Early Screening of Colorectal Precancerous Lesions Based on Combined Measurement of Multiple Serum Tumor Markers Using Artificial Neural Network Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measurement of Protein Marker Concentration Using ECL Immunoassay
2.3. Development of ANN-Based Prediction Model
2.4. Testing the Performance of ANN-Based Prediction Model
2.5. Statistical Analysis
3. Results
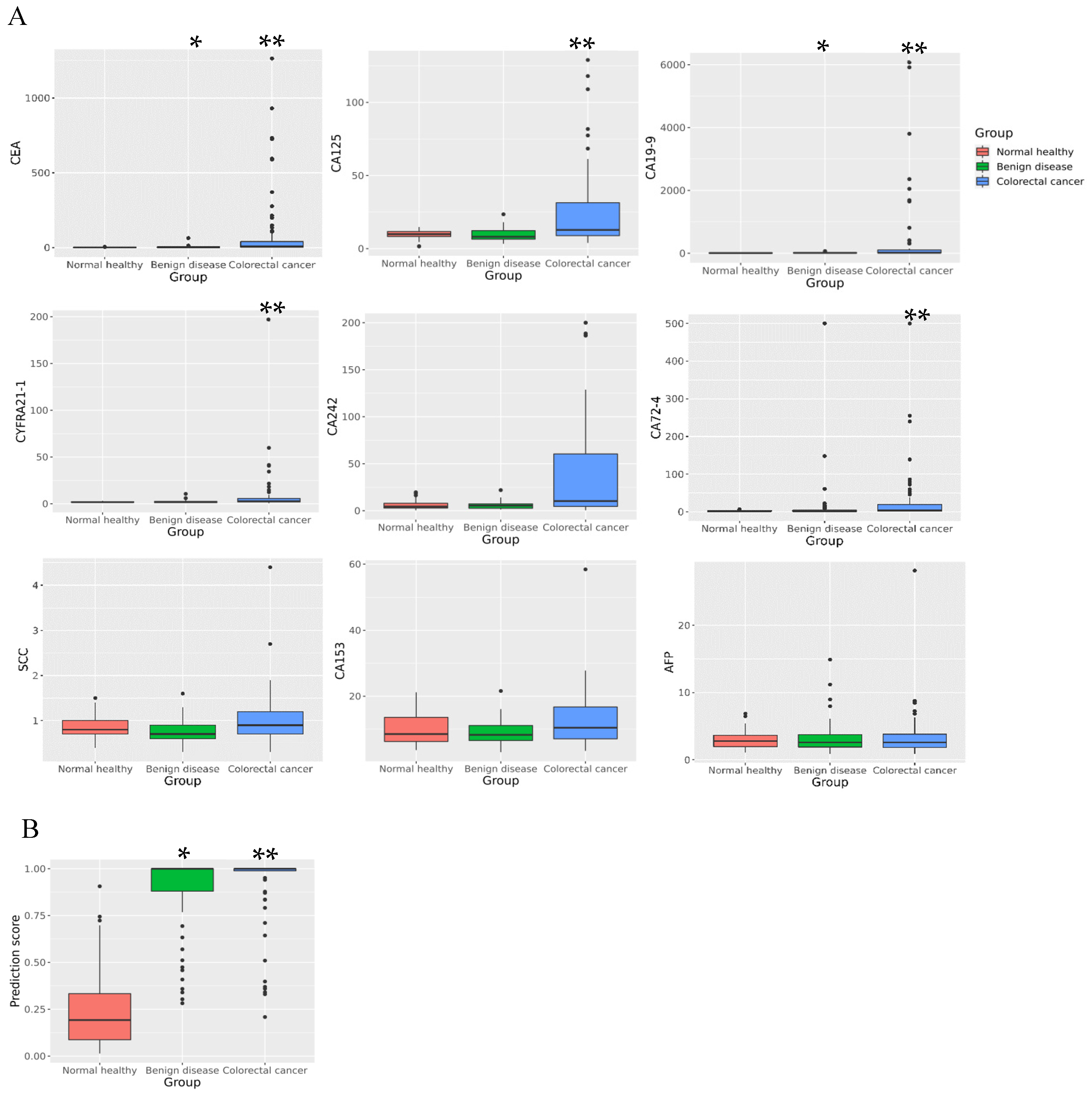
3.1. Comparison of Tumor Marker Levels among Different Groups
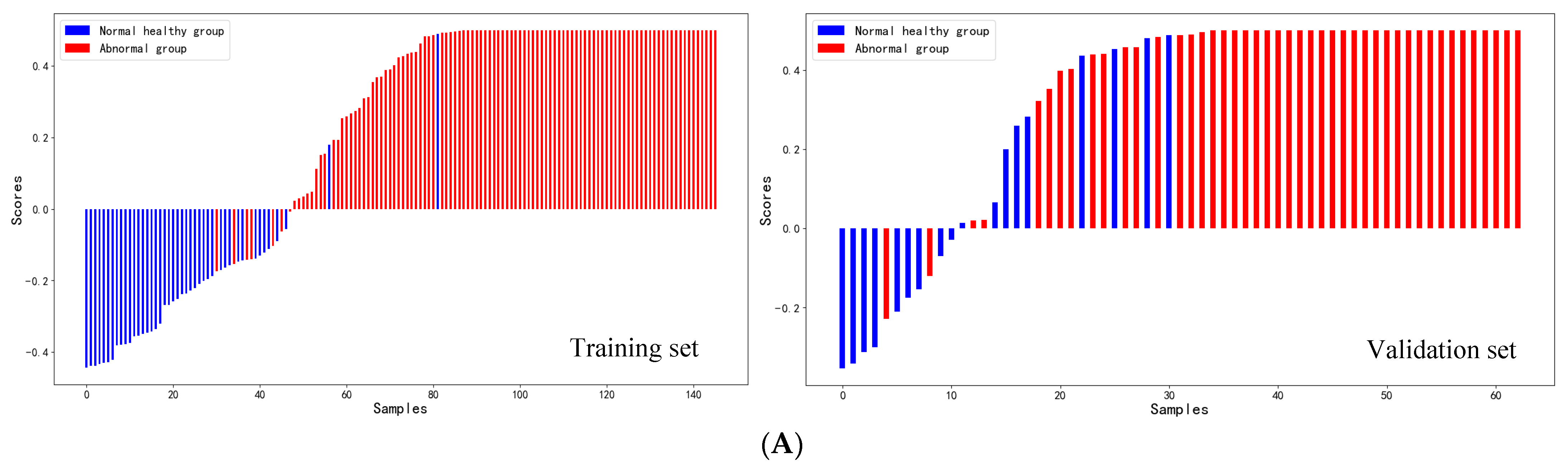
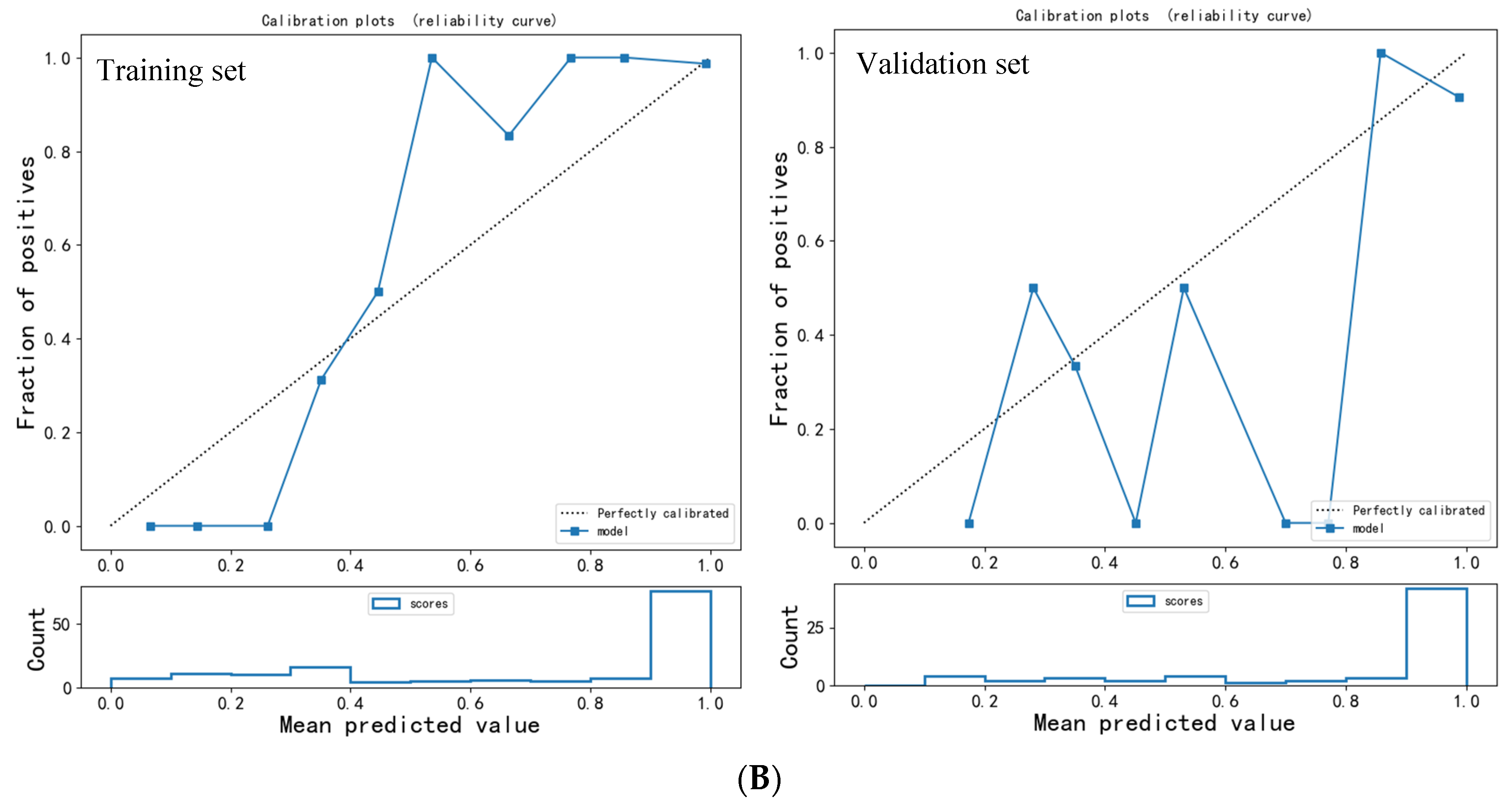
3.2. Evaluation of ANN Model Prediction Efficiency
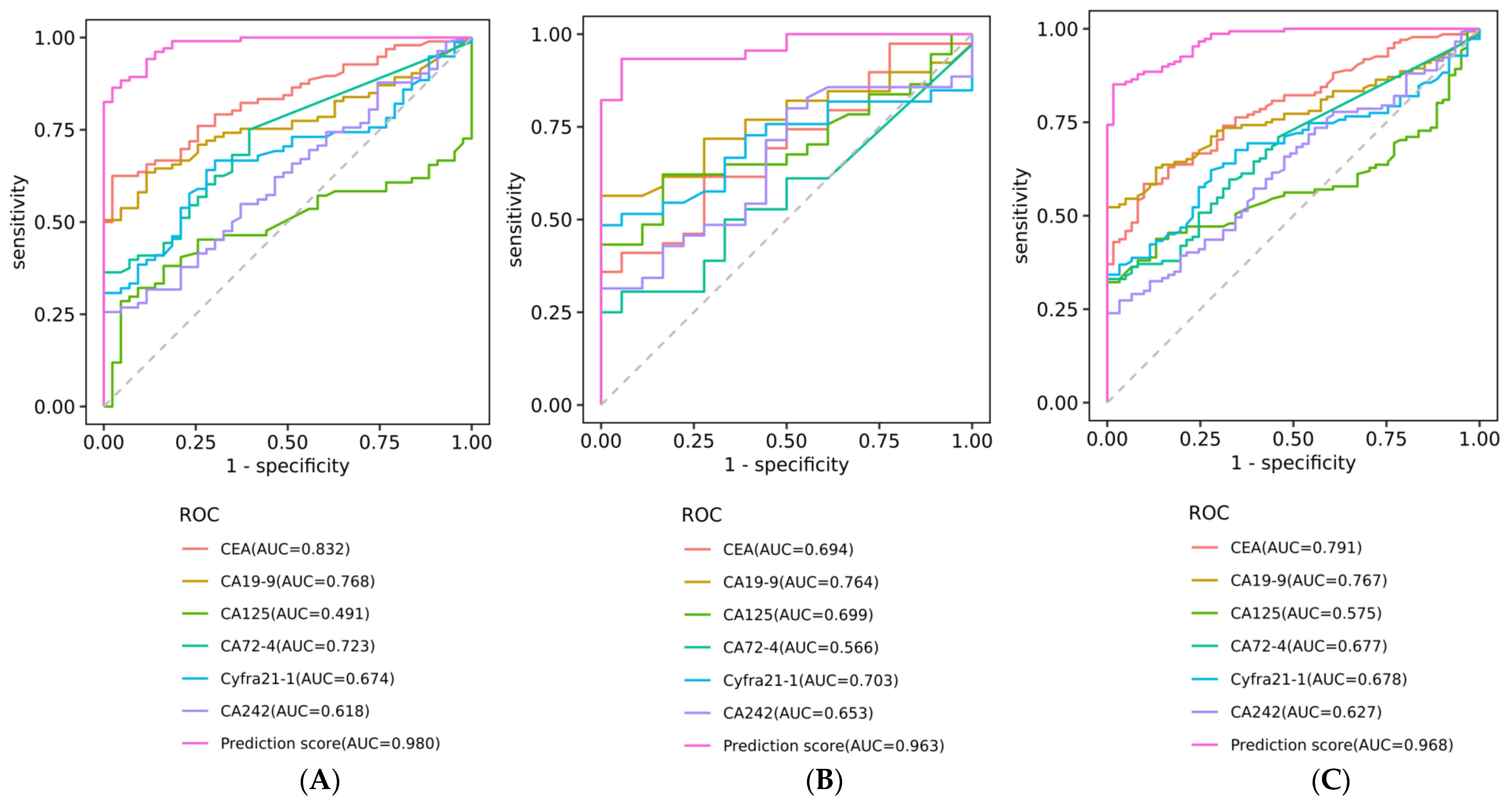
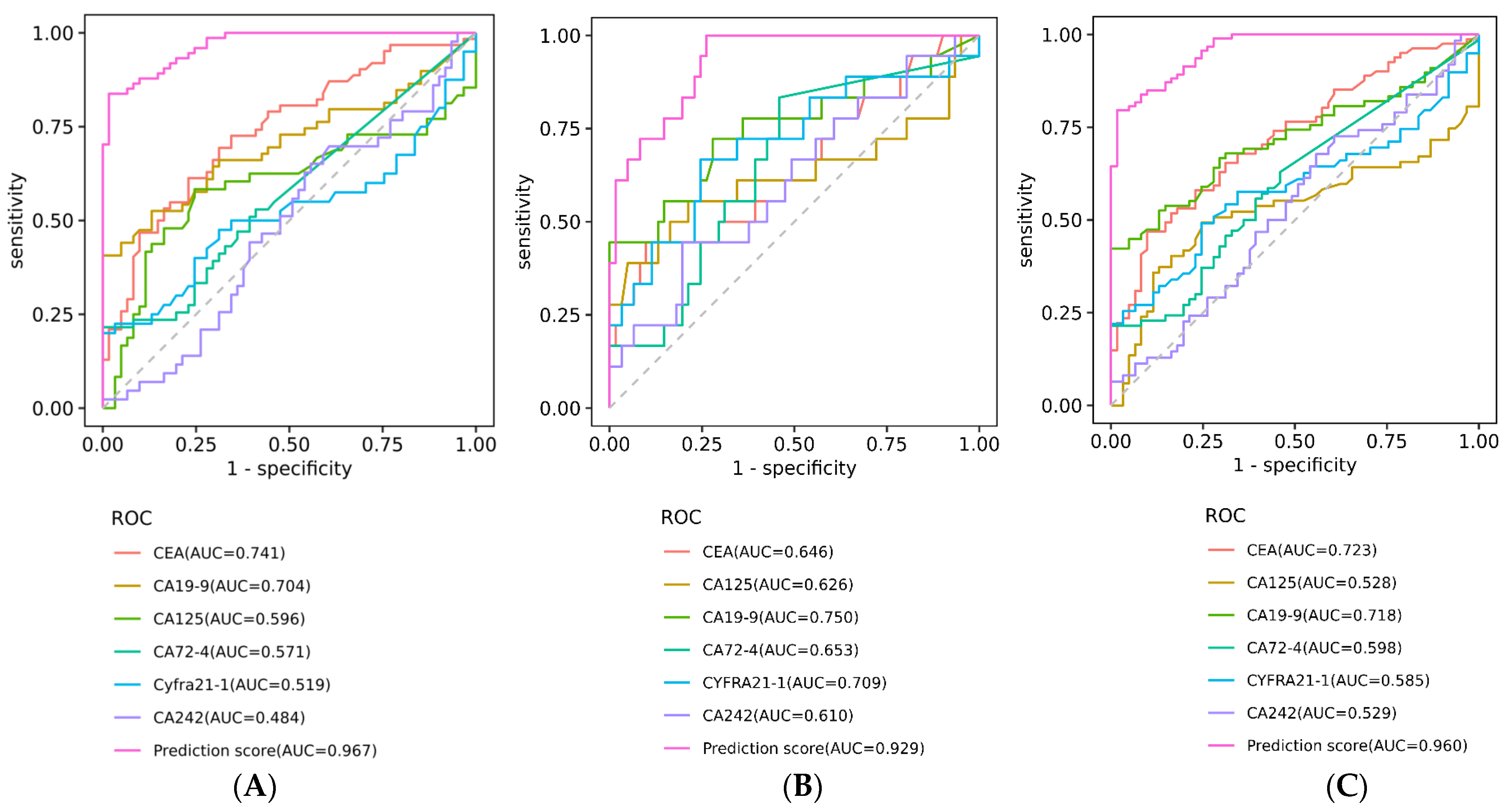
3.3. Diagnostic Efficacy Comparison of ANN Model with Other Markers
3.4. Consistency between ANN Model and Clinical Diagnosis
3.5. Evaluation of ANN Model Prediction Efficiency in Early Colorectal Diseases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chuang, J.P.; Tsai, H.L.; Chen, P.J.; Chang, T.K.; Su, W.C.; Yeh, Y.S.; Huang, C.W.; Wang, J.Y. Comprehensive Review of Biomarkers for the Treatment of Locally Advanced Colon Cancer. Cells 2022, 11, 3744. [Google Scholar] [CrossRef] [PubMed]
- Lichtenstern, C.R.; Ngu, R.K.; Shalapour, S.; Karin, M. Immunotherapy, Inflammation and Colorectal Cancer. Cells 2020, 9, 618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Tan, X.; Wang, P.; Qin, J. Application of Polypyrrole-Based Electrochemical Biosensor for the Early Diagnosis of Colorectal Cancer. Nanomaterials 2023, 13, 674. [Google Scholar] [CrossRef] [PubMed]
- Ribe, S.G.; Botteri, E.; Løberg, M.; Randel, K.R.; Kalager, M.; Nilsen, J.A.; Gulichsen, E.H.; Holme, Ø. Impact of time between faecal immunochemical tests in colorectal cancer screening on screening results: A natural experiment. Int. J. Cancer 2023, 152, 1414–1424. [Google Scholar] [CrossRef] [PubMed]
- Alustiza, M.; Ripoll, L.; Canals, A.; Murcia, O.; Martínez-Roca, A.; García-Heredia, A.; Giner-Calabuig, M.; Jover, R.; Vidal, L. A novel non-invasive colorectal cancer diagnostic method: Volatile organic compounds as biomarkers. Clin. Chim. Acta 2023, 542, 117273. [Google Scholar] [CrossRef] [PubMed]
- Yuan, R.Q.; Zhao, H.; Wang, Y.; Song, K.; Yang, J.; He, W.; Miao, D.Z.; Wang, Q.; Jia, Y.H. SEPTIN9-SDC2-VIM methylation signature as a biomarker for the early diagnosis of colorectal cancer. Am. J. Cancer Res. 2022, 12, 3128–3140. [Google Scholar]
- Qi, C.; Zhou, T.; Bai, Y.; Chen, H.; Yuan, J.; Zhao, F.; Liu, C.; Ma, M.; Bei, T.; Chen, S.; et al. China Special Issue on Gastrointestinal Tumor-NTRK Fusion in a Large Real-World Population and Clinical Utility of Circulating Tumor DNA Genotyping to Guide TRK Inhibitor treatment. Int. J. Cancer, 2023; online ahead of print. [Google Scholar] [CrossRef]
- Cao, H.; Zhu, L.; Li, L.; Wang, W.; Niu, X. Serum CA724 Has No Diagnostic Value for Gastrointestinal Tumors. Clin. Exp. Med. 2023; online ahead of print. [Google Scholar] [CrossRef]
- Paku, M.; Uemura, M.; Kitakaze, M.; Miyoshi, N.; Takahashi, H.; Mizushima, T.; Doki, Y.; Eguchi, H. Clinical Significance of Preoperative and Postoperative Serum CEA and Carbohydrate Antigen 19-9 Levels in Patients Undergoing Curative Resection of Locally Recurrent Rectal Cancer. Dis. Colon Rectum 2023, 66, 392–400. [Google Scholar] [CrossRef]
- Luo, H.; Shen, K.; Li, B.; Li, R.; Wang, Z.; Xie, Z. Clinical significance and diagnostic value of serum NSE, CEA, CA19-9, CA125 and CA242 levels in colorectal cancer. Oncol. Lett. 2020, 20, 742–750. [Google Scholar] [CrossRef]
- Yajima, S.; Suzuki, T.; Oshima, Y.; Shiratori, F.; Funahashi, K.; Kawai, S.; Nanki, T.; Muraoka, S.; Urita, Y.; Saida, Y.; et al. New Assay System Elecsys Anti-p53 to Detect Serum Anti-p53 Antibodies in Esophageal Cancer Patients and Colorectal Cancer Patients: Multi-institutional Study. Ann. Surg. Oncol. 2021, 28, 4007–4015. [Google Scholar] [CrossRef]
- Zanut, A.; Fiorani, A.; Canola, S.; Saito, T.; Ziebart, N.; Rapino, S.; Rebeccani, S.; Barbon, A.; Irie, T.; Josel, H.P.; et al. Insights into the mechanism of coreactant electrochemiluminescence facilitating enhanced bioanalytical performance. Nat. Commun. 2020, 11, 2668. [Google Scholar] [CrossRef]
- Lippi, G.; Salvagno, G.L.; Pegoraro, M.; Militello, V.; Caloi, C.; Peretti, A.; De Nitto, S.; Bovo, C.; Lo Cascio, G. Preliminary evaluation of Roche Cobas Elecsys Anti-SARS-CoV-2 chemiluminescence immunoassay. Clin. Chem. Lab. Med. 2020, 58, e251–e253. [Google Scholar] [CrossRef] [PubMed]
- Koppad, S.; Basava, A.; Nash, K.; Gkoutos, G.V.; Acharjee, A. Machine Learning Based Identification of Colon Cancer Candidate Diagnostics Genes. Biology 2022, 11, 365. [Google Scholar] [CrossRef]
- Du, G.; Ren, C.; Wang, J.; Ma, J. The Clinical Value of Blood miR-654-5p, miR-126, miR-10b, and miR-144 in the Diagnosis of Colorectal Cancer. Comput. Math. Methods Med. 2022, 2022, 8225966. [Google Scholar] [CrossRef] [PubMed]
- Skrede, O.J.; De Raedt, S.; Kleppe, A.; Hveem, T.S.; Liestøl, K.; Maddison, J.; Askautrud, H.A.; Pradhan, M.; Nesheim, J.A.; Albregtsen, F.; et al. Deep learning for prediction of colorectal cancer outcome: A discovery and validation study. Lancet 2020, 395, 350–360. [Google Scholar] [CrossRef] [PubMed]
- Kavitha, M.S.; Gangadaran, P.; Jackson, A.; Venmathi Maran, B.A.; Kurita, T.; Ahn, B.C. Deep Neural Network Models for Colon Cancer Screening. Cancers 2022, 14, 3707. [Google Scholar] [CrossRef] [PubMed]
- Niehues, J.M.; Quirke, P.; West, N.P.; Grabsch, H.I.; van Treeck, M.; Schirris, Y.; Veldhuizen, G.P.; Hutchins, G.G.A.; Richman, S.D.; Foersch, S.; et al. Generalizable biomarker prediction from cancer pathology slides with self-supervised deep learning: A retrospective multi-centric study. Cell Rep. Med. 2023, 4, 100980. [Google Scholar] [CrossRef]
- Chan, H.C.; Chattopadhyay, A.; Chuang, E.Y.; Lu, T.P. Development of a Gene-Based Prediction Model for Recurrence of Colorectal Cancer Using an Ensemble Learning Algorithm. Front. Oncol. 2021, 11, 631056. [Google Scholar] [CrossRef]
- Wang, L. Predicting Colorectal Cancer Using Residual Deep Learning with Nursing Care. Contrast Media Mol. Imaging 2022, 2022, 7996195. [Google Scholar] [CrossRef]
- Stulp, F.; Sigaud, O. Many regression algorithms, one unified model: A review. Neural Netw. 2015, 69, 60–79. [Google Scholar] [CrossRef] [Green Version]
- Fan, Z.; Guo, Y.; Gu, X.; Huang, R.; Miao, W. Development and validation of an artificial neural network model for non-invasive gastric cancer screening and diagnosis. Sci. Rep. 2022, 12, 21795. [Google Scholar] [CrossRef]
- Nasser, M.; Yusof, U.K. Deep Learning Based Methods for Breast Cancer Diagnosis: A Systematic Review and Future Direction. Diagnostics 2023, 13, 161. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Qian, H.; Shao, X.; Zhang, H.; Liu, S.; Pan, J.; Xue, W. Multimodal convolutional neural networks based on the Raman spectra of serum and clinical features for the early diagnosis of prostate cancer. Spectrochim. Acta A Mol. Biomol. Spectrosc. 2023, 293, 122426. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Maes-Carballo, M.; García-García, M.; Martín-Díaz, M.; Estrada-López, C.R.; Iglesias-Álvarez, A.; Filigrana-Valle, C.M.; Khan, K.S.; Bueno-Cavanillas, A. A comprehensive systematic review of colorectal cancer screening clinical practices guidelines and consensus statements. Br. J. Cancer 2023, 128, 946–957. [Google Scholar] [CrossRef] [PubMed]
- Hanna, M.; Dey, N.; Grady, W.M. Emerging Tests for Noninvasive Colorectal Cancer Screening. Clin. Gastroenterol. Hepatol. 2023, 21, 604–616. [Google Scholar] [CrossRef]
- Ding, Q.; Kong, X.; Zhong, W.; Liu, W. Fecal biomarkers: Non-invasive diagnosis of colorectal cancer. Front. Oncol. 2022, 12, 971930. [Google Scholar] [CrossRef]
- Shaukat, A.; Levin, T.R. Current and future colorectal cancer screening strategies. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 521–531. [Google Scholar] [CrossRef]
- Swanson, K.; Wu, E.; Zhang, A.; Alizadeh, A.A.; Zou, J. From patterns to patients: Advances in clinical machine learning for cancer diagnosis, prognosis, and treatment. Cell 2023, 186, 1772–1791. [Google Scholar] [CrossRef]
- Gao, Y.; Wang, J.; Zhou, Y.; Sheng, S.; Qian, S.Y.; Huo, X. Evaluation of Serum CEA, CA19-9, CA72-4, CA125 and Ferritin as Diagnostic Markers and Factors of Clinical Parameters for Colorectal Cancer. Sci. Rep. 2018, 8, 2732. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Xu, M.; Qiao, X.; Ji, C.; Li, L.; Zhou, Z. Prediction of serosal invasion in gastric cancer: Development and validation of multivariate models integrating preoperative clinicopathological features and radiographic findings based on late arterial phase CT images. BMC Cancer 2021, 21, 1038. [Google Scholar] [CrossRef]
- Gawel, S.H.; Lucht, M.; Gomer, H.; Treado, P.; Christensen, I.J.; Nielsen, H.J.; Davis, G.J. Danish Research Group on Early Detection of Colorectal Cancer.Evaluation of algorithm development approaches: Development of biomarker panels for early detection of colorectal lesions. Clin. Chim. Acta 2019, 498, 108–115. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, M.; Pan, X.; Zhao, M.; Huang, L.; Hu, X.; Wang, X.; Qiao, L.; Guo, Q.; Xu, W.; et al. Integrative Serum Metabolic Fingerprints Based Multi-Modal Platforms for Lung Adenocarcinoma Early Detection and Pulmonary Nodule Classification. Adv. Sci. 2022, 9, e2203786. [Google Scholar] [CrossRef]
- Dihge, L.; Bendahl, P.O.; Skarping, I.; Hjärtström, M.; Ohlsson, M.; Rydén, L. The implementation of NILS: A web-based artificial neural network decision support tool for noninvasive lymph node staging in breast cancer. Front. Oncol. 2023, 13, 1102254. [Google Scholar] [CrossRef]
- Matsuda, S.; Irino, T.; Kawakubo, H.; Takeuchi, M.; Nishimura, E.; Hisaoka, K.; Sano, J.; Kobayashi, R.; Fukuda, K.; Nakamura, R.; et al. Evaluation of Endoscopic Response Using Deep Neural Network in Esophageal Cancer Patients Who Received Neoadjuvant Chemotherapy. Ann. Surg. Oncol. 2023, 30, 3733–3742. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Georgakopoulos-Soares, I.; Ahituv, N.; Wong, K.C. Risk scoring based on DNA methylation-driven related DEGs for colorectal cancer prognosis with systematic insights. Life Sci. 2023, 316, 121413. [Google Scholar] [CrossRef] [PubMed]
- Abdul Rahman, H.; Ottom, M.A.; Dinov, I.D. Machine learning-based colorectal cancer prediction using global dietary data. BMC Cancer 2023, 23, 144. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Feature | Training Set | Validation Set | Total |
|---|---|---|---|---|
| Colorectal cancer | n | 51 | 23 | 74 |
| Age (years), mean ± SD | 65 ± 11 | 65 ± 11 | 65 ± 11 | |
| Gender | ||||
| Male | 27 | 12 | 39 | |
| Female | 24 | 11 | 35 | |
| Clinical stage | ||||
| Early stage | 12 | 6 | 18 | |
| Advanced stage | 39 | 17 | 56 | |
| Benign disease | n | 52 | 22 | 74 |
| Age (years), mean ± SD | 62 ± 10 | 63 ± 10 | 62 ± 10 | |
| Gender | ||||
| Male | 28 | 13 | 41 | |
| Female | 24 | 9 | 33 | |
| Pathological classification | ||||
| Adenomatous polyp | 22 | 11 | 33 | |
| Hyperplastic polyp | 18 | 7 | 25 | |
| Inflammatory polyp | 12 | 4 | 16 | |
| Normal healthy control | n | 42 | 19 | 61 |
| Age (years), mean ± SD | 58 ± 12 | 59 ± 12 | 58 ± 12 | |
| Gender | ||||
| Male | 21 | 9 | 30 | |
| Female | 21 | 10 | 31 | |
| Total | \ | 94 | 41 | 135 |
| Set | Index | AUC | Standard Error | 95% CI | p |
|---|---|---|---|---|---|
| Training set | Prediction score | 0.98 | 0.008 | 0.96–1.00 | 0.000 ** |
| Validation set | Prediction score | 0.96 | 0.021 | 0.92–1.00 | 0.000 ** |
| Total cases | Prediction score | 0.97 | 0.010 | 0.95–0.99 | 0.000 ** |
| Set | Label Class | Normal Healthy | Abnormal Group | χ2 | p |
|---|---|---|---|---|---|
| Training | Normal healthy group | 41 | 2 | 107.794 | 0.000 ** |
| Abnormal group | 7 | 96 | |||
| Validation | Normal healthy group | 9 | 9 | 18.515 | 0.000 ** |
| Abnormal group | 2 | 43 |
| Group | Index | AUC | Standard Error | 95% CI | p | Cut-Off | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|---|---|---|---|
| Benign disease | Prediction score | 0.97 | 0.012 | 0.94–0.99 | 0.000 ** | 0.39 | 94% | 80% | 83% | 93% |
| Early-stage CRC | Prediction score | 0.93 | 0.029 | 0.87–0.99 | 0.000 ** | 0.34 | 0.94% | 75% | 79% | 93% |
| Benign disease and early-stage CRC | Prediction score | 0.96 | 0.013 | 0.94–0.99 | 0.000 ** | 0.30 | 0.97% | 72% | 78% | 96% |
| Label Class | Normal Healthy | Benign Disease & Early CRC | χ2 | p |
|---|---|---|---|---|
| Normal healthy | 44 | 17 | 89.172 | 0.000 ** |
| Benign disease & Early CRC | 1 | 91 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ke, X.; Liu, W.; Shen, L.; Zhang, Y.; Liu, W.; Wang, C.; Wang, X. Early Screening of Colorectal Precancerous Lesions Based on Combined Measurement of Multiple Serum Tumor Markers Using Artificial Neural Network Analysis. Biosensors 2023, 13, 685. https://doi.org/10.3390/bios13070685
Ke X, Liu W, Shen L, Zhang Y, Liu W, Wang C, Wang X. Early Screening of Colorectal Precancerous Lesions Based on Combined Measurement of Multiple Serum Tumor Markers Using Artificial Neural Network Analysis. Biosensors. 2023; 13(7):685. https://doi.org/10.3390/bios13070685
Chicago/Turabian StyleKe, Xing, Wenxue Liu, Lisong Shen, Yue Zhang, Wei Liu, Chaofu Wang, and Xu Wang. 2023. "Early Screening of Colorectal Precancerous Lesions Based on Combined Measurement of Multiple Serum Tumor Markers Using Artificial Neural Network Analysis" Biosensors 13, no. 7: 685. https://doi.org/10.3390/bios13070685