
Tinnitus, Suicide, and Suicidal Ideation: A Scoping Review of Primary Research
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion/Exclusion Criteria
2.2. Information Sources
2.3. Search
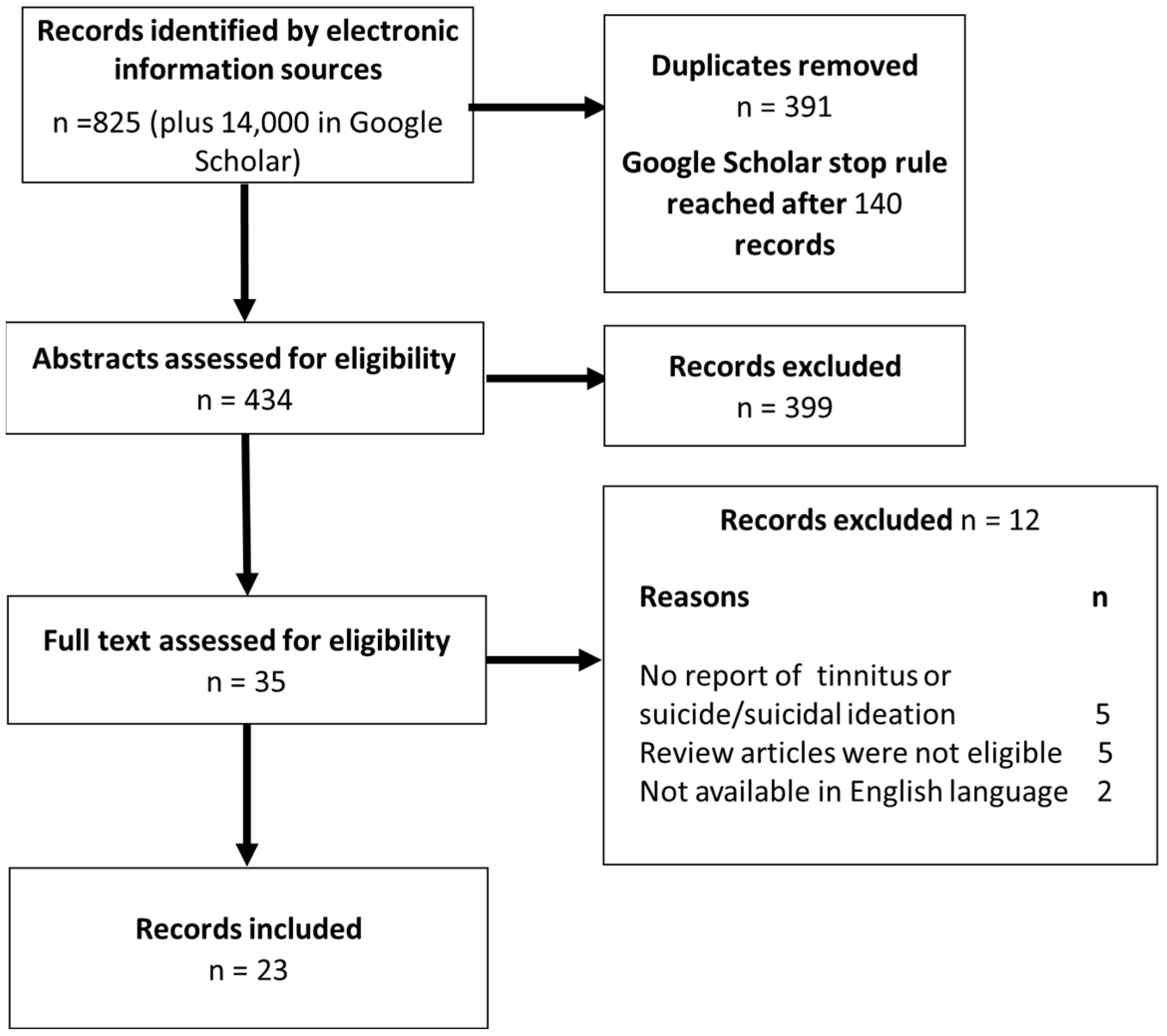
2.4. Selection of Sources of Evidence
2.5. Data Extraction and Charting
2.6. Expert Consultation
3. Results
3.1. Epidemiological Studies
3.1.1. Suicidal Ideation
3.1.2. Suicidal Ideation and Behaviour
3.1.3. Death by Suicide
3.2. Case Studies
3.2.1. Suicidal Ideation
3.2.2. Suicidal Behaviour
3.2.3. Death by Suicide
3.3. Observational Studies
3.3.1. Suicidal Ideation
3.3.2. Suicidal Behaviour
3.4. Research Recommendations in the Included Records
4. Discussion
4.1. Associations between Tinnitus and Suicide and Other Factors
4.2. Suicidal Ideation as a Predictor of Risk
4.3. Suicide Nomenclature in Tinnitus Studies
4.4. Issues with Diagnoses and Treatment in Research Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McCormack, A.; Edmondson-Jones, M.; Somerset, S.; Hall, D. A systematic review of the reporting of tinnitus prevalence and severity. Hear. Res. 2016, 337, 70–79. [Google Scholar] [CrossRef]
- Pinto, P.C.L.; Marcelos, C.M.; Mezzasalma, M.A.; Osterne, F.J.V.; De Lima, M.D.M.T.; Nardi, A.E. Tinnitus and its association with psychiatric disorders: Systematic review. J. Laryngol. Otol. 2014, 128, 660–664. [Google Scholar] [CrossRef] [PubMed]
- Cima, R.F.; Kikidis, D.; Mazurek, B.; Haider, H.; Cederroth, C.R.; Norena, A.; Lapira, A.; Bibas, A.; Hoare, D.J. Tinnitus healthcare: A survey revealing extensive variation in opinion and practices across Europe. BMJ Open 2020, 10, e029346. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, D.; Schlee, W.; Vanneste, S.; Londero, A.; Weisz, N.; Kleinjung, T.; Shekhawat, G.S.; Elgoyhen, A.B.; Song, J.J.; Andersson, G.; et al. Tinnitus and tinnitus disorder: Theoretical and operational definitions (an international multidisciplinary proposal). Prog. Brain Res. 2021, 260, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Cima, R.F.; van Breukelen, G.; Vlaeyen, J.W. Tinnitus-related fear: Mediating the effects of a cognitive behavioural specialised tinnitus treatment. Hear. Res. 2018, 358, 86–97. [Google Scholar] [CrossRef]
- Handscomb, L.; Shorter, G.W.; Hoare, D.J.; Hall, D.A. Evaluation of a cognitive behavioral model of tinnitus distress: A cross-sectional study using structural equation modeling. Ear Hear. 2020, 41, 1028–1039. [Google Scholar] [CrossRef]
- Probst, T.; Pryss, R.; Langguth, B.; Schlee, W. Emotional states as mediators between tinnitus loudness and tinnitus distress in daily life: Results from the “TrackYourTinnitus” application. Sci. Rep. 2016, 6, 20382. [Google Scholar] [CrossRef]
- Szibor, A.; Mäkitie, A.; Aarnisalo, A.A. Tinnitus and suicide: An unresolved relation. Audiol. Res. 2021, 9, 222. [Google Scholar] [CrossRef]
- Tailor, B.V.; Thompson, R.E.; Nunney, I.; Agius, M.; Phillips, J.S. Suicidal ideation in people with tinnitus: A systematic review and meta-analysis. Laryngol. Otol. 2021, 135, 1042–1050. [Google Scholar] [CrossRef]
- World Health Organization. Suicide: Key Facts Geneva: World Health Organization. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 21 February 2022).
- Turecki, G.; Brent, D.A.; Gunnell, D.; O’Connor, R.C.; Oquendo, M.A.; Pirkis, J.; Stanley, B.H. Suicide and suicide risk. Nat. Rev. Dis. Primers 2019, 5, 74. [Google Scholar] [CrossRef]
- Silverman, M.M. The language of suicidology. Suicide Life Threat. Behav. 2006, 36, 519–532. [Google Scholar] [CrossRef]
- Sveticic, J.; De Leo, D. The hypothesis of a continuum in suicidality: A discussion on its validity and practical implications. Mental Illn. 2012, 4, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Hawton, K.; van Heeringen, K. Suicide. Lancet 2009, 373, 1372–1381. [Google Scholar] [CrossRef] [PubMed]
- Bryan, B.; May, J.E.; Rugo, A.M.; Harris, K.F.; Oakey, J.A.; Rozek, D.N.; Rozek, D.C.; Bryan, A.O. Nonlinear change processes and the emergence of suicidal behavior: A conceptual model based on the fluid vulnerability theory of suicide. New Ideas Psychol. 2020, 57, 100758. [Google Scholar] [CrossRef]
- Coppersmith, D.D.; Ryan, O.; Fortgang, R.G.; Millner, A.J.; Kleiman, E.M.; Nock, M.K. Mapping the timescale of suicidal thinking. Proc. Natl. Acad. Sci. USA 2023, 120, e2215434120. [Google Scholar] [CrossRef]
- Liu, R.T.; Bettis, A.H.; Burke, T.A. Characterizing the phenomenology of passive suicidal ideation: A systematic review and meta-analysis of its prevalence, psychiatric comorbidity, correlates, and comparisons with active suicidal ideation. Psychol. Med. 2020, 50, 367–383. [Google Scholar] [CrossRef]
- Millner, A.J.; Robinaugh, D.J.; Nock, M.K. Advancing the Understanding of Suicide: The Need for formal theory and rigorous descriptive research. Trends Cogn. Sci. 2020, 24, 704–716. [Google Scholar] [CrossRef]
- Franklin, J.C.; Ribeiro, J.D.; Fox, K.R.; Bentley, K.H.; Kleiman, E.M.; Huang, X.; Musacchio, K.M.; Jaroszewski, A.C.; Chang, B.P.; Nock, M.K. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research. Psychol. Bull. 2017, 143, 187–232. [Google Scholar] [CrossRef]
- Jobes, D.A.; Joiner, T.E. Reflections on suicidal ideation. Crisis 2019, 40, 227–230. [Google Scholar] [CrossRef]
- Borges, G.; Angst, J.; Nock, M.K.; Ruscio, A.M.; Kessler, R.C. Risk factors for the incidence and persistence of suicide-related outcomes: A 10-year follow-up study using the National Comorbidity Surveys. J. Affect. Disord. 2008, 105, 25–33. [Google Scholar] [CrossRef]
- Nock, M.K.; Borges, G.; Bromet, E.J.; Cha, C.B.; Kessler, R.C.; Lee, S. Suicide and suicidal behavior. Epidemiol. Rev. 2008, 30, 133–154. [Google Scholar] [CrossRef] [PubMed]
- McManus, S.; Bebbington, P.; Jenkins, R.; Brugha, T. (Eds.) Mental Health and Wellbeing in England Adult Psychiatric Morbidity Survey; NHS Digital: Leeds, UK, 2016. [Google Scholar]
- Carrasco-Barrios, M.T.; Huertas, P.; Martín, P.; Martín, C.; Castillejos, M.C.; Petkari, E.; Moreno-Küstner, B. Determinants of suicidality in the European general population: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 4115. [Google Scholar] [CrossRef] [PubMed]
- Wastler, H.M.; Khazem, L.R.; Ammendola, E.; Baker, J.C.; Bauder, C.R.; Tabares, J.; Bryan, A.O.; Szeto, E.; Bryan, C.J. An empirical investigation of the distinction between passive and active ideation: Understanding the latent structure of suicidal thought content. Suicide Life Threat. Behav. 2023, 53, 219–226. [Google Scholar] [CrossRef]
- Wastler, H.M.; Bryan, A.O.; Bryan, C.J. Suicide attempts among adults denying active suicidal ideation: An examination of the relationship between suicidal thought content and suicidal behavior. J. Clin. Psychol. 2022, 78, 1103–1117. [Google Scholar] [CrossRef]
- Nock, M.K. Suicidal behavior among adolescents: Correlates, confounds, and (the search for) causal mechanisms. J. Am. Acad. Child. Adolesc. Psychiatry 2009, 48, 237–239. [Google Scholar] [CrossRef] [PubMed]
- Nock, M.; O’Connor, R. The psychology of suicidal behavior. Lancet Psychiatry 2014, 1, 73–85. [Google Scholar] [CrossRef]
- O’Connor, R.C.; Kirtley, O.J. The integrated motivational–volitional model of suicidal behaviour. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2018, 373, 20170268. [Google Scholar] [CrossRef] [PubMed]
- Arsenault-Lapierre, G.; Kim, C.; Turecki, G. Psychiatric diagnoses in 3275 suicides: A meta-analysis. BMC Psychiatry 2004, 4, 37. [Google Scholar] [CrossRef]
- Turecki, G.; Brent, D.A. Suicide and suicidal behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- Turner, O.; Windfuhr, K.; Kapur, N. Suicide in deaf populations: A literature review. Ann. Gen. Psych. 2007, 6, 26. [Google Scholar] [CrossRef] [PubMed]
- Bolton, J.; Walld, R.; Chateau, D.; Finlayson, G.; Sareen, J. Risk of suicide and suicide attempts associated with physical disorders: A population-based, balancing score-matched analysis. Psychol. Med. 2015, 45, 495–504. [Google Scholar] [CrossRef] [PubMed]
- Erlangsen, A.; Stenager, E.; Conwell, Y. Physical diseases as predictors of suicide in older adults: A nationwide, register-based cohort study. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1427–1439. [Google Scholar] [CrossRef] [PubMed]
- Druss, B.; Pincus, H. Suicidal ideation and suicide attempts in general medical illnesses. Arch. Intern. Med. 2000, 160, 1522–1526. [Google Scholar] [CrossRef] [PubMed]
- Ahmedani, B.K.; Peterson, E.L.; Hu, Y.; Rossom, R.C.; Lynch, F.; Lu, C.Y.; Waitzfelder, B.E.; Owen-Smith, A.A.; Hubley, S.; Prabhakar, D.; et al. Major physical health conditions and risk of suicide. Am. J. Prev. Med. 2017, 53, 308–315. [Google Scholar] [CrossRef]
- Pompili, M.; O’Connor, R.C.; Van Heeringen, K. Suicide prevention in the European Region. Crisis 2020, 41, S8–S20. [Google Scholar] [CrossRef]
- Jacobson, G.P.; McCaslin, D.L. A search for evidence of a direct relationship between tinnitus and suicide. J. Am. Acad. Audiol. 2001, 12, 493–496. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Implement. 2021, 19, 3–10. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Ensink, R.J.; Vingerhoets, H.M.; Schmidt, C.T.H.; Cremers, C.W. Treatment for severe palatoclonus by occlusion of the eustachian tube. Otol. Neurotol. 2003, 24, 714–716. [Google Scholar] [CrossRef]
- Lewis, J.E.; Stephens, S.D.G.; McKenna, L. Tinnitus and suicide. Clin. Otolaryngol. Allied Sci. 1994, 19, 50–54. [Google Scholar] [CrossRef]
- Seo, J.H.; Kang, J.M.; Hwang, S.H.; Han, K.D.; Joo, Y.H. Relationship between tinnitus and suicidal behaviour in Korean men and women: A cross-sectional study. Clin. Otolaryngol. 2016, 41, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.N.; Nam, G.E.; Han, K.; Kim, J.S.; Kim, Y.H.; Cho, K.H.; Kang, G.; Roh, Y.K. Association between menstrual cycle irregularity and tinnitus: A nationwide population-based study. Sci. Rep. 2019, 9, 14038. [Google Scholar] [CrossRef] [PubMed]
- Park, H.M.; Jung, J.; Kim, J.K.; Lee, Y.J. Tinnitus and its association with mental health and health-related quality of life in an older population: A nationwide cross-sectional study. J. Appl. Gerontol. 2020, 41, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Han, K.M.; Ko, Y.H.; Shin, C.; Lee, J.H.; Choi, J.; Kwon, D.Y.; Yoon, H.K.; Han, C.; Kim, Y.K. Tinnitus, depression, and suicidal ideation in adults: A nationally representative general population sample. J. Psychiatr. Res. 2018, 98, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-S. Association between tinnitus and mental health among Korean adolescents: The Korea National Health and Nutrition Examination Survey. Cent. Eur. J. Public Health 2018, 26, 65–70. [Google Scholar] [CrossRef]
- Park, E.; Kim, H.; Choi, I.H.; Han, H.M.; Han, K.; Jung, H.H.; Im, G.J. Psychiatric distress as a common risk factor for tinnitus and joint pain: A national population-based survey. Clin. Exp. Otorhinolaryngol. 2020, 13, 234–240. [Google Scholar] [CrossRef]
- Martz, E.; Jelleberg, C.; Dougherty, D.D.; Wolters, C.; Schneiderman, A. Tinnitus, depression, anxiety, and suicide in recent veterans: A retrospective analysis. Ear Hear. 2018, 39, 1046–1056. [Google Scholar] [CrossRef]
- Chang, J.P.C.; Wu, C.C. Serotonin-norepinephrine reuptake inhibitor treatment for tinnitus and depression. J. Clin. Psychopharmacol. 2012, 32, 729. [Google Scholar] [CrossRef]
- Da Silva Souza, D.; Diniz da Rosa, M.R.; Camurça, R.S.; dos Santos Andrade, S.M.M.; Almeida, A.A. Effects of transcranial direct current stimulation in chronic tinnitus treatment: Case study. Int. Arch. Otorhinolaryngol. 2016, 20 (Supp. 1), S94. Available online: https://forl.org.br/anais-dos-congressos/ (accessed on 9 October 2023).
- Fox-Thomas, L.G. Suicidal ideation among patients with chronic tinnitus. Hear. J. 2016, 69, 10–11. [Google Scholar] [CrossRef]
- Dijkstra, E.; Figee, M.; Schuurman, P.R.; Denys, D. Effective deep brain stimulation of intractable tinnitus: A case study. Brain Stimul. 2018, 11, 1205–1207. [Google Scholar] [CrossRef]
- Frankenburg, F.R.; Hegarty, J.D. Tinnitus, psychosis, and suicide. Arch. Intern. Med. 1994, 154, 2371–2375. [Google Scholar] [CrossRef]
- Joshi, P.S.; Sharma, A. A case of asenapine-induced tinnitus. Prim. Care Companion CNS Disord. 2012, 14, 26752. [Google Scholar] [CrossRef]
- Lewis, J.; Stephens, D. Parasuicide and tinnitus. J. Audiol. Med. 1995, 4, 34–39. [Google Scholar]
- Lewis, J.; Stephens, D.; Huws, D. Suicide in tinnitus sufferers. J. Audiologic Med. 1992, 1, 30–37. [Google Scholar]
- Pridmore, S.; Walter, G.; Friedland, P. Tinnitus and suicide: Recent cases on the public record give cause for reconsideration. Otolaryngol. Head. Neck Surg. 2012, 147, 193–195. [Google Scholar] [CrossRef]
- Sisler, K.; Meyer, A.; Miller, S.; Antisdel, J.L. Self-Decapitation Attempt Attributed to Tinnitus and Oral Corticosteroids. Case Report. J. Otol. Rhinol. 2015, 4, 5. [Google Scholar] [CrossRef]
- Wilson, P.H.; Henry, J.; Bowen, M.; Haralambous, G. Tinnitus reaction questionnaire: Psychometric properties of a measure of distress associated with tinnitus. J. Speech Hear. Res. 1991, 34, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Aazh, H.; Moore, B.C. Thoughts about suicide and self-harm in patients with tinnitus and hyperacusis. J. Am. Acad. Audiol. 2018, 29, 255–261. [Google Scholar] [CrossRef]
- Aazh, H.; Landgrebe, M.; Danesh, A.A. Parental mental illness in childhood as a risk factor for suicidal and self-harm ideations in adults seeking help for tinnitus and/or hyperacusis. Am. J. Audiol. 2019, 28, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Ren, L.; Xue, X.; Yu, N.; Liu, P.; Shen, W.; Zhou, H.; Wang, B.; Zhou, J.; Yang, S.; et al. The Comorbidity of Depression and Anxiety Symptoms in Tinnitus Sufferers: A Network Analysis. Brain Sci. 2023, 13, 583. [Google Scholar] [CrossRef] [PubMed]
- Lugo, A.; Trpchevska, N.; Liu, X.; Biswas, R.; Magnusson, C.; Gallus, S.; Cederroth, C.R. Sex-specific association of tinnitus with suicide attempts. JAMA Otolaryngol. Head. Neck Surg. 2019, 145, 685–687. [Google Scholar] [CrossRef]
- Cheng, Y.F.; Xirasagar, S.; Kuo, N.W.; Lin, H.C. Tinnitus and risk of attempted suicide: A one year follow-up study. J. Affect. Disord. 2023, 322, 141–145. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Snaith, R.P.; Zigmond, A.S. The hospital anxiety and depression scale. Br. Med. J. (Clin. Res. Ed.) 1986, 292, 344. [Google Scholar] [CrossRef] [PubMed]
- May, A.M.; Klonsky, E.D. What distinguishes suicide attempters from suicide ideators? A meta-analysis of potential factors. Clin. Psychol. Sci. Pract. 2016, 23, 5. [Google Scholar] [CrossRef]
- Glenn, C.R.; Kleiman, E.M.; Cha, C.B.; Deming, C.A.; Franklin, J.C.; Nock, M.K. Understanding suicide risk within the Research Domain Criteria (RDoC) framework: A meta-analytic review. Depress. Anxiety 2018, 35, 65–88. [Google Scholar] [CrossRef]
- Van Orden, K.A.; Witte, T.K.; Cukrowicz, K.C.; Braithwaite, S.R.; Selby, E.A.; Joiner, T.E., Jr. The interpersonal theory of suicide. Psychol. Rev. 2010, 117, 575–600. [Google Scholar] [CrossRef] [PubMed]
- Kirtley, O.J.; Rodham, K.; Crane, C. Understanding suicidal ideation and behaviour in individuals with chronic pain: A review of the role of novel transdiagnostic psychological factors. Lancet Psychiatry 2020, 7, 282–290. [Google Scholar] [CrossRef]
- De Beurs, D.; Fried, E.I.; Wetherall, K.; Cleare, S.; O’Connor, D.B.; Ferguson, E.; O’Carroll, R.; Connor, R.O. Exploring the psychology of suicidal ideation: A theory driven network analysis. Behav. Res. Ther. 2019, 120, 103419. [Google Scholar] [CrossRef]
- Cima, R.F.F. Bothersome tinnitus: Cognitive behavioral perspectives. HNO 2018, 66, 369. [Google Scholar] [CrossRef]
- Watts, E.J.; Fackrell, K.; Smith, S.; Sheldrake, J.; Haider, H.; Hoare, D.J. Why is tinnitus a problem? A qualitative analysis of problems reported by tinnitus patients. Trends Hear. 2018, 22, 2331216518812250. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, J.W.; Morley, S.; Crombez, G. The experimental analysis of the interruptive, interfering, and identity-distorting effects of chronic pain. Behav. Res. Ther. 2016, 86, 23–34. [Google Scholar] [CrossRef]
- Ribeiro, J.D.; Huang, X.; Fox, K.R.; Walsh, C.G.; Linthicum, K.P. Predicting imminent suicidal thoughts and nonfatal attempts: The role of complexity. Clin. Psychol. Sci. 2019, 7, 941–957. [Google Scholar] [CrossRef]
- Oakey-Frost, N.; Moscardini, E.H.; Cowan, T.; Cohen, A.; Tucker, R.P. The temporal dynamics of wish to live, wish to die, and their short-term prospective relationships with suicidal desire. Behav. Ther. 2023, 54, 584–594. [Google Scholar] [CrossRef] [PubMed]
- De Beurs, D.; Bockting, C.; Kerkhof, A.; Scheepers, F.; O’Connor, R.; Penninx, B.; van de Leemput, I. A network perspective on suicidal behavior: Understanding suicidality as a complex system. Suicide Life Threat. Behav. 2021, 51, 115–126. [Google Scholar] [CrossRef] [PubMed]
- Bryan, C.J.; Stone, S.L.; Rudd, M.D. A practical, evidence-based approach for means-restriction counseling with suicidal patients. Prof. Psychol. Res. Pract. 2011, 42, 339–346. [Google Scholar] [CrossRef]
- Rudd, M.D. Fluid vulnerability theory: A cognitive approach to understanding the process of acute and chronic risk. In Cognition and Suicide: Theory, Research, and Therapy; Ellis, T.E., Ed.; American Psychological Association: Washington, DC, USA, 2006. [Google Scholar]
- Goodfellow, B.; Kolves, K.; De Leo, D. Contemporary nomenclatures of suicidal behaviors: A systematic literature review. Suicide Life Threat. Behav. 2018, 48, 353–366. [Google Scholar] [CrossRef] [PubMed]
- Hallensleben, N.; Spangenberg, L.; Forkmann, T.; Rath, D.; Hegerl, U.; Kersting, A.; Kallert, T.W.; Glaesmer, H. Investigating the dynamics of suicidal ideation. Crisis 2018, 39, 65–69. [Google Scholar] [CrossRef]
- De Leo, D.; Goodfellow, B.; Silverman, M. International study of definitions of English-language terms for suicidal behaviours: A survey exploring preferred terminology. BMJ Open 2021, 11, e043409. [Google Scholar] [CrossRef]
- Nielsen, E.; Padmanathan, P.; Knipe, D. Commit* to change? A call to end the publication of the phrase ‘commit* suicide’. Wellcome Open Res. 2016, 1, 21. [Google Scholar] [CrossRef]
- Padmanathan, P.; Biddle, L.; Hall, K.; Scowcroft, E.; Nielsen, E.; Knipe, D. Language use and suicide: An online cross-sectional survey. PLoS ONE 2019, 14, e0217473. [Google Scholar] [CrossRef]
- Heilbron, N.; Compton, J.S.; Daniel, S.S.; Goldston, D.B. The problematic label of suicide gesture: Alternatives for clinical research and practice. Prof. Psychol. Res. Pract. 2010, 41, 221–227. [Google Scholar] [CrossRef]
- Platt, S. Epidemiology of suicide and parasuicide. J. Psychopharmacol. 1992, 6, 291–299. [Google Scholar] [CrossRef] [PubMed]
- Kapur, N.; Cooper, J.; O’Connor, R.C.; Hawton, K. Non-suicidal self-injury vs. attempted suicide: New diagnosis or false dichotomy? Br. J. Psychiatry 2013, 202, 326–328. [Google Scholar] [CrossRef] [PubMed]
- Zortea, T.C.; Cleare, S.; Melson, A.J.; Wetherall, K.; O’Connor, R.C. Understanding and managing suicide risk. Br. Med. Bull. 2020, 134, 73–84. [Google Scholar] [CrossRef]
- Haw, C.; Hawton, K.; Houston, K.; Townsend, E. Correlates of relative lethality and suicidal intent among deliberate self-harm patients. Suicide Life Threat. Behav. 2003, 33, 353–364. [Google Scholar] [CrossRef]
- Nock, M.K.; Favazza, A.R. Nonsuicidal self-injury: Definition and classification. In Understanding Nonsuicidal Self-Injury: Origins, Assessment, and Treatment; Nock, M.K., Ed.; American Psychological Association: Washington, DC, USA, 2009; pp. 9–18. [Google Scholar]
- National Institute for Health and Care Excellence. Self-Harm: Assessment, Management and Preventing Recurrence; Guideline Scope; NICE: London, UK, 2019. [Google Scholar]
- Carroll, R.; Metcalfe, C.; Gunnell, D. Hospital presenting self-harm and risk of fatal and non-fatal repetition: Systematic review and meta-analysis. PLoS ONE 2014, 9, e89944. [Google Scholar] [CrossRef] [PubMed]
- Chan, M.K.; Bhatti, H.; Meader, N.; Stockton, S.; Evans, J.; O’Connor, R.C.; Kapur, N.; Kendall, T. Predicting suicide following self-harm: Systematic review of risk factors and risk scales. Br. J. Psychiatry 2016, 209, 277–283. [Google Scholar] [CrossRef]
- Lourenco, M.P.; Fuller, T.E.; Ranson, S.; Vlaeyen, J.W.; Cima, R.F. Better Together. Group versus individual Cognitive-Behavioral Therapy for tinnitus: A Multiple-Baseline Single-Case Experimental Design. Ear Hear. 2023, 44, 167–178. [Google Scholar] [CrossRef]
- Kleiman, E.M.; Turner, B.J.; Fedor, S.; Beale, E.E.; Huffman, J.C.; Nock, M.K. Examination of real-time fluctuations in suicidal ideation and its risk factors: Results from two ecological momentary assessment studies. J. Abnorm. Psychol. 2017, 126, 726. [Google Scholar] [CrossRef]
- Mournet, A.M.; Smith, J.T.; Bridge, J.A.; Boudreaux, E.D.; Snyder, D.J.; Claassen, C.A.; Jobes, D.A.; Pao, M.; Horowitz, L.M. Limitations of screening for depression as a proxy for suicide risk in adult medical inpatients. J. Acad. Consult. Liaison Psychiatry 2021, 62, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Na, P.J.; Yaramala, S.R.; Kim, J.A.; Kim, H.; Goes, F.S.; Zandi, P.P.; Vande Voort, J.L.; Sutor, B.; Croarkin, P.; Bobo, W.V. The PHQ-9 Item 9 based screening for suicide risk: A validation study of the Patient Health Questionnaire (PHQ)− 9 Item 9 with the Columbia Suicide Severity Rating Scale (C-SSRS). J. Affect. Disord. 2018, 232, 34–40. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Common Mental Health Problems: Identification and Pathways to Care; Clinical Guideline [CG123]; NICE: London, UK, 2011. [Google Scholar]
- National Institute for Health and Care Excellence. Tinnitus: Assessment and Management; NICE Guideline [NG155]; NICE: London, UK, 2020. [Google Scholar]
- Wang, S.B.; Coppersmith, D.D.; Kleiman, E.M.; Bentley, K.H.; Millner, A.J.; Fortgang, R.; Mair, P.; Dempsey, W.; Huffman, J.C.; Nock, M.K. A pilot study using frequent inpatient assessments of suicidal thinking to predict short-term postdischarge suicidal behavior. JAMA Netw. Open. 2021, 4, e210591. [Google Scholar] [CrossRef]
- Coppersmith, D.D.; Fortgang, R.G.; Kleiman, E.M.; Millner, A.J.; Yeager, A.L.; Mair, P.; Nock, M.K. Effect of frequent assessment of suicidal thinking on its incidence and severity: High-resolution real-time monitoring study. Br. J. Psychiatry 2022, 220, 41–43. [Google Scholar] [CrossRef] [PubMed]
- British Society of Audiology. Practice Guidance Tinnitus in Adults 2021. Available online: https://www.thebsa.org.uk/ (accessed on 1 September 2023).
- Evans, C.; Connell, J.; Barkham, M.; Margison, F.; McGrath, G.; Mellor-Clark, J.; Audin, K. Towards a standardised brief outcome measure: Psychometric properties and utility of the CORE–OM. Br. J. Psychiatry 2002, 180, 51–60. [Google Scholar] [CrossRef]
- Hallford, D.J.; Rusanov, D.J.; Winestone, B.; Kaplan, R.; Fuller-Tyszkiewicz, M.; Melvin, G. Disclosure of suicidal ideation and behaviours: A systematic review and meta-analysis of prevalence. Clin. Psychol. Rev. 2023, 101, 102272102272. [Google Scholar] [CrossRef]
- Cima, R.F.F.; Mazurek, B.; Haider, H.; Kikidis, D.; A Lapira, A.; Noreña, A.; Hoare, D.J. A multidisciplinary European guideline for tinnitus: Diagnostics, assessment, and treatment. HNO 2019, 67, 10–42. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Search: ((tinnitus) AND (suicide)) OR (suicidal ideation) ((“tinnitus”[MeSH Terms] OR “tinnitus”[All Fields]) AND (“suicid”[All Fields] OR “suicidal ideation”[MeSH Terms] OR (“suicidal”[All Fields] AND “ideation”[All Fields]) OR “suicidal ideation”[All Fields] OR “suicidality”[All Fields] OR “suicidal”[All Fields] OR “suicidally”[All Fields] OR “suicidals”[All Fields] OR “suicide”[MeSH Terms] OR “suicide”[All Fields] OR “suicides”[All Fields] OR “suicide s”[All Fields] OR “suicided”[All Fields] OR “suiciders”[All Fields])) OR (“suicidal ideation”[MeSH Terms] OR (“suicidal”[All Fields] AND “ideation”[All Fields]) OR “suicidal ideation”[All Fields]) Translations tinnitus: “tinnitus”[MeSH Terms] OR “tinnitus”[All Fields] suicide: “suicid”[All Fields] OR “suicidal ideation”[MeSH Terms] OR (“suicidal”[All Fields] AND “ideation”[All Fields]) OR “suicidal ideation”[All Fields] OR “suicidality”[All Fields] OR “suicidal”[All Fields] OR “suicidally”[All Fields] OR “suicidals”[All Fields] OR “suicide”[MeSH Terms] OR “suicide”[All Fields] OR “suicides”[All Fields] OR “suicide’s”[All Fields] OR “suicided”[All Fields] OR “suiciders”[All Fields] suicidal ideation: “suicidal ideation”[MeSH Terms] OR (“suicidal”[All Fields] AND “ideation”[All Fields]) OR “suicidal ideation”[All Fields] |
| Author | Date | Title | Country | Population | Sample Size | Participants with Tinnitus (n) | Tinnitus Severity | Method/Question Used to Identify Tinnitus | Method/Question Used to Identify Bothersome Tinnitus | Method/Question Used to Identify Suicide/Suicidal Ideation | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Han et al. [46] | 2018 | Tinnitus, depression, and suicidal ideation in adults: A nationally representative general population sample | Korea | Respondents of tinnitus evaluation questionnaires of the KNHANES aged 19+ | 28,930 | 6391 | Mild, moderate, and severe (no disturbance, annoying and very annoying) | During the past year, did you ever hear a sound (buzzing, hissing, ringing, humming, roaring, machinery noise) originating in your ear? (yes, no, cannot remember) | How much did the sound originating in your ear disturb your daily life? (no, annoying, very annoying level causing sleep disturbance). | Within the past year, have you ever seriously considered attempting suicide? (yes or no) | No suicide—ideation reported |
| Martz et al. [49] | 2018 | Tinnitus, Depression, Anxiety, and Suicide in Recent Veterans: A Retrospective Analysis | USA | Veterans who separated from service and who were not killed in action. | 769,934 | 116,358 (15%) | Not reported | NA-diagnosed with tinnitus | Not reported | Not reported | ICD-10 codes were used to identify cause of death. |
| Kim et al. [47] | 2018 | Association between tinnitus and mental health among Korean adolescents: The Korea National Health and Nutrition Examination Survey | Korea | Adolescent respondents of the KNHANES V | 1587 | 286 | No problem, bothering, having trouble sleeping | In the past 12 months, have you been bothered by buzzing in your ears? (yes, no) | How much of a problem is the ringing in your ears? (no problem, bothering, having trouble sleeping) | Have you ever thought of committing suicide in the last year? (yes, no) | No suicide-ideation reported |
| Seo et al. [43] | 2015 | Relationship between tinnitus and suicidal behaviour in Korean men and women: a cross-sectional study | Korea | Korean individuals who participated in 2010 to 2012 Korean National Health and Nutrition Examination Survey (KNHANES) | 17,446 | 3949 21.4% | Not annoying/annoying; irritating; severely annoying and causes sleep problems | Within the past year, did you ever hear a sound (buzzing, hissing, ringing, humming, roaring, machinery noise) originating in your ear? | How severe is this noise in your daily life? | In the last 12 months, did you think about committing suicide? | NA |
| Park et al. [48] | 2020 | Psychiatric Distress as a Common Risk Factor for Tinnitus and Joint Pain: A National Population-Based Survey | Korea | General over 50s | 9032 | 2413 | Classified as none, not annoying, annoying, and severely annoying | Single question | Single question: none, not annoying, annoying, severely annoying. | Positive answer to the question about suicidal ideation and suicide attempt over the past year | NA |
| Park et al. [45] | 2020 | Tinnitus and Its Association with Mental Health and Health-Related Quality of Life in an Older Population: A Nationwide Cross-Sectional Study | Korea | General over 60s | 5129 | 1402 | Rated ‘annoying’ by 605 participants | For the past executive 12 months, have you ever had ringing, roaring, or buzzing in your ears? | Survey questions: normal, tolerable tinnitus, and annoying tinnitus identified by asking participants with tinnitus. How much do these sounds create annoyance in your life? | Have you ever thought about committing suicide within 12 months? | NA |
| Yu et al. [44] | 2019 | Association between menstrual cycle irregularity and tinnitus: a nationwide population-based study | Korea | General, premenopausal Korean women | 4633 | 934 | Rated ‘annoying’ by 605 participants | For the past executive 12 months, have you ever had ringing, roaring, or buzzing in your ears? | How much do these sounds create annoyance in your life? | Have you ever thought about committing suicide within the last 12 months? | NA |
| Author | Date | Title | Country | Population | Sample Size | Participants with Tinnitus (n) | Tinnitus Severity | Method/Question Used to Identify Tinnitus | Method/Question Used to Identify Bothersome Tinnitus | Method/Question Used to Identify Suicide/Suicidal Ideation | Method of Suicide |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Chang and Wu [50] | 2012 | Serotonin-Norepinephrine Reuptake Inhibitor Treatment for Tinnitus and Depression | Taiwan | Male with bilateral tinnitus | 1 | 1 | Severe- interfering with mood, sleep, and psychosocial functioning | Not reported | Not reported | Not reported | No suicide—ideation reported |
| Da Silva Souza et al. [51] | 2016 | Effects of Transcranial Direct Current Stimulation in Chronic Tinnitus Treatment: Case Study | Brazil | Female with bilateral tinnitus | 1 | 1 | Not reported | Acuphenometry, VAS | Acuphenometry, VAS | Not reported | No suicide—patient reported ideation |
| Dijkstra et al. [53] | 2018 | Effective deep brain stimulation of intractable tinnitus: A case study | Netherlands | Female tinnitus patient | 1 | 1 | Intractable tinnitus causing severe suffering | Tinnitus Handicap Inventory, Tinnitus Functional Index | Tinnitus Handicap Inventory, Tinnitus Functional Index | Hamilton Depression Rating Scale | Previous suicide attempt with autointoxication |
| Ensink et al. [41] | 2003 | Treatment for Severe Palatoclonus by Occlusion of the Eustachian Tube | Netherlands | Male child with tinnitus | 1 | 1 | Intense, loud, severely interfering with sleep | Tinnitus heard by examiner by bringing own ear at a distance of approximately 20 to 30 cm to the left ear of the patient | Not reported | Expressed suicide wish from patient | No suicide—ideation reported |
| Frankenburg and Hegarty [54] | 1994 | Tinnitus, Psychosis, and Suicide | USA | Tinnitus patients | 4 | 4 | Reported as unrelenting, tiresome | Not reported | Not reported | Expressed suicide wishes from patients. One patient attempted suicide | Not reported |
| Joshi and Sharma [55] | 2012 | A Case of Asenapine-Induced Tinnitus | USA | Female patient | 1 | 1 | Distressing | Not reported | Not reported | Not reported | No suicide—ideation reported. Suicidal ideation |
| Lewis and Stephens [56] | 1995 | Parasuicide and tinnitus | UK | Patients admitted for overdose to Poisons Unit | 184 | 3 | Not reported | Do you suffer from tinnitus, that is, noise(s) in your ears or head? (yes, no). Please describe the tinnitus (pulsatile, buzzing, whistling, hissing, other) | What influence did the tinnitus have on your decision to take an overdose? (none, it contributed, the main reason) | Patients were admitted for previous overdose | Self-harm /Attempted suicide by overdose |
| Lewis, Stephens, and Huws [57] | 1992 | Suicide in tinnitus sufferers | UK | Clinical tinnitus patients, and one additional account | 6 | 6 | Severe | Various | Not reported | Reported suicides in clinic patients | Hanging, attempted overdose, of alcohol and drugs, overdose of antidepressants, overdose of pain medication, suffocation |
| Lewis, Stephens, and McKenna [42] | 1994 | Tinnitus and suicide | UK | Clinical tinnitus patients | 28 | 28 | Not reported | Tinnitus duration: Years and months Tinnitus ear: right/left/both/head Nature of tinnitus: pulsatile/whistling/buzzing/hissing/other | Not reported | Clinics required to report on patients who die by suicide | Self-poisoning, firearm, suffocation, hanging, drowning |
| Pridmore et al. [58] | 2012 | Tinnitus and Suicide: Recent Cases on the Public Record Give Cause for Reconsideration | USA | 4 cases assessed by a coroner over 10 years- found in newspaper articles and online | 4 | 4 | Not reported | Not reported | Not reported | Newspaper and Web search for articles published over the last 10 years | Jumped from height. Hanging. Firearms. Self-stabbing |
| Fox-Thomas [52] | 2016 | Suicidal Ideation Among Patients with Chronic Tinnitus | USA | Clinical records which included the Tinnitus Reaction Questionnaire (TRQ) | 200 | 200 | Not significant, significant, mild, moderate, severe, profound | TRQ in clinical record | Using a 5-point Likert scale (0–4), patients rated tinnitus distress for 26 items ranging from “not at all” to “almost all of the time” | My tinnitus has led me to think about suicide (#24 on TRQ). how tinnitus has affected you over the past week | NA |
| Sisler et al. [59] | 2015 | Self-Decapitation Attempt Attributed to Tinnitus and Oral Corticosteroids | USA | Clinical patient | 1 | 1 | Severe tinnitus | Case report | Case report | Case report | NA—attempted by self-poisoning and self-laceration |
| Author | Date | Title | Country | Population | Sample Size | Participants with Tinnitus (n) | Tinnitus Severity | Method/Question Used to Identify Tinnitus | Method/Question Used to Identify Bothersome Tinnitus | Method/Question Used to Identify Suicide/Suicidal Ideation | Method of Suicide |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Aazh and Moore [61] | 2018 | Thoughts about Suicide and Self-Harm in Patients with Tinnitus and Hyperacusis | UK | Clinical tinnitus patients—specialist clinic for patients seeking help with tinnitus | 150 | 144 | 32 mild, 42 moderate, 54 severe | Questionnaire | Tinnitus Handicap Inventory, VAS | Question 9 on PHQ9 | No suicide—study measured ideation |
| Lugo et al. [64] | 2019 | Sex-Specific Association of Tinnitus With Suicide Attempts | Sweden | Adults from Stockholm County (Sweden) | 71,542 | 16,066 (any tinnitus), of which 1995 were severe | “No; Yes (moderate problem); Yes (severe problem”) | “Do you have any of the following health problems or symptoms?” …tinnitus…. | Not reported | “Have you ever tried to take your own life?” | NA |
| Aazh et al. [62] | 2019 | Parental Mental Illness in Childhood as a Risk Factor for Suicidal and Self-Harm Ideations in Adults Seeking Help for Tinnitus and/or Hyperacusis | UK | Patients at Tinnitus and Hyperacusis Therapy Specialist Clinic | 292 | 286 | Mild, moderate, severe | Tinnitus Handicap Inventory | Tinnitus Handicap Inventory | Question 9 on PHQ99. | No suicide—ideation reported |
| Cheng et al. [65] | 2023 | Tinnitus and risk of attempted suicide: A one year follow-up study | Taiwan | Patients aged ≥20 years old who received a first-time diagnosis of tinnitus and no history of suicide for 3 years before tinnitus onset. Matched controls with no tinnitus | 386,055 | Subjective Any—includes codes for tinnitus, unspecified | Not reported | At least two outpatient medical claims with a diagnosis of tinnitus filed by an otorhinolaryngologist or a neurologist | none | None–not recorded in ICD codes. Whether or not a sampled patient had received a diagnosis of suicide attempt during one-year follow-up. ICD codes | NA |
| Chen et al. [63] | 2023 | The Comorbidity of Depression and Anxiety Symptoms in Tinnitus Sufferers: A Network Analysis | China | Tinnitus sufferers aged over 11 years followed up at the tinnitus outpatient department | 566 | 566 | 0–10 VAS; Minimal = 0–3, mild = 4–6), Severe = 7–10 | Not reported | VAS | Question 9 on PHQ9 | NA |
| Suicide | Intentionally ending one’s own life |
| Suicidal behaviour | Behaviours that may result in ending one’s life, whether fatal or not. This term excludes suicidal ideation |
| Suicidal ideation | Any thoughts about ending one’s own life. May be active, with a clear plan for suicide, or passive, with thoughts about wishing to die |
| Suicide attempt | Self-injurious non-fatal behaviour with inferred or actual intent to die |
| Self-harm | Self-injurious behaviours with or without intent to die. Does not distinguish between suicide attempt and non-suicidal self-injury |
| Non-suicidal self-injury | Self-injurious behaviours without any intent to die |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MacDonald, C.; Caimino, C.; Burns-O’Connell, G.; Hartley, D.; Lockwood, J.; Sereda, M.; Whitmer, W.; Cima, R.; Turton, L.; Hoare, D.J. Tinnitus, Suicide, and Suicidal Ideation: A Scoping Review of Primary Research. Brain Sci. 2023, 13, 1496. https://doi.org/10.3390/brainsci13101496
MacDonald C, Caimino C, Burns-O’Connell G, Hartley D, Lockwood J, Sereda M, Whitmer W, Cima R, Turton L, Hoare DJ. Tinnitus, Suicide, and Suicidal Ideation: A Scoping Review of Primary Research. Brain Sciences. 2023; 13(10):1496. https://doi.org/10.3390/brainsci13101496
Chicago/Turabian StyleMacDonald, Carol, Charlotte Caimino, Georgina Burns-O’Connell, Douglas Hartley, Joanna Lockwood, Magdalena Sereda, William Whitmer, Rilana Cima, Laura Turton, and Derek J. Hoare. 2023. "Tinnitus, Suicide, and Suicidal Ideation: A Scoping Review of Primary Research" Brain Sciences 13, no. 10: 1496. https://doi.org/10.3390/brainsci13101496