


Decomposing Working Memory in Recurrent Major Depression: Impaired Encoding and Limited Maintenance Immune-to-Encoding Constraint
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
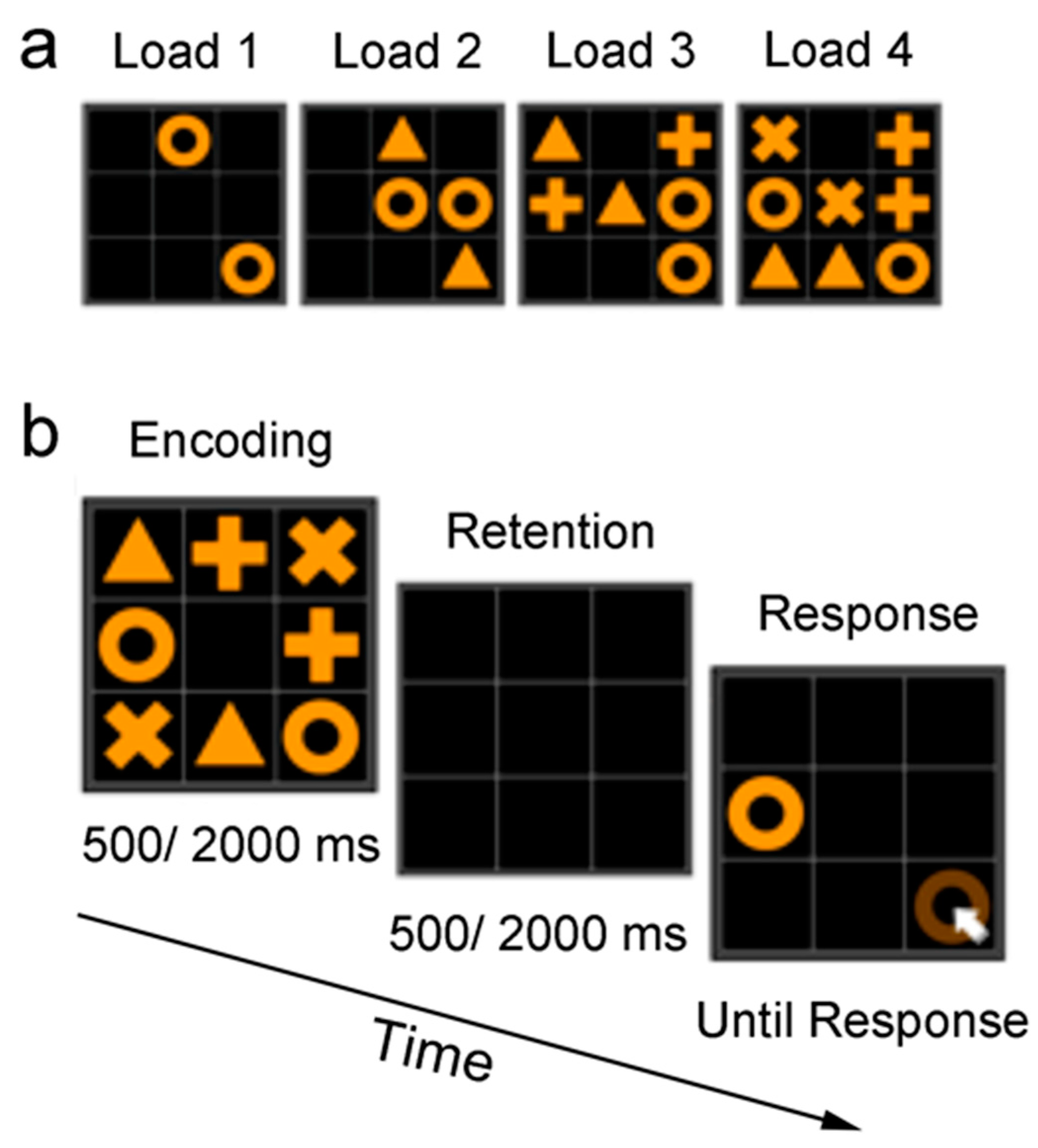
2.2. Design and procedure
2.3. Statistical Analysis
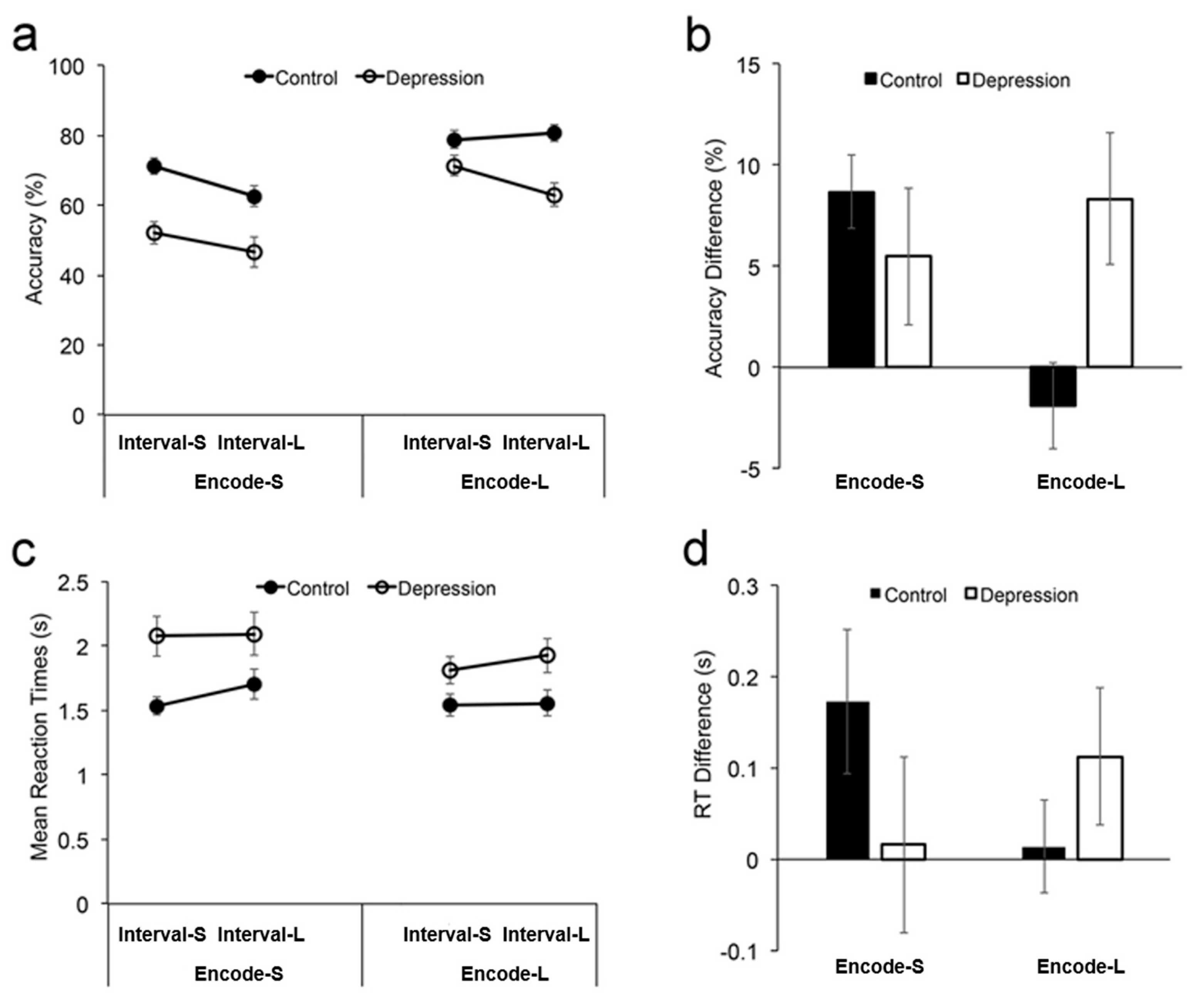
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- James, S.L.; Abate, D.; Abate, K.; Abay, S.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sim, K.; Lau, W.; Sim, J.; Sum, M.; Baldessarini, R. Prevention of relapse and recurrence in adults with major depressive disorder: Systematic review and meta-analyses of controlled trials. Int. J. Neuropsychopharmacol. 2016, 19, pyv076. [Google Scholar] [CrossRef]
- Beck, A.T. Cognitive Therapy and the Emotional Disorders; Penguin: New York, NY, USA, 1979. [Google Scholar]
- Gotlib, I.H.; Joormann, J. Cognition and depression: Current status and future directions. Annu. Rev. Clin. Psychol. 2010, 6, 285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathews, A.; MacLeod, C. Cognitive vulnerability to emotional disorders. Annu. Rev. Clin. Psychol. 2005, 1, 167–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, P.-O.; Fossati, P.; Pochon, J.-B.; Levy, R.; LeBastard, G.; Lehéricy, S.; Allilaire, J.-F.; Dubois, B. Cognitive control and brain resources in major depression: An fMRI study using the n-back task. Neuroimage 2005, 26, 860–869. [Google Scholar] [CrossRef] [PubMed]
- Snyder, H.R. Major depressive disorder is associated with broad impairments on neuropsychological measures of executive function: A meta-analysis and review. Psychol. Bull. 2013, 139, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchweitz, A. Models of working memory:Mechanisms of active maintenance and executive control. Ilha do Desterro 2002, 43, 193–200. [Google Scholar]
- Rose, E.; Ebmeier, K. Pattern of impaired working memory during major depression. J. Affect. Disord. 2006, 90, 149–161. [Google Scholar] [CrossRef]
- Fouladi, A.; Goli, S. Comparing working memory, verbal memory and keeping attention in the manic phase and depression in bipolar disorder. J. Adv. Pharm. Educ. Res.|Apr-Jun 2018, 8, 83. [Google Scholar]
- Nikolin, S.; Tan, Y.; Schwaab, A.; Moffa, A.; Loo, C.; Martin, D. An investigation of working memory deficits in depression using the n-back task: A systematic review and meta-analysis. J. Affect. Disord. 2021, 284, 1–8. [Google Scholar] [CrossRef]
- Pelosi, L.; Slade, T.; Blumhardt, L.; Sharma, V. Working memory dysfunction in major depression: An event-related potential study. Clin. Neurophysiol. 2000, 111, 1531–1543. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Edition, F. Diagnostic and statistical manual of mental disorders. Am Psychiatr. Assoc 2013, 21, 591–643. [Google Scholar]
- Steer, R. Manual for the Beck Depression Inventory-II. Available online: https://www.scienceopen.com/document?vid=9feb932d-1f91-4ff9-9d27-da3bda716129 (accessed on 27 September 2022).
- Song, W.; Zhang, K.; Sun, J.; Ma, L.; Jesse, F.; Teng, X.; Zhou, Y.; Bao, H.; Chen, S.; Wang, S. A simple spatial working memory and attention test on paired symbols shows developmental deficits in schizophrenia patients. Neural Plast. 2013, 2013, 130642. [Google Scholar] [CrossRef]
- Rouder, J.N.; Morey, R.; Speckman, P.; Province, J. Default Bayes factors for ANOVA designs. J. Math. Psychol. 2012, 56, 356–374. [Google Scholar] [CrossRef]
- Wagenmakers, E.-J.; Marsman, M.; Jamil, T.; Ly, A.; Verhagen, J.; Love, J.; Selker, R.; Gronau, Q.; Šmíra, M.; Epskamp, S. Bayesian inference for psychology. Part I: Theoretical advantages and practical ramifications. Psychon. Bull. Rev. 2018, 25, 35–57. [Google Scholar] [CrossRef]
- Wagenmakers, E.-J.; Love, J.; Marsman, M.; Jamil, T.; Ly, A.; Verhagen, J.; Selker, R.; Gronau, Q.; Dropmann, D.; Boutin, B. Bayesian inference for psychology. Part II: Example applications with JASP. Psychon. Bull. Rev. 2018, 25, 58–76. [Google Scholar] [CrossRef] [Green Version]
- Awh, E.; Jonides, J. Overlapping mechanisms of attention and spatial working memory. Trends Cogn. Sci. 2001, 5, 119–126. [Google Scholar] [CrossRef]
- Gazzaley, A.; Nobre, A. Top-down modulation: Bridging selective attention and working memory. Trends Cogn. Sci. 2012, 16, 129–135. [Google Scholar] [CrossRef] [Green Version]
- Rowe, G.; Hirsh, J.; Anderson, A. Positive affect increases the breadth of attentional selection. Proc. Natl. Acad. Sci. USA 2007, 104, 383–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Japee, S.; Safiullah, Z.; Mlynaryk, N.; Ungerleider, L. A normalization framework for emotional attention. PLoS Biol. 2016, 14, e1002578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Fockert, J.W.; Cooper, A. Higher levels of depression are associated with reduced global bias in visual processing. Cogn. Emot. 2014, 28, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Nolen-Hoeksema, S. The role of rumination in depressive disorders and mixed anxiety/depressive symptoms. J. Abnorm. Psychol. 2000, 109, 504. [Google Scholar] [CrossRef]
- Spasojević, J.; Alloy, L.B. Rumination as a common mechanism relating depressive risk factors to depression. Emotion 2001, 1, 25. [Google Scholar] [CrossRef]
- Joormann, J.; Levens, S.; Gotlib, I. Sticky thoughts: Depression and rumination are associated with difficulties manipulating emotional material in working memory. Psychol. Sci. 2011, 22, 979–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Lissnyder, E.; Koster, E.; Everaert, J.; Schacht, R.; Van den Abeele, D.; De Raedt, R. Internal cognitive control in clinical depression: General but no emotion-specific impairments. Psychiatry Res. 2012, 199, 124–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chun, M.M.; Golomb, J.; Turk-Browne, N. A taxonomy of external and internal attention. Annu. Rev. Psychol. 2011, 62, 73–101. [Google Scholar] [CrossRef] [Green Version]
- Keller, A.S.; Ball, T.; Williams, L. Deep phenotyping of attention impairments and the ‘Inattention Biotype’in Major Depressive Disorder. Psychol. Med. 2020, 50, 2203–2212. [Google Scholar] [CrossRef]
- Postle, B.R. Distraction-spanning sustained activity during delayed recognition of locations. Neuroimage 2006, 30, 950–962. [Google Scholar] [CrossRef]
- Kiyonaga, A.; Egner, T. Working memory as internal attention: Toward an integrative account of internal and external selection processes. Psychon. Bull. Rev. 2013, 20, 228–242. [Google Scholar] [CrossRef] [PubMed]
- Keller, A.S.; Leikauf, J.; Holt-Gosselin, B.; Staveland, B.; Williams, L. Paying attention to attention in depression. Transl. Psychiatry 2019, 9, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, O.; Hoy, K.; Wong, D.; Bailey, N.; Fitzgerald, P.; Segrave, R. Individuals with depression display abnormal modulation of neural oscillatory activity during working memory encoding and maintenance. Biol. Psychol. 2019, 148, 107766. [Google Scholar] [CrossRef] [PubMed]
- Chapman, L.J.; Chapman, J.P. Problems in the measurement of cognitive deficits. Psychol. Bull. 1973, 79, 380. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Control | Depression | Statistics | |
|---|---|---|---|
| Gender (F/M) | 26/13 | 23/7 | χ2 (1) = 0.82 |
| Age (years) | 30.4 ± 9.2 | 31.4 ± 13.1 | t(67) = 0.38 |
| BDI score | 5.0 ± 4.1 | 24.0 ± 12.6 | t(67) = 8.85, p < 0.001 |
| Medication (yes/no) | 0/39 | 30/0 | |
| Total duration of medication (months) | 22.4 ± 23.7 |
| Depression Group | Control Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| M (%) | SE (%) | RT (s) | SE (s) | M (%) | SE (%) | RT (s) | SE (s) | |||
| Load 3 | Encode-S | Interval-S | 69.4 | 4.0 | 1.90 | 0.16 | 82.6 | 2.7 | 1.37 | 0.06 |
| Interval-L | 58.9 | 5.0 | 2.16 | 0.26 | 76.2 | 3.6 | 1.60 | 0.12 | ||
| Encode-L | Interval-S | 81.9 | 3.4 | 1.64 | 0.09 | 85.8 | 2.6 | 1.40 | 0.08 | |
| Interval-L | 76.1 | 4.1 | 1.80 | 0.15 | 88.6 | 2.4 | 1.44 | 0.09 | ||
| Load 4 | Encode-S | Interval-S | 34.8 | 3.9 | 2.25 | 0.18 | 59.9 | 3.0 | 1.70 | 0.09 |
| Interval-L | 34.3 | 4.4 | 2.03 | 0.13 | 49.0 | 3.6 | 1.82 | 0.13 | ||
| Encode-L | Interval-S | 60.7 | 3.3 | 1.98 | 0.14 | 71.7 | 3.2 | 1.69 | 0.11 | |
| Interval-L | 49.9 | 3.5 | 2.05 | 0.14 | 72.7 | 3.5 | 1.68 | 0.12 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Z.; Dou, Z.; Xu, H.; Wang, Z.; Zeng, S.; Yang, X.; Takahashi, E.; Popovic, M.R.; Wang, L.; Li, W. Decomposing Working Memory in Recurrent Major Depression: Impaired Encoding and Limited Maintenance Immune-to-Encoding Constraint. Brain Sci. 2023, 13, 38. https://doi.org/10.3390/brainsci13010038
Chen Z, Dou Z, Xu H, Wang Z, Zeng S, Yang X, Takahashi E, Popovic MR, Wang L, Li W. Decomposing Working Memory in Recurrent Major Depression: Impaired Encoding and Limited Maintenance Immune-to-Encoding Constraint. Brain Sciences. 2023; 13(1):38. https://doi.org/10.3390/brainsci13010038
Chicago/Turabian StyleChen, Zhitang, Zheng Dou, Hui Xu, Zhenghua Wang, Suhua Zeng, Xiangyu Yang, Eiki Takahashi, Milos R. Popovic, Lihui Wang, and Weidong Li. 2023. "Decomposing Working Memory in Recurrent Major Depression: Impaired Encoding and Limited Maintenance Immune-to-Encoding Constraint" Brain Sciences 13, no. 1: 38. https://doi.org/10.3390/brainsci13010038