
Resting-State Functional Magnetic Resonance Imaging for Surgical Neuro-Oncology Planning: Towards a Standardization in Clinical Settings

 , ,
, ,
Abstract
:1. Introduction
2. Principles of Rest-fMRI
3. Clinical Application of Rest-fMRI
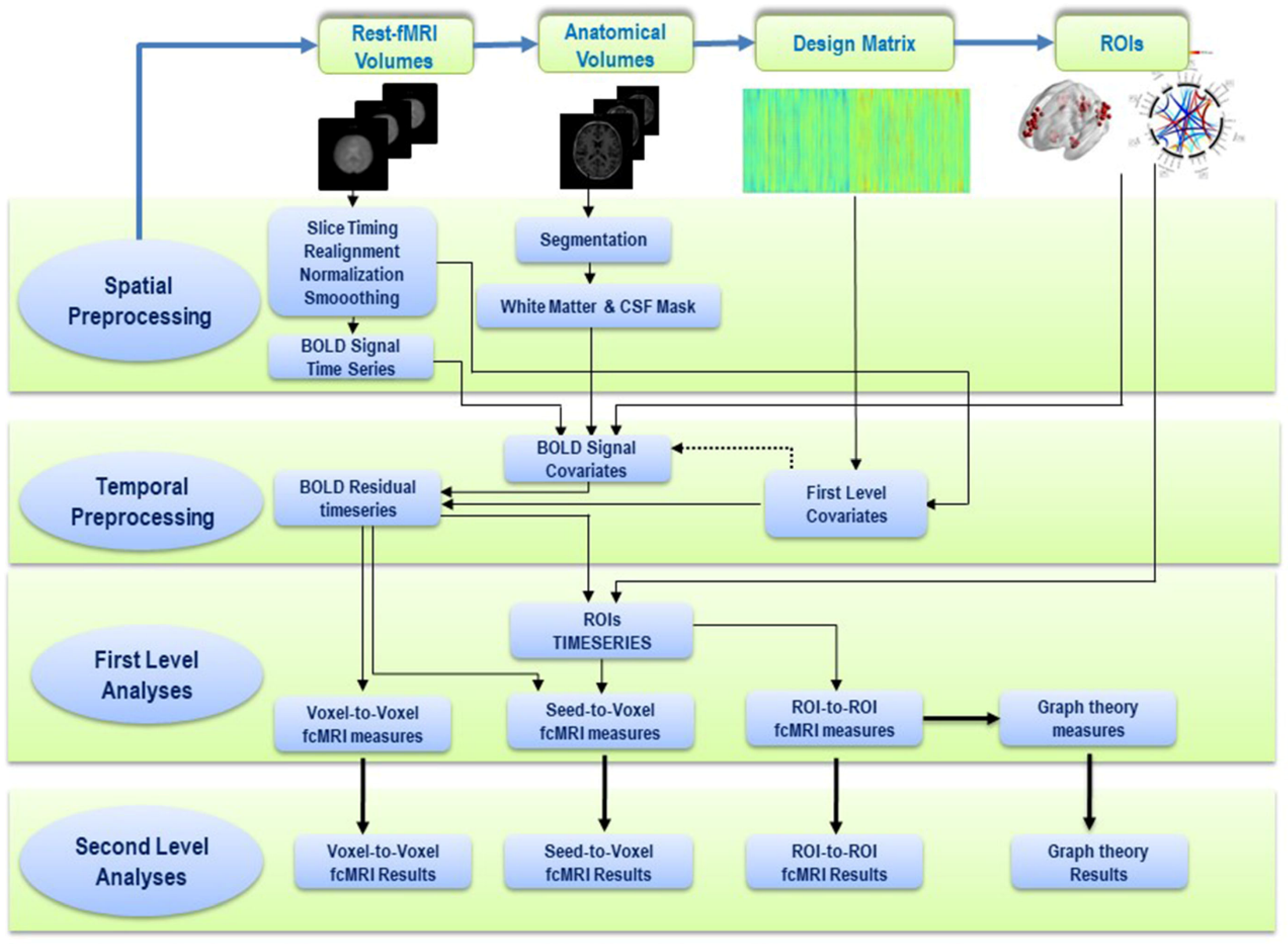
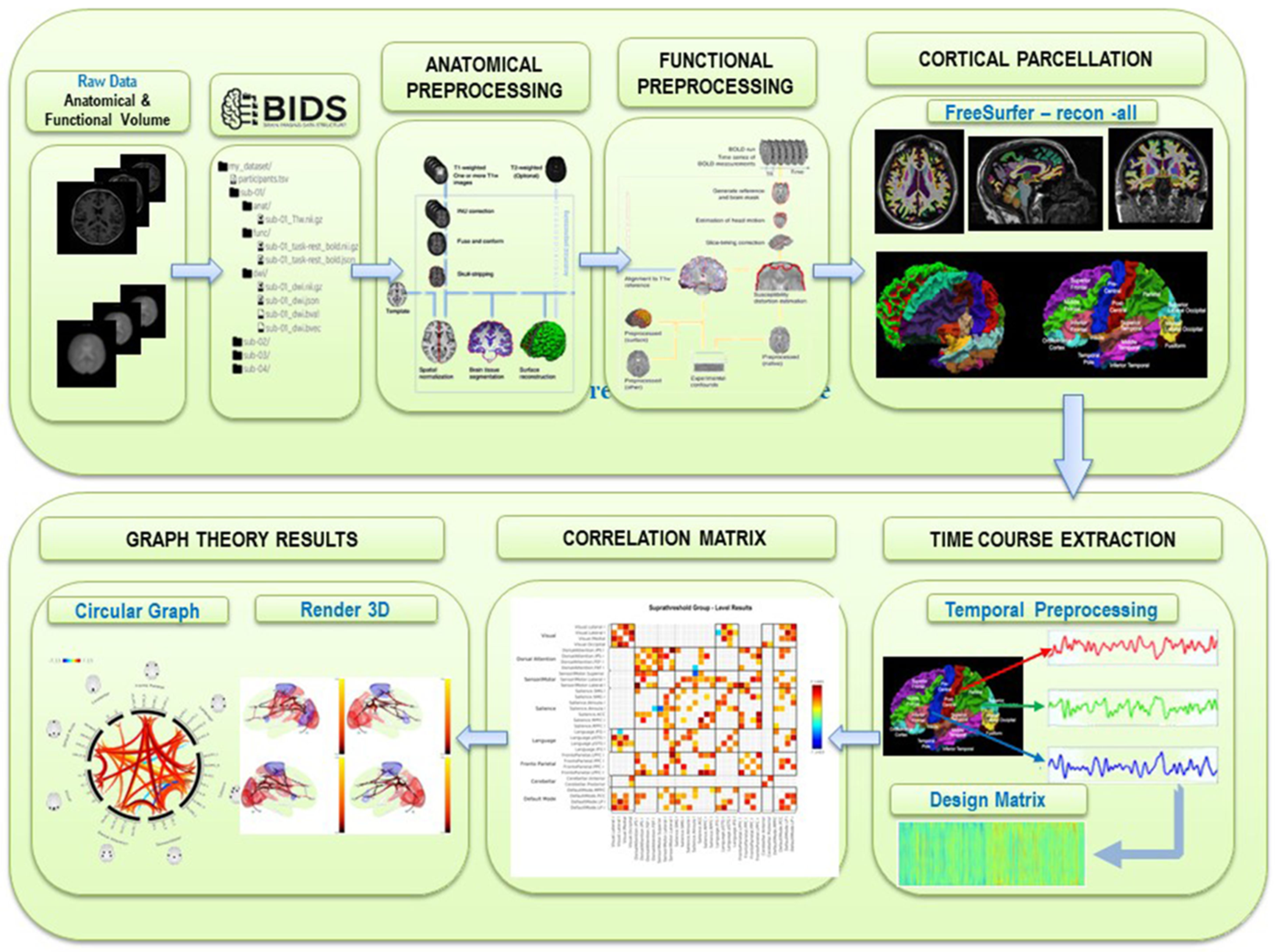
4. Postprocessing of Resting-State fMRI and Analysis of Brain Networks
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rossi, M.; Nibali, M.C.; Torregrossa, F.; Bello, L.; Grasso, G. Innovation in Neurosurgery: The Concept of Cognitive Mapping. World Neurosurg. 2019, 131, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Grasso, G.; Torregrossa, F.; Leone, L. Maximizing the Extent of Resection in High-Grade Glioma. World Neurosurg. 2019, 123, 256–258. [Google Scholar] [CrossRef]
- Grasso, G. Extent of Resection and Survival in Glioblastoma Multiforme. JAMA Oncol. 2016, 2, 1508–1509. [Google Scholar] [CrossRef]
- Grasso, G. Innovation in Neurosurgery: Integration Between Cutting-Edge Devices and “Old-Fashioned” Surgical Technique. World Neurosurg. 2019, 131, 311–312. [Google Scholar] [CrossRef]
- Sparacia, G.; Parla, G.; Lo Re, V.; Cannella, R.; Mamone, G.; Carollo, V.; Midiri, M.; Grasso, G. Resting-State Functional Connectome in Patients with Brain Tumors Before and After Surgical Resection. World Neurosurg. 2020, 141, e182–e194. [Google Scholar] [CrossRef]
- Sparacia, G.; Parla, G.; Cannella, R.; Perri, A.; Lo Re, V.; Mamone, G.; Miraglia, R.; Torregrossa, F.; Grasso, G. Resting-State Functional Magnetic Resonance Imaging for Brain Tumor Surgical Planning: Feasibility in Clinical Setting. World Neurosurg. 2019, 131, 356–363. [Google Scholar] [CrossRef]
- Ostrom, Q.T.; Gittleman, H.; Liao, P.; Rouse, C.; Chen, Y.; Dowling, J.; Wolinsky, Y.; Kruchko, C.; Barnholtz-Sloan, J. CBTRUS statistical report: Primary brain and central nervous system tumors diagnosed in the United States in 2007–2011. Neuro Oncol. 2014, 16 (Suppl. 4). [Google Scholar] [CrossRef]
- Kawaguchi, T.; Sonoda, Y.; Shibahara, I.; Saito, R.; Kanamori, M.; Kumabe, T.; Tominaga, T. Impact of gross total resection in patients with WHO grade III glioma harboring the IDH 1/2 mutation without the 1p/19q co-Deletion. J. Neurooncol. 2016, 129, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, S.B.; Hendricks, B.K.; Torregrossa, F.; Grasso, G.; Cohen-Gadol, A.A. Innovations in the Art of Microneurosurgery for Reaching Deep-Seated Cerebral Lesions. World Neurosurg. 2019, 131, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Torregrossa, F.; Aguennouz, M.; La Torre, D.; Sfacteria, A.; Grasso, G. Role of Erythropoietin in Cerebral Glioma: An Innovative Target in Neuro-Oncology. World Neurosurg. 2019, 131, 346–355. [Google Scholar] [CrossRef]
- Grasso, G.; Torregrossa, F. When Neuroprotection Becomes a Potential Ally of High-Grade Glioma. World Neurosurg. 2019, 125, 529–530. [Google Scholar] [CrossRef]
- Grasso, G. Erythropoietin: A new paradigm for neuroprotection. J. Neurosurg. Anesthesiol. 2006, 18, 91–92. [Google Scholar] [CrossRef]
- Lv, H.; Wang, Z.; Tong, E.; Williams, L.M.; Zaharchuk, G.; Zeineh, M.; Goldstein-Piekarski, A.N.; Ball, T.M.; Liao, C.; Wintermark, M. Resting-State Functional MRI: Everything That Nonexperts Have Always Wanted to Know. AJNR Am. J. Neuroradiol. 2018, 39, 1390–1399. [Google Scholar] [CrossRef] [Green Version]
- Raichle, M.E.; Mintun, M.A. Brain work and brain imaging. Annu. Rev. Neurosci. 2006, 29, 449–476. [Google Scholar] [CrossRef]
- Metwali, H.; Samii, A. Seed-Based Connectivity Analysis of Resting-State fMRI in Patients with Brain Tumors: A Feasibility Study. World Neurosurg. 2019, 128, e165–e176. [Google Scholar] [CrossRef]
- Duyn, J. Spontaneous fMRI activity during resting wakefulness and sleep. Prog. Brain Res. 2011, 193, 295–305. [Google Scholar] [CrossRef] [Green Version]
- Barkhof, F.; Haller, S.; Rombouts, S.A. Resting-State functional MR imaging: A new window to the brain. Radiology 2014, 272, 29–49. [Google Scholar] [CrossRef] [PubMed]
- Biswal, B.; Yetkin, F.Z.; Haughton, V.M.; Hyde, J.S. Functional connectivity in the motor cortex of resting human brain using echo-Planar MRI. Magn. Reson. Med. 1995, 34, 537–541. [Google Scholar] [CrossRef]
- Lee, M.H.; Smyser, C.D.; Shimony, J.S. Resting-State fMRI: A review of methods and clinical applications. AJNR Am. J. Neuroradiol. 2013, 34, 1866–1872. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Buckner, R.L.; Fox, M.D.; Holt, D.J.; Holmes, A.J.; Stoecklein, S.; Langs, G.; Pan, R.; Qian, T.; Li, K.; et al. Parcellating cortical functional networks in individuals. Nat. Neurosci. 2015, 18, 1853–1860. [Google Scholar] [CrossRef] [Green Version]
- Shirer, W.R.; Ryali, S.; Rykhlevskaia, E.; Menon, V.; Greicius, M.D. Decoding subject-Driven cognitive states with whole-Brain connectivity patterns. Cereb. Cortex 2012, 22, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Seeley, W.W.; Menon, V.; Schatzberg, A.F.; Keller, J.; Glover, G.H.; Kenna, H.; Reiss, A.L.; Greicius, M.D. Dissociable intrinsic connectivity networks for salience processing and executive control. J. Neurosci. 2007, 27, 2349–2356. [Google Scholar] [CrossRef]
- Koch, W.; Teipel, S.; Mueller, S.; Benninghoff, J.; Wagner, M.; Bokde, A.L.; Hampel, H.; Coates, U.; Reiser, M.; Meindl, T. Diagnostic power of default mode network resting state fMRI in the detection of Alzheimer’s disease. Neurobiol. Aging 2012, 33, 466–478. [Google Scholar] [CrossRef] [PubMed]
- Barnett, A.; Audrain, S.; McAndrews, M.P. Applications of Resting-State Functional MR Imaging to Epilepsy. Neuroimaging Clin. N. Am. 2017, 27, 697–708. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, T.J.; Davenport, E.M.; Murugesan, G.; Montillo, A.; Maldjian, J.A. Applications of Resting State Functional MR Imaging to Traumatic Brain Injury. Neuroimaging Clin. N. Am. 2017, 27, 685–696. [Google Scholar] [CrossRef]
- Zaca, D.; Jovicich, J.; Corsini, F.; Rozzanigo, U.; Chioffi, F.; Sarubbo, S. ReStNeuMap: A tool for automatic extraction of resting-State functional MRI networks in neurosurgical practice. J. Neurosurg. 2018, 131, 764–771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shurtleff, H.; Warner, M.; Poliakov, A.; Bournival, B.; Shaw, D.W.; Ishak, G.; Yang, T.; Karandikar, M.; Saneto, R.P.; Browd, S.R.; et al. Functional magnetic resonance imaging for presurgical evaluation of very young pediatric patients with epilepsy. J. Neurosurg. Pediatr. 2010, 5, 500–506. [Google Scholar] [CrossRef]
- Lu, J.; Zhang, H.; Hameed, N.U.F.; Zhang, J.; Yuan, S.; Qiu, T.; Shen, D.; Wu, J. An automated method for identifying an independent component analysis-Based language-Related resting-State network in brain tumor subjects for surgical planning. Sci. Rep. 2017, 7, 13769. [Google Scholar] [CrossRef] [Green Version]
- Dierker, D.; Roland, J.L.; Kamran, M.; Rutlin, J.; Hacker, C.D.; Marcus, D.S.; Milchenko, M.; Miller-Thomas, M.M.; Benzinger, T.L.; Snyder, A.Z.; et al. Resting-State Functional Magnetic Resonance Imaging in Presurgical Functional Mapping: Sensorimotor Localization. Neuroimaging Clin. N. Am. 2017, 27, 621–633. [Google Scholar] [CrossRef]
- Lang, S.; Duncan, N.; Northoff, G. Resting-State functional magnetic resonance imaging: Review of neurosurgical applications. Neurosurgery 2014, 74, 453–464. [Google Scholar] [CrossRef] [Green Version]
- Metwali, H.; Raemaekers, M.; Kniese, K.; Samii, A. Intraoperative Resting-State Functional Connectivity and Resting-State Networks in Patients with Intracerebral Lesions: Detectability and Variations Between Sessions. World Neurosurg. 2020, 133, e197–e204. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Johnston, J.M.; Fox, M.D.; Leuthardt, E.C.; Grubb, R.L.; Chicoine, M.R.; Smyth, M.D.; Snyder, A.Z.; Raichle, M.E.; Shimony, J.S. Preoperative sensorimotor mapping in brain tumor patients using spontaneous fluctuations in neuronal activity imaged with functional magnetic resonance imaging: Initial experience. Neurosurgery 2009, 65, 226–236. [Google Scholar] [CrossRef] [Green Version]
- Mannfolk, P.; Nilsson, M.; Hansson, H.; Stahlberg, F.; Fransson, P.; Weibull, A.; Svensson, J.; Wirestam, R.; Olsrud, J. Can resting-State functional MRI serve as a complement to task-Based mapping of sensorimotor function? A test-Retest reliability study in healthy volunteers. J. Magn. Reson. Imaging 2011, 34, 511–517. [Google Scholar] [CrossRef]
- Sair, H.I.; Yahyavi-Firouz-Abadi, N.; Calhoun, V.D.; Airan, R.D.; Agarwal, S.; Intrapiromkul, J.; Choe, A.S.; Gujar, S.K.; Caffo, B.; Lindquist, M.A.; et al. Presurgical brain mapping of the language network in patients with brain tumors using resting-State fMRI: Comparison with task fMRI. Hum. Brain Mapp 2016, 37, 913–923. [Google Scholar] [CrossRef]
- Sair, H.I.; Agarwal, S.; Pillai, J.J. Application of Resting State Functional MR Imaging to Presurgical Mapping: Language Mapping. Neuroimaging Clin. N Am. 2017, 27, 635–644. [Google Scholar] [CrossRef]
- Hart, M.G.; Price, S.J.; Suckling, J. Functional connectivity networks for preoperative brain mapping in neurosurgery. J. Neurosurg. 2017, 126, 1941–1950. [Google Scholar] [CrossRef]
- Esposito, R.; Mattei, P.A.; Briganti, C.; Romani, G.L.; Tartaro, A.; Caulo, M. Modifications of default-Mode network connectivity in patients with cerebral glioma. PLoS ONE 2012, 7, e40231. [Google Scholar] [CrossRef] [Green Version]
- Shimony, J.S.; Zhang, D.; Johnston, J.M.; Fox, M.D.; Roy, A.; Leuthardt, E.C. Resting-State spontaneous fluctuations in brain activity: A new paradigm for presurgical planning using fMRI. Acad. Radiol. 2009, 16, 578–583. [Google Scholar] [CrossRef] [Green Version]
- Tie, Y.; Rigolo, L.; Norton, I.H.; Huang, R.Y.; Wu, W.; Orringer, D.; Mukundan, S., Jr.; Golby, A.J. Defining language networks from resting-State fMRI for surgical planning—Feasibility study. Hum. Brain Mapp. 2014, 35, 1018–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Heuvel, M.P.; Hulshoff Pol, H.E. Exploring the brain network: A review on resting-State fMRI functional connectivity. Eur. Neuropsychopharmacol. 2010, 20, 519–534. [Google Scholar] [CrossRef]
- Li, K.; Guo, L.; Nie, J.; Li, G.; Liu, T. Review of methods for functional brain connectivity detection using fMRI. Comput. Med. Imaging Graph. 2009, 33, 131–139. [Google Scholar] [CrossRef] [Green Version]
- Guo, Y.; Pagnoni, G. A unified framework for group independent component analysis for multi-Subject fMRI data. Neuroimage 2008, 42, 1078–1093. [Google Scholar] [CrossRef] [Green Version]
- Esposito, F.; Scarabino, T.; Hyvarinen, A.; Himberg, J.; Formisano, E.; Comani, S.; Tedeschi, G.; Goebel, R.; Seifritz, E.; Di Salle, F. Independent component analysis of fMRI group studies by self-Organizing clustering. Neuroimage 2005, 25, 193–205. [Google Scholar] [CrossRef]
- Schmithorst, V.J.; Holland, S.K. Comparison of three methods for generating group statistical inferences from independent component analysis of functional magnetic resonance imaging data. J. Magn. Reson Imaging 2004, 19, 365–368. [Google Scholar] [CrossRef] [Green Version]
- Bullmore, E.; Sporns, O. Complex brain networks: Graph theoretical analysis of structural and functional systems. Nat. Rev. Neurosci. 2009, 10, 186–198. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zuo, X.; He, Y. Graph-Based network analysis of resting-State functional MRI. Front. Syst. Neurosci. 2010, 4, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behzadi, Y.; Restom, K.; Liau, J.; Liu, T.T. A component based noise correction method (CompCor) for BOLD and perfusion based fMRI. Neuroimage 2007, 37, 90–101. [Google Scholar] [CrossRef] [Green Version]
- Pruim, R.H.R.; Mennes, M.; van Rooij, D.; Llera, A.; Buitelaar, J.K.; Beckmann, C.F. ICA-AROMA: A robust ICA-Based strategy for removing motion artifacts from fMRI data. Neuroimage 2015, 112, 267–277. [Google Scholar] [CrossRef]
- Grasso, G.; Torregrossa, F. Magnetic Resonance Spectrobiopsy for Prediction of Isocitrate Dehydrogenase Mutation in Glioma. World Neurosurg. 2020, 134, 187–189. [Google Scholar] [CrossRef] [PubMed]
- Torregrossa, F.; Grasso, G. Concept of Spectrobiopsy Facing Gliomas: Rational and Future Perspectives Related to Target Therapy. World Neurosurg. 2020, 134, 308–310. [Google Scholar] [CrossRef]
- Håberg, A.; Kvistad, K.A.; Unsgård, G.; Haraldseth, O. Preoperative blood oxygen level-Dependent functional magnetic resonance imaging in patients with primary brain tumors: Clinical application and outcome. Neurosurgery 2004, 54, 902–914. [Google Scholar] [CrossRef] [PubMed]
- Lemée, J.M.; Berro, D.H.; Bernard, F.; Chinier, E.; Leiber, L.M.; Menei, P.; Ter Minassian, A. Resting-State functional magnetic resonance imaging versus task-Based activity for language mapping and correlation with perioperative cortical mapping. Brain Behav. 2019, 9, e01362. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.; Ding, Z.; Mao, D.; Yuan, J.; Zhu, F.; Chen, S.; Xu, Y.; Lou, L.; Feng, X.; Qi, L.; et al. PreSurgMapp: A MATLAB Toolbox for Presurgical Mapping of Eloquent Functional Areas Based on Task-Related and Resting-State Functional MRI. Neuroinformatics 2016, 14, 421–438. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.C.; Kosteniuk, S.E.; Bihari, F.; Megyesi, J.F. Functional Magnetic Resonance Imaging for Preoperative Planning in Brain Tumour Surgery. Can. J. Neurol. Sci. 2017, 44, 59–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catalino, M.P.; Yao, S.; Green, D.L.; Laws, E.R.; Golby, A.J.; Tie, Y. Mapping cognitive and emotional networks in neurosurgical patients using resting-State functional magnetic resonance imaging. Neurosurg. Focus. 2020, 8, E9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, C.C.; Ward, H.A.; Sharbrough, F.W.; Meyer, F.B.; Marsh, W.R.; Raffel, C.; So, L.E.; Cascino, G.D.; Shin, C.; Xu, Y.; et al. Assessment of functional MR imaging in neurosurgical planning. AJNR Am. J. Neuroradiol. 1999, 20, 1511–1519. [Google Scholar] [PubMed]
- Petrella, J.R.; Shah, L.M.; Harris, K.M.; Friedman, A.H.; Timothy, M.G.; Sampson, J.H.; Pekala, J.S.; Voyvodic, J.T. Preoperative functional MR imaging localization of language and motor areas: Effect on therapeutic decision making in patients with potentially resectable brain tumors. Radiology 2006, 240, 793–802. [Google Scholar] [CrossRef]
- Nucifora, P.G.; Verma, R.; Lee, S.K.; Melhem, E.R. Diffusion-Tensor MR imaging and tractography: Exploring brain microstructure and connectivity. Radiology 2007, 245, 367–384. [Google Scholar] [CrossRef] [Green Version]
- Tae, W.S.; Ham, B.J.; Pyun, S.B.; Kang, S.H.; Kim, B.J. Current Clinical Applications of Diffusion-Tensor Imaging in Neurological Disorders. J. Clin. Neurol. 2018, 14, 129–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, S.; Sair, H.I.; Pillai, J.J. Limitations of Resting-State Functional MR Imaging in the Setting of Focal Brain Lesions. Neuroimaging Clin. N Am. 2017, 27, 645–661. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
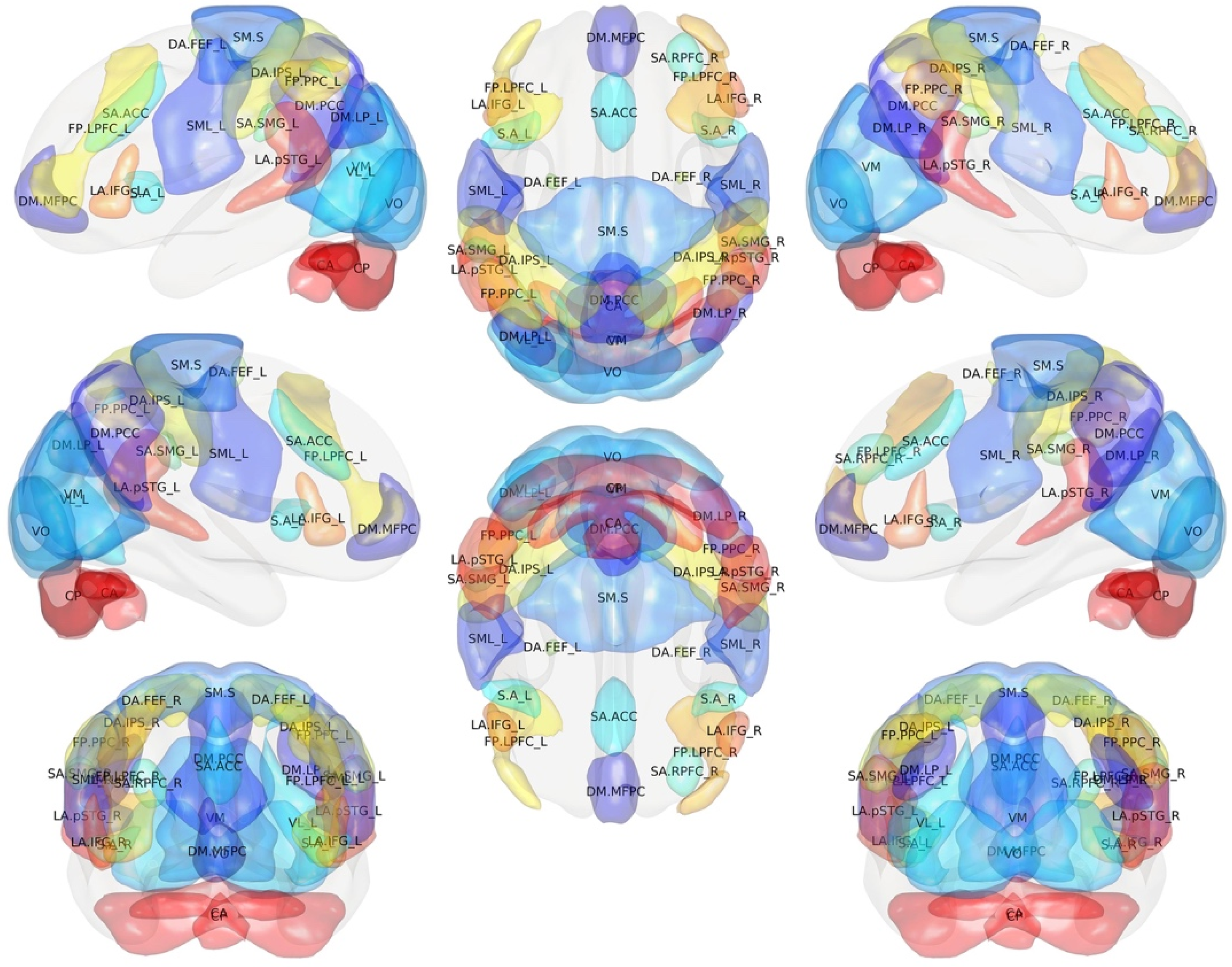
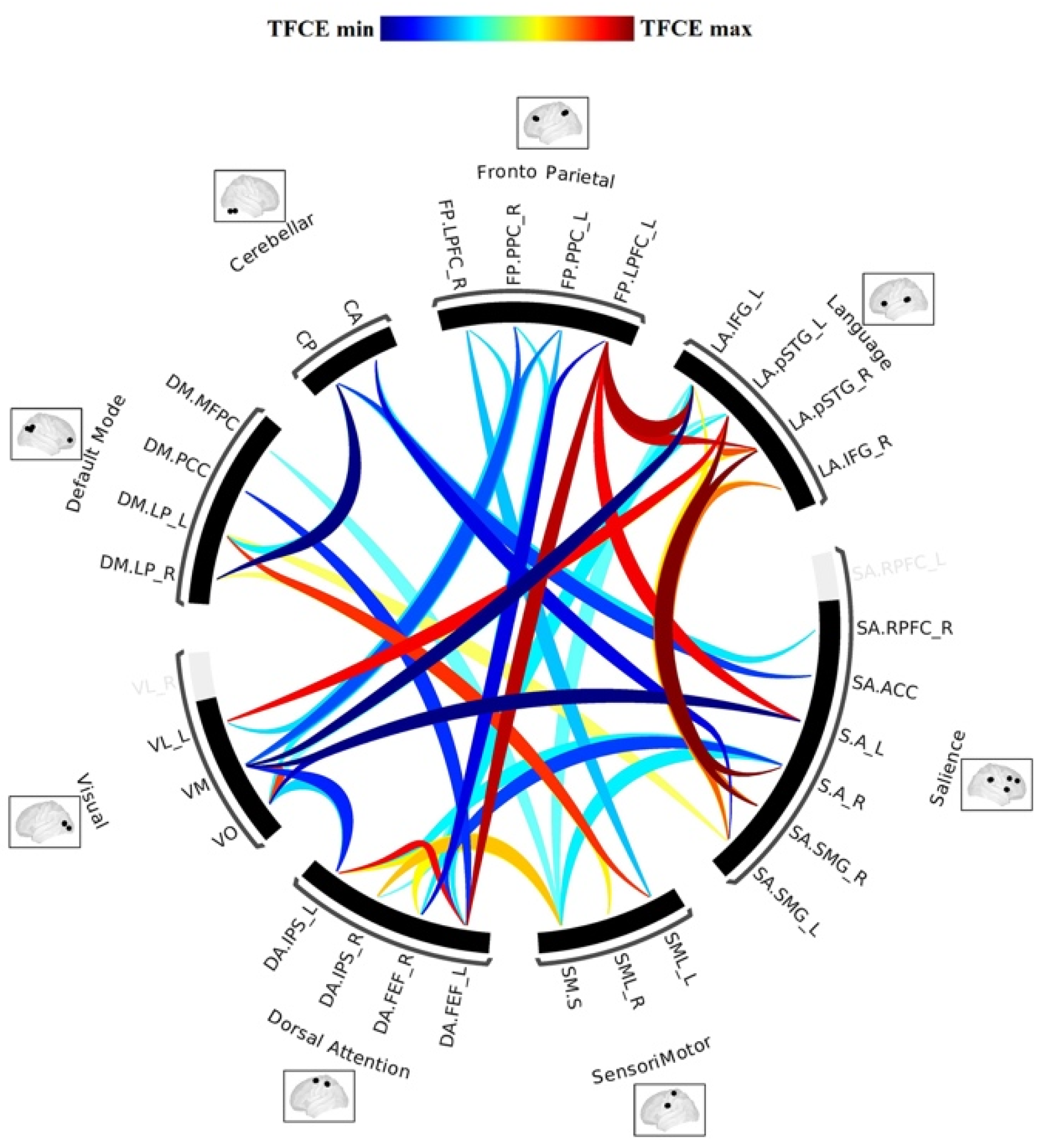
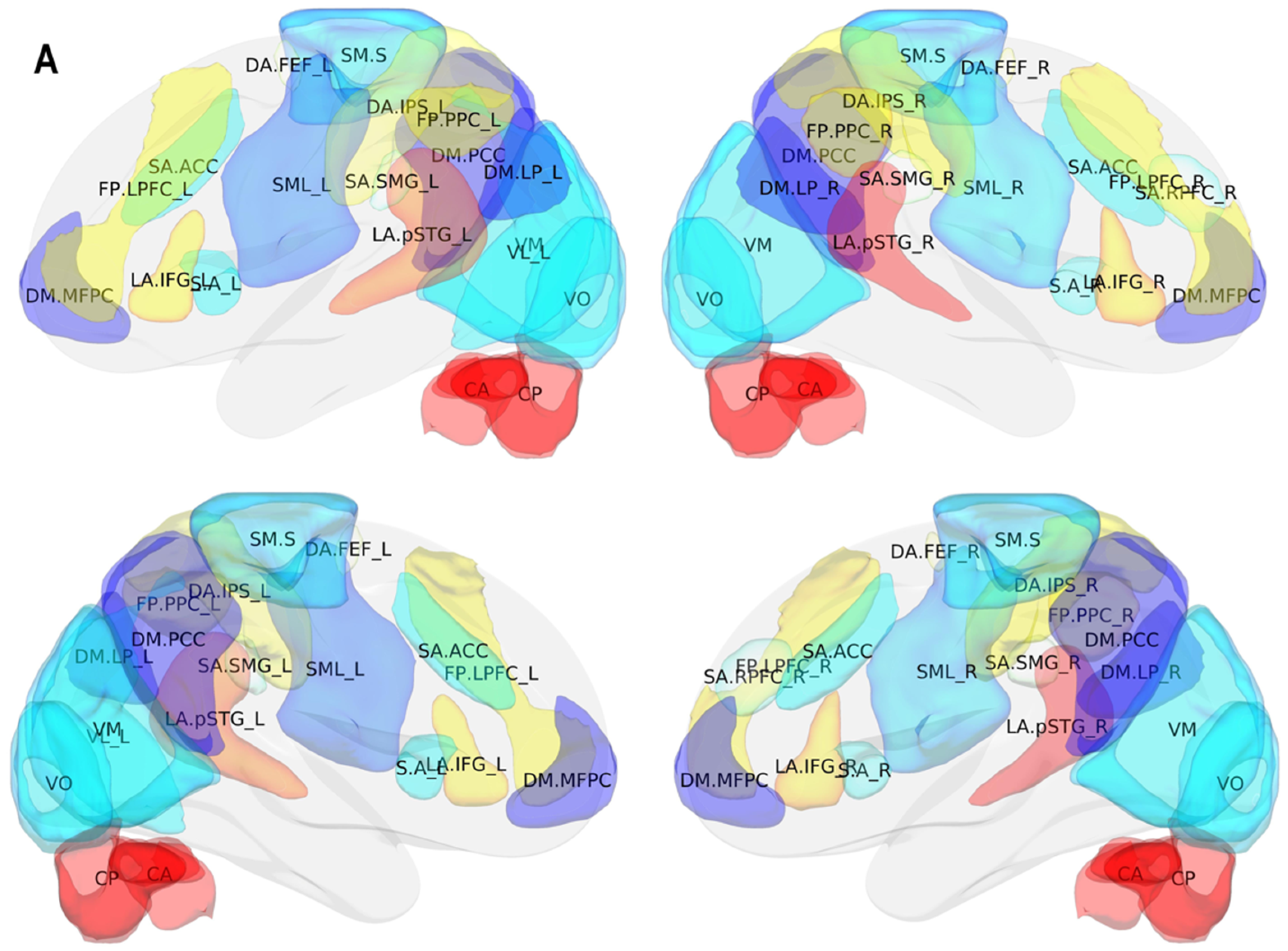
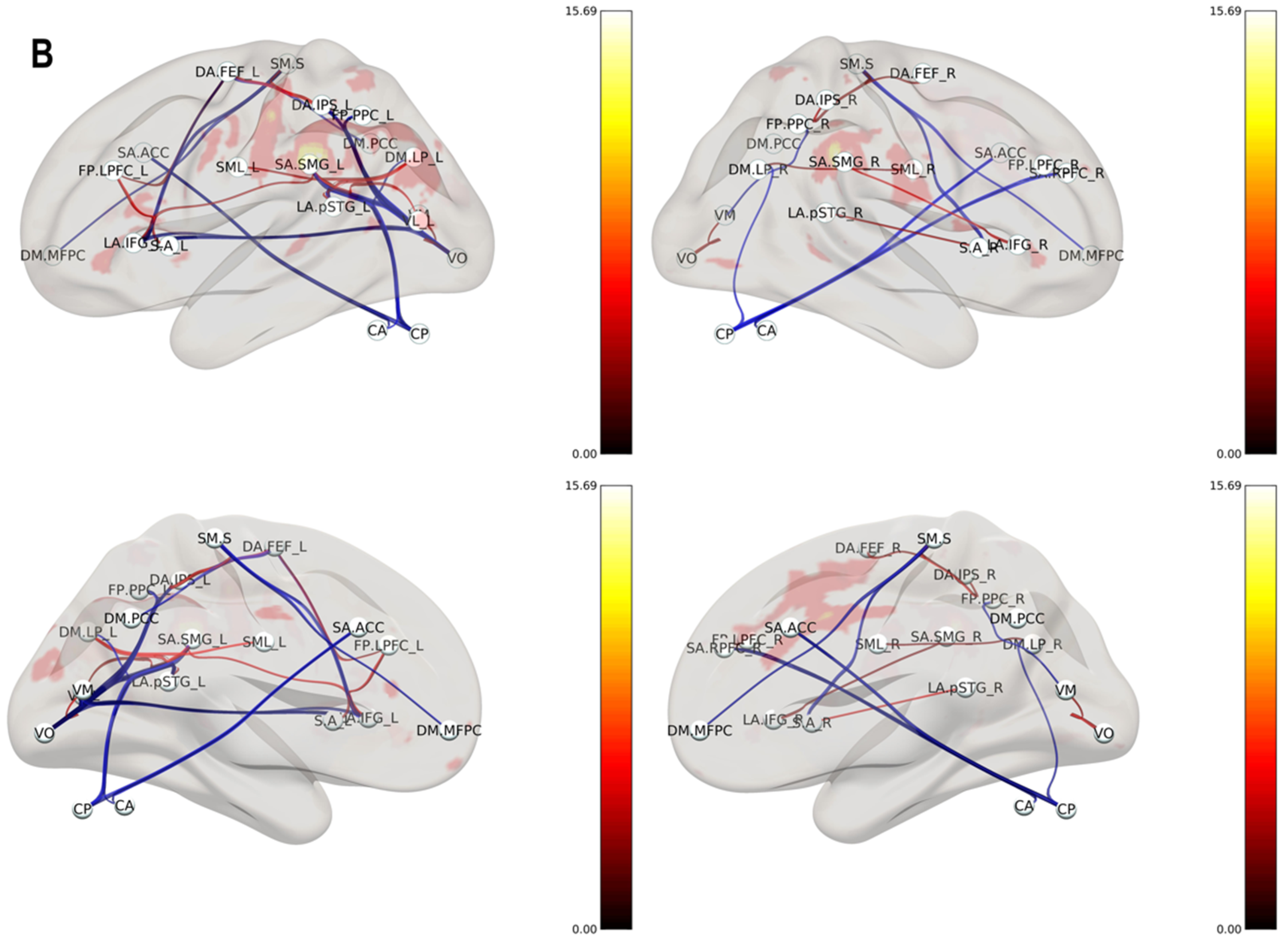
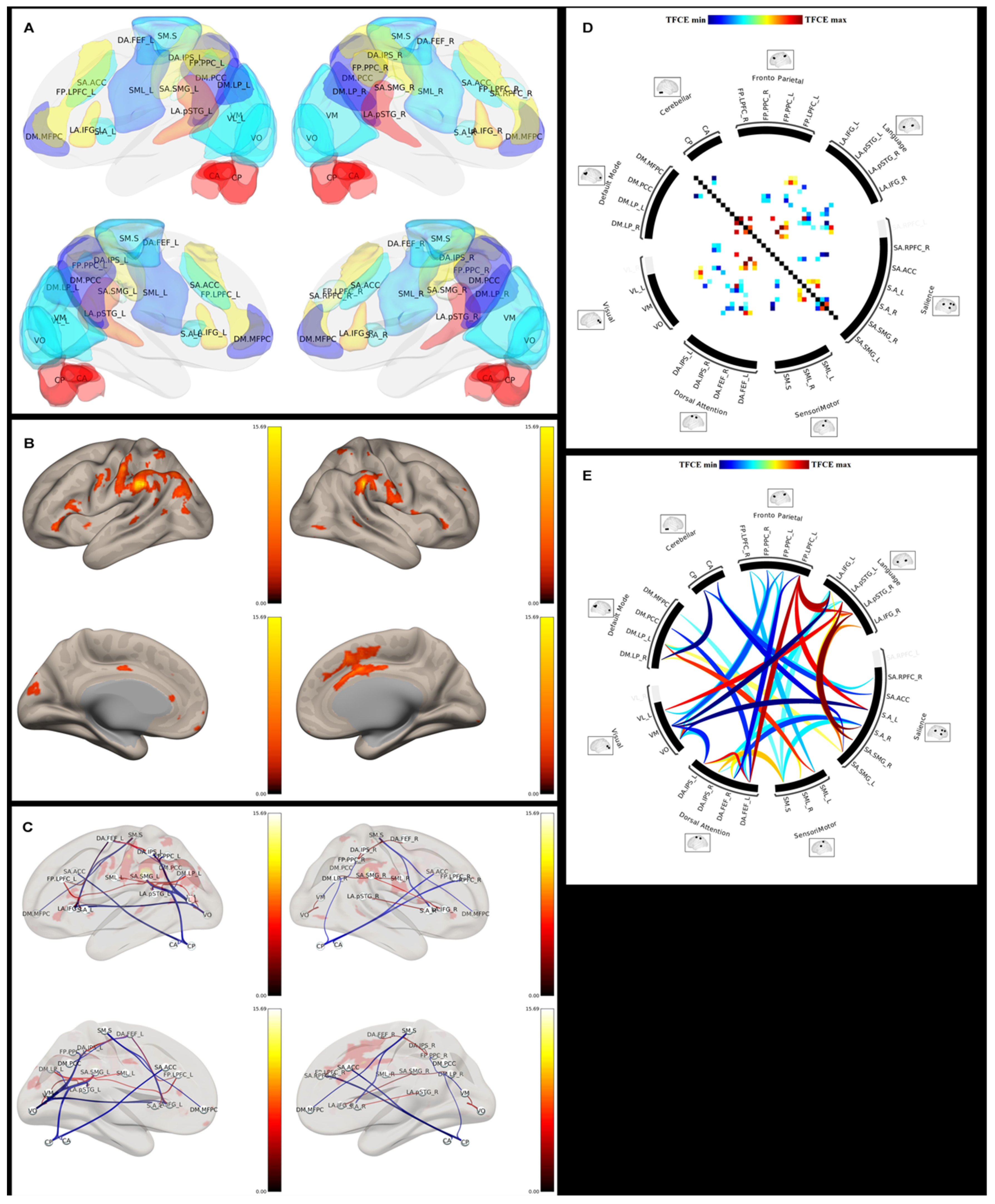
| Id | Extensive Name | Short Name | Id | Extensive Name | Short Name |
|---|---|---|---|---|---|
| 1 | DefaultMode.MPFC | DM.MFPC | 17 | Salience.SMG l | SA.SMG_L |
| 2 | DefaultMode.LP l | DM.LP_L | 18 | Salience.SMG r | SA.SMG_R |
| 3 | DefaultMode.LP r | DM.LP_R | 19 | DorsalAttention.FEF l | DA.FEF_L |
| 4 | DefaultMode.PCC | DM.PCC | 20 | DorsalAttention.FEF r | DA.FEF_R |
| 5 | SensoriMotor.Lateral l | SML_L | 21 | DorsalAttention.IPS l | DA.IPS_L |
| 6 | SensoriMotor.Lateral r | SML_R | 22 | DorsalAttention.IPS r | DA.IPS_R |
| 7 | SensoriMotor.Superior | SM.S | 23 | FrontoParietal.LPFC l | FP.LPFC_L |
| 8 | Visual.Medial | VM | 24 | FrontoParietal.PPC l | FP.PPC_L |
| 9 | Visual.Occipital | VO | 25 | FrontoParietal.LPFC r | FP.LPFC_R |
| 10 | Visual.Lateral l | VL_L | 26 | FrontoParietal.PPC r | FP.PPC_R |
| 11 | Visual.Lateral r | VL_R | 27 | Language.IFG l | LA.IFG_L |
| 12 | Salience.ACC | SA.ACC | 28 | Language.IFG r | LA.IFG_R |
| 13 | Salience.AInsula l | S.A_L | 29 | Language.pSTG l | LA.pSTG_L |
| 14 | Salience.AInsula r | S.A_R | 30 | Language.pSTG r | LA.pSTG_R |
| 15 | Salience.RPFC l | SA.RPFC_L | 31 | Cerebellar.Anterior | CA |
| 16 | Salience.RPFC r | SA.RPFC_R | 32 | Cerebellar.Posterior | CP |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sparacia, G.; Parla, G.; Mamone, G.; Caruso, M.; Torregrossa, F.; Grasso, G. Resting-State Functional Magnetic Resonance Imaging for Surgical Neuro-Oncology Planning: Towards a Standardization in Clinical Settings. Brain Sci. 2021, 11, 1613. https://doi.org/10.3390/brainsci11121613
Sparacia G, Parla G, Mamone G, Caruso M, Torregrossa F, Grasso G. Resting-State Functional Magnetic Resonance Imaging for Surgical Neuro-Oncology Planning: Towards a Standardization in Clinical Settings. Brain Sciences. 2021; 11(12):1613. https://doi.org/10.3390/brainsci11121613
Chicago/Turabian StyleSparacia, Gianvincenzo, Giuseppe Parla, Giuseppe Mamone, Mariangela Caruso, Fabio Torregrossa, and Giovanni Grasso. 2021. "Resting-State Functional Magnetic Resonance Imaging for Surgical Neuro-Oncology Planning: Towards a Standardization in Clinical Settings" Brain Sciences 11, no. 12: 1613. https://doi.org/10.3390/brainsci11121613