
The Efficacy of Cognitive Training on Neuropsychological Outcomes in Mild Cognitive Impairment: A Meta-Analysis
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Registration
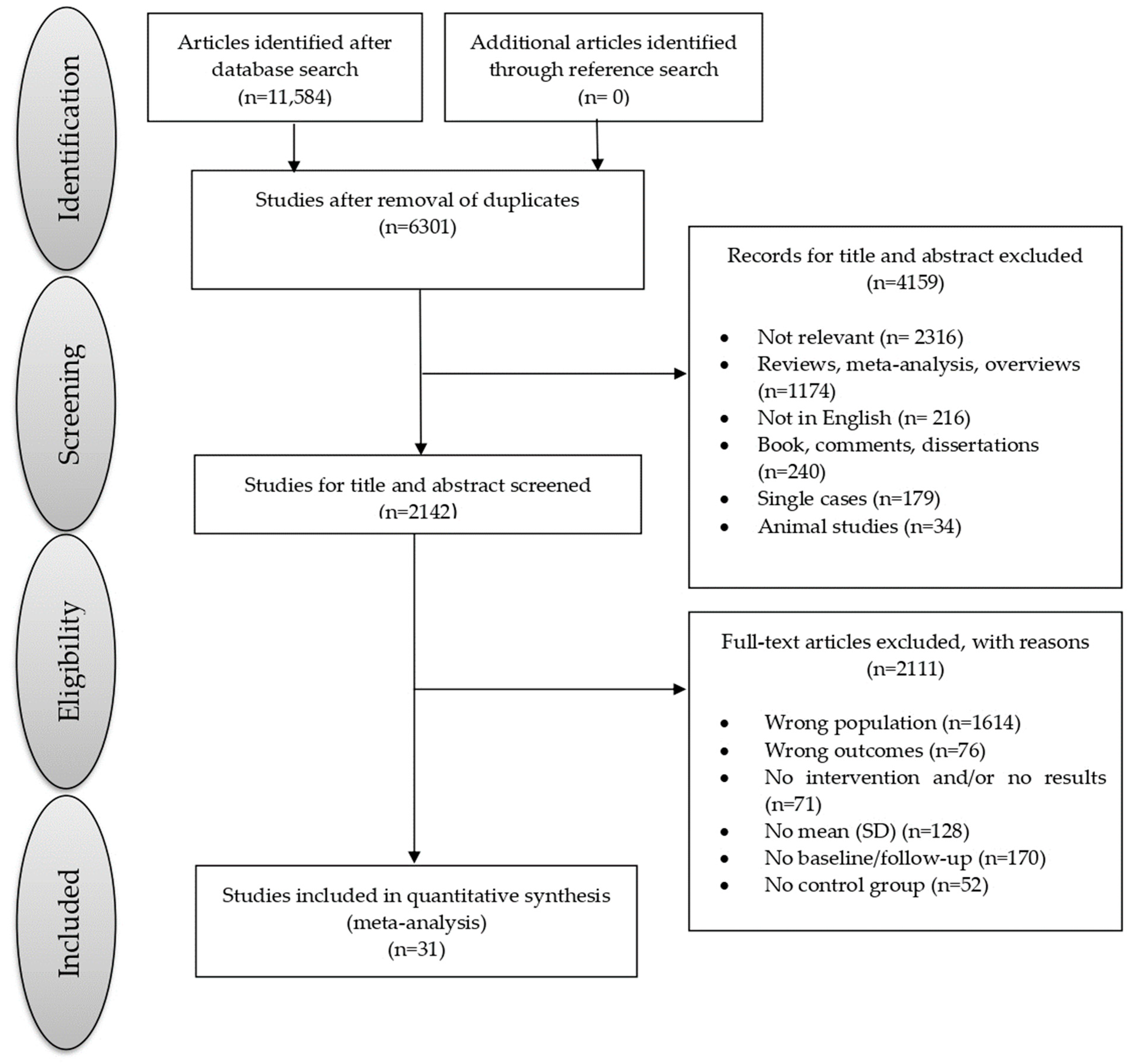
2.2. Data Sources and Study Selection
2.3. Screening and Data Extraction
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Meta-Analytic Results
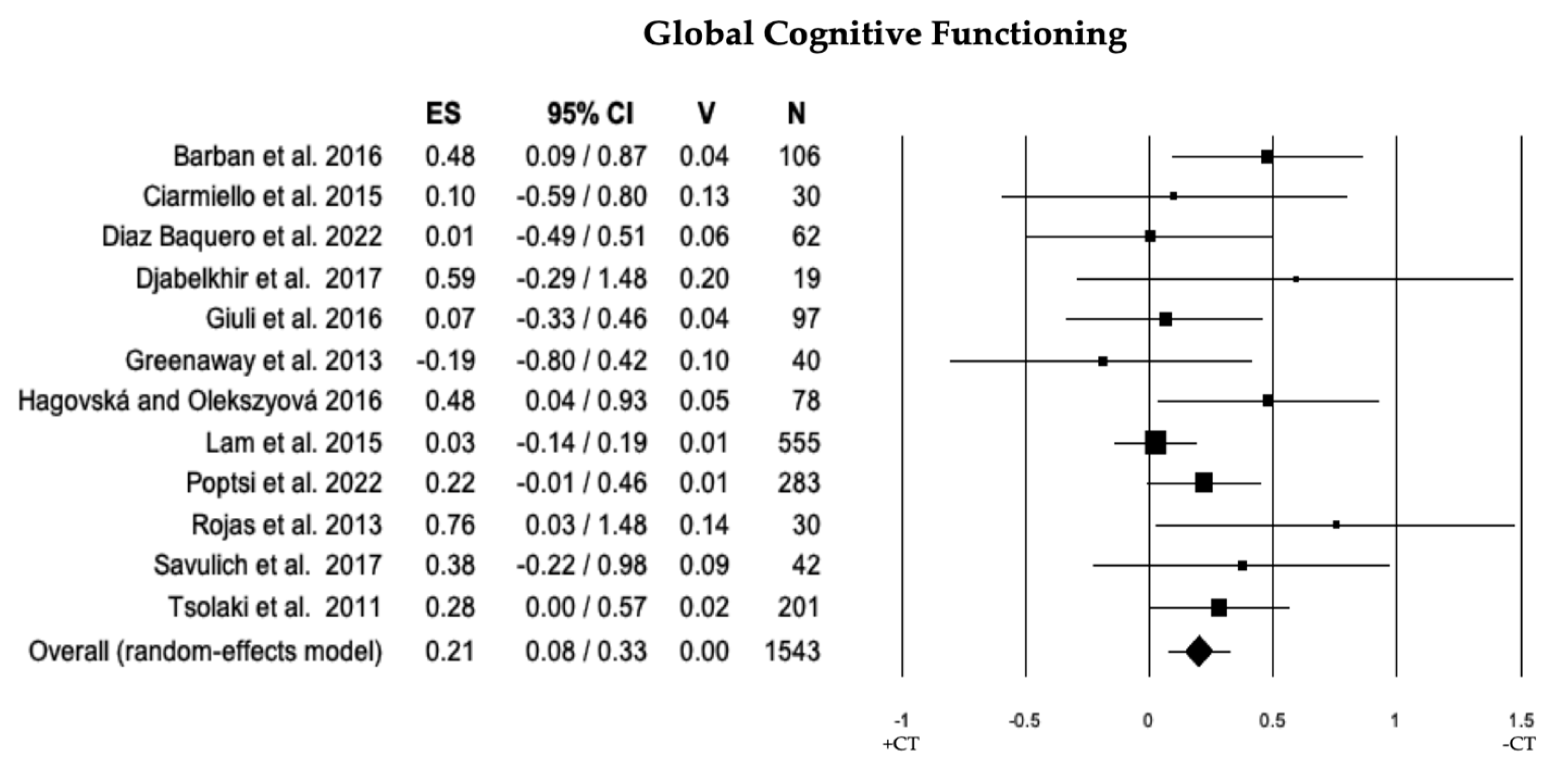
3.2.1. Global Cognitive Functioning
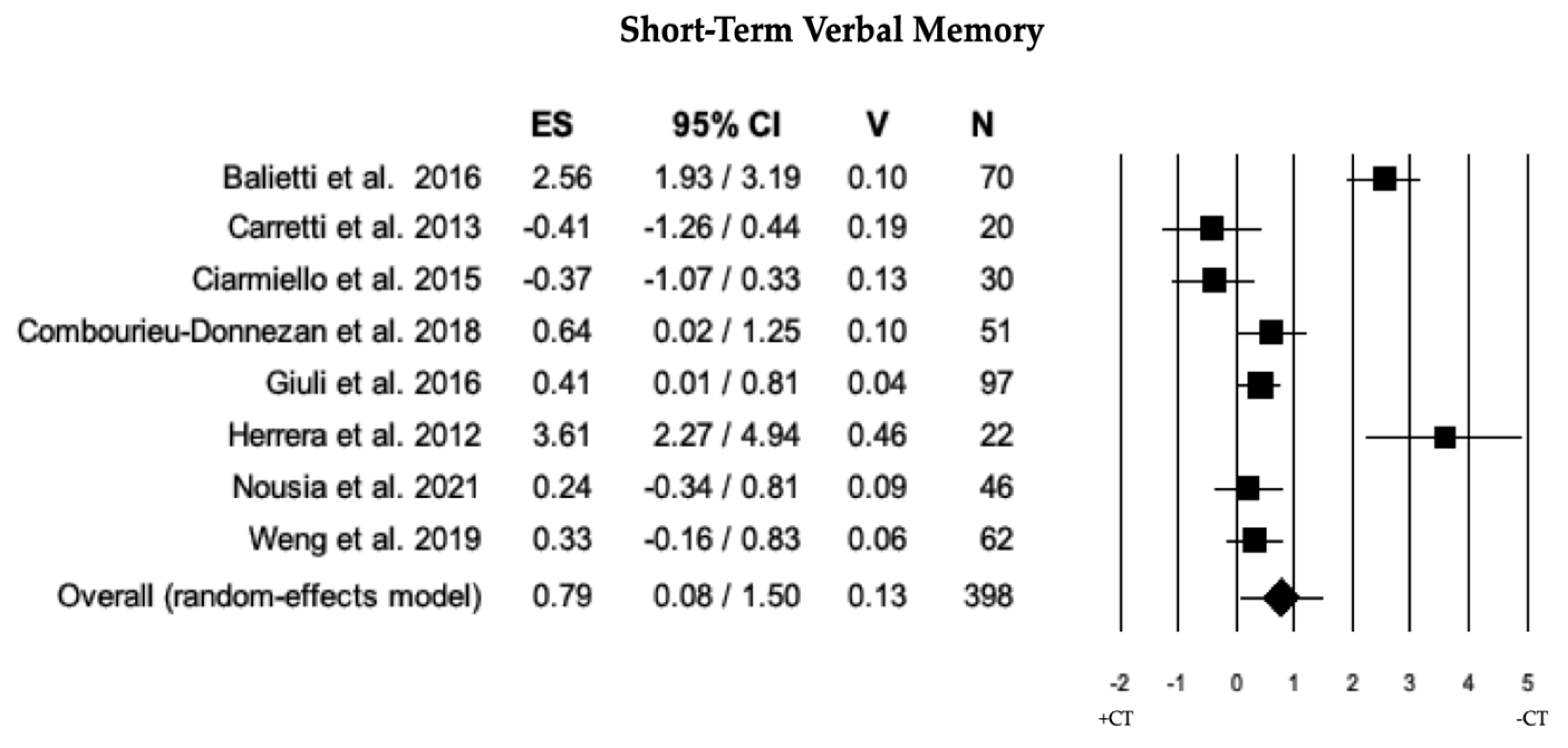
3.2.2. Short-Term Verbal Memory
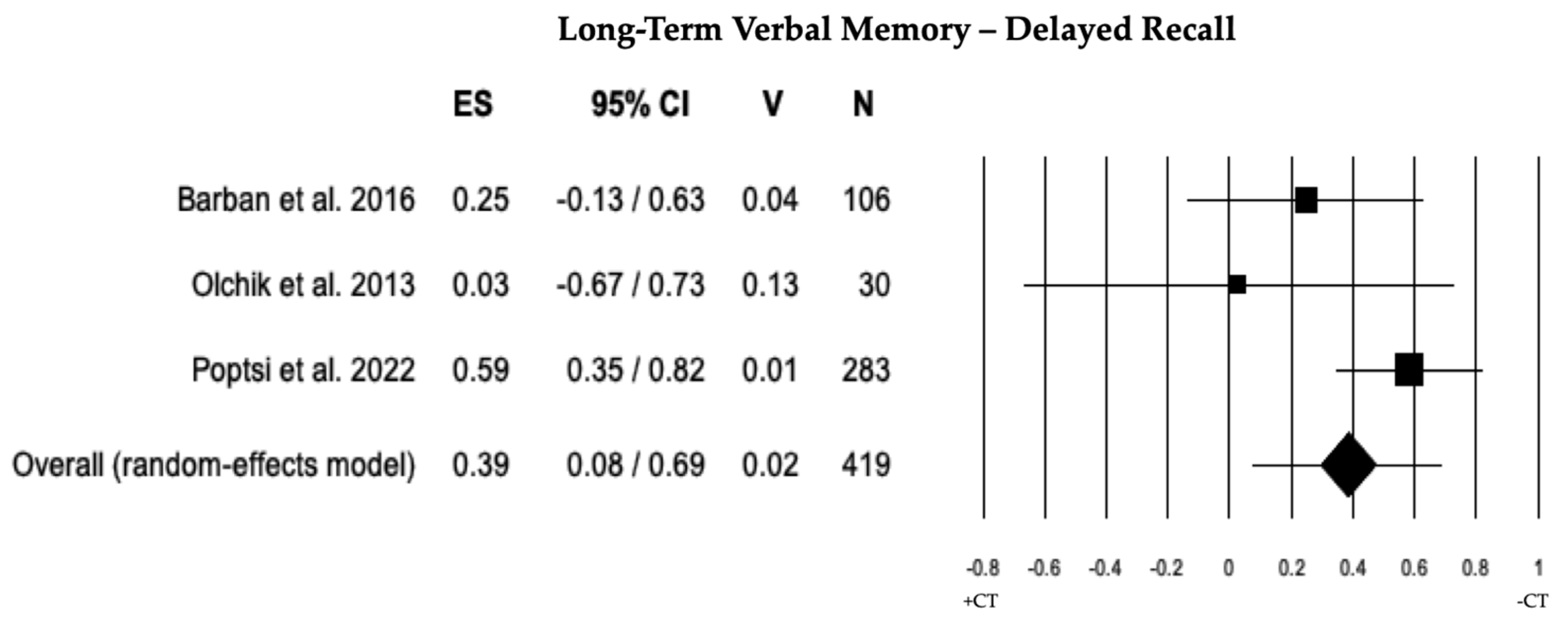
3.2.3. Long-Term Verbal Memory
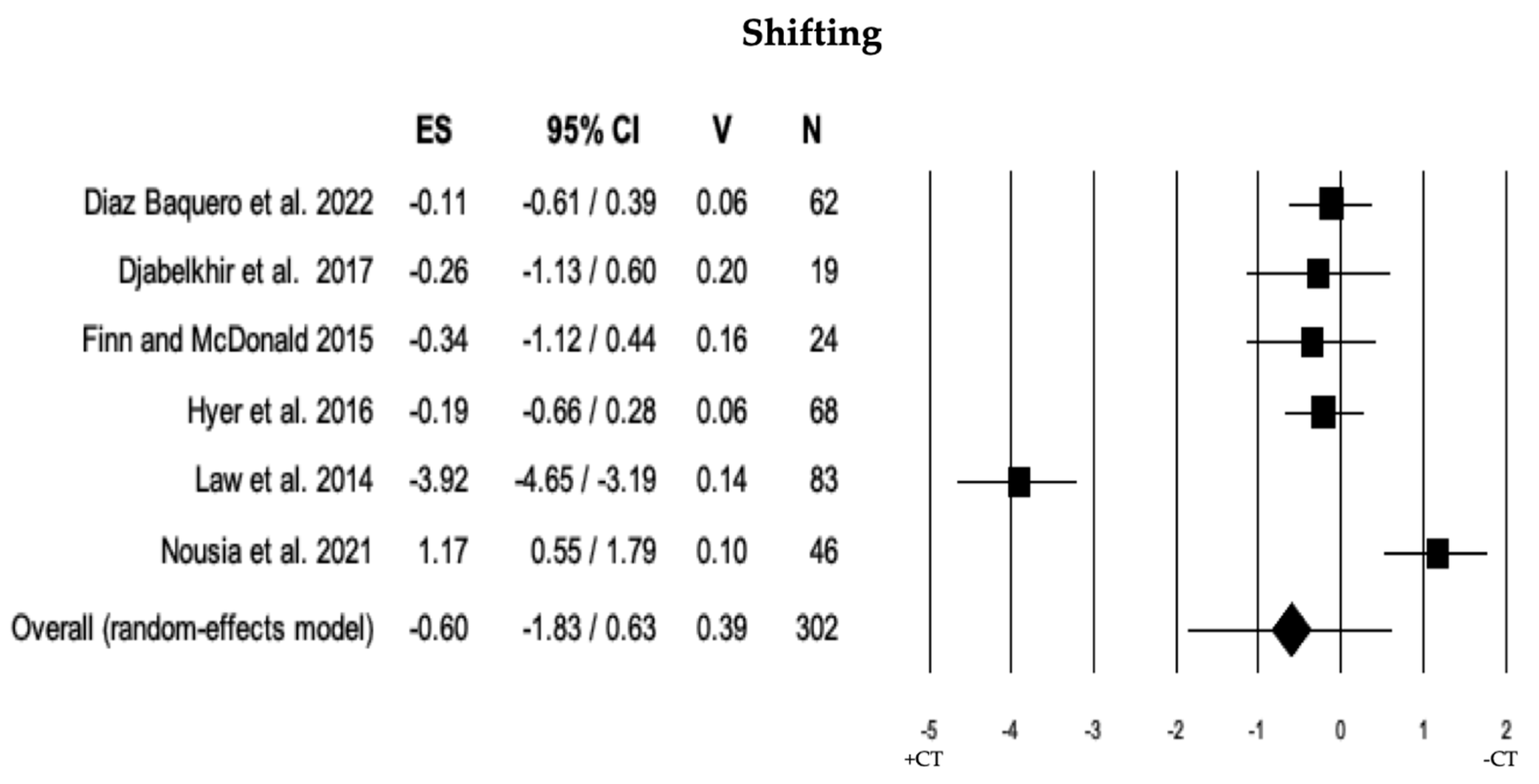
3.2.4. Shifting
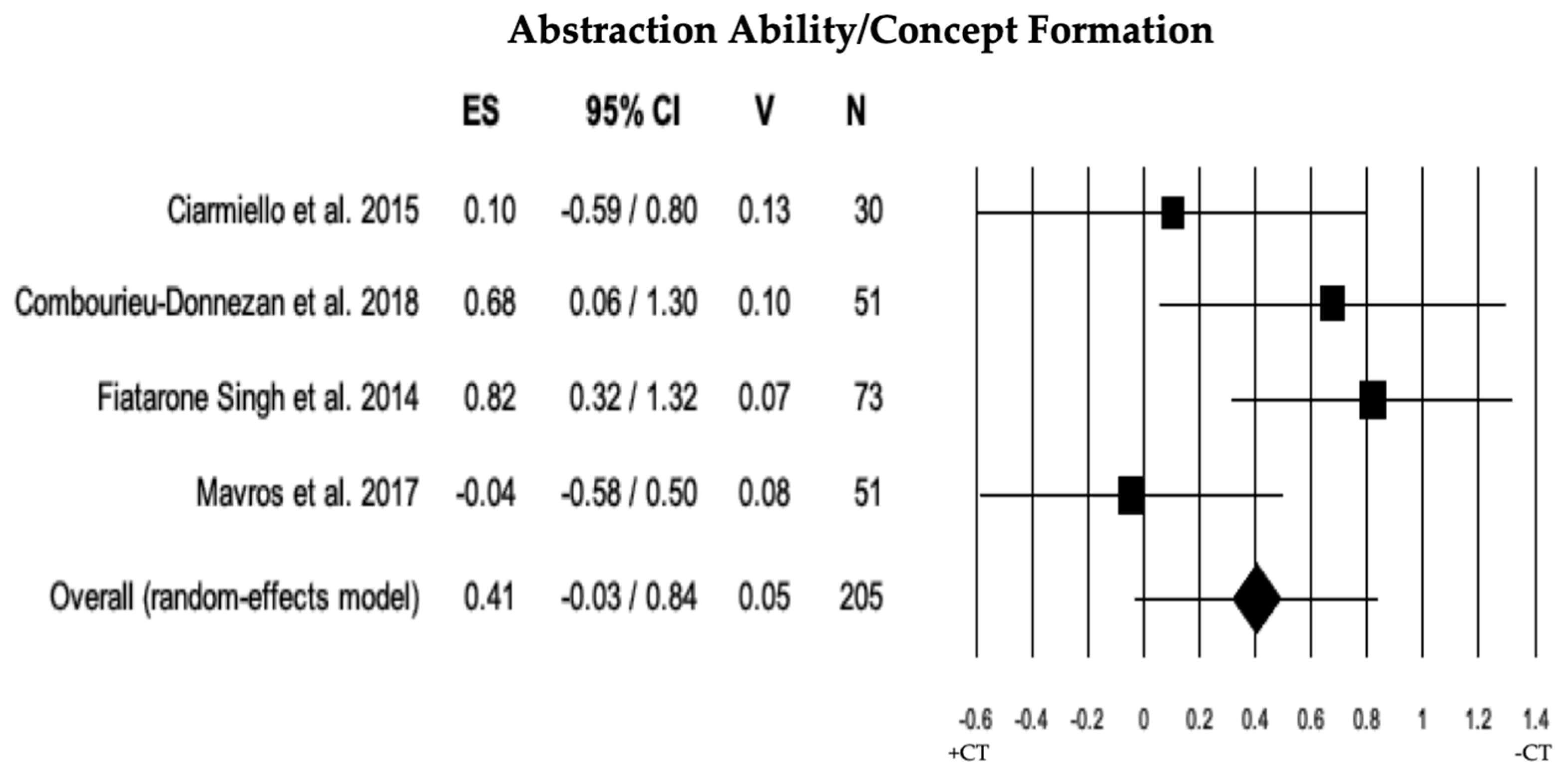
3.2.5. Abstraction Ability/Concept Formation
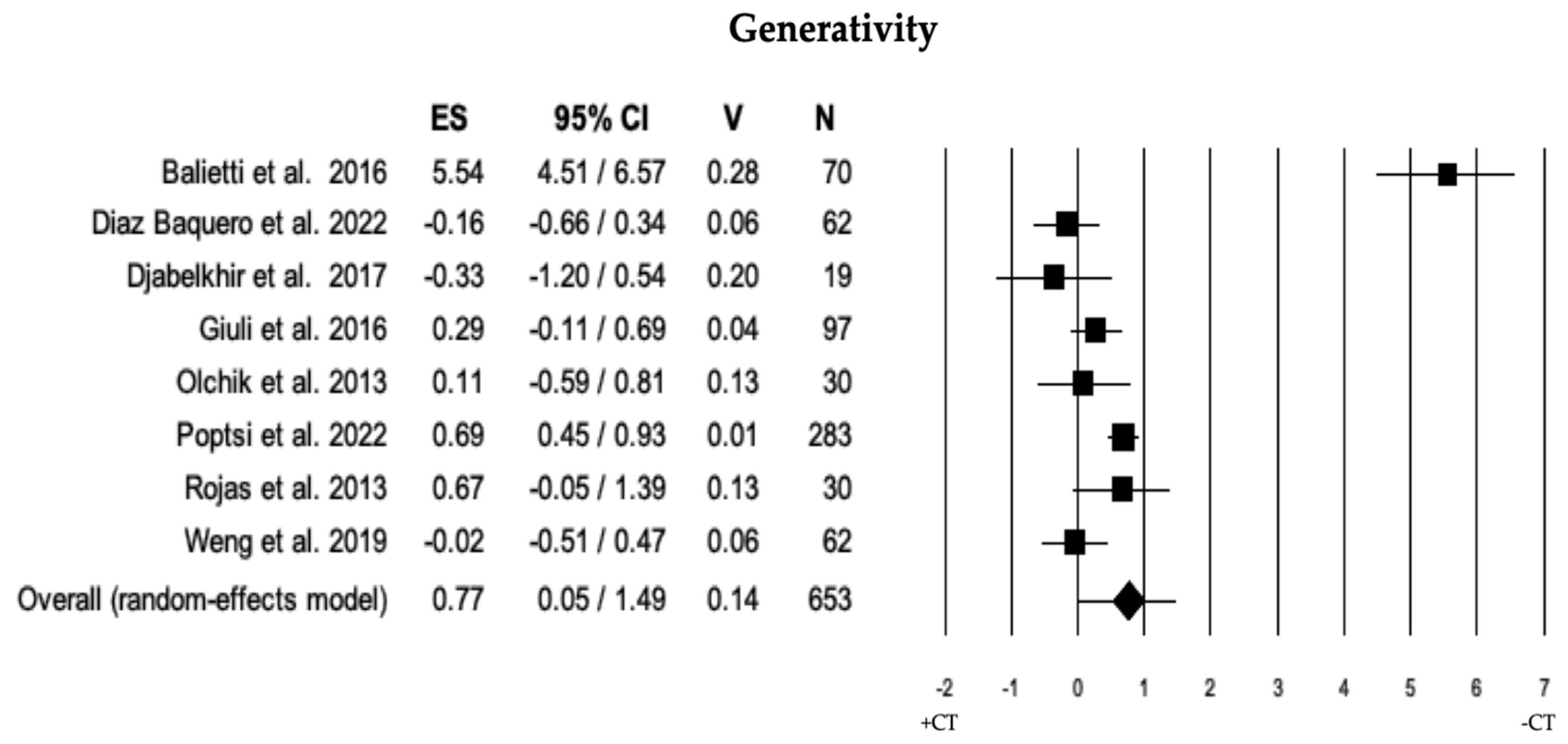
3.2.6. Generativity
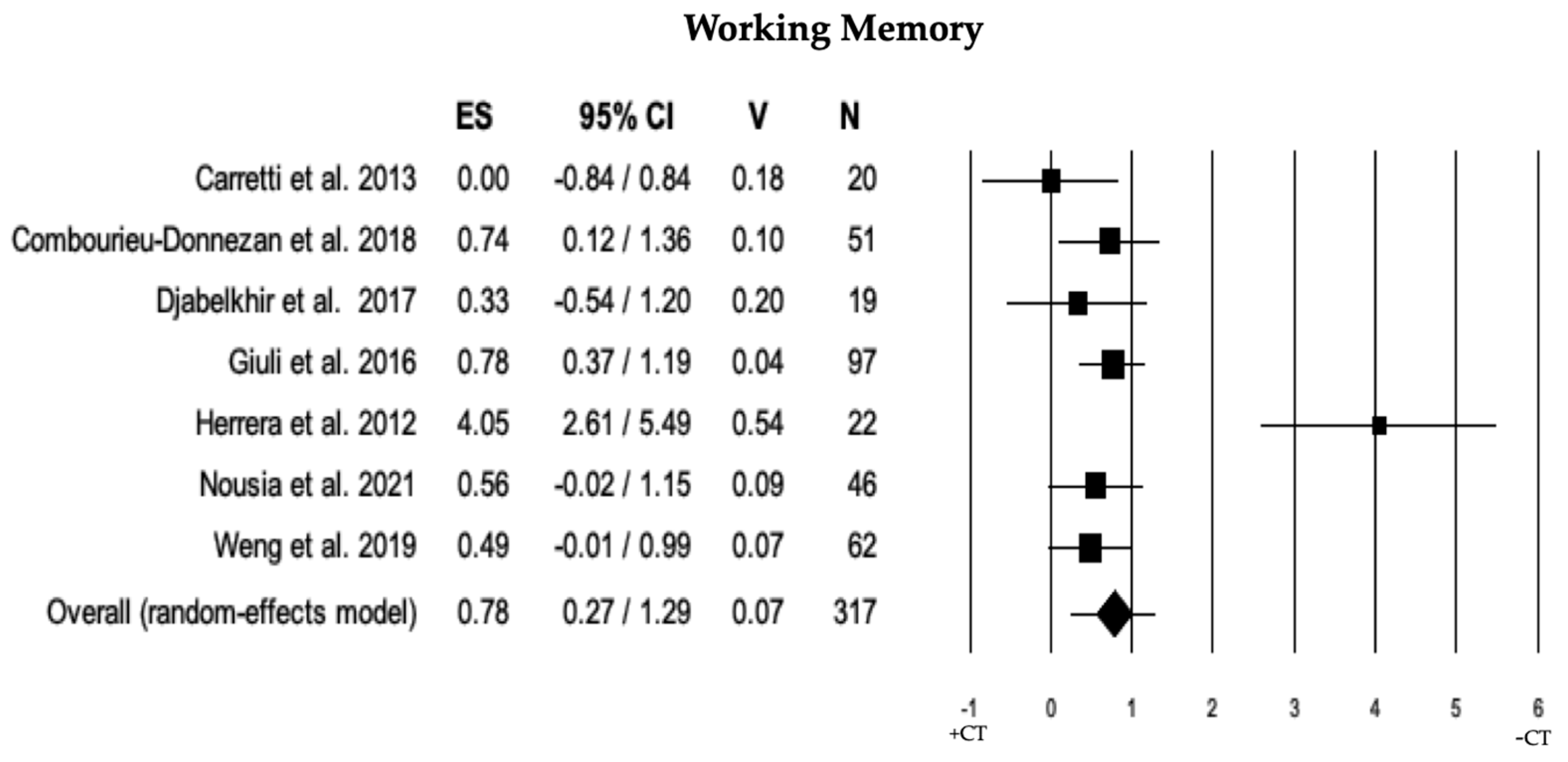
3.2.7. Working Memory
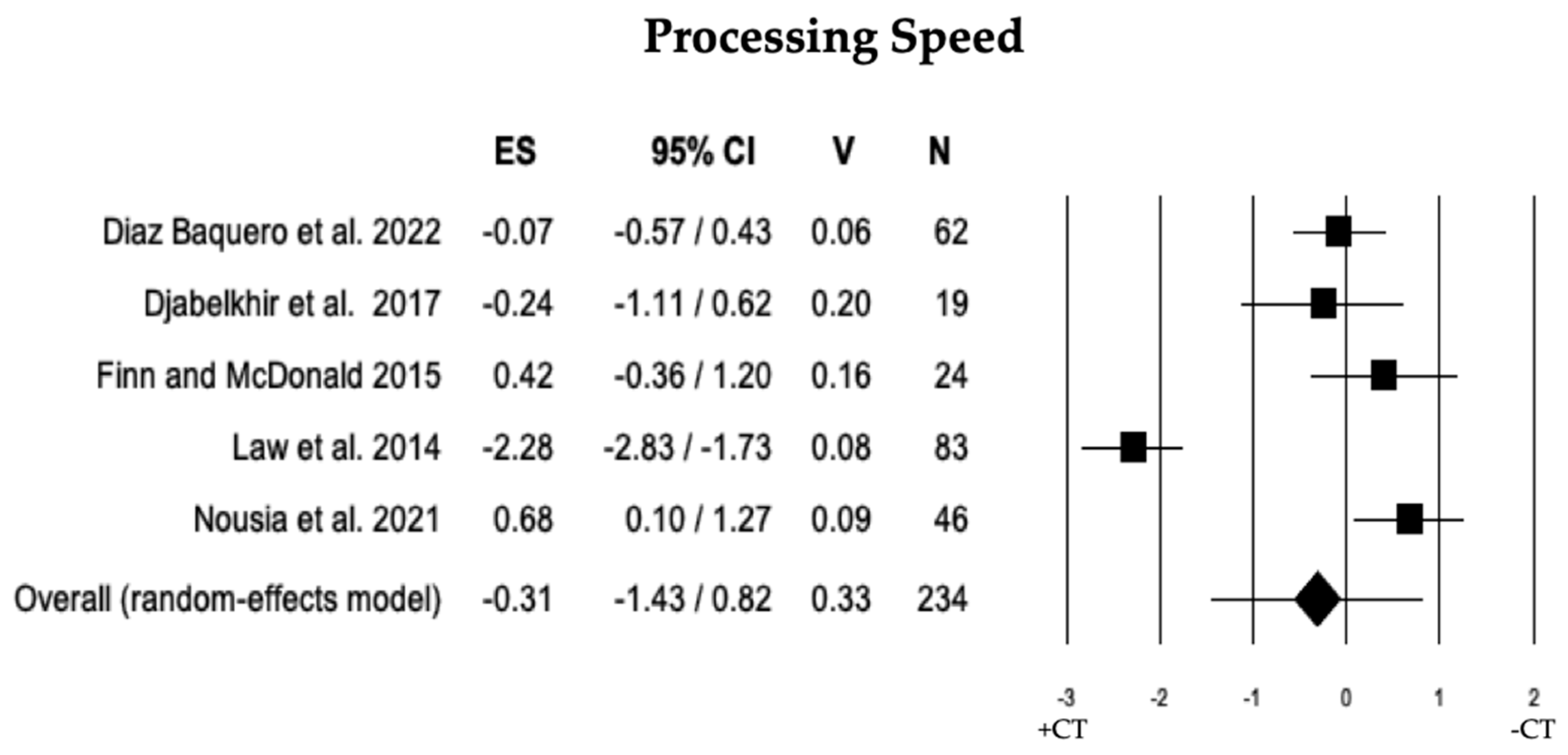
3.2.8. Processing Speed
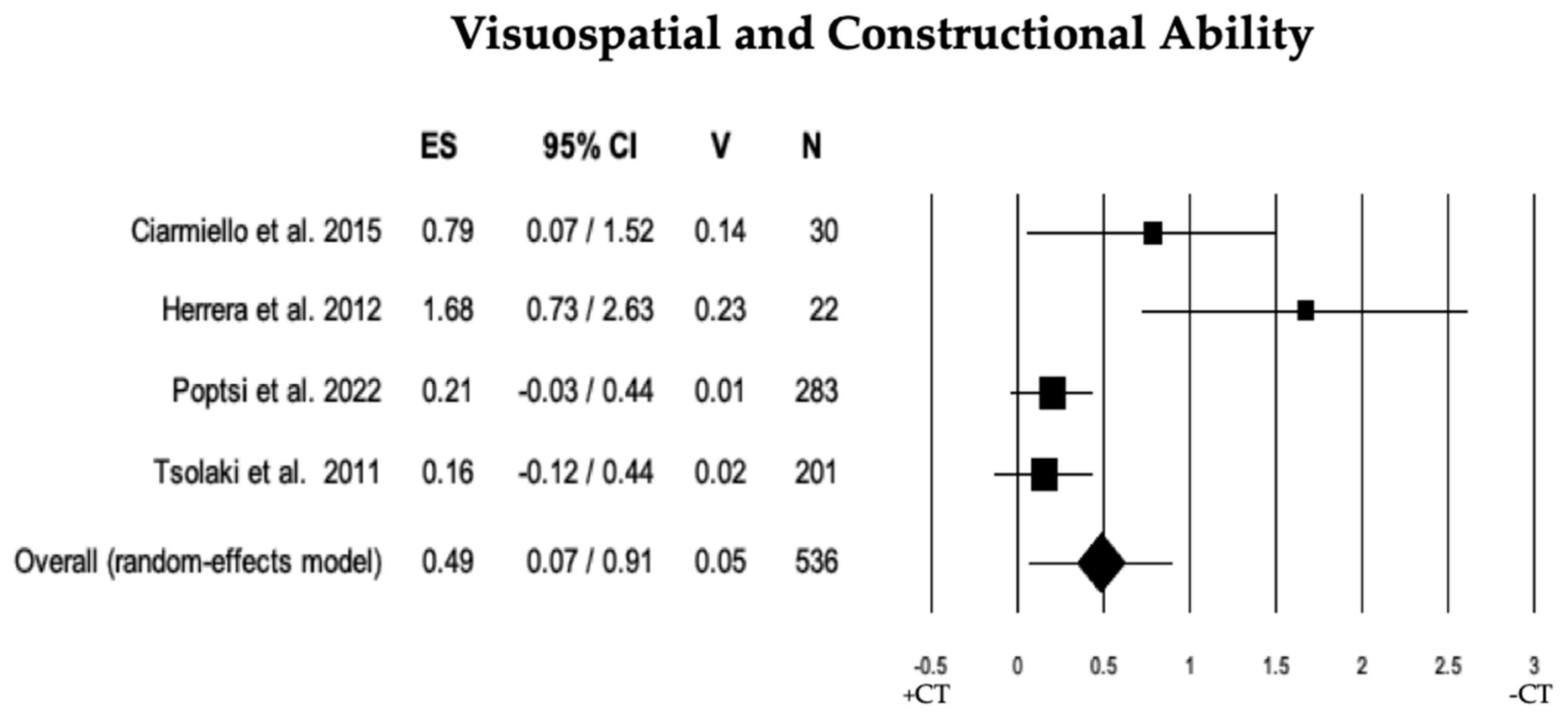
3.2.9. Visuospatial and Constructional Ability
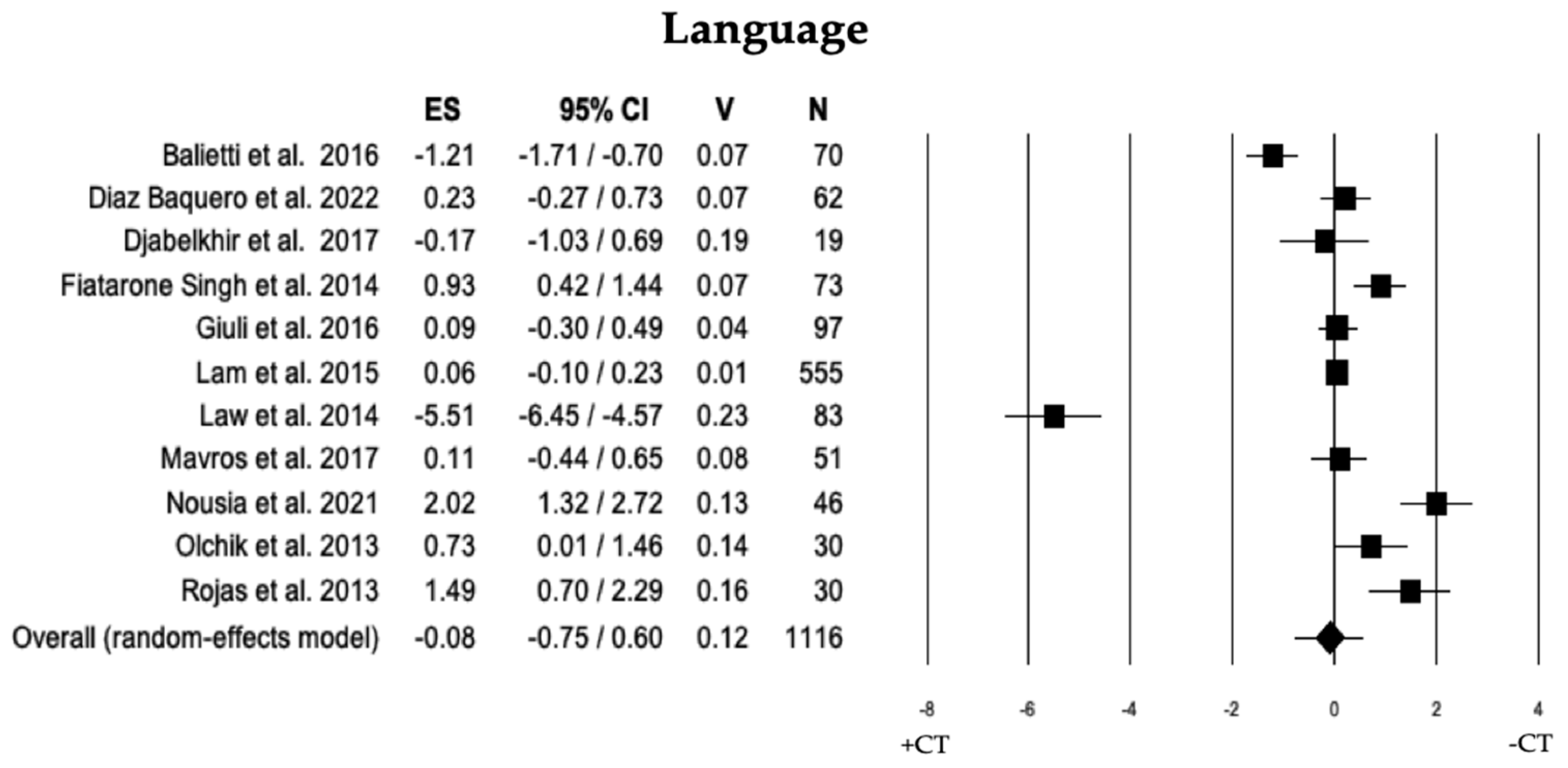
3.2.10. Language
3.3. Moderator Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing, Inc.: Arlington, VA, USA, 2013. [Google Scholar]
- Koepsell, T.D.; Monsell, S.E. Reversion from mild cognitive impairment to normal or near-normal cognition: Risk factors and prognosis. Neurology 2012, 79, 1591–1598. [Google Scholar] [CrossRef]
- Gauthier, S.; Reisberg, B.; Zaudig, M.; Petersen, R.C.; Ritchie, K.; Broich, K.; Belleville, S.; Brodaty, H.; Bennett, D.; Chertkow, H.; et al. Mild cognitive impairment. Lancet 2006, 367, 1262–1270. [Google Scholar] [CrossRef] [PubMed]
- Alves, J.; Magalhaes, R.; Thomas, R.E.; Goncalves, O.F.; Petrosyan, A.; Sampaio, A. Is there evidence for cognitive intervention in Alzheimer disease? A systematic review of efficacy, feasibility, and cost-effectiveness. Alzheimer Dis. Assoc. Disord. 2013, 27, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Abrahamson, K. Cognitive interventions for individuals with mild cognitive impairment: A systematic review. Int. J. Nurs. Sci. 2016, 3, 180–195. [Google Scholar] [CrossRef]
- Sherman, D.S.; Mauser, J.; Nuno, M. A randomized controlled trial of cognitive training using a visual speed of processing intervention in middle aged and older adults. PLoS ONE 2017, 12, e0169002. [Google Scholar] [CrossRef]
- Giuli, C.; Fattoretti, P.; Lattanzio, F.; Balietti, M.; Di Stefano, G.; Solazzi, M. Cognitive rehabilitation in patients affected by mild cognitive impairment: A systematic review. Front. Aging Neurosci. 2016, 8, 206. [Google Scholar] [CrossRef]
- Clare, L.; Woods, R.T. Cognitive training and cognitive rehabilitation for people with early-stage Alzheimer’s disease: A review. Neuropsychol. Rehabil. 2003, 13, 293–341. [Google Scholar] [CrossRef]
- Clare, L.; Woods, R.T. Cognitive training and cognitive rehabilitation for people with mild to moderate dementia of the Alzheimer’s or vascular type: A review. Neuropsychol. Rehabil. 2004, 14, 385–401. [Google Scholar] [CrossRef]
- Bahar-Fuchs, A.; Clare, L.; Woods, B. Cognitive training and cognitive rehabilitation for mild to moderate Alzheimer’s disease and vascular dementia. Cochrane Database Syst. Rev. 2013, 2013, CD003260. [Google Scholar] [CrossRef]
- Martin, M.; Clare, L.; Altgassen, A.M.; Cameron, M.H.; Zehnder, F. Cognition-based interventions for healthy older people and people with mild cognitive impairment. Cochrane Database Syst. Rev. 2011, 1, CD006220. [Google Scholar] [CrossRef]
- Simon, S.S.; Yokomizo, J.E.; Bottino, C.M. Cognitive intervention in amnestic Mild Cognitive Impairment: A systematic review. Neurosci. Biobehav. Rev. 2012, 36, 1163–1178. [Google Scholar] [CrossRef]
- Liao, Y.Y.; Tseng, H.Y.; Lin, Y.J.; Wang, C.J.; Hsu, W.C. Using virtual reality-based training to improve cognitive function, instrumental activities of daily living and neural efficiency in older adults with mild cognitive impairment. Eur. J. Phys. Rehabil. Med. 2020, 56, 47–57. [Google Scholar] [CrossRef]
- Stern, Y. Cognitive reserve in ageing and Alzheimer’s disease. Lancet Neurol. 2012, 11, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Wirth, M.; Haase, C.M.; Villeneuve, S.; Vogel, J.; Jagust, W.J. Neuroprotective pathways: Lifestyle activity, brain pathology, and cognition in cognitively normal older adults. Neurobiol. Aging 2014, 35, 1873–1882. [Google Scholar] [CrossRef] [PubMed]
- Passow, S.; Thurm, F.; Li, S.C. Activating Developmental Reserve Capacity Via Cognitive Training or Non-invasive Brain Stimulation: Potentials for Promoting Fronto-Parietal and Hippocampal-Striatal Network Functions in Old Age. Front. Aging Neurosci. 2017, 9, 33. [Google Scholar] [CrossRef]
- Gutchess, A. Plasticity of the aging brain: New directions in cognitive neuroscience. Science 2014, 346, 579–582. [Google Scholar] [CrossRef]
- Zhang, H.; Huntley, J.; Bhome, R.; Holmes, B.; Cahill, J.; Gould, R.L.; Wang, H.; Yu, X.; Howard, R. Effect of computerised cognitive training on cognitive outcomes in mild cognitive impairment: A systematic review and meta-analysis. BMJ Open 2019, 9, e027062. [Google Scholar] [CrossRef] [PubMed]
- Reijnders, J.; van Heugten, C.; van Boxtel, M. Cognitive interventions in healthy older adults and people with mild cognitive impairment: A systematic review. Ageing Res. Rev. 2013, 12, 263–275. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; The PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Santangelo, G.; Raimo, S.; Cropano, M.; Vitale, C.; Barone, P.; Trojano, L. Neural bases of impulse control disorders in Parkinson’s disease: A systematic review and an ALE meta-analysis. Neurosci. Biobehav. 2019, 107, 672–685. [Google Scholar] [CrossRef] [PubMed]
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G.; ESH Working Group on CV Risk in Low Resource Settings. Panethnic differences in blood pressure in Europe: A systematic review and meta-analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Huedo-Medina, T.B.; Sánchez-Meca, J.; Marín-Martínez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193–206. [Google Scholar] [CrossRef]
- Rothstein, H.R.; Sutton, A.J.; Borenstein, M. Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments; John Wiley & Sons: Hoboken, NJ, USA, 2005. [Google Scholar]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Balietti, M.; Giuli, C.; Fattoretti, P.; Fabbietti, P.; Postacchini, D.; Conti, F. Cognitive Stimulation Modulates Platelet Total Phospholipases A2 Activity in Subjects with Mild Cognitive Impairment. J. Alzheimers Dis. 2016, 50, 957–962. [Google Scholar] [CrossRef]
- Barban, F.; Annicchiarico, R.; Pantelopoulos, S.; Federici, A.; Perri, R.; Fadda, L.; Carlesimo, G.A.; Ricci, C.; Giuli, S.; Scalici, F.; et al. Protecting cognition from aging and Alzheimer’s disease: A computerized cognitive training combined with reminiscence therapy. Int. J. Geriatr. Psychiatry 2016, 31, 340–348. [Google Scholar] [CrossRef]
- Carretti, B.; Borella, E.; Fostinelli, S.; Zavagnin, M. Benefits of training working memory in amnestic mild cognitive impairment: Specific and transfer effects. Int. Psychogeriatr. 2013, 25, 617–626. [Google Scholar] [CrossRef]
- Chen, Q.; Yang, H.; Rooks, B.; Anthony, M.; Zhang, Z.; Tadin, D.; Heffner, K.L.; Lin, F.V. Autonomic flexibility reflects learning and associated neuroplasticity in old age. Hum. Brain Mapp. 2020, 41, 3608–3619. [Google Scholar] [CrossRef] [PubMed]
- Ciarmiello, A.; Gaeta, M.C.; Benso, F.; Del Sette, M. FDG-PET in the Evaluation of Brain Metabolic Changes Induced by Cognitive Stimulation in aMCI Subjects. Curr. Radiopharm. 2015, 8, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Donnezan, L.C.; Perrot, A.; Belleville, S.; Bloch, F.; Kemoun, G. Effects of simultaneous aerobic and cognitive training on executive functions, cardiovascular fitness and functional abilities in older adults with mild cognitive impairment. Ment. Health Phys. Act. 2018, 15, 78–87. [Google Scholar] [CrossRef]
- Diaz Baquero, A.A.; Franco-Martín, M.A.; Parra Vidales, E.; Toribio-Guzmán, J.M.; Bueno-Aguado, Y.; Martínez Abad, F.; Perea Bartolomé, M.V.; Asl, A.M.; van der Roest, H.G. The Effectiveness of GRADIOR: A Neuropsychological Rehabilitation Program for People with Mild Cognitive Impairment and Mild Dementia. Results of a Randomized Controlled Trial After 4 and 12 Months of Treatment. J. Alzheimers Dis. 2022, 86, 711–727. [Google Scholar] [CrossRef]
- Djabelkhir, L.; Wu, Y.H.; Vidal, J.S.; Cristancho-Lacroix, V.; Marlats, F.; Lenoir, H.; Carno, A.; Rigaud, A.S. Computerized cognitive stimulation and engagement programs in older adults with mild cognitive impairment: Comparing feasibility, acceptability, and cognitive and psychosocial effects. Clin. Interv. Aging 2017, 12, 1967–1975. [Google Scholar] [CrossRef] [PubMed]
- Duff, K.; Ying, J.; Suhrie, K.R.; Dalley, B.C.A.; Atkinson, T.J.; Porter, S.M.; Dixon, A.M.; Hammers, D.B.; Wolinsky, F.D. Computerized Cognitive Training in Amnestic Mild Cognitive Impairment: A Randomized Clinical Trial. J. Geriatr. Psychiatry Neurol. 2022, 35, 400–409. [Google Scholar] [CrossRef] [PubMed]
- Fiatarone Singh, M.A.; Gates, N.; Saigal, N.; Wilson, G.C.; Meiklejohn, J.; Brodaty, H.; Wen, W.; Singh, N.; Baune, B.T.; Suo, C.; et al. The Study of Mental and Resistance Training (SMART) study—Resistance training and/or cognitive training in mild cognitive impairment: A randomized, double-blind, double-sham controlled trial. J. Am. Med. Dir. Assoc. 2014, 15, 873–880. [Google Scholar] [CrossRef] [PubMed]
- Finn, M.; McDonald, S. Repetition-lag training to improve recollection memory in older people with amnestic mild cognitive impairment. A randomized controlled trial. Neuropsychology, development, and cognition. Neuropsychol. Dev. Cogn. B Aging Neuropsychol. Cogn. 2015, 22, 244–258. [Google Scholar] [CrossRef]
- Giuli, C.; Papa, R.; Lattanzio, F.; Postacchini, D. The Effects of Cognitive Training for Elderly: Results from My Mind Project. Rejuvenation Res. 2016, 19, 485–494. [Google Scholar] [CrossRef]
- Greenaway, M.C.; Duncan, N.L.; Smith, G.E. The memory support system for mild cognitive impairment: Randomized trial of a cognitive rehabilitation intervention. Int. J. Geriatr. Psychiatry 2013, 28, 402–409. [Google Scholar] [CrossRef]
- Hagovská, M.; Olekszyová, Z. Impact of the combination of cognitive and balance training on gait, fear and risk of falling and quality of life in seniors with mild cognitive impairment. Geriatr. Gerontol. Int. 2016, 16, 1043–1050. [Google Scholar] [CrossRef]
- Herrera, C.; Chambon, C.; Michel, B.F.; Paban, V.; Alescio-Lautier, B. Positive effects of computer-based cognitive training in adults with mild cognitive impairment. Neuropsychologia 2012, 50, 1871–1881. [Google Scholar] [CrossRef]
- Hughes, T.F.; Flatt, J.D.; Fu, B.; Butters, M.A.; Chang, C.C.; Ganguli, M. Interactive video gaming compared with health education in older adults with mild cognitive impairment: A feasibility study. Int. J. Geriatr. Psychiatry 2014, 29, 890–898. [Google Scholar] [CrossRef]
- Hyer, L.; Scott, C.; Atkinson, M.M.; Mullen, C.M.; Lee, A.; Johnson, A.; Mckenzie, L.C. Cognitive Training Program to Improve Working Memory in Older Adults with MCI. Clin. Gerontol. 2016, 39, 410–427. [Google Scholar] [CrossRef]
- Lam, L.C.; Chan, W.C.; Leung, T.; Fung, A.W.; Leung, E.M. Would older adults with mild cognitive impairment adhere to and benefit from a structured lifestyle activity intervention to enhance cognition?: A cluster randomized controlled trial. PLoS ONE 2015, 10, e0118173. [Google Scholar] [CrossRef]
- Law, L.L.; Barnett, F.; Yau, M.K.; Gray, M.A. Effects of functional tasks exercise on older adults with cognitive impairment at risk of Alzheimer's disease: A randomised controlled trial. Age Ageing 2014, 43, 813–820. [Google Scholar] [CrossRef]
- Lin, F.; Heffner, K.L.; Ren, P.; Tivarus, M.E.; Brasch, J.; Chen, D.G.; Mapstone, M.; Porsteinsson, A.P.; Tadin, D. Cognitive and Neural Effects of Vision-Based Speed-of-Processing Training in Older Adults with Amnestic Mild Cognitive Impairment: A Pilot Study. J. Am. Geriatr. Soc. 2016, 64, 1293–1298. [Google Scholar] [CrossRef]
- Mavros, Y.; Gates, N.; Wilson, G.C.; Jain, N.; Meiklejohn, J.; Brodaty, H.; Wen, W.; Singh, N.; Baune, B.T.; Suo, C.; et al. Mediation of Cognitive Function Improvements by Strength Gains After Resistance Training in Older Adults with Mild Cognitive Impairment: Outcomes of the Study of Mental and Resistance Training. J. Am. Geriatr. Soc. 2017, 63, 550–559. [Google Scholar] [CrossRef]
- Nousia, A.; Martzoukou, M.; Siokas, V.; Aretouli, E.; Aloizou, A.M.; Folia, V.; Peristeri, E.; Messinis, L.; Nasios, G.; Dardiotis, E. Beneficial effect of computer-based multidomain cognitive training in patients with mild cognitive impairment. Appl. Neuropsychol. Adult 2021, 28, 717–726. [Google Scholar] [CrossRef]
- Olchik, M.R.; Farina, J.; Steibel, N.; Teixeira, A.R.; Yassuda, M.S. Memory training (MT) in mild cognitive impairment (MCI) generates change in cognitive performance. Arch. Gerontol. Geriatr. 2013, 56, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Poptsi, E.; Tsatali, M.; Agogiatou, C.; Bakoglidou, E.; Batsila, G.; Dellaporta, D.; Kounti-Zafeiropoulou, F.; Liapi, D.; Lysitsas, K.; Markou, N.; et al. Longitudinal Cognitive and Physical Training Effectiveness in MCI, Based on the Experience of the Alzheimer's Hellas Day Care Centre. J. Geriatr. Psychiatry Neurol. 2022, 35, 512–526. [Google Scholar] [CrossRef] [PubMed]
- Rapp, S.; Brenes, G.; Marsh, A.P. Memory enhancement training for older adults with mild cognitive impairment: A preliminary study. Aging Ment. Health 2002, 6, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Rojas, G.J.; Villar, V.; Iturry, M.; Harris, P.; Serrano, C.M.; Herrera, J.A.; Allegri, R.F. Efficacy of a cognitive intervention program in patients with mild cognitive impairment. Int. Psychogeriatr. 2013, 25, 825–831. [Google Scholar] [CrossRef]
- Schmitter-Edgecombe, M.; Dyck, D.G. Cognitive rehabilitation multi-family group intervention for individuals with mild cognitive impairment and their care-partners. J. Int. Neuropsychol. Soc. 2014, 20, 897–908. [Google Scholar] [CrossRef] [PubMed]
- Savulich, G.; Piercy, T.; Fox, C.; Suckling, J.; Rowe, J.B.; O'Brien, J.T.; Sahakian, B.J. Cognitive Training Using a Novel Memory Game on an iPad in Patients with Amnestic Mild Cognitive Impairment (aMCI). Int. J. Neuropsychopharmacol. 2017, 20, 624–633. [Google Scholar] [CrossRef]
- Sukontapol, C.; Kemsen, S.; Chansirikarn, S.; Nakawiro, D.; Kuha, O.; Taemeeyapradit, U. The effectiveness of a cognitive training program in people with mild cognitive impairment: A study in urban community. Asian J. Psychiatr. 2021, 35, 18–23, Erratum in Asian J. Psychiatr. 2021, 55, 102000. [Google Scholar] [CrossRef]
- Tsolaki, M.; Kounti, F.; Agogiatou, C.; Poptsi, E.; Bakoglidou, E.; Zafeiropoulou, M.; Soumbourou, A.; Nikolaidou, E.; Batsila, G.; Siambani, A.; et al. Effectiveness of nonpharmacological approaches in patients with mild cognitive impairment. Neurodegener Dis. 2011, 8, 138–145. [Google Scholar] [CrossRef]
- Weng, W.; Liang, J.; Xue, J.; Zhu, T.; Jiang, Y.; Wang, J.; Chen, S. The Transfer Effects of Cognitive Training on Working Memory Among Chinese Older Adults with Mild Cognitive Impairment: A Randomized Controlled Trial. Front. Aging Neurosci. 2019, 11, 212. [Google Scholar] [CrossRef] [PubMed]
- Raimo, S.; Trojano, L.; Siciliano, M.; Cuoco, S.; D'Iorio, A.; Santangelo, F.; Abbamonte, L.; Grossi, D.; Santangelo, G. Psychometric properties of the Italian version of the multifactorial memory questionnaire for adults and the elderly. Neurol. Sci. 2016, 37, 681–691. [Google Scholar] [CrossRef] [PubMed]
- Vega, J.N.; Newhouse, P.A. Mild cognitive impairment: Diagnosis, longitudinal course, and emerging treatments. Curr. Psychiatry Rep. 2014, 16, 490. [Google Scholar] [CrossRef]
- Bahar-Fuchs, A.; Martyr, A.; Goh, A.M.; Sabates, J.; Clare, L. Cognitive training for people with mild to moderate dementia. Cochrane Database Syst. Rev. 2019, 3, CD013069. [Google Scholar] [CrossRef]
- Hill, N.T.; Mowszowski, L.; Naismith, S.L.; Chadwick, V.L.; Valenzuela, M.; Lampit, A. Computerized Cognitive Training in Older Adults with Mild Cognitive Impairment or Dementia: A Systematic Review and Meta-Analysis. Am. J. Psychiatry 2017, 174, 329–340. [Google Scholar] [CrossRef]
- Gates, N.J.; Vernooij, R.W.; Di Nisio, M.; Karim, S.; March, E.; Martínez, G.; Rutjes, A.W. Computerised cognitive training for preventing dementia in people with mild cognitive impairment. Cochrane Database Syst. Rev. 2019, 3, CD012279. [Google Scholar] [CrossRef]
- Orgeta, V.; McDonald, K.R.; Poliakoff, E.; Hindle, J.V.; Clare, L.; Leroi, I. Cognitive training interventions for dementia and mild cognitive impairment in Parkinson’s disease. Cochrane Database Syst. Rev. 2020, 2, CD011961. [Google Scholar] [CrossRef]
- Corbo, I.; Casagrande, M. Higher-Level Executive Functions in Healthy Elderly and Mild Cognitive Impairment: A Systematic Review. J. Clin. Med. 2022, 11, 1204. [Google Scholar] [CrossRef]
- Joubert, C.; Chainay, H. Aging brain: The effect of combined cognitive and physical training on cognition as compared to cognitive and physical training alone—A systematic review. Clin. Interv. Aging 2018, 13, 1267–1301. [Google Scholar] [CrossRef] [PubMed]
- Ten Brinke, L.F.; Best, J.R.; Chan, J.L.C.; Ghag, C.; Erickson, K.I.; Handy, T.C.; Liu-Ambrose, T. The Effects of Computerized Cognitive Training with and Without Physical Exercise on Cognitive Function in Older Adults: An 8-Week Randomized Controlled Trial. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Karssemeijer, E.G.A.; Aaronson, J.A.; Bossers, W.J.; Smits, T.; Olde Rikkert, M.G.M.; Kessels, R.P.C. Positive effects of combined cognitive and physical exercise training on cognitive function in older adults with mild cognitive impairment or dementia: A meta-analysis. Ageing Res. Rev. 2017, 40, 75–83. [Google Scholar] [CrossRef]
- Stanmore, E.; Stubbs, B.; Vancampfort, D.; de Bruin, E.D.; Firth, J. The effect of active video games on cognitive functioning in clinical and non-clinical populations: A meta-analysis of randomized controlled trials. Neurosci. Biobehav. Rev. 2017, 78, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Sherman, D.S.; Mauser, J.; Nuno, M.; Sherzai, D. The Efficacy of Cognitive Intervention in Mild Cognitive Impairment (MCI): A Meta-Analysis of Outcomes on Neuropsychological Measures. Neuropsychol. Rev. 2017, 27, 440–484. [Google Scholar] [CrossRef] [PubMed]
- Gonnermann, A.; Framke, T.; Großhennig, A.; Koch, A. No solution yet for combining two independent studies in the presence of heterogeneity. Stat. Med. 2011, 34, 2476–2480. [Google Scholar] [CrossRef] [PubMed]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristic | Type of Training | Cognitive Training Characteristic | Neuropsychological Assessment | Quality Score | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Age | Education | n M | Intervention Duration (Weeks) | Session Duration (Minutes) | Session for Week | Cognitive Test | Baseline Means (SD) | Follow-Up Means (SD) | |||
| Balietti et al. [29] (MCI) | 37 | N.R. | N.R. | N.R. | Cognitive Training | 10 | 60 | 1 | Digit span forward | 4.36 (0.15) | 4.65 (0.16) | 7 |
| Corsi supraspan | 4.84 (0.16) | 5.17 (0.15) | ||||||||||
| Attentive matrices | 39.65 (1.66) | 43.39 (1.60) | ||||||||||
| Semantic verbal fluency | 1.84 (0.23) | 2.13 (0.28) | ||||||||||
| Phonological verbal fluency | 28.46 (1.31) | 31.27 (1.60) | ||||||||||
| Prose memory | 6.83 (0.68) | 8.8 (0.66) | ||||||||||
| Word-pairing test | 8.65 (0.72) | 8.98 (0.82) | ||||||||||
| 33 | N.R. | N.R. | N.R. | Active Control Training | N.R. | N.R. | N.R. | Digit span forward | 4.56 (0.13) | 4.47 (0.13) | ||
| Corsi supraspan | 5.12 (0.12) | 5.01 (0.13) | ||||||||||
| Attentive matrices | 41.32 (1.57) | 40.04 (1.43) | ||||||||||
| Semantic verbal fluency | 2.42 (0.24) | 2.40 (0.22) | ||||||||||
| Phonological verbal fluency | 24.83 (1.36) | 24.01 (1.03) | ||||||||||
| Prose memory | 7.55 (0.76) | 6.71 (0.76) | ||||||||||
| Word-pairing test | 6.91 (0.53) | 7.04 (0.50) | ||||||||||
| Barban et al. [30] (MCI) | 46 | 74.4 (5.7) | 9 (4.3) | 25 | Computer- based Cognitive Training | 12 | 60 | 2 | MMSE | 27.3 (2.1) | 27.9 (1.9) | 8 |
| RAVLT delayed recall | 4.1 (3.2) | 5 (3.6) | ||||||||||
| 60 | 72.9 (6) | 11 (4.7) | 31 | Passive Control Training | - | - | - | MMSE | 28.1 (1.4) | 27.7 (2.2) | ||
| RAVLT delayed recall | 5 (3.2) | 5 (3.6) | ||||||||||
| Carretti et al. [31] (a-MCI) | 10 | 71.8 (2.20) | 6.50 (2.83) | 6 | Cognitive Training | 5 | 90 | 1 | Dot matrix | 5.60 (2.45) | 7.90 (0.99) | 8 |
| Digit span forward | 5.40 (1.77) | 5.2 (1.68) | ||||||||||
| Digit span backward | 4 (1.63) | 4.70 (1.05) | ||||||||||
| List recall | 3 (1.15) | 4.40 (0.96) | ||||||||||
| Pattern comparison task | 153.5 (42.4) | 63.6 (55.97) | ||||||||||
| Cattel test | 13.70 (4.76) | 17.40 (4.47) | ||||||||||
| 10 | 70.6 (2.63) | 7.20 (3.29) | 4 | Active Control Training | 5 | 90 | 1 | Dot matrix | 6.70 (2.45) | 7.30 (2.05) | ||
| Digit span forward | 5.10 (1.44) | 5.50 (1.08) | ||||||||||
| Digit span backward | 3.60 (0.84) | 4.30 (1.16) | ||||||||||
| List recall | 3.30 (1.76) | 3.60 (1.77) | ||||||||||
| Pattern comparison task | 142.70 (43.60) | 141.60 (27.75) | ||||||||||
| Cattel test | 14.30 (4.21) | 13.90 (3.69) | ||||||||||
| Chen et al. [32] (a-MCI) | 46 | 75.13 (7.56) | 15.98 (2.29) | 27 | Vision-based speed of processing training | 6 | 60 | 4 | UFOV | 5.87 (0.53) | 5.52 (0.49) | 6 |
| 28 | 73.68 (6.92) | 16.68 (2.87) | 13 | Active Control Training | 6 | 60 | 4 | UFOV | 5.89 (0.50) | 5.76 (0.48) | ||
| Ciarmiello et al. [33] (MCI) | 15 | 71.22 (7.66) | 9.30 (3.02) | 5 | Computer- based Cognitive Training | 16 | 45 | 2 | MMSE | 27.87 (1.82) | 28.26 (1.54) | 8 |
| Matrix reasoning test | 29.34 (4.56) | 30.61 (3.89) | ||||||||||
| Digit span forward | 5.21 (0.81) | 5.39 (1.02) | ||||||||||
| Word span | 4.21 (0.63) | 4.13 (0.48) | ||||||||||
| Corsi span | 4.54 (0.53) | 4.72 (0.68) | ||||||||||
| Prose memory | 10.44 (2.21) | 11.57 (2.04) | ||||||||||
| Rey figure copy | 31.56 (2.81) | 32.05 (3.50) | ||||||||||
| Rey figure delayed recall | 12.64 (2.95) | 16.26 (7.55) | ||||||||||
| RAVLT immediate recall | 32.15 (7.66) | 33.91 (7.82) | ||||||||||
| RAVLT delayed recall | 6.09 (2.91) | 6.32 (2.91) | ||||||||||
| 15 | 71.95 (7.13) | 7.83 (2.63) | 7 | Passive Control Training | - | - | - | MMSE | 27.83 (1.86) | 28.04 (1.85) | ||
| Matrix reasoning test | 27.07 (6.64) | 27.83 (5.53) | ||||||||||
| Digit span forward | 5.14 (0.66) | 5.63 (0.55) | ||||||||||
| Word span | 4.19 (0.41) | 4.13 (0.48) | ||||||||||
| Corsi span | 4.36 (0.93) | 4.63 (0.98) | ||||||||||
| Prose memory | 9.92 (3.11) | 9.97 (3.09) | ||||||||||
| Rey figure copy | 31.88 (4.06) | 29.40 (3.79) | ||||||||||
| Rey figure delayed recall | 15.49 (6.48) | 14.65 (5.60) | ||||||||||
| RAVLT immediate recall | 33.32 (8.17) | 33.69 (9.38) | ||||||||||
| RAVLT delayed recall | 6.85 (2.95) | 7.27 (3.26) | ||||||||||
| Combourieu- Donnezan et al. [34] (MCI) | 21 | 75.2 (1.3) | 5.9 (0.31) | N.R. | Physical and Cognitive Training | 12 | 60 | 2 | Matrix reasoning test | 12.38 (6.48) | 16.42 (7.33) | 9 |
| Stroop | 26.52 (6.8) | 29.05 (7.19) | ||||||||||
| Digit span forward | 5.48 (0.88) | 6.15 (1.06) | ||||||||||
| Digit span backward | 4.10 (1.18) | 4.95 (1.12) | ||||||||||
| 16 | 76.3 (1.5) | 5.5 (0.36) | N.R. | Cognitive Training | 12 | 60 | 2 | Matrix reasoning test | 11.35 (6.84) | 15.18 (6.84) | ||
| Stroop | 27.19 (8.82) | 25.5(8.37) | ||||||||||
| Digit span forward | 5.18 (0.91) | 6.18 (1.11) | ||||||||||
| Digit span backward | 4.06 (0.68) | 4.63 (1.09) | ||||||||||
| 14 | 79.2 (4) | 5.8 (0.4) | N.R. | Passive Control Training | - | - | - | Matrix reasoning test | 9.85 (6.21) | 9.5 (4.95) | ||
| Stroop | 24.71 (10.16) | 26.42 (6.53) | ||||||||||
| Digit span forward | 5.21 (1.12) | 5.36 (0.84) | ||||||||||
| Digit span backward | 3.86 (0.86) | 3.79 (0.97) | ||||||||||
| Diaz Baquero et al. [35] (MCI) | 36 | 73.64 (6.56) | 9.35 (2.60) | 13 | Computer- based Cognitive Training | 16 | 30 | 2/3 | MMSE | 24.28 (2.54) | 24.97 (2.91) | 9 |
| ADAS-Cog | 14.00 (4.99) | 14.43 (6.48) | ||||||||||
| TMT—A time | 11.21 (11.32) | 13.43 (16.21) | ||||||||||
| TMT—A mistakes | 0.42 (0.77) | 0.25 (0.44) | ||||||||||
| TMT—B time | 15.91 (18.68) | 15.33 (11.26) | ||||||||||
| TMT—B mistakes | 2.14 (1.46) | 2.23 (1.52) | ||||||||||
| WAIS-III digits | 10.47 (2.61) | 10.58 (2.95) | ||||||||||
| WAIS-III digit symbol | 9.83 (2.87) | 10.11 (2.41) | ||||||||||
| WAIS-III arithmetic | 9.75 (3.08) | 10.22 (2.82) | ||||||||||
| CAMCOG visual reasoning | 2.22 (1.42) | 2.43 (1.20) | ||||||||||
| RBMT visual memory | 7.94 (2.10) | 7.78 (2.38) | ||||||||||
| CDT order | 7.35 (2.24) | 7.60 (2.38) | ||||||||||
| CDT copy | 9.10 (1.14) | 8.99 (1.50) | ||||||||||
| Semantic verbal fluency | 7.03 (2.88) | 7.62 (3.59) | ||||||||||
| Phonological verbal fluency—P | 7.56 (3.04) | 7.82 (2.76) | ||||||||||
| Phonological verbal fluency—M | 7.68 (3.44) | 8.26 (3.42) | ||||||||||
| Phonological verbal fluency—R | 8.50 (2.57) | 8.97 (2.58) | ||||||||||
| 26 | 76.23 (6.56) | 9.36 (2.86) | 4 | Passive Control Training | - | - | - | MMSE | 24.15 (4.16) | 24.81 (4.06) | ||
| ADAS-Cog | 14.88 (7.75) | 14.31 (7.29) | ||||||||||
| TMT—A time | 7.80 (5.61) | 9.09 (6.66) | ||||||||||
| TMT—A mistakes | 0.54 (1.07) | 0.64 (1.19) | ||||||||||
| TMT—B time | 14.44 (11.02) | 15.00 (9.13) | ||||||||||
| TMT—B mistakes | 1.59 (1.42) | 1.40 (1.31) | ||||||||||
| WAIS-III digits | 10.65 (2.17) | 11.48 (2.20) | ||||||||||
| WAIS-III digit symbol | 10.17 (2.06) | 10.35 (2.21) | ||||||||||
| WAIS-III arithmetic | 10.50 (2.34) | 10.68 (2.67) | ||||||||||
| CAMCOG visual reasoning | 2.00 (1.10) | 1.96 (1.06) | ||||||||||
| RBMT visual memory | 7.00 (3.02) | 6.84 (3.01) | ||||||||||
| CDT order | 7.25 (2.74) | 7.56 (2.07) | ||||||||||
| CDT copy | 8.81 (1.86) | 8.76 (1.93) | ||||||||||
| Semantic verbal fluency | 7.80 (3.28) | 7.56 (3.37) | ||||||||||
| Phonological verbal fluency—P | 7.72 (3.55) | 8.16 (3.22) | ||||||||||
| Phonological verbal fluency—M | 7.48 (3.66) | 8.28 (3.69) | ||||||||||
| Phonological verbal fluency—R | 8.84 (2.53) | 9.40 (2.90) | ||||||||||
| Djabelkhir et al. [36] (MCI) | 9 | 78.2 (7) | N.R. | 4 | Computer- based Cognitive Training | 12 | 90 | 1 | MMSE | 27 (2) | 28 (1.4) | 9 |
| 16-FCRT | 22.8 (10.7) | 25.1 (10) | ||||||||||
| TMT—A | 52.1 (18.8) | 47 (22.8) | ||||||||||
| TMT—B | 135.7 (65.6) | 111.5 (65.6) | ||||||||||
| Digit span backward | 4 (0.61) | 4 (0.61) | ||||||||||
| Phonological verbal fluency | 19.6 (9.7) | 22.4 (8) | ||||||||||
| Semantic verbal fluency | 24.2 (3.8) | 25.8 (6) | ||||||||||
| 10 | 75.2 (6.4) | N.R. | 3 | Active Control Training | 12 | 90 | 1 | MMSE | 27.7 (1.9) | 27.8 (1.5) | ||
| 16-FCRT | 26.6 (8.7) | 26.3 (7.5) | ||||||||||
| TMT—A | 50.8 (18.3) | 41.1 (12.3) | ||||||||||
| TMT—B | 112 (19.8) | 101.5 (29.2) | ||||||||||
| Digit span backward | 4 (0.61) | 3.75 (0.82) | ||||||||||
| Phonological verbal fluency | 22.1 (6.4) | 22.5 (5.9) | ||||||||||
| Semantic verbal fluency | 27 (8) | 27.4 (7.4) | ||||||||||
| Duff et al. [37] (a-MCI) | 55 | 74.9 (6.3) | 16.5 (2.8) | 29 | Computer- based Cognitive Training | 12/13 | 45 | 4/5 | RBANS | 85.1 (13.5) | 85.6 (14.6) | 10 |
| 58 | 74.9 (5.8) | 16 (2.9) | 33 | Active Control Training | 12/13 | 45 | 4/5 | RBANS | 85.7 (14.2) | 89.1 (13.5) | ||
| Fiatarone Singh et al. [38] (MCI) | 22 | N.R. | N.R. | N.R. | Computer- based Cognitive Training | 26 | 75 | 2/3 | ADAS-cog | 8.79 (0.98) | 7.31 (0.73) | 9 |
| WAIS III similarities | 19.11 (1.05) | 21.52 (1.08) | ||||||||||
| Matrix reasoning test | 11.98 (1.07) | 11.82 (1.08) | ||||||||||
| Semantic verbal fluency | 20.2 (1.11) | 20.5 (1.12) | ||||||||||
| COWAT | 38.24 (2.83) | 41.85 (2.85) | ||||||||||
| List learning memory | 18.59 (0.89) | 19.72 (0.90) | ||||||||||
| BVRT | 5.98 (0.43) | 5.88 (0.44) | ||||||||||
| Logical memory I | 10.13 (0.97) | 10.61 (0.96) | ||||||||||
| Logical memory delayed recall | 8.17 (1.11) | 9.08 (1.09) | ||||||||||
| SDMT | 45.58 (2.40) | 46.8 (2.42) | ||||||||||
| 27 | N.R. | N.R. | N.R. | Physical and Computer- based Cognitive Training | 26 | 75 | 2/3 | ADAS-cog | 8.02 (0.69) | 6.26 (0.69) | ||
| WAIS III similarities | 19.05 (1.01) | 20.57 (1.01) | ||||||||||
| Matrix reasoning test | 12.04 (1.06) | 13.26 (1.01) | ||||||||||
| Semantic Verbal Fluency | 17.9 (0.55) | 18.2 (1.03) | ||||||||||
| COWAT | 36.40 (2.66) | 37.88 (2.66) | ||||||||||
| List learning memory | 20.13 (0.84) | 20.79 (0.84) | ||||||||||
| BVRT | 5.86 (0.41) | 6.27 (0.41) | ||||||||||
| Logical memory I | 9.46 (0.90) | 10.42 (0.90) | ||||||||||
| Logical memory delayed recall | 8.71 (1.03) | 8.04 (1.01) | ||||||||||
| SDMT | 44.94 (2.25) | 47.92 (2.25) | ||||||||||
| 24 | N.R. | N.R. | N.R. | Active Control Training | 26 | 60 | 2/3 | ADAS-cog | 8.09 (0.10) | 7.14 (0.70) | ||
| WAIS III similarities | 17.84 (1.01) | 19.02 (1.03) | ||||||||||
| Matrix reasoning test | 11.53 (1.01) | 11.27 (1.03) | ||||||||||
| Semantic verbal fluency | 18.4 (1.03) | 17.7 (1.05) | ||||||||||
| COWAT | 35.23 (2.65) | 41.09 (2.69) | ||||||||||
| List learning memory | 18.84 (0.83) | 19.09 (0.85) | ||||||||||
| BVRT | 6.51 (0.41) | 5.46 (0.42) | ||||||||||
| Logical memory I | 9.60 (0.92) | 10.99 (0.90) | ||||||||||
| Logical memory delayed recall | 8.17 (1.01) | 7.75 (1.03) | ||||||||||
| SDMT | 41.68 (2.25) | 44.11 (2.29) | ||||||||||
| Finn and McDonald [39] (a-MCI) | 12 | 72.83 (5.7) | 13.75 (2.8) | 8 | Computer-based Cognitive Training | 4 | N.R. | 2 | VPA immediate recall | 5.41 (3.7) | 7.75 (4.2) | 8 |
| VPA delayed recall | 1.50 (1.3) | 2.42 (1.7) | ||||||||||
| TMT—A | 49.67 (22.6) | 42.67 (15.8) | ||||||||||
| TMT—B | 128.92 (47.5) | 120.42 (48.2) | ||||||||||
| Symbol span | 14.42 (4.4) | 16.83 (3.3) | ||||||||||
| 12 | 75.08 (7.5) | 13.67 (3.8) | 9 | Passive Control Training | - | - | - | VPA immediate recall | 6.50 (5.8) | 8.67 (7.2) | ||
| VPA delayed recall | 2.25 (1.9) | 2.08 (1.9) | ||||||||||
| TMT—A | 45.42 (12.8) | 46.92 (22.7) | ||||||||||
| TMT—B | 141.33 (54.4) | 115.42 (49.8) | ||||||||||
| Symbol span | 14.17 (6) | 14.75 (6.2) | ||||||||||
| Giuli et al. [40] (MCI) | 48 | 76 (6.3) | 6.7 (3.8) | 17 | Cognitive Training | 10 | 90 | 1 | Digit span forward | 4.52 (0.8) | 4.68 (0.9) | 7 |
| Digit span backward | 2.76 (0.9) | 3.04 (0.9) | ||||||||||
| MMSE | 25.85 (1.9) | 25.62 (2.5) | ||||||||||
| Prose memory | 7.05 (3.8) | 8.78 (3.9) | ||||||||||
| Word-pairing learning test | 8.45 (3.6) | 9.6 (4.7) | ||||||||||
| Corsi supraspan | 4.84 (0.8) | 5.11 (0.8) | ||||||||||
| Semantic verbal fluency | 1.87 (1.3) | 2 (1.5) | ||||||||||
| Phonological verbal fluency | 29.23 (8.2) | 30.85 (8.6) | ||||||||||
| Attentive matrices | 38.61 (10.1) | 42.15 (9.9) | ||||||||||
| 49 | 76.5 (5.7) | 5.3 (3) | 19 | Passive Control Training | - | - | - | Digit span forward | 4.69 (0.8) | 4.5 (0.8) | ||
| Digit span backward | 2.75 (0.8) | 2.40 (0.7) | ||||||||||
| MMSE | 25.85 (2.3) | 25.43 (3.2) | ||||||||||
| Prose memory | 7.2 (4.5) | 6.56 (4.1) | ||||||||||
| Word-pairing learning test | 6.69 (3.2) | 6.41 (2.9) | ||||||||||
| Corsi supraspan | 5.04 (0.7) | 4.8 (0.9) | ||||||||||
| Semantic verbal fluency | 2.19 (1.3) | 2.19 (1.3) | ||||||||||
| Phonological verbal fluency | 24.39 (7.9) | 23.85 (5.9) | ||||||||||
| Attentive matrices | 40.75 (9.6) | 39.16 (10) | ||||||||||
| Greenaway et al. [41] (a-MCI) | 20 | 72.7 (6.9) | 16.4 (2.8) | 8 | Cognitive Training | 12 | 60 | 2 | DRS-2 | 131.1 (6.3) | 131.6 (6.8) | 8 |
| MMSE | 26.4 (2.2) | 26 (2.9) | ||||||||||
| 20 | 72.3 (7.9) | 16.4 (2.8) | 7 | Passive Control Training | - | - | - | DRS-2 | 133.8 (4.2) | 134.8 (5.1) | ||
| MMSE | 27.2 (2.4) | 27.3 (2.2) | ||||||||||
| Hagovská and Olekszyová [42] (MCI) | 40 | 68 (4.4) | N.R. | 22 | Physical and Computer- based Cognitive Training | 10 | 30 | 2 | MMSE | 25.97 (2.57) | 26.97 (2.21) | 8 |
| 38 | 65.9 (6.2) | N.R. | 19 | Passive Control Training | - | - | - | MMSE | 26.02 (1.47) | 26.10 (1.46) | ||
| Herrera et al. [43] (a-MCI) | 11 | 75.09 (1.97) | N.R. | 6 | Computer- based Cognitive Training | 12 | 60 | 2 | Digit span forward | 4.45 (0.31) | 4.91 (0.21) | 7 |
| Digit span-backward | 3.36 (0.24) | 4.00 (0.19) | ||||||||||
| BEM recall test | 6.23 (0.35) | 7.28 (0.26) | ||||||||||
| 16-FCRT | 40.55 (0.41) | 42.91 (0.76) | ||||||||||
| Rey figure copy | 10.09 (1.52) | 10.45 (1.36) | ||||||||||
| 11 | 78.18 (1.44) | N.R. | 5 | Active Control Training | 12 | 60 | 2 | Digit span forward | 4.36 (0.24) | 4.18 (0.12) | ||
| Digit span-backward | 3.82 (0.18) | 3.64 (0.20) | ||||||||||
| BEM recall test | 6.40 (0.46) | 6.05 (0.25) | ||||||||||
| 16-FCRT | 41.09 (0.44) | 39.91 (0.44) | ||||||||||
| Rey figure copy | 11.86 (1.27) | 10.23 (0.87) | ||||||||||
| Hughes et al. [44] (MCI) | 10 | 78.5 (7.1) | 13.8 (2.4) | 2 | Computer- based Cognitive Training | 24 | 90 | 1 | CAMCI | 25.55 (6.24) | 29.41 (5.48) | 6 |
| 10 | 76.2 (4.3) | 13.1 (1.9) | 4 | Active Control Training | 24 | 30 | 1 | CAMCI | 25.49 (6.34) | 25.59 (6.86) | ||
| Hyer et al. [45] (MCI) | 34 | 75.1 (7.4) | N.R. | 17 | Computer- based Cognitive Training | 5–7 | 40 | 5 | TMT—B | 132.38 (47.92) | 118.92 (43.49) | 9 |
| Span board | 8.79 (2.48) | 11.54 (3.37) | ||||||||||
| 34 | 75.2 (7.8) | N.R. | 15 | Passive Control Training | - | - | - | TMT—B | 133.97 (41.56) | 112.57 (39.74) | ||
| Span board | 9.73 (3.10) | 10.77 (3.07) | ||||||||||
| Lam et al. [46] (MCI) | 145 | 74.4 (6.4) | 5.2 (4.3) | 30 | Cognitive Training | 16 | 60 | 3 | MMSE | 25.7 (2.4) | 25.8 (2.6) | 10 |
| ADAS-Cog | 11.3 (3.2) | 8.8 (3.5) | ||||||||||
| Word list delayed recall | 3.5 (2.2) | 5.8 (2.1) | ||||||||||
| Semantic verbal fluency | 34.2 (7.3) | 36.2 (8.2) | ||||||||||
| 132 | 76.3 (6.6) | 5.7 (4.9) | 28 | Cognitive and Physical Training | 16 | 60 | 3 | MMSE | 25.2 (2.3) | 25.7 (2.5) | ||
| ADAS-Cog | 11.6 (3.4) | 8.9 (3.2) | ||||||||||
| Word list delayed recall | 3.2 (2.2) | 5.3 (2.1) | ||||||||||
| Semantic verbal fluency | 32.8 (6.7) | 35.8 (7.2) | ||||||||||
| 147 | 75.5 (6.7) | 5.7 (4.3) | 34 | Active Control Training (Physical) | 16 | 60 | 3 | MMSE | 25.8 (2.3) | 26.2 (2.2) | ||
| ADAS-Cog | 11.7 (3.3) | 8.8 (3.6) | ||||||||||
| Word list delayed recall | 2.5 (3.3) | 5.7 (2.3) | ||||||||||
| Semantic verbal fluency | 33.3 (7.3) | 35.7 (8) | ||||||||||
| 131 | 75.4 (6.1) | 5.7 (4.9) | 29 | Active Control Training (Social) | 16 | 60 | 3 | MMSE | 25.6 (2.4) | 25.8 (2.4) | ||
| ADAS-Cog | 11.5 (3.4) | 9.2 (3.3) | ||||||||||
| Word list delayed recall | 3.4 (2.1) | 5.4 (2.1) | ||||||||||
| Semantic verbal fluency | 32.7 (7.4) | 34.4 (7.9) | ||||||||||
| Law et al. [47] (MCI) | 40 | 74.1 (7.6) | N.R. | 17 | Computer- based Cognitive Training | 10 | 60 | N.R. | CVLT immediate recall | 16.35 (0.94) | 17.90 (0.61) | 7 |
| CVLT delayed recall | 5.26 (0.71) | 6.29 (0.29) | ||||||||||
| Semantic verbal fluency | 10.43 (0.65) | 11.19 (0.46) | ||||||||||
| TMT—A | 134.31 (13.76) | 123.38 (6.13) | ||||||||||
| TMT—B | 228.27 (13.83) | 213.38 (8.29) | ||||||||||
| 43 | 73.68 (6.8) | N.R. | 16 | Active Control Training | 10 | 45/50 | N.R. | CVLT immediate recall | 15.49 (0.74) | 19.84 (0.59) | ||
| CVLT delayed recall | 5.00 (0.51) | 7.24 (0.28) | ||||||||||
| Semantic verbal fluency | 9.33 (0.56) | 12.62 (0.45) | ||||||||||
| TMT—A | 136.28 (10.55) | 111.51 (5.91) | ||||||||||
| TMT—B | 236.97 (13.08) | 189.90 (7.99) | ||||||||||
| Lin et al. [48] (a-MCI) | 10 | 72.90 (8.23) | N.R. | 5 | Vision based speed of processing training | 6 | 60 | 4 | UFOV | 136.35 (87.42) | 63.96 (22.22) | 6 |
| 11 | 73.09 (9.60) | N.R. | 6 | Active Control Training | 6 | 60 | 4 | UFOV | 96.63 (48.67) | 87.65 (59.53) | ||
| Mavros et al. [49] (MCI) | 24 | N.R. | N.R. | N.R. | Cognitive Training | 26 | N.R. | 2/3 | ADAS-Cog | 8.4 (3.2) | 6.7 (3.2) | 9 |
| WAIS III Similarities | 8.4 (3.2) | 6.7 (3.2) | ||||||||||
| Matrix reasoning test | 12.0 (4.6) | 12.5 (4.6) | ||||||||||
| Semantic verbal fluency | 19.2 (4.4) | 19.6 (4.5) | ||||||||||
| COWAT | 38.2 (11.3) | 40.8 (11.4) | ||||||||||
| BVRT | 5.9 (1.7) | 6.3 (1.7) | ||||||||||
| Logical memory I | 10.8 (3.8) | 10.1 (3.8) | ||||||||||
| Logical memory delayed recall | 8.7 (4.2) | 8.8 (4.2) | ||||||||||
| SDMT | 45.3 (9.4) | 47.2 (9.5) | ||||||||||
| 27 | N.R. | N.R. | N.R. | Active Control Training | 26 | N.R. | 2/3 | ADAS-Cog | 8.2 (3.2) | 6.3 (3.3) | ||
| WAIS III Similarities | 8.2 (3.2) | 6.3 (3.3) | ||||||||||
| Matrix reasoning test | 12.4 (4.6) | 13.1 (4.9) | ||||||||||
| Semantic verbal fluency | 18.5 (4.5) | 19.3 (4.7) | ||||||||||
| COWAT | 38.0 (11.3) | 43.1 (11.8) | ||||||||||
| BVRT | 6.0 (1.7) | 5.8 (1.8) | ||||||||||
| Logical memory I | 11.7 (3.8) | 10.1 (4.1) | ||||||||||
| Logical memory delayed recall | 11.7 (4.1) | 10.1 (4.4) | ||||||||||
| SDMT | 43.1 (9.4) | 45.3 (9.7) | ||||||||||
| Nousia et al. [50] (MCI) | 25 | 71.20 (5.07) | 8.92 (3.37) | 6 | Computer- based Cognitive Training | 15 | 60 | 2 | WMT immediate recall | 19.36 (3.38) | 21.00 (2.72) | 10 |
| WMT delayed recall | 1.80 (0.76) | 3.04 (1.21) | ||||||||||
| Boston naming test | 13.56 (1.45) | 14.60 (0.65) | ||||||||||
| Semantic verbal fluency | 30.44 (7.76) | 40.60 (7.17) | ||||||||||
| CDT | 13.68 (1.25) | 14.44 (0.82) | ||||||||||
| Digit span forward | 6.60 (1.32) | 6.72 (1.34) | ||||||||||
| Digit span backward | 4.48 (1.23) | 4.64 (1.08) | ||||||||||
| TMT—A | 98.44 (27.31) | 80.72 (23.45) | ||||||||||
| TMT—B | 222.48 (53.79) | 174.16 (37.11) | ||||||||||
| 21 | 71.90 (6.24) | 8.42 (3.06) | 5 | Passive Control Training | - | - | - | WMT immediate recall | 19.90 (3.78) | 20.57 (2.93) | ||
| WMT delayed recall | 1.43 (1.29) | 0.67 (0.58) | ||||||||||
| Boston naming test | 13.10 (1.64) | 12.90 (2.63) | ||||||||||
| Semantic verbal fluency | 38.05 (7.49) | 34.90 (5.54) | ||||||||||
| CDT | 14.00 (1.34) | 13.90 (1.18) | ||||||||||
| Digit span forward | 6.33 (1.59) | 6.10 (1.58) | ||||||||||
| Digit span backward | 4.52 (1.29) | 4 (1.30) | ||||||||||
| TMT—A | 110.14 (37.02) | 113.67 (37.36) | ||||||||||
| TMT—B | 238.38 (52.25) | 237.86 (43.73) | ||||||||||
| Olchik et al. [51] (a-MCI) | 16 | 70.3 (4.3) | 14.3 (4.9) | 4 | Cognitive Training | 4 | 90 | 2 | Semantic verbal fluency | 15.2 (4.6) | 17.0 (4.1) | 7 |
| Phonological verbal fluency | 30.5 (9.8) | 35.3 (9.1) | ||||||||||
| RAVLT immediate recall | 34.5 (10.3) | 40.3 (8.8) | ||||||||||
| RAVLT delayed recall | 5.4 (4.0) | 7.3 (3.3) | ||||||||||
| RBMT story immediate recall | 5.9 (2.0) | 8.8 (2.4) | ||||||||||
| RBMT story delayed recall | 4.6 (2.6) | 8.6 (2.9) | ||||||||||
| 14 | 70.2 (5.7) | 11.2 (4.2) | 2 | Passive Control Training | - | - | - | Semantic verbal fluency | 15.4 (3.2) | 14.0 (4.4) | ||
| Phonological verbal fluency | 28.9 (10.5) | 32.6 (10.4) | ||||||||||
| RAVLT immediate recall | 34.5 (8.3) | 36.2 (8.8) | ||||||||||
| RAVLT delayed recall | 4.2 (2.2) | 6.0 (2.6) | ||||||||||
| RBMT story immediate recall | 5.0 (2.6) | 9.0 (3.2) | ||||||||||
| RBMT story delayed recall | 4.7 (3.1) | 7.3 (3.1) | ||||||||||
| Poptsi et al. [52] (a-MCI) | 150 | 68.12 (6.31) | 11.31 (4.19) | 31 | Physical and Computer- based Cognitive Training | N.R. | N.R. | N.R. | MMSE | 27.70 (1.82) | 27.90 (2.65) | 10 |
| RAVLT immediate recall | 10.55 (2.59) | 11.78 (2.47) | ||||||||||
| RAVLT delayed recall | 7.68 (3.23) | 9.65 (3.29) | ||||||||||
| RBMT history recall | 11.42 (3.90) | 11.13 (3.62) | ||||||||||
| Rey figure copy | 12.94 (6.34) | 15.60 (7.06) | ||||||||||
| RBMT working memory | 12.39 (3.53) | 11.85 (3.49) | ||||||||||
| Phonological verbal fluency | 9.77 (3.47) | 12.00 (3.34) | ||||||||||
| TEA | 47.00 (11.72) | 47.29 (11.72) | ||||||||||
| 133 | 67.11 (9.10) | 10.69 (4.68) | 22 | Passive Control Training | N.R. | N.R. | N.R. | MMSE | 27.28 (2.24) | 26.79 (3.47) | ||
| RAVLT immediate recall | 10.73 (4.15) | 10.75 (3.97) | ||||||||||
| RAVLT delayed recall | 7.90 (3.25) | 7.80 (3.77) | ||||||||||
| RBMT history recall | 11.06 (3.67) | 9.82 (4.33) | ||||||||||
| Rey figure copy | 11.71 (6.42) | 12.98 (6.25) | ||||||||||
| RBMT working memory | 12.11 (3.39) | 10.72 (3.90) | ||||||||||
| Phonological verbal fluency | 10.26 (4.15) | 10.05 (3.69) | ||||||||||
| TEA | 47.82 (12.63) | 43.83 (14.82) | ||||||||||
| Rapp et al. [53] (MCI) | 9 | 73.33 (6.61) | N.R. | 1 | Cognitive Training | 6 | 120 | 1 | Word list immediate recall | 8.11 (3.02) | 11.56 (2.83) | 8 |
| Word list delayed recall | 3.56 (2.92) | 8.44 (4.22) | ||||||||||
| 10 | 75.10 (7.03) | N.R. | 7 | Passive Control Training | - | - | - | Word list immediate recall | 5.10 (0.99) | 7.80 (3.22) | ||
| Word list delayed recall | 1.90 (1.45) | 4.70 (3.62) | ||||||||||
| Rojas et al. [54] (MCI) | 15 | 72 (14.29) | 10.53 (3.78) | 9 | Cognitive Training | 24 | 120 | 1 | MMSE | 27.53 (2.33) | 27.53 (2.00) | 9 |
| Memory free recall | 11.07 (1.33) | 10.64 (1.74) | ||||||||||
| Boston naming test | 44.20 (7.25) | 47.07 (9.20) | ||||||||||
| Semantic verbal fluency | 13.47 (3.09) | 16.50 (3.67) | ||||||||||
| Phonological verbal fluency | 10.47 (4.64) | 11.93 (4.46) | ||||||||||
| 15 | 77.93 (7.5) | 10.53 (3.85) | 8 | Passive Control Training | - | - | - | MMSE | 27.13 (2.10) | 25.36 (2.53) | ||
| Memory free recall | 9.64 (2.22) | 8.64 (2.34) | ||||||||||
| Boston naming test | 42.93 (6.78) | 43.14 (8.10) | ||||||||||
| Semantic verbal fluency | 13.47 (3.66) | 11.07 (3.40) | ||||||||||
| Phonological verbal fluency | 10.50 (3.91) | 9.07 (3.91) | ||||||||||
| Schmitter-Edgecombe and Dyck [55] (MCI) | 23 | 72.96 (7.05) | 14.48 (2.81) | 7 | Cognitive Training | 10 | 120 | 2 | RBMT-II | 15.35 (5.31) | 17.35 (6.11) | 8 |
| RBANS immediate memory | 84.91 (17.37) | 92.78 (19.85) | ||||||||||
| RBANS delayed memory | 79.39 (19.59) | 86.10 (24.50) | ||||||||||
| 23 | 73.35 (7.89) | 15.78 (3.32) | 12 | Passive Control Training | - | - | - | RBMT-II | 15.22 (6.99) | 15.13 (6.85) | ||
| RBANS immediate memory | 87.56 (18.64) | 88.52 (23.15) | ||||||||||
| RBANS delayed memory | 77.57 (23.53) | 78.52 (26.25) | ||||||||||
| Savulich et al. [56] (a-MCI) | 21 | 75.2 (7.4) | 15.9 (1.3) | 11 | Computer- based Cognitive Training | 4 | 60 | 2 | MMSE | 26.6 (2.9) | 27.4 (1.5) | 9 |
| 21 | 76.9 (8.3) | 16 (2.1) | 14 | Passive Control Training | - | - | - | MMSE | 26.8 (2.2) | 26.1 (2.4) | ||
| Sukontapol et al. [57] (MCI) | 30 | N.R. | N.R. | 7 | Cognitive Training | N.R. | 180 | N.R. | MoCA | 21.37 (2.04) | 25.40 (1.58) | 8 |
| 30 | N.R. | N.R. | 14 | Passive Control Training | - | - | - | MoCA | 18.43 (4.06) | 18.77 (4.35) | ||
| Tsolaki et al. [58] (MCI) | 122 | 68.45 (6.99) | 9.31 (4.11) | 32 | Cognitive Training | N.R. | 90 | 3 | MMSE | 28.09 (1.59) | 29.00 (6.18) | 9 |
| MoCA | 22.98 (3.36) | 24.71 (3.05) | ||||||||||
| FUCAS planning | 6.20 (0.60) | 6.04 (0.25) | ||||||||||
| Rey figure copy | 29.85 (5.89) | 31.53 (5.30) | ||||||||||
| 79 | 66.86 (8.79) | 8.97 (4.19) | 18 | Passive Control Training | - | - | - | MMSE | 27.59 (1.88) | 27.06 (2.34) | ||
| MoCA | 22.20 (3.54) | 22.45 (4.78) | ||||||||||
| FUCAS planning | 6.18 (0.56) | 6.18 (0.56) | ||||||||||
| Rey figure copy | 28.48 (8.24) | 29.18 (7.19) | ||||||||||
| Weng et al. [59] (MCI) | 33 | 81.82 (11.28) | N.R. | 4 | Computer- based Cognitive Training | 8 | 40–60 | 2 | MoCA | 17.45 (4.65) | 18.09 (4.71) | 9 |
| Digit span forward | 4.42 (1.25) | 4.55 (1.23) | ||||||||||
| Digit span backward | 2.45 (0.94) | 2.73 (0.91) | ||||||||||
| WAIS-IV digit symbol | 19.03 (8.12) | 21.48 (6.70) | ||||||||||
| Phonological verbal fluency | 8.94 (3.03) | 9.06 (2.68) | ||||||||||
| WAIS-IV similarities | 10.61 (4.96) | 11.06 (4.44) | ||||||||||
| 29 | 80.72 (9.91) | N.R. | 1 | Active Control Training | 8 | 40–60 | 2 | MoCA | 18.41 (3.40) | 17.86 (3.32) | ||
| Digit span forward | 4.03 (1.12) | 3.76 (1.12) | ||||||||||
| Digit span backward | 2.69 (0.97) | 2.52 (0.91) | ||||||||||
| WAIS-IV digit symbol | 21.45 (7.78) | 20.10 (8.03) | ||||||||||
| Phonological verbal fluency | 9.59 (2.71) | 9.66 (2.76) | ||||||||||
| WAIS-IV similarities | 11.17 (3.96) | 11.55 (4.37) | ||||||||||
| Domain/Outcomes | K | N | EG | CG | Pooled Effect Size Hedges’ g (p Value) | (95% Confidence Intervals) | Homogeneity Statistics | Egger’s t Test for Publication Bias (p Value) | Trim and Fill (Estimated Effect Size) | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| LL | UL | Q (df) | P | I2 | ||||||||
| Global Cognitive Function (Mini Mental State Examination; 66.6%) | 12 | 1543 | 799 | 744 | 0.21 (0.001) | 0.08 | 0.33 | 13.88 (11) | 0.240 | 20.73 | 1.61 (0.139) | 2 [0.18 (0.005)] |
| Memory | ||||||||||||
| 8 | 398 | 216 | 182 | 0.79 (0.029) | 0.08 | 1.50 | 73.09 (7) | <0.001 | 90.42 | 0.87 (0.417) | 0 |
| 4 | 449 | 227 | 222 | 0.31 (0.044) | 0.01 | 0.62 | 5.65 (3) | 0.130 | 46.86 | −4.72 (0.042) | 0 |
| Sensitivity Analysis after removing Ciarmiello et al., 2015 [33] | 3 | 419 | 212 | 207 | 0.39 (0.014) | 0.08 | 0.69 | 3.69 (2) | 0.158 | 45.80 | −2.64 (0.231) | 0 |
| Executive Functions | ||||||||||||
| 6 | 302 | 156 | 146 | −0.60 (0.339) | −1.83 | 0.63 | 115.42 (5) | <0.001 | 95.67 | −0.69 (0.529) | 2 [−1.18 (0.056)] |
| 4 | 205 | 125 | 80 | 0.41 (0.069) | −0.03 | 0.84 | 6.71 (3) | 0.082 | 55.32 | −0.52 (0.652) | 0 |
| 8 | 653 | 344 | 309 | 0.77 (0.037) | 0.05 | 1.49 | 111.67 (7) | <0.001 | 93.73 | 0.50 (0.635) | 0 |
| 7 | 317 | 173 | 144 | 0.78 (0.003) | 0.27 | 1.29 | 25.07 (6) | <0.001 | 76.06 | 1.09 (0.325) | 0 |
| Processing Speed/Attention (Trail Making Test—Part A; 50%) | 5 | 234 | 122 | 112 | −0.31 (0.594) | −1.43 | 0.82 | 63.97 (4) | <0.001 | 93.75 | 0.43 (0.697) | 1 [−0.56 (0.284)] |
| Visuospatial and Constructional Ability (Rey Osterrieth Complex Figure-Copy Task; 66.6%) | 4 | 536 | 298 | 238 | 0.49 (0.022) | 0.07 | 0.91 | 11.39 (3) | 0.010 | 73.67 | 4.13 (0.054) | 1 [0.31 (0.215)] |
| Language (Semantic Verbal Fluency; 100%) | 11 | 1116 | 576 | 540 | −0.08 (0.828) | −0.75 | 0.60 | 216.78 (10) | <0.001 | 95.39 | −0.25 (0.810) | 4 [−0.85 (0.032)] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Raimo, S.; Cropano, M.; Gaita, M.; Maggi, G.; Cavallo, N.D.; Roldan-Tapia, M.D.; Santangelo, G. The Efficacy of Cognitive Training on Neuropsychological Outcomes in Mild Cognitive Impairment: A Meta-Analysis. Brain Sci. 2023, 13, 1510. https://doi.org/10.3390/brainsci13111510
Raimo S, Cropano M, Gaita M, Maggi G, Cavallo ND, Roldan-Tapia MD, Santangelo G. The Efficacy of Cognitive Training on Neuropsychological Outcomes in Mild Cognitive Impairment: A Meta-Analysis. Brain Sciences. 2023; 13(11):1510. https://doi.org/10.3390/brainsci13111510
Chicago/Turabian StyleRaimo, Simona, Maria Cropano, Mariachiara Gaita, Gianpaolo Maggi, Nicola Davide Cavallo, Maria Dolores Roldan-Tapia, and Gabriella Santangelo. 2023. "The Efficacy of Cognitive Training on Neuropsychological Outcomes in Mild Cognitive Impairment: A Meta-Analysis" Brain Sciences 13, no. 11: 1510. https://doi.org/10.3390/brainsci13111510