High-Performance PMN-PT Single-Crystal-Based 1-3 Composite Transducer Integrated with a Biopsy Needle

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
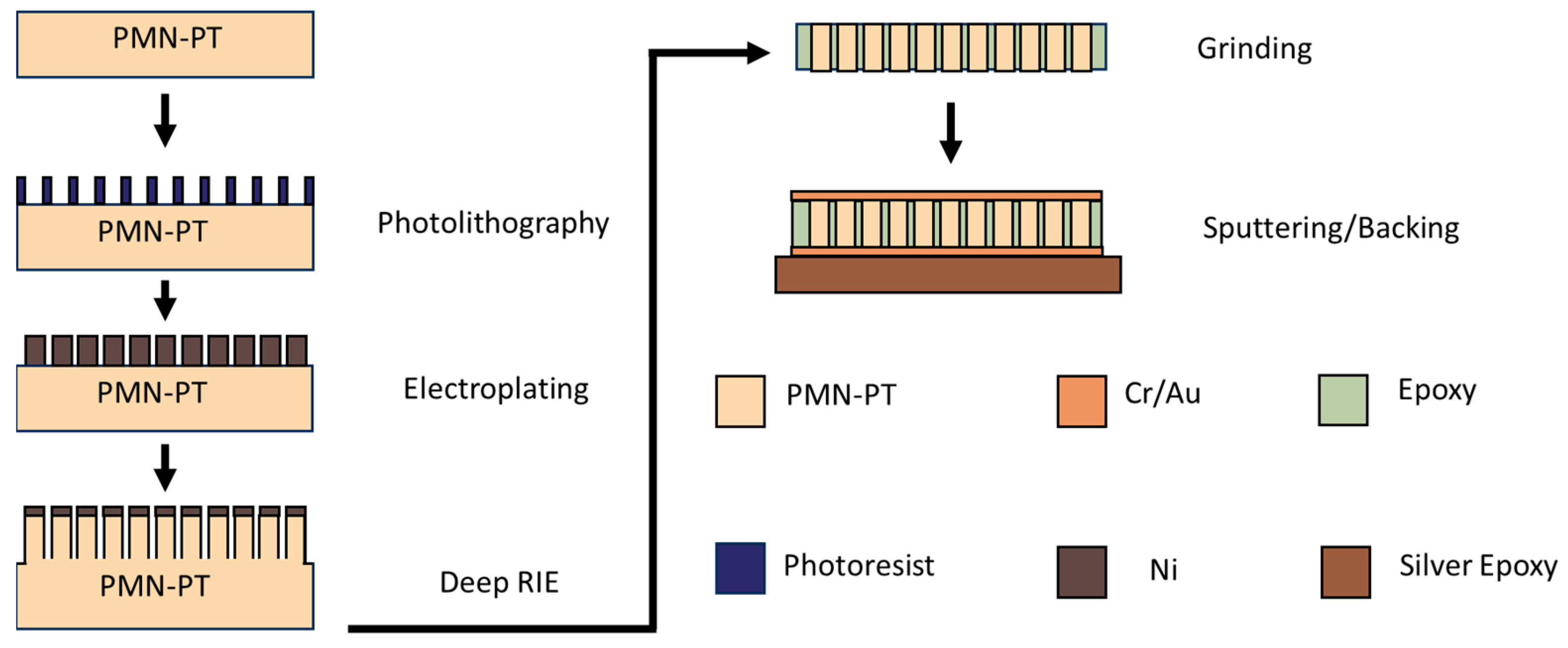
2.1. PMN-PT 1-3 Composite Design and Fabrication
2.2. 50 MHz 1-3 Composite Transducer Design and Fabrication
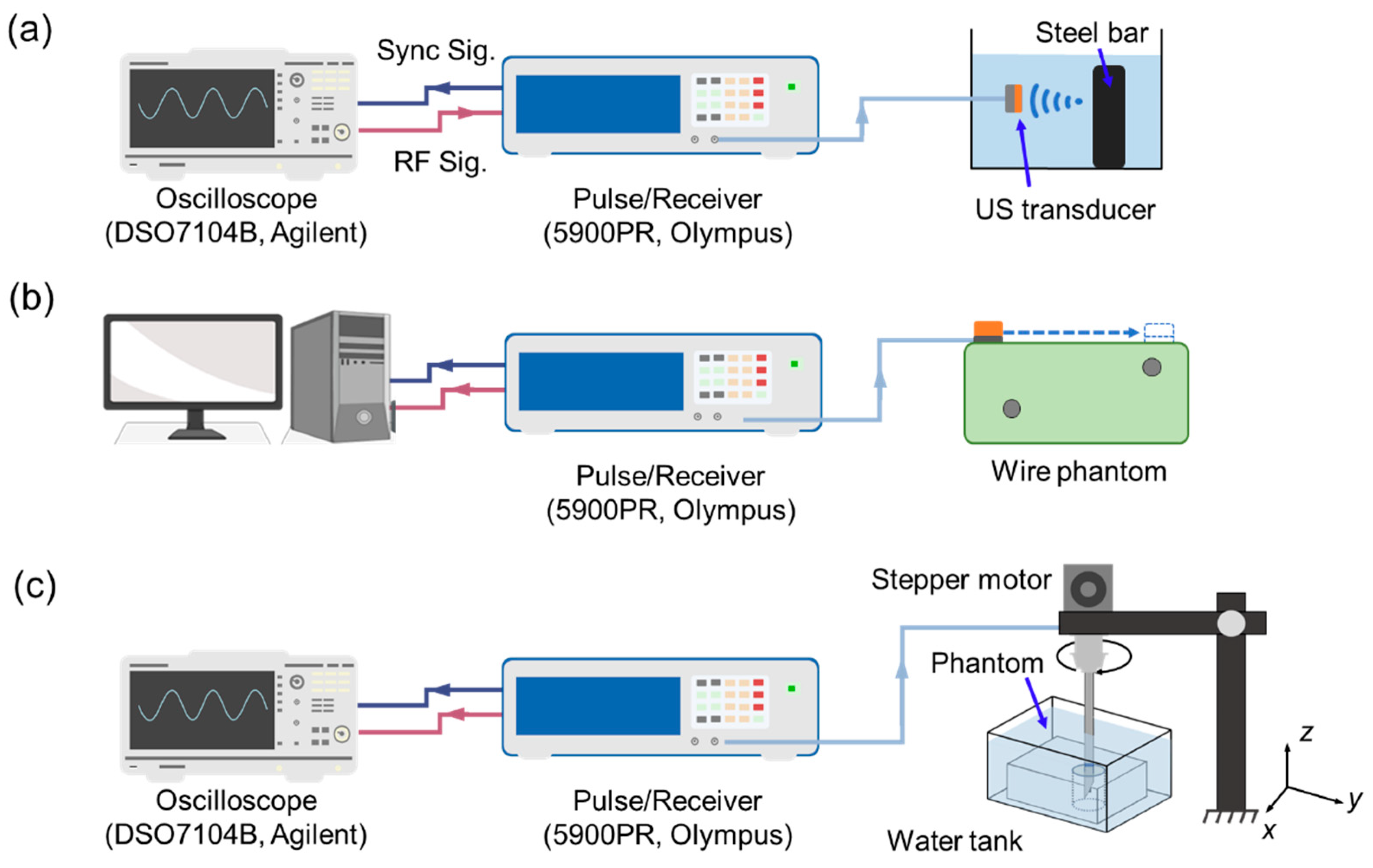
2.3. Transducer Characterization
2.4. Tissue-Mimicking Phantom Preparation
2.5. Tissue-Mimicking Phantom Testing
3. Results
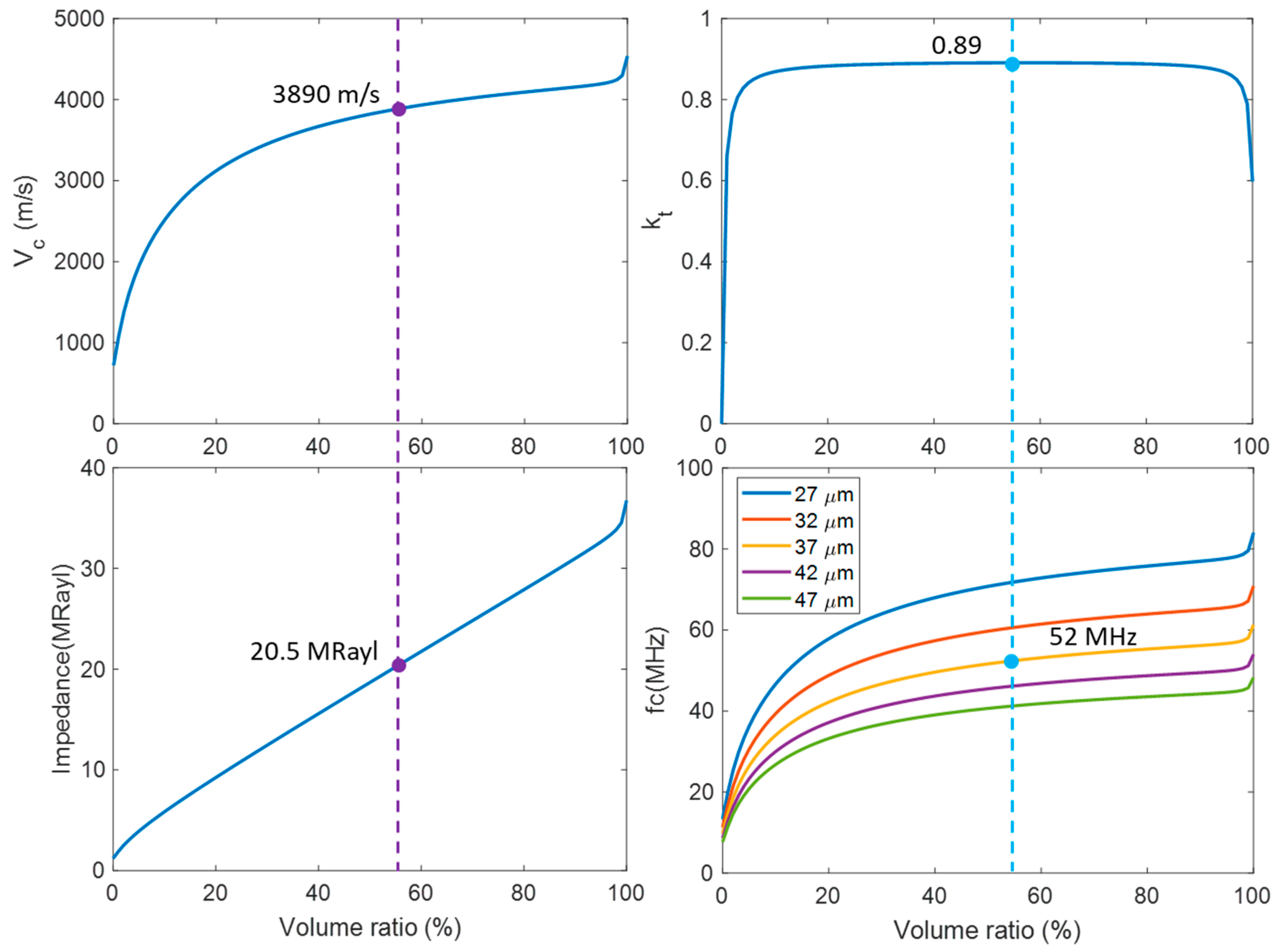
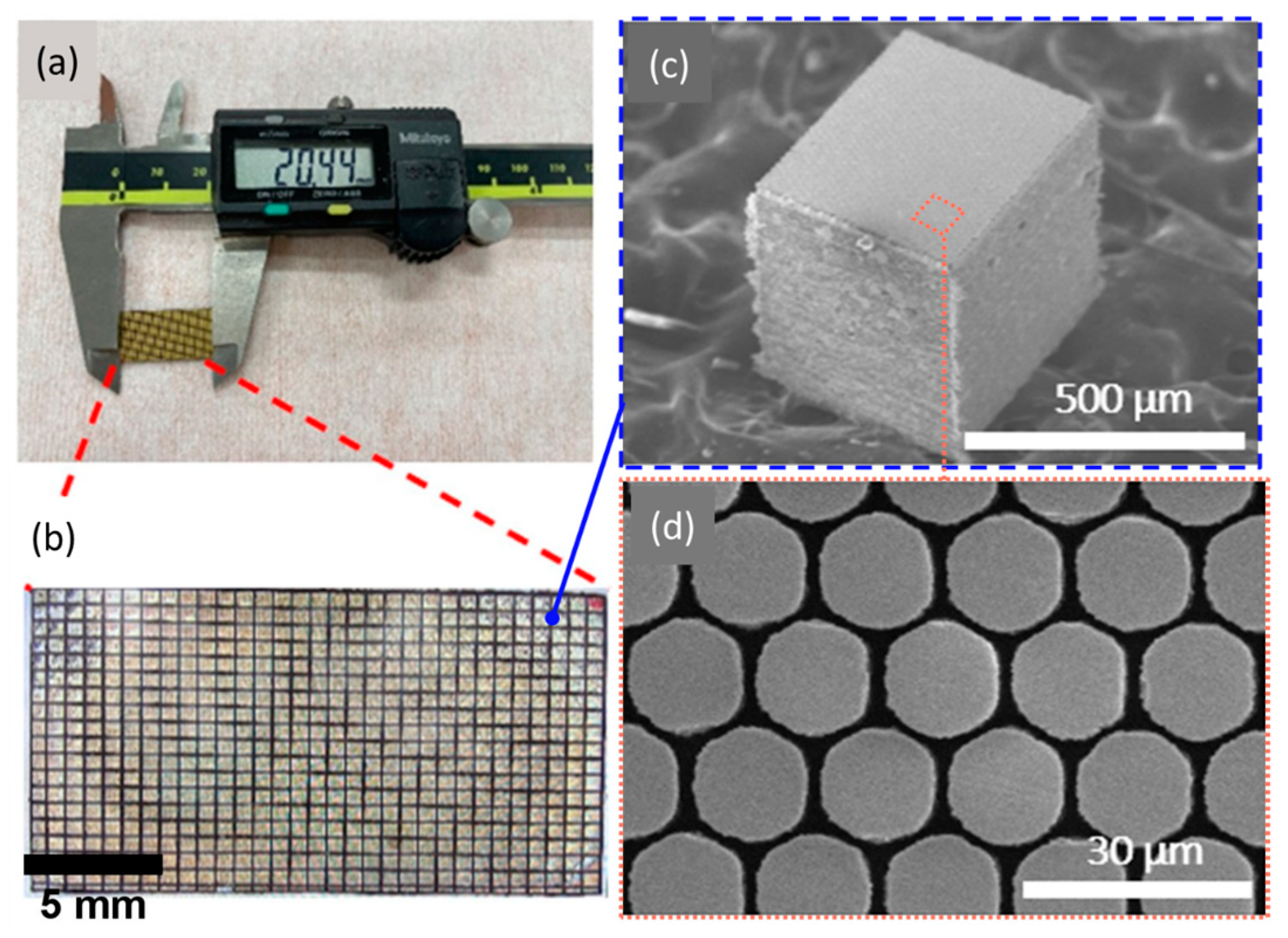
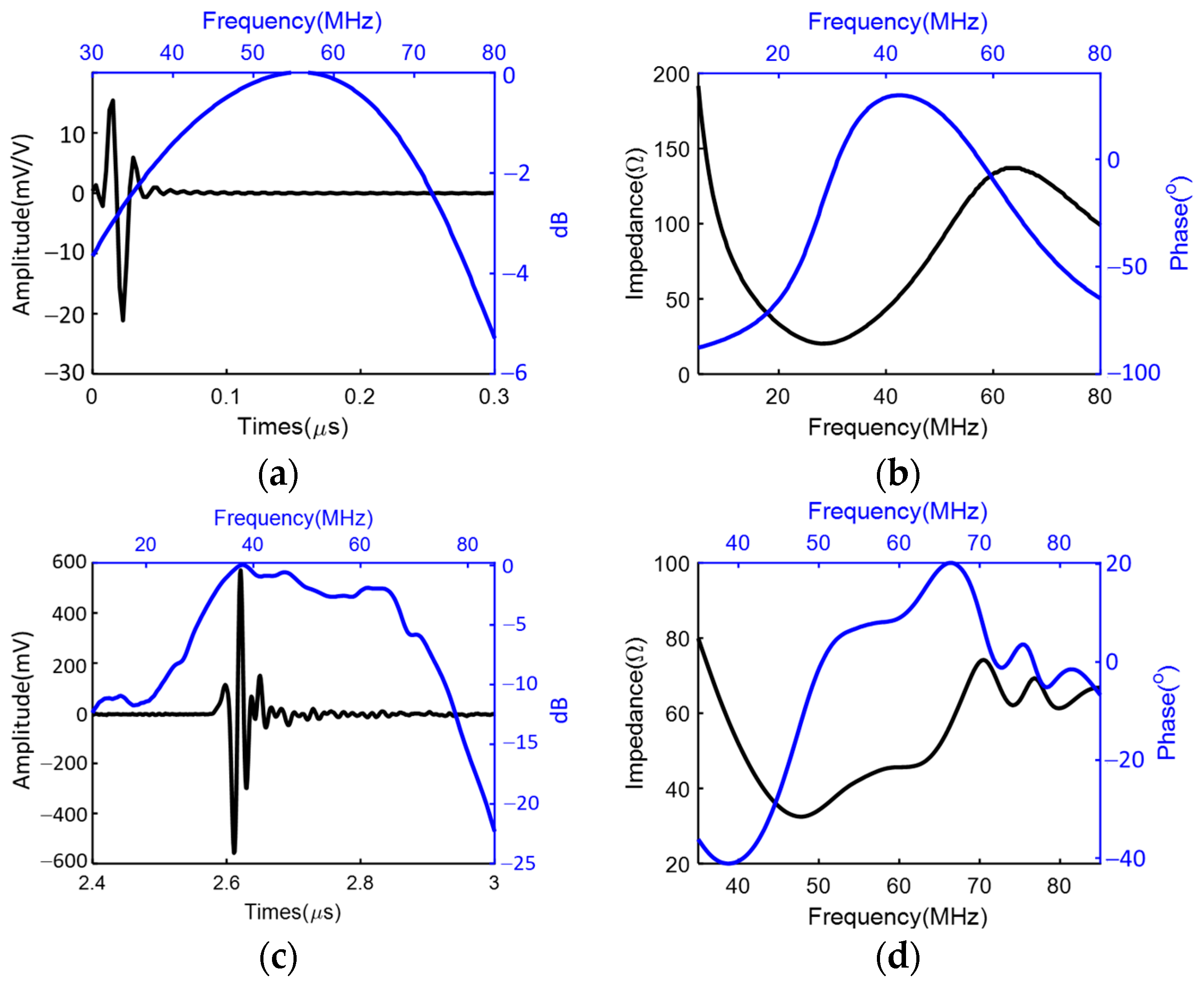
3.1. Characterization of the PMN-PT 1-3 Composite Material
3.2. Characterization of the Miniaturized Transducer
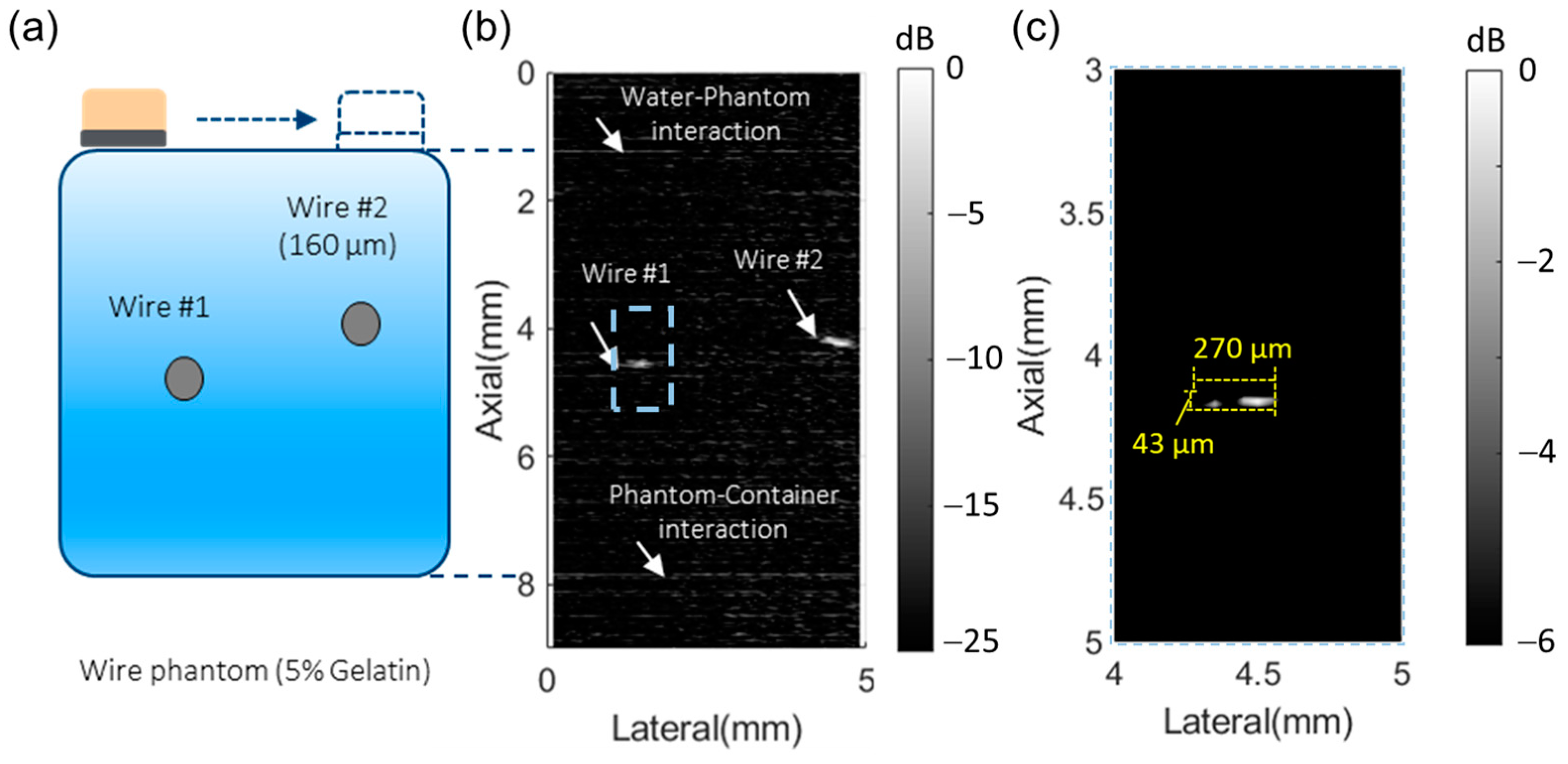
3.3. Imaging Performance Characterization of the 50 MHz Transducer with Wire Phantom
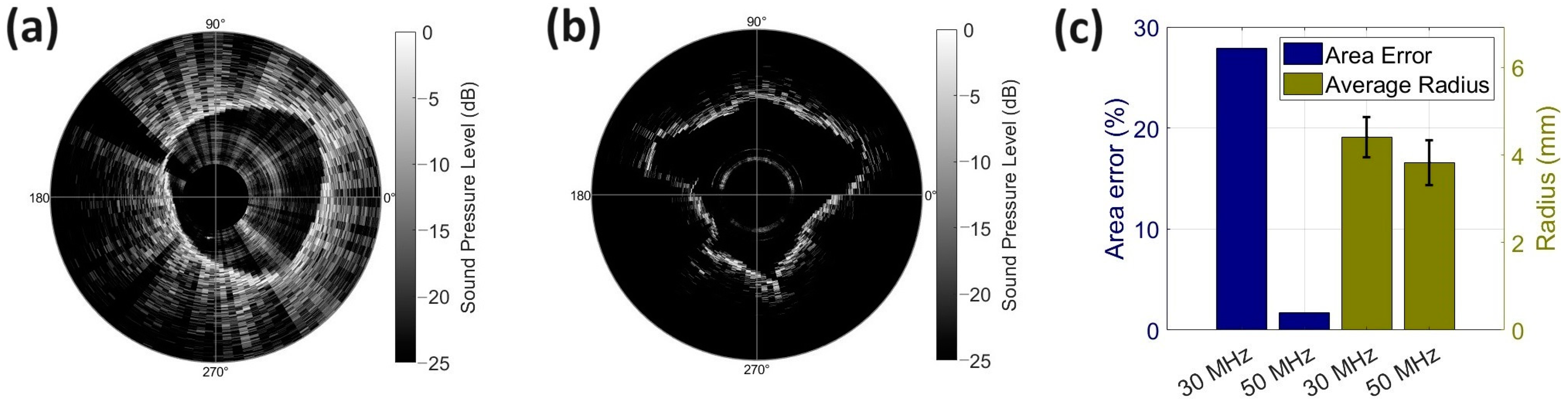
3.4. Tissue-Mimicking Phantom Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cancer Data and Statistics. Available online: https://www.cdc.gov/cancer/dcpc/data/index.htm (accessed on 18 October 2023).
- Etzioni, R.; Urban, N.; Ramsey, S.; McIntosh, M.; Schwartz, S.; Reid, B.; Radich, J.; Anderson, G.; Hartwell, L. The Case for Early Detection. Nat. Rev. Cancer 2003, 3, 243–252. [Google Scholar] [CrossRef]
- World Health Organization. Cancer Control: Knowledge into Action: WHO Guide for Effective Programmes; World Health Organization: Geneva, Switzerland, 2007; Volume 2. [Google Scholar]
- Ott, J.J.; Ullrich, A.; Miller, A.B. The Importance of Early Symptom Recognition in the Context of Early Detection and Cancer Survival. Eur. J. Cancer 1990 2009, 45, 2743–2748. [Google Scholar] [CrossRef]
- Chaffer, C.L.; Weinberg, R.A. A perspective on cancer cell metastasis. Sci. Am. Assoc. Adv. Sci. 2011, 331, 1559–1564. [Google Scholar] [CrossRef] [PubMed]
- Chambers, A.F.; Groom, A.C.; MacDonald, I.C. Dissemination and Growth of Cancer Cells in Metastatic Sites. Nat. Rev. Cancer 2002, 2, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, R.A.; Hanahan, D. The hallmarks of cancer. Cell 2000, 100, 57–70. [Google Scholar]
- Li, T.; Gianchandani, R.Y.; Gianchandani, Y.B. Micromachined Bulk PZT Tissue Contrast Sensor for Fine Needle Aspiration Biopsy. Lab Chip 2007, 7, 179–185. [Google Scholar] [CrossRef] [PubMed]
- VanderLaan, P.A. Fine-Needle Aspiration and Core Needle Biopsy: An Update on 2 Common Minimally Invasive Tissue Sampling Modalities. Cancer Cytopathol. 2016, 124, 862–870. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, A.; Hirokawa, M.; Higuchi, M.; Kanematsu, R.; Suzuki, A.; Kuma, S.; Hayashi, T.; Kudo, T.; Miyauchi, A. Optimal Needle Size for Thyroid Fine Needle Aspiration Cytology. Endocr. J. 2019, 66, 143–147. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Choi, J.H.; Lee, K.H.; Kim, K.M.; Shin, J.U.; Lee, J.K.; Lee, K.T.; Jang, K.-T. A prospective, Comparative Trial to Optimize Sampling Techniques in EUS-Guided FNA of Solid Pancreatic Masses. Gastrointest. Endosc. 2013, 77, 745–751. [Google Scholar] [CrossRef] [PubMed]
- Diamantis, A.; Magiorkinis, E.; Koutselini, H. Fine-Needle Aspiration (FNA) Biopsy: Historical Aspects. Folia Histochem. Cytobiol. 2009, 47, 191–197. [Google Scholar] [CrossRef]
- Park, J.; Choi, W.; Kim, K.; Jeong, W.; Seo, J.; Park, I. Biopsy Needle Integrated with Electrical Impedance Sensing Microelectrode Array Towards Real-Time Needle Guidance and Tissue Discrimination. Sci. Rep. 2018, 8, 264. [Google Scholar] [CrossRef] [PubMed]
- Jenssen, C.; Dietrich, C.F. Endoscopic Ultrasound-Guided Fine-Needle Aspiration Biopsy and Trucut Biopsy in Gastroenterology—An Overview. Baillière’s Best Pract. Res. Clin. Gastroenterol. 2009, 23, 743–759. [Google Scholar] [CrossRef]
- Costache, M.; Iordache, S.; Karstensen, J.G.; Săftoiu, A.; Vilmann, P. Endoscopic Ultrasound-Guided Fine Needle Aspiration: From the Past to the Future. Endosc. Ultrasound 2013, 2, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Shen, Z.; Zhou, Y.; Miao, J.; Vu, K.F. Enhanced Visualization of Fine Needles under Sonographic Guidance Using a MEMS Actuator. Sensors 2015, 15, 3107–3115. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Gianchandani, R.Y.; Gianchandani, Y.B. A bulk PZT microsensor for in-situ tissue contrast detection during fine needle aspiration biopsy of thyroid nodules. In Proceedings of the 19th IEEE International Conference on Micro Electro Mechanical Systems, Istanbul, Turkey, 22–26 January 2006; pp. 12–15. [Google Scholar]
- Cummins, T.; Eliahoo, P.; Shung, K.K. High-Frequency Ultrasound Array Designed for Ultrasound-Guided Breast Biopsy. T-UFFC 2016, 63, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.; Wodnicki, R.; Lim, H.G.; Yoon, C.W.; Kang, B.J.; Yoon, C.; Lee, C.; Hwang, J.Y.; Kim, H.H.; Choi, H.; et al. CMOS High-Voltage Analog 1–64 Multiplexer/Demultiplexer for Integrated Ultrasound Guided Breast Needle Biopsy. T-UFFC 2018, 65, 1334–1345. [Google Scholar] [CrossRef]
- Park, J.; Jeong, Y.; Kim, J.; Gu, J.; Wang, J.; Park, I. Biopsy needle integrated with multi-modal physical/chemical sensor array. Biosensors Bioelectron. 2020, 148, 111822. [Google Scholar] [CrossRef]
- McLaughlin, R.A.; Yang, X.; Quirk, B.C.; Lorenser, D.; Kirk, R.W.; Noble, P.B.; Sampson, D.D.; Puliyakote, A.S.K.; Vasilescu, D.M.; Newell, J.D.; et al. Static and dynamic imaging of alveoli using optical coherence tomography needle probes. J. Appl. Physiol. 1985 2012, 113, 967–974. [Google Scholar] [CrossRef]
- Yeo, B.Y.; McLaughlin, R.A.; Kirk, R.W.; Sampson, D.D. Enabling Freehand Lateral Scanning of Optical Coherence Tomography Needle Probes with a Magnetic Tracking System. Biomed. Opt. Express 2012, 3, 1565–1578. [Google Scholar] [CrossRef]
- Pisla, D.; Tucan, P.; Gherman, B.; Crisan, N.; Andras, I.; Vaida, C.; Plitea, N. Development of a Parallel Robotic System for Transperineal Biopsy of the Prostate. Mech. Sci. 2017, 8, 195–213. [Google Scholar] [CrossRef]
- Lee, S.Y.; Pakela, J.M.; Na, K.; Shi, J.; McKenna, B.J.; Simeone, D.M.; Yoon, E.; Scheiman, J.M.; Mycek, M.-A. Needle-Compatible Miniaturized Optoelectronic Sensor for Pancreatic Cancer Detection. Sci. Adv. 2020, 6, eabc1746. [Google Scholar] [CrossRef]
- Wiersema, M.J.; Kochman, M.L.; Cramer, H.M.; Tao, L.C.; Wiersema, L.M. Endosonography-guided real-time fine-needle aspiration biopsy. Gastrointest. Endosc. 1994, 40, 700–707. [Google Scholar] [CrossRef]
- Regunathan, R.; Woo, J.; Pierce, M.C.; Polydorides, A.D.; Raoufi, M.; Roayaie, S.; Schwartz, M.; Labow, D.; Shin, D.; Suzuki, R.; et al. Feasibility and preliminary accuracy of high-resolution imaging of the liver and pancreas using FNA compatible microendoscopy (with video). Gastrointest. Endosc. 2012, 76, 293–300. [Google Scholar] [CrossRef]
- Lehmann, S.; Frank, N. An overview of percutaneous CT-guided lung biopsies. J. Radiol. Nurs. 2018, 37, 2–8. [Google Scholar] [CrossRef]
- Parker, S.H.; Stavros, A.T.; Dennis, M.A. Needle Biopsy Techniques. Radiol. Clin. N. Am. 1995, 33, 1171–1186. [Google Scholar] [CrossRef]
- Manhire, A.; Charig, M.; Clelland, C.; Gleeson, F.; Miller, R.; Moss, H.; Pointon, K.; Richardson, C.; Sawicka, E. Guidelines for radiologically guided lung biopsy. Thorax 2003, 58, 920–936. [Google Scholar] [CrossRef]
- Deng, C.; Cao, X.; Wu, D.; Ding, H.; You, R.; Chen, Q.; Chen, L.; Zhang, X.; Zhang, Q.; Wu, Y. Small lung lesions invisible under fluoroscopy are located accurately by three-dimensional localization technique on chest wall surface and performed bronchoscopy procedures to increase diagnostic yields. BMC Pulm. Med. 2016, 16, 166. [Google Scholar] [CrossRef] [PubMed]
- National Guideline Centre (UK). Imaging for Fine Needle Aspiration; NICE: London, UK, 2019. [Google Scholar]
- Yoon, J.H.; Kim, E.; Kwak, J.Y.; Moon, H.J. Effectiveness and Limitations of Core Needle Biopsy in the Diagnosis of Thyroid Nodules: Review of current literature. J. Pathol. Transl. Med. 2015, 49, 230–235. [Google Scholar] [CrossRef] [PubMed]
- Chuang, W.-Y.; Chen, C.-C.; Yu, W.-H.; Yeh, C.-J.; Chang, S.-H.; Ueng, S.-H.; Wang, T.-H.; Hsueh, C.; Kuo, C.-F.; Yeh, C.-Y. Identification of nodal micrometastasis in colorectal cancer using deep learning on annotation-free whole-slide images. Mod. Pathol. 2021, 34, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Saito, T.; Kobayashi, H.; Kitamura, S. Ultrasonographic approach to diagnosing chest wall tumors. Chest 1988, 94, 1271–1275. [Google Scholar] [CrossRef] [PubMed]
- Sugama, Y.; Tamaki, S.; Kitamura, S.; Kira, S. Ultrasonographic evaluation of pleural and chest wall invasion of lung cancer. Chest 1988, 93, 275–279. [Google Scholar] [CrossRef]
- Hernandez, D.J.; Sinkov, V.A.; Roberts, W.W.; Allaf, M.E.; Patriciu, A.; Jarrett, T.W.; Kavoussi, L.R.; Stoianovici, D. Measurement of bio-impedance with a smart needle to confirm percutaneous kidney access. J. Urol. 2001, 166, 1520–1523. [Google Scholar] [CrossRef]
- Zhang, L.; Pleskow, D.K.; Turzhitsky, V.; Yee, E.U.; Berzin, T.M.; Sawhney, M.; Shinagare, S.; Vitkin, E.; Zakharov, Y.; Khan, U.; et al. Light Scattering Spectroscopy Identifies the Malignant Potential of Pancreatic Cysts during Endoscopy. Nat. Biomed. Eng. 2017, 1, 40. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-C.; Zhou, Q.; Ameri, H.; Wu, D.W.; Sun, L.; Wang, S.-H.; Humayun, M.S.; Shung, K.K. Determining the Acoustic Properties of the Lens Using A High-Frequency Ultrasonic Needle Transducer. Ultrasound Med. Biol. 2007, 33, 1971–1977. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Chen, R.; Tsui, P.; Zhou, Q.; Humayun, M.S.; Shung, K.K. Measurements of Attenuation Coefficient for Evaluating the Hardness of a Cataract Lens by a High-Frequency Ultrasonic Needle Transducer. Phys. Med. Biol. 2009, 54, 5981–5994. [Google Scholar] [CrossRef] [PubMed]
- Tsui, P.; Huang, C.; Zhou, Q.; Shung, K.K. Cataract Measurement by Estimating the Ultrasonic Statistical Parameter Using an Ultrasound Needle Transducer: An In Vitro Study. Physiol. Meas. 2011, 32, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Kreager, B.; Moon, S.; Mitchell, J.; Wu, H.; Peng, C.; Muller, M.; Huang, C.-C.; Jiang, X. Lung nodule biopsy guided using a 30 MHz ultrasound transducer: In vitro study. In Health Monitoring of Structural and Biological Systems XVII; SPIE: Long Beach, CA, USA, 2023; Volume 12488, pp. 292–299. [Google Scholar]
- Or, S.W.; Chan, H.L.W. Mode Coupling in Lead Zirconate Titanate/Epoxy 1–3 Piezocomposite Rings. J. Appl. Phys. 2001, 90, 4122–4129. [Google Scholar] [CrossRef]
- Smith, W.A.; Auld, B.A. Modeling 1–3 Composite Piezoelectrics: Thickness-Mode Oscillations. T-UFFC 1991, 38, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Roh, Y. Homogenization of PMN-PT/epoxy 1–3 piezocomposites by resonator measurements and finite element analysis. Sens. Actuators A Phys. 2014, 206, 97–106. [Google Scholar] [CrossRef]
- Jiang, X.; Kim, J.; Kim, K. Relaxor-PT Single Crystal Piezoelectric Sensors. Crystals 2014, 4, 351–376. [Google Scholar] [CrossRef]
- Jiang, X.; Snook, K.; Walker, T.; Portune, A.; Haber, R.; Geng, X.; Welter, J.; Hackenberger, W.S. Single crystal piezoelectric composite transducers for ultrasound NDE applications. Proc. SPIE 2008, 6934, 69340D-10. [Google Scholar]
- Yuan, J.R.; Jiang, X.; Cao, P.-J.; Sadaka, A.; Bautista, R.; Snook, K.; Rehrig, P. 5C-5 high frequency piezo composites microfabricated ultrasound transducers for intravascular imaging (invited). In Proceedings of the 2006 IEEE Ultrasonics Symposium, Vancouver, BC, Canada, 2–6 October 2006; pp. 264–268. [Google Scholar] [CrossRef]
- Krimholtz, R.; Leedom, D.A.; Matthaei, G.L. New equivalent circuits for elementary piezoelectric transducers. Electron. Lett. 1970, 6, 398. [Google Scholar] [CrossRef]
- Ultrasound Transducer Technical Notes. Olympus IMS Web Site. Available online: https://www.olympus-ims.com/en/resources/white-papers/ultrasonic-transducer-technical-notes/ (accessed on 12 November 2023).
- Important Characteristics of Sound Fields of Ultrasonic Transducers. Olympus IMS Web Site. Available online: https://www.olympus-ims.com/en/.downloads/download/?file=285213495&fl=en_US (accessed on 12 November 2023).
- Cook, J.R.; Bouchard, R.R.; Emelianov, S.Y. Tissue-Mimicking Phantoms for Photoacoustic and Ultrasonic Imaging. Biomed. Opt. Express 2011, 2, 3193–3206. [Google Scholar] [CrossRef] [PubMed]
- Ochs, M.; Nyengaard, J.R.; Jung, A.; Knudsen, L.; Voigt, M.; Wahlers, T.; Richter, J.; Gundersen, H.J.G. The number of alveoli in the human lung. Am. J. Respir. Crit. Care Med. 2004, 169, 120–124. [Google Scholar] [CrossRef]
- Hasgall, P.A.; Di Gennaro, F.; Baumgartner, C.; Neufeld, E.; Lloyd, B.; Gosselin, M.C.; Payne, D.; Klingenböck, A.; Kuster, N. IT’IS Database for Thermal and Electromagnetic Parameters of Biological Tissues, Version 4.1; IT’IS Foundation: Zurich, Switzerland, 2022. [Google Scholar] [CrossRef]
- ANSI/IEEE Standard 176-1987; IEEE Standard on Piezoelectricity. IEEE: New York, NY, USA, 1988.
- Zhang, H.K.; Kim, Y.; Lin, M.; Paredes, M.; Kannan, K.; Moghekar, A.; Durr, N.J.; Boctor, E.M. Toward Dynamic Lumbar Puncture Guidance Using Needle-Based Single-Element Ultrasound Imaging. J. Med. Imaging 2018, 5, 021224. [Google Scholar] [CrossRef]
- Chiang, H.K.; Zhou, Q.; Mandell, M.S.; Tsou, M.-Y.; Lin, S.-P.; Shung, K.K.; Ting, C.-K. Eyes in the Needle: Novel Epidural Needle with Embedded High-Frequency Ultrasound Transducer--Epidural access in Porcine Model. Anesthesiology 2011, 114, 1320–1324. [Google Scholar] [CrossRef]
- Lee, P.-Y.; Huang, C.-C.; Chiang, H.K. Implementation of a novel high frequency ultrasound device for guiding epidural anesthesia-in vivo animal study. In Proceedings of the 2013 IEEE International Ultrasonics Symposium, IUS 2013, Prague, Czech Republic, 21–25 July 2013; pp. 2049–2052. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sensing Modality | Axial Resolution | Lateral Resolution | Reference |
|---|---|---|---|
| Electrical Impedance | N/A | 200 μm | Li, T. et al. [17,18] |
| US Array | 33.2 μm | 115.6 μm | Cummins, T. et al. [18] |
| US Array | 90 μm | 392 μm | Jung, H. et al. [19] |
| Single Element US Transducer | 53 μm | 400 μm | Huang, C. et al. [38,39] |
| Material | Thickness | Velocity | Density | Acoustic Impedance | |
|---|---|---|---|---|---|
| Active layer | PMN-PT 1-3 composite | 37 μm | 3890 m/s | 5272 kg/m3 | 20.5 MRayl |
| Matching layer | Parylene C | 9 μm | 2770 m/s | 1140 kg/m3 | 3.16 MRayl |
| Backing layer | E-solder 3022 | 500 μm | 2110 m/s | 2590 kg/m3 | 5.5 MRayl |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kreager, B.C.; Wu, H.; Chang, W.-Y.; Moon, S.; Mitchell, J.; Peng, C.; Huang, C.-C.; Muller, M.; Tian, J.; Jiang, X. High-Performance PMN-PT Single-Crystal-Based 1-3 Composite Transducer Integrated with a Biopsy Needle. Biosensors 2024, 14, 74. https://doi.org/10.3390/bios14020074
Kreager BC, Wu H, Chang W-Y, Moon S, Mitchell J, Peng C, Huang C-C, Muller M, Tian J, Jiang X. High-Performance PMN-PT Single-Crystal-Based 1-3 Composite Transducer Integrated with a Biopsy Needle. Biosensors. 2024; 14(2):74. https://doi.org/10.3390/bios14020074
Chicago/Turabian StyleKreager, Benjamin C., Huaiyu Wu, Wei-Yi Chang, Sunho Moon, Josh Mitchell, Chang Peng, Chih-Chung Huang, Marie Muller, Jian Tian, and Xiaoning Jiang. 2024. "High-Performance PMN-PT Single-Crystal-Based 1-3 Composite Transducer Integrated with a Biopsy Needle" Biosensors 14, no. 2: 74. https://doi.org/10.3390/bios14020074