
An Update on the Efficacy of Single and Serial Intravenous Ketamine Infusions and Esketamine for Bipolar Depression: A Systematic Review and Meta-Analysis
 , ,
, ,
Abstract
:1. Introduction
2. Methods

2.1. Data Sources and Search Strategies
2.2. Study Selection
2.3. Data Collection
2.4. Methodological Quality and Risk of Bias Assessment
2.5. Statistical Analyses
3. Results
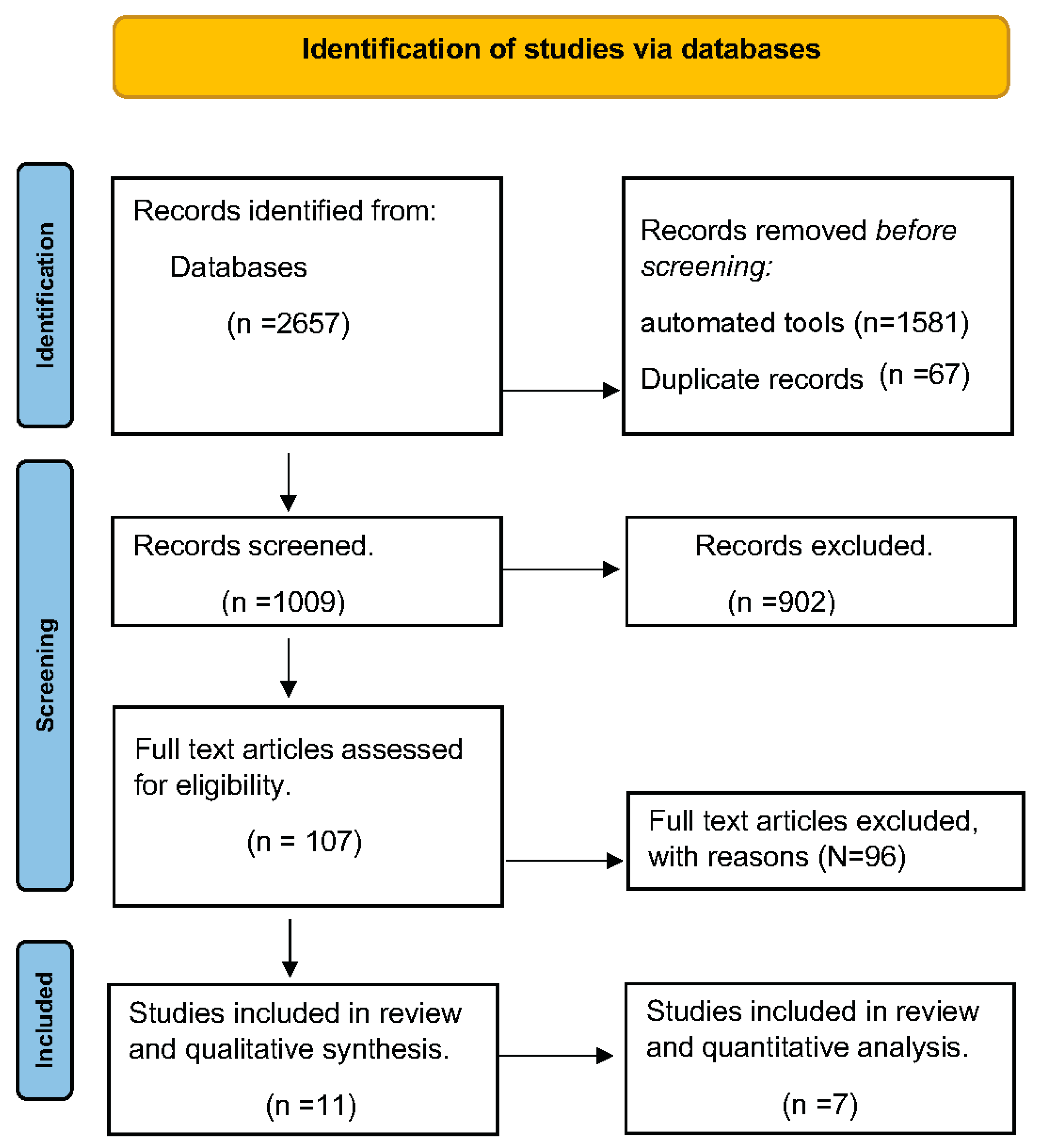
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Methodological Quality and Risk of Bias Assessment
3.4. Adverse Events
4. Discussion
4.1. Strengths and Limitations
4.2. Clinical Considerations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Judd, L.L.; Schettler, P.J.; Akiskal, H.S. The prevalence, clinical relevance, and public health significance of subthreshold depressions. Psychiatr. Clin. 2002, 25, 685–698. [Google Scholar] [CrossRef] [PubMed]
- Merikangas, K.R.; Jin, R.; He, J.P.; Kessler, R.C.; Lee, S.; Sampson, N.A.; Viana, M.C.; Andrade, L.H.; Hu, C.; Karam, E.G.; et al. Prevalence and correlates of bipolar spectrum disorder in the world mental health survey initiative. Arch. Gen. Psychiatry 2011, 68, 241–251. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, R.S.; Cha, D.S.; Kim, R.D.; Mansur, R.B. A review of FDA-approved treatment options in bipolar depression. CNS Spectr. 2013, 18, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, O.H.; Ercis, M.; Pahwa, M.; Singh, B. Treatment-resistant bipolar depression: Therapeutic trends, challenges and future directions. Neuropsychiatr. Dis. Treat. 2022, 18, 2927–2943. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Vande Voort, J.L.; Frye, M.A.; Kung, S. Can ketamine be a safe option for treatment-resistant bipolar depression? Expert Opin. Drug Saf. 2022, 21, 717–720. [Google Scholar] [CrossRef] [PubMed]
- Solovitch, S. Onetime party drug hailed as miracle for treating severe depression. The Washington Post, 1 February 2016. [Google Scholar]
- Singh, B.; Romo-Nava, F.; Cuellar-Barboza, A.B. Neurobiological Underpinnings of Bipolar Disorder and Its Treatment. Front. Psychiatry 2021, 12, 726362. [Google Scholar] [CrossRef]
- Wilkinson, S.T.; Ballard, E.D.; Bloch, M.H.; Mathew, S.J.; Murrough, J.W.; Feder, A.; Sos, P.; Wang, G.; Zarate, C.A., Jr.; Sanacora, G. The effect of a single dose of intravenous ketamine on suicidal ideation: A systematic review and individual participant data meta-analysis. Am. J. Psychiatry 2018, 175, 150–158. [Google Scholar] [CrossRef]
- Joseph, B.; Parsaik, A.K.; Ahmed, A.T.; Erwin, P.J.; Singh, B. A systematic review on the efficacy of intravenous racemic ketamine for bipolar depression. J. Clin. Psychopharmacol. 2021, 41, 71–75. [Google Scholar] [CrossRef]
- Kryst, J.; Kawalec, P.; Pilc, A. Efficacy and safety of intranasal esketamine for the treatment of major depressive disorder. Expert Opin. Pharmacother. 2020, 21, 9–20. [Google Scholar] [CrossRef]
- Correia-Melo, F.S.; Leal, G.C.; Vieira, F.; Jesus-Nunes, A.P.; Mello, R.P.; Magnavita, G.; Caliman-Fontes, A.T.; Echegaray, M.V.; Bandeira, I.D.; Silva, S.S.; et al. Efficacy and safety of adjunctive therapy using esketamine or racemic ketamine for adult treatment-resistant depression: A randomized, double-blind, non-inferiority study. J. Affect. Disord. 2020, 264, 527–534. [Google Scholar] [CrossRef]
- Medeiros, G.C.; Gould, T.D.; Prueitt, W.L.; Nanavati, J.; Grunebaum, M.F.; Farber, N.B.; Singh, B.; Selvaraj, S.; Machado-Vieira, R.; Achtyes, E.D.; et al. Blood-based biomarkers of antidepressant response to ketamine and esketamine: A systematic review and meta-analysis. Mol. Psychiatry 2022, 27, 3658–3669. [Google Scholar] [CrossRef]
- Rasmussen, K.G.; Lineberry, T.W.; Galardy, C.W.; Kung, S.; Lapid, M.I.; Palmer, B.A.; Ritter, M.J.; Schak, K.M.; Sola, C.L.; Hanson, A.J.; et al. Serial infusions of low-dose ketamine for major depression. J. Psychopharmacol. 2013, 27, 444–450. [Google Scholar] [CrossRef]
- Murrough, J.W.; Perez, A.M.; Pillemer, S.; Stern, J.; Parides, M.K.; aan het Rot, M.; Collins, K.A.; Mathew, S.J.; Charney, D.S.; Iosifescu, D.V. Rapid and longer-term antidepressant effects of repeated ketamine infusions in treatment-resistant major depression. Biol. Psychiatry 2013, 74, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Singh, B.; Kung, S.; Pazdernik, V.; Schak, K.M.; Geske, J.; Schulte, P.J.; Frye, M.A.; Voort, J.L.V. Comparative effectiveness of intravenous ketamine and intranasal esketamine in clinical practice among patients with treatment-refractory depression: An observational study. J. Clin. Psychiatry 2023, 84, 45331. [Google Scholar] [CrossRef] [PubMed]
- Fancy, F.; Rodrigues, N.B.; Di Vincenzo, J.D.; Chau, E.H.; Sethi, R.; Husain, M.I.; Gill, H.; Tabassum, A.; Mckenzie, A.; Phan, L.; et al. Real-world effectiveness of repeated ketamine infusions for treatment-resistant bipolar depression. Bipolar Disord. 2023, 25, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Singh, B. Ketamine For Treatment-Resistant Bipolar Depression—A Reality Check! Bipolar Disord. 2023, 25, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann. Intern. Med. 2009, 151, W-65–W-94. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (MINORS): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Sterne, J.A.; Gavaghan, D.; Egger, M. Publication and related bias in meta-analysis: Power of statistical tests and prevalence in the literature. J. Clin. Epidemiol. 2000, 53, 1119–1129. [Google Scholar] [CrossRef]
- Schwarzer, G. meta: An R package for meta-analysis. R. News 2007, 7, 40–45. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing. 2013. Available online: https://apps.dtic.mil/sti/citations/AD1039033 (accessed on 5 October 2023).
- Der Simonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Diazgranados, N.; Ibrahim, L.; Brutsche, N.E.; Newberg, A.; Kronstein, P.; Khalife, S.; Kammerer, W.A.; Quezado, Z.; Luckenbaugh, D.A.; Salvadore, G.; et al. A randomized add-on trial of an N-methyl-D-aspartate antagonist in treatment-resistant bipolar depression. Arch. Gen. Psychiatry 2010, 67, 793–802. [Google Scholar] [CrossRef] [PubMed]
- Zarate, C.A., Jr.; Brutsche, N.E.; Ibrahim, L.; Franco-Chaves, J.; Diazgranados, N.; Cravchik, A.; Selter, J.; Marquardt, C.A.; Liberty, V.; Luckenbaugh, D.A. Replication of ketamine’s antidepressant efficacy in bipolar depression: A randomized controlled add-on trial. Biol. Psychiatry 2012, 71, 939–946. [Google Scholar] [CrossRef]
- Rybakowski, J.K.; Permoda-Osip, A.; Bartkowska-Sniatkowska, A. Ketamine augmentation rapidly improves depression scores in inpatients with treatment-resistant bipolar depression. Int. J. Psychiatry Clin. Pract. 2017, 21, 99–103. [Google Scholar] [CrossRef]
- Kantrowitz, T.J.; Halberstam, B.; Gangwisch, J. Single-dose ketamine followed by daily D-cycloserine in treatment-resistant bipolar depression. J. Clin. Psychiatry 2015, 76, 738. [Google Scholar] [CrossRef]
- Zhuo, C.; Ji, F.; Tian, H.; Wang, L.; Jia, F.; Jiang, D.; Chen, C.; Zhou, C.; Lin, X.; Zhu, J. Transient effects of multi-infusion ketamine augmentation on treatment-resistant depressive symptoms in patients with treatment-resistant bipolar depression—An open-label three-week pilot study. Brain Behav. 2020, 10, e01674. [Google Scholar] [CrossRef]
- Zheng, W.; Zhou, Y.L.; Liu, W.J.; Wang, C.Y.; Zhan, Y.N.; Lan, X.F.; Zhang, B.; Ning, Y.P. A preliminary study of adjunctive ketamine for treatment-resistant bipolar depression. J. Affect. Disord. 2020, 275, 38–43. [Google Scholar] [CrossRef]
- Grunebaum, M.F.; Ellis, S.P.; Keilp, J.G.; Moitra, V.K.; Cooper, T.B.; Marver, J.E.; Burke, A.K.; Milak, M.S.; Sublette, M.E.; Oquendo, M.A.; et al. Ketamine versus midazolam in bipolar depression with suicidal thoughts: A pilot midazolam-controlled randomized clinical trial. Bipolar Disord. 2017, 19, 176–183. [Google Scholar] [CrossRef]
- Wilkowska, A.; Włodarczyk, A.; Gałuszko-Węgielnik, M.; Wiglusz, M.S.; Cubała, W.J. Intravenous ketamine infusions in treatment-resistant bipolar depression: An open-label naturalistic observational study. Neuropsychiatr. Dis. Treat. 2021, 17, 2637–2646. [Google Scholar] [CrossRef] [PubMed]
- Martinotti, G.; Dell’Osso, B.; Di Lorenzo, G.; Maina, G.; Bertolino, A.; Clerici, M.; Barlati, S.; Rosso, G.; Di Nicola, M.; Marcatili, M.; et al. Treating bipolar depression with esketamine: Safety and effectiveness data from a naturalistic multicentric study on esketamine in bipolar versus unipolar treatment-resistant depression. Bipolar Disord. 2023, 25, 233–244. [Google Scholar] [CrossRef] [PubMed]
- Delfino, R.S.; Del-Porto, J.A.; Surjan, J.; Magalhães, E.; Del Sant, L.C.; Lucchese, A.C.; Tuena, M.A.; Nakahira, C.; Fava, V.A.R.; Steglich, M.S.; et al. Comparative effectiveness of esketamine in the treatment of anhedonia in bipolar and unipolar depression. J. Affect. Disord. 2021, 278, 515–518. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. A coefficient of agreement for nominal scales. Educ. Psychol. Meas. 1960, 20, 37–46. [Google Scholar] [CrossRef]
- Xu, Y.; Hackett, M.; Carter, G.; Loo, C.; Gálvez, V.; Glozier, N.; Glue, P.; Lapidus, K.; McGirr, A.; Somogyi, A.A.; et al. Effects of low-dose and very low-dose ketamine among patients with major depression: A systematic review and meta-analysis. Int. J. Neuropsychopharmacol. 2016, 19, pyv124. [Google Scholar] [CrossRef]
- Wilkowska, A.; Wiglusz, M.S.; Gałuszko-Wegielnik, M.; Włodarczyk, A.; Cubała, W.J. Antianhedonic effect of repeated ketamine infusions in patients with treatment resistant depression. Front. Psychiatry 2021, 12, 704330. [Google Scholar] [CrossRef]
- Ballard, E.D.; Wills, K.; Lally, N.; Richards, E.M.; Luckenbaugh, D.A.; Walls, T.; Ameli, R.; Niciu, M.J.; Brutsche, N.E.; Park, L.; et al. Anhedonia as a clinical correlate of suicidal thoughts in clinical ketamine trials. J. Affect. Disord. 2017, 218, 195–200. [Google Scholar] [CrossRef]
- Singh, B.; Voort, J.L.V.; Riva-Posse, P.; Pazdernik, V.M.; Frye, M.A.; Tye, S.J. Ketamine-Associated Change in Anhedonia and mTOR Expression in Treatment-Resistant Depression. Biol. Psychiatry 2023, 93, e65–e68. [Google Scholar] [CrossRef]
- Banwari, G.; Desai, P.; Patidar, P. Ketamine-induced affective switch in a patient with treatment-resistant depression. Indian J. Pharmacol. 2015, 47, 454. [Google Scholar] [CrossRef]
- von Hippel, P.T. The heterogeneity statistic I2 can be biased in small meta-analyses. BMC Med. Res. Methodol. 2015, 15, 35. [Google Scholar] [CrossRef]
- Zheng, W.; Yang, X.H.; Gu, L.M.; Tan, J.Q.; Zhou, Y.L.; Wang, C.Y.; Ning, Y.P. Gender differences in the antianhedonic effects of repeated ketamine infusions in patients with depression. Front. Psychiatry 2022, 13, 981981. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| References, Year | Type of Study | Total Patients, Females (n(%)) | Age (Years) (Mean ± SD) | Number of Infusions | Outcome Measures | Conclusions |
|---|---|---|---|---|---|---|
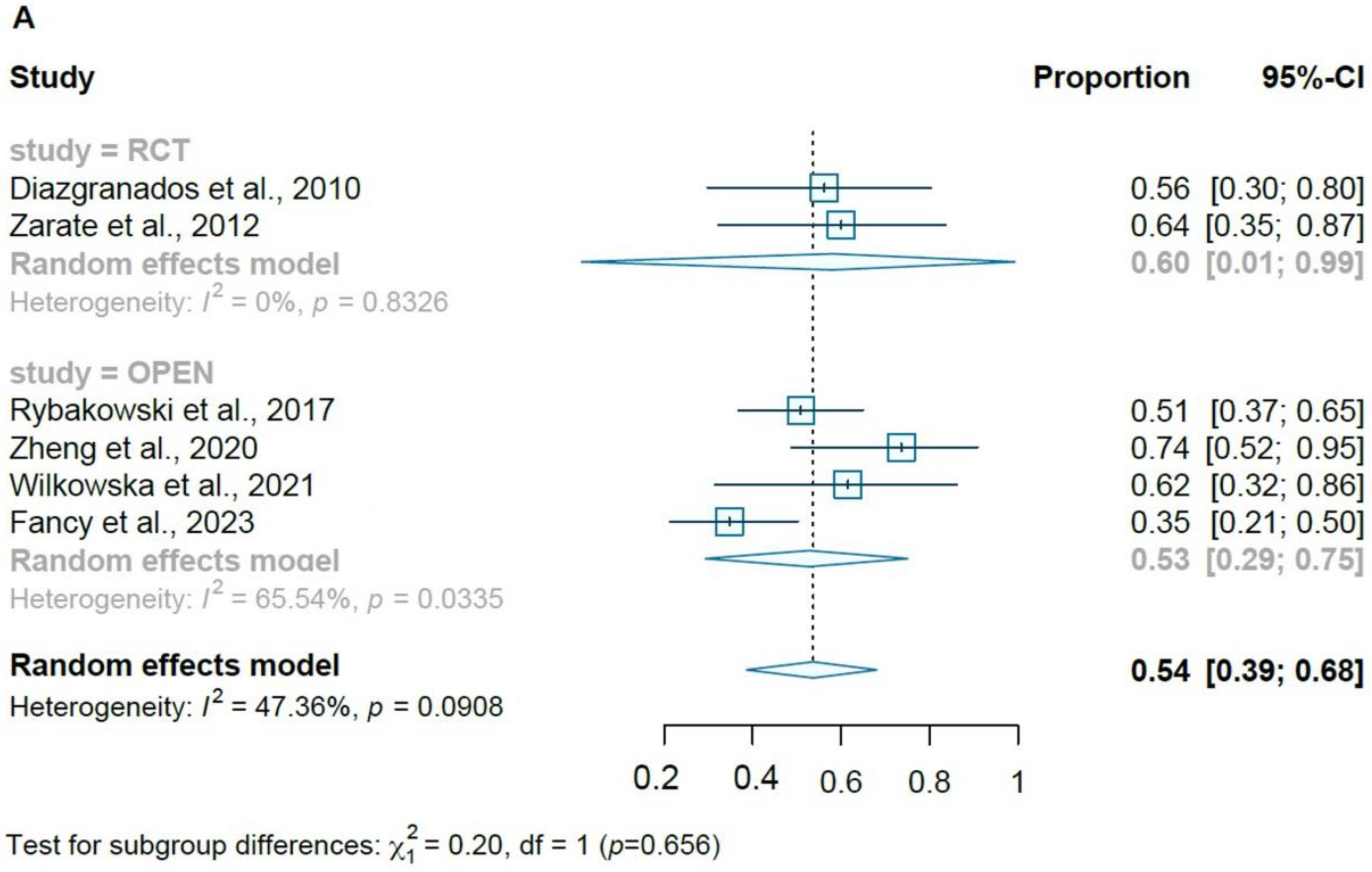
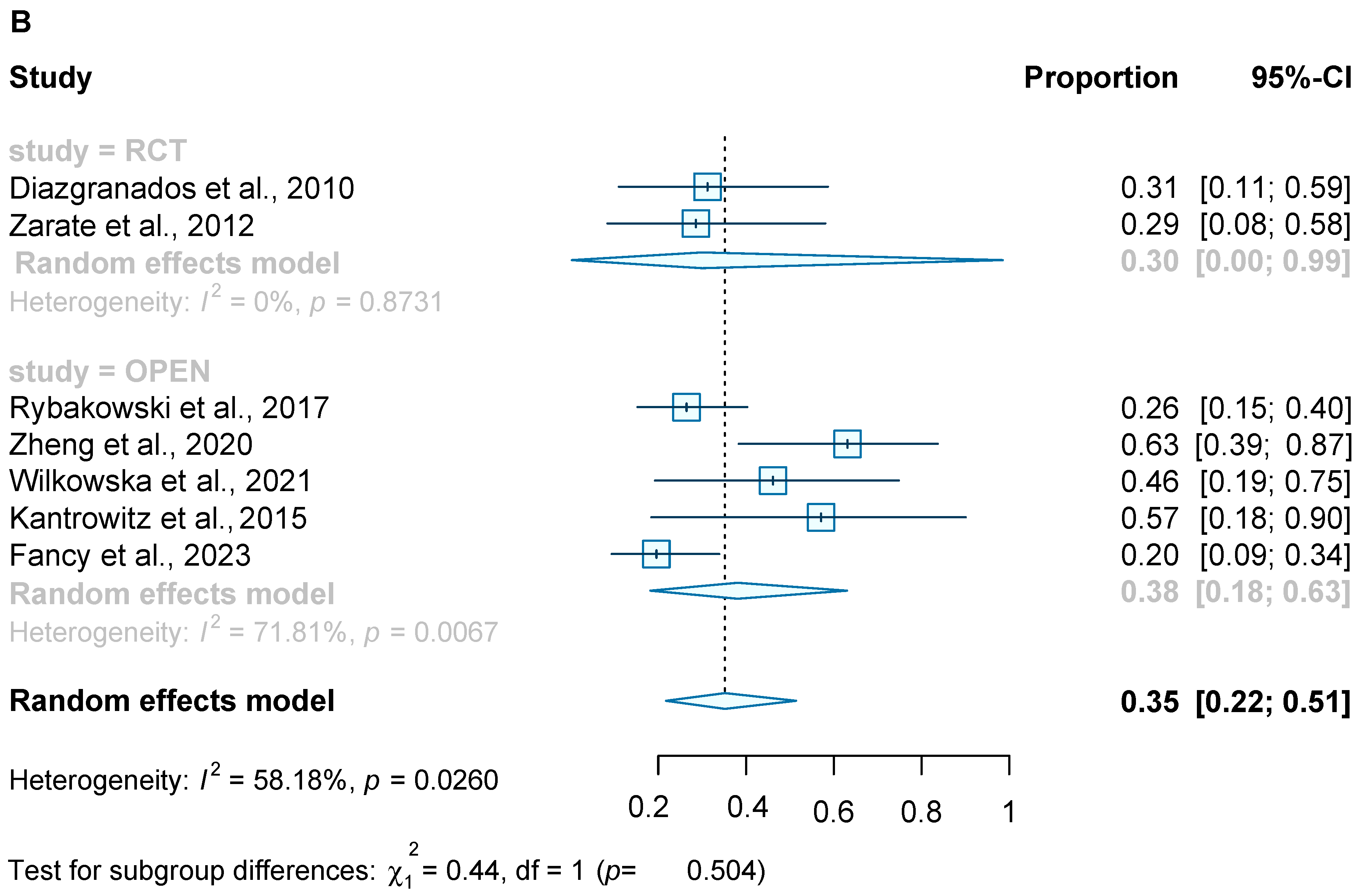
| Diazgranados et al., 2010 [26] | RCT, Crossover (ketamine–saline placebo) | 18, 12 (66.7) | 47.9 (13.1) | one | HAMD-17, MADRS, BDI, YMRS, CADSS, BPRS | Single intravenous dose of ketamine resulted in a robust and rapid antidepressant effect |
| Zarate et al., 2012 [27] | RCT, Crossover (ketamine–saline placebo) | 15, 8 (53.3) | 46.7 (10.4) | one | HAMD-17, MADRS, BDI, YMRS, CADSS, BPRS | Rapid and robust antidepressant response and rapid improvement in suicidal ideation following a single intravenous dose of ketamine |
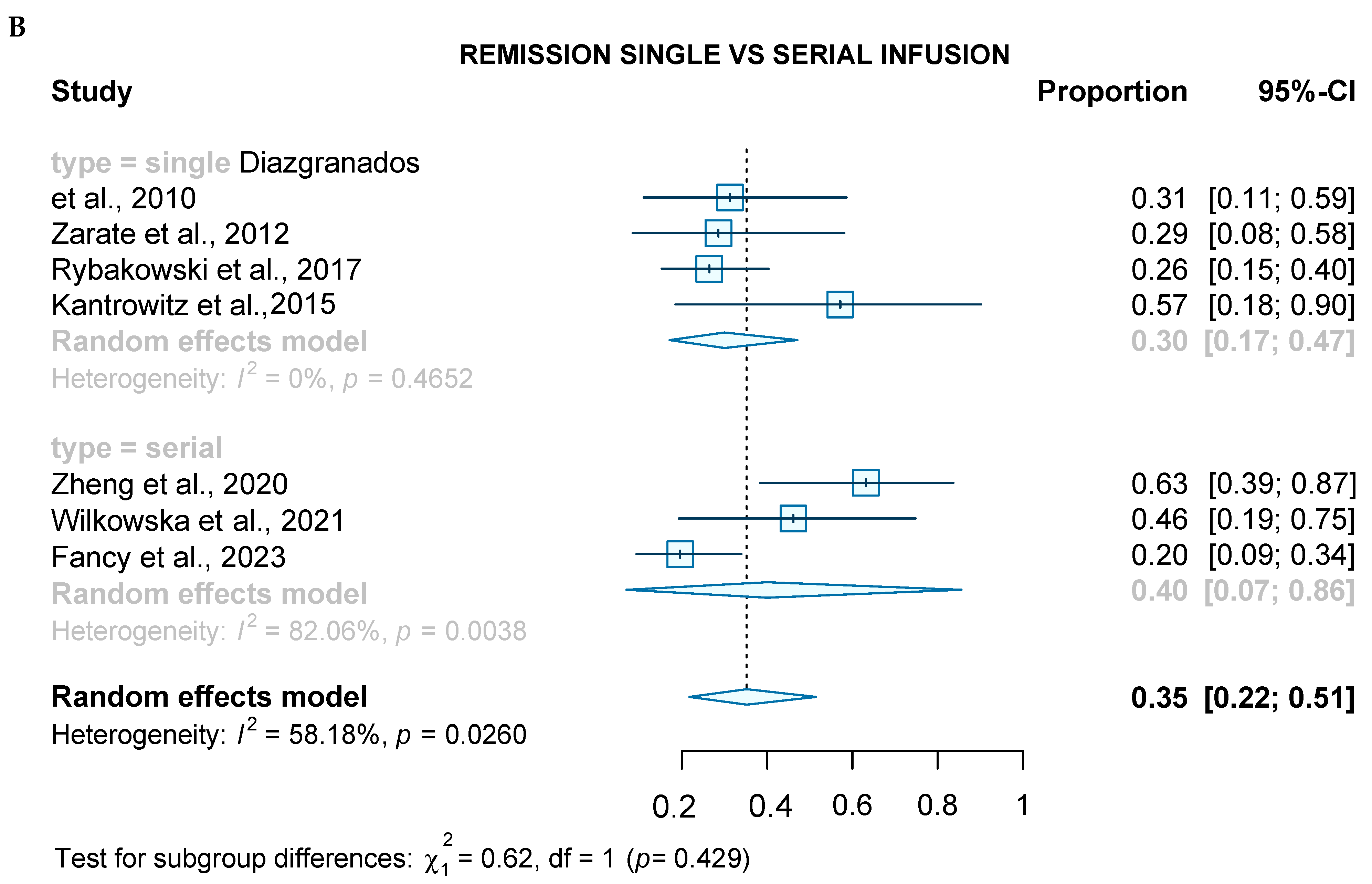
| Kantrowitz et al., 2015 [29] | Open label | 8, 5 (62.5) | 37 (16) | one | HAMD-17, BDI | 25% or more improvement in HAM-D in 7 patients after ketamine infusion |
| Grunebaum et al., 2016 [32] | RCT (ketamine–midazolam) | 16, 10 (62.5) | 41.25 (12.45) | one | HAMD-17, SSI, BDI, POMS, YMRS, CGI | Suicidal thoughts were lower after ketamine than after midazolam at a trend level of significance. Reduction in depression scores not statistically significant in ketamine group when compared to midazolam |
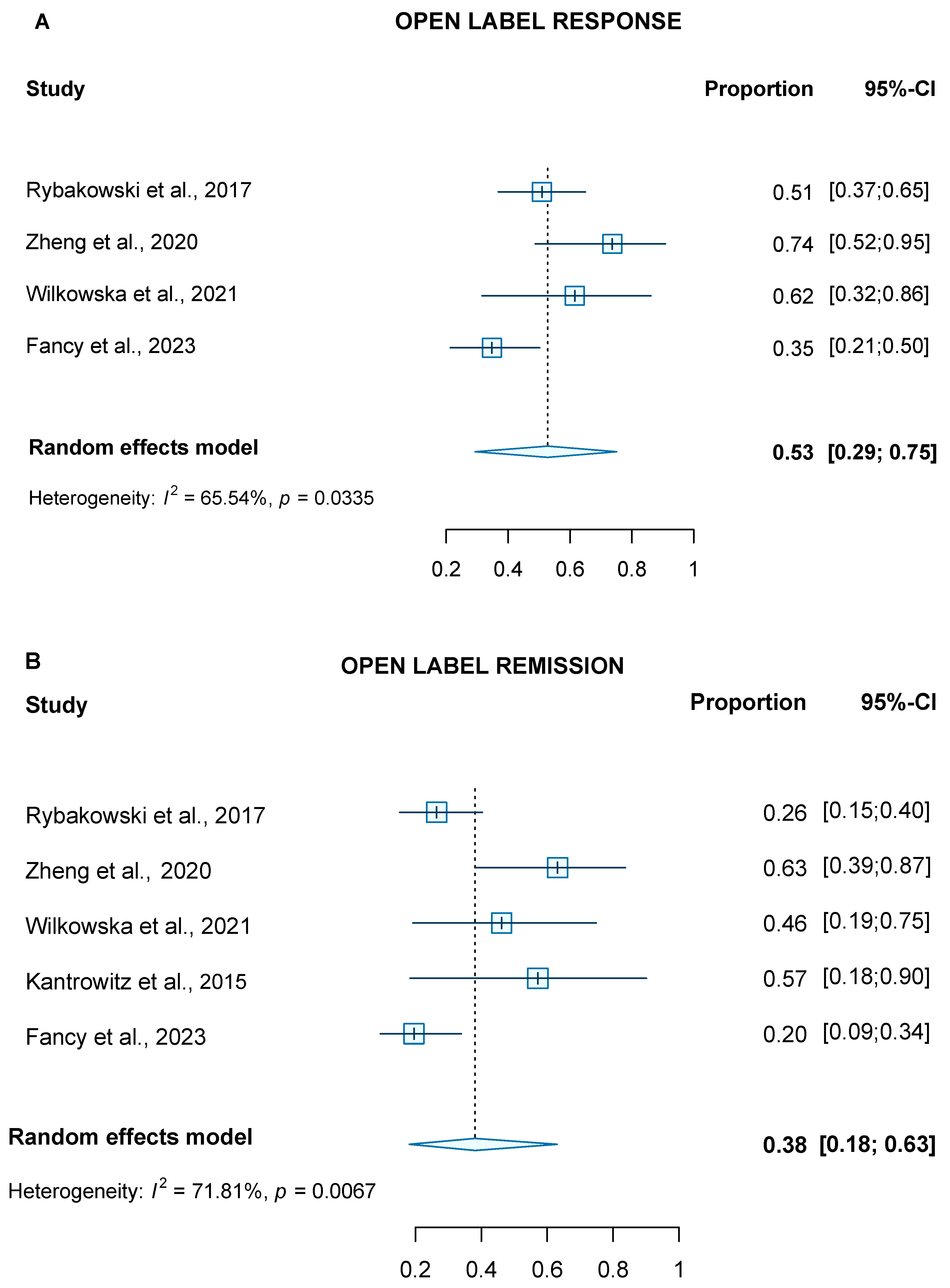
| Rybakowski et al., 2017 [28] | Open label | 53, 40 (75.5) | 47 (12.6) | one | HAMD-17 | Rapid antidepressant effect after single intravenous dose of ketamine infusion and a reduction of ≥50% on HAM-D in 24.5% patients at 24 h and in 51% patients on the seventh day after infusion |
| Zhou et al., 2020 [30] | Open label | 38, 16 (42.1) | 43.1 (5.3) | nine | HAMD-17, YMRS | Significant differences were observed in HAMD scores after one week of ketamine plus antidepressant treatment with an average reduction of 49.8% Patients at end of trial exhibited an increase in symptom severity relative to the baseline potentially related to a neural desensitization |
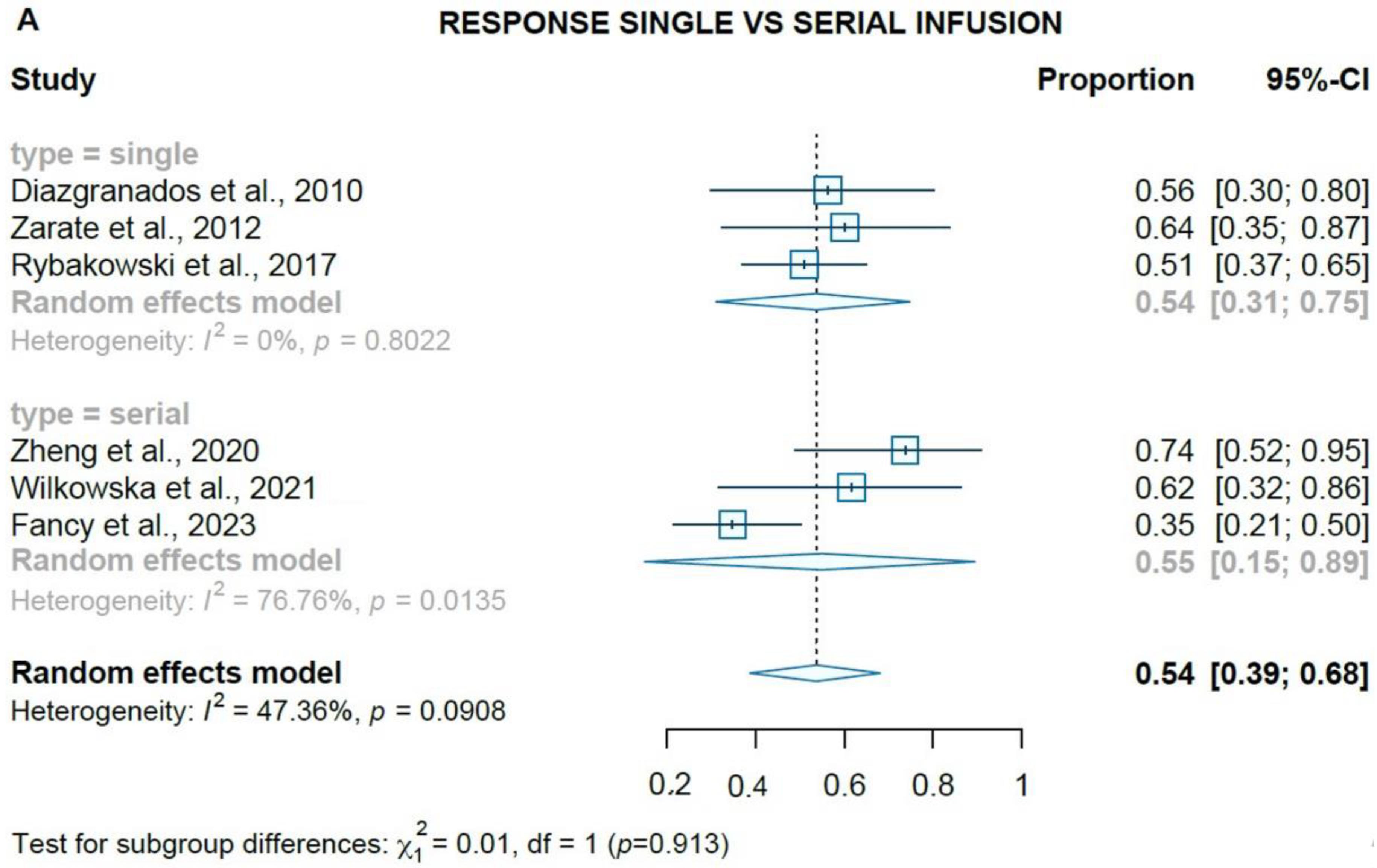
| Zheng et al., 2020 [31] | Open label | 19, 6 (31.6) | 35.8 (12.7) | six | MADRS, HAMD-17, BPRS, CDRS | Time to response and remission was 9 and 12 days, respectively, reaching rates of 73.7% and 63.2%. Improvement of depressive symptoms and suicidal ideation were sustained with subsequent infusions. No significant cardiovascular or psychomimetic side effects. |
| Wilkowska et al., 2021 [33] | Open label | 13, 6 (76.9) | 49.5 (15.1) | eight | MADRS, BPRS, CADSS, YMRS | IV ketamine was effective and well tolerated in the TRBD sample with response rates of 61.5% and remission of 46.2% following an average of 22.1 days to either response or remission. Side effects were mild (cardiovascular and psychomimetic) with no serious adverse events or affective switches |
| Delfino et al., 2021 [35] | Open label observational | 70, 45 (64) | 39.5 (12.3) | Six | MADRS (anhedonia) | Significant reduction in anhedonia after the first subcutaneous infusion and increased with repetitive infusions (p < 0.001) in both groups. No significant differences in esketamine anti-anhedonic effect. Subcutaneous administration seems to be equally effective in anti-anhedonic effects with good tolerability as simpler and inexpensive procedure. |
| Fancy et al., 2023 [16] | Open label observational | 66, 39 (59.1) | 45.7 (13.4) | four | QIDS-SR 16 | There was an improvement of depressive and anxiety symptoms, as well as psychosocial functioning (family and social domains) after repeated IV infusions of ketamine with a 6.08 ± 1.39 reduction in QIDS-SR16. After four infusions response rates were of 35% and 20% for remission. Ketamine was well tolerated and treatment emergent hypomania was observed in 4.5% of the sample. |
| Martinotti et al., 2023 [34] | Open label observational | 70, 38 (54.2) | 52.7 (10.9) | 2 weekly doses in the 1st month and 1 dose per week in the following 2 months. | MADRS, HAMD-17 | Reduction in depressive symptoms starting after 1 month of intranasal esketamine with no significant differences between groups. No significant side effects in terms of affective switch (low risk for mania/hypomania). Patients with TRBD showed lower side effects than TRD (57.14% vs. 77.15%). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nunez, N.A.; Joseph, B.; Kumar, R.; Douka, I.; Miola, A.; Prokop, L.J.; Mickey, B.J.; Singh, B. An Update on the Efficacy of Single and Serial Intravenous Ketamine Infusions and Esketamine for Bipolar Depression: A Systematic Review and Meta-Analysis. Brain Sci. 2023, 13, 1672. https://doi.org/10.3390/brainsci13121672
Nunez NA, Joseph B, Kumar R, Douka I, Miola A, Prokop LJ, Mickey BJ, Singh B. An Update on the Efficacy of Single and Serial Intravenous Ketamine Infusions and Esketamine for Bipolar Depression: A Systematic Review and Meta-Analysis. Brain Sciences. 2023; 13(12):1672. https://doi.org/10.3390/brainsci13121672
Chicago/Turabian StyleNunez, Nicolas A., Boney Joseph, Rakesh Kumar, Ioanna Douka, Alessandro Miola, Larry J. Prokop, Brian J. Mickey, and Balwinder Singh. 2023. "An Update on the Efficacy of Single and Serial Intravenous Ketamine Infusions and Esketamine for Bipolar Depression: A Systematic Review and Meta-Analysis" Brain Sciences 13, no. 12: 1672. https://doi.org/10.3390/brainsci13121672