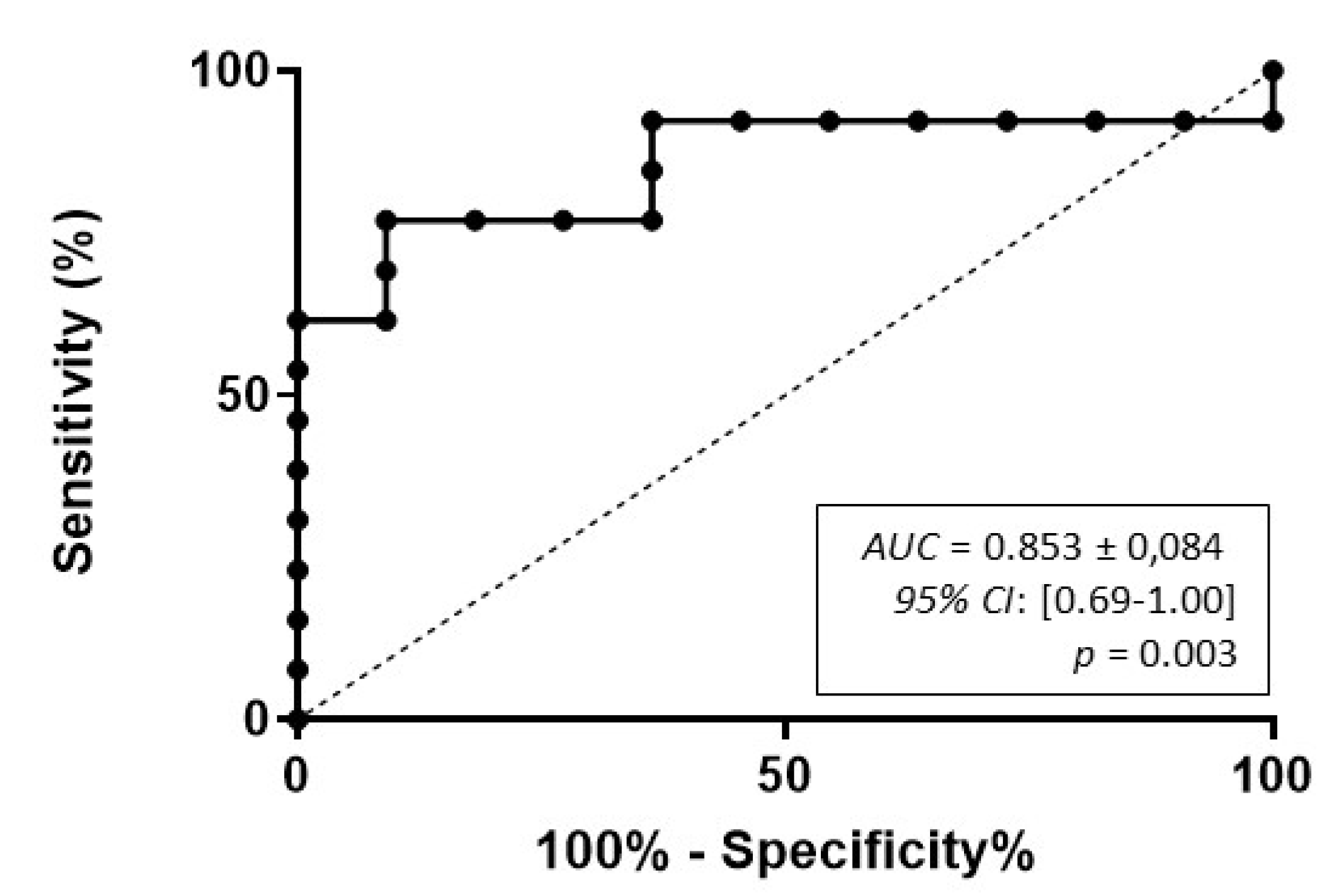
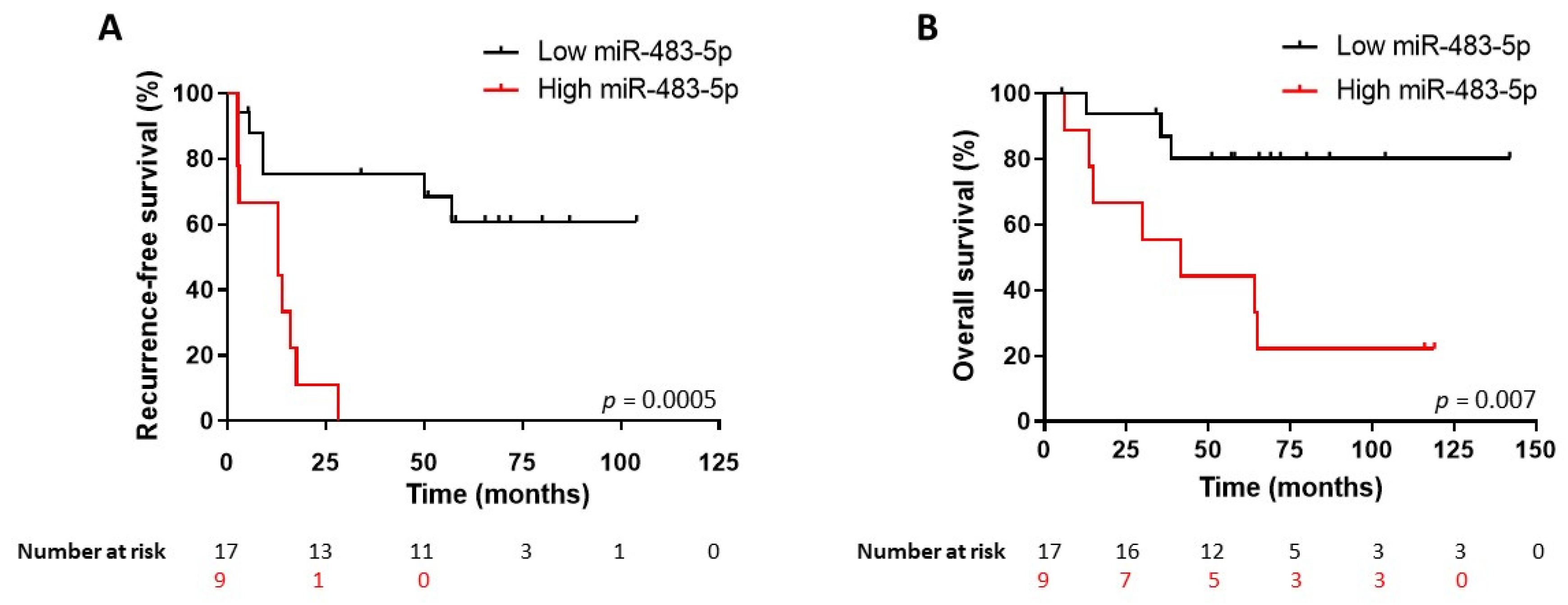
2.3. Survival Predictive Value of miR-483-5p Levels in 3 Months Post-Operative Serum Samples
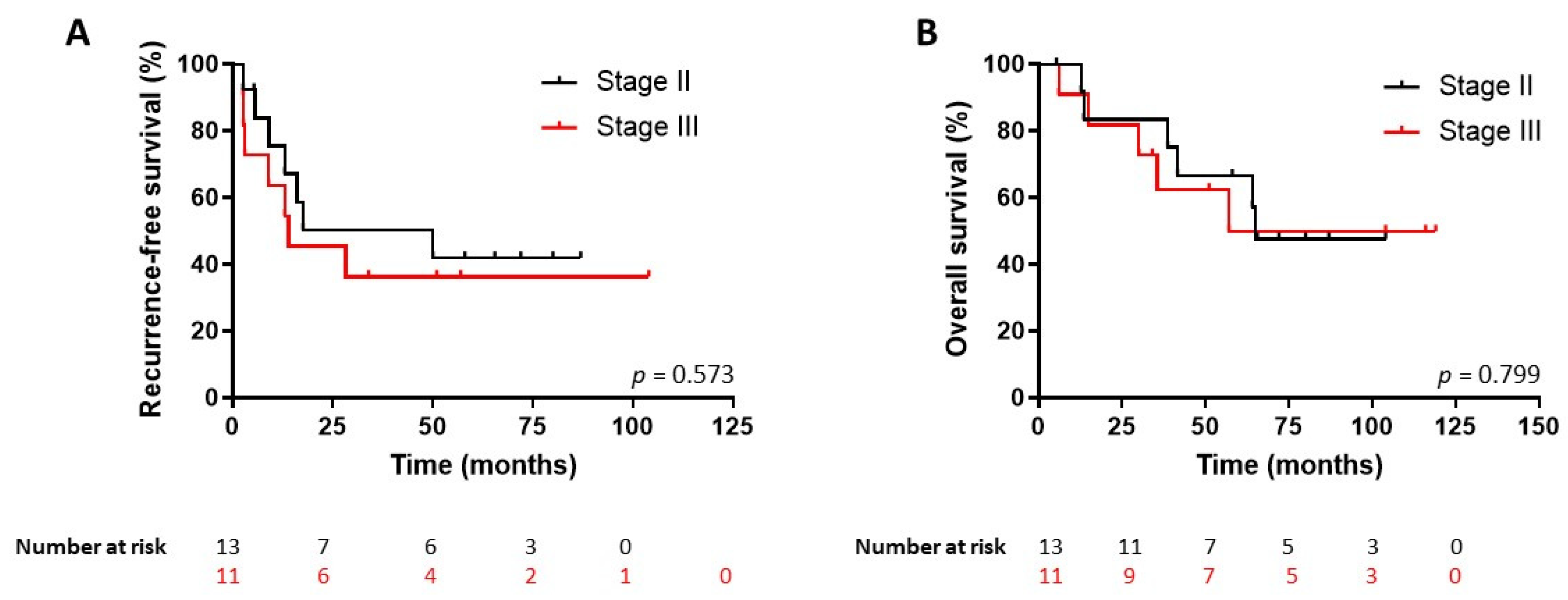
2.4. The Prognostic Value of miR-483-5p is Independent from Ki67 Index and Tumor Stage
3. Discussion
4. Materials and Methods
4.1. Patients and Clinical Samples
4.2. RNA Extraction
4.3. Quantification of Serum miRNA by Reverse Transcription-Quantitative PCR (RT-qPCR)
4.4. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Fassnacht, M.; Johanssen, S.; Quinkler, M.; Bucsky, P.; Willenberg, H.S.; Beuschlein, F.; Terzolo, M.; Mueller, H.H.; Hahner, S.; Allolio, B.; et al. Limited prognostic value of the 2004 International Union Against Cancer staging classification for adrenocortical carcinoma: Proposal for a Revised TNM Classification. Cancer 2009, 115, 243–250. [Google Scholar] [CrossRef]
- Else, T.; Kim, A.C.; Sabolch, A.; Raymond, V.M.; Kandathil, A.; Caoili, E.M.; Jolly, S.; Miller, B.S.; Giordano, T.J.; Hammer, G.D. Adrenocortical carcinoma. Endocr. Rev. 2014, 35, 282–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jouinot, A.; Bertherat, J. Management of endocrine disease: Adrenocortical carcinoma: Differentiating the good from the poor prognosis tumors. Eur. J. Endocrinol. 2018, 178, R215–R230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lughezzani, G.; Sun, M.; Perrotte, P.; Jeldres, C.; Alasker, A.; Isbarn, H.; Budaus, L.; Shariat, S.F.; Guazzoni, G.; Montorsi, F.; et al. The European Network for the Study of Adrenal Tumors staging system is prognostically superior to the international union against cancer-staging system: A North American validation. Eur. J. Cancer 2010, 46, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Chabre, O.; Libe, R.; Assie, G.; Barreau, O.; Bertherat, J.; Bertagna, X.; Feige, J.J.; Cherradi, N. Serum miR-483-5p and miR-195 are predictive of recurrence risk in adrenocortical cancer patients. Endocr. Relat. Cancer 2013, 20, 579–594. [Google Scholar] [CrossRef] [PubMed]
- Ambros, V. The functions of animal microRNAs. Nature 2004, 431, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Cherradi, N. microRNAs as Potential Biomarkers in Adrenocortical Cancer: Progress and Challenges. Front. Endocrinol. (Lausanne) 2015, 6, 195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozata, D.M.; Caramuta, S.; Velazquez-Fernandez, D.; Akcakaya, P.; Xie, H.; Hoog, A.; Zedenius, J.; Backdahl, M.; Larsson, C.; Lui, W.O. The role of microRNA deregulation in the pathogenesis of adrenocortical carcinoma. Endocr. Relat. Cancer 2011, 18, 643–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, E.E.; Holloway, A.K.; Weng, J.; Fojo, T.; Kebebew, E. MicroRNA profiling of adrenocortical tumors reveals miR-483 as a marker of malignancy. Cancer 2011, 117, 1630–1639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soon, P.S.; Tacon, L.J.; Gill, A.J.; Bambach, C.P.; Sywak, M.S.; Campbell, P.R.; Yeh, M.W.; Wong, S.G.; Clifton-Bligh, R.J.; Robinson, B.G.; et al. miR-195 and miR-483-5p Identified as Predictors of Poor Prognosis in Adrenocortical Cancer. Clin. Cancer Res. 2009, 15, 7684–7692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assie, G.; Letouze, E.; Fassnacht, M.; Jouinot, A.; Luscap, W.; Barreau, O.; Omeiri, H.; Rodriguez, S.; Perlemoine, K.; Rene-Corail, F.; et al. Integrated genomic characterization of adrenocortical carcinoma. Nat. Genet. 2014, 46, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Patel, D.; Boufraqech, M.; Jain, M.; Zhang, L.; He, M.; Gesuwan, K.; Gulati, N.; Nilubol, N.; Fojo, T.; Kebebew, E. MiR-34a and miR-483-5p are candidate serum biomarkers for adrenocortical tumors. Surgery 2013, 154, 1224–1228, discussion 1229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szabo, D.R.; Luconi, M.; Szabo, P.M.; Toth, M.; Szucs, N.; Horanyi, J.; Nagy, Z.; Mannelli, M.; Patocs, A.; Racz, K.; et al. Analysis of circulating microRNAs in adrenocortical tumors. Lab. Investig. 2014, 94, 331–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvianti, F.; Canu, L.; Poli, G.; Armignacco, R.; Scatena, C.; Cantini, G.; Di Franco, A.; Gelmini, S.; Ercolino, T.; Pazzagli, M.; et al. New insights in the clinical and translational relevance of miR483-5p in adrenocortical cancer. Oncotarget 2017, 8, 65525–65533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perge, P.; Butz, H.; Pezzani, R.; Bancos, I.; Nagy, Z.; Paloczi, K.; Nyiro, G.; Decmann, A.; Pap, E.; Luconi, M.; et al. Evaluation and diagnostic potential of circulating extracellular vesicle-associated microRNAs in adrenocortical tumors. Sci. Rep. 2017, 7, 5474. [Google Scholar] [CrossRef] [PubMed]
- Fassnacht, M.; Dekkers, O.M.; Else, T.; Baudin, E.; Berruti, A.; de Krijger, R.; Haak, H.R.; Mihai, R.; Assie, G.; Terzolo, M. European Society of Endocrinology Clinical Practice Guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors. Eur. J. Endocrinol. 2018, 179, G1–G46. [Google Scholar] [CrossRef] [PubMed]
- Agosta, C.; Laugier, J.; Guyon, L.; Denis, J.; Bertherat, J.; Libe, R.; Boisson, B.; Sturm, N.; Feige, J.J.; Chabre, O.; et al. MiR-483-5p and miR-139-5p promote aggressiveness by targeting N-myc downstream-regulated gene family members in adrenocortical cancer. Int. J. Cancer 2018, 143, 944–957. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tkach, M.; Thery, C. Communication by Extracellular Vesicles: Where We Are and Where We Need to Go. Cell 2016, 164, 1226–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Age | Sex | Ensat Stage | Mitotane Post-op Adjuvant Therapy | Recur-rence | Time to Recurrence (Months) | Death | Time to Death (Months) | Last Follow-up Without Recurrence or Death (Months) | Group |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 38 | F | I | N | N | - | N | - | 69 | NR3yrs |
| 2 | 30 | F | II | N | N | - | N | - | 5.3 | - |
| 3 | 60 | M | II | N | N | - | N | - | 58 | NR3yrs |
| 4 | 52 | F | II | Y | N | - | N | - | 72 | NR3yrs |
| 5 | 70 | F | II | Y a | N | - | N | - | 80 | NR3yrs |
| 6 | 46 | F | II | Y | N | - | N | - | 87 | NR3yrs |
| 7 | 21 | M | II | Y | N | - | N | - | 65.5 | NR3yrs |
| 8 | 48 | F | III | Y a | N | - | N | - | 57 | NR3yrs |
| 9 | 64 | M | III | N | N | - | N | - | 51 | NR3yrs |
| 10 | 70 | F | III | Y | N | - | N | - | 104 | NR3yrs |
| 11 | 53 | M | III | Y | N | - | N | - | 34 | - |
| 12 | 44 | F | I | N | Y | 57 | N | - | 142 | NR3yrs |
| 13 | 42 | F | II | Y | Y | 50 | N | - | 104 | NR3yrs |
| 14 | 59 | F | II | Y | Y | 5.65 | Y | 12.7 | - | R < 3yrs |
| 15 | 56 | M | II | Y | Y | 2.6 | Y | 13.5 | - | R < 3yrs |
| 16 | 40 | F | II | N b | Y | 9.1 | Y | 38.7 | - | R < 3yrs |
| 17 | 66 | F | II | N b | Y | 17.6 | Y | 41.6 | - | R < 3yrs |
| 18 | 46 | F | II | N b | Y | 13 | Y | 64 | - | R < 3yrs |
| 19 | 42 | M | II | Y | Y | 16 | Y | 65 | - | R < 3yrs |
| 20 | 62 | M | III | Y | Y | 9 | Y | 57 | - | R < 3yrs |
| 21 | 51 | F | III | Y | Y | 3 | Y | 6 | - | R < 3yrs |
| 22 | 78 | F | III | Y | Y | 2.7 | Y | 14.9 | - | R < 3yrs |
| 23 | 37 | M | III | Y | Y | 13 | Y | 30 | - | R < 3yrs |
| 24 | 47 | F | III | Y | Y | 2.6 | Y | 35.5 | - | R < 3yrs |
| 25 | 47 | M | III | Y | Y | 14 | N | - | 119 | R < 3yrs |
| 26 | 43 | F | III | Y | Y | 28.3 | N | - | 116 | R < 3yrs |
| Variable | OS | RFS | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Age | 1.02 | 0.97–1.07 | 0.373 | 1.01 | 0.97–1.05 | 0.601 |
| Sex | 0.90 | 0.26–3.08 | 0.862 | 0.87 | 0.28–2.68 | 0.817 |
| Tumor size | 1.02 | 0.92–1.13 | 0.684 | 1.05 | 0.96–1.15 | 0.274 |
| Ki67 > 10% | 0.45 | 0.12–1.69 | 0.239 | 0.38 | 0.11–1.26 | 0.083 |
| ENSAT stage I–II vs. III | 0.70 | 0.21–2.33 | 0.566 | 0.54 | 0.18–1.61 | 0.269 |
| miR-483-5p cut-off | 2.79 | 0.85–9.19 | 0.090 | 4.84 | 1.53–15.3 | 0.007 |
| Variable | OS | RFS | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| Tumor size | 0.92 | 0.80–1.05 | 0.212 | 0.90 | 0.79–1.03 | 0.125 |
| Ki67 > 10% | 0.44 | 0.11–1.75 | 0.245 | 0.36 | 0.10–1.33 | 0.092 |
| ENSAT stage I–II vs. III | 0.41 | 0.09–1.92 | 0.260 | 0.28 | 0.06–1.32 | 0.109 |
| miR-483-5p cut-off | 3.11 | 0.66–14.6 | 0.150 | 5.98 | 1.30–27.6 | 0.011 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oreglia, M.; Sbiera, S.; Fassnacht, M.; Guyon, L.; Denis, J.; Cristante, J.; Chabre, O.; Cherradi, N. Early Postoperative Circulating miR-483-5p Is a Prognosis Marker for Adrenocortical Cancer. Cancers 2020, 12, 724. https://doi.org/10.3390/cancers12030724
Oreglia M, Sbiera S, Fassnacht M, Guyon L, Denis J, Cristante J, Chabre O, Cherradi N. Early Postoperative Circulating miR-483-5p Is a Prognosis Marker for Adrenocortical Cancer. Cancers. 2020; 12(3):724. https://doi.org/10.3390/cancers12030724
Chicago/Turabian StyleOreglia, Maurine, Silviu Sbiera, Martin Fassnacht, Laurent Guyon, Josiane Denis, Justine Cristante, Olivier Chabre, and Nadia Cherradi. 2020. "Early Postoperative Circulating miR-483-5p Is a Prognosis Marker for Adrenocortical Cancer" Cancers 12, no. 3: 724. https://doi.org/10.3390/cancers12030724