1. Introduction
Internet gaming disorder (IGD) has been included by the American Psychiatric Association (APA) in the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) [
1] as a new condition that requires further research evidence. IGD has been defined as featured by a “persistent and recurrent” use of the Internet for gaming that leads to significant impairment and distress in several areas of functioning [
1]. IGD currently refers to the specific dimension of pathological online gaming, although numerous other terms have been suggested in the literature to describe the pathological use of technological devices such as Internet addiction [
2], problematic Internet use [
3], Internet use disorder [
4], smartphone addiction [
5], etc. IGD is also under debate among clinicians and researchers since, even though the DSM-5 defined it as a separate diagnostic category, the evidence from the literature demonstrates its comorbid presence within several different psychiatric disorders. Therefore, this would lead to considering it as an epiphenomenon of other clinical conditions with which it is associated [
4], making it difficult to find it as a single disorder in patients. Specifically, IGD appears to be often associated with conditions featured by social withdrawal [
6], such as anxiety and depression [
7], and it is plausible to hypothesize that Internet gaming represents a way of keeping social relationships that would be otherwise precluded and limited in real life [
6], which also accounts for the frequent comorbidity with autism spectrum disorder (ASD) [
8]. Furthermore, several studies in the literature have found associations between attention deficit and hyperactivity disorder (ADHD) and Internet gaming disorder [
9,
10], as well as for behavioral disorders closely connected to ADHD such as oppositional defiant disorder [
11].
By definition, ASD is characterized by persistent deficits in social communication and social interaction in multiple contexts, which manifest themselves specifically in deficits in socio-emotional reciprocity. These are associated with restricted and repetitive patterns of behavior, interests, or activities [
1]. A recent review [
12] found a significant association between these two conditions. The main hypotheses regarding the association between IGD and ASD evaluated the use of video games as a tool for “facilitating” relationships with peers [
13], as well as the possibility that the better visuospatial abilities typically found in autistic patients make them skilled in gaming, which requires identifying numerous stimuli in complex virtual environments [
14]. However, many of the reported studies are based on adult patients and differences can be found in the use of standardized tests to investigate IGD [
12].
ADHD instead is a condition characterized by a persistent pattern of inattention and/or hyperactivity–impulsivity that interferes with functioning or development [
1]. It has been widely highlighted in the literature that ADHD can be a significant predictor of both substance use disorder [
15] and behavioral addictions [
16], as these disorders share neuropsychological characteristics with ADHD [
17,
18]. A recent systematic review summarized 29 studies evaluating the association between ADHD and gaming disorder, of which only 11 were based on clinical samples [
19]. The review found a consistent positive association between ADHD and IGD, either in clinical-based or community-based samples, particularly for the inattention subscale. In contrast, hyperactivity was less commonly associated with IGD.
Although the literature has consistently found associations between IGD and both clinical ASD and ADHD, there are only a few studies on such associations in the pediatric population [
12,
19]. Furthermore, there is only one study that evaluated the IGD symptoms in both ASD and ADHD in a pediatric population [
20]. According to this, the present study has the following objectives: (1) investigating the prevalence of IGD in a population of pediatric patients diagnosed with ASD and comparing it with that of a population of pediatric patients with ADHD and to a control sample; and (2) describing the psychopathological and neuropsychological profile of patients with ASD and IGD compared with ASD patients without IGD and comparing it with that of ADHD patients. Moreover, we aimed to longitudinally assess the effectiveness of clinical monitoring and pharmacological and/or psychotherapeutic treatment on the reduction in IGD symptoms in a population of patients suffering from ASD.
4. Discussion
Internet addiction and more specifically Internet gaming disorder (IGD) are recently introduced diagnostic categories, often comorbid with other psychiatric disorders [
7]. In the literature, ADHD is typically associated with a greater risk of developing IGD [
10], although the clinical phenotype of ADHD patients with comorbid IGD is currently poorly described. Similarly, patients with ASD tend to be more prone to excessive use of technological devices [
38,
39]. However, only one study so far compared the clinical characteristics of IGD in ADHD and ASD pediatric patients [
20]. The first objective of the present study was to evaluate IGD prevalence in a sample of pediatric patients with ASD and to compare it with a group of ADHD patients, as well as with a group of healthy controls. Previous studies reported variable rates of prevalence in this clinical population likely because IGD symptoms have been measured by means of multiple instruments and in adult populations [
12]. Moreover, we aimed to compare ASD patients with and without comorbid IGD, in order to characterize those who are at higher risk of this behavioral addiction. As already highlighted by other studies in the literature, our study supports the idea that patients with ADHD and ASD have a greater risk of developing IGD, given the greatly higher rate of patients in both groups exceeding the IGDS9-SF cut-off compared with the control population. Specifically, patients with ADHD are those with the highest prevalence of IGD, followed by patients with ASD. The association between IGD and ADHD can be easily explained by the psychological features of ADHD itself, such as the impulsive need for a quick reward, as well as by the tendency toward sensation-seeking behaviors, which are provided by video games and Internet (which is indeed supported by functional MRI evidence of a common neurobiological pattern between the two disorders [
40]); moreover, the association between ASD and IGD could be related instead, as already mentioned, both to greater visual skills often present in people with ASD [
14] and the possibility to use electronic devices as a possible tool to “facilitate” relationships with others [
41]. In order to better clarify this association in patients with ASD, we investigated the clinical and cognitive characteristics of ASD patients with IGDS9-SF scores above the clinical cut-off. Overall, the clinical features of ASD patients with scores above the cut-off on the IGDS9-SF are largely comparable to patients with scores below the cut-off, as are the indices assessed on cognitive tests. Furthermore, no clinically significant differences were found in ASD core symptoms; this evidence was already found in a pediatric population in a 2013 study [
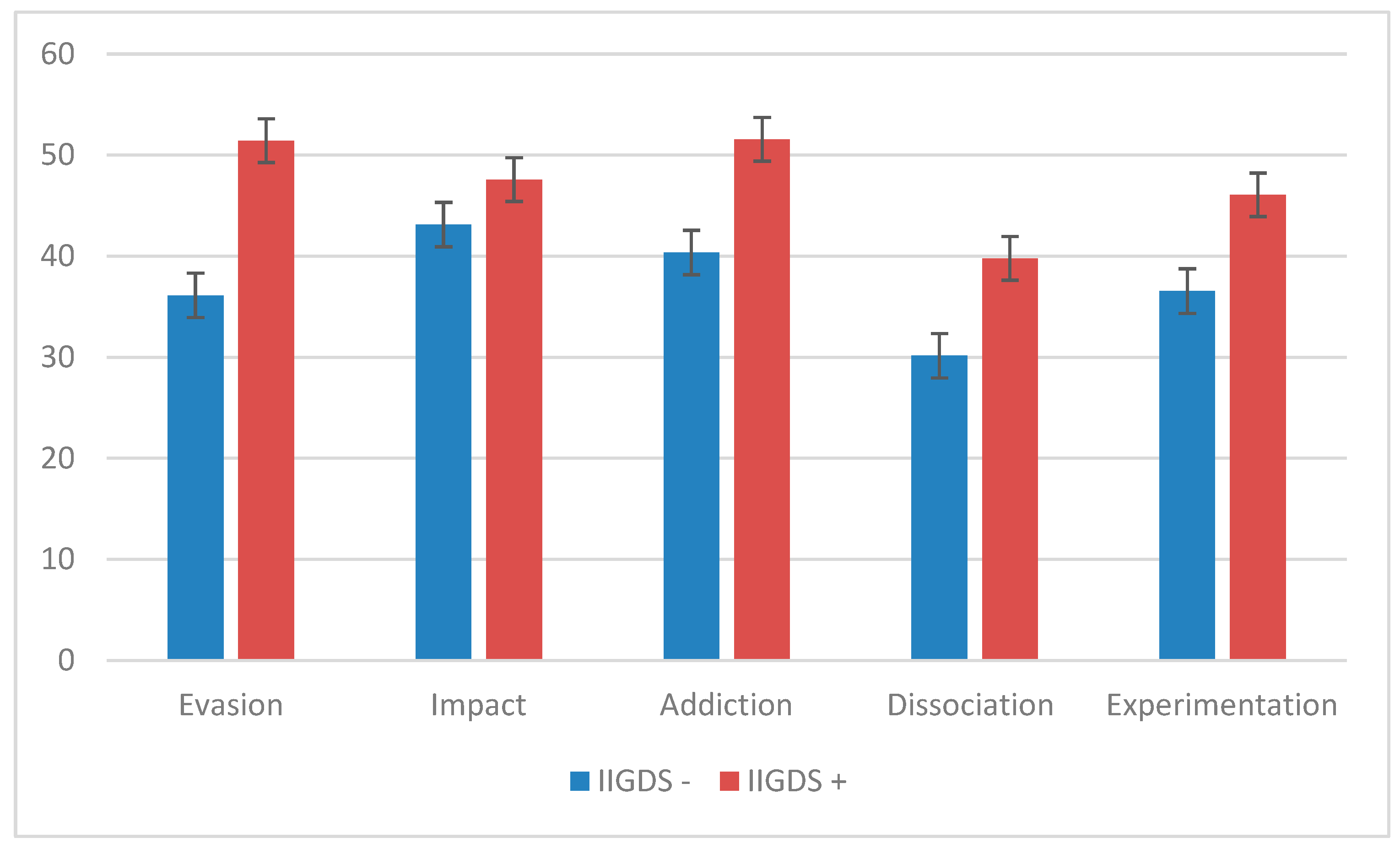
20], even if in that case the assessment of autistic symptoms was carried out only by using SCQ, suggesting that the extent of ASD-specific symptoms does not correlate with the presence of IGD. The greatest differences have been found in attention difficulties, investigated using the related syndromic subscale of the CBCL, configuring a phenotype of patients who tend to show a more severe clinical picture. It is also noted that, overall, all the dimensions investigated in the UADI test are highly represented in patients with IGDS9-SF scores higher than the cut-off and, in particular, the dimensions of “dependence” and “evasion”. This evidence was also found in a group of pediatric ADHD patients [
42], suggesting that, similarly, patients with ADHD and patients with ASD are more inclined to escape from the real world and dissociate from reality, despite those with addictive and sensation-seeking tendencies being at greater risk of developing IGD. These data are in line with previous studies that showed a marked tendency of ASD patients to use the Internet and video games as a form of escape rather than as a simpler and less anxiety-provoking form of communication [
43]. The neuropsychological profile that emerged by comparing the subscales of the WISC-IV and the WAIS-IV showed no differences between the ASD patients who were screened as positive and negative at the IGD standardized tests. This suggests that the cognitive profile does not influence the initial propensity to develop Internet addictions, as found in a pediatric study on ADHD patients [
42].
Subsequently, we compared, by using the CGAS and CGI clinical scales and the CBCL 6–18 questionnaire, the group of ASD patients and IGDS9-SF scores above the cut-off with the group of ADHD patients and IGDS9-SF scores above the cut-off; similarly, a comparison was made between the group of ASD patients and IGDS9-SF scores below the cut-off with the group of ADHD patients and IGDS9-SF scores below the cut-off. In both cases, the ASD patient group was, albeit slightly, clinically more severe than the ADHD patient group. In the first comparison, ADHD patients showed higher values in the subscales concerning externalizing problems and disruptive behaviors, while in ASD patients higher scores have been found in the subscale concerning withdrawn/depressive symptoms. In the second comparison, the group of ASD patients presented higher scores in the subscales concerning internalizing problems, anxious/depressive symptoms, and somatic problems. The differences found in the CBCL 6–18 appear, in general, to be attributable to the main clinical condition of the patients, therefore not configuring a peculiar psychopathological profile. It appears important to consider how the various overlaps present within the groups can be partly explained by the frequent comorbidity between ASD and ADHD within the ASD clinical group (but not in the ADHD clinical group), also suggesting the possibility that the characteristics of the two disorders cannot be completely separated and that further studies with larger sample sizes and, especially, with samples of ASD patients without comorbid ADHD could highlight this distinction, which could have relevant implications for identifying personalized therapeutic approaches. In light of these results, in the second phase of the study, we aimed to verify whether psychiatric monitoring and pharmacological and/or psychotherapeutic treatment could be effective in reducing the symptoms of Internet gaming disorder. The results obtained in our sample of ASD patients highlighted a global improvement in the patients’ clinical pictures, assessed using CGAS and CGI. However, no significant improvements were found in the scores of the video addiction tests, nor in the scores assessed on the CBCL 6–18.
However, the generalizability of our findings may be prevented by some limitations in the study design. First, it must be considered that (1) drug prescription was based on the main clinical picture of the patient and not on the presence of IGD, as no specific pharmacological treatments are currently available for this disorder; (2) the small size of our sample leads to less consistency in drawing statistically reliable conclusions; (3) the duration of the follow-up was between 4 and 6 months, thus preventing any improvements to be assessed over a longer period of time; and (4) the number and type of pharmacological and psychotherapeutic treatments and the association between these was particularly heterogeneous, a detail that prevented a direct comparison between the different treatments implemented. Furthermore, the type of study did not allow a comparison with a placebo condition. The wide age range can be also considered as a limitation of the study, as the clinical manifestation of both ASD and ADHD can change over time.
In a similar study conducted on pediatric ADHD patients [
42], the “follow-up” variable was associated with a significant reduction in IGD symptoms, while pharmacological treatment did not show the same association. In our sample of ASD patients, the follow-up, although it showed a significant association with improvement from a clinical point of view (measured with CGI) and social adaptability (measured with CGAS), did not show any association with improvement in addiction symptoms. Since the design of the two studies is largely comparable, this difference could be an indication of the fact that the diagnosis of ASD could represent a negative prognostic factor in the long-term regarding Internet gaming disorder compared with ADHD. This conclusion could be also supported by some literature evidence, as specific pharmacological treatments are currently available for ADHD and not for ASD, which have also shown some evidence of effectiveness on IGD symptoms in two studies [
44,
45], although both studies present some limitations that may raise doubts about the real effectiveness of this pharmacological treatment. These studies, combined with the evidence on the neurobiological mechanisms common between ADHD and IGD [
40,
46], suggest that if the greater sensitivity to immediate reward mechanisms (not surprisingly stimulated by video games) may be implicated in a greater prevalence of IGD in ADHD patients, the same mechanisms can be a potential target for pharmacological treatments.
Finally, several studies highlight that, concerning addictions to electronic devices [
47] and other behavioral addictions [
48], no specific “projectiles” or “magic bullets” have been put in place yet [
48]; therefore, it is preferable to set up multimodal treatments, based not only on pharmacological but also psychoeducational and psychological therapies [
47].



 ,
, 

{kind=link}