
Screening of Parkinson’s Disease Using Geometric Features Extracted from Spiral Drawings

 , , , , ,
, , , , ,
Abstract
:1. Introduction
1.1. Parkinson’s Disease Symptoms and Standard Diagnosis Methods
1.2. Advantages of Automation in Screening
1.3. Handwriting Analysis for Parkinson’s Disease
1.4. Archimedean Spiral Drawings for Diagnosis of Parkinson’s Disease
1.5. Our Study
2. Methods
2.1. The ParkinsonHW Dataset
2.2. Data Preprocessing
2.3. Feature Engineering
2.4. Feature Importance
2.5. Subject Classification
3. Results
3.1. Feature Selection
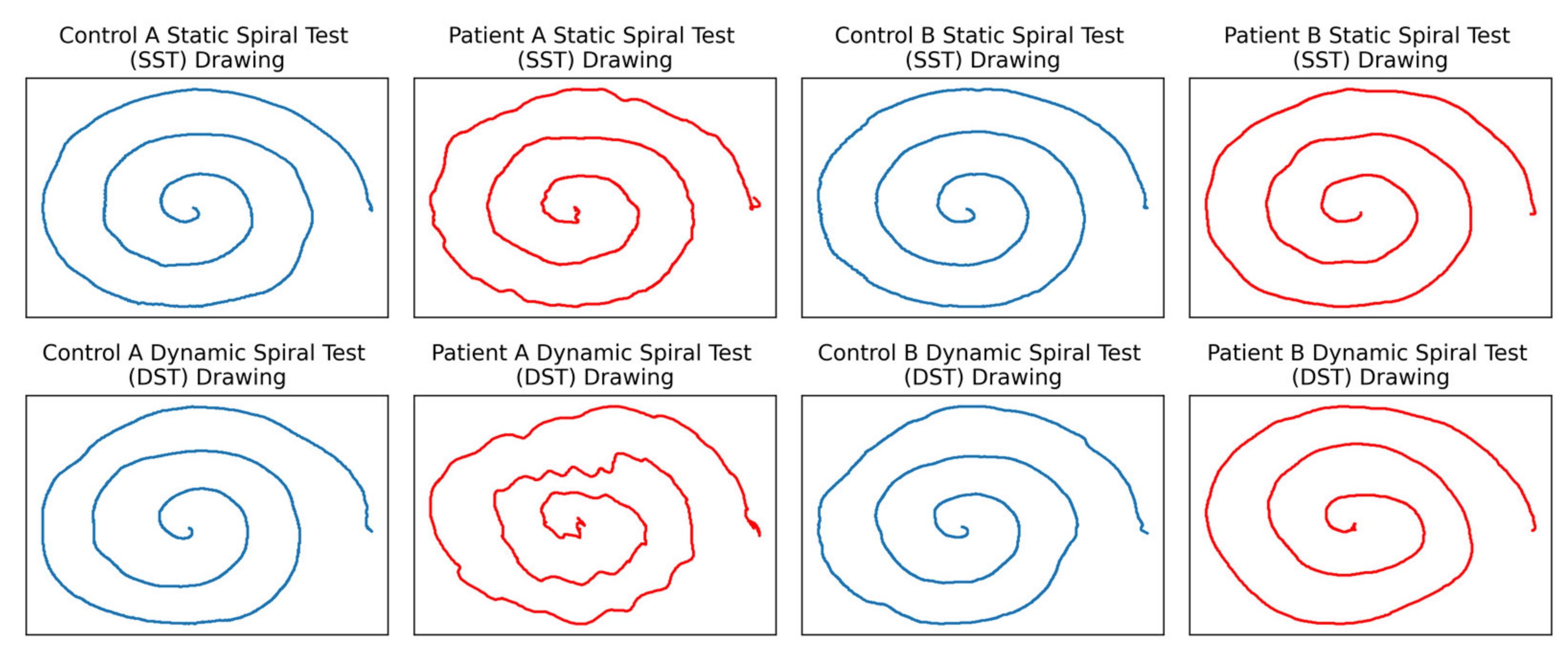
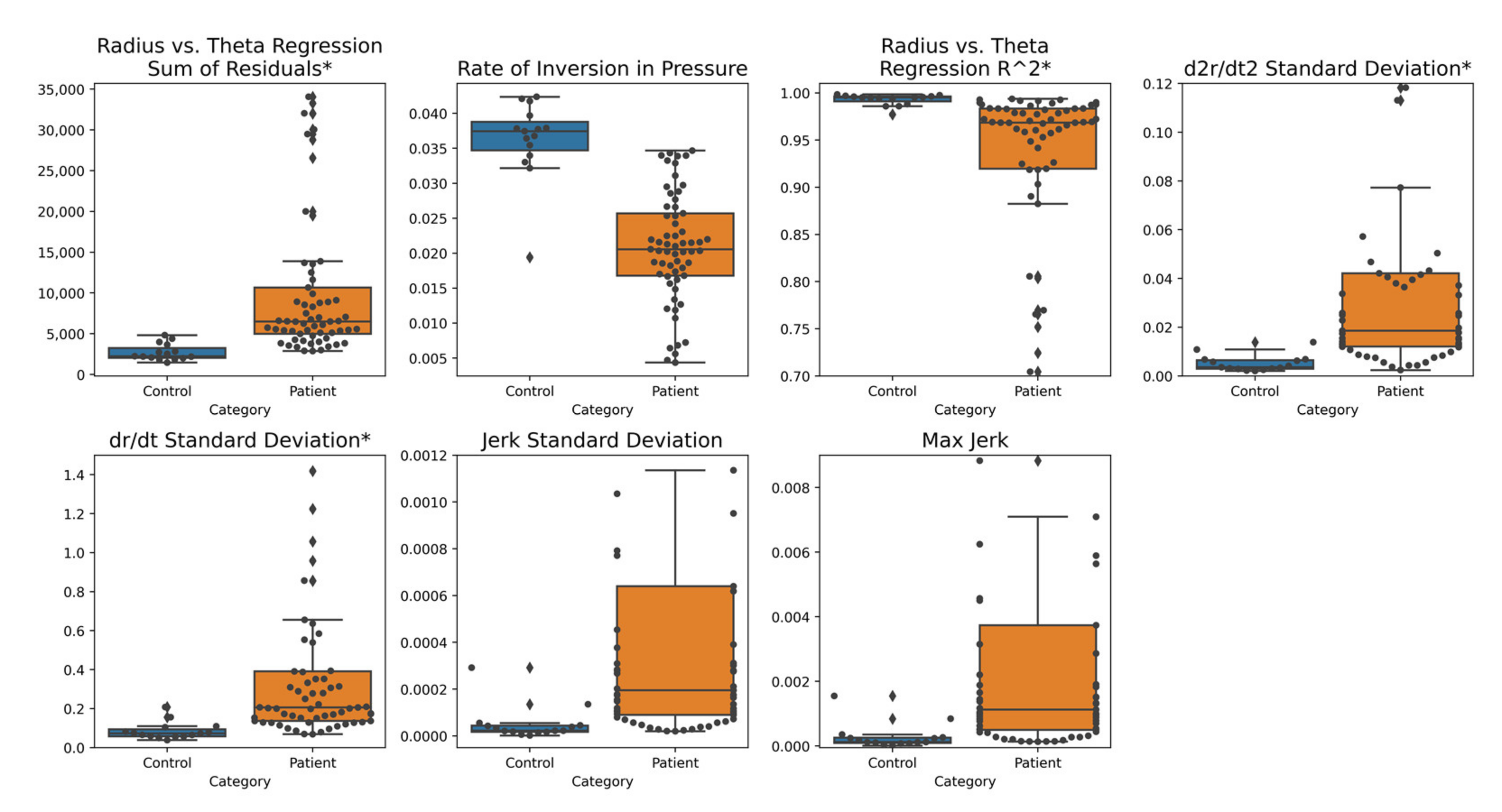
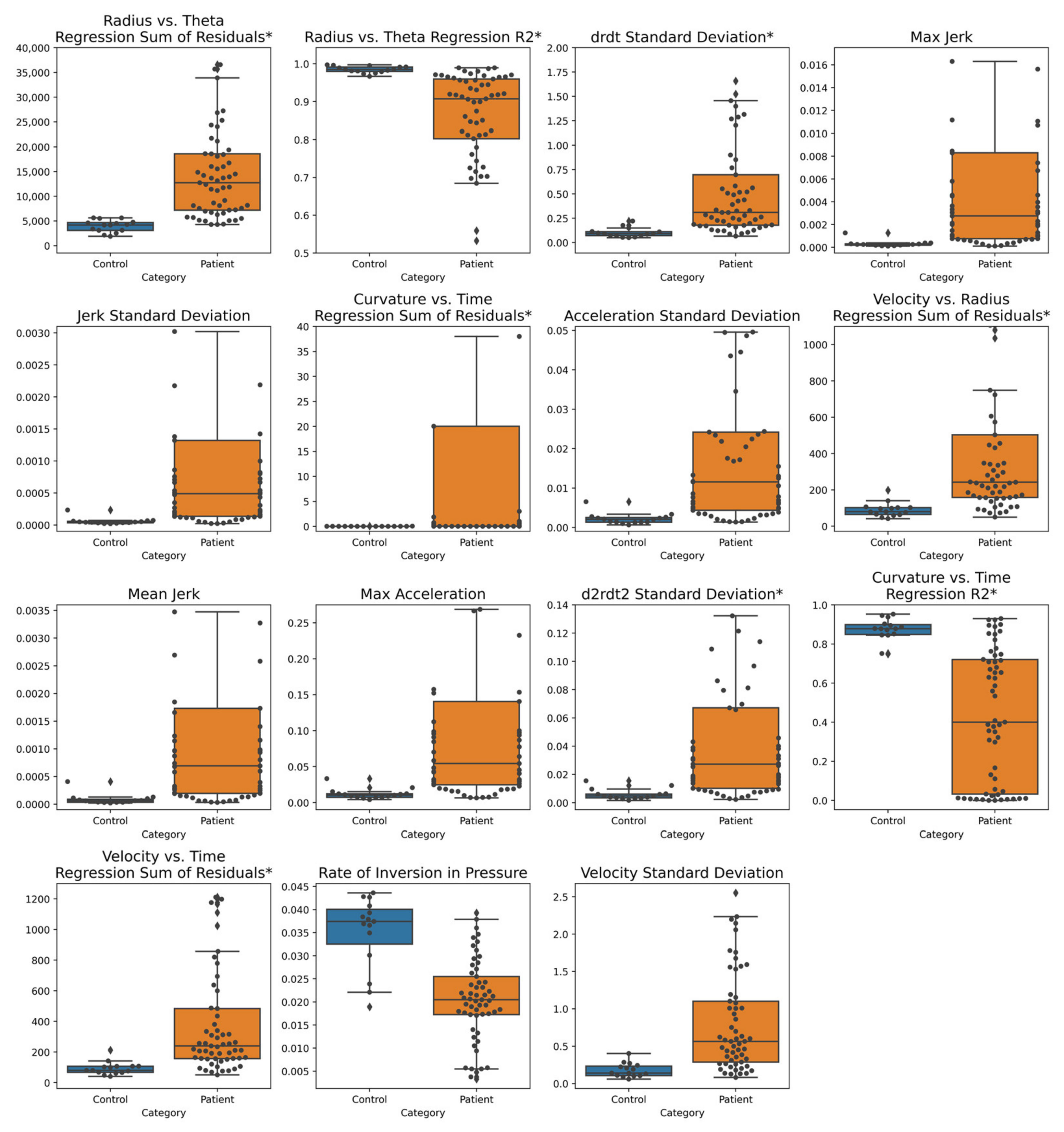
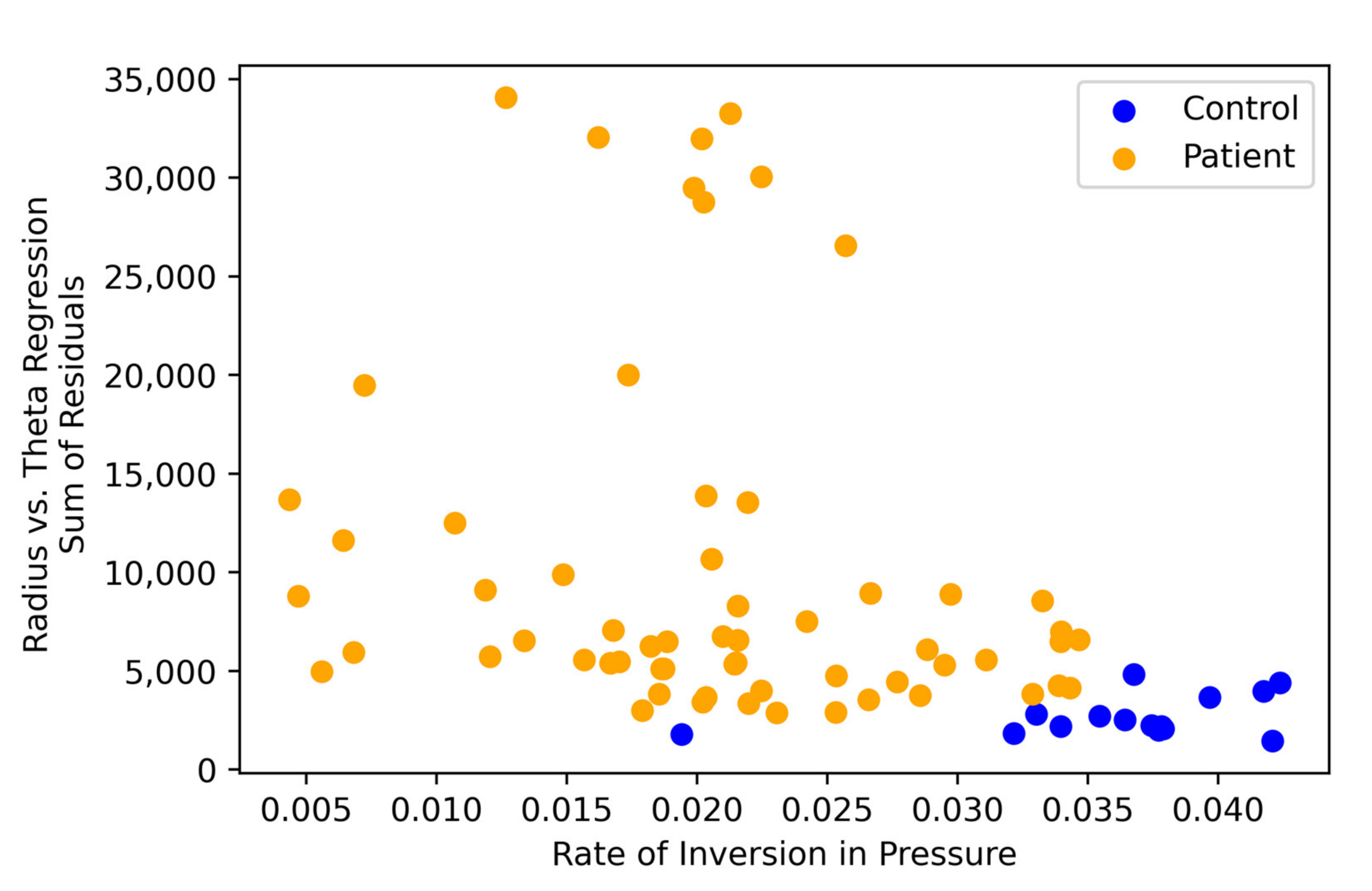
3.2. Feature Visualizations
3.3. Classification Results
4. Discussion
4.1. Discussion of Classification Results
4.1.1. Model Accuracy
4.1.2. Important Features
4.2. Future Diagnostic Recommendations
4.2.1. Drawing Shape Recommendations
4.2.2. Template for Drawing
4.2.3. Adaptive Framework
4.2.4. Task Variation
4.2.5. Data Sharing
4.2.6. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tarakad, A.; Jankovic, J. Diagnosis and Management of Parkinson’s Disease. Semin. Neurol. 2017, 37, 118–126. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS Clinical Diagnostic Criteria for Parkinson’s Disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale Presentation and Clinimetric Testing Results: MDS-UPDRS: Clinimetric Assessment. Mov. Disord. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]
- Goetz, C.G.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stebbins, G.T.; Stern, M.B.; Tilley, B.C.; Dodel, R.; Dubois, B.; et al. Movement Disorder Society-Sponsored Revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Process, Format, and Clinimetric Testing Plan. Mov. Disord. 2007, 22, 41–47. [Google Scholar] [CrossRef]
- AlMahadin, G.; Lotfi, A.; Zysk, E.; Siena, F.L.; Carthy, M.M.; Breedon, P. Parkinson’s Disease: Current Assessment Methods and Wearable Devices for Evaluation of Movement Disorder Motor Symptoms—A Patient and Healthcare Professional Perspective. BMC Neurol. 2020, 20, 419. [Google Scholar] [CrossRef] [PubMed]
- Van Rumund, A.; Aerts, M.B.; Esselink, R.A.J.; Meijer, F.J.A.; Verbeek, M.M.; Bloem, B.R. Parkinson’s Disease Diagnostic Observations (PADDO): Study Rationale and Design of a Prospective Cohort Study for Early Differentiation of Parkinsonism. BMC Neurol. 2018, 18, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jankovic, J. Parkinson’s Disease: Clinical Features and Diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef] [Green Version]
- Atarashi, R.; Sano, K.; Satoh, K.; Nishida, N. Real-Time Quaking-Induced Conversion: A Highly Sensitive Assay for Prion Detection. Prion 2011, 5, 150–153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gibbons, C.H.; Wang, N.; Freeman, R. Cutaneous Alpha-Synuclein From Paraffin Embedded Autopsy Specimens in Parkinson’s Disease. J. Park. Dis. 2017, 7, 503–509. [Google Scholar] [CrossRef] [Green Version]
- Espay, A.J.; Bonato, P.; Nahab, F.B.; Maetzler, W.; Dean, J.M.; Klucken, J.; Eskofier, B.M.; Merola, A.; Horak, F.; Lang, A.E.; et al. Technology in Parkinson’s Disease: Challenges and Opportunities: Technology in PD. Mov. Disord. 2016, 31, 1272–1282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singhal, B.S.; Khadilkar, S.V. Neurology in the Developing World. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2014; Volume 121, pp. 1773–1782. [Google Scholar] [CrossRef]
- Burton, A. How Do We Fix the Shortage of Neurologists? Lancet Neurol. 2018, 17, 502–503. [Google Scholar] [CrossRef] [Green Version]
- Smits, E.J.; Tolonen, A.J.; Cluitmans, L.; van Gils, M.; Conway, B.A.; Zietsma, R.C.; Leenders, K.L.; Maurits, N.M. Standardized Handwriting to Assess Bradykinesia, Micrographia and Tremor in Parkinson’s Disease. PLoS ONE 2014, 9, e97614. [Google Scholar] [CrossRef]
- Cobbah, W.G.K.; Fairhurst, M.C. Computer Analysis of Handwriting Dynamics during Dopamimetic Tests in Parkinson’s Disease. In Proceedings of the 26th Euromicro Conference. EUROMICRO 2000. Informatics: Inventing the Future, Maastricht, The Netherlands, 5–7 September 2000; Volume 2, pp. 414–418. [Google Scholar] [CrossRef]
- Impedovo, D.; Pirlo, G. Automatic Signature Verification: The State of the Art. IEEE Trans. Syst. Man Cybern. Part C Appl. Rev. 2008, 38, 609–635. [Google Scholar] [CrossRef] [Green Version]
- Impedovo, D.; Pirlo, G. Dynamic Handwriting Analysis for the Assessment of Neurodegenerative Diseases: A Pattern Recognition Perspective. IEEE Rev. Biomed. Eng. 2019, 12, 209–220. [Google Scholar] [CrossRef]
- Pan, G.D.; Stern, Y.; Sano, M.; Mayeux, R. Clock-Drawing in Neurological Disorders. Behav. Neurol. 1989, 2, 39–48. [Google Scholar] [CrossRef]
- Rentz, D.M.; Papp, K.V.; Mayblyum, D.V.; Sanchez, J.S.; Klein, H.; Souillard-Mandar, W.; Sperling, R.A.; Johnson, K.A. Association of Digital Clock Drawing With PET Amyloid and Tau Pathology in Normal Older Adults. Neurology 2021, 96, e1844–e1854. [Google Scholar] [CrossRef]
- Rosenblum, S.; Samuel, M.; Zlotnik, S.; Erikh, I.; Schlesinger, I. Handwriting as an Objective Tool for Parkinson’s Disease Diagnosis. J. Neurol. 2013, 260, 2357–2361. [Google Scholar] [CrossRef]
- Thomas, M.; Lenka, A.; Kumar Pal, P. Handwriting Analysis in Parkinson’s Disease: Current Status and Future Directions. Mov. Disord. Clin. Pract. 2017, 4, 806–818. [Google Scholar] [CrossRef]
- Diaz, M.; Moetesum, M.; Siddiqi, I.; Vessio, G. Sequence-Based Dynamic Handwriting Analysis for Parkinson’s Disease Detection with One-Dimensional Convolutions and BiGRUs. Expert Syst. Appl. 2021, 168, 114405. [Google Scholar] [CrossRef]
- Eichhorn, T.E.; Gasser, T.; Mai, N.; Marquardt, C.; Arnold, G.; Schwarz, J.; Oertel, W.H. Computational Analysis of Open Loop Handwriting Movements in Parkinson’s Disease: A Rapid Method to Detect Dopamimetic Effects. Mov. Disord. 1996, 11, 289–297. [Google Scholar] [CrossRef]
- Randhawa, B.K.; Farley, B.G.; Boyd, L.A. Repetitive Transcranial Magnetic Stimulation Improves Handwriting in Parkinson’s Disease. Park. Dis. 2013, 2013, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Galli, M.; Vimercati, S.L.; Manetti, E.; Cimolin, V.; Albertini, G.; De Pandis, M.F. Spiral Analysis in Subjects with Parkinson’s Disease before and after Levodopa Treatment: A New Protocol with Stereophotogrammetric Systems. J. Appl. Biomater. Funct. Mater. 2014, 12, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Westin, J.; Dougherty, M.; Nyholm, D.; Groth, T. A Home Environment Test Battery for Status Assessment in Patients with Advanced Parkinson’s Disease. Comput. Methods Programs Biomed. 2010, 98, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Danna, J.; Velay, J.-L.; Eusebio, A.; Véron-Delor, L.; Witjas, T.; Azulay, J.-P.; Pinto, S. Digitalized Spiral Drawing in Parkinson’s Disease: A Tool for Evaluating beyond the Written Trace. Hum. Mov. Sci. 2019, 65, 80–88. [Google Scholar] [CrossRef]
- Stanley, K.; Hagenah, J.; Brüggemann, N.; Reetz, K.; Severt, L.; Klein, C.; Yu, Q.; Derby, C.; Pullman, S.; Saunders-Pullman, R. Digitized Spiral Analysis Is a Promising Early Motor Marker for Parkinson Disease. Parkinsonism Relat. Disord. 2010, 16, 233–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drotár, P.; Mekyska, J.; Rektorová, I.; Masarová, L.; Smékal, Z.; Faundez-Zanuy, M. Evaluation of Handwriting Kinematics and Pressure for Differential Diagnosis of Parkinson’s Disease. Artif. Intell. Med. 2016, 67, 39–46. [Google Scholar] [CrossRef]
- Chakraborty, S.; Aich, S.; Jong-Seong-Sim; Han, E.; Park, J.; Kim, H.-C. Parkinson’s Disease Detection from Spiral and Wave Drawings Using Convolutional Neural Networks: A Multistage Classifier Approach. In Proceedings of the 2020 22nd International Conference on Advanced Communication Technology (ICACT), Phoenix Park, Korea, 16–19 February 2020; pp. 298–303. [Google Scholar] [CrossRef]
- Cantürk, İ. Fuzzy Recurrence Plot-Based Analysis of Dynamic and Static Spiral Tests of Parkinson’s Disease Patients. Neural Comput. Appl. 2021, 33, 349–360. [Google Scholar] [CrossRef]
- Cavaliere, F.; Cioppa, A.D.; Marcelli, A.; Parziale, A.; Senatore, R. Parkinson’s Disease Diagnosis: Towards Grammar-Based Explainable Artificial Intelligence. In Proceedings of the 2020 IEEE Symposium on Computers and Communications (ISCC), Rennes, France, 7–10 July 2020; pp. 1–6. [Google Scholar] [CrossRef]
- Kurt, I.; Ulukaya, S.; Erdem, O. Classification of Parkinson’s Disease Using Dynamic Time Warping. In Proceedings of the 2019 27th Telecommunications Forum (TELFOR), Belgrade, Serbia, 26–27 November 2019; pp. 1–4. [Google Scholar] [CrossRef]
- Gil-Martín, M.; Montero, J.M.; San-Segundo, R. Parkinson’s Disease Detection from Drawing Movements Using Convolutional Neural Networks. Electronics 2019, 8, 907. [Google Scholar] [CrossRef] [Green Version]
- Parziale, A.; Senatore, R.; Della Cioppa, A.; Marcelli, A. Cartesian Genetic Programming for Diagnosis of Parkinson Disease through Handwriting Analysis: Performance vs. Interpretability Issues. Artif. Intell. Med. 2021, 111, 101984. [Google Scholar] [CrossRef]
- Castrillon, R.; Acien, A.; Orozco-Arroyave, J.R.; Morales, A.; Vargas, J.F.; Vera-Rodriguez, R.; Fierrez, J.; Ortega-Garcia, J.; Villegas, A. Characterization of the Handwriting Skills as a Biomarker for Parkinson’s Disease. In Proceedings of the 2019 14th IEEE International Conference on Automatic Face & Gesture Recognition (FG 2019), Lille, France, 14–18 May 2019; pp. 1–5. [Google Scholar] [CrossRef]
- Zham, P.; Arjunan, S.P.; Raghav, S.; Kumar, D.K. Efficacy of Guided Spiral Drawing in the Classification of Parkinson’s Disease. IEEE J. Biomed. Health Inform. 2018, 22, 1648–1652. [Google Scholar] [CrossRef] [PubMed]
- San Luciano, M.; Wang, C.; Ortega, R.A.; Yu, Q.; Boschung, S.; Soto-Valencia, J.; Bressman, S.B.; Lipton, R.B.; Pullman, S.; Saunders-Pullman, R. Digitized Spiral Drawing: A Possible Biomarker for Early Parkinson’s Disease. PLoS ONE 2016, 11, e0162799. [Google Scholar] [CrossRef] [Green Version]
- Kamble, M.; Shrivastava, P.; Jain, M. Digitized Spiral Drawing Classification for Parkinson’s Disease Diagnosis. Meas. Sens. 2021, 16, 100047. [Google Scholar] [CrossRef]
- Saunders-Pullman, R.; Derby, C.; Stanley, K.; Floyd, A.; Bressman, S.; Lipton, R.B.; Deligtisch, A.; Severt, L.; Yu, Q.; Kurtis, M.; et al. Validity of Spiral Analysis in Early Parkinson’s Disease. Mov. Disord. 2008, 23, 531–537. [Google Scholar] [CrossRef]
- Alty, J.; Cosgrove, J.; Thorpe, D.; Kempster, P. How to Use Pen and Paper Tasks to Aid Tremor Diagnosis in the Clinic. Pract. Neurol. 2017, 17, 456–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, P.-C.; Chen, K.-H.; Yang, B.-S.; Chen, Y.-J. A Digital Assessment System for Evaluating Kinetic Tremor in Essential Tremor and Parkinson’s Disease. BMC Neurol. 2018, 18, 25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zham, P.; Kumar, D.K.; Dabnichki, P.; Poosapadi Arjunan, S.; Raghav, S. Distinguishing Different Stages of Parkinson’s Disease Using Composite Index of Speed and Pen-Pressure of Sketching a Spiral. Front. Neurol. 2017, 8, 435. [Google Scholar] [CrossRef] [PubMed]
- Isenkul, M.E.; Sakar, B.E.; Kursun, O. Improved Spiral Test Using Digitized Graphics Tablet for Monitoring Parkinson’s Disease. In Proceedings of the 2nd International Conference on E-Health and TeleMedicine—ICEHTM 2014, Istanbul, Turkey, 22–24 May 2014. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef] [Green Version]
- Rasnake, D. Wacom Cintiq 12WX Pen Display Review. DigitalCameraReview. Available online: http://www.digitalcamerareview.com/review/wacom-cintiq-12wx-pen-display-review/ (accessed on 17 August 2021).
- Lee, H.J.; Lee, W.W.; Kim, S.K.; Park, H.; Jeon, H.S.; Kim, H.B.; Jeon, B.S.; Park, K.S. Tremor Frequency Characteristics in Parkinson’s Disease under Resting-State and Stress-State Conditions. J. Neurol. Sci. 2016, 362, 272–277. [Google Scholar] [CrossRef]
- Souillard-Mandar, W.; Davis, R.; Rudin, C.; Au, R.; Libon, D.J.; Swenson, R.; Price, C.C.; Lamar, M.; Penney, D.L. Learning Classification Models of Cognitive Conditions from Subtle Behaviors in the Digital Clock Drawing Test. Mach. Learn. 2016, 102, 393–441. [Google Scholar] [CrossRef]
- Seitz, D.P.; Chan, C.C.; Newton, H.T.; Gill, S.S.; Herrmann, N.; Smailagic, N.; Nikolaou, V.; Fage, B.A. Mini-Cog for the Diagnosis of Alzheimer’s Disease Dementia and Other Dementias within a Primary Care Setting. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef]
- Kotsavasiloglou, C.; Kostikis, N.; Hristu-Varsakelis, D.; Arnaoutoglou, M. Machine Learning-Based Classification of Simple Drawing Movements in Parkinson’s Disease. Biomed. Signal Process. Control 2017, 31, 174–180. [Google Scholar] [CrossRef]
- Lonini, L.; Dai, A.; Shawen, N.; Simuni, T.; Poon, C.; Shimanovich, L.; Daeschler, M.; Ghaffari, R.; Rogers, J.A.; Jayaraman, A. Wearable Sensors for Parkinson’s Disease: Which Data Are Worth Collecting for Training Symptom Detection Models. NPJ Digit. Med. 2018, 1, 64. [Google Scholar] [CrossRef] [PubMed]
- Watson, G.S.; Leverenz, J.B. Profile of Cognitive Impairment in Parkinson’s Disease. Brain Pathol. Zurich Switz. 2010, 20, 640–645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeMaagd, G.; Philip, A. Parkinson’s Disease and Its Management: Part 1: Disease Entity, Risk Factors, Pathophysiology, Clinical Presentation, and Diagnosis. Pharm. Ther. Peer-Rev. J. Formul. Manag. 2015, 40, 504–532. [Google Scholar]
- Bloem, B.R.; Okun, M.S.; Klein, C. Parkinson’s Disease. Lancet 2021, 397, 2284–2303. [Google Scholar] [CrossRef]
- Stegemöller, E.L.; Zaman, A.; Uzochukwu, J. Repetitive Finger Movement and Circle Drawing in Persons with Parkinson’s Disease. PLoS ONE 2019, 14, e0222862. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.G.; Marsden, C.D. Dual Task Performance and Processing Resources in Normal Subjects and Patients with Parkinson’s Disease. Brain J. Neurol. 1991, 114 Pt 1A, 215–231. [Google Scholar]
- Panch, T.; Mattie, H.; Celi, L.A. The “Inconvenient Truth” about AI in Healthcare. NPJ Digit. Med. 2019, 2, 77. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Harrell, F.E. Prediction Models Need Appropriate Internal, Internal–External, and External Validation. J. Clin. Epidemiol. 2016, 69, 245–247. [Google Scholar] [CrossRef] [Green Version]
- Datasets|Parkinson’s Disease. Available online: https://www.michaeljfox.org/data-sets (accessed on 23 August 2021).
- Ali, K.; Morris, H.R. Parkinson’s Disease: Chameleons and Mimics. Pract. Neurol. 2015, 15, 14–25. [Google Scholar] [CrossRef] [Green Version]
- Thanawattano, C.; Pongthornseri, R.; Anan, C.; Dumnin, S.; Bhidayasiri, R. Temporal Fluctuations of Tremor Signals from Inertial Sensor: A Preliminary Study in Differentiating Parkinson’s Disease from Essential Tremor. Biomed. Eng. OnLine 2015, 14, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kikuchi, A.; Baba, T.; Hasegawa, T.; Sugeno, N.; Konno, M.; Takeda, A. Differentiating Parkinson’s Disease from Multiple System Atrophy by [123I] Meta-Iodobenzylguanidine Myocardial Scintigraphy and Olfactory Test. Parkinsonism Relat. Disord. 2011, 17, 698–700. [Google Scholar] [CrossRef] [PubMed]
- Ghaemi, M. Differentiating Multiple System Atrophy from Parkinson’s Disease: Contribution of Striatal and Midbrain MRI Volumetry and Multi-Tracer PET Imaging. J. Neurol. Neurosurg. Psychiatry 2002, 73, 517–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ling, H.; Massey, L.A.; Lees, A.J.; Brown, P.; Day, B.L. Hypokinesia without Decrement Distinguishes Progressive Supranuclear Palsy from Parkinson’s Disease. Brain 2012, 135, 1141–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amboni, M.; Ricciardi, C.; Picillo, M.; De Santis, C.; Ricciardelli, G.; Abate, F.; Tepedino, M.F.; D’Addio, G.; Cesarelli, G.; Volpe, G.; et al. Gait Analysis May Distinguish Progressive Supranuclear Palsy and Parkinson Disease since the Earliest Stages. Sci. Rep. 2021, 11, 9297. [Google Scholar] [CrossRef]
- Foguem, C.; Manckoundia, P. Lewy Body Disease: Clinical and Pathological “Overlap Syndrome” Between Synucleinopathies (Parkinson Disease) and Tauopathies (Alzheimer Disease). Curr. Neurol. Neurosci. Rep. 2018, 18, 24. [Google Scholar] [CrossRef]
- Cahn-Weiner, D.A.; Williams, K.; Grace, J.; Tremont, G.; Westervelt, H.; Stern, R.A. Discrimination of Dementia with Lewy Bodies From Alzheimer Disease and Parkinson Disease Using the Clock Drawing Test. Cogn. Behav. Neurol. 2003, 16, 85–92. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| p-Value Cutoff | AUC Cutoff | |
|---|---|---|
| Static Drawing |
|
|
| Dynamic Drawing |
|
|
| Features | Static AUC | Dynamic AUC |
|---|---|---|
| Rate of Inversion in Pressure, Radius vs. Theta Regression Sum of Residuals | 0.999 | 0.975 |
| Curvature vs. Time Regression Sum of Residuals, Radius vs. Theta Regression Sum of Residuals | 0.894 | 0.996 |
| Rate of Inversion in Pressure | 0.934 | 0.779 |
| Radius vs. Theta Regression R2 | 0.910 | 0.906 |
| Radius vs. Theta Regression Sum of Residuals | 0.887 | 0.956 |
| Curvature vs. Time Regression Sum of Residuals | 0.666 | 0.911 |
| Velocity vs. Radius Regression Sum of Residuals | 0.675 | 0.843 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chandra, J.; Muthupalaniappan, S.; Shang, Z.; Deng, R.; Lin, R.; Tolkova, I.; Butts, D.; Sul, D.; Marzouk, S.; Bose, S.; et al. Screening of Parkinson’s Disease Using Geometric Features Extracted from Spiral Drawings. Brain Sci. 2021, 11, 1297. https://doi.org/10.3390/brainsci11101297
Chandra J, Muthupalaniappan S, Shang Z, Deng R, Lin R, Tolkova I, Butts D, Sul D, Marzouk S, Bose S, et al. Screening of Parkinson’s Disease Using Geometric Features Extracted from Spiral Drawings. Brain Sciences. 2021; 11(10):1297. https://doi.org/10.3390/brainsci11101297
Chicago/Turabian StyleChandra, Jay, Siva Muthupalaniappan, Zisheng Shang, Richard Deng, Raymond Lin, Irina Tolkova, Dignity Butts, Daniel Sul, Sammer Marzouk, Soham Bose, and et al. 2021. "Screening of Parkinson’s Disease Using Geometric Features Extracted from Spiral Drawings" Brain Sciences 11, no. 10: 1297. https://doi.org/10.3390/brainsci11101297