
Rumination as a Transdiagnostic Phenomenon in the 21st Century: The Flow Model of Rumination
by
 , and
, and
Stephanie M. Y. Wong
1,† ,
,
Eric Y. H. Chen
1,2,*,†,
Michelle C. Y. Lee
1,
Y. N. Suen
1 and
Christy L. M. Hui
1 1
Department of Psychiatry, School of Clinical Medicine, LKS Faculty of Medicine, The University of Hong Kong, Hong Kong
2
The State Key Laboratory of Brain and Cognitive Sciences, The University of Hong Kong, Hong Kong
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Brain Sci. 2023, 13(7), 1041; https://doi.org/10.3390/brainsci13071041
Submission received: 30 May 2023
/
Revised: 15 June 2023
/
Accepted: 6 July 2023
/
Published: 8 July 2023
(This article belongs to the Special Issue Cognitive Neuroscience Approaches to the Psychopathology of Psychotic Disorders)
{kind=link}
Abstract
:Rumination and its related mental phenomena share associated impairments in cognition, such as executive functions and attentional processes across different clinical conditions (e.g., in psychotic disorders). In recent decades, however, the notion of rumination has been increasingly narrowed to the “self-focused” type in depressive disorders. A closer review of the literature shows that rumination may be construed as a broader process characterized by repetitive thoughts about certain mental contents that interfere with one’s daily activities, not only limited to those related to “self”. A further examination of the construct of rumination beyond the narrowly focused depressive rumination would help expand intervention opportunities for mental disorders in today’s context. We first review the development of the clinical construct of rumination with regard to its historical roots and its roles in psychopathology. This builds the foundation for the introduction of the “Flow Model of Rumination (FMR)”, which conceptualizes rumination as a disruption of a smooth flow of mental contents in conscious experience that depends on the coordinated interactions between intention, memory, affect, and external events. The conceptual review concludes with a discussion of the impact of rapid technological advances (such as smartphones) on rumination. Particularly in contemporary societies today, a broader consideration of rumination not only from a cognition viewpoint, but also incorporating a human–device interaction perspective, is necessitated. The implications of the FMR in contemporary mental health practice are discussed.
1. Introduction
The phenomenon of rumination has long been recognized as a symptom of psychiatric conditions. Rumination may generally be construed as a process of repetitive thoughts [1]. While rumination was described as “fixed ideas” (French: idees fixes) and the “compulsion to repeat” (German: Wiederholungszwang) [2] in the 19th century, recent research has increasingly confined the phenomenon to a narrowed focus on rumination of the depressive type [3,4,5]. As a result, the study of the mechanisms underlying rumination may have been limited to a narrower construct of depressive rumination. Such a focus might have inadvertently limited a broader understanding of its phenomenology and its application to mental health work and research.
Narrowed attention span and reduced executive capacity have been suggested to play critical roles in rumination and a broader range of mental health conditions [6,7]. In addition, in contrast to depressive rumination, the content of rumination can consist of not only the self but also environmental factors [8,9,10,11]. It is recognized that rumination is a transdiagnostic symptom observed across psychiatric conditions, including not only depression and generalized anxiety but also post-traumatic stress disorder (PTSD), social anxiety disorder, obsessive compulsive disorder, bipolar disorder, and psychosis spectrum disorders [12,13,14,15].
A broader investigation into the mechanisms underlying rumination not limited to the depressive type can help widen future intervention opportunities for some of the most complex and debilitating psychiatric conditions. We begin with a conceptual review of existing accounts of rumination and its related phenomena in this paper, followed by the introduction of a comprehensive integrative framework—the Flow Model of Rumination (FMR)—wherein rumination is conceptualized as a neurocognitive process that encompasses a wide range of experiences related to the “flow” of mental contents. From this perspective, rumination may be understood not only as a form of internally triggered self-focused attention but also as “outward-focused” attention. This renewed reflection on rumination is built upon both earlier and recent work to offer a parsimonious account of both internally and externally focused ruminative experiences. Importantly, the increasing availability of mobile online technologies [16,17,18,19] has provided additional mechanisms for triggering and maintaining ruminative experiences, which has important implications for modern challenges in global mental health. The potential application of the FMR in contemporary mental health practices in today’s context will also be discussed.
2. Existing Accounts of Rumination
2.1. Early Accounts of Rumination
The notion that ideas flow in succession by “connexion and association” [20] has been implicit in major accounts of human thought processes from the writings of Aristotle—see Buckingham and Finger (1997) [21]—as well as Hobbes (1651) [22], Locke (1689) [23], and Hume (1748) [24]. These perspectives laid the foundations for the account of the “stream of consciousness” in James (1890) [25], which characterized different modes of “forward-flowing ideas”. On this basis, more recent theories have defined “mental progression” as the smooth advancement of relevant mental contents embedded within coherent contexts (e.g., [26]), which presumes spontaneous progression unless there is a deliberate intent to “focus” on the idea [24,25,26,27,28]. By the 1800s and 1900s, the excessive and involuntary tendency to fixate on certain thoughts and ideas had also been described as “idee irresistible” [29] and “idees fixes” [30]. These early formulations of repetitive internal experiences shed light on the relevance of intentionality and regulatory processes in the genesis of experiential contents and draw similarities with recent neuroscientific research on the role of mental representations in thought suppression [31].
2.2. Recent Accounts of Rumination
2.2.1. Models of Depressive Rumination
Various models of depressive rumination have since been proposed. The Response Styles Theory (RST) [3] describes rumination as repetitive thoughts about one’s distress symptoms and their causes and consequences. This type of self-focused rumination is also termed “brooding”, which is characterized by thoughts such as “Why did this happen to me and not others?”, “What am I doing to deserve this?”, and “Why do I have problems other people don’t have?” [32]. Similarly, the Rumination on Sadness model that was later postulated [33] also conceptualized ruminative thoughts as being fixated on negative affect rather than being goal-directed. The H-EX-A-GO-N model of rumination [34], which considers the individual components of Habit development, Executive control, Abstract processing, Goal discrepancies, and Negative bias, is among the latest efforts to organize existing models with the aim to better understand the onset and maintenance of depressive rumination, although its focus is also limited to the self-focused type of rumination. Rumination about non-self-focused contents, but rather those concerning other people and environmental stressors, has been less discussed.
2.2.2. Goal Progress Theory of Rumination
Several other models have considered the relevance of rumination to other personal intentions and internal mechanisms, such as one’s goals, over-general memory, and spontaneous thoughts. Goal-oriented rumination is another example of a commonly studied form of rumination that has been described in the Goal Progress Theory of Rumination. This type of rumination contrasts with depressive rumination in that its thought content is focused not on depressive symptoms but rather on one’s failure to make progress towards personally significant goals [35]. In addition, while negative affect can also arise as a result of goal failure, the maintenance of goals in one’s awareness may also facilitate problem-solving, self-evaluation, and, in turn, goal attainment. Goal-oriented rumination may thus at times also be considered to be a healthy adaptive form of rumination. Nevertheless, there is still little understanding of when goal-oriented rumination can be beneficial or detrimental to mental health. This theory also puts more emphasis on mental contents that are directly related to oneself, with little consideration for how one’s rumination state can be affected by one’s external environment.
2.2.3. Accounts of Rumination in Relation to External Events
The Stress-Reactive Model of Rumination [36] and the Post-Event Processing (PEP) theory [37] are two examples of rumination that also consider the relevance of external events in one’s rumination content. Stress-reactive rumination refers to repetitive thoughts about the negative inferences arising from stressful experiences [36]. Interestingly, longitudinal and ecological momentary assessment studies have found that stress-reactive rumination, but not self-focused depressive rumination, can interact with external life stressors to increase depressive symptoms [38,39]. Nonetheless, as exemplified by its measurement instrument (the Stress-Reactive Rumination Scale [39]), this form of rumination remains largely “self-focused” in that its content largely revolves around oneself rather than the event (e.g., “Think about how the stressful event was all your fault,” “Think about how things like this always happen to you”).
Meanwhile, the PEP theory postulates that those with social anxiety tend to internally review their behaviors following engagement in distressing social events [37,40]. The excessive encoding of negative details related to one’s performance can result in negative self-perceptions after the event. Thoughts related to whether one “could have done differently” in the situation (self-focused) also appear to play a bigger role in PEP as compared to details of the event.
2.2.4. Neurocognitive Models of Rumination
Various neurocognitive models have also been proposed with the aim of explaining rumination and its underlying cognitive mechanisms. Their explanations of the phenomenon and its roles provide a relatively broader framework that can also be applied to other psychiatric conditions.
For instance, the “Capture and Rumination, Functional Avoidance, and Executive Control” (CaRFAX) Model hypothesized that the activation of important, though unpleasant, conceptual self-relevant information could “capture” one’s attention and increase the retrieval of related autobiographical memories [41]. This may also be understood in the context of psychotic symptoms, such as “ideas of reference” (i.e., attribution of often irrelevant information in the social environment as targeting oneself), which have often been discussed in relation to attentional biases to threatening stimuli [42,43,44,45]. Attentional biases to and “attentional capture by” threat, including emotionally salient threat signals (e.g., angry faces), have also been recorded in those with prior trauma exposure and PTSD [46,47,48]. According to the CaRFAX model, the fixation on selected thoughts and the further diminishing of executive resources could also contribute to overgeneral memories [49,50], and it has been shown to be implicated in not only depression but also PTSD and psychosis spectrum disorders [51,52,53,54].
The Attentional Scope Model of Rumination views rumination as a narrowed array of thoughts, percepts, and actions in one’s working memory or long-term memory. This in turn leads to the continuation of focus on certain thought contents and difficulties in shifting [7]. From this perspective, rumination may be viewed as a more general form of perseverative cognition.
Indeed, several researchers have viewed rumination as a process characterized by strong automatic constraints and limited mental flexibility relative to daydreaming and mind-wandering [27,55,56,57]. Recent neurobiological accounts have also identified altered connectivity of the default mode network (DMN) to be associated with rumination [58,59], which has also been considered to underlie the self-referential processes seen in other mood and anxiety disorders, PTSD, and psychotic disorders [60,61,62,63].
Importantly, in addition to the focus on rumination as a marker of increased cognitive vulnerability to depressive disorders, an abundance of studies have in fact provided evidence to suggest its impact on anxiety disorders [64,65,66], as well as other psychiatric conditions including PTSD, social anxiety disorder, OCD, bipolar disorder, and psychotic disorders [13,67,68,69,70]. These studies provide a strong basis to consider rumination beyond the narrowly defined depressive type.
2.2.5. Neurobiological Accounts of Rumination and Related Processes
One example of ruminative processes is the phenomenon of “obsessions” in OCD, which are described as self-generated intrusive repetitive thinking that is difficult to control and disengage from [71,72]. Increased activity has been detected in functional imaging studies in the orbitofrontal cortex, the anterior and posterior cingulate gyrus, the insula, the caudate nucleus, and the anterior thalamus regions [73]. These components, particularly involving the cortico-striato-thalamo-cortical loop, are linked to obsessive thoughts (e.g., [74,75,76]) in OCD, the increase in which may be normalized with treatment (e.g., selective serotonin reuptake inhibitors). Another potentially relevant brain process in rumination may involve perseveration, which refers to the persistence of a previously appropriate response that is no longer appropriate due to the change in context. The inability to shift-set and switch responses relevant to the context may be related to the failure of multiple inhibitory systems in the lateral prefrontal cortex [77]. It is thus likely that ruminative processes are related to multiple excitatory and inhibitory brain mechanisms in the prefrontal cortex as well as the cortico-striato-pallidal-thalamic loops.
2.3. Rumination beyond Depressive Disorders
2.3.1. Post-Traumatic Stress Disorder
In fact, one of the earlier works that formed the foundations of RST examined the ruminative response styles in both depressive and PTSD symptoms following the 1989 Loma Prieta Earthquake [8]. Measures of the study consisted of not only depressive rumination but also rumination about the earthquake (e.g., thoughts about “the moment the earthquake happened,” “the people who were killed,” and “what might have happened during the earthquake”)—a type of “event-based rumination”. Beyond depressive rumination, rumination in PTSD has been defined as repeated thoughts about a traumatic event, its consequences, and the retrospective possibilities of prevention [69,78]. More recent studies have also confirmed the manifestation of this type of event-based rumination subsequent to significant stressors and trauma and have confirmed its associations with not only symptoms of depression but also PTSD and ideas of reference [9,79,80,81,82].
Notably, the study on survivors of the 2008 Wenchuan earthquake found that intrusive rumination about the earthquake (e.g., “I cannot help thinking about the earthquake”) was associated with PTSD symptoms, whereas deliberate rumination about the earthquake (e.g., “I thought about what I could learn from the earthquake experience”) was associated with symptoms of post-traumatic growth (e.g., realization and appreciation of personal strength and life and new possibilities) [82], which further suggest differential pathways between involuntary and voluntary ruminative thoughts, with the latter showing more resemblance to constructive repetitive thinking and goal-oriented rumination.
2.3.2. Rumination in Suicidal Ideation and Related Behaviors
Of note, while depressive rumination has also been found to be a precursor of suicidal ideation and behaviors [83,84], a number of studies have discussed the phenomenon of perseverative cognitions about suicide (termed “suicide-specific cognitions” or “suicide-related rumination”), which describes persistent thoughts about suicide to the extent that current tasks are affected [85,86,87,88,89]. Suicide-related rumination offers an example of fixed thoughts about an intention. Although suicidal thoughts are closely related to depression, further studies of this important phenomenon may benefit from a broadened framework from the narrowly focused depressive rumination.
2.3.3. Psychotic Symptoms and Disorders
Perseverative thinking and difficulties in set-shifting, representing other related forms of perseverative cognitions, have also long been linked to prefrontal dysfunctions in schizophrenia [90,91]. Like rumination, perseveration involves unintentional yet persistent and context-inappropriate thoughts [92], although multiple modalities can be implicated, spanning beyond semantic repetitions to perseverative cognition and motor phenomena [93]. Of note, using a “content-free” measure of perseverative thoughts (e.g., “I keep thinking about the same issues all the time” in the Perseverative Thinking Questionnaire [94]), a study has reported significantly higher levels of negative perseverative thoughts in patients with persecutory delusions as compared to healthy controls [95]. At the same time, preoccupation has been considered to be a key dimension of delusions and related experiences (e.g., [96,97,98,99]) and is also directly relevant to experiences of paranoia and hallucinations in subthreshold psychotic-like experiences [100].
Indeed, rumination has been linked to proneness to psychosis and psychosis disorders, plausibly via the fixation on negative information and excessive cognitive load [101,102,103]. A study conducted among remitted schizophrenia patients has in fact found that rumination was associated with negative symptoms—particularly stereotyped thinking and emotional withdrawal—but not depressive symptoms [104]. This suggests that rumination may be differentially manifested across psychiatric conditions. In another study that explored the content of rumination in a group of schizophrenia patients, 70% of patients perceived their ruminative thoughts to be related to their mental illness, with some noting contents of not only “life failure” and significant life events but also their psychotic symptoms, such as “voices” [105]. A recent study conducted amid large-scale social unrest and COVID-19 in Hong Kong has also reported event-based rumination to be significantly associated with the psychotic-like experience of ideas of reference in a large community sample [81].
3. The Flow Model of Rumination
Based on the aforementioned gaps in existing models of rumination, we propose the Flow Model of Rumination (FMR) to broaden the understanding and applicability of the phenomenon. The notion of “flow” in the FMR differs from that described by Csikszentmihalyi (1975) (i.e., an “optimal” state of consciousness characterized by focused concentration of one’s present experience) [106] but rather places emphasis on the “flow of thoughts” with time (e.g., the moment-to-moment awareness and thought contents), likened to that described in the work of Klinger and Cox (1987) and other neurocognitive models of mental states and experiences (e.g., [57,107,108]).
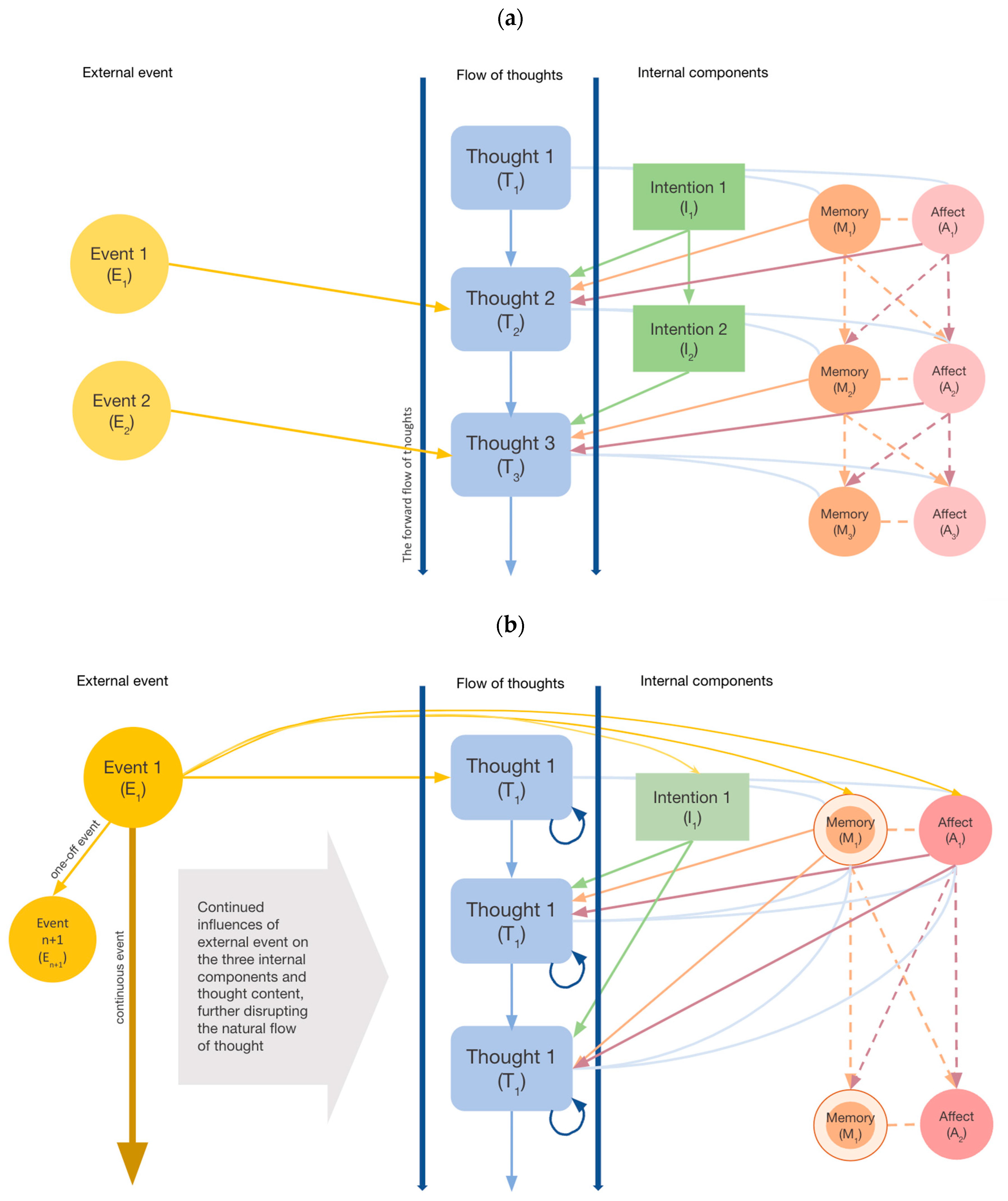
In the FMR, a smooth flow of content of consciousness results from coordinated interactions between three internal components and one external component. Experiential content at a future time point is determined by contents at TN+1, namely intention (I), memory (M), affect (A), and external events (E) at the previous time point (Figure 1). Figure 1a illustrates the forward-regulated flow of thoughts in the absence of rumination, while Figure 1b illustrates the stagnated flow of thoughts (state of rumination) in the presence of significant external events. These components are expected to interact in a dynamic manner and involve mechanisms including intentional activation, temporal decay, attentional shifts, affective reactivity, and inhibitory processes in regulating the “flow” of thoughts. It is also postulated that each experiential content at the present moment contributes as a source of input that partially determines the mental content at the next moment (TN+1). Details of each of these components are further described below.
This model stands out from existing concepts of mental progression in highlighting the combined influences of both internal cognitive processes, affective states, and the external environment in determining whether a thought would “flow” or become stagnated (presented as two extremes on a continuum), as in the case of rumination.
Note. In Figure 1a, the Flow Model of Rumination (FMR) illustrates four key factors contributing to the forward-regulated flow of thoughts in the absence of rumination. On the left are conscious processes, including the influence of external events and deliberate intentions over subsequent thoughts (TN+1). The right side depicts the relationship between moving thoughts and affective states and preconscious memory. Figure 1b illustrates the occurrence of rumination in the presence of a significant external event. The event E1, which may either be a one-off incident or an ongoing situation, can feed into persistent event-related thought in spite of other events occurring in the environment (En+1). Such an event can also stimulate certain affective states, activate certain preconscious memory deemed to be associated with the current experiences (which could be spurious in some conditions), and influence the intent to repeatedly focus on the same thought. All these processes also depend on one’s cognitive state and attentional control. Together, external events and internal processes can stagnate thought progression, which can result in a process of rumination.
3.1. Intentional and Involuntary Activation
One key component of the model concerns the intentional or involuntary modes of thought maintenance (Figure 1). The intention to actively focus on specific thoughts is typically involved in task-relevant, goal-directed problem-solving [35,109,110]. While typical problem-solving situations require a degree of cognitive flexibility to accommodate alternative thinking [111], involuntarily triggered thought contents can increase the likelihood of fixated thoughts. Indeed, incidental, as compared to intentional, encoding and consolidation of information have been found to be associated with poorer attentional control [112]. Neuroimaging observations have also suggested that intentional thinking is associated with Task Positive Network activations as opposed to DMN activities [113].
3.2. Affect and Interactions with Cognitive Processes and Memory
The experience of different affective states can be associated with stagnation in thoughts in different manners and may relate to the form of attentional biases present across psychiatric conditions.
3.2.1. Negative Affect
The role of negative affect in exacerbating ruminative thoughts has been elaborately discussed in the literature. Those with more depressive symptoms have been shown to have a greater tendency to focus their attention on negatively valenced information [32,34,114], which can, in turn, contribute to increased preoccupations and narrowed attention [3,7,115,116,117,118].
3.2.2. Angry Affect
Aside from negative affect, angry affect (e.g., after a traumatic event, being provoked) has also been found to be a key factor that contributes to rumination [10,119]. In a brain imaging study, significant activation in areas such as the hippocampus, insula, and cingulate cortex has been found to be associated with angry rumination following provocation [10]. Despite significant correlations between anger and depressive rumination [120], several studies have found anger rumination to be at least partially distinct from depressive rumination, wherein anger rumination is uniquely associated with aggression and externalizing disorders in females [121,122].
3.2.3. Positive Affect
While less frequent, it is also possible that individuals also dwell on positive aspects of themselves and positive life events [123,124]. This type of “positive rumination” has received less scientific attention, although a number of studies have found that engagement in positive rumination is in fact associated with fewer depressive symptoms [125] and improved working memory-updating ability [126,127].
It is indeed possible that “positive rumination” requires effort to fixate on positive thoughts (as in the case of constructive repetitive thinking [128]). Notably, some aspects of positive rumination (e.g., emotion-focused rather than self-focused) may be more pronounced in conditions such as mania [11]. This may also relate to an increased attentional bias to positive stimuli, avoidance of negative stimuli, and difficulties in focusing attention [129,130,131,132].
3.2.4. Suspiciousness and Paranoia
Furthermore, particularly in psychotic disorders, increased experiences of suspiciousness can be triggered by external stressors [133,134]. These experiences can interact with altered cognitive processes, such as heightened attention and prolonged fixation on threatening cues and negative information [114,135,136,137], reduced cognitive flexibility [138], working memory deficits [139], over-general autobiographical memory [140], reduced memory specificity and richness of detail [141], and other negative affective states (e.g., social anxiety, generalized anxiety, depressive mood) [142]. Notably, the tendency to attend to perceived threatening stimuli and make spurious associations between coincidental thoughts and environmental cues [143] may further perpetuate the cycle of fixated thoughts related to delusional ideas.
3.3. Interactions between Internal and External Influences in the Flow of Mental States
In the FMR, mental contents activated during a rumination-free state tend to fade with time as new content emerges [144,145,146]. The constant dynamic interplay between intrinsic and extrinsic factors determines the “flow” of mental states.
In situations where the external environment is relatively stable, the contribution to the stagnation in thoughts would largely be the result of dysregulations of internal cognitive processes (e.g., reduced attentional resources and cognitive biases [1]). For instance, the failure of inhibitory processes can compromise disengagement from repetitive thoughts in the working memory and limit the emergence of new mental contents [147,148]. At the same time, the failure to update mental representations is also considered to be one of the key processes underlying a stagnated mental flow state [149] and deficits in inhibiting mental representations of the previous moment [150]. Notably, as affect often does not fade quickly and is susceptible to reactivation and intensification [119,151,152], the persistence of affect-laden thoughts can further interfere with information updating and increase the likelihood of rumination [153].
However, when faced with significant, intense triggers in the environment (e.g., traumatic, threatening events, and large-scale stressors), particularly those that do not integrate well with one’s pre-existing worldviews [154,155], the flow of thoughts could become disrupted even when internal processes are relatively intact.
Exposure to significant stressors could activate pre-existing memories and intensify the affective experiences [151], which can in turn perpetuate the rumination cycle (Figure 1b). The activation of mental representations of significant events is also often emotionally intense and value-laden [156], which can make disengagement challenging. The experience of “event-based rumination” has been discussed in the realms of personal events [10,157], socio-political instabilities [9,158], and the collective experiences of natural disasters and pandemics [3,159].
4. The Experience of Rumination in the 21st Century
The increasing reliance on digital technologies today may offer a new avenue that further promotes rumination. The abundant flow of largely unfiltered and externally organized online information from the Internet into individual awareness can not only increase one’s cognitive load but also increase the possibility of receiving highly triggering salient information [19,160,161,162,163,164], both of which can contribute to the activation and maintenance of ruminative thoughts.
While smartphone use may first appear to be a coping strategy in distracting one from negative real-life experiences [165], studies have shown that increased dependence on the Internet and smartphones is in fact associated with alterations in neurobiological structures and cognitive deficits, as well as poorer mental health [161,164,166]. The use of digital devices for “escaping” from negative affective states could also increase the risks for attentional biases (e.g., searching for more negative contents, bias toward negatively valenced content online), which may further promote ruminative thoughts. Indeed, exposure to some online information, such as crime scenes, accidents, and conflicts and public health crises such as COVID-19, have been reported to increase not only depressive mood but also anger and fear [167,168,169]. The link between Internet and smartphone use and repetitive thoughts has been reported [170,171,172]. The continuous looping and passive intake of online information on smartphones in fact also show resemblance to the difficulties in breaking away from locked cycles of thoughts and behaviors in rumination. The fear of online surveillance and other related self-referential and delusional thoughts have also been reported in several studies [117,173,174], which can possibly trigger rumination in those with higher paranoid affect.
From the perspective of the FMR, the reliance on smartphone technologies today acts as an external mechanism that not only prolongs the exposure and effects of one-off external stressors but also reduces one’s intentionality in one’s behaviors, reinforces one’s affective states and memory of the past event, and depletes one’s cognitive resources, thereby altogether increasing the stagnation in the flow of thoughts.
As discussed, the narrowing of research focus towards depressive rumination took off in the 1990s before the advent of smartphones, which have critically transformed human interactions with social and digital environments [19,175]. Re-conceptualizing rumination in the age of digitalization by taking into account the extensive role of digital information in everyday experiences is required.
5. Opportunities for Intervention: Current Work and Future Directions
Various interventions have been designed for depressive rumination. For instance, rumination-focused cognitive behavioral therapy (RFCBT) has been noted to be effective in improving depressive rumination as well as mood and anxiety disorders [176,177,178]. Elements of behavioral activation, including the identification of how and when rumination occurs, the potential triggers of rumination, its possible function, behavioral experiments (e.g., limiting future exposure and practicing alternative habits in response to such cues), and the devising of specific plans to remove or replace the ruminative thoughts, have been identified to facilitate intervention outcomes [34]. In addition, mindfulness-based cognitive therapies (MBCTs) have also been used to reduce rigid repetitive thinking [179,180], aiming to disengage and redirect individuals’ attention from automatic ruminative content to their stream of conscious bodily experiences [181,182]. It has also been noted that supplementing attentional training with CBT can further enhance cognitive flexibility [183], which may be useful for reducing rumination.
With relevance to the FMR, interventions may be designed to interrupt the stagnation in thoughts with consideration of each of the following four components: intention (I), memory (M), affect (A), and external events (E). Elements integral to RFCBT and MBCT may be utilized, given that such approaches can help redirect one’s attention from originally fixated thoughts. Other studies have shown that cognitive-based treatments targeting attentional bias, reasoning, and interpretation, as well as cognitive remediation, are effective in reducing rumination [184] and not only depressive or anxiety but also psychotic symptoms [185,186]. Improving cognitive flexibility and attentional control may also help reduce “jumping-to-conclusion” tendencies (as in psychotic disorders) and emotional reactivity to stress [187,188], which may lessen both the activation and impact of negative affective states (e.g., low mood, anger, paranoia) and prior beliefs in the working memory [7]. Engagement in creativity, distraction tasks, and exercise are some techniques that may help improve attentional scope [189,190]. Recently, ecological momentary intervention, facilitated by smartphones, has offered promising directions in tackling patterns of ruminative thoughts in the everyday realm by supporting individuals in locating sources of distress and offering restorative tasks as distractions [191]. This may also be particularly useful as a prompt to reduce smartphone use and facilitate engagement in other behaviors to reduce rumination. The incorporation of the aforementioned elements in this novel intervention mode should be considered in future work.
Given the differential capacity in emotional and cognitive processing across the age span, it could be expected that the factors that determine the degree of thought stagnation would considerably differ between young people and older adults. While several studies have found rumination to be less frequent among those of older age [192,193,194], further studies would be required to examine the specific mechanisms underlying rumination in this age group in greater depth, wherein different intervention modalities may be required. The present FMR, which takes external events, intentional activation, affect, and memory into account, may be adopted as a guide in such future studies.
6. Conclusions
The current review re-examined ruminative constructs in relation to phenomenological experiences of associative thinking and streams of consciousness across psychiatric conditions. Moving away from compartmentalized approaches to understanding rumination as a form of self-focused cognition, the integrative Flow Model of Rumination bridges the influences of internal and external processes on rumination and accommodates a broad range of content and psychiatric conditions, thereby facilitating its application beyond depressive disorders as in the previous literature.
Notably, the experience of rumination has understandably evolved in an unprecedented manner in the age of digitalization and global crises, which call for timely revisions to the conceptualization and understanding of the phenomenon. The ongoing global socio-political instabilities, as well as the rapid developments of digitalization and the emerging age of artificial intelligence, require individuals to continuously adjust to new modes of living, which has considerable impacts on cognition. Ultimately, rumination reflects a higher-level experience representing a disruption to the flow of thoughts. By recognizing the complexity underlying rumination and its related phenomena, a comprehensive framework such as the Flow Model of Rumination could help lay the foundation for future research and practice. Identifying individuals at risk of rumination not limited to depressive thought contents may also contribute to future developments of more holistic and efficacious targeted interventions.
Author Contributions
E.Y.H.C., S.M.Y.W., and M.C.Y.L. conceived the idea of the model and drafted the first version of the manuscript. M.C.Y.L. and S.M.Y.W. reviewed the literature. Later versions of the manuscript were prepared by S.M.Y.W. and E.Y.H.C., with further review done by M.C.Y.L., Y.N.S., and C.L.M.H. All authors have read and approved the final version of the manuscript.
Funding
Not applicable.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Smith, J.M.; Alloy, L.B. A roadmap to rumination: A review of the definition, assessment, and conceptualization of this multifaceted construct. Clin. Psychol. Rev. 2009, 29, 116–128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freud, S. Remembering, repeating and working-through. Stand. Ed. 1914, 13, 147–156. [Google Scholar]
- Nolen-Hoeksema, S. Responses to depression and their effects on the duration of depressive episodes. J. Abnorm. Psychol. 1991, 100, 569–582. [Google Scholar] [CrossRef]
- Nolen-Hoeksema, S.; Wisco, B.E.; Lyubomirsky, S. Rethinking rumination. Perspect. Psychol. Sci. 2008, 3, 400–424. [Google Scholar] [CrossRef] [PubMed]
- Lyubomirsky, S.; Nolen-Hoeksema, S. Self-perpetuating properties of dysphoric rumination. J. Personal. Soc. Psychol. 1993, 65, 339–349. [Google Scholar] [CrossRef]
- Joormann, J.; Tanovic, E. Cognitive vulnerability to depression: Examining cognitive control and emotion regulation. Curr. Opin. Psychol. 2015, 4, 86–92. [Google Scholar] [CrossRef]
- Whitmer, A.J.; Gotlib, I.H. An attentional scope model of rumination. Psychol. Bull. 2013, 139, 1036–1061. [Google Scholar] [CrossRef] [Green Version]
- Nolen-Hoeksema, S.; Morrow, J. A prospective study of depression and posttraumatic stress symptoms after a natural disaster: The 1989 Loma Prieta Earthquake. J. Personal. Soc. Psychol. 1991, 61, 115–121. [Google Scholar] [CrossRef]
- Wong, S.M.Y.; Hui, C.L.M.; Wong, C.S.M.; Suen, Y.N.; Chan, S.K.W.; Lee, E.H.M.; Chang, W.C.; Chen, E.Y.H. Mental Health Risks after Repeated Exposure to Multiple Stressful Events during Ongoing Social Unrest and Pandemic in Hong Kong: The Role of Rumination: Risques pour la santé mentale après une exposition répétée à de multiples événements stressants d’agitation sociale durable et de pandémie à Hong Kong: Le rôle de la rumination. Can. J. Psychiatry 2021, 66, 577–585. [Google Scholar]
- Denson, T.F.; Pedersen, W.C.; Ronquillo, J.; Nandy, A.S. The angry brain: Neural correlates of anger, angry rumination, and aggressive personality. J. Cogn. Neurosci. 2009, 21, 734–744. [Google Scholar] [CrossRef]
- Johnson, S.L.; McKenzie, G.; McMurrich, S. Ruminative Responses to Negative and Positive Affect Among Students Diagnosed with Bipolar Disorder and Major Depressive Disorder. Cogn. Ther. Res. 2008, 32, 702–713. [Google Scholar] [CrossRef] [Green Version]
- Snyder, H.R.; Friedman, N.P.; Hankin, B.L. Transdiagnostic mechanisms of psychopathology in youth: Executive functions, dependent stress, and rumination. Cogn. Ther. Res. 2019, 43, 834–851. [Google Scholar] [CrossRef]
- Grierson, A.; Hickie, I.; Naismith, S.; Scott, J. The role of rumination in illness trajectories in youth: Linking trans-diagnostic processes with clinical staging models. Psychol. Med. 2016, 46, 2467–2484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, K.J.; Beard, C.; Rifkin, L.; Dillon, D.G.; Pizzagalli, D.A.; Björgvinsson, T. Transdiagnostic mechanisms in depression and anxiety: The role of rumination and attentional control. J. Affect. Disord. 2015, 188, 22–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Júnior, É.D.M.S.; Passos, I.C.; Scott, J.; Bristot, G.; Scotton, E.; Mendes, L.S.T.; Knackfuss, A.C.U.; Gerchmann, L.; Fijtman, A.; Trasel, A.R.; et al. Decoding rumination: A machine learning approach to a transdiagnostic sample of outpatients with anxiety, mood and psychotic disorders. J. Psychiatr. Res. 2020, 121, 207–213. [Google Scholar]
- Chen, E.Y.H.; Wong, S.M.Y. Youth mental health care in a context of large-scale collective stress. World Psychiatry 2022, 21, 85–86. [Google Scholar] [CrossRef]
- Elhai, J.D.; Yang, H.; Dempsey, A.E.; Montag, C. Rumination and negative smartphone use expectancies are associated with greater levels of problematic smartphone use: A latent class analysis. Psychiatry Res. 2020, 285, 112845. [Google Scholar] [CrossRef]
- Hou, W.K.; Lee TM, C.; Liang, L.; Li, T.W.; Liu, H.; Ettman, C.K.; Galea, S. Civil unrest, COVID-19 stressors, anxiety, and depression in the acute phase of the pandemic: A population-based study in Hong Kong. Soc. Psychiatry Psychiatr. Epidemiol. 2021, 56, 1499–1508. [Google Scholar] [CrossRef]
- Zsido, A.N.; Arato, N.; Lang, A.; Labadi, B.; Stecina, D.; Bandi, S.A. The role of maladaptive cognitive emotion regulation strategies and social anxiety in problematic smartphone and social media use. Personal. Individ. Differ. 2021, 173, 110647. [Google Scholar] [CrossRef]
- Stout, G.F. A Manual of Psychology; Hinds & Noble: New York, NY, USA, 1899. [Google Scholar]
- Buckingham, H.W.; Finger, S. David Hartley’s psychobiological associationism and the legacy of Aristotle. J. Hist. Neurosci. 1997, 6, 21–37. [Google Scholar] [CrossRef]
- Hobbes, T. Leviathan; Tuck, R., Ed.; Cambridge University Press: Singapore, 1651. [Google Scholar]
- Locke, J. An Essay Concerning Human Understanding; Woolhouse, R., Ed.; Penguin: London, UK, 1689. [Google Scholar]
- Hume, D. Enquiries Concerning Human Understanding and Concerning the Principles of Morals; Selby-Bigge, L.A., Ed.; Clarendon Press: Oxford, UK, 1748. [Google Scholar]
- James, W. Principles of Psychology; Project Gutenberg: Salt Lake City, UT, USA, 1890; Volume 1. [Google Scholar]
- Mason, M.F.; Bar, M. The effect of mental progression on mood. J. Exp. Psychol. Gen. 2012, 141, 217–221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christoff, K. Undirected thought: Neural determinants and correlates. Brain Res. 2012, 1428, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Sripada, C.; Taxali, A. Structure in the stream of consciousness: Evidence from a verbalized thought protocol and automated text analytic methods. Conscious. Cogn. 2020, 85, 103007. [Google Scholar] [CrossRef] [PubMed]
- Esquiro, J.E.D. Des Maladies Mentales Considérées sous les Rapports Médical, Hygiénique et Médico-Légal (Mental Illnesses Considered from Medical, Hygienic, and Medico-Legal Aspects); Baillière; Nabu Press: New York, NY, USA, 1838. [Google Scholar]
- Berrios, G.E. Obsessive-compulsive disorder: Its conceptual history in France during the 19th century. Compr. Psychiatry 1989, 30, 283–295. [Google Scholar] [CrossRef]
- Koenig-Robert, R.; Pearson, J. Why do imagery and perception look and feel so different? Philos. Trans. Biol. Sci. 2021, 376, 20190703. [Google Scholar] [CrossRef]
- Treynor, W.; Gonzalez, R.; Nolen-Hoeksema, S. Rumination reconsidered: A psychometric analysis. Cogn. Ther. Res. 2003, 27, 247–259. [Google Scholar] [CrossRef] [Green Version]
- Conway, M.; Csank, P.A.; Holm, S.L.; Blake, C.K. On assessing individual differences in rumination on sadness. J. Personal. Assess. 2000, 75, 404–425. [Google Scholar] [CrossRef]
- Watkins, E.R.; Roberts, H. Reflecting on rumination: Consequences, causes, mechanisms and treatment of rumination. Behav. Res. Ther. 2020, 127, 103573. [Google Scholar] [CrossRef]
- Martin, L.L.; Tesser, A. Toward a motivational and structural theory of ruminative thought. In Unintended Thought; Uleman, J.S., Bargh, J.A., Eds.; The Guilford Press: New York, NY, USA, 1989; pp. 306–326. [Google Scholar]
- Alloy, L.B.; Abramson, L.Y.; Hogan, M.E.; Whitehouse, W.G.; Rose, D.T.; Robinson, M.S.; Kim, R.S.; Lapkin, J.B. The Temple-Wisconsin Cognitive Vulnerability to Depression Project: Lifetime history of Axis I psychopathology in individuals at high and low cognitive risk for depression. J. Abnorm. Psychol. 2000, 109, 403–418. [Google Scholar] [CrossRef]
- Rachman, S.; Grüter-Andrew, J.; Shafran, R. Post-event processing in social anxiety. Behav. Res. Ther. 2000, 38, 611–617. [Google Scholar] [CrossRef]
- Connolly, S.L.; Alloy, L.B. Rumination interacts with life stress to predict depressive symptoms: An ecological momentary assessment study. Behav. Res. Ther. 2017, 97, 86–95. [Google Scholar] [CrossRef]
- Robinson, M.S.; Alloy, L.B. Negative cognitive styles and stress-reactive rumination interact to predict depression: A prospective study. Cogn. Ther. Res. 2003, 27, 275–291. [Google Scholar] [CrossRef]
- Clark, D.M.; Wells, A. A cognitive model of social phobia. In Social Phobia: Diagnosis, Assessment, and Treatment; Heimberg, R.G., Liebowitz, M.R., Hope, D.A., Schneier, F.R., Eds.; Guilford Press: New York, NY, USA, 1995; pp. 69–91. [Google Scholar]
- Williams, J.M.G. Capture and rumination, functional avoidance, and executive control (CaRFAX): Three processes that underlie overgeneral memory. Cogn. Emot. 2006, 20, 548–568. [Google Scholar] [CrossRef]
- Bendala-Rodríguez, P.; Senín-Calderón, C.; Peluso-Crespi, L.; Rodríguez-Testal, J.F. Vulnerability to Psychosis, Ideas of Reference and Evaluation with an Implicit Test. J. Clin. Med. Res. 2019, 8, 1956. [Google Scholar] [CrossRef] [Green Version]
- Bendall, S.; Lim, M.H.; Alvarez-Jimenez, M.; Hulbert, C.A.; McGorry, P.D.; Jackson, H.J. Selective Attention to Threat is Specific to Delusions in First-Episode Psychosis. J. Exp. Psychopathol. 2014, 5, 191–199. [Google Scholar] [CrossRef] [Green Version]
- Reininghaus, U.; Kempton, M.J.; Valmaggia, L.; Craig, T.K.J.; Garety, P.; Onyejiaka, A.; Gayer-Anderson, C.; So, S.H.; Hubbard, K.; Beards, S.; et al. Stress Sensitivity, Aberrant Salience, and Threat Anticipation in Early Psychosis: An Experience Sampling Study. Schizophr. Bull. 2016, 42, 712–722. [Google Scholar] [CrossRef] [Green Version]
- Underwood, R.; Kumari, V.; Peters, E. Cognitive and neural models of threat appraisal in psychosis: A theoretical integration. Psychiatry Res. 2016, 239, 131–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bomyea, J.; Johnson, A.; Lang, A.J. Information Processing in PTSD: Evidence for Biased Attentional, Interpretation, and Memory Processes. Psychopathol. Rev. 2017, a4, 218–243. [Google Scholar] [CrossRef] [Green Version]
- Olatunji, B.O.; Naragon-Gainey, K.; Wolitzky-Taylor, K.B. Specificity of rumination in anxiety and depression: A multimodal meta-analysis. Clin. Psychol. Sci. Pract. 2013, 20, 225–257. [Google Scholar]
- Powers, A.; Fani, N.; Murphy, L.; Briscione, M.; Bradley, B.; Tone, E.B.; Norrholm, S.D.; Jovanovic, T. Attention bias toward threatening faces in women with PTSD: Eye tracking correlates by symptom cluster. Eur. J. Psychotraumatology 2019, 10, 1568133. [Google Scholar] [CrossRef] [Green Version]
- Fisk, J.; Ellis, J.A.; Reynolds, S.A. A test of the CaR-FA-X mechanisms and depression in adolescents. Memory 2019, 27, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Sumner, J.A.; Mineka, S.; Adam, E.K.; Craske, M.G.; Vrshek-Schallhorn, S.; Wolitzky-Taylor, K.; Zinbarg, R.E. Testing the CaR-FA-X model: Investigating the mechanisms underlying reduced autobiographical memory specificity in individuals with and without a history of depression. J. Abnorm. Psychol. 2014, 123, 471–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamlat, E.J.; Connolly, S.L.; Hamilton, J.L.; Stange, J.P.; Abramson, L.Y.; Alloy, L.B. Rumination and overgeneral autobiographical memory in adolescents: An integration of cognitive vulnerabilities to depression. J. Youth Adolesc. 2015, 44, 806–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobsen, P.; Peters, E.; Ward, T.; Garety, P.A.; Jackson, M.; Chadwick, P. Overgeneral autobiographical memory bias in clinical and non-clinical voice hearers. Psychol. Med. 2019, 49, 113–120. [Google Scholar] [CrossRef]
- Moore, S.A.; Zoellner, L.A. Overgeneral autobiographical memory and traumatic events: An evaluative review. Psychol. Bull. 2007, 133, 419–437. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Kuhn, S.K.; Jobson, L.; Haque, S. A review of autobiographical memory studies on patients with schizophrenia spectrum disorders. BMC Psychiatry 2019, 19, 361. [Google Scholar] [CrossRef] [Green Version]
- Christoff, K.; Irving, Z.C.; Fox, K.C.; Spreng, R.N.; Andrews-Hanna, J.R. Mind-wandering as spontaneous thought: A dynamic framework. Nat. Rev. Neurosci. 2016, 17, 718–731. [Google Scholar] [CrossRef]
- Dorsch, F. Focused daydreaming and mind-wandering. Rev. Philos. Psychol. 2015, 6, 791–813. [Google Scholar] [CrossRef]
- Marchetti, I.; Koster, E.H.; Klinger, E.; Alloy, L.B. Spontaneous thought and vulnerability to mood disorders: The dark side of the wandering mind. Clin. Psychol. Sci. 2016, 4, 835–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrews-Hanna, J.R.; Smallwood, J.; Spreng, R.N. The default network and self-generated thought: Component processes, dynamic control, and clinical relevance. Ann. N. Y. Acad. Sci. 2014, 1316, 29–52. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, J.P.; Farmer, M.; Fogelman, P.; Gotlib, I.H. Depressive rumination, the default-mode network, and the dark matter of clinical neuroscience. Biol. Psychiatry 2015, 78, 224–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Ezzi, A.; Kamel, N.; Faye, I.; Gunaseli, E. Analysis of Default Mode Network in Social Anxiety Disorder: EEG Resting-State Effective Connectivity Study. Sensors 2021, 21, 4098. [Google Scholar] [CrossRef] [PubMed]
- Doucet, G.E.; Janiri, D.; Howard, R.; O’Brien, M.; Andrews-Hanna, J.R.; Frangou, S. Transdiagnostic and disease-specific abnormalities in the default-mode network hubs in psychiatric disorders: A meta-analysis of resting-state functional imaging studies. Eur. Psychiatry 2020, 63, e57. [Google Scholar] [CrossRef] [PubMed]
- Hilland, E.; Johannessen, C.; Jonassen, R.; Alnæs, D.; Jørgensen, K.N.; Barth, C.; Andreou, D.; Nerland, S.; Wortinger, L.A.; Smelror, R.E.; et al. Aberrant default mode connectivity in adolescents with early-onset psychosis: A resting state fMRI study. NeuroImage Clin. 2022, 33, 102881. [Google Scholar] [CrossRef]
- Viard, A.; Mutlu, J.; Chanraud, S.; Guenolé, F.; Egler, P.-J.; Gérardin, P.; Baleyte, J.-M.; Dayan, J.; Eustache, F.; Guillery-Girard, B. Altered default mode network connectivity in adolescents with post-traumatic stress disorder. NeuroImage Clin. 2019, 22, 101731. [Google Scholar] [CrossRef] [PubMed]
- Ehring, T. Thinking too much: Rumination and psychopathology. World Psychiatry 2021, 20, 441–442. [Google Scholar] [CrossRef] [PubMed]
- Michl, L.C.; McLaughlin, K.A.; Shepherd, K.; Nolen-Hoeksema, S. Rumination as a mechanism linking stressful life events to symptoms of depression and anxiety: Longitudinal evidence in early adolescents and adults. J. Abnorm. Psychol. 2013, 122, 339–352. [Google Scholar] [CrossRef] [Green Version]
- Ruscio, A.M.; Gentes, E.L.; Jones, J.D.; Hallion, L.S.; Coleman, E.S.; Swendsen, J. Rumination predicts heightened responding to stressful life events in major depressive disorder and generalized anxiety disorder. J. Abnorm. Psychol. 2015, 124, 17–26. [Google Scholar] [CrossRef] [Green Version]
- Kovács, L.N.; Takacs, Z.K.; Tóth, Z.; Simon, E.; Schmelowszky, Á.; Kökönyei, G. Rumination in major depressive and bipolar disorder—A meta-analysis. J. Affect. Disord. 2020, 276, 1131–1141. [Google Scholar] [CrossRef]
- Ludwig, L.; Werner, D.; Lincoln, T.M. The relevance of cognitive emotion regulation to psychotic symptoms—A systematic review and meta-analysis. Clin. Psychol. Rev. 2019, 72, 101746. [Google Scholar] [CrossRef]
- Michael, T.; Halligan, S.L.; Clark, D.M.; Ehlers, A. Rumination in posttraumatic stress disorder. Depress. Anxiety 2007, 24, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Wahl, K.; van den Hout, M.; Heinzel, C.V.; Kollárik, M.; Meyer, A.; Benoy, C.; Berberich, G.; Domschke, K.; Gloster, A.; Gradwohl, G.; et al. Rumination about obsessive symptoms and mood maintains obsessive-compulsive symptoms and depressed mood: An experimental study. J. Abnorm. Psychol. 2021, 130, 435–442. [Google Scholar] [CrossRef] [PubMed]
- Calkins, A.W.; Berman, N.C.; Wilhelm, S. Recent advances in research on cognition and emotion in OCD: A review. Curr. Psychiatry Rep. 2013, 15, 357. [Google Scholar] [CrossRef]
- Shin, N.Y.; Lee, T.Y.; Kim, E.; Kwon, J.S. Cognitive functioning in obsessive-compulsive disorder: A meta-analysis. Psychol. Med. 2014, 44, 1121–1130. [Google Scholar] [CrossRef]
- Makovac, E.; Fagioli, S.; Rae, C.L.; Critchley, H.D.; Ottaviani, C. Can’t get it off my brain: Meta-analysis of neuroimaging studies on perseverative cognition. Psychiatry Res. Neuroimaging 2020, 295, 111020. [Google Scholar] [CrossRef]
- de Oliveira, K.C.; Grinberg, L.T.; Hoexter, M.Q.; Brentani, H.; Suemoto, C.K.; Nery, F.G.; Lima, L.C.; Alho, A.T.D.L.; Farfel, J.M.; Ferretti-Rebustini, R.E.D.L.; et al. Layer-specific reduced neuronal density in the orbitofrontal cortex of older adults with obsessive-compulsive disorder. Brain Struct. Funct. 2019, 224, 191–203. [Google Scholar] [CrossRef]
- Maia, T.V.; Cooney, R.E.; Peterson, B.S. The neural bases of obsessive-compulsive disorder in children and adults. Dev. Psychopathol. 2008, 20, 1251. [Google Scholar] [CrossRef] [Green Version]
- Posner, J.; Marsh, R.; Maia, T.V.; Peterson, B.S.; Gruber, A.; Simpson, H.B. Reduced functional connectivity within the limbic cortico-striato-thalamo-cortical loop in unmedicated adults with obsessive-compulsive disorder. Hum. Brain Mapp. 2014, 35, 2852–2860. [Google Scholar] [CrossRef] [Green Version]
- Konishi, S.; Chikazoe, J.; Jimura, K.; Asari, T.; Miyashita, Y. Neural mechanism in anterior prefrontal cortex for inhibition of prolonged set interference. Proc. Natl. Acad. Sci. USA 2005, 102, 12584–12588. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, A.; Clark, D.M. A cognitive model of posttraumatic stress disorder. Behav. Res. Ther. 2000, 38, 319–345. [Google Scholar] [CrossRef]
- Wong, S.M.Y.; Hui, C.L.M.; Suen, Y.N.; Wong, C.S.M.; Chan, S.K.W.; Lee, E.H.M.; Chang, W.C.; Chen, E.Y.H. The impact of social unrest and pandemic on mental health of young people in Hong Kong: The transdiagnostic role of event-based rumination. Aust. N. Z. J. Psychiatry 2021, 56, 376–384. [Google Scholar] [CrossRef]
- Wong, S.M.Y.; Hui, C.L.M.; Wong, C.S.M.; Suen, Y.N.; Chan, S.K.W.; Lee, E.H.M.; Chang, W.C.; Chen, E.Y.H. Prospective prediction of PTSD and depressive symptoms during social unrest and COVID-19 using a brief online tool. Psychiatry Res. 2021, 298, 113773. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.M.Y.; Hui, C.L.M.; Wong, C.S.M.; Suen, Y.N.; Chan, S.K.W.; Lee, E.H.M.; Chang, W.C.; Wong, G.H.Y.; Chen, E.Y.H. Induced ideas of reference during social unrest and pandemic in Hong Kong. Schizophr. Res. 2021, 229, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zhou, X.; Wu, Y.; An, Y. The role of rumination in posttraumatic stress disorder and posttraumatic growth among adolescents after the wenchuan earthquake. Front. Psychol. 2015, 6, 1335. [Google Scholar] [CrossRef] [Green Version]
- Horwitz, A.G.; Czyz, E.K.; Berona, J.; King, C.A. Rumination, brooding, and reflection: Prospective associations with suicide ideation and suicide attempts. Suicide Life-Threat. Behav. 2019, 49, 1085–1093. [Google Scholar] [CrossRef]
- Miranda, R.; Nolen-Hoeksema, S. Brooding and reflection: Rumination predicts suicidal ideation at 1-year follow-up in a community sample. Behav. Res. Ther. 2007, 45, 3088–3095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, S.M.Y.; Ip, C.H.; Hui, C.L.M.; Suen, Y.N.; Wong, C.S.M.; Chang, W.C.; Chan, S.K.W.; Lee, E.H.M.; Lui, S.S.Y.; Chan, K.T.; et al. Prevalence and correlates of suicidal behaviours in a representative epidemiological youth sample in Hong Kong: The significance of suicide-related rumination, family functioning, and ongoing population-level stressors. Psychol. Med. 2022, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Mortier, P.; Kiekens, G.; Auerbach, R.P.; Cuijpers, P.; Demyttenaere, K.; Green, J.G.; Kessler, R.C.; Nock, M.K.; Zaslavsky, A.M.; Bruffaerts, R. A risk algorithm for the persistence of suicidal thoughts and behaviors during college. J. Clin. Psychiatry 2017, 78, e828–e836. [Google Scholar] [CrossRef] [Green Version]
- Nock, M.K.; Millner, A.J.; Joiner, T.E.; Gutierrez, P.M.; Han, G.; Hwang, I.; King, A.; Naifeh, J.A.; Sampson, N.A.; Zaslavsky, A.M.; et al. Risk factors for the transition from suicide ideation to suicide attempt: Results from the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS). J. Abnorm. Psychol. 2018, 127, 139–149. [Google Scholar] [CrossRef] [Green Version]
- Rogers, M.L.; Joiner, T.E. Suicide-specific rumination relates to lifetime suicide attempts above and beyond a variety of other suicide risk factors. J. Psychiatr. Res. 2018, 98, 78–86. [Google Scholar] [CrossRef]
- Rogers, M.L.; Law, K.C.; Houtsma, C.; Tucker, R.P.; Anestis, M.D.; Joiner, T.E. Development and initial validation of a scale assessing suicide-specific rumination: The suicide rumination scale. Assessment 2022, 29, 1777–1794. [Google Scholar] [CrossRef]
- Ceaser, A.E.; Goldberg, T.E.; Egan, M.F.; McMahon, R.P.; Weinberger, D.R.; Gold, J.M. Set-shifting ability and schizophrenia: A marker of clinical illness or an intermediate phenotype? Biol. Psychiatry 2008, 64, 782–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crider, A. Perseveration in schizophrenia. Schizophr. Bull. 1997, 23, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Sandson, J.; Albert, M.L. Varieties of perseveration. Neuropsychologia 1984, 22, 715–732. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, E. Varieties of perseveration: A comparison of two taxonomies. J. Clin. Exp. Neuropsychol. 1986, 8, 710–726. [Google Scholar] [CrossRef]
- Ehring, T.; Zetsche, U.; Weidacker, K.; Wahl, K.; Schönfeld, S.; Ehlers, A. The Perseverative Thinking Questionnaire (PTQ): Validation of a content-independent measure of repetitive negative thinking. J. Behav. Ther. Exp. Psychiatry 2011, 42, 225–232. [Google Scholar] [CrossRef] [Green Version]
- Černis, E.; Dunn, G.; Startup, H.; Kingdon, D.; Wingham, G.; Evans, N.; Lister, R.; Pugh, K.; Cordwell, J.; Mander, H.; et al. The Perseverative Thinking Questionnaire in Patients with Persecutory Delusions. Behav. Cogn. Psychother. 2016, 44, 472–481. [Google Scholar] [CrossRef]
- Hartley, S.; Haddock, G.; e Sa, D.V.; Emsley, R.; Barrowclough, C. An experience sampling study of worry and rumination in psychosis. Psychol. Med. 2014, 44, 1605–1614. [Google Scholar] [CrossRef]
- Lebert, L.; Turkington, D.; Freeston, M.; Dudley, R. Rumination, intolerance of uncertainty and paranoia in treatment resistant psychosis. Psychosis 2021, 13, 65–70. [Google Scholar] [CrossRef]
- Peters, E.R.; Joseph, S.A.; Garety, P.A. Measurement of delusional ideation in the normal population: Introducing the PDI (Peters et al. Delusions Inventory). Schizophr. Bull. 1999, 25, 553–576. [Google Scholar] [CrossRef] [Green Version]
- Ricarte, J.J.; Ros, L.; Fernández, D.; Nieto, M.; Latorre, J.M. Effects of analytical (abstract) versus experiential (concrete) induced rumination of negative self defining memories on schizotypic symptoms. Scand. J. Psychol. 2018, 59, 553–559. [Google Scholar] [CrossRef]
- Sisti, D.; Rocchi, M.B.; Siddi, S.; Mura, T.; Manca, S.; Preti, A.; Petretto, D.R. Preoccupation and distress are relevant dimensions in delusional beliefs. Compr. Psychiatry 2012, 53, 1039–1043. [Google Scholar] [CrossRef]
- Jones, S.R.; Fernyhough, C. Rumination, reflection, intrusive thoughts, and hallucination-proneness: Towards a new model. Behav. Res. Ther. 2009, 47, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Lam, A.H.Y.; Cheung, Y.T.D.; Wong, K.H.; Leung, S.F.; Chien, W.T. Dispositional Mindfulness and Psychotic Symptoms in Schizophrenia Spectrum Disorders: The Mediating Roles of Rumination and Negative Emotion. Neuropsychiatr. Dis. Treat. 2022, 18, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Kang, N.I.; Lee, K.H.; Piao, Y.; Cui, Y.; Kim, S.W.; Lee, B.J.; Kim, J.J.; Yu, J.C.; Lee, K.Y.; et al. Effects of antipsychotics on rumination in patients with first-episode psychosis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2020, 103, 109983. [Google Scholar] [CrossRef] [PubMed]
- Halari, R.; Premkumar, P.; Farquharson, L.; Fannon, D.; Kuipers, E.; Kumari, V. Rumination and negative symptoms in schizophrenia. J. Nerv. Ment. Dis. 2009, 197, 703–706. [Google Scholar] [CrossRef]
- Thomas, N.; Ribaux, D.; Phillips, L.J. Rumination, depressive symptoms and awareness of illness in schizophrenia. Behav. Cogn. Psychother. 2014, 42, 143–155. [Google Scholar] [CrossRef]
- Csikszentmihalyi, M. Beyond Boredom and Anxiety; Jossey-Bass Publishers: Francisco, CA, USA, 1975. [Google Scholar]
- Klinger, E.; Cox, W.M. Dimensions of thought flow in everyday life. Imagin. Cogn. Personal. 1987, 7, 105–128. [Google Scholar] [CrossRef]
- Vago, D.R.; Zeidan, F. The brain on silent: Mind wandering, mindful awareness, and states of mental tranquility. Ann. N. Y. Acad. Sci. 2016, 1373, 96–113. [Google Scholar] [CrossRef] [Green Version]
- Watkins, E.D.; Moulds, M. Distinct modes of ruminative self-focus: Impact of abstract versus concrete rumination on problem solving in depression. Emotion 2005, 5, 319–328. [Google Scholar] [CrossRef]
- Watkins, E.R.; Nolen-Hoeksema, S. A habit-goal framework of depressive rumination. J. Abnorm. Psychol. 2014, 123, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Kalyuga, S.; Renkl, A.; Paas, F. Facilitating flexible problem solving: A cognitive load perspective. Educ. Psychol. Rev. 2010, 22, 175–186. [Google Scholar] [CrossRef] [Green Version]
- Kontaxopoulou, D.; Beratis, I.N.; Fragkiadaki, S.; Pavlou, D.; Yannis, G.; Economou, A.; Papanicolaou, A.C.; Papageorgiou, S.G. Incidental and Intentional Memory: Their Relation with Attention and Executive Functions. Arch. Clin. Neuropsychol. Off. J. Natl. Acad. Neuropsychol. 2017, 32, 519–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, J.P.; Furman, D.J.; Chang, C.; Thomason, M.E.; Dennis, E.; Gotlib, I.H. Default-mode and task-positive network activity in major depressive disorder: Implications for adaptive and maladaptive rumination. Biol. Psychiatry 2011, 70, 327–333. [Google Scholar] [CrossRef] [Green Version]
- Waters FA, V.; Badcock, J.C.; Maybery, M.T. Selective attention for negative information and depression in schizophrenia. Psychol. Med. 2006, 36, 455–464. [Google Scholar] [CrossRef]
- Friedman, R.S.; Förster, J. Implicit affective cues and attentional tuning: An integrative review. Psychol. Bull. 2010, 136, 875–893. [Google Scholar] [CrossRef] [Green Version]
- Gable, P.A.; Harmon-Jones, E. Reducing attentional capture of emotion by broadening attention: Increased global attention reduces early electrophysiological responses to negative stimuli. Biol. Psychol. 2012, 90, 150–153. [Google Scholar] [CrossRef]
- Mason, O.J.; Stevenson, C.; Freedman, F. Ever-present threats from information technology: The Cyber-Paranoia and Fear Scale. Front. Psychol. 2014, 5, 1298. [Google Scholar] [CrossRef] [Green Version]
- Vasquez, E.A.; Pedersen, W.C.; Bushman, B.J.; Kelley, N.J.; Demeestere, P.; Miller, N. Lashing out after stewing over public insults: The effects of public provocation, provocation intensity, and rumination on triggered displaced aggression. Aggress. Behav. 2013, 39, 13–29. [Google Scholar] [CrossRef]
- McHugh, T.; Forbes, D.; Bates, G.; Hopwood, M.; Creamer, M. Anger in PTSD: Is there a need for a concept of PTSD-related posttraumatic anger? Clin. Psychol. Rev. 2012, 32, 93–104. [Google Scholar] [CrossRef]
- Baer, R.A.; Sauer, S.E. Relationships between depressive rumination, anger rumination, and borderline personality features. Personal. Disord. 2011, 2, 142–150. [Google Scholar] [CrossRef] [Green Version]
- du Pont, A.; Rhee, S.H.; Corley, R.P.; Hewitt, J.K.; Friedman, N.P. Are rumination and neuroticism genetically or environmentally distinct risk factors for psychopathology? J. Abnorm. Psychol. 2019, 128, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Peled, M.; Moretti, M.M. Ruminating on Rumination: Are Rumination on Anger and Sadness Differentially Related to Aggression and Depressed Mood? J. Psychopathol. Behav. Assess. 2010, 32, 108–117. [Google Scholar] [CrossRef]
- Feldman, G.C.; Joormann, J.; Johnson, S.L. Responses to Positive Affect: A Self-Report Measure of Rumination and Dampening. Cogn. Ther. Res. 2008, 32, 507–525. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, K.; Luking, K.; Pagliaccio, D.; Luby, J.; Barch, D. Dampening, Positive Rumination, and Positive Life Events: Associations with Depressive Symptoms in Children at Risk for Depression. Cogn. Ther. Res. 2017, 41, 31–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.I.; Starr, L.R.; Hershenberg, R. Responses to Positive Affect in Daily Life: Positive Rumination and Dampening Moderate the Association Between Daily Events and Depressive Symptoms. J. Psychopathol. Behav. Assess. 2017, 39, 412–425. [Google Scholar] [CrossRef]
- Danhauer, S.C.; Legault, C.; Bandos, H.; Kidwell, K.; Costantino, J.; Vaughan, L.; Avis, N.E.; Rapp, S.; Coker, L.H.; Naughton, M.; et al. Positive and negative affect, depression, and cognitive processes in the Cognition in the Study of Tamoxifen and Raloxifene (Co-STAR) Trial. Neuropsychol. Dev. Cogn. Sect. B Aging Neuropsychol. Cogn. 2013, 20, 532–552. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.; Li, H. Training Positive Rumination in Expressive Writing to Enhance Psychological Adjustment and Working Memory Updating for Maladaptive Ruminators. Front. Psychol. 2020, 11, 789. [Google Scholar] [CrossRef]
- Watkins, E.R. Constructive and unconstructive repetitive thought. Psychol. Bull. 2008, 134, 163. [Google Scholar] [CrossRef] [Green Version]
- Gruber, J.; Maclaine, E.; Avard, E.; Purcell, J.; Cooper, G.; Tobias, M.; Earls, H.; Wieland, L.; Bothe, E.; Boggio, P.; et al. Associations between hypomania proneness and attentional bias to happy, but not angry or fearful, faces in emerging adults. Cogn. Emot. 2021, 35, 207–213. [Google Scholar] [CrossRef]
- Liu, Y.H.; Liu, T.B.; Zhao, J.; Huang, S.W.; Lai, W.T.; Yang, H.C.; Xu, D.; Zhang, M.; Rong, H. A study on attentional bias and response inhibition of facial expressions in manic patients: Evidence from eye movement. Int. J. Psychiatry Clin. Pract. 2019, 23, 164–170. [Google Scholar] [CrossRef]
- Murphy, F.C.; Sahakian, B.J.; Rubinsztein, J.S.; Michael, A.; Rogers, R.D.; Robbins, T.W.; Paykel, E.S. Emotional bias and inhibitory control processes in mania and depression. Psychol. Med. 1999, 29, 1307–1321. [Google Scholar] [CrossRef]
- Peckham, A.D.; Johnson, S.L.; Gotlib, I.H. Attentional bias in euthymic bipolar I disorder. Cogn. Emot. 2016, 30, 472–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freeman, D.; Thompson, C.; Vorontsova, N.; Dunn, G.; Carter, L.-A.; Garety, P.; Kuipers, E.; Slater, M.; Antley, A.; Glucksman, E.; et al. Paranoia and post-traumatic stress disorder in the months after a physical assault: A longitudinal study examining shared and differential predictors. Psychol. Med. 2013, 43, 2673–2684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klippel, A.; Viechtbauer, W.; Reininghaus, U.; Wigman, J.; van Borkulo, C.; ESM-MERGE Investigators; Myin-Germeys, I.; Wichers, M. The Cascade of Stress: A Network Approach to Explore Differential Dynamics in Populations Varying in Risk for Psychosis. Schizophr. Bull. 2018, 44, 328–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moritz, S.; Laudan, A. Attention bias for paranoia-relevant visual stimuli in schizophrenia. Cogn. Neuropsychiatry 2007, 12, 381–390. [Google Scholar] [CrossRef]
- Navalón, P.; Perea, M.; Benavent, P.; Sierra, P.; Domínguez, A.; Iranzo, C.; Serrano-Lozano, E.; Almansa, B.; García-Blanco, A. Attentional processing biases to threat in schizophrenia: Evidence from a free-viewing task with emotional scenes. J. Psychiatr. Res. 2021, 144, 80–86. [Google Scholar] [CrossRef]
- Navalón, P.; Serrano, E.; Almansa, B.; Perea, M.; Benavent, P.; Domínguez, A.; Sierra, P.; Cañada, Y.; García-Blanco, A. Attentional biases to emotional scenes in schizophrenia: An eye-tracking study. Biol. Psychol. 2021, 160, 108045. [Google Scholar] [CrossRef]
- Waltz, J.A. The neural underpinnings of cognitive flexibility and their disruption in psychotic illness. Neuroscience 2017, 345, 203–217. [Google Scholar] [CrossRef] [Green Version]
- Wobrock, T.; Ecker UK, H.; Scherk, H.; Schneider-Axmann, T.; Falkai, P.; Gruber, O. Cognitive impairment of executive function as a core symptom of schizophrenia. World J. Biol. Psychiatry Off. J. World Fed. Soc. Biol. Psychiatry 2009, 10 Pt 2, 442–451. [Google Scholar] [CrossRef]
- Ricarte, J.J.; Ros, L.; Latorre, J.M.; Watkins, E. Mapping autobiographical memory in schizophrenia: Clinical implications. Clin. Psychol. Rev. 2017, 51, 96–108. [Google Scholar] [CrossRef] [PubMed]
- Berna, F.; Potheegadoo, J.; Aouadi, I.; Ricarte, J.J.; Allé, M.C.; Coutelle, R.; Boyer, L.; Cuervo-Lombard, C.V.; Danion, J.-M. A Meta-Analysis of Autobiographical Memory Studies in Schizophrenia Spectrum Disorder. Schizophr. Bull. 2016, 42, 56–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Januška, J.; Straková, A.; Dančík, D.; Pečeňák, J.; Heretik, A.; Hajdúk, M. The interplay among paranoia, social relationships and negative affectivity in a heterogeneous clinical sample: A network analysis. J. Exp. Psychopathol. 2021, 12, 20438087211067626. [Google Scholar] [CrossRef]
- Corlett, P.R.; Taylor, J.R.; Wang, X.-J.; Fletcher, P.C.; Krystal, J.H. Toward a neurobiology of delusions. Prog. Neurobiol. 2010, 92, 345–369. [Google Scholar] [CrossRef] [Green Version]
- Altmann, E.M.; Gray, W.D. Forgetting to remember: The functional relationship of decay and interference. Psychol. Sci. 2002, 13, 27–33. [Google Scholar] [CrossRef]
- Davis, R.L.; Zhong, Y. The biology of forgetting—A perspective. Neuron 2017, 95, 490–503. [Google Scholar] [CrossRef]
- Meiran, N.; Chorev, Z.; Sapir, A. Component processes in task switching. Cogn. Psychol. 2000, 41, 211–253. [Google Scholar] [CrossRef]
- Friedman, N.P.; Miyake, A. The relations among inhibition and interference control functions: A latent-variable analysis. J. Exp. Psychol. Gen. 2004, 133, 101. [Google Scholar] [CrossRef] [Green Version]
- Horowitz, M.J.; Becker, S.S.; Moskowitz, M.L. Intrusive and repetitive thought after stress: A replication study. Psychol. Rep. 1971, 29, 763–767. [Google Scholar] [CrossRef]
- Davis, R.N.; Nolen-Hoeksema, S. Cognitive inflexibility among ruminators and nonruminators. Cogn. Ther. Res. 2000, 24, 699–711. [Google Scholar] [CrossRef]
- Banich, M.T.; Mackiewicz, K.L.; Depue, B.E.; Whitmer, A.J.; Miller, G.A.; Heller, W. Cognitive control mechanisms, emotion and memory: A neural perspective with implications for psychopathology. Neurosci. Biobehav. Rev. 2009, 33, 613–630. [Google Scholar] [CrossRef] [Green Version]
- Rusting, C.L.; Nolen-Hoeksema, S. Regulating responses to anger: Effects of rumination and distraction on angry mood. J. Personal. Soc. Psychol. 1998, 74, 790–803. [Google Scholar] [CrossRef] [PubMed]
- Sukhodolsky, D.G.; Golub, A.; Cromwell, E.N. Development and validation of the anger rumination scale. Personal. Individ. Differ. 2001, 31, 689–700. [Google Scholar] [CrossRef]
- Bernblum, R.; Mor, N. Rumination and emotion-related biases in refreshing information. Emotion 2010, 10, 423–432. [Google Scholar] [CrossRef]
- Park, C.L.; Mills, M.A.; Edmondson, D. PTSD as Meaning Violation: Testing a Cognitive Worldview Perspective. Psychol. Trauma Theory Res. Pract. Policy 2012, 4, 66–73. [Google Scholar] [CrossRef] [Green Version]
- Watkins, L.E.; Sprang, K.R.; Rothbaum, B.O. Treating PTSD: A Review of Evidence-Based Psychotherapy Interventions. Front. Behav. Neurosci. 2018, 12, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Northoff, G.; Heinzel, A.; De Greck, M.; Bermpohl, F.; Dobrowolny, H.; Panksepp, J. Self-referential processing in our brain—A meta-analysis of imaging studies on the self. Neuroimage 2006, 31, 440–457. [Google Scholar] [CrossRef] [PubMed]
- Cann, A.; Calhoun, L.G.; Tedeschi, R.G.; Triplett, K.N.; Vishnevsky, T.; Lindstrom, C.M. Assessing post traumatic cognitive processes: The event related rumination inventory. Anxiety Stress Coping 2011, 24, 137–156. [Google Scholar] [CrossRef] [PubMed]
- Silove, D.; Liddell, B.; Rees, S.; Chey, T.; Nickerson, A.; Tam, N.; Zwi, A.B.; Brooks, R.; Sila, L.L.; Steel, Z. Effects of recurrent violence on post-traumatic stress disorder and severe distress in conflict-affected Timor-Leste: A 6-year longitudinal study. Lancet Glob. Health 2014, 2, e293–e300. [Google Scholar] [CrossRef] [Green Version]
- García, F.E.; Wlodarczyk, A. Communal coping and rumination in the aftermath of Chile earthquake: Multiple mediation analysis of the relationship between subjective severity and posttraumatic growth. J. Community Appl. Soc. Psychol. 2018, 28, 191–199. [Google Scholar] [CrossRef]
- Contractor, A.A.; Weiss, N.H.; Elhai, J.D. Examination of the relation between PTSD symptoms, smartphone feature uses, and problematic smartphone use. Soc. Sci. Comput. Rev. 2019, 37, 385–403. [Google Scholar] [CrossRef]
- Firth, J.; Torous, J.; Stubbs, B.; Firth, J.A.; Steiner, G.Z.; Smith, L.; Alvarez-Jimenez, M.; Gleeson, J.; Vancampfort, D.; Armitage, C.J.; et al. The “online brain”: How the Internet may be changing our cognition. World Psychiatry 2019, 18, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.Q.; Zhou, Z.K.; Yang, X.J.; Kong, F.C.; Niu, G.F.; Fan, C.Y. Mobile phone addiction and sleep quality among Chinese adolescents: A moderated mediation model. Comput. Hum. Behav. 2017, 72, 108–114. [Google Scholar] [CrossRef]
- Wolniewicz, C.A.; Tiamiyu, M.F.; Weeks, J.W.; Elhai, J.D. Problematic smartphone use and relations with negative affect, fear of missing out, and fear of negative and positive evaluation. Psychiatry Res. 2018, 262, 618–623. [Google Scholar] [CrossRef]
- Tymofiyeva, O.; Yuan, J.P.; Kidambi, R.; Huang, C.Y.; Henje, E.; Rubinstein, M.L.; Jariwala, N.; Max, J.E.; Yang, T.T.; Xu, D. Neural correlates of smartphone dependence in adolescents. Front. Hum. Neurosci. 2020, 14, 428. [Google Scholar] [CrossRef] [PubMed]
- Khoo, S.S.; Yang, H. Mental disengagement mediates the effect of rumination on smartphone use: A latent growth curve analysis. Comput. Hum. Behav. 2021, 120, 106757. [Google Scholar] [CrossRef]
- Wong, S.M.Y.; Chen, E.Y.H.; Wong, C.S.M.; Suen, Y.N.; Chan, D.L.K.; Tsang, S.H.S.; Wong, T.Y.; Cheung, C.; Chan, K.T.; Lui, S.S.Y.; et al. Impact of smartphone overuse on 1-year severe depressive symptoms and momentary negative affect: Longitudinal and experience sampling findings from a representative epidemiological youth sample in Hong Kong. Psychiatry Res. 2022, 318, 114939. [Google Scholar] [CrossRef]
- Blades, R. Protecting the brain against bad news. CMAJ 2021, 193, E428–E429. [Google Scholar] [CrossRef]
- Giri, S.P.; Maurya, A.K. A neglected reality of mass media during COVID-19: Effect of pandemic news on individual’s positive and negative emotion and psychological resilience. Personal. Individ. Differ. 2021, 180, 110962. [Google Scholar] [CrossRef]
- Goodall, C.E.; Slater, M.D.; Myers, T.A. Fear and Anger Responses to Local News Coverage of Alcohol-Related Crimes, Accidents, and Injuries: Explaining News Effects on Policy Support Using a Representative Sample of Messages and People. J. Commun. 2013, 63, 373–392. [Google Scholar] [CrossRef]
- Elhai, J.D.; Tiamiyu, M.; Weeks, J. Depression and social anxiety in relation to problematic smartphone use. Internet Res. 2018, 28, 315–332. [Google Scholar] [CrossRef]
- Elhai, J.D.; Gallinari, E.F.; Rozgonjuk, D.; Yang, H. Depression, anxiety and fear of missing out as correlates of social, non-social and problematic smartphone use. Addict. Behav. 2020, 105, 106335. [Google Scholar] [CrossRef] [PubMed]
- McNicol, M.L.; Thorsteinsson, E.B. Internet addiction, psychological distress, and coping responses among adolescents and adults. Cyberpsychology Behav. Soc. Netw. 2017, 20, 296–304. [Google Scholar] [CrossRef] [Green Version]
- Catalano, G.; Catalano, M.C.; Embi, C.S.; Frankel, R.L. Delusions about the Internet. South. Med. J. 1999, 92, 609–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitzan, U.; Shoshan, E.; Lev-Ran, S.; Fennig, S. Internet-Related Psychosis—A Sign of the Times? Isr. J. Psychiatry Relat. Sci. Jerus. 2011, 48, 207–211. [Google Scholar]
- Brand, M.; Wegmann, E.; Stark, R.; Müller, A.; Wölfling, K.; Robbins, T.W.; Potenza, M.N. The Interaction of Person-Affect-Cognition-Execution (I-PACE) model for addictive behaviors: Update, generalization to addictive behaviors beyond internet-use disorders, and specification of the process character of addictive behaviors. Neurosci. Biobehav. Rev. 2019, 104, 1–10. [Google Scholar] [CrossRef]
- Watkins, E.R. Rumination-Focused Cognitive-Behavioral Therapy for Depression; Guilford Publications: New York, NY, USA, 2016. [Google Scholar]
- Watkins, E.R.; Mullan, E.; Wingrove, J.; Rimes, K.; Steiner, H.; Bathurst, N.; Eastman, R.; Scott, J. Rumination-focused cognitive–behavioural therapy for residual depression: Phase II randomised controlled trial. Br. J. Psychiatry 2011, 199, 317–322. [Google Scholar] [CrossRef] [Green Version]
- Feldhaus, C.G.; Jacobs, R.H.; Watkins, E.R.; Peters, A.T.; Bessette, K.L.; Langenecker, S.A. Rumination-focused cognitive behavioral therapy decreases anxiety and increases behavioral activation among remitted adolescents. J. Child Fam. Stud. 2020, 29, 1982–1991. [Google Scholar] [CrossRef]
- Heeren, A.; Philippot, P. Changes in ruminative thinking mediate the clinical benefits of mindfulness: Preliminary findings. Mindfulness 2011, 2, 8–13. [Google Scholar] [CrossRef]
- Greenberg, J.; Reiner, K.; Meiran, N. “Mind the trap”: Mindfulness practice reduces cognitive rigidity. PLoS ONE 2012, 7, e36206. [Google Scholar] [CrossRef]
- Bishop, S.R.; Lau, M.; Shapiro, S.; Carlson, L.; Anderson, N.D.; Carmody, J.; Segal, Z.V.; Abbey, S.; Speca, M.; Velting, D.; et al. Mindfulness: A proposed operational definition. Clin. Psychol. Sci. Pract. 2004, 10, 125–143. [Google Scholar] [CrossRef]
- Segal, Z.V.; Teasdale, J.D.; Williams, J.M.G. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse; Guilford Press: New York, NY, USA, 2002. [Google Scholar]
- McEvoy, P.M.; Perini, S.J. Cognitive behavioral group therapy for social phobia with or without attention training: A controlled trial. J. Anxiety Disord. 2009, 23, 519–528. [Google Scholar] [CrossRef]
- Hirsch, C.R.; Krahé, C.; Whyte, J.; Loizou, S.; Bridge, L.; Norton, S.; Mathews, A. Interpretation training to target repetitive negative thinking in generalized anxiety disorder and depression. J. Consult. Clin. Psychol. 2018, 86, 1017–1030. [Google Scholar] [CrossRef] [PubMed]
- Sauvé, G.; Lavigne, K.M.; Pochiet, G.; Brodeur, M.B.; Lepage, M. Efficacy of psychological interventions targeting cognitive biases in schizophrenia: A systematic review and meta-analysis. Clin. Psychol. Rev. 2020, 78, 101854. [Google Scholar] [CrossRef] [PubMed]
- Yiend, J.; Lam, C.L.M.; Schmidt, N.; Crane, B.; Heslin, M.; Kabir, T.; McGuire, P.; Meek, C.; Mouchlianitis, E.; Peters, E.; et al. Cognitive bias modification for paranoia (CBM-pa): A randomised controlled feasibility study in patients with distressing paranoid beliefs. Psychol. Med. 2022, 1–13. [Google Scholar] [CrossRef]
- Rozenman, M.; Gonzalez, A.; Logan, C.; Goger, P. Cognitive bias modification for threat interpretations: Impact on anxiety symptoms and stress reactivity. Depress. Anxiety 2020, 37, 438–448. [Google Scholar] [CrossRef]
- Xiu, L.; Wu, J.; Chang, L.; Zhou, R. Working Memory Training Improves Emotion Regulation Ability. Sci. Rep. 2018, 8, 15012. [Google Scholar] [CrossRef] [Green Version]
- Clarke, S.C.; Cooper, N.R.; Rana, M.; Mackintosh, B. Cognitive Interpretation Bias: The Effect of a Single Session Moderate Exercise Protocol on Anxiety and Depression. Front. Psychol. 2018, 9, 1363. [Google Scholar] [CrossRef]
- Wronska, M.K.; Kolańczyk, A.; Nijstad, B.A. Engaging in Creativity Broadens Attentional Scope. Front. Psychol. 2018, 9, 1772. [Google Scholar] [CrossRef] [Green Version]
- Beute, F.; de Kort, Y.A. The natural context of wellbeing: Ecological momentary assessment of the influence of nature and daylight on affect and stress for individuals with depression levels varying from none to clinical. Health Place 2018, 49, 7–18. [Google Scholar] [CrossRef]
- Ricarte, J.J.; Ros, L.; Latorre, J.M.; Barry, T.J. Ruminative and mood associations for age differences in social and directive reasons to think and talk about life experiences. PLoS ONE 2020, 15, e0235378. [Google Scholar] [CrossRef] [PubMed]
- Sütterlin, S.; Paap, M.; Babic, S.; Kübler, A.; Vögele, C. Rumination and age: Some things get better. J. Aging Res. 2016, 2012, 267327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, H.; Hou, W.K.; Liang, L.; Li, T.W.; Liu, H.; Lee, T.M. Age-Related Differences of Rumination on the Loneliness–Depression Relationship: Evidence from a Population-Representative Cohort. Innov. Aging 2021, 5, igab034. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The Flow Model of Rumination under normal and stressful circumstances. (a) Ruminative experiences under normal circumstances. (b) Ruminative experiences under stressful situations.
Figure 1.
The Flow Model of Rumination under normal and stressful circumstances. (a) Ruminative experiences under normal circumstances. (b) Ruminative experiences under stressful situations.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Wong, S.M.Y.; Chen, E.Y.H.; Lee, M.C.Y.; Suen, Y.N.; Hui, C.L.M. Rumination as a Transdiagnostic Phenomenon in the 21st Century: The Flow Model of Rumination. Brain Sci. 2023, 13, 1041. https://doi.org/10.3390/brainsci13071041
AMA Style
Wong SMY, Chen EYH, Lee MCY, Suen YN, Hui CLM. Rumination as a Transdiagnostic Phenomenon in the 21st Century: The Flow Model of Rumination. Brain Sciences. 2023; 13(7):1041. https://doi.org/10.3390/brainsci13071041
Chicago/Turabian StyleWong, Stephanie M. Y., Eric Y. H. Chen, Michelle C. Y. Lee, Y. N. Suen, and Christy L. M. Hui. 2023. "Rumination as a Transdiagnostic Phenomenon in the 21st Century: The Flow Model of Rumination" Brain Sciences 13, no. 7: 1041. https://doi.org/10.3390/brainsci13071041
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.