
Bilateral Facial Weakness with Distal Paresthesia Following COVID-19 Vaccination: A Scoping Review for an Atypical Variant of Guillain–Barré Syndrome


Abstract
:1. Introduction
2. Materials and Methods
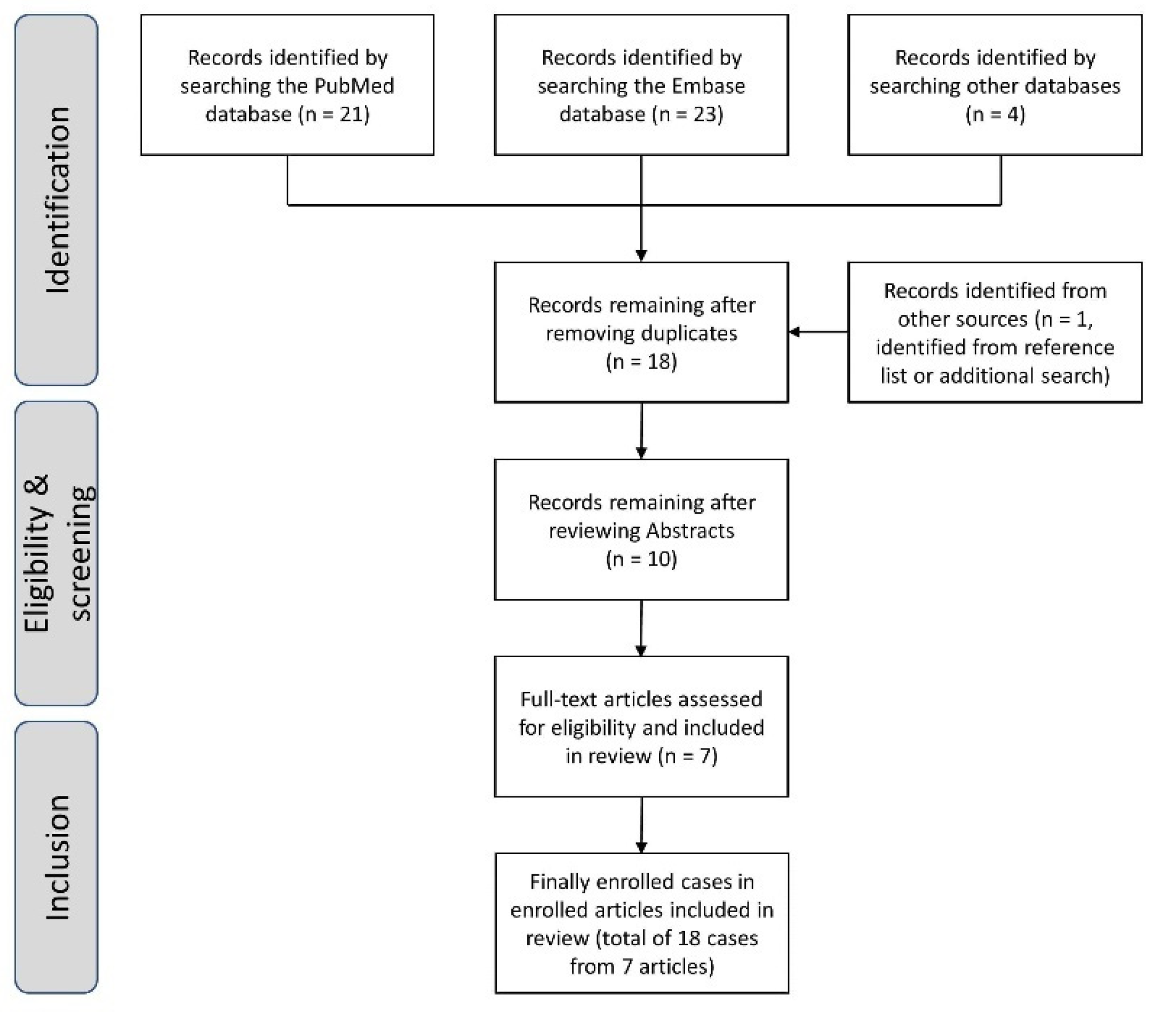
2.1. Data Sources and Study Selection
2.2. Final Enrollment of Studies and Data Extraction
2.3. Standard Protocol Approval, Registration, and Patient Consent
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patone, M.; Handunnetthi, L.; Saatci, D.; Pan, J.; Katikireddi, S.V.; Razvi, S.; Hunt, D.; Mei, X.W.; Dixon, S.; Zaccardi, F.; et al. Neurological complications after first dose of COVID-19 vaccines and SARS-CoV-2 infection. Nat. Med. 2021, 27, 2144–2153. [Google Scholar] [CrossRef] [PubMed]
- Keh, R.Y.S.; Scanlon, S.; Datta-Nemdharry, P.; Donegan, K.; Cavanagh, S.; Foster, M.; Skelland, D.; Palmer, J.; Machado, P.M.; Keddie, S.; et al. COVID-19 vaccination and Guillain-Barré syndrome: Analyses using the National Immunoglobulin Database. Brain 2022. [Google Scholar] [CrossRef] [PubMed]
- Frontera, J.A.; Tamborska, A.A.; Doheim, M.F.; Garcia-Azorin, D.; Gezegen, H.; Guekht, A.; Yusof Khan, A.H.K.; Santacatterina, M.; Sejvar, J.; Thakur, K.T.; et al. Neurological Events Reported after COVID-19 Vaccines: An Analysis of VAERS. Ann. Neurol. 2022, 91, 756–771. [Google Scholar] [CrossRef] [PubMed]
- Wakerley, B.R.; Uncini, A.; Yuki, N. Guillain-Barré and Miller Fisher syndromes--new diagnostic classification. Nat. Rev. Neurol. 2014, 10, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.M.; Ramsamy, S.; Tarr, A.W.; Tighe, P.J.; Irving, W.L.; Tanasescu, R.; Evans, J.R. Guillain-Barré Syndrome Variant Occurring after SARS-CoV-2 Vaccination. Ann. Neurol. 2021, 90, 315–318. [Google Scholar] [CrossRef]
- Castiglione, J.I.; Crespo, J.M.; Lecchini, L.; Silveira, F.O.; Luis, M.B.; Cotti, N.; Simison, C.J.; Aguirre, F.; Piedrabuena, M.A.; Alonso, R.N.; et al. Bilateral facial palsy with paresthesias, variant of Guillain-Barré syndrome following COVID-19 vaccine: A case series of 9 patients. Neuromuscul. Disord. 2022, 32, 572–574. [Google Scholar] [CrossRef]
- Bonifacio, G.B.; Patel, D.; Cook, S.; Purcaru, E.; Couzins, M.; Domjan, J.; Ryan, S.; Alareed, A.; Tuohy, O.; Slaght, S.; et al. Bilateral facial weakness with paraesthesia variant of Guillain-Barré syndrome following Vaxzevria COVID-19 vaccine. J. Neurol. Neurosurg. Psychiatry 2022, 93, 341–342. [Google Scholar] [CrossRef]
- Andreozzi, V.; D’Arco, B.; Pagliano, P.; Toriello, A.; Barone, P. Bilateral facial palsy after COVID-19 vaccination. Neurol. Sci. 2022, 43, 4069–4079. [Google Scholar] [CrossRef]
- Nasuelli, N.A.; De Marchi, F.; Cecchin, M.; De Paoli, I.; Onorato, S.; Pettinaroli, R.; Savoini, G.; Godi, L. A case of acute demyelinating polyradiculoneuropathy with bilateral facial palsy after ChAdOx1 nCoV-19 vaccine. Neurol. Sci. 2021, 42, 4747–4749. [Google Scholar] [CrossRef]
- Jain, E.; Pandav, K.; Regmi, P.; Michel, G.; Altshuler, I. Facial Diplegia: A Rare, Atypical Variant of Guillain-Barré Syndrome and Ad26.COV2.S Vaccine. Cureus 2021, 13, e16612. [Google Scholar] [CrossRef]
- Rossetti, A.; Gheihman, G.; O’Hare, M.; Kosowsky, J.M. Guillain-Barré Syndrome Presenting as Facial Diplegia after COVID-19 Vaccination: A Case Report. J. Emerg. Med. 2021, 61, e141–e145. [Google Scholar] [CrossRef] [PubMed]
- Susuki, K.; Koga, M.; Hirata, K.; Isogai, E.; Yuki, N. A Guillain-Barré syndrome variant with prominent facial diplegia. J. Neurol. 2009, 256, 1899–1905. [Google Scholar] [CrossRef] [PubMed]
- Maramattom, B.V.; Krishnan, P.; Paul, R.; Padmanabhan, S.; Cherukudal Vishnu Nampoothiri, S.; Syed, A.A.; Mangat, H.S. Guillain-Barré Syndrome following ChAdOx1-S/nCoV-19 Vaccine. Ann. Neurol. 2021, 90, 312–314. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.; Hurlburt, G.; Podury, S.; Tandon, M.; Kingree, S.; Sriwastava, S. A Novel Case of Bifacial Diplegia Variant of Guillain-Barré Syndrome Following Janssen COVID-19 Vaccination. Neurol. Int. 2021, 13, 404–409. [Google Scholar] [CrossRef] [PubMed]
- Oo, W.M.; Giri, P.; de Souza, A. AstraZeneca COVID-19 vaccine and Guillain-Barré Syndrome in Tasmania: A causal link? J. Neuroimmunol. 2021, 360, 577719. [Google Scholar] [CrossRef] [PubMed]
- Badoiu, A.; Moranne, O.; Coudray, S.; Ion, I.M. Clinical Variant of Guillain-Barre Syndrome with Prominent Facial Diplegia After AstraZeneca Coronavirus Disease 2019 Vaccine. J. Clin. Neuromuscul. Dis. 2021, 23, 115–116. [Google Scholar] [CrossRef]
- McKean, N.; Chircop, C. Guillain-Barré syndromee after COVID-19 vaccination. BMJ Case Rep. 2021, 14, e244125. [Google Scholar] [CrossRef]
- Kanabar, G.; Wilkinson, P. Guillain-Barré syndrome presenting with facial diplegia following COVID-19 vaccination in two patients. BMJ Case Rep. 2021, 14, e244527. [Google Scholar] [CrossRef]
- Leemans, W.; Antonis, S.; De Vooght, W.; Lemmens, R.; Van Damme, P. Neuromuscular complications after COVID-19 vaccination: A series of eight patients. Acta Neurol. Belg. 2022, 122, 753–761. [Google Scholar] [CrossRef]
- Kim, J.K.; Oh, S.Y.; Sohn, E.H.; Hong, Y.H.; Jun, S.M.; Bae, J.S. When is facial diplegia regarded as a variant of Guillain-Barré syndrome? J. Peripher. Nerv. Syst. 2015, 20, 32–36. [Google Scholar] [CrossRef]
- Fantini, J.; Di Scala, C.; Chahinian, H.; Yahi, N. Structural and molecular modelling studies reveal a new mechanism of action of chloroquine and hydroxychloroquine against SARS-CoV-2 infection. Int. J. Antimicrob. Agents 2020, 55, 105960. [Google Scholar] [CrossRef] [PubMed]
- Gigli, G.L.; Vogrig, A.; Nilo, A.; Fabris, M.; Biasotto, A.; Curcio, F.; Miotti, V.; Tascini, C.; Valente, M. HLA and immunological features of SARS-CoV-2-induced Guillain-Barré syndrome. Neurol. Sci. 2020, 41, 3391–3394. [Google Scholar] [CrossRef] [PubMed]
- Schonberger, L.B.; Bregman, D.J.; Sullivan-Bolyai, J.Z.; Keenlyside, R.A.; Ziegler, D.W.; Retailliau, H.F.; Eddins, D.L.; Bryan, J.A. Guillain-Barre syndrome following vaccination in the National Influenza Immunization Program, United States, 1976–1977. Am. J. Epidemiol. 1979, 110, 105–123. [Google Scholar] [CrossRef] [PubMed]
- Lasky, T.; Terracciano, G.J.; Magder, L.; Koski, C.L.; Ballesteros, M.; Nash, D.; Clark, S.; Haber, P.; Stolley, P.D.; Schonberger, L.B.; et al. The Guillain-Barré syndrome and the 1992–1993 and 1993–1994 influenza vaccines. N. Engl. J. Med. 1998, 339, 1797–1802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anand, P.; Stahel, V.P. The safety of Covid-19 mRNA vaccines: A review. Patient Saf. Surg. 2021, 15, 20. [Google Scholar] [CrossRef]
- Yasmin, F.; Najeeb, H.; Moeed, A.; Naeem, U.; Asghar, M.S.; Chughtai, N.U.; Yousaf, Z.; Seboka, B.T.; Ullah, I.; Lin, C.-Y.; et al. COVID-19 Vaccine Hesitancy in the United States: A Systematic Review. Front. Public Health 2021, 9, 770985. [Google Scholar] [CrossRef]


{kind=link}
| First Author. Reference | Country | Journal | Year | Study Type | No. of Patients | Case No. |
|---|---|---|---|---|---|---|
| Nasuelli [9] | Italy | Neurological Sciences | 2021 | Case report | 1 | [1] |
| Jain [10] | US | Cureus | 2021 | Case report | 1 | [2] |
| Allen [5] | UK | Annals of Neurology | 2021 | Case series | 3/4 (cases 1, 2, and 4) | [3,4,5] |
| Rossetti [11] | US | Journal of Emergency Medicine | 2021 | Case report | 1 | [6] |
| Andreozzi [8] | Italy | Neurological Sciences | 2022 | Case series | 1/2 (case 1) | [7] |
| Bonifacio [7] | UK | Journal of Neurology, Neurosurgery, and Psychiatry | 2022 | Case series | 2/5 (cases 1 and 5) | [8,9] |
| Castiglione [6] | Argentina | Neuromuscular Disorders | 2022 | Case series | 9/9 | [10,11,12,13,14,15,16,17,18] |
| Case No. | Age (Years) | Sex | Vaccine Type | Dose | Comorbidities | Interval between Vaccination and Initial Symptoms (Days) | Initial Subjective Symptoms | BFW | Distal Paresthesia | Other Findings | A/C Dissociation | NCS Findings (Limbs) | Antiganglioside Antibodies | Microbiology Test for Lyme Disease |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [1] | 59 | M | AZ | First | HT, hyperuricemia | 10 | Distal paresthesia | + | + | Postural instability | + | AIDP | - | NA |
| [2] | 65 | F | Janssen | First | HT, DM, DL, drug allergy | 15 | Pain, ageusia, hyposalivation | + | - | Dysarthria, dysphagia, dysphasia | + | NA | NA | NA |
| [3] | 54 | M | AZ | First | - | 12 | Distal paresthesia | + | + | - | + | Normal | NA | NA |
| [4] | 20 | M | AZ | First | UC | 20–21 | Headache, distal paresthesia | + | + | - | + | Normal | NA | NA |
| [5] | 55 | M | AZ | First | HT | 22–23 | Thigh paresthesia, lumbosacral numbness | + | ? | Facial nerve enhancement on MRI | + | NA | NA | NA |
| [6] | 38 | M | Janssen | First | Anxiety, depression, marijuana user | 12–14 | Distal (limbs, tongue, lip) paresthesia, numbness, facial palsy | + | + | Facial nerve enhancement on MRI, hyponatremia | + | NA | NA | NA |
| [7] | 59 | F | AZ | First | Hashimoto thyroiditis | 15 | Lower limbs and back paresthesia, pain, BFP | + | + | - | + | AIDP | NA | NA |
| [8] | 66 | M | AZ | First | - | 7 | Back/leg pain, distal paresthesia | + | + | Facial nerve enhancement on MRI | + | AIDP | - | - |
| [9] | 53 | M | AZ | First | - | 8 | Lower back discomfort and radiating pain | + | + | - | + | NA | NA | - |
| [10] | 56 | F | Sputnik V | First | NA | 19 | NA | + | + | - | - | Normal | - | NA |
| [11] | 55 | M | Sputnik V | First | NA | 28 | NA | + | + | - | + | Normal | - | NA |
| [12] | 87 | M | Sputnik V | First | NA | 17 | NA | + | + | Sudden arrhythmia onset, death | + | Normal | GD1a (+) | NA |
| [13] | 50 | M | AZ | First | NA | 20 | NA | + | + | - | + | Normal | - | NA |
| [14] | 39 | M | Sputnik V | First | NA | 10 | NA | + | + | - | + | NA | Sulfatide (+) | NA |
| [15] | 42 | F | AZ | First | NA | 28 | NA | + | + | - | + | Normal | NA | NA |
| [16] | 52 | M | AZ | First | NA | 13 | NA | + | + | - | + | AIDP | GM1 (+) | NA |
| [17] | 43 | M | Sputnik V | Second | NA | 13 | NA | + | + | - | + | AIDP | - | NA |
| [18] | 65 | M | AZ | Second | NA | 13 | NA | + | + | Facial nerve enhancement on MRI | + | Normal | GM1 (+) | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.-H.; Kim, J.-E.; Yoon, B.-A.; Kim, J.-K.; Bae, J.-S. Bilateral Facial Weakness with Distal Paresthesia Following COVID-19 Vaccination: A Scoping Review for an Atypical Variant of Guillain–Barré Syndrome. Brain Sci. 2022, 12, 1046. https://doi.org/10.3390/brainsci12081046
Kim Y-H, Kim J-E, Yoon B-A, Kim J-K, Bae J-S. Bilateral Facial Weakness with Distal Paresthesia Following COVID-19 Vaccination: A Scoping Review for an Atypical Variant of Guillain–Barré Syndrome. Brain Sciences. 2022; 12(8):1046. https://doi.org/10.3390/brainsci12081046
Chicago/Turabian StyleKim, Yoo-Hwan, Jee-Eun Kim, Byeol-A Yoon, Jong-Kuk Kim, and Jong-Seok Bae. 2022. "Bilateral Facial Weakness with Distal Paresthesia Following COVID-19 Vaccination: A Scoping Review for an Atypical Variant of Guillain–Barré Syndrome" Brain Sciences 12, no. 8: 1046. https://doi.org/10.3390/brainsci12081046