
Implications of Social Anxiety Symptoms in Adults with Autism Spectrum Disorder: Is There a Predictive Role of Interpersonal Sensitivity and Substance Abuse?

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Sample and Procedure
2.2. Measures
2.2.1. The SHY-SV Questionnaire
2.2.2. AdAS Spectrum
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2023. [Google Scholar]
- Spain, D.; Zıvralı Yarar, E.; Happé, F. Social anxiety in adults with autism: A qualitative study. Int. J. Qual. Stud. Health Well-Being 2020, 15, 1803669. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Autism: Recognition, Referral, Diagnosis and Management of Adults on the Autism Spectrum, NICE Guidelines [CG142]; U.S. Department of Health and Human Services (HHS): Washington, DC, USA, 2012. [Google Scholar]
- Lai, M.C.; Kassee, C.; Besney, R.; Bonato, S.; Hull, L.; Mandy, W.; Szatmari, P.; Ameis, S.H. Prevalence of co-occurring mental health diagnoses in the autism population: A systematic review and meta-analysis. Lancet Psychiatry 2019, 6, 819–829. [Google Scholar] [CrossRef]
- Simonoff, E.; Pickles, A.; Charman, T.; Chandler, T.; Baird, G. Psychiatric disorders in children with autism spectrum disorders: Prevalence, comorbidity, and associated factors in a population-derived sample. J. Am. Acad. Child. Adolesc. Psychiatry 2008, 47, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Joshi, G.; Wozniak, J.; Petty, C.; Martelon, M.K.; Fried, R.; Bolfek, A.; Kotte, A.; Stevens, J.; Furtak, S.L.; Bourgeois, M.; et al. Psychiatric comorbidity and functioning in a clinically referred population of adults with autism spectrum disorders: A comparative study. J. Autism Dev. Disord. 2013, 43, 1314–1325. [Google Scholar] [CrossRef] [PubMed]
- Lever, A.G.; Geurts, H.M. Psychiatric co-occurring symptoms and disorders in young, middle-aged, and older adults with autism spectrum disorder. J. Autism Dev. Disord. 2016, 46, 1916–1930. [Google Scholar] [CrossRef] [PubMed]
- Russell, A.J.; Murphy, C.M.; Wilson, E.; Gillan, N.; Brown, C.; Robertson, D.M.; Murphy, C.M.; Craig, M.C.; Deeley, Q.; Zinkstok, J.; et al. The mental health of individuals referred for assessment of autism spectrum disorder in adulthood: A clinic report. Autism 2016, 20, 623–627. [Google Scholar] [CrossRef]
- Dell’Osso, L.; Cremone, I.M.; Amatori, G.; Cappelli, A.; Cuomo, A.; Barlati, S.; Massimetti, G.; Vita, A.; Fagiolini, A.; Carmassi, C.; et al. Investigating the Relationship between Autistic Traits, Ruminative Thinking, and Suicidality in a Clinical Sample of Subjects with Bipolar Disorder and Borderline Personality Disorder. Brain Sci. 2021, 11, 621. [Google Scholar] [CrossRef]
- Ambrose, K.; Simpson, K.; Adams, D. The relationship between social and academic outcomes and anxiety for children and adolescents on the autism spectrum: A systematic review. Clin. Psychol. Rev. 2021, 90, 102086. [Google Scholar] [CrossRef]
- van Steensel, F.J.; Bögels, S.M.; Perrin, S. Anxiety disorders in children and adolescents with autistic spectrum disorders: A meta-analysis. Clin. Child. Fam. Psychol. Rev. 2011, 14, 302–317. [Google Scholar] [CrossRef]
- Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A.; Rohde, L.A. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child. Psychol. Psychiatry 2015, 56, 345–365. [Google Scholar] [CrossRef]
- Kerns, C.M.; Kendall, P.C. The presentation and classification of anxiety in autism spectrum disorder. Clin. Psychol. Sci. Pract. 2012, 19, 323. [Google Scholar] [CrossRef]
- Kerns, C.M.; Kendall, P.C.; Berry, L.; Souders, M.C.; Franklin, M.E.; Schultz, R.T.; Miller, J.; Herrington, J. Traditional and atypical presentations of anxiety in youth with autism spectrum disorder. J. Autism Dev. Disord. 2014, 44, 2851–2861. [Google Scholar] [CrossRef] [PubMed]
- Belardinelli, C.; Raza, M. Comorbid behavioral problems and psychiatric disorders in autism spectrum disorders. J. Child. Dev. Disord. 2016, 2, 11. [Google Scholar] [CrossRef]
- Shephard, E.; Bedford, R.; Milosavljevic, B.; Gliga, T.; Jones, E.J.H.; Pickles, A.; Johnson, M.H.; Charman, T.; BASIS Team. Early developmental pathways to childhood symptoms of attention-deficit hyperactivity disorder, anxiety and autism spectrum disorder. J. Child. Psychol. Psychiatry 2019, 60, 963–974. [Google Scholar] [CrossRef] [PubMed]
- Hofvander, B.; Delorme, R.; Chaste, P.; Nydén, A.; Wentz, E.; Ståhlberg, O.; Herbrecht, E.; Stopin, A.; Anckarsäter, H.; Gillberg, C.; et al. Psychiatric and psychosocial problems in adults with normal-intelligence autism spectrum disorders. BMC Psychiatry 2009, 9, 35. [Google Scholar] [CrossRef] [PubMed]
- Ketelaars, C.; Horwitz, E.; Sytema, S.; Bos, J.; Wiersma, D.; Minderaa, R.; Hartman, C. Brief report: Adults with mild autism spectrum disorders (ASD): Scores on the autism spectrum quotient (AQ) and comorbid psychopathology. J. Autism Dev. Disord. 2008, 38, 176–180. [Google Scholar] [CrossRef]
- Lugnegård, T.; Hallerbäck, M.U.; Gillberg, C. Psychiatric comorbidity in young adults with a clinical diagnosis of Asperger syndrome. Res. Dev. Disabil. 2011, 32, 1910–1917. [Google Scholar] [CrossRef]
- Roy, R.M.; Prox-Vagedes, V.; Ohlmeier, M.D.; Dillo, W. Beyond childhood: Psychiatric comorbidities and social background of adults with Asperger syndrome. Psychiatr. Danub. 2015, 27, 1–59. [Google Scholar]
- Capriola, N.N.; Maddox, B.B.; White, S.W. No offense intended: Fear of negative evaluation in adolescents and adults with autism spectrum disorder. J. Autism Dev. Disord. 2016, 47, 3803–3813. [Google Scholar] [CrossRef]
- Spain, D.; Happé, F.G.; Johnston, P.; Campbell, M.; Sin, J.; Daly, E.; Ecker, C.; Anson, M.; Chaplin, E.; Glaser, K.; et al. Social anxiety in adult males with autism spectrum disorders. Res. Autism Spectr. Disord. 2016, 32, 13–23. [Google Scholar] [CrossRef]
- Spain, D. Social Anxiety in Adults with Autism Spectrum Disorders. Unpublished. Ph.D. Thesis, King’s College, London, UK, 2018. [Google Scholar]
- Farrugia, S.; Hudson, J. Anxiety in adolescents with Asperger syndrome: Negative thoughts, behavioral problems, and life interference. Focus. Autism Dev. Disabil. 2006, 21, 25–35. [Google Scholar] [CrossRef]
- Kuusikko, S.; Pollock-Wurman, R.; Jussila, K.; Carter, A.S.; Mattila, M.L.; Ebeling, H.; Pauls, D.L.; Moilanen, I. Social anxiety in high-functioning children and adolescents with Autism and Asperger syndrome. J. Autism Dev. Disord. 2008, 38, 1697–1709. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, L.; Abelli, M.; Pini, S.; Carpita, B.; Carlini, M.; Mengali, F.; Tognetti, R.; Rivetti, F.; Massimetti, G. The influence of gender on social anxiety spectrum symptoms in a sample of university students. Riv. Psichiatr. 2015, 50, 295–301. [Google Scholar]
- Marazziti, D.; Abelli, M.; Baroni, S.; Carpita, B.; Piccinni, A.; Dell’Osso, L. Recent findings on the pathophysiology of social anxiety disorder. Clin. Neuropsychiatry 2014, 11, 91–100. [Google Scholar]
- Keller, M.B. The lifelong course of social anxiety disorder: A clinical perspective. Acta Psychiatr. Scand. Suppl. 2003, 2003, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.B.; Kean, Y.M. Disability and quality of life in social phobia: Epidemiologic findings. Am. J. Psychiatry 2000, 157, 1606–1613. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Petukhova, M.; Sampson, N.A.; Zaslavsky, A.M.; Wittchen, H.U. Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int. J. Methods Psychiatr. Res. 2012, 21, 169–184. [Google Scholar] [CrossRef]
- Schneier, F.; Socha, J. Is there a spectrum of social anxiety disorder? In Anxiety Disorders-Theory, Research, and Clinical Perspectives; Simpson, H., Neria, Y., Lewis-Fernándex, R., Schneier, F., Eds.; Cambridge University Press: Cambridge, UK, 2010. [Google Scholar]
- Fehm, L.; Pelissolo, A.; Furmark, T.; Wittchen, H.-U. Size and burden of social phobia in Europe. Eur. Neuropsychopharmacol. 2005, 15, 453–462. [Google Scholar] [CrossRef]
- Bellini, S. Social skill deficits and anxiety in high-functioning adolescents with autism spectrum disorders. Focus. Autism Dev. Disabil. 2004, 19, 78–86. [Google Scholar] [CrossRef]
- Maddox, B.B.; White, S.W. Comorbid social anxiety disorder in adults with autism spectrum disorder. J. Autism Dev. Disord. 2015, 45, 3949–3960. [Google Scholar] [CrossRef]
- Spain, D.; Sin, J.; Freeman, D. Conceptualising paranoia in ASD: A systematic review and development of a theoretical framework. Res. Autism Spectr. Disord. 2016, 25, 97–111. [Google Scholar] [CrossRef]
- White, S.W.; Oswald, D.; Ollendick, T.; Scahill, L. Anxiety in children and adolescents with autism spectrum disorders. Clin. Psychol. Rev. 2009, 29, 216–229. [Google Scholar] [CrossRef]
- Schreibman, L.; Anderson, A. Focus on integration: The future of the behavioral treatment of autism. Behav. Ther. 2011, 32, 619–632. [Google Scholar] [CrossRef]
- Constantino, J.N.; Todd, R.D. Intergenerational transmission of subthreshold autistic traits in the general population. Biol. Psychiatry 2005, 57, 655–660. [Google Scholar] [CrossRef] [PubMed]
- White, S.W.; Ollendick, T.; Bray, B.C. College students on the autism spectrum: Prevalence and associated problems. Autism 2011, 15, 683–701. [Google Scholar] [CrossRef] [PubMed]
- Bejerot, S.; Mörtberg, E. Do autistic traits play a role in the bullying of obsessive-compulsive disorder and social phobia sufferers? Psychopathology 2009, 42, 170–176. [Google Scholar] [CrossRef]
- Salazar, F.; Baird, G.; Chandler, S.; Tseng, E.; O’sullivan, T.; Howlin, P.; Pickles, A.; Simonoff, E. Co-occurring Psychiatric Disorders in Preschool and Elementary School-Aged Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2015, 45, 2283–2294. [Google Scholar] [CrossRef]
- Vickerstaff, S.; Heriot, S.; Wong, M.; Lopes, A.; Dossetor, D. Intellectual ability, self-perceived social competence, and depressive symptomatology in children with high-functioning autistic spectrum disorders. J. Autism Dev. Disord. 2007, 37, 1647–1664. [Google Scholar] [CrossRef]
- Piven, J.; Palmer, P. Psychiatric disorder and the broad autism phenotype: Evidence from a family study of multiple-incidence autism families. Am. J. Psychiatry 1999, 156, 557–563. [Google Scholar] [CrossRef]
- Adams, D.; Young, K.; Simpson, K.; Keen, D. Parent descriptions of the presentation and management of anxiousness in children on the autism spectrum. Autism 2019, 23, 980–992. [Google Scholar] [CrossRef]
- Swan, A.J.; Kendall, P.C. Fear and missing out: Youth anxiety and functional outcomes. Clin. Psychol. Sci. Pract. 2016, 23, 417. [Google Scholar] [CrossRef]
- Pellecchia, M.; Connell, J.E.; Kerns, C.M.; Xie, M.; Marcus, S.C.; Mandell, D.S. Child characteristics associated with outcome for children with autism in a school-based behavioral intervention. Autism 2016, 20, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Mylett, M.L.; Boucher, T.Q.; Scheerer, N.E.; Iarocci, G. Examining the Relations between Social Competence, Autistic Traits, Anxiety and Depression in Autistic and Non-Autistic Children. J. Autism Dev. Disord. 2023, 1–3. [Google Scholar] [CrossRef]
- Zukerman, G.; Yahav, G.; Ben-Itzchak, E. The Gap Between Cognition and Adaptive Behavior in Students with Autism Spectrum Disorder: Implications for Social Anxiety and the Moderating Effect of Autism Traits. J. Autism Dev. Disord. 2021, 51, 1466–1478. [Google Scholar] [CrossRef]
- First, M.B.; Williams, J.B.W.; Karg, R.S.; Spitzer, R.L. Structured Clinical Interview for DSM-5—Research Version (SCID-5 for DSM-5, Research Version; SCID-5-RV); American Psychiatric Association: Arlington, VA, USA, 2015. [Google Scholar]
- Dell’Osso, L.; Cremone, I.M.; Nardi, B.; Amatori, G.; Bonelli, C.; Gravina, D.; Benedetti, F.; Del Prete, L.; Massimetti, G.; Carpita, B. Measuring the neglected anxiety disorder: Validation of the Social Anxiety Spectrum-Short Version (SHY-SV) questionnaire. BMC Psychiatry 2023, in press. [CrossRef] [PubMed]
- Dell’Osso, L.; Rucci, P.; Cassano, G.B.; Maser, J.D.; Endicott, J.; Shear, M.K.; Sarno, N.; Saettoni, M.; Grochocinski, V.J.; Frank, E. Measuring social anxiety and obsessive-compulsive spectra: Comparison of interviews and self-report instruments. Compr. Psychiatry 2002, 43, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, L.; Gesi, C.; Massimetti, E.; Cremone, I.M.; Barbuti, M.; Maccariello, G.; Moroni, I.; Barlati, S.; Castellini, G.; Luciano, M.; et al. Adult Autism Subthreshold Spectrum (AdAS Spectrum): Validation of a questionnaire investigating subthreshold autism spectrum. Compr. Psychiatry 2017, 73, 61–83. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, L.; Carmassi, C.; Cremone, I.M.; Muti, D.; Salerni, A.; Barberi, F.M.; Massimetti, E.; Gesi, C.; Politi, P.; Aguglia, E.; et al. Defining the optimal threshold scores for Adult Autism Subthreshold Spectrum (AdAS Spectrum) in clinical and general population. Clin. Pract. Epidemiol. Ment. Health 2020, 16, 204. [Google Scholar] [CrossRef]
- Donati, M.A.; Berrocal, C.; Primi, C.; Petracchi, G.; Carpita, B.; Cosci, F.; Ruiz, A.; Carmassi, C.; Dell’Osso, L. Measuring subthreshold autistic traits in the general population: Psychometric properties of the Adult Autism Subthreshold Spectrum (AdAS Spectrum) scale. Psychiatry Res. 2019, 281, 112576. [Google Scholar] [CrossRef]
- Solomon, M.; Goodlin-Jones, B.; Anders, T. A social adjustment enhancement intervention for high functioning autism, Asperger’s syndrome, and pervasive developmental disorder NOS. J. Autism Dev. Disord. 2004, 34, 649–668. [Google Scholar] [CrossRef]
- White, S.W.; Keonig, K.; Scahill, L. Social skills development in children with autism spectrum disorders: A review of the intervention research. J. Autism Dev. Disord. 2007, 37, 1858–1868. [Google Scholar] [CrossRef]
- Spain, D.; Sin, J.; Linder, K.B.; McMahon, J.; Happé, F. Social anxiety in autism spectrum disorder: A systematic review. Res. Autism Spectr. Disord. 2018, 52, 51–68. [Google Scholar] [CrossRef]
- Chang, Y.C.; Quan, J.; Wood, J.J. Effects of anxiety disorder severity on social functioning in children with autism spectrum disorders. J. Dev. Physical Disabil. 2012, 24, 235–245. [Google Scholar] [CrossRef]
- Sreckovic, M.A.; Brunsting, N.C.; Able, H. Victimization of students with autism spectrum disorder: A review of prevalence and risk factors. Res. Autism Spectr. Disord. 2014, 8, 1155–1172. [Google Scholar] [CrossRef]
- Van Roekel, E.; Scholte, R.; Didden, R. Bullying among adolescents with autism spectrum disorders: Prevalence and perception. J. Autism Dev. Disord. 2010, 40, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Amore, M.; Murri, M.B.; Calcagno, P.; Rocca, P.; Rossi, A.; Aguglia, E.; Bellomo, A.; Blasi, G.; Carpiniello, B.; Cuomo, A.; et al. The association between insight and depressive symptoms in schizophrenia: Undirected and Bayesian network analyses. Eur. Psychiatry 2020, 63, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Miers, A.C.; Blöte, A.W.; Bögels, S.M.; Westenberg, P.M. Interpretation bias and social anxiety in adolescents. J. Anxiety Disord. 2008, 22, 1462–1471. [Google Scholar] [CrossRef]
- Blöte, A.W.; Miers, A.C.; Van den Bos, E.; Westenberg, P.M. Negative social self-cognitions: How shyness may lead to social anxiety. J. Appl. Dev. Psychol. 2019, 63, 9–15. [Google Scholar] [CrossRef]
- Bellini, S. The development of social anxiety in adolescents with autism spectrum disorders. Focus. Autism Dev. Disabil. 2006, 21, 138–145. [Google Scholar] [CrossRef]
- Rapee, R.M.; Spence, S.H. The etiology of social phobia: Empirical evidence and an initial model. Clin. Psychol. Rev. 2004, 24, 737–767. [Google Scholar] [CrossRef]
- Dickter, C.L.; Burk, J.A.; Fleckenstein, K.; Kozikowski, C.T. Autistic traits and social anxiety predict differential performance on social cognitive tasks in typically developing young adults. PLoS ONE 2018, 13, e0195239. [Google Scholar] [CrossRef] [PubMed]
- White, S.; Bray, B.; Ollendick, T. Examining shared and unique aspects of social anxiety disorder and autism spectrum disorder using factor analysis. J. Autism Dev. Disord. 2012, 42, 874–884. [Google Scholar] [CrossRef] [PubMed]
- White, S.; Kreiser, N.L.; Pugliese, C.; Scarpa, A. Social anxiety mediates the effect of autism spectrum disorder characteristics on hostility in young adults. Autism 2012, 16, 453–464. [Google Scholar] [CrossRef]
- Jamison, T.R.; Schuttler, J.O. Examining social competence, self-perception, quality of life, and internalizing and externalizing symptoms in adolescent females with and without autism spectrum disorder: A quantitative design including between-groups and correlational analyses. Mol. Autism 2015, 6, 53. [Google Scholar] [CrossRef] [PubMed]
- Arkowitz, H.; Lichtenstein, E.; McGovern, K.; Hines, P. The behavioral assessment of social competence in males. Behav. Ther. 1975, 6, 3–13. [Google Scholar] [CrossRef]
- Farrell, A.D.; Mariotto, M.J.; Conger, A.J.; Curran, J.P.; Wallander, J.L. Self-ratings and judges’ ratings of heterosexual social anxiety and skill: A generalizability study. J. Consult. Clin. Psychol. 1979, 43, 522–527. [Google Scholar] [CrossRef]
- Glenn, L.E.; Keeley, L.M.; Szollos, S.; Okuno, H.; Wang, X.; Rausch, E.; De Los Reyes, A. Trained observers’ ratings of adolescents’ social anxiety and social skills within controlled, cross-contextual social interactions with unfamiliar peer confederates. J. Psychopathol. Behav. Assess. 2019, 41, 1–15. [Google Scholar] [CrossRef]
- Halford, K.; Foddy, M. Cognitive and social correlates of social anxiety. Br. J. Clin. Psychol. 1982, 21, 17–28. [Google Scholar] [CrossRef]
- Twentyman, C.T.; McFall, R.M. Behavioral training of social skills in shy males. J. Consult. Clin. Psychol. 1975, 43, 384–395. [Google Scholar] [CrossRef]
- Pellecchia, G.; Moroni, F.; Colle, L.; Semerari, A.; Carcione, A.; Fera, T.; Fiore, D.; Nicolò, G.; Pedone, R.; Procacci, M. Avoidant personality disorder and social phobia: Does mindreading make the difference? Compr. Psychiatry 2018, 80, 163–169. [Google Scholar] [CrossRef]
- Carpita, B.; Marazziti, D.; Palego, L.; Giannaccini, G.; Betti, L.; Dell’Osso, L. Microbiota, Immune System and Autism Spectrum Disorders: An Integrative Model towards Novel Treatment Options. Curr. Med. Chem. 2020, 27, 5119–5136. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Ring, H.A.; Bullmore, E.T.; Wheelwright, S.; Ashwin, C.; Williams, S.C. The amygdala theory of autism. Neurosci. Biobehav. Rev. 2000, 24, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Frith, U.; Frith, C.D. Development and neurophysiology of mentalizing. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 2003, 358, 459–473. [Google Scholar] [CrossRef] [PubMed]
- Krämer, K.; Vetter, A.; Schultz-Venrath, U.; Vogeley, K.; Reul, S. Mentalization-Based Treatment in Groups for Adults with Autism Spectrum Disorder. Front. Psychol. 2021, 12, 708557. [Google Scholar] [CrossRef]
- Simonsen, S.; Popolo, R.; Juul, S.; Frandsen, F.W.; Sørensen, P.; Dimaggio, G. Treating Avoidant Personality Disorder With Combined Individual Metacognitive Interpersonal Therapy and Group Mentalization-Based Treatment: A Pilot Study. J. Nerv. Ment. Dis. 2022, 210, 163–171. [Google Scholar] [CrossRef]
- Sanvicente-Vieira, B.; Romani-Sponchiado, A.; Kluwe-Schiavon, B.; Brietzke, E.; Araujo, R.B.; Grassi-Oliveira, R. Theory of mind in substance users: A systematic minireview. Subst. Use Misuse 2017, 52, 127–133. [Google Scholar] [CrossRef]
- Caumiant, E.P.; Fairbairn, C.E.; Bresin, K.; Gary Rosen, I.; Luczak, S.E.; Kang, D. Social anxiety and alcohol consumption: The role of social context. Addict. Behav. 2023, 143, 107672. [Google Scholar] [CrossRef]
- Buckner, J.D.; Morris, P.E.; Abarno, C.N.; Glover, N.I.; Lewis, E.M. Biopsychosocial Model Social Anxiety and Substance Use Revised. Curr. Psychiatry Rep. 2021, 23, 35. [Google Scholar] [CrossRef]
- Buckner, J.D.; Heimberg, R.G.; Ecker, A.H.; Vinci, C. A biopsychosocial model of social anxiety and substance use. Depress. Anxiety 2013, 30, 276–284. [Google Scholar] [CrossRef]
- Butwicka, A.; Långström, N.; Larsson, H.; Lundström, S.; Serlachius, E.; Almqvist, C.; Frisén, L.; Lichtenstein, P. Increased Risk for Substance Use-Related Problems in Autism Spectrum Disorders: A Population-Based Cohort Study. J. Autism Dev. Disord. 2017, 47, 80–89. [Google Scholar] [CrossRef]
- Tinsley, M.; Hendrickx, S. Asperger Syndrome and Alcohol: Drinking to Cope? Jessica Kingsley Publishers: London, UK, 2008. [Google Scholar]
- National Institute on Drug Abuse. Principles of Adolescent Substance Use Disorder Treatment: A Research-Based Guide. 2014. Available online: https://www.drugabuse.gov/publications/principles-adolescent-substance-use-disorder-treatment-research-based-guide/frequently-asked-questions/why-do-adolescents-take-drugs (accessed on 13 March 2017).
- White, P.D.; Rickards, H.; Zeman, A.Z.J. Time to end the distinction between mental and neurological illnesses. BMJ 2012, 344, e3454. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, L.; Lorenzi, P.; Carpita, B. The neurodevelopmental continuum towards a neurodevelopmental gradient hypothesis. J. Psychopathol. 2019, 25, 179–182. [Google Scholar]
- Wong, N.; Sarver, D.E.; Beidel, D.C. Quality of life impairments among adults with social phobia: The impact of subtype. J. Anxiety Disord. 2012, 26, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.B.; Fuetsch, M.; Müller, N.; Höfler, M.; Lieb, R.; Wittchen, H.U. Social anxiety disorder and the risk of depression: A prospective community study of adolescents and young adults. Arch. Gen. Psychiatry 2001, 58, 251–256. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ASD | HC | ||||
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | T | p | ||
| Age | 34.02 ± 11.37 | 34.15 ± 11.10 | 0.054 | 0.096 | |
| n (%) | n (%) | Chi-square | |||
| Sex | M | 24 (50.0) | 21 (43.8) | 0.376 | 539 |
| F | 24 (50.0) | 27 (56.3) | |||
| Scales | Number of Items | Group | Cronbach’s Alpha |
|---|---|---|---|
| SHY-SV | 108 | HC | 0.857 |
| ASD | 0.945 | ||
| AdAS Spectrum Total score | 160 | HC | 0.781 |
| ASD | 0.904 |
| Group | AdAS Spectrum | SHY-SV | ||
|---|---|---|---|---|
| HC | Mean | 5.31 | 5.75 | |
| Median | 5.00 | 4.00 | ||
| Mode | 5.00 | 4.00 | ||
| St. deviation | 4.75 | 6.01 | ||
| Minimun | 0 | 0 | ||
| Maximum | 22 | 36 | ||
| Percentiles | 25 | 2.00 | 2.00 | |
| 50 | 5.00 | 4.00 | ||
| 75 | 6.75 | 8.00 | ||
| ASD | Mean | 85.79 | 46.10 | |
| Median | 83.00 | 43.00 | ||
| Mode | 82.00 | 25.00 | ||
| St. deviation | 19.37 | 19.66 | ||
| Minimun | 50 | 7 | ||
| Maximum | 142 | 92 | ||
| Percentiles | 25 | 73.00 | 31.25 | |
| 50 | 83.00 | 43.00 | ||
| 75 | 95.50 | 61.25 | ||
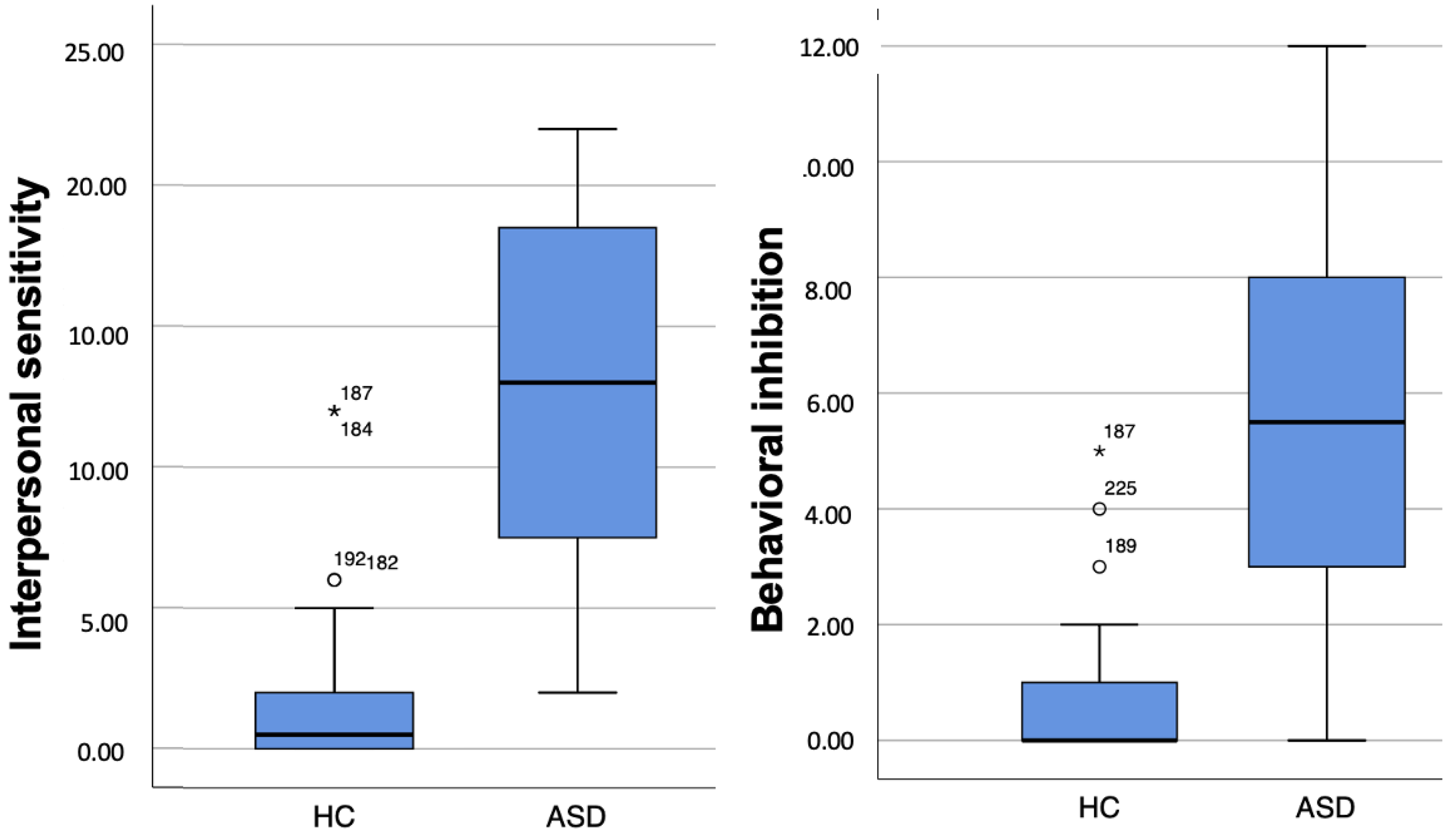
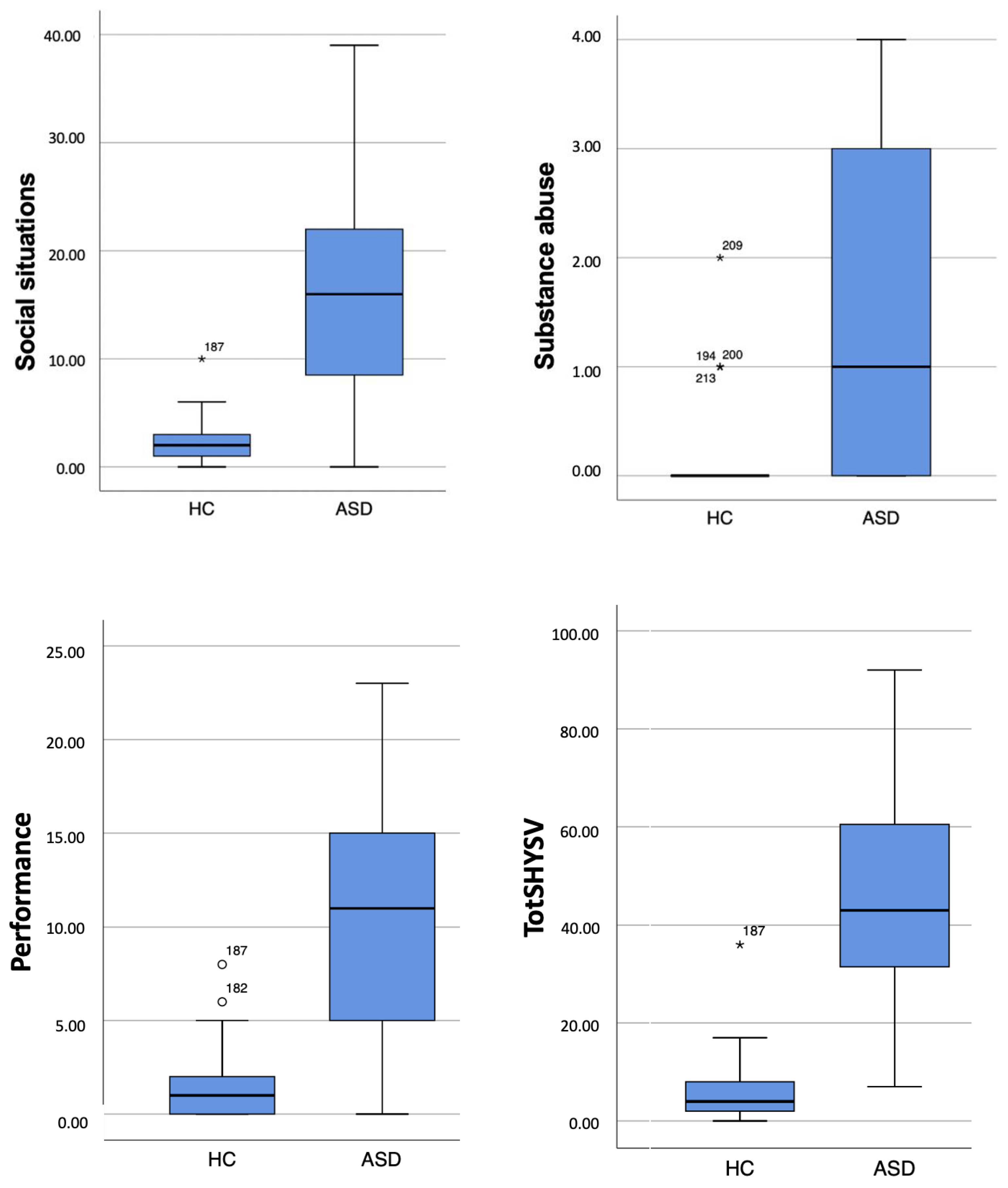
| SHY-SV Scores | ASD Group Mean ± SD | HC Group Mean ± SD | t | p |
|---|---|---|---|---|
| Interpersonal sensitivity | 12.62 ± 6.37 | 1.52 ± 2.67 | −11.41 | <0.001 |
| Behavioral inhibition | 5.81 ± 3.38 | 0.62 ± 1.10 | −10.10 | <0.001 |
| Social situations | 15.83 ± 9.48 | 2.14 ± 1.99 | −9.79 | <0.001 |
| Substance abuse | 1.50 ± 1.43 | 0.23 ± 0.47 | −5.85 | <0.001 |
| Performance | 10.33 ± 6.20 | 1.23 ± 1.63 | −9.84 | <0.001 |
| Total | 46.10 ± 19.66 | 5.75 ± 6.01 | −13.60 | <0.001 |
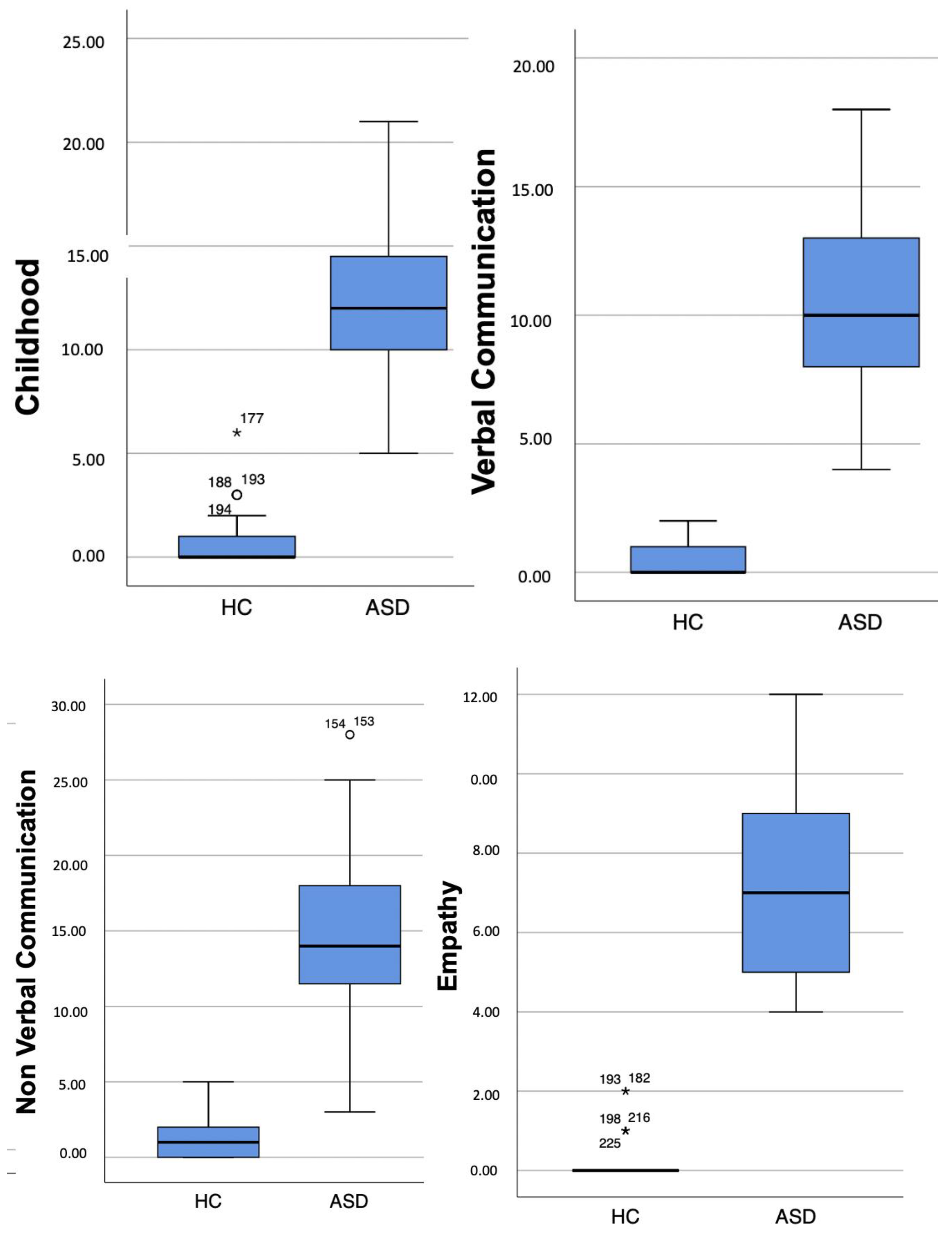
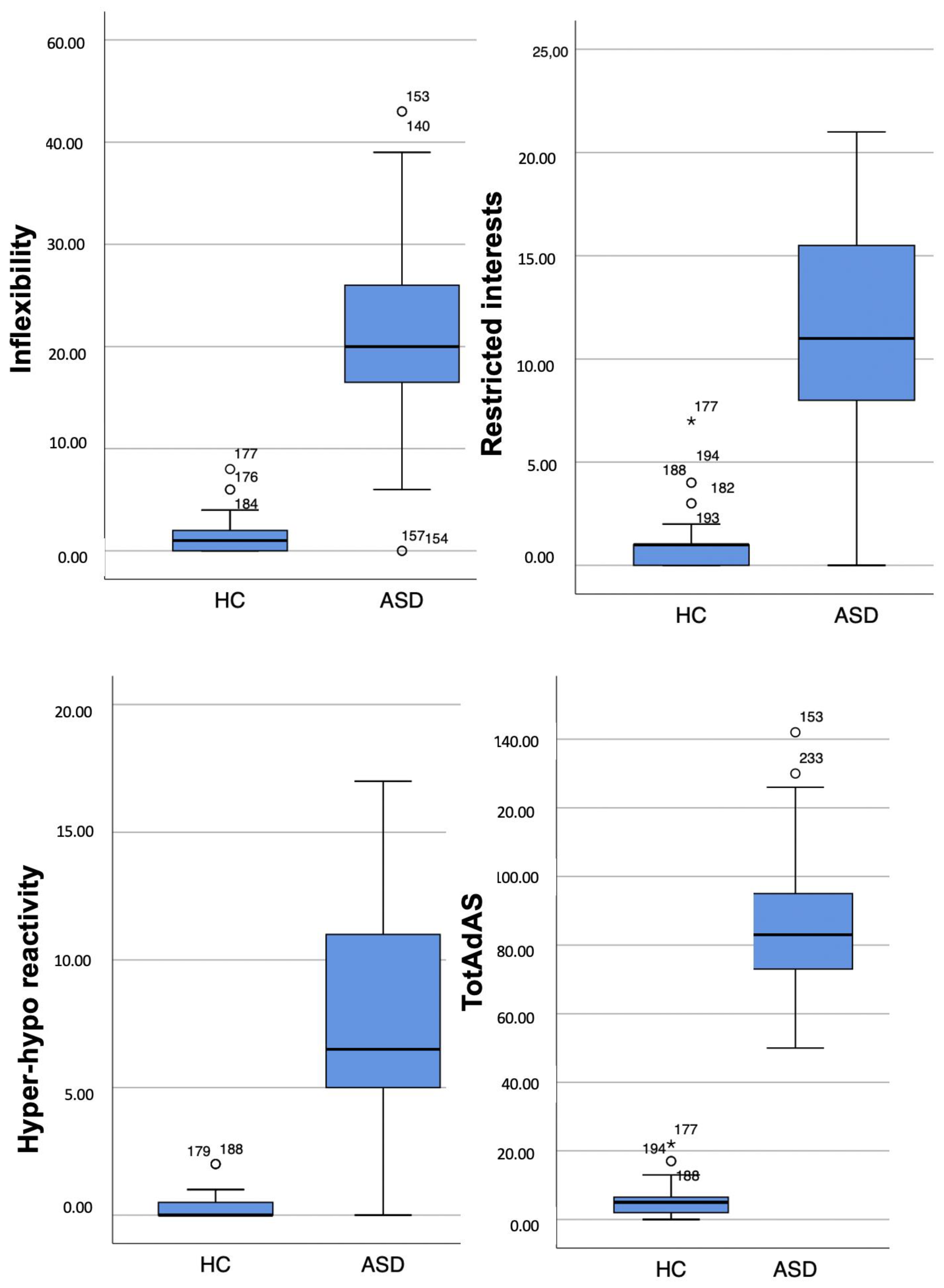
| AdAS Spectrum Scores | ASD Group Mean ± SD | HC Group Mean ± SD | t | p |
|---|---|---|---|---|
| Childhood/Adolescence | 12.69 ± 4.01 | 0.83 ± 1.21 | −19.60 | <0.001 |
| Verbal communication | 10.52 ± 3.61 | 0.48 ± 0.62 | −19.00 | <0.001 |
| Non-verbal communication | 14.39 ± 5.92 | 1.04 ± 1.34 | −15.25 | <0.001 |
| Empathy | 7.46 ± 2.53 | 0.21 ± 0.50 | −19.44 | <0.001 |
| Inflexibility & adherence to routine | 20.85 ± 9.87 | 1.54 ± 1.75 | −13.35 | <0.001 |
| Restricted interest & rumination | 11.87 ± 5.03 | 0.89 ± 1.36 | −14.59 | <0.001 |
| Hyper-/hypo-reactivity to sensory input | 8.00 ± 5.00 | 0.31 ± 0.59 | −10.57 | <0.001 |
| Total Score | 85.79 ± 19.37 | 5.31 ± 4.75 | −27.96 | <0.001 |
| Interpers. Sens. | Behav. Inhib. | Social Sit. | Subst. Abuse | Performance | Tot. Score | |
|---|---|---|---|---|---|---|
| Child./Adolesc. | 0.778 * | 0.627 * | 0.607 * | 0.440 * | 0.560 * | 0.724 * |
| Verb. comm. | 0.792 * | 0.726 * | 0.638 * | 0.518 * | 0.643 * | 0.780 * |
| Non-verb. comm. | 0.784 * | 0.617 * | 0.626 * | 0.478 * | 0.568 * | 0.736 * |
| Empathy | 0.740 * | 0.652 * | 0.609 * | 0.510 * | 0.655 * | 0.745 * |
| Inflex. & routine | 0.563 * | 0.603 * | 0.646 * | 0.401 * | 0.662 * | 0.696 * |
| Restrict. interest & rum. | 0.626 * | 0.629 * | 0.664 * | 0.452 * | 0.649 * | 0.725 * |
| Hyper-hyporeact. | 0.702 * | 0.579 * | 0.497 * | 0.377 * | 0.458 * | 0.622 * |
| Tot. Score | 0.782 * | 0.707 * | 0.698 * | 0.503 * | 0.682 * | 0.807 * |
| Interpers. Sens. | Behav. Inhib. | Social Sit. | Subst. Abuse | Performance | Tot. Score | |
|---|---|---|---|---|---|---|
| Child./Adolesc. | 0.093 | −0.191 | 0.046 | −0.081 | 0.009 | 0.018 |
| Verb. comm. | 0.373 * | 0.331 * | 0.288 * | 0.199 | 0.185 | 0.388 * |
| Non-verb. comm. | 0.149 | 0.170 | 0.142 | 0.119 | −0.093 | 0.129 |
| Empathy | 0.234 | −0.010 | 0.033 | −0.026 | 0.174 | 0.158 |
| Inflex. & routine | 0.139 | −0.003 | 0.087 | −0.205 | −0.089 | 0.050 |
| Restrict. interest & rum. | 0.174 | −0.083 | 0.037 | 0.005 | 0.040 | 0.085 |
| Hyper-hyporeact. | 0.111 | −0.143 | 0.251 | −0.033 | −0.010 | 0.101 |
| Tot. Score | 0.253 | −0.002 | 0.166 | −0.042 | −0.004 | 0.163 |
| Interpers. Sens. | Behav. Inhib. | Social Sit. | Subst. Abuse | Performance | Tot. Score | |
|---|---|---|---|---|---|---|
| Child./Adolesc. | 0.386 * | −0.053 | −0.105 | −0.058 | −0.273 | −0.025 |
| Verb. comm. | 0.416 * | 0.265 | 0.006 | 0.146 | 0.021 | 0.200 |
| Non-verb. comm. | 0.451 * | 0.012 | 0.068 | 0.089 | −0.088 | 0.159 |
| Empathy | 0.226 | 0.023 | −0.090 | 0.135 | 0.050 | 0.059 |
| Inflex. & routine | −0.146 | 0.050 | 0.174 | −0.025 | 0.222 | 0.113 |
| Restrict. interest & rum. | −0.027 | 0.086 | 0.195 | 0.050 | 0.150 | 0.151 |
| Hyper-hyporeact. | 0.353 * | 0.112 | −0.065 | −0.006 | −0.146 | 0.056 |
| Tot. Score | 0.334 * | 0.122 | 0.111 | 0.059 | 0.041 | 0.200 |
| b (S.E) | p | Exp(B) | CI 95% | ||
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| constant | −5.44 (1.29) | <0.001 | 0.004 | ||
| Interpers. sens. | 0.29 (0.10) | 0.006 | 1.330 | 1.09 | 1.63 |
| Behav. inhib. | 0.36 (0.34) | 0.320 | 1.430 | 0.72 | 2.82 |
| Social sit. | 0.34 (0.19) | 0.072 | 1.402 | 0.97 | 2.02 |
| Subst. abuse | 1.49 (0.64) | 0.020 | 4.444 | 1.26 | 15.67 |
| Performance | 0.07 (0.18) | 0.679 | 1.076 | 0.76 | 1.52 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carpita, B.; Cremone, I.M.; Nardi, B.; Amatori, G.; Bonelli, C.; Massimetti, E.; Casagrande, D.; Pini, S.; Dell’Osso, L. Implications of Social Anxiety Symptoms in Adults with Autism Spectrum Disorder: Is There a Predictive Role of Interpersonal Sensitivity and Substance Abuse? Brain Sci. 2023, 13, 1559. https://doi.org/10.3390/brainsci13111559
Carpita B, Cremone IM, Nardi B, Amatori G, Bonelli C, Massimetti E, Casagrande D, Pini S, Dell’Osso L. Implications of Social Anxiety Symptoms in Adults with Autism Spectrum Disorder: Is There a Predictive Role of Interpersonal Sensitivity and Substance Abuse? Brain Sciences. 2023; 13(11):1559. https://doi.org/10.3390/brainsci13111559
Chicago/Turabian StyleCarpita, Barbara, Ivan Mirko Cremone, Benedetta Nardi, Giulia Amatori, Chiara Bonelli, Enrico Massimetti, Danila Casagrande, Stefano Pini, and Liliana Dell’Osso. 2023. "Implications of Social Anxiety Symptoms in Adults with Autism Spectrum Disorder: Is There a Predictive Role of Interpersonal Sensitivity and Substance Abuse?" Brain Sciences 13, no. 11: 1559. https://doi.org/10.3390/brainsci13111559