Development of a Prognostic Nomogram for Liver Metastasis of Uveal Melanoma Patients Selected by Liver MRI

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Univariate Analysis
2.2. Multivariate Analysis
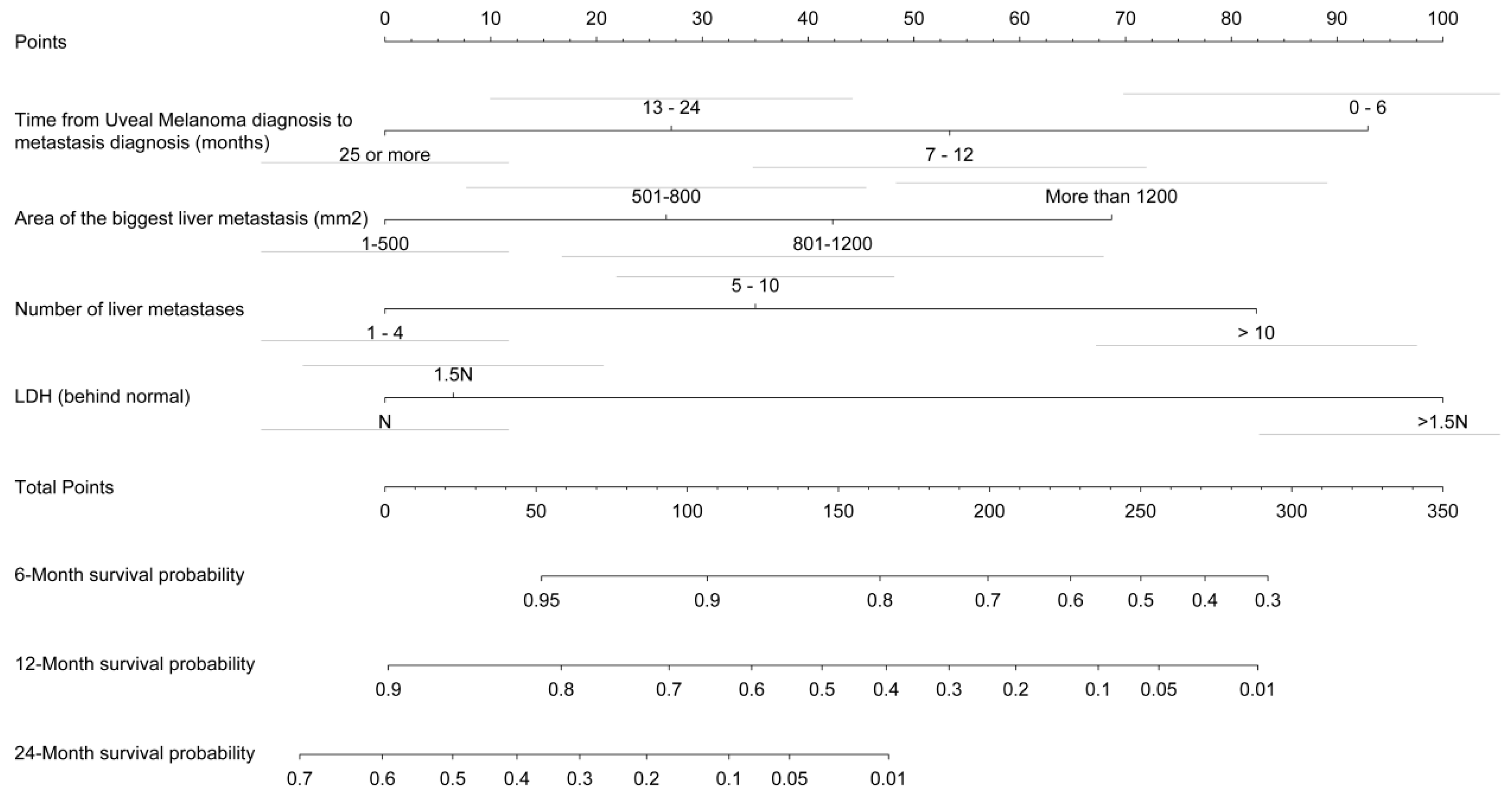
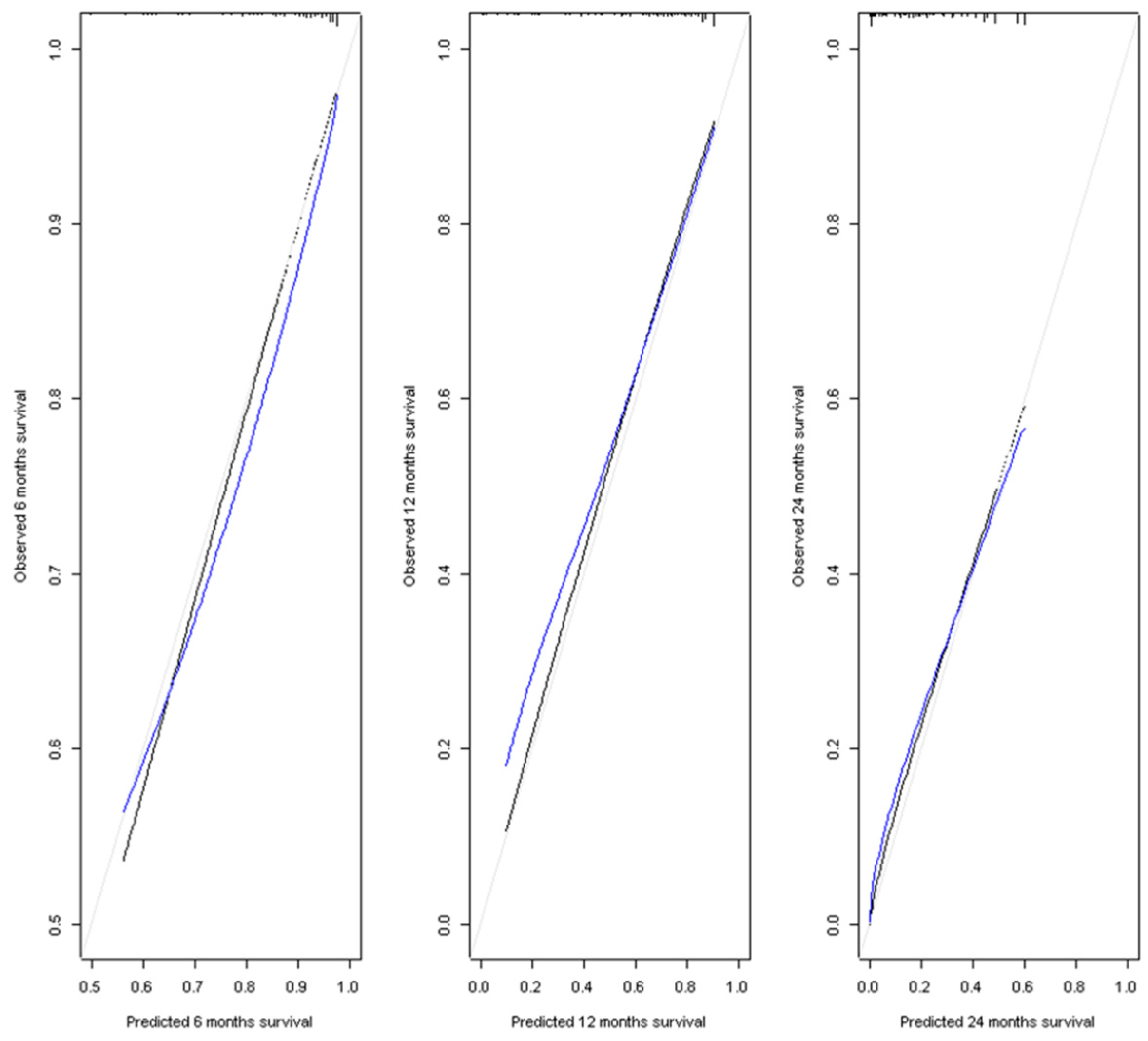
2.3. Prognostic Profile Nomogram
3. Discussion
3.1. Nomogram Interests
3.2. Nomogram Limitations
4. Materials and Methods
4.1. Study Design and Participants
4.2. Radiological Evaluation
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mallone, S.; De Vries, E.; Guzzo, M.; Midena, E.; Verne, J.; Coebergh, J.W.; Marcos-Gragera, R.; Ardanaz, E.; Martinez, R.; Chirlaque, M.D.; et al. Descriptive epidemiology of malignant mucosal and uveal melanomas and adnexal skin carcinomas in Europe. Eur. J. Cancer 2012, 48, 1167–1175. [Google Scholar] [CrossRef] [PubMed]
- Diener-West, M.; Reynolds, S.M.; Agugliaro, D.J.; Caldwell, R.; Cumming, K.; Earle, J.D.; Hawkins, B.S.; Hayman, J.A.; Jaiyesimi, I.; Jampol, L.M.; et al. Development of metastatic disease after enrollment in the COMS trials for treatment of choroidal melanoma: Collaborative Ocular Melanoma Study Group Report No. 26. Arch. Ophthalmol. 2005, 123, 1639–1643. [Google Scholar] [PubMed]
- Onken, M.D.; Worley, L.A.; Ehlers, J.P.; Harbour, J.W. Gene expression profiling in uveal melanoma reveals two molecular classes and predicts metastatic death. Cancer Res. 2004, 64, 7205–7209. [Google Scholar] [CrossRef] [PubMed]
- Cassoux, N.; Rodrigues, M.J.; Plancher, C.; Asselain, B.; Levy-Gabriel, C.; Lumbroso-Le Rouic, L.; Piperno-Neumann, S.; Dendale, R.; Sastre, X.; Desjardins, L.; et al. Genome-wide profiling is a clinically relevant and affordable prognostic test in posterior uveal melanoma. Br. J. Ophthalmol. 2014, 98, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.D.; Turell, M.E.; Topham, A.K. Uveal melanoma: Trends in incidence, treatment and survival. Ophtalmology 2011, 118, 1881–1885. [Google Scholar] [CrossRef] [PubMed]
- Kujala, E.; Damato, B.; Coupland, S.E.; Desjardins, L.; Bechrakis, N.E.; Grange, J.D.; Kivelä, T. Staging of ciliary body and choroidal melanomas based on anatomic extent. J. Clin. Oncol. 2013, 31, 2825–2831. [Google Scholar] [CrossRef] [PubMed]
- Carvajal, R.D.; Schwartz, G.K.; Tezel, T.; Marr, B.; Francis, J.H.; Nathan, P.D. Metastatic disease from uveal melanoma: Treatment option and future prospects. Br. J. Ophtalmol. 2017, 101, 38–44. [Google Scholar] [CrossRef]
- Bender, C.; Enk, A.; Gutzmer, R.; Hassel, J.C. Anti-PD-1 antibodies in metastatic uveal melanoma: A treatment option? Cancer Med. 2017, 6, 1581–1586. [Google Scholar] [CrossRef]
- Mariani, P.; Piperno-Neumann, S.; Servois, V.; Berry, M.G.; Dorval, T.; Plancher, C.; Couturier, J.; Levy-Gabriel, C.; Lumbroso-Le Rouic, L.; Desjardins, L.; et al. Surgical management of liver metastases from uveal melanoma: 16 years’ experience at the Institut Curie. Eur. J. Surg. Oncol. 2009, 35, 1192–1197. [Google Scholar] [CrossRef]
- Gomez, D.; Wetherill, C.; Cheong, J.; Jones, L.; Marshall, E.; Damato, B.; Coupland, S.E.; Ghaneh, P.; Poston, G.J.; Malik, H.Z.; et al. The Liverpool uveal melanoma liver metastases pathway: Outcome following liver resection. J. Surg. Oncol. 2014, 109, 542–547. [Google Scholar] [CrossRef]
- Mariani, P.; Almubarak, M.M.; Kollen, M.; Wagner, M.; Plancher, C.; Audollent, R.; Piperno-Neumann, S.; Cassoux, N.; Servois, V. Radiofrequency ablation and surgical resection of liver metastases from uveal melanoma. Eur. J. Surg. Oncol. 2016, 42, 706–710. [Google Scholar] [CrossRef] [PubMed]
- Leyvraz, S.; Piperno-Neumann, S.; Suciu, S.; Baurain, J.F.; Zdzienicki, M.; Testori, A.; Marshall, E.; Scheulen, M.; Jouary, T.; Negrier, S.; et al. Hepatic intra-arterial versus intravenous fotemustine in patients with liver metastases from uveal melanoma (EORTC 18021): A multicentric randomized trial. Ann. Oncol. 2014, 25, 742–746. [Google Scholar] [CrossRef] [PubMed]
- Olofsson, R.; Cahlin, C.; All-Ericsson, C.; Hashimi, F.; Mattsson, J.; Rizell, M.; Lindnér, P. Isolated hepatic perfusion for ocular melanoma metastasis: Registry data suggests a survival benefit. Ann. Surg. Oncol. 2014, 21, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shabat, I.; Belgrano, V.; Ny, L.; Nilsson, J.; Lindnér, P.; Olofsson Bagge, R. Long-term follow-up evaluation of 68 patients with uveal melanoma liver metastases treated with isolated hepatic perfusion. Ann. Surg. Oncol. 2016, 23, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Eschelman, D.J.; Gonsalves, C.F.; Sato, T. Transhepatic therapies for metastatic uveal melanoma. Semin. Intervent. Radiol. 2013, 30, 39–48. [Google Scholar] [PubMed]
- Mariani, P.; Servois, V.; Piperno-Neumann, S. Therapeutic options in metastatic uveal melanoma. Dev. Ophthalmol. 2012, 49, 166–181. [Google Scholar] [PubMed]
- Hsueh, E.C.; Essner, R.; Foshag, L.J.; Ye, X.; Wang, H.J.; Morton, D.L. Prolonged survival after complete resection of metastases from intraocular melanoma. Cancer 2004, 100, 122–129. [Google Scholar] [CrossRef]
- Buzzacco, D.M.; Abdel-Rahman, M.H.; Park, S.; Davidorf, F.; Olencki, T.; Cebulla, C.M. Long-term survivors with metastatic uveal melanoma. Open Ophtal. J. 2012, 6, 49–53. [Google Scholar] [CrossRef]
- Valpione, S.; Moser, J.C.; Parrozzani, R.; Bazzi, M.; Mansfield, A.S.; Mocellin, S.; Pigozzo, J.; Midena, E.; Markovic, S.N.; Aliberti, C.; et al. Development and external validation of a prognostic nomogram for metastatic uveal melanoma. PLoS ONE 2015, 10, e0120181. [Google Scholar] [CrossRef]
- Wagner, M.; Mariani, P.; Bidard, F.C.; Rodrigues, M.J.; Farkhondeh, F.; Cassoux, N.; Piperno-Neumann, S.; Petras, S.; Servois, V. Diffusion-weighted MRI for uveal melanoma liver metastasis detection. Eur. Radiol. 2015, 25, 2263–2273. [Google Scholar] [CrossRef]
- Niekel, M.C.; Bipat, S.; Stoker, J. Diagnostic imaging of colorectal liver metastases with CT, MR imaging, FDG PET, and/or FDG PET/CT: A meta-analysis of prospective studies including patients who have not previously undergone treatment. Radiology 2010, 257, 674–684. [Google Scholar] [CrossRef] [PubMed]
- Eiber, M.; Fingerle, A.A.; Brügel, M.; Gaa, J.; Rummeny, E.J.; Holzapfe, K. Detection and classification of focal liver lesions in patients with colorectal cancer: Retrospective comparison of diffusion-weighted MR imaging and multi-slice CT. Eur. J. Radiol. 2012, 81, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Gragoudas, E.S.; Egan, K.M.; Seddon, J.M.; Glynn, R.J.; Walsh, S.M.; Finn, S.M.; Munzenrider, J.E.; Spar, M.D. Survival of patients with metastases from uveal melanoma. Ophthalmology 1991, 98, 383–389. [Google Scholar] [CrossRef]
- Bedikian, A.Y.; Legha, S.S.; Mavligit, G.; Carrasco, C.H.; Khorana, S.; Plager, C.; Papadopoulos, N.; Benjamin, R.S. Treatment of uveal melanoma metastatic to the liver: A review of the M. D. Anderson Cancer Center experience and prognostic factors. Cancer 1995, 76, 1665–1670. [Google Scholar] [CrossRef]
- Eskelin, S.; Pyrhönen, S.; Hahka-Kemppinen, M.; Tuomaala, S.; Kivelä, T. A prognostic model and staging for metastatic uveal melanoma. Cancer 2003, 97, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Rietschel, P.; Panageas, K.S.; Hanlon, C.; Patel, A.; Abramson, D.H.; Chapman, P.B. Variates of survival in metastatic uveal melanoma. J. Clin. Oncol. 2005, 23, 8076–8080. [Google Scholar] [CrossRef] [PubMed]
- Kodjikian, L.; Grange, J.D.; Baldo, S.; Baillif, S.; Garweg, J.G.; Rivoire, M. Prognostic factors of liver metastases from uveal melanoma. Graefe’s Arch. Clin. Exp. Ophthalmol. 2005, 243, 985–993. [Google Scholar] [CrossRef] [Green Version]
- Pons, F.; Plana, M.; Caminal, J.M.; Pera, J.; Fernandes, I.; Perez, J.; Garcia-Del-Muro, X.; Marcoval, J.; Penin, R.; Fabra, A.; et al. Metastatic uveal melanoma: Is there a role for conventional chemotherapy? A single center study based on 58 patients. Melanoma Res. 2011, 21, 217–222. [Google Scholar] [CrossRef]
- Kivelä, T.T.; Piperno-Neumann, S.; Desjardins, L.; Schmittel, A.; Bechrakis, N.; Midena, E.; Leyvraz, S.; Zografos, L.; Grange, J.D.; Ract-Madoux, G.; et al. Validation of a prognostic staging for metastatic Uveal melanoma: A collaborative study of the European Ophthalmic Oncology Group. Am. J. Ophthalmol. 2016, 168, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo, D.; Ochoa, M.; Piulats, J.M.; Gutiérrez, C.; Arias, L.; Català, J.; Grau, M.; Peñafiel, J.; Cobos, E.; Garcia-Bru, P.; et al. Pronostic factors and decision tree for long-term survival in metastatic uveal melanoma. Cancer Res. Treat. 2018, 50, 1130–1139. [Google Scholar] [CrossRef]
- Nishino, M.; Jagannathan, J.P.; Ramaiya, N.H.; Van den Abbeele, A.D. Revised RECIST guideline version 1.1: What oncologists want to know and what radiologists need to know. Am. J. Roentgenol. 2010, 195, 281–289. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.B.; Hoogstraten, B.; Staquet, M.; Winkler, A. Reporting results of cancer treatment. Cancer 1981, 47, 207–214. [Google Scholar] [CrossRef]
- Warner, A.B.; Postow, M.A. Bigger is not always better: Tumor size and pronosis in advanced melanoma. Clin. Cancer Res. 2018, 24, 4915–4917. [Google Scholar] [CrossRef] [PubMed]
- Joseph, R.W.; Elassaiss-Schaap, J.; Kefford, R.; Hwu, W.J.; Wolchok, J.D.; Joshua, A.M.; Ribas, A.; Hodi, F.S.; Hamid, O.; Robert, C.; et al. Baseline tumor size is an independent prognostic factor for overall survival in patients with melanoma treated with Pembrolizumab. Clin. Cancer Res. 2018, 24, 4960–4967. [Google Scholar] [CrossRef] [PubMed]
- Bidard, F.C.; Madic, J.; Mariani, P.; Piperno-Neumann, S.; Rampanou, A.; Servois, V.; Cassoux, N.; Desjardins, L.; Milder, M.; Vaucher, I.; et al. Detection rate and prognostic value of circulating tumor cells and circulating tumor DNA in metastatic uveal melanoma. Int. J. Cancer 2014, 134, 1207–1213. [Google Scholar] [CrossRef]
- Madic, J.; Piperno-Neumann, S.; Servois, V.; Rampanou, A.; Milder, M.; Trouiller, B.; Gentien, D.; Saada, S.; Assayag, F.; Thuleau, A.; et al. Pyrophosphorolysis-activated polymerization detects circulating tumor DNA in metastatic uveal melanoma. Clin. Cancer Res. 2012, 18, 3934–3941. [Google Scholar] [CrossRef] [PubMed]
- Trolet, J.; Hupé, P.; Huon, I.; Lebigot, I.; Decraene, C.; Delattre, O.; Sastre-Garau, X.; Saule, S.; Thiéry, J.P.; Plancher, C.; et al. Genomic profiling and identification of high-risk uveal melanoma by array CGH analysis of primary tumors and liver metastases. Invest. Ophthalmol. Vis. Sci. 2009, 50, 2572–2580. [Google Scholar] [CrossRef]
- McCarthy, C.; Kalirai, H.; Lake, S.L.; Dodson, A.; Damato, B.E.; Coupland, S.E. Insights into genetic alterations of liver metastases from uveal melanoma. Pigment Cell Melanoma Res. 2016, 29, 60–67. [Google Scholar] [CrossRef]
- Griewank, K.G.; van de Nes, J.; Schilling, B.; Moll, I.; Sucker, A.; Kakavand, H.; Haydu, L.E.; Asher, M.; Zimmer, L.; Hillen, U.; et al. Genetic and clinico-pathologic analysis of metastatic uveal melanoma. Mod. Pathol. 2014, 27, 175–183. [Google Scholar] [CrossRef]
- Couinaud, C. Variations of the right bile ducts: The futility of complete anatomical classifications. Chirurgie 1993, 119, 354–356. [Google Scholar]



{kind=link}
{kind=link}
| Variables | Patients (n = 224) | % | HR (CI 0.95) | p |
|---|---|---|---|---|
| Sex | ||||
| M | 113 | 50.4 | 1 | |
| F | 111 | 49.6 | 0.93 (0.69–1.26) | 0.66 |
| Age at diagnosis of UM (year) | ||||
| Median value (IQR) | 57 (49–66) | |||
| ≤60 | 137 | 61.2 | 1 | |
| >60 | 87 | 38.8 | 1.68 (1.23–2.30) | 0.001 |
| Largest UM diameter (mm) (n = 221) | ||||
| Median value (IQR) | 17.1 (15–19.4) | |||
| <18 | 128 | 57.9 | 1 | |
| ≥18 | 93 | 42.1 | 1.14 | 0.41 |
| Ciliary body involvement (n = 211) | ||||
| No | 127 | 60.2 | 1 | |
| Yes | 84 | 39.8 | 1.42 (1.03–1.96) | 0.03 |
| Extra-scleral extension (n = 206) | ||||
| No | 191 | 92.7 | 1 | |
| Yes | 15 | 7.3 | 0.74 (0.40–1.37) | 0.34 |
| Treatment of UM | ||||
| Enucleation | 95 | 42.4 | 1 | |
| Proton beam radiotherapy | 129 | 57.6 | 0.76 (0.56–1.03) | 0.07 |
| Genomic analysis of UM (n = 97) | ||||
| High | 78 | 80.4 | 1 | |
| Intermediate | 18 |  | 1.06 (0.54–2.08) | 0.87 |
| Low | 1 | |||
| Disease-Free Interval between UM and LMUM | ||||
| Median value (IQR) | 26.1 (13.6–41.4) | |||
| 0–6 months | 16 | 7.2 | 2.35 (1.35–4.1) | 0.003 |
| 6–12 months | 31 | 13.8 | 1.54 (0.97–2.44) | 0.07 |
| 12–24 months | 52 | 23.2 | 1.74 (1.19–2.53) | 0.004 |
| >24 months | 125 | 55.8 | 1 | |
| Concomitant extrahepatic disease (n = 220) | ||||
| No | 199 | 90.5 | 1 | |
| Yes | 21 | 9.5 | 2.03 (1.31–3.16) | 0.002 |
| First treatment of LMUM | ||||
| Surgery | 60 | 30.5 | 1 | |
| Systemic | 123 | 62.4 | 2.75 (1.80–4.2) | <0.001 |
| Best supportive care | 14 | 7.1 | 2.73 (1.43–5.24) | <0.002 |
| PS | ||||
| 0 | 160 | 71.4 | 1 | |
| 1 | 54 | 24.1 | ||
| 2 | 9 | 4 | 1.87 (0.95–3.67) | 0.07 |
| 3 | 1 | 0.4 | ||
| LDH (n = 221) | ||||
| Median value (IQR) | 394 (305–495) | |||
| ≤N | 108 | 48.9 | 1 | |
| >N–≤1.5N | 78 | 35.3 | 1.30 (0.93–1.83) | 0.13 |
| >1.5N | 35 | 15.8 | 4.15 (2.71–6.33) | <0.001 |
| Localization of liver metastases | ||||
| Bilobar | 147 | 65.6 | 1 | |
| Right lobe | 65 | 29 | 0.66 (0.46–0.94) | 0.02 |
| Left lobe | 12 | 5.4 | 0.62 (0.31–1.23) | 0.16 |
| Number of liver segments involved (MRI) | ||||
| 1 to 3 | 119 | 53.1 | 1 | |
| 4 to 6 | 66 | 29.5 | 1.32 (0.94–1.86) | 0.11 |
| 7 to 8 | 39 | 17.4 | 3.57 (2.34–5.44) | <0.001 |
| LMUM number (MRI) | ||||
| 1 to 4 | 109 | 48.7 | 1 | |
| 5 to 10 | 57 | 25.4 | 1.27 (0.87–1.83) | 0.22 |
| >10 | 58 | 25.9 | 2.89 (2.0–4.18) | <0.001 |
| LMUM largest size (mm2) (MRI) | ||||
| Median value (IQR) | 361 (144–784) | |||
| [1–500] | 143 | 63.8 | 1 | |
| [501–800] | 27 | 12.1 | 1.17 (0.74–1.86) | 0.51 |
| [801–1200] | 20 | 8.9 | 2.56 (1.56–4.19) | <0.001 |
| [1201– | 34 | 15.2 | 3.28 (2.14–5.02) | <0.001 |
| Miliary (MRI) | ||||
| No | 107 | 47.8 | 1 | |
| Yes | 117 | 52.2 | 1.43 (1.06–1.94) | 0.02 |
| Variables | HR (CI 0.95) | p |
|---|---|---|
| Disease Free Interval between UM and LMUM | ||
| >24 months | 1 | |
| 12–24 months | 1.43 (0.94–2.16) | 0.09 |
| 6–12 months | 2.02 (1.24–3.27) | 0.004 |
| 0–6 months | 3.39 (1.90–6.05) | <0.001 |
| LDH | ||
| ≤N | 1 | |
| >N–≤1.5N | 1.09 (0.75–1.57) | 0.65 |
| >1.5N | 3.72 (2.30–6.00) | <0.001 |
| LMUM number (MRI) | ||
| [1–4] | 1 | |
| [5–10] | 1.58 (1.07–2.33) | 0.02 |
| >10 | 2.95 (1.97–4.43) | <0.001 |
| LMUM largest size (mm2) (MRI) | ||
| [1–500] | 1 | |
| [501–800] | 1.42 (0.88–2.28) | 0.15 |
| [801–1200] | 1.74 (1.00–3.05) | 0.05 |
| [1201– | 2.47 (1.53–3.98) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mariani, P.; Dureau, S.; Savignoni, A.; Rouic, L.L.-L.; Levy-Gabriel, C.; Piperno-Neumann, S.; Rodrigues, M.J.; Desjardins, L.; Cassoux, N.; Servois, V. Development of a Prognostic Nomogram for Liver Metastasis of Uveal Melanoma Patients Selected by Liver MRI. Cancers 2019, 11, 863. https://doi.org/10.3390/cancers11060863
Mariani P, Dureau S, Savignoni A, Rouic LL-L, Levy-Gabriel C, Piperno-Neumann S, Rodrigues MJ, Desjardins L, Cassoux N, Servois V. Development of a Prognostic Nomogram for Liver Metastasis of Uveal Melanoma Patients Selected by Liver MRI. Cancers. 2019; 11(6):863. https://doi.org/10.3390/cancers11060863
Chicago/Turabian StyleMariani, Pascale, Sylvain Dureau, Alexia Savignoni, Livia Lumbroso-Le Rouic, Christine Levy-Gabriel, Sophie Piperno-Neumann, Manuel J. Rodrigues, Laurence Desjardins, Nathalie Cassoux, and Vincent Servois. 2019. "Development of a Prognostic Nomogram for Liver Metastasis of Uveal Melanoma Patients Selected by Liver MRI" Cancers 11, no. 6: 863. https://doi.org/10.3390/cancers11060863