Body Fluid Biomarkers for Alzheimer’s Disease—An Up-To-Date Overview




1
Târgu Mures, Emergency Clinical Hospital, “George Emil Palade” University of Medicine, Pharmacy, Science and Technology of Târgu Mures, RO-540142 Târgu Mures, Romania
2
Faculty of Applied Chemistry and Materials Science, University Politehnica of Bucharest, RO-060042 Bucharest, Romania
*
Author to whom correspondence should be addressed.
Biomedicines 2020, 8(10), 421; https://doi.org/10.3390/biomedicines8100421
Submission received: 26 August 2020
/
Revised: 9 October 2020
/
Accepted: 13 October 2020
/
Published: 15 October 2020
(This article belongs to the Special Issue Biomarkers in Neurodegenerative Diseases)
Abstract
:Neurodegeneration is a highly complex process which is associated with a variety of molecular mechanisms related to ageing. Among neurodegenerative disorders, Alzheimer’s disease (AD) is the most common, affecting more than 45 million individuals. The underlying mechanisms involve amyloid plaques and neurofibrillary tangles (NFTs) deposition, which will subsequently lead to oxidative stress, chronic neuroinflammation, neuron dysfunction, and neurodegeneration. The current diagnosis methods are still limited in regard to the possibility of the accurate and early detection of the diseases. Therefore, research has shifted towards the identification of novel biomarkers and matrices as biomarker sources, beyond amyloid-β and tau protein levels within the cerebrospinal fluid (CSF), that could improve AD diagnosis. In this context, the aim of this paper is to provide an overview of both conventional and novel biomarkers for AD found within body fluids, including CSF, blood, saliva, urine, tears, and olfactory fluids.
1. Introduction
Neurodegeneration is a complex process that encompasses several different molecular pathways and a multifaceted interplay between a variety of regulatory factors [1,2]. It is characterized by a progressive and irreversible neuronal loss from the specific brain and spinal cord regions, mainly the nuclei of the base within the subcortical areas and the cerebral cortex, consequently leading to damage and dysfunction manifested through cognitive and motor dysfunctions [2,3,4]. Generally, the causal factors include the following: oxidative stress and free radical formation; protein misfolding, oligomerization and aggregation; mitochondrial dysfunction, axonal transport deficits and abnormal neuron–glial interactions; calcium deregulation, phosphorylation impairment; neuroinflammation; DNA damage and aberrant RNA processing [2,5,6].
Neurodegeneration is the underlying factor for many debilitating and incurable age-dependent disorders [3,7,8]. The prevalence of neurodegenerative disorders is continuously increasing as a consequence of the dramatic rise in life expectancy due to scientific achievements and progress, thus posing a significant threat to human health [5,7,9,10]. Moreover, neurodegeneration is associated with various neurodegenerative, neurotraumatic, and neuropsychiatric disorders, with considerably diverse pathophysiology, including memory and cognitive impairments, muscle weakness and/or paralysis, abnormal control of the voluntary movement, seizures, confusion, and pain [2,4,7,11,12,13]. Specifically, such diseases vary from progressive degenerative disorders, including Alzheimer’s disease (AD), Parkinson’s disease, Huntington’s disease, amyotrophic lateral sclerosis and multiple sclerosis [4,5,10,14,15], to acute traumatic injuries, such as traumatic brain injury, stroke or spinal cord injury [15,16].
Among them, AD is the most common neurodegenerative disorder, affecting more than 45 million individuals worldwide and is expected to reach 60 million by 2030 due to the increase in the elderly population [17,18]. AD is characterized by the progressive death of cholinergic neurons within the hippocampal and cortical regions, the consequent atrophy, abnormal neurotransmission and loss of synapses, and neurodegeneration [4,18,19,20,21]. At molecular levels, the underlying mechanisms of AD involve the extracellular deposition of amyloid-β (Aβ) peptides, known as amyloid plaques, and the intracellular formation of hyperphosphorylated tau (Tubulin Associated Unit) protein aggregates, known as neurofibrillary tangles (NFTs), which subsequently induce oxidative stress, chronic neuroinflammation, neuron dysfunction, and neurodegeneration [4,10,17,19,22,23].
In addition to cognitive tests, the current diagnostic methods rely on imaging techniques [24,25,26,27] and cerebrospinal fluid (CSF) assays. On one hand, the purpose of the neuroimaging methods is assessing the hippocampal atrophy through magnetic resonance imaging and the cortical Aβ deposition through positron emission tomography. On the other hand, CSF analyses aim to provide quantitative measurements of Aβ and tau protein levels as AD biomarkers [18]. However, the available methods are expensive, relatively invasive [18,28], and have low sensitivity and specificity, which result in the risks of either overdiagnosis or undiagnosed, misattributed, or dismissed and ignored symptoms [29,30]. Additionally, as there is a serious lack of AD diagnosis assays at all illness stages, patients are generally diagnosed late, which places a great burden on the health systems [17,18]. Therefore, the development of novel methods of AD early detection and accurate diagnosis is essential [17,29].
Detection strategies based on novel biomarkers beyond Aβ and tau protein could represent a promising solution for the early diagnosis of AD [18]. However, as no single biomarker can be used to accurately diagnose AD, a combination of biomarkers could significantly increase diagnostic accuracy [30,31]. Moreover, such biomarkers should ideally be easy to sample and should be measurable through simple and cost-efficient methods and at all stages of the disease, allowing for standardization processes [30,32]. In this context, the aim of this manuscript is to provide an up-to-date overview of both conventional and novel AD biomarkers, which could play fundamental roles in its accurate and timely diagnosis.
2. Cerebrospinal Fluid Biomarkers
Biomarkers can be described as molecules that can be detected and quantified within body fluids, such as blood, CSF, urine or saliva, and changes in their levels or activity are generally associated with different pathologies. Offering the possibility of early disease diagnosis, most biomarkers involve the measurement of structural, metabolic or enzymatic proteins and should be non-invasive, easy to use, and cost-efficient [33,34].
Residing in the subarachnoid space and ventricular system of the brain and spinal cord, the CSF is a fundamental neuropathology indicator as it carries the brain’s interstitial fluid across the ventricular ependymal lining, and thus it reflects any biochemical change within the brain [35,36]. Moreover, as the blood–CSF barrier restricts the transport of molecules and proteins, the CSF is isolated from the peripheral system. Thus, it is a useful matrix for the detection of neurodegenerative disorder markers, providing the tools for disease screening, prognosis and monitoring [37,38,39]. Among them, AD biomarkers have received a great deal of clinical interest, allowing for the depiction of AD pathology [35,39,40]. Furthermore, such biomarkers could also be applied for the diagnosis of mild cognitive impairment (MCI), the transitional phase from normal cognition to dementia, that generally manifests as a silent pre-clinical phase in 6–15% of AD patients [40,41,42].
The CSF biomarkers most indicative of AD are associated with the main pathological changes in the brain, namely the deposition of extracellular Aβ plaques, the formation of NFTs, and the loss of neurons [37]. Thus, the biomarkers that have received clinical attention for AD diagnosis are Aβ, total-tau (T-tau) and phosphorylated-tau (P-tau), as they are recognized by the International Working Group (IWG) 2 Criteria for AD and the National Institute on Aging-Alzheimer’s Association (NIA-AA) Criteria for AD and MCI associated with AD [35,39].
Generally, the transmembrane protein amyloid precursor protein (APP) predominantly expressed in the brain is enzymatically processed via two routes. Thus, it can be cleaved either by the α-secretase followed by γ-secretase, resulting in the release of soluble APPα through the non-amyloidogenic pathway or by β-secretase followed by γ-secretase, leading to the formation of the highly insoluble Aβ1-42 (composed of 42 amino acids) peptide through the amyloidogenic pathway [34,37] (Figure 1). Among the various Aβ isoforms found in the CSF, the levels of Aβ40 and Aβ42 are the most reliable in terms of assessment for AD diagnosis. Specifically, as Aβ42 aggregates into fibrils and plaques within the brain, its concentration in the CSF is considerably reduced, thus serving as an AD indicator [43,44]. However, while Aβ40 is the most abundant isoform, there are no significant changes in its levels in AD patients. In this case, its levels are analyzed by the Aβ42/Aβ40 ratio, which is more reliable than only assessing Aβ42 concentrations due to individual fluctuation compensations [35,42,45]. Specifically, the Aβ42 values are normalized, as Aβ40 is used as a proxy for the total Aβ values [46]. Moreover, other truncated forms of the Aβ42 amyloidogenic peptide, including Aβ37, Aβ38 and Aβ39, could provide additional diagnostic information. Among them, the accuracy of the Aβ42/Aβ38 ratio is comparable to that of Aβ42/Aβ40 in terms of predicting AD [35,46]. Evidence for these findings relies on autopsy studies, antemortem lumbar CSF analyses, and functional imaging studies based on positron emission tomography using Aβ ligands, e.g., 11c-labelled Pittsburgh Compound [42]. Nonetheless, the use of these biomarkers in routine clinical practice is still in its infancy [40], as there are still some limitations that must be overcome, such as the interindividual differences in the production of Aβ or the overlapping between CSF and Aβ1-42 between neurodegenerative disorders, as in Creutzfeldt–Jakob disease, dementia with Lewy bodies, frontotemporal lobar degeneration, and prodromal and manifest (subcortical) vascular dementia [47,48]. As such, most studies analyze Aβ levels in comparison with T-tau and P-tau values in order to increase accuracy [35]. Furthermore, several studies have investigated the levels of APP cleavage metabolites, including soluble APPα, soluble APPβ and total soluble APP, as biomarkers for AD. However, the results are generally inconsistent due to several reasons, including disease heterogeneity, co-morbidities, assay specificity and sensitivity, antibody cross-reactivity, sampling differences, and CSF processing and storage [49,50]. In this context, one study suggested higher levels of soluble APPα in MCI-AD patients compared with non-AD and control groups, and higher levels of APPβ in both AD and MCI-AD patients [50]. Moreover, soluble APPα and soluble APPβ levels have been associated with biomarkers of BACE1 activity.
Tau is a highly important microtubule-regulating protein abundantly expressed in the cytosol of axons. Its activity mainly focuses on microtubule-related functions, namely tubulin assembly promotion, dynamic instability regulation, a spatial organization in a parallel network, and axonal transport of kinesins and dyneins, which contribute to microtubule stabilization [37,51,52]. The kinase and phosphatase imbalances in AD lead to the hyperphosphorylation of tau and its consequent detachment from microtubules and accumulation into NFTs (Figure 2). Subsequently, tau and P-tau proteins are released into the extracellular space of the CSF, resulting in increased levels characteristic for neurodegeneration [37]. On one hand, tau proteins are assessed by using monoclonal antibodies, which detect all isoforms independently of their phosphorylation state. In AD patients, T-tau concentrations increase by 200–300%, which is further associated with the severity of neuronal/axonal damage and neurodegeneration. However, increased levels of T-tau have also been observed in other neurological disorders, including stroke, brain trauma, or Creutzfeldt–Jakob disease [53,54,55], which makes it less specific for AD. On the other hand, moderately increased levels of P-tau proteins are more accurately associated with AD, as they indicate both the brain phosphorylation state and the NFTs’ formation and load [35,42].
While the deposition of Aβ plaques occurs years or even decades before the onset of the symptoms, and could be used for early diagnosis, tau biomarkers change later as the disease progresses, and are strongly correlated with local degeneration and cognitive decline [37,56]. The most effective strategy for developing a biomarker-based diagnostic tool is to combine both disease-specific and non-specific biomarkers. In this context, the decrease in Aβ42, and concomitant increase in Aβ42/Aβ40 and Aβ42/Aβ38 ratios and T-tau and P-tau levels is commonly referred to as the Alzheimer profile or signature, as it offers the possibility of detecting AD in its early stages [35,42,57,58]. Additionally, their combined use for AD diagnosis is characterized by sensitivity and specificity of approximately 85–95% [59]. Similarly, by increasing the palette of biomarkers, the discrimination between AD and other differential diagnoses, such as MCI, dementia or depression, could be possible.
In this context, recent years have witnessed the rise of a new generation of biomarkers related to AD pathological mechanisms, such as neurofilament light (NFL) for neuronal injury, neurogranin, BACE1, SNAP-25 and synaptotagmin for synaptic dysfunction and/or loss, and sTREM2 and YKL-40 for neuroinflammation, due to the activation of microglia and astrocytes [38,60,61].
The neurofilament heteropolymers are the primary cytoskeleton proteins predominantly found in axons. Among the four subunits, namely the three isoforms NFL, neurofilament medium and neurofilament heavy, and alpha-internexin, NFL is the most abundant [59,62]. Forming the core of the neurofilament, NFL is a triplet protein essential to the structure of the myelin that surrounds the axons within the central nervous system [62,63]. As their presence within the CSF is specific for axonal injury, elevated NFL concentrations have been widely reported in neurodegenerative disorders, especially in AD patients [59,62,63,64]. While the mechanisms of NFL aggregation are still unelucidated, they are thought to be similar to the hyperphosphorylation process of tau proteins [65].
Neurogranin is a small neuron-specific and post-synaptic protein abundantly expressed in the brain, especially in the hippocampal and cerebrocortical dendritic spine [66,67,68]. Neurogranin has been found to play key roles in synaptic plasticity and long-term potentiation as a major regulator of the calcium-binding protein calmodulin and of calcium-signal transduction and memory formation [66,67,68,69]. Autopsy studies revealed a possible correlation between neurogranin and AD, as analyses showed reduced levels of neurogranin in brains and increased levels in the CSF of AD patients [68]. In this regard, there is accumulated evidence confirming the potential of neurogranin as an AD biomarker, both as a full-length molecule and as fragments from the C-terminal half [66,70]. Moreover, it has been shown to be able to detect early-stage pathological changes, even in the MCI stage, and predict and monitor AD-related cognitive decline, thus serving as a promising pre-symptomatic biomarker [67,68]. BACE1 (β-site APP cleaving enzyme-1) is an aspartyl protease discovered in 1999, which, by contrast to other peptidases of the pepsin family, such as cathepsin D and E, is a type I transmembrane protein [69,71]. Commonly expressed in neurons, oligodendrocytes and astrocytes, BACE1 is more abundantly found within certain neuronal cell types [69]. The generation of Aβ monomeric forms is dependent upon the activity of BACE1, this being directly related to synaptic functions, plasticity and homeostasis [69,72]. Studies have shown the significantly increased concentrations and activity rates of BACE1 in AD brains and CSF, which is thought to cause a vicious cycle by producing Aβ peptides near synapses [69,72,73,74,75]. Other synaptic dysfunction-associated biomarkers for AD include synaptotagmin, a calcium sensor protein, SNAP-25, a component of the soluble N-ethylmaleimide sensitive factor attachment protein receptor complex, GAP-43, a pre-synaptic membrane protein, and synaptophysin, which has exhibited increased levels in the CSF of AD patients [69,76].
On one hand, TREM2, the triggering receptor expressed on myeloid cells 2, is a type I transmembrane receptor protein of the innate immune system, selectively expressed on the plasma membrane of microglia and dendrocytes within the central nervous system [77,78,79,80,81]. TREM2 plays fundamental roles in microglial functions, including in the phagocytosis of apoptotic neurons, damaged myelin and amyloid plaques, biosynthetic metabolism, proliferation, migration, survival, cytokine release, lipid sensing, and inflammatory signaling inhibition, and it has been proven to be essential in synapse pruning during early development [79,80,81]. Furthermore, its ectodomain is cleaved in the cell surface and shed at the plasma membrane, thus releasing a soluble fragment (sTREM2) which can be measured in the CSF as an indicator of microglial activity [78,79,80]. As it is involved in the regulation of microglia dynamics, and the subsequent amyloid plaque formation and synaptic plasticity, increased levels of sTREM2 within the CSF have been related to a protective response against AD pathology, thus serving as a potential biomarker [80,81,82,83]. On the other hand, YKL-40, the inflammation-related glycoprotein known as chitinase-3-like protein 1, breast regression protein 39, human cartilage glycoprotein 39 or chondrex, belongs to the family of chitinase-like proteins, but lacks the enzymatic activity of chitinases [84,85]. Normally expressed in the fibrillar astrocytes within the white matter, YKL-40 plays key roles in inflammation, proliferation, angiogenesis and tissue remodeling [84,85,86], and CSF YKL-40 is a biomarker for astroglial activity [80]. Furthermore, elevated levels of YKL-40 in the brain and CSF are generally associated with neurodegeneration, appearing as a pre-clinical sign of AD pathology [80,86,87].
Another important group of AD biomarkers is the microRNAs (miRNAs), which are small non-coding RNAs with an average length of 22 nucleotides, involved in gene expression at the post-transcriptional level, regulation through binding to mRNA targets, and the subsequent translational repression or degradation of the target by the RNA-induced silencing complex [88,89,90]. Although recent studies have been intensively focusing on miRNA deregulation associated with AD, the lack of standardization in the quantification methods and protocols used is considerably challenging for establishing the discrimination power of miRNAs as biomarkers for AD [91]. Thus, the available results are generally not comparable since they target different miRNA molecules, which further increases the complexity of the subject [91,92,93,94,95,96].
The previously described CSF biomarkers for AD and the associated mechanisms of pathology are summarized in Table 1.
3. Blood Biomarkers
Although CSF biomarkers provide significantly more accurate diagnostics of AD and/or MCI, their clinical application is generally limited due to their invasive nature, which is traumatic to patients, and their high costs. Therefore, the scientific focus has shifted towards more accessible biomarkers that could increase their application for clinical practice. In this context, the use of peripheral blood biomarkers for AD diagnosis possesses a series of advantages, namely minimal invasiveness, facile sampling, cost- and time-efficiency, and widespread adoption [67,105].
Nonetheless, although blood communicates with the brain through the blood–brain barrier, the lymph vessels and the glymphatic system, the interchange is indirect. Therefore, the applicability of blood biomarkers in clinical practice is still not possible due to a series of challenges, in terms of both biological and technical issues [60,105,106,107]. First, the central nervous system is an isolated environment and the concentration of the potential biomarkers might be relatively low, as they must cross the blood–brain barrier as intact molecules [106]. Additionally, the volume ratio between the blood and the CSF will cause a significant analyte dilution [60]. However, there is strong evidence of barrier dysfunction in AD patients, which leads to increased protein and other molecule exchanges [105,106]. Second, as blood is a highly complex fluid comprising various molecules and cells, non-specific biomarkers, such as inflammatory or acute phase proteins, could be expressed by sources other than the central nervous system, which further introduces and increases variability within analyses [60,106]. Additionally, the variety of proteins and heterophilic antibodies present in the blood might potentially cause interference in the analysis [60]. Third, blood biomarkers might undergo liver or plasma proteolytic degradation, matrix effects due to plasma protein or blood cell adhesion, or kidney excretion, which will further substantially lower their concentration [60,106]. Fourth, the sensitivity and specificity of blood biomarkers are still considerably low, as there is a high risk of the overlapping of neurodegenerative disorders and other co-morbidities of AD patients that could also change plasma protein profiles [67,106]. Therefore, blood biomarker assays for AD diagnosis still lack standardization between instruments and laboratories, and the complexity of the blood is associated with a series of variables that are challenging in terms of result replication [60,105].
Among the conventional biomarkers for AD, Aβ42, Aβ40 and Aβ42/Aβ40 have been recognized as potential screening molecules [108]. However, early studies led to inconsistency between results and a lack of correlation between CSF and blood Aβ [46,106,109,110,111]. Such results were probably due to low Aβ concentrations in blood and the influences of matrix effects, as plasma proteins have a tendency of binding to Aβ, and the analytical sensitivity of the assay did not allow for diluting these effects [46,109], as measurements were performed using enzyme-linked immunosorbent assay (ELISA) methods [106,110,112]. However, more recent studies are considerably more promising, as they use ultrasensitive immunoassay techniques, such as single-molecule array or SIMOA, immunoprecipitation coupled with mass spectrometry, and stable isotope labeling kinetics followed by immunoprecipitation coupled with mass spectrometry [46,105,106,109,110,111]. As such, the results showed the expected decrease in blood Aβ42, Aβ40 and Aβ42/Aβ40 levels in AD and MCI patients [106,109,110,111,113]. However, the presence of various factors that introduce variability to the results limits the applicability of Aβ as a blood biomarker for AD [105].
Similarly, the introduction of ultrasensitive immunoassay techniques, including SIMOA, mesoscale discovery or MSD, label-free real-time surface plasmon resonance technology, and immunomagnetic reduction, has led to more promising results in terms of T-tau and P-tau blood levels. In this regard, results have shown that increased levels of blood T-tau and P-tau are generally associated with AD [46,106,109]. However, more accurate results have been obtained by using enzymes involved in tau protein hyperphosphorylation processes, such as glycogen synthase kinase 3β (GSK-3β) and dual-specificity tyrosine-phosphorylation regulated kinase A (DYRK1A) [105]. On one hand, GSK-3β is a GSK-3 isoform, part of the serine/threonine kinase family, known for its important roles in neuron polarity and synapse plasticity. Consequently, there is strong evidence of its implications in the pathological mechanisms of neurodegeneration disease development and the progression of tauopathies associated with AD [114,115,116,117]. In this context, blood levels of GSK-3β are considerably elevated in AD and MCI patients, which proves its potential as a blood-based AD biomarker [105,118]. On the other hand, DYRK1A, a member of the proline-directed serine/threonine kinases, is widely known for its implications for cell proliferation, as well as various signaling pathways fundamental for brain development and function, namely neuron survival, synaptic plasticity, and actin cytoskeleton and microtubule regulation [119,120,121]. As AD patients present considerably reduced blood levels, DYRK1A could be used as a potential biomarker [105,122].
The emergence of the ultrasensitive techniques has also allowed for the accurate quantification of blood NFL, which has been shown to closely correlate with CSF results, thus reflecting brain pathology [46,106,110]. Both plasma and serum levels of NFL are elevated in AD and MCI patients years before symptom onset [46,105,109,110,111,123,124]. Additionally, as NFL levels could also serve as biomarkers for disease severity, namely brain atrophy, cognitive impairment or glucose hypometabolism, it can also be used as a biomarker for disease staging [46]. Although it is among the most consistent blood biomarkers [111,123,125], increased concentrations of NFL are not specific for AD, as they have been observed in other neurodegenerative disorders [105,109].
Moreover, several studies have demonstrated that sustained chronic inflammation is directly related to AD development, as postmortem tissues of AD models exhibited inflammatory responses [126]. Among the mediators involved in the systemic immune response regulation, including transcriptional factors, cytokines, chemokines, complements, coagulation factors, enzymes, various peptides and lipids [127], interleukins (IL-1, IL-4, IL-6 and IL-10), cytokine I-309, interferon-γ, and tumor necrosis factor α (TNF-α) are particularly important biomarkers for the early diagnosis of AD [105].
Furthermore, clusterin, also termed as apolipoprotein J, is a highly sialylated multifunctional glycoprotein that is highly expressed in the brain, liver, testicles and ovaries [128,129,130]. Studies show that clusterin is involved in a series of pathophysiological states, including cell death, oxidative stress, proteotoxic stress and neurodegenerative processes [130]. As its main function is to act as a chaperone for various extracellular proteins, it has been demonstrated that clusterin is capable of binding Aβ peptides, thus decreasing Aβ toxicity and the associated apoptosis and oxidative stress [105,130,131]. In this context, as it is found in higher concentrations in the blood of AD patients, clusterin could be a promising AD biomarker [105].
The previously described blood biomarkers for AD and the associated mechanisms of pathology are summarized in Table 2.
4. Saliva Biomarkers
Saliva is a complex biological fluid secreted in the mouth by three main pairs of salivary glands, namely the parotid, the submandibular, and the sublingual, which generate 0.75–1.5 L daily. The compositions of their secretions depend on the sympathetic and parasympathetic stimulation, circadian rhythm, health status, eating habits and drug intake [138,139]. Considering the direct relation between the salivary gland and the nervous system, as the facial nerve innervates the sublingual and submandibular glands through the submandibular ganglion and the glossopharyngeal nerve innervates the parotid gland through the otic ganglion, saliva could represent an important source of biomarkers for nervous system disorders [139,140]. In contrast to blood, saliva is a matrix that can be collected easily and non-invasively, at all ages and many times per day, and assessed through different assays [139,141,142,143,144], which is promising for its future clinical application in the timely detection, diagnosis, prognosis and monitoring of neurological disorders [142,145]. In this regard, a novel term has been introduced, salivaomics, which encompasses all biomarkers discovered within the genome, microbiome, epigenome, transcriptome, proteome and metabolome for the development of translational and clinical tools for diagnosis [145,146].
Therefore, due to the capacity of molecules to pass from the blood to the saliva through passive diffusion, active transport or microfiltration, saliva is a promising AD-related biomarker pool that could be used for its early and accurate diagnosis [147,148]. The most important AD biomarkers found within the saliva are Aβ peptides, T-tau and P-tau, acetylcholine, lactoferrin, and trehalose, each related to different AD pathophysiological mechanism.
Owing to the saliva–blood interactions and the buccal cell degradation, Aβ peptides should also be present in the saliva, as APP is a widely expressed protein in the peripheral tissues. Although the number of studies on the matter is still considerably limited, recent results have shown that salivary Aβ42 is increased in AD patients, while Aβ40 does not change [148,149,150]. However, there are no studies regarding the Aβ42/Aβ40 ratio in the saliva, which should also be validated considering its significant relevance in the CSF [151].
Similarly, studies on salivary T-tau and P-tau are still limited, with preliminary results demonstrating elevated levels of T-tau and P-tau, and also an elevated P-tau/T-tau ratio [152,153]. However, the results are not conclusive, as tau proteins are also expressed and secreted by acinar epithelial cells, the subunits of salivary glands, and released from the cranial nerves [151,154].
Furthermore, as salivary glands are under cholinergic innervation, acetylcholinesterase, a type-B carboxylesterase enzyme mainly found in the synaptic cleft at the post-synaptic neuromuscular junctions, further diffuses into the saliva [151,155,156]. Its primary function is the termination of neuron transmission and signaling, but recent studies have demonstrated its role in the development of AD by promoting Aβ fibril formation [156,157,158]. In this context, the available studies reported reduced levels of salivary acetylcholinesterase associated with aging and even lower levels for AD patients [139,148,151]. However, while they proved its potential as a salivary AD biomarker, the conclusiveness of the results is still limited due to a lack of standardization [151].
Antimicrobial peptides have been previously proposed as biomarkers for brain infections involved in the AD developmental processes [151]. An example of such biomarkers is lactoferrin, a globular non-hemic iron-binding glycoprotein that belongs to the family of serum transferrin proteins, and it is mostly synthesized by glandular epithelial cells and neutrophils [159,160,161,162]. Owing to its iron-binding activity, lactoferrin is a multifunctional protein that exhibits antibacterial, antiviral, antifungal, antioxidant, immunomodulatory, anti-cancer, anti-inflammatory and anti-allergenic properties [160,162,163,164]. Moreover, while there is evidence of lactoferrin presence within the human brain, its levels are substantially increased in AD patients and those with related neurodegenerative disorders, which could be attributed to its Aβ-binding ability [165,166,167]. Therefore, lactoferrin has been associated with AD pathogenesis, as it has been detected in the amyloid plaques, NFTs and microglia of AD brains [164,165]. Studies on AD patients are still limited, but there is strong evidence that the salivary levels of lactoferrin significantly decrease when compared to healthy controls and elderly subjects [139,148,164,168]. Moreover, lactoferrin has also demonstrated its potential for early disease detection, as the accuracy of AD diagnosis using it was greater than with CSF T-tau and Aβ42 [139,151].
The previously described saliva biomarkers for AD and the associated mechanisms of pathology are summarized in Table 3.
5. Emerging Body Fluid Biomarkers
Recent years have witnessed significant advancements in the profiling technologies, which have improved the detection sensitivity and allowed for the quantification of minute samples. In this manner, previously difficult-to-assess body fluids, such as urine, tears or olfactory fluids, have become a rich source of biocompounds that could reflect the pathological state of an individual [171].
Urine has become a highly desirable source of disease biomarkers, as it can easily and non-invasively be collected in relatively large volumes. Additionally, it contains cellular components, biochemical compounds, and proteins originating from plasma glomerular filtration, renal tubule excretion or urogenital tract secretion, thus reflecting the metabolic and pathophysiological condition of an individual. In this context, recent works have focused on the plethora of biomarkers present within the urinary proteins, glycoproteins and exosomes that could allow for the early diagnosis, prognosis, prevention or treatment of various diseases [172,173]. Furthermore, urine can also reflect AD pathology signs, generally associated with modifications in protein and lipid metabolism caused by oxidative stress [174,175]. Moreover, since the concentration of the creatinine waste product is physiologically stable, it can be used for normalizing urine biomarker concentrations [174]. In this context, the most promising urinary biomarkers include isoprostane [176], glycine and total free amino acids [177], and 8-hydroxy-2‘-deoxyguanosine [178], which have achieved over 90% accuracy [174,175].
While tears are available in considerably reduced volumes for sampling, they are a neglected key reservoir of biomarkers, with great potential in medical diagnostics [179,180]. Tears are complex protein, lipid, mucin, water and salt mixtures, and the development of novel proteomic, lipidomic and glycomic techniques has allowed for a complete understanding of these components and their changes associated with ocular or non-ocular disorders [171,181,182]. For example, proteomic techniques have revealed the presence of AD-related peptides within aqueous humor samples [183], while tear fluid has proven to be clinically relevant through the discovery of a combination of four tear proteins, namely lipocalin-1, dermicidin, lysozyme C and lactritin, with a sensitivity of 81% and a specificity of 77% for AD [184,185]. Another study suggested the discriminatory power of tear T-tau and Aβ42, as their levels increased in AD patients [186]. Additionally, total microRNA abundance was also found at increased levels in AD patients, with microRNA-200b-5p as the most promising AD biomarker [183,187].
Moreover, several studies have reported the isolation of NFTs and identified increased levels of T-tau and P-tau in AD patients’ nasal secretions [35], thus proving the potential of olfactory fluids as non-invasive AD biomarkers.
6. Conclusions and Future Perspectives
AD is the most common neurodegenerative disorder that predominantly affects the elderly population. Thus, it is expected that the number of AD patients worldwide will reach 60 million by 2030, which will have a significant impact on the global health system. The current diagnosis methods involve cognitive tests, neuroimaging techniques and CSF assays. However, there is still no clinical strategy available for the accurate and early detection of AD. Recent trends have focused on identifying novel biomarkers beyond Aβ and tau proteins, as well as new matrices as biomarker sources, such as the blood, saliva, urine, tear or olfactory fluids. While there have been considerable advancements in the field, the lack of standardized sampling and assays poses significant challenges for the use of such biomarkers in the clinical practice. In this context, recent trends have been focusing on the identification of protein or lipid panels, which could better reflect the complete mechanisms of AD.
Furthermore, research should also focus on the development of advanced platforms and biosensor devices that could provide real-time information regarding the health status of AD patients [188]. In this context, biosensor-on-chip devices could represent a promising strategy for accurately assessing a great pallet of AD biomarkers.
Author Contributions
A.F.B., C.C., A.M.G. have participated in review writing and revision. All authors have read and agreed to the published version of the manuscript.
Funding
This manuscript received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Mythri, R.B.; Srinivas Bharath, M.M. Chapter 9-Omics and Epigenetics of Polyphenol-Mediated Neuroprotection: The Curcumin Perspective. In Curcumin for Neurological and Psychiatric Disorders; Farooqui, T., Farooqui, A.A., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 169–189. [Google Scholar] [CrossRef]
- Farooqui, A.A. Chapter 1-Classification and Molecular Aspects of Neurotraumatic Diseases: Similarities and Differences With Neurodegenerative and Neuropsychiatric Diseases. In Ischemic and Traumatic Brain and Spinal Cord Injuries; Farooqui, A.A., Ed.; Academic Press: Cambridge, MA, USA, 2018; pp. 1–40. [Google Scholar] [CrossRef]
- Peña-Bautista, C.; Casas-Fernández, E.; Vento, M.; Baquero, M.; Cháfer-Pericás, C. Stress and neurodegeneration. Clin. Chim. Acta 2020, 503, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Lima, J.A.; Hamerski, L. Chapter 8-Alkaloids as Potential Multi-Target Drugs to Treat Alzheimer’s Disease. In Studies in Natural Products Chemistry; Atta ur, R., Ed.; Elsevier: Amsterdam, The Netherlands, 2019; Volume 61, pp. 301–334. [Google Scholar]
- Sheikh, S.; Safia; Haque, E.; Mir, S.S. Neurodegenerative Diseases: Multifactorial Conformational Diseases and Their Therapeutic Interventions. J. Neurodegener. Dis. 2013, 2013, 563481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zyuz’kov, G.N.; Suslov, N.I.; Miroshnichenko, L.A.; Simanina, E.V.; Polykova, T.Y.; Stavrova, L.A.; Zhdanov, V.V.; Minakova, M.Y.; Udut, E.V.; Udut, V.V. Halogenated (CL-ion) songorine is a new original agonist of fibroblast growth factor receptors of neuronal-committed progenitors possessing neuroregenerative effect after cerebral ischemia and hypoxia in experimental animals. Biointerface Res. Appl. Chem. 2019, 9, 4317–4326. [Google Scholar] [CrossRef]
- Gitler, A.D.; Dhillon, P.; Shorter, J. Neurodegenerative disease: Models, mechanisms, and a new hope. Dis. Model. Mech. 2017, 10, 499–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farkhondeh, T.; Forouzanfar, F.; Roshanravan, B.; Samarghandian, S. Curcumin effect on non-amyloidogenic pathway for preventing alzheimer’s disease. Biointerface Res. Appl. Chem. 2019, 9, 4085–4089. [Google Scholar] [CrossRef]
- Steffen, J. “A Battle You Would Never Choose to Fight”: The Management of Neurodegenerative Diseases as a Societal Challenge. Neurodegener. Dis. 2019, 19, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Sardoiwala, M.N.; Kaundal, B.; Roy Choudhury, S. Chapter 37-Development of Engineered Nanoparticles Expediting Diagnostic and Therapeutic Applications Across Blood–Brain Barrier. In Handbook of Nanomaterials for Industrial Applications; Mustansar Hussain, C., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 696–709. [Google Scholar] [CrossRef]
- Balasa, A.; Balasa, R.; Egyed-Zsigmond, I.; Chinezu, R.J.T.N. Bilateral thalamic glioma: Case report and review of the literature. Turk. Neurosurg. 2016, 26, 321–324. [Google Scholar] [CrossRef] [Green Version]
- Gherasim, D.N.; Gherman, B.; Balasa, A.J.R.J.O.N. Clinical Evolution of Primary Intramedullary Tumors in Adults. Rom. J. Neurol. 2012, 11, 165–171. [Google Scholar]
- Balasa, A.; Tamas, F.; Hurghis, C.; Maier, S.; Motataianu, A.; Chinezu, R. First-Onset Hypokalemic Periodic Paralysis Following Surgery for Myxopapillary Ependymoma. World Neurosurg. 2020, 141, 389–394. [Google Scholar] [CrossRef]
- Sánchez-López, E.; Marina, M.L. Chapter 20-Neuroscience Applications of Capillary Electrophoretic Methods. In Capillary Electromigration Separation Methods; Poole, C.F., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 481–510. [Google Scholar] [CrossRef]
- Aravalli, R.N.; Shiao, M.; Lu, W.-C.; Xie, H.; Pearce, C.; Toman, N.G.; Danczyk, G.; Sipe, C.; Miller, Z.D.; Crane, A.; et al. Chapter 15-The Bioengineering of Exogenic Organs and/or Cells for Use in Regenerative Medicine. In Engineering in Medicine; Iaizzo, P.A., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 381–415. [Google Scholar] [CrossRef]
- Gherasim, D.N.; Gyorki, G.; Balasa, A.J.R.N. Single center experience and technical nuances in the treatment of distal anterior cerebral artery aneurysms. Rom. Neurosurg. 2017, 31, 17–24. [Google Scholar] [CrossRef]
- Serafín, V.; Gamella, M.; Pedrero, M.; Montero-Calle, A.; Razzino, C.A.; Yáñez-Sedeño, P.; Barderas, R.; Campuzano, S.; Pingarrón, J.M. Enlightening the advancements in electrochemical bioanalysis for the diagnosis of Alzheimer’s disease and other neurodegenerative disorders. J. Pharm. Biomed. Anal. 2020, 189, 113437. [Google Scholar] [CrossRef] [PubMed]
- Brazaca, L.C.; Sampaio, I.; Zucolotto, V.; Janegitz, B.C. Applications of biosensors in Alzheimer’s disease diagnosis. Talanta 2020, 210, 120644. [Google Scholar] [CrossRef]
- Chávez-Gutiérrez, L.; Szaruga, M. Mechanisms of neurodegeneration—Insights from familial Alzheimer’s disease. Semin. Cell Dev. Biol. 2020, 105, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Monajjemi, M. Molecular vibration of dopamine neurotransmitter: A relation between its normal modes and harmonic notes. Biointerface Res. Appl. Chem. 2019, 9, 3956–3962. [Google Scholar] [CrossRef]
- Pham, T.T.; Monajjemi, M.; Dang, D.M.T.; Mollaamin, F.; Dang, C.M. Reaction of cell membrane bilayers “as a variable capacitor” with G-protein: A reason for neurotransmitter signaling. Biointerface Res. Appl. Chem. 2019, 9, 3874–3883. [Google Scholar] [CrossRef]
- Gupta, J.; Fatima, M.T.; Islam, Z.; Khan, R.H.; Uversky, V.N.; Salahuddin, P. Nanoparticle formulations in the diagnosis and therapy of Alzheimer’s disease. Int. J. Biol. Macromol. 2019, 130, 515–526. [Google Scholar] [CrossRef]
- Yao, F.; Zhang, K.; Zhang, Y.; Guo, Y.; Li, A.; Xiao, S.; Liu, Q.; Shen, L.; Ni, J. Identification of Blood Biomarkers for Alzheimer’s Disease Through Computational Prediction and Experimental Validation. Front. Neurol. 2019, 9, 1158. [Google Scholar] [CrossRef]
- Adina, S.; Anca, M.; Zoltan, B.; Adrian, B. Guillain–Barré and Acute Transverse Myelitis Overlap Syndrome Following Obstetric Surgery. J. Crit. Care Med. 2020, 6, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Maier, S.; Motataianu, A.; Bajko, Z.; Romaniuc, A.; Balasa, A. Pontine cavernoma haemorrhage at 24 weeks of pregnancy that resulted in eight-and-a-half syndrome. Acta Neurol. Belg. 2019, 119, 471–474. [Google Scholar] [CrossRef]
- Balasa, A.; Chinezu, R.; Gherasim, D.N.J.R.N. Surgical management of tuberculum sellae and planum sphenoidale meningiomas. Rom. Neurosurg. 2013, 20, 92–99. [Google Scholar]
- Anca, M.; Laura Iulia, B.; Smaranda, M.; Adrian, B.; Adina, S. Cardiac Autonomic Neuropathy in Diabetes Mellitus Patients–Are We Aware of the Consequences? Acta Marisiensis-Ser. Med. 2020, 66, 3–8. [Google Scholar] [CrossRef]
- Rossini, P.M.; Di Iorio, R.; Vecchio, F.; Anfossi, M.; Babiloni, C.; Bozzali, M.; Bruni, A.C.; Cappa, S.F.; Escudero, J.; Fraga, F.J.; et al. Early diagnosis of Alzheimer’s disease: The role of biomarkers including advanced EEG signal analysis. Report from the IFCN-sponsored panel of experts. Clin. Neurophysiol. 2020, 131, 1287–1310. [Google Scholar] [CrossRef]
- Atri, A. The Alzheimer’s Disease Clinical Spectrum: Diagnosis and Management. Med. Clin. N. Am. 2019, 103, 263–293. [Google Scholar] [CrossRef]
- Khoury, R.; Ghossoub, E. Diagnostic biomarkers of Alzheimer’s disease: A state-of-the-art review. Biomark. Neuropsychiatry 2019, 1, 100005. [Google Scholar] [CrossRef]
- Premi, E.; Calhoun, V.D.; Diano, M.; Gazzina, S.; Cosseddu, M.; Alberici, A.; Archetti, S.; Paternicò, D.; Gasparotti, R.; van Swieten, J.; et al. The inner fluctuations of the brain in pre-symptomatic Frontotemporal Dementia: The chronnectome fingerprint. NeuroImage 2019, 189, 645–654. [Google Scholar] [CrossRef] [Green Version]
- Mobed, A.; Hasanzadeh, M. Biosensing: The best alternative for conventional methods in detection of Alzheimer’s disease biomarkers. Int. J. Biol. Macromol. 2020, 161, 59–71. [Google Scholar] [CrossRef] [PubMed]
- Kawata, K.; Tierney, R.; Langford, D. Blood and cerebrospinal fluid biomarkers. Handb. Clin. Neurol. 2018, 158, 217–233. [Google Scholar] [CrossRef] [PubMed]
- Lewczuk, P.; Riederer, P.; O’Bryant, S.E.; Verbeek, M.M.; Dubois, B.; Visser, P.J.; Jellinger, K.A.; Engelborghs, S.; Ramirez, A.; Parnetti, L.; et al. Cerebrospinal fluid and blood biomarkers for neurodegenerative dementias: An update of the Consensus of the Task Force on Biological Markers in Psychiatry of the World Federation of Societies of Biological Psychiatry. World J. Biol. Psychiatry 2018, 19, 244–328. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.C.; Kim, S.J.; Hong, S.; Kim, Y. Diagnosis of Alzheimer’s disease utilizing amyloid and tau as fluid biomarkers. Exp. Mol. Med. 2019, 51, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, G.A. Chapter 4-Cerebrospinal Fluid: Formation, Absorption, Markers, and Relationship to Blood–Brain Barrier. In Primer on Cerebrovascular Diseases (Second Edition); Caplan, L.R., Biller, J., Leary, M.C., Lo, E.H., Thomas, A.J., Yenari, M., Zhang, J.H., Eds.; Academic Press: San Diego, CA, USA, 2017; pp. 25–31. [Google Scholar] [CrossRef]
- Niemantsverdriet, E.; Valckx, S.; Bjerke, M.; Engelborghs, S. Alzheimer’s disease CSF biomarkers: Clinical indications and rational use. Acta Neurol. Belg. 2017, 117, 591–602. [Google Scholar] [CrossRef] [Green Version]
- Teunissen, C.E.; Verheul, C.; Willemse, E.A.J. Chapter 1-The use of cerebrospinal fluid in biomarker studies. In Handbook of Clinical Neurology; Deisenhammer, F., Teunissen, C.E., Tumani, H., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 146, pp. 3–20. [Google Scholar]
- Robey, T.T.; Panegyres, P.K. Cerebrospinal fluid biomarkers in neurodegenerative disorders. Future Neurol. 2019, 14, FNL6. [Google Scholar] [CrossRef] [Green Version]
- Cognat, E.; Mouton Liger, F.; Troussière, A.-C.; Wallon, D.; Dumurgier, J.; Magnin, E.; Duron, E.; Gabelle, A.; Croisile, B.; de la Sayette, V.; et al. What is the clinical impact of cerebrospinal fluid biomarkers on final diagnosis and management in patients with mild cognitive impairment in clinical practice? Results from a nation-wide prospective survey in France. BMJ Open 2019, 9, e026380. [Google Scholar] [CrossRef] [PubMed]
- Mounsey, A.L.; Zeitler, M.R. Cerebrospinal Fluid Biomarkers for Detection of Alzheimer Disease in Patients with Mild Cognitive Impairment. Am. Fam. Physician 2018, 97, 714–715. [Google Scholar]
- Pawlowski, M.; Meuth, S.G.; Duning, T. Cerebrospinal Fluid Biomarkers in Alzheimer’s Disease-From Brain Starch to Bench and Bedside. Diagnostics 2017, 7, 42. [Google Scholar] [CrossRef] [Green Version]
- Boumenir, A.; Cognat, E.; Sabia, S.; Hourregue, C.; Lilamand, M.; Dugravot, A.; Bouaziz-Amar, E.; Laplanche, J.-L.; Hugon, J.; Singh-Manoux, A.; et al. CSF level of β-amyloid peptide predicts mortality in Alzheimer’s disease. Alzheimer’s Res. Ther. 2019, 11, 29. [Google Scholar] [CrossRef] [Green Version]
- Hu, W.T.; Watts, K.D.; Shaw, L.M.; Howell, J.C.; Trojanowski, J.Q.; Basra, S.; Glass, J.D.; Lah, J.J.; Levey, A.I. CSF beta-amyloid 1-42-what are we measuring in Alzheimer’s disease? Ann. Clin. Transl. Neurol. 2015, 2, 131–139. [Google Scholar] [CrossRef]
- Biscetti, L.; Salvadori, N.; Farotti, L.; Cataldi, S.; Eusebi, P.; Paciotti, S.; Parnetti, L. The added value of Aβ42/Aβ40 in the CSF signature for routine diagnostics of Alzheimer’s disease. Clin. Chim. Acta 2019, 494, 71–73. [Google Scholar] [CrossRef]
- Milà-Alomà, M.; Suárez-Calvet, M.; Molinuevo, J.L. Latest advances in cerebrospinal fluid and blood biomarkers of Alzheimer’s disease. Ther. Adv. Neurol. Disord. 2019, 12, 1756286419888819. [Google Scholar] [CrossRef] [Green Version]
- Bjerke, M.; Engelborghs, S. Cerebrospinal Fluid Biomarkers for Early and Differential Alzheimer’s Disease Diagnosis. J. Alzheimers Dis. 2018, 62, 1199–1209. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.C.; Zheng, T.; Duan, R.; Zhu, L.; Zhang, Q.G. On the Biomarkers of Alzheimer’s Disease. Adv. Exp. Med. Biol. 2020, 1232, 409–414. [Google Scholar] [CrossRef]
- Habib, A.; Sawmiller, D.; Tan, J. Restoring Soluble Amyloid Precursor Protein α Functions as a Potential Treatment for Alzheimer’s Disease. J. Neurosci. Res. 2017, 95, 973–991. [Google Scholar] [CrossRef] [Green Version]
- Araki, W.; Hattori, K.; Kanemaru, K.; Yokoi, Y.; Omachi, Y.; Takano, H.; Sakata, M.; Yoshida, S.; Tsukamoto, T.; Murata, M.; et al. Re-evaluation of soluble APP-α and APP-β in cerebrospinal fluid as potential biomarkers for early diagnosis of dementia disorders. Biomark. Res. 2017, 5, 28. [Google Scholar] [CrossRef] [Green Version]
- Barbier, P.; Zejneli, O.; Martinho, M.; Lasorsa, A.; Belle, V.; Smet-Nocca, C.; Tsvetkov, P.O.; Devred, F.; Landrieu, I. Role of Tau as a Microtubule-Associated Protein: Structural and Functional Aspects. Front. Aging Neurosci. 2019, 11, 204. [Google Scholar] [CrossRef] [Green Version]
- Hervy, J.; Bicout, D.J. Dynamical decoration of stabilized-microtubules by Tau-proteins. Sci. Rep. 2019, 9, 12473. [Google Scholar] [CrossRef] [Green Version]
- Andone, S.; Petrutiu, S.; Bajko, Z.; Motataianu, A.; Maier, S.; Macavei, I.; Stoian, A.; Balasa, A.; Balasa, R.J.R.J.O.N. Sporadic Creutzfeldt-Jakob Disease: A Clinical Approach of A Small Case Series and Literature Review. Rom. J. Neurol. 2017, 16, 109–115. [Google Scholar]
- Motataianu, A.; Barcutean, L.; Gherman, I.; Maier, S.; Bajko, Z.; Balasa, A.J.R.J.O.N. Cerebellar and brainstem infarction secondary to basilar artery dolichoectasia. Rom. J. Neurol. 2019, 18, 109–115. [Google Scholar]
- Rares, C.; Hurghis, C.; Tamas, F.; Balasa, A.J.R.N. Our Experience with the Use of Oich Score in Intracerebral Haemorrhage. Rom. Neurosurg. 2019, 33, 41–43. [Google Scholar]
- Vogel, J.W.; Iturria-Medina, Y.; Strandberg, O.T.; Smith, R.; Levitis, E.; Evans, A.C.; Hansson, O.; Weiner, M.; Aisen, P.; Petersen, R.; et al. Spread of pathological tau proteins through communicating neurons in human Alzheimer’s disease. Nat. Commun. 2020, 11, 2612. [Google Scholar] [CrossRef]
- Hansson, O.; Lehmann, S.; Otto, M.; Zetterberg, H.; Lewczuk, P. Advantages and disadvantages of the use of the CSF Amyloid β (Aβ) 42/40 ratio in the diagnosis of Alzheimer’s Disease. Alzheimer’s Res. Ther. 2019, 11, 34. [Google Scholar] [CrossRef]
- Zetterberg, H.; Bendlin, B.B. Biomarkers for Alzheimer’s disease-preparing for a new era of disease-modifying therapies. Mol. Psychiatry 2020. [Google Scholar] [CrossRef]
- Jin, M.; Cao, L.; Dai, Y.-P. Role of Neurofilament Light Chain as a Potential Biomarker for Alzheimer’s Disease: A Correlative Meta-Analysis. Front. Aging Neurosci. 2019, 11, 254. [Google Scholar] [CrossRef] [PubMed]
- Zetterberg, H.; Blennow, K. From Cerebrospinal Fluid to Blood: The Third Wave of Fluid Biomarkers for Alzheimer’s Disease. J. Alzheimer’s Dis. 2008, 64, S271–S279. [Google Scholar] [CrossRef] [Green Version]
- Park, S.A.; Han, S.M.; Kim, C.E. New fluid biomarkers tracking non-amyloid-β and non-tau pathology in Alzheimer’s disease. Exp. Mol. Med. 2020, 52, 556–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glushakova, O.Y.; Glushakov, A.V.; Mannix, R.; Miller, E.R.; Valadka, A.B.; Hayes, R.L. Chapter 8-The Use of Blood-Based Biomarkers to Improve the Design of Clinical Trials of Traumatic Brain Injury. In Handbook of Neuroemergency Clinical Trials, 2nd ed.; Skolnick, B.E., Alves, W.M., Eds.; Academic Press: Cambridge, MA, USA, 2018; pp. 139–166. [Google Scholar] [CrossRef]
- Sillman, B.; Woldstad, C.; McMillan, J.; Gendelman, H.E. Chapter 3-Neuropathogenesis of human immunodeficiency virus infection. In Handbook of Clinical Neurology; Brew, B.J., Ed.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 152, pp. 21–40. [Google Scholar]
- Zetterberg, H.; Skillbäck, T.; Mattsson, N.; Trojanowski, J.Q.; Portelius, E.; Shaw, L.M.; Weiner, M.W.; Blennow, K.; Initiative, F.T.A.S.D.N. Association of Cerebrospinal Fluid Neurofilament Light Concentration With Alzheimer Disease Progression. JAMA Neurol. 2016, 73, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Didonna, A.; Opal, P. The role of neurofilament aggregation in neurodegeneration: Lessons from rare inherited neurological disorders. Mol. Neurodegener. 2019, 14, 19. [Google Scholar] [CrossRef] [PubMed]
- Becker, B.; Nazir, F.H.; Brinkmalm, G.; Camporesi, E.; Kvartsberg, H.; Portelius, E.; Boström, M.; Kalm, M.; Höglund, K.; Olsson, M.; et al. Alzheimer-associated cerebrospinal fluid fragments of neurogranin are generated by Calpain-1 and prolyl endopeptidase. Mol. Neurodegener. 2018, 13, 47. [Google Scholar] [CrossRef]
- Liu, W.; Lin, H.; He, X.; Chen, L.; Dai, Y.; Jia, W.; Xue, X.; Tao, J.; Chen, L. Neurogranin as a cognitive biomarker in cerebrospinal fluid and blood exosomes for Alzheimer’s disease and mild cognitive impairment. Transl. Psychiatry 2020, 10, 125. [Google Scholar] [CrossRef]
- Willemse, E.A.J.; De Vos, A.; Herries, E.M.; Andreasson, U.; Engelborghs, S.; van der Flier, W.M.; Scheltens, P.; Crimmins, D.; Ladenson, J.H.; Vanmechelen, E.; et al. Neurogranin as Cerebrospinal Fluid Biomarker for Alzheimer Disease: An Assay Comparison Study. Clin. Chem. 2018, 64, 927–937. [Google Scholar] [CrossRef]
- Hampel, H.; Vassar, R.; De Strooper, B.; Hardy, J.; Willem, M.; Singh, N.; Zhou, J.; Yan, R.; Vanmechelen, E.; De Vos, A.; et al. The β-Secretase BACE1 in Alzheimer’s Disease. Biol. Psychiatry 2020. [Google Scholar] [CrossRef]
- Schipke, C.G.; De Vos, A.; Fuentes, M.; Jacobs, D.; Vanmechelen, E.; Peters, O. Neurogranin and BACE1 in CSF as Potential Biomarkers Differentiating Depression with Cognitive Deficits from Early Alzheimer’s Disease: A Pilot Study. Dement. Geriatr. Cogn. Disord. Extra 2018, 8, 277–289. [Google Scholar] [CrossRef]
- Kellner, S.; Ferchichi, M.J.I.J.O.A.R. Diagnosis and monitoring of Alzheimer Disease with saliva biomarker BACE1. Int. J. Aging Res. 2018, 1, 21. [Google Scholar]
- Das, B.; Yan, R. Role of BACE1 in Alzheimer’s synaptic function. Transl. Neurodegener. 2017, 6, 23. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, P.; Thierjung, N.; Grimmer, T.; Ortner, M.; Economou, P.; Assimakopoulos, K.; Gourzis, P.; Politis, A.; Perneczky, R. Cerebrospinal Fluid BACE1 Activity and sAβPPβ as Biomarker Candidates of Alzheimer’s Disease. Dement. Geriatr. Cogn. Disord. 2018, 45, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Wang, P.; Bian, X.; Xu, S.; Zhou, Q.; Zhang, Y.; Ding, M.; Han, M.; Huang, L.; Bi, J.; et al. Elevated plasma levels of exosomal BACE1-AS combined with the volume and thickness of the right entorhinal cortex may serve as a biomarker for the detection of Alzheimer’s disease. Mol. Med. Rep. 2020, 22, 227–238. [Google Scholar] [CrossRef]
- Tam, J.M.; Josephson, L.; Pilozzi, A.R.; Huang, X. A Novel Dual Fluorochrome Near-Infrared Imaging Probe for Potential Alzheimer’s Enzyme Biomarkers-BACE1 and Cathepsin D. Molecules 2020, 25, 274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calderon-Garcidueñas, A.L.; Duyckaerts, C. Chapter 23-Alzheimer disease. In Handbook of Clinical Neurology; Kovacs, G.G., Alafuzoff, I., Eds.; Elsevier: Amsterdam, The Netherlands, 2018; Volume 145, pp. 325–337. [Google Scholar]
- Belsare, K.; Wu, H.; DeGrado, W. Interaction of sTREM2 with Amyloid Beta: Implication on the Protective Role of sTREM2 in Alzheimer’s Disease. FASEB J. 2020, 34, 1. [Google Scholar] [CrossRef]
- Halaas, N.B.; Henjum, K.; Blennow, K.; Dakhil, S.; Idland, A.-V.; Nilsson, L.N.; Sederevicius, D.; Vidal-Piñeiro, D.; Walhovd, K.B.; Wyller, T.B.; et al. CSF sTREM2 and Tau Work Together in Predicting Increased Temporal Lobe Atrophy in Older Adults. Cereb. Cortex 2019, 30, 2295–2306. [Google Scholar] [CrossRef]
- Suárez-Calvet, M.; Morenas-Rodríguez, E.; Kleinberger, G.; Schlepckow, K.; Araque Caballero, M.Á.; Franzmeier, N.; Capell, A.; Fellerer, K.; Nuscher, B.; Eren, E.; et al. Early increase of CSF sTREM2 in Alzheimer’s disease is associated with tau related-neurodegeneration but not with amyloid-β pathology. Mol. Neurodegener. 2019, 14, 1. [Google Scholar] [CrossRef] [Green Version]
- Falcon, C.; Monté-Rubio, G.C.; Grau-Rivera, O.; Suárez-Calvet, M.; Sánchez-Valle, R.; Rami, L.; Bosch, B.; Haass, C.; Gispert, J.D.; Molinuevo, J.L. CSF glial biomarkers YKL40 and sTREM2 are associated with longitudinal volume and diffusivity changes in cognitively unimpaired individuals. Neuroimage Clin. 2019, 23, 101801. [Google Scholar] [CrossRef]
- Zhong, L.; Xu, Y.; Zhuo, R.; Wang, T.; Wang, K.; Huang, R.; Wang, D.; Gao, Y.; Zhu, Y.; Sheng, X.; et al. Soluble TREM2 ameliorates pathological phenotypes by modulating microglial functions in an Alzheimer’s disease model. Nat. Commun. 2019, 10, 1365. [Google Scholar] [CrossRef] [Green Version]
- Knapskog, A.-B.; Henjum, K.; Idland, A.-V.; Eldholm, R.S.; Persson, K.; Saltvedt, I.; Watne, L.O.; Engedal, K.; Nilsson, L.N.G. Cerebrospinal fluid sTREM2 in Alzheimer’s disease: Comparisons between clinical presentation and AT classification. Sci. Rep. 2020, 10, 15886. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Calvet, M.; Kleinberger, G.; Araque Caballero, M.; Brendel, M.; Rominger, A.; Alcolea, D.; Fortea, J.; Lleó, A.; Blesa, R.; Gispert, J.D.; et al. sTREM2 cerebrospinal fluid levels are a potential biomarker for microglia activity in early-stage Alzheimer’s disease and associate with neuronal injury markers. EMBO Mol. Med. 2016, 8, 466–476. [Google Scholar] [CrossRef] [PubMed]
- Väänänen, T.; Vuolteenaho, K.; Kautiainen, H.; Nieminen, R.; Möttönen, T.; Hannonen, P.; Korpela, M.; Kauppi, M.J.; Laiho, K.; Kaipiainen-Seppänen, O.; et al. Glycoprotein YKL-40: A potential biomarker of disease activity in rheumatoid arthritis during intensive treatment with csDMARDs and infliximab. Evidence from the randomised controlled NEO-RACo trial. PLoS ONE 2017, 12, e0183294. [Google Scholar] [CrossRef] [Green Version]
- Salomon, J.; Matusiak, Ł.; Nowicka-Suszko, D.; Szepietowski, J.C. Chitinase-3-Like Protein 1 (YKL-40) Is a New Biomarker of Inflammation in Psoriasis. Mediat. Inflamm. 2017, 2017, 9538451. [Google Scholar] [CrossRef] [Green Version]
- Llorens, F.; Thüne, K.; Tahir, W.; Kanata, E.; Diaz-Lucena, D.; Xanthopoulos, K.; Kovatsi, E.; Pleschka, C.; Garcia-Esparcia, P.; Schmitz, M.; et al. YKL-40 in the brain and cerebrospinal fluid of neurodegenerative dementias. Mol. Neurodegener. 2017, 12, 83. [Google Scholar] [CrossRef]
- Wang, L.; Gao, T.; Cai, T.; Li, K.; Zheng, P.; Liu, J. Cerebrospinal fluid levels of YKL-40 in prodromal Alzheimer’s disease. Neurosci. Lett. 2020, 715, 134658. [Google Scholar] [CrossRef]
- Schmitz, U.; Gupta, S.K.; Vera, J.; Wolkenhauer, O. Computational Approaches in microRNA Biology. In Encyclopedia of Biomedical Engineering; Narayan, R., Ed.; Elsevier: Oxford, UK, 2019; pp. 317–330. [Google Scholar] [CrossRef]
- O’Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of MicroRNA Biogenesis, Mechanisms of Actions, and Circulation. Front. Endocrinol. 2018, 9, 402. [Google Scholar] [CrossRef] [Green Version]
- Jevšinek Skok, D.; Hauptman, N.; Boštjančič, E.; Zidar, N. The integrative knowledge base for miRNA-mRNA expression in colorectal cancer. Sci. Rep. 2019, 9, 18065. [Google Scholar] [CrossRef] [Green Version]
- Swarbrick, S.; Wragg, N.; Ghosh, S.; Stolzing, A. Systematic Review of miRNA as Biomarkers in Alzheimer’s Disease. Mol. Neurobiol. 2019, 56, 6156–6167. [Google Scholar] [CrossRef] [Green Version]
- Wiedrick, J.T.; Phillips, J.I.; Lusardi, T.A.; McFarland, T.J.; Lind, B.; Sandau, U.S.; Harrington, C.A.; Lapidus, J.A.; Galasko, D.R.; Quinn, J.F.; et al. Validation of MicroRNA Biomarkers for Alzheimer’s Disease in Human Cerebrospinal Fluid. J. Alzheimers Dis. 2019, 67, 875–891. [Google Scholar] [CrossRef]
- Mushtaq, G.; Greig, N.H.; Anwar, F.; Zamzami, M.A.; Choudhry, H.; Shaik, M.M.; Tamargo, I.A.; Kamal, M.A. miRNAs as Circulating Biomarkers for Alzheimer’s Disease and Parkinson’s Disease. Med. Chem. 2016, 12, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Angelucci, F.; Cechova, K.; Valis, M.; Kuca, K.; Zhang, B.; Hort, J. MicroRNAs in Alzheimer’s Disease: Diagnostic Markers or Therapeutic Agents? Front. Pharm. 2019, 10, 665. [Google Scholar] [CrossRef]
- Wei, W.; Wang, Z.-Y.; Ma, L.-N.; Zhang, T.-T.; Cao, Y.; Li, H. MicroRNAs in Alzheimer’s Disease: Function and Potential Applications as Diagnostic Biomarkers. Front. Mol. Neurosci. 2020, 13, 160. [Google Scholar] [CrossRef]
- Zendjabil, M. Circulating microRNAs as novel biomarkers of Alzheimer’s disease. Clin. Chim. Acta 2018, 484, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Tariciotti, L.; Casadei, M.; Honig, L.S.; Teich, A.F.; McKhann Ii, G.M.; Tosto, G.; Mayeux, R. Clinical Experience with Cerebrospinal Fluid Aβ42, Total and Phosphorylated Tau in the Evaluation of 1,016 Individuals for Suspected Dementia. J. Alzheimers Dis. 2018, 65, 1417–1425. [Google Scholar] [CrossRef] [Green Version]
- Slaets, S.; Le Bastard, N.; Martin, J.J.; Sleegers, K.; Van Broeckhoven, C.; De Deyn, P.P.; Engelborghs, S. Cerebrospinal fluid Aβ1-40 improves differential dementia diagnosis in patients with intermediate P-tau181P levels. J. Alzheimers Dis. 2013, 36, 759–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spies, P.E.; Slats, D.; Sjögren, J.M.; Kremer, B.P.; Verhey, F.R.; Rikkert, M.G.; Verbeek, M.M. The cerebrospinal fluid amyloid beta42/40 ratio in the differentiation of Alzheimer’s disease from non-Alzheimer’s dementia. Curr. Alzheimer Res. 2010, 7, 470–476. [Google Scholar] [CrossRef] [Green Version]
- Dhiman, K.; Gupta, V.B.; Villemagne, V.L.; Eratne, D.; Graham, P.L.; Fowler, C.; Bourgeat, P.; Li, Q.-X.; Collins, S.; Bush, A.I.; et al. Cerebrospinal fluid neurofilament light concentration predicts brain atrophy and cognition in Alzheimer’s disease. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2020, 12, e12005. [Google Scholar] [CrossRef]
- Janelidze, S.; Zetterberg, H.; Mattsson, N.; Palmqvist, S.; Vanderstichele, H.; Lindberg, O.; van Westen, D.; Stomrud, E.; Minthon, L.; Blennow, K.; et al. CSF Aβ42/Aβ40 and Aβ42/Aβ38 ratios: Better diagnostic markers of Alzheimer disease. Ann. Clin. Transl. Neurol. 2016, 3, 154–165. [Google Scholar] [CrossRef] [Green Version]
- Wellington, H.; Paterson, R.W.; Portelius, E.; Törnqvist, U.; Magdalinou, N.; Fox, N.C.; Blennow, K.; Schott, J.M.; Zetterberg, H. Increased CSF neurogranin concentration is specific to Alzheimer disease. Neurology 2016, 86, 829–835. [Google Scholar] [CrossRef] [Green Version]
- Mouton-Liger, F.; Dumurgier, J.; Cognat, E.; Hourregue, C.; Zetterberg, H.; Vanderstichele, H.; Vanmechelen, E.; Bouaziz-Amar, E.; Blennow, K.; Hugon, J.; et al. CSF levels of the BACE1 substrate NRG1 correlate with cognition in Alzheimer’s disease. Alzheimer’s Res. Ther. 2020, 12, 88. [Google Scholar] [CrossRef]
- Antonell, A.; Mansilla, A.; Rami, L.; Lladó, A.; Iranzo, A.; Olives, J.; Balasa, M.; Sanchez-Valle, R.; Molinuevo, J. Cerebrospinal Fluid Level of YKL-40 Protein in Preclinical and Prodromal Alzheimer’s Disease. J. Alzheimers Dis. 2014, 42, 901–908. [Google Scholar] [CrossRef]
- Altuna-Azkargorta, M.; Mendioroz-Iriarte, M. Blood biomarkers in Alzheimer’s disease. Neurol. (Engl. Ed.) 2020. [Google Scholar] [CrossRef]
- Hampel, H.; O’Bryant, S.E.; Molinuevo, J.L.; Zetterberg, H.; Masters, C.L.; Lista, S.; Kiddle, S.J.; Batrla, R.; Blennow, K. Blood-based biomarkers for Alzheimer disease: Mapping the road to the clinic. Nat. Rev. Neurol. 2018, 14, 639–652. [Google Scholar] [CrossRef] [PubMed]
- Balasa, R.; Barcutean, L.; Balasa, A.; Motataianu, A.; Roman-Filip, C.; Manu, D. The action of TH17 cells on blood brain barrier in multiple sclerosis and experimental autoimmune encephalomyelitis. Hum. Immunol. 2020, 81, 237–243. [Google Scholar] [CrossRef]
- Zetterberg, H. Blood-based biomarkers for Alzheimer’s disease-An update. J. Neurosci. Methods 2018, 319. [Google Scholar] [CrossRef] [Green Version]
- Zetterberg, H.; Burnham, S.C. Blood-based molecular biomarkers for Alzheimer’s disease. Mol. Brain 2019, 12, 26. [Google Scholar] [CrossRef] [PubMed]
- Gabelli, C. Blood and cerebrospinal fluid biomarkers for Alzheimer’s disease. J. Lab. Precis. Med. 2020, 5. [Google Scholar] [CrossRef]
- Toombs, J.; Zetterberg, H. In the blood: Biomarkers for amyloid pathology and neurodegeneration in Alzheimer’s disease. Brain Commun. 2020, 2, fcaa054. [Google Scholar] [CrossRef] [PubMed]
- Oeckl, P.; Otto, M. A Review on MS-Based Blood Biomarkers for Alzheimer’s Disease. Neurol. Ther. 2019, 8, 113–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Bryant, S.E. Blood Biomarkers for Use in Alzheimer Disease—Moving From “If” to “How?”. JAMA Neurol. 2019, 76, 1009–1010. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Chen, H.; Wold, E.A.; Zhou, J. 2.13-Small-Molecule Inhibitors of Protein–Protein Interactions. In Comprehensive Medicinal Chemistry III; Chackalamannil, S., Rotella, D., Ward, S.E., Eds.; Elsevier: Oxford, UK, 2017; pp. 329–353. [Google Scholar] [CrossRef] [Green Version]
- Mercier, J.; Provins, L.; Hannestad, J. 7.02-Progress and Challenges in the Development of PET Ligands to Aid CNS Drug Discovery. In Comprehensive Medicinal Chemistry III; Chackalamannil, S., Rotella, D., Ward, S.E., Eds.; Elsevier: Oxford, UK, 2017; pp. 20–64. [Google Scholar] [CrossRef]
- Patel, P.; Woodgett, J.R. Chapter Eight-Glycogen Synthase Kinase 3: A Kinase for All Pathways? In Current Topics in Developmental Biology; Jenny, A., Ed.; Academic Press: Cambridge, MA, USA, 2017; Volume 123, pp. 277–302. [Google Scholar]
- Shi, X.-L.; Yan, N.; Cui, Y.-J.; Liu, Z.-P. A Unique GSK-3β inhibitor B10 Has a Direct Effect on Aβ, Targets Tau and Metal Dyshomeostasis, and Promotes Neuronal Neurite Outgrowth. Cells 2020, 9, 649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hugon, J.; Mouton-Liger, F.; Cognat, E.; Dumurgier, J.; Paquet, C. Blood-Based Kinase Assessments in Alzheimer’s Disease. Front Aging Neurosci. 2018, 10, 338. [Google Scholar] [CrossRef]
- Paciorkowski, A.R.; Seltzer, L.E.; Neul, J.L. 32-Developmental Encephalopathies. In Swaiman’s Pediatric Neurology (Sixth Edition); Swaiman, K.F., Ashwal, S., Ferriero, D.M., Schor, N.F., Finkel, R.S., Gropman, A.L., Pearl, P.L., Shevell, M.I., Eds.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 242–248. [Google Scholar] [CrossRef]
- McNerney, M.W.; Mobley, W.C.; Salehi, A. Down Syndrome or Trisomy 21☆. In Reference Module in Neuroscience and Biobehavioral Psychology; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar] [CrossRef]
- Kaas, G.A.; Hawkins, K.E.; Sweatt, J.D. 4.19-Genetic Mechanisms of Memory Disorders (Excluding Alzheimer’s Disease). In Learning and Memory: A Comprehensive Reference, 2nd ed.; Byrne, J.H., Ed.; Academic Press: Oxford, UK, 2017; pp. 371–401. [Google Scholar] [CrossRef]
- Dowjat, K.; Adayev, T.; Wojda, U.; Brzozowska, K.; Barczak, A.; Gabryelewicz, T.; Hwang, Y.-W. Abnormalities of DYRK1A-Cytoskeleton Complexes in the Blood Cells as Potential Biomarkers of Alzheimer’s Disease. J. Alzheimers Dis. 2019, 72, 1059–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mattsson, N.; Cullen, N.C.; Andreasson, U.; Zetterberg, H.; Blennow, K. Association Between Longitudinal Plasma Neurofilament Light and Neurodegeneration in Patients With Alzheimer Disease. JAMA Neurol. 2019, 76, 791–799. [Google Scholar] [CrossRef] [PubMed]
- van der Ende, E.L.; Meeter, L.H.; Poos, J.M.; Panman, J.L.; Jiskoot, L.C.; Dopper, E.G.P.; Papma, J.M.; de Jong, F.J.; Verberk, I.M.W.; Teunissen, C.; et al. Serum neurofilament light chain in genetic frontotemporal dementia: A longitudinal, multicentre cohort study. Lancet Neurol. 2019, 18, 1103–1111. [Google Scholar] [CrossRef]
- Weston, P.S.J.; Poole, T.; Ryan, N.S.; Nair, A.; Liang, Y.; Macpherson, K.; Druyeh, R.; Malone, I.B.; Ahsan, R.L.; Pemberton, H.; et al. Serum neurofilament light in familial Alzheimer disease: A marker of early neurodegeneration. Neurology 2017, 89, 2167–2175. [Google Scholar] [CrossRef] [Green Version]
- Kinney, J.W.; Bemiller, S.M.; Murtishaw, A.S.; Leisgang, A.M.; Salazar, A.M.; Lamb, B.T. Inflammation as a central mechanism in Alzheimer’s disease. Alzheimers Dement 2018, 4, 575–590. [Google Scholar] [CrossRef]
- Newcombe, E.A.; Camats-Perna, J.; Silva, M.L.; Valmas, N.; Huat, T.J.; Medeiros, R. Inflammation: The link between co-morbidities, genetics, and Alzheimer’s disease. J. Neuroinflamm. 2018, 15, 276. [Google Scholar] [CrossRef]
- Figueroa, D.M.; Gordon, E.M.; Yao, X.; Levine, S.J. Chapter 13-Apolipoproteins as context-dependent regulators of lung inflammation. In Mechanisms and Manifestations of Obesity in Lung Disease; Johnston, R.A., Suratt, B.T., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 301–326. [Google Scholar] [CrossRef]
- Bornhorst, J.A.; Mbughuni, M.M. Chapter 3-Alcohol Biomarkers: Clinical Issues and Analytical Methods. In Critical Issues in Alcohol and Drugs of Abuse Testing, 2nd ed.; Dasgupta, A., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 25–42. [Google Scholar] [CrossRef]
- Foster, E.M.; Dangla-Valls, A.; Lovestone, S.; Ribe, E.M.; Buckley, N.J. Clusterin in Alzheimer’s Disease: Mechanisms, Genetics, and Lessons From Other Pathologies. Front. Neurosci. 2019, 13, 164. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.-C.; Yu, J.-T.; Li, Y.; Tan, L. Chapter 5-Clusterin in Alzheimer’s disease. In Advances in Clinical Chemistry; Makowski, G.S., Ed.; Elsevier: Amsterdam, The Netherlands, 2012; Volume 56, pp. 155–173. [Google Scholar]
- Kaneko, N.; Nakamura, A.; Washimi, Y.; Kato, T.; Sakurai, T.; Arahata, Y.; Bundo, M.; Takeda, A.; Niida, S.; Ito, K.; et al. Novel plasma biomarker surrogating cerebral amyloid deposition. Proc. Jpn. Acad. Ser. B Phys. Biol. Sci. 2014, 90, 353–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janelidze, S.; Stomrud, E.; Palmqvist, S.; Zetterberg, H.; van Westen, D.; Jeromin, A.; Song, L.; Hanlon, D.; Tan Hehir, C.A.; Baker, D.; et al. Plasma β-amyloid in Alzheimer’s disease and vascular disease. Sci. Rep. 2016, 6, 26801. [Google Scholar] [CrossRef] [PubMed]
- Fossati, S.; Ramos Cejudo, J.; Debure, L.; Pirraglia, E.; Sone, J.Y.; Li, Y.; Chen, J.; Butler, T.; Zetterberg, H.; Blennow, K.; et al. Plasma tau complements CSF tau and P-tau in the diagnosis of Alzheimer’s disease. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2019, 11, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Karikari, T.K.; Pascoal, T.A.; Ashton, N.J.; Janelidze, S.; Benedet, A.L.; Rodriguez, J.L.; Chamoun, M.; Savard, M.; Kang, M.S.; Therriault, J.J.T.L.N. Blood phosphorylated tau 181 as a biomarker for Alzheimer’s disease: A diagnostic performance and prediction modelling study using data from four prospective cohorts. Lancet Neurol. 2020, 19, 422–433. [Google Scholar] [CrossRef]
- Lewczuk, P.; Ermann, N.; Andreasson, U.; Schultheis, C.; Podhorna, J.; Spitzer, P.; Maler, J.M.; Kornhuber, J.; Blennow, K.; Zetterberg, H. Plasma neurofilament light as a potential biomarker of neurodegeneration in Alzheimer’s disease. Alzheimer’s Res. Ther. 2018, 10, 71. [Google Scholar] [CrossRef] [PubMed]
- Vishnu, V.Y.; Modi, M.; Sharma, S.; Mohanty, M.; Goyal, M.K.; Lal, V.; Khandelwal, N.; Mittal, B.R.; Prabhakar, S. Role of Plasma Clusterin in Alzheimer’s Disease-A Pilot Study in a Tertiary Hospital in Northern India. PLoS ONE 2016, 11, e0166369. [Google Scholar] [CrossRef]
- Lorenzo-Pouso, A.I.; Pérez-Sayáns, M.; Bravo, S.B.; López-Jornet, P.; García-Vence, M.; Alonso-Sampedro, M.; Carballo, J.; García-García, A. Protein-Based Salivary Profiles as Novel Biomarkers for Oral Diseases. Dis. Markers 2018, 2018, 6141845. [Google Scholar] [CrossRef]
- Farah, R.; Haraty, H.; Salame, Z.; Fares, Y.; Ojcius, D.M.; Said Sadier, N. Salivary biomarkers for the diagnosis and monitoring of neurological diseases. Biomed. J. 2018, 41, 63–87. [Google Scholar] [CrossRef]
- Jasim, H.; Carlsson, A.; Hedenberg-Magnusson, B.; Ghafouri, B.; Ernberg, M. Saliva as a medium to detect and measure biomarkers related to pain. Sci. Rep. 2018, 8, 3220. [Google Scholar] [CrossRef] [Green Version]
- Smith, R.; Chepisheva, M.; Cronin, T.; Seemungal, B.M. Chapter 16-Diagnostic Approaches Techniques in Concussion/Mild Traumatic Brain Injury: Where are we? In Neurosensory Disorders in Mild Traumatic Brain Injury; Hoffer, M.E., Balaban, C.D., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 247–277. [Google Scholar] [CrossRef]
- Güvenç, I.A. Salivary Glands: New Approaches in Diagnostics and Treatment; BoD–Books on Demand: Hamburg, Germany, 2019. [Google Scholar]
- Engeland, C.G.; Bosch, J.A.; Rohleder, N.J.C.O.I.B.S. Salivary biomarkers in psychoneuroimmunology. Curr. Opin. Behav. Sci. 2019, 28, 58–65. [Google Scholar] [CrossRef]
- Andrews, J.L.; Fernandez, F. Salivary biomarkers in Alzheimer’s disease. In Diagnosis and Management in Dementia; Elsevier: Amsterdam, The Netherlands, 2020; pp. 239–254. [Google Scholar]
- Rapado-González, Ó.; Martínez-Reglero, C.; Salgado-Barreira, Á.; Takkouche, B.; López-López, R.; Suárez-Cunqueiro, M.M.; Muinelo-Romay, L. Salivary biomarkers for cancer diagnosis: A meta-analysis. Ann. Med. 2020, 52, 131–144. [Google Scholar] [CrossRef] [PubMed]
- Cristaldi, M.; Mauceri, R.; Di Fede, O.; Giuliana, G.; Campisi, G.; Panzarella, V. Salivary Biomarkers for Oral Squamous Cell Carcinoma Diagnosis and Follow-Up: Current Status and Perspectives. Front. Physiol. 2019, 10, 1476. [Google Scholar] [CrossRef] [PubMed]
- Tvarijonaviciute, A.; Zamora, C.; Ceron, J.J.; Bravo-Cantero, A.F.; Pardo-Marin, L.; Valverde, S.; Lopez-Jornet, P. Salivary biomarkers in Alzheimer’s disease. Clin. Oral Investig. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ashton, N.J.; Ide, M.; Zetterberg, H.; Blennow, K. Salivary Biomarkers for Alzheimer’s Disease and Related Disorders. Neurol. Ther. 2019, 8, 83–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabbagh, M.N.; Shi, J.; Lee, M.; Arnold, L.; Al-Hasan, Y.; Heim, J.; McGeer, P. Salivary beta amyloid protein levels are detectable and differentiate patients with Alzheimer’s disease dementia from normal controls: Preliminary findings. BMC Neurol. 2018, 18, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, M.; Guo, J.-P.; Kennedy, K.; McGeer, E.; McGeer, P. A Method for Diagnosing Alzheimer’s Disease Based on Salivary Amyloid-β Protein 42 Levels. J. Alzheimer’s Dis. 2016, 55, 1–8. [Google Scholar] [CrossRef]
- Liang, D.; Lu, H. Salivary biological biomarkers for Alzheimer’s disease. Arch. Oral Biol. 2019, 105, 5–12. [Google Scholar] [CrossRef]
- Gleerup, H.S.; Hasselbalch, S.G.; Simonsen, A.H. Biomarkers for Alzheimer’s Disease in Saliva: A Systematic Review. Dis. Markers 2019, 2019, 4761054. [Google Scholar] [CrossRef]
- Pekeles, H.; Qureshi, H.Y.; Paudel, H.K.; Schipper, H.M.; Gornistky, M.; Chertkow, H. Development and validation of a salivary tau biomarker in Alzheimer’s disease. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2019, 11, 53–60. [Google Scholar] [CrossRef]
- Ashton, N.J.; Ide, M.; Schöll, M.; Blennow, K.; Lovestone, S.; Hye, A.; Zetterberg, H. No association of salivary total tau concentration with Alzheimer’s disease. Neurobiol. Aging 2018, 70, 125–127. [Google Scholar] [CrossRef] [Green Version]
- Bittner, E.A.; Martyn, J.A.J. 21-Neuromuscular Physiology and Pharmacology. In Pharmacology and Physiology for Anesthesia, 2nd ed.; Hemmings, H.C., Egan, T.D., Eds.; Elsevier: Philadelphia, PA, USA, 2019; pp. 412–427. [Google Scholar] [CrossRef]
- Trang, A.; Khandhar, P.B. Physiology, Acetylcholinesterase. In StatPearls [Internet]; StatPearls Publishing: St, Petersburd, FL, USA, 2019. [Google Scholar]
- Lushchekina, S.V.; Masson, P. Slow-binding inhibitors of acetylcholinesterase of medical interest. Neuropharmacology 2020, 177, 108236. [Google Scholar] [CrossRef] [PubMed]
- Reale, M.; Gonzales-Portillo, I.; Borlongan, C.V. Saliva, an easily accessible fluid as diagnostic tool and potent stem cell source for Alzheimer’s Disease: Present and future applications. Brain Res. 2020, 1727, 146535. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R. Chapter 17-Whey Proteins in Functional Foods. In Whey Proteins; Deeth, H.C., Bansal, N., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 637–663. [Google Scholar] [CrossRef]
- Mudgil, D.; Barak, S. 3-Dairy-Based Functional Beverages. In Milk-Based Beverages; Grumezescu, A.M., Holban, A.M., Eds.; Woodhead Publishing Sawton: Cambridge, UK, 2019; pp. 67–93. [Google Scholar] [CrossRef]
- Bourbon, A.I.; Martins, J.T.; Pinheiro, A.C.; Madalena, D.A.; Marques, A.; Nunes, R.; Vicente, A.A. 6-Nanoparticles of lactoferrin for encapsulation of food ingredients. In Biopolymer Nanostructures for Food Encapsulation Purposes; Jafari, S.M., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 147–168. [Google Scholar] [CrossRef]
- Mehmood, A.M.M.T.; Iyer, A.B.; Arif, S.; Junaid, M.; Khan, R.S.; Nazir, W.; Khalid, N. 5-Whey Protein-Based Functional Energy Drinks Formulation and Characterization. In Sports and Energy Drinks; Grumezescu, A.M., Holban, A.M., Eds.; Woodhead Publishing Sawton: Cambridge, UK, 2019; pp. 161–181. [Google Scholar] [CrossRef]
- Karav, S. Chapter 22-Application of a Novel Endo-β-N-Acetylglucosaminidase to Isolate an Entirely New Class of Bioactive Compounds: N-Glycans. In Enzymes in Food Biotechnology; Kuddus, M., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 389–404. [Google Scholar] [CrossRef]
- González-Sánchez, M.; Bartolome, F.; Antequera, D.; Puertas-Martín, V.; González, P.; Gómez-Grande, A.; Llamas-Velasco, S.; San Martín, A.H.; Pérez-Martínez, D.; Villarejo-Galende, A. Decreased salivary lactoferrin levels are specific to Alzheimer’s disease. EBioMedicine 2020, 57. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, W.A.; Salama, R.M.; Schaalan, M.F. A pilot study on the effect of lactoferrin on Alzheimer’s disease pathological sequelae: Impact of the p-Akt/PTEN pathway. Biomed. Pharmacother. 2019, 111, 714–723. [Google Scholar] [CrossRef]
- Paraskevaidi, M.; Allsop, D.; Karim, S.; Martin, F.L.; Crean, S. Diagnostic Biomarkers for Alzheimer’s Disease Using Non-Invasive Specimens. J. Clin. Med. 2020, 9, 1673. [Google Scholar] [CrossRef]
- Dupree, E.J.; Darie, C.C.J.E. Examination of a non-invasive biomarker for the diagnosis of prodromal Alzheimer’s disease and Alzheimer’s disease Dementia. EBioMedicine 2020, 57. [Google Scholar] [CrossRef]
- Carro, E.; Bartolomé, F.; Bermejo-Pareja, F.; Villarejo-Galende, A.; Molina, J.A.; Ortiz, P.; Calero, M.; Rabano, A.; Cantero, J.L.; Orive, G. Early diagnosis of mild cognitive impairment and Alzheimer’s disease based on salivary lactoferrin. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2017, 8, 131–138. [Google Scholar] [CrossRef]
- Bermejo-Pareja, F.; Antequera, D.; Vargas, T.; Molina, J.A.; Carro, E. Saliva levels of Abeta1-42 as potential biomarker of Alzheimer’s disease: A pilot study. BMC Neurol. 2010, 10, 108. [Google Scholar] [CrossRef] [Green Version]
- Bakhtiari, S.; Moghadam, N.B.; Ehsani, M.; Mortazavi, H.; Sabour, S.; Bakhshi, M.J.J.O.C.; JCDR, D.R. Can salivary acetylcholinesterase be a diagnostic biomarker for Alzheimer? J. Clin. Diagn. Res. 2017, 11, ZC58. [Google Scholar] [CrossRef]
- Hagan, S.; Martin, E.; Enríquez-de-Salamanca, A. Tear fluid biomarkers in ocular and systemic disease: Potential use for predictive, preventive and personalised medicine. EPMA J. 2016, 7, 15. [Google Scholar] [CrossRef] [Green Version]
- Jing, J.; Gao, Y. Urine biomarkers in the early stages of diseases: Current status and perspective. Discov. Med. 2018, 25, 57–65. [Google Scholar]
- Harpole, M.; Davis, J.; Espina, V. Current state of the art for enhancing urine biomarker discovery. Expert Rev. Proteom. 2016, 13, 609–626. [Google Scholar] [CrossRef] [Green Version]
- Hrubešová, K.; Fousková, M.; Habartová, L.; Fišar, Z.; Jirák, R.; Raboch, J.; Setnička, V. Search for biomarkers of Alzheimer‘s disease: Recent insights, current challenges and future prospects. Clin. Biochem. 2019, 72, 39–51. [Google Scholar] [CrossRef]
- Hartmann, S.; Kist, T.B.L. A review of biomarkers of Alzheimer’s disease in non-invasive samples. Biomark. Med. 2018, 12, 677–690. [Google Scholar] [CrossRef] [PubMed]
- García-Blanco, A.; Peña-Bautista, C.; Oger, C.; Vigor, C.; Galano, J.-M.; Durand, T.; Martín-Ibáñez, N.; Baquero, M.; Vento, M.; Cháfer-Pericás, C. Reliable determination of new lipid peroxidation compounds as potential early Alzheimer Disease biomarkers. Talanta 2018, 184, 193–201. [Google Scholar] [CrossRef] [PubMed]
- Dunstan, R.H.; Sparkes, D.L.; Macdonald, M.M.; De Jonge, X.J.; Dascombe, B.J.; Gottfries, J.; Gottfries, C.G.; Roberts, T.K. Diverse characteristics of the urinary excretion of amino acids in humans and the use of amino acid supplementation to reduce fatigue and sub-health in adults. Nutr. J. 2017, 16, 19. [Google Scholar] [CrossRef] [Green Version]
- Zengi, O.; Karakas, A.; Ergun, U.; Senes, M.; Inan, L.; Yucel, D. Urinary 8-hydroxy-2′-deoxyguanosine level and plasma paraoxonase 1 activity with Alzheimer’s disease %J Clinical Chemistry and Laboratory Medicine (CCLM). Clin. Chem. Lab. Med. 2012, 50, 529. [Google Scholar] [CrossRef] [PubMed]
- Tamhane, M.; Cabrera-Ghayouri, S.; Abelian, G.; Viswanath, V. Review of Biomarkers in Ocular Matrices: Challenges and Opportunities. Pharm. Res. 2019, 36, 40. [Google Scholar] [CrossRef] [Green Version]
- Iyengar, M.F.; Soto, L.F.; Requena, D.; Ruiz-Alejos, A.O.; Huaylinos, Y.; Velasquez, R.; Bernabe-Ortiz, A.; Gilman, R.H. Tear biomarkers and corneal sensitivity as an indicator of neuropathy in type 2 diabetes. Diabetes Res. Clin. Pract. 2020, 163, 108143. [Google Scholar] [CrossRef]
- Willcox, M.D. Tear film, contact lenses and tear biomarkers. Clin. Exp. Optom. 2019, 102, 350–363. [Google Scholar] [CrossRef] [Green Version]
- Fong, P.Y.; Shih, K.C.; Lam, P.Y.; Chan, T.C.Y.; Jhanji, V.; Tong, L. Role of tear film biomarkers in the diagnosis and management of dry eye disease. Taiwan J. Ophthalmol. 2019, 9, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.K.H.; Li, Q.-X.; He, Z.; Vingrys, A.J.; Wong, V.H.Y.; Currier, N.; Mullen, J.; Bui, B.V.; Nguyen, C.T.O. The Eye as a Biomarker for Alzheimer’s Disease. Front. Neurosci. 2016, 10, 536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, H. Could tear proteins be biomarkers for Alzheimer disease? Nat. Rev. Neurol. 2016, 12, 432. [Google Scholar] [CrossRef] [PubMed]
- Kalló, G.; Emri, M.; Varga, Z.; Ujhelyi, B.; Tőzsér, J.; Csutak, A.; Csősz, É. Changes in the Chemical Barrier Composition of Tears in Alzheimer’s Disease Reveal Potential Tear Diagnostic Biomarkers. PLoS ONE 2016, 11, e0158000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gijs, M.; Nuijts, R.M.; Ramakers, I.; Verhey, F.; Webers, C.A.J.I.O.; Science, V. Differences in tear protein biomarkers between patients with Alzheimer’s disease and controls. Investig. Ophthalmol. Vis. Sci. 2019, 60, 1744. [Google Scholar]
- Kenny, A.; Jiménez-Mateos, E.M.; Zea-Sevilla, M.A.; Rábano, A.; Gili-Manzanaro, P.; Prehn, J.H.M.; Henshall, D.C.; Ávila, J.; Engel, T.; Hernández, F. Proteins and microRNAs are differentially expressed in tear fluid from patients with Alzheimer’s disease. Sci. Rep. 2019, 9, 15437. [Google Scholar] [CrossRef] [Green Version]
- François, M.; Bull, C.F.; Fenech, M.F.; Leifert, W.R.J.C.A.R. Current state of saliva biomarkers for aging and Alzheimer’s disease. Curr. Alzheimer Res. 2019, 16, 56–66. [Google Scholar] [CrossRef]
Figure 1.
The non-amyloidogenic and amyloidogenic pathways involved in the enzymatic processing of APP.
Figure 1.
The non-amyloidogenic and amyloidogenic pathways involved in the enzymatic processing of APP.

Figure 2.
The formation of neurofibrillary tangles through the process of tau protein hyperphosphorylation.
Figure 2.
The formation of neurofibrillary tangles through the process of tau protein hyperphosphorylation.


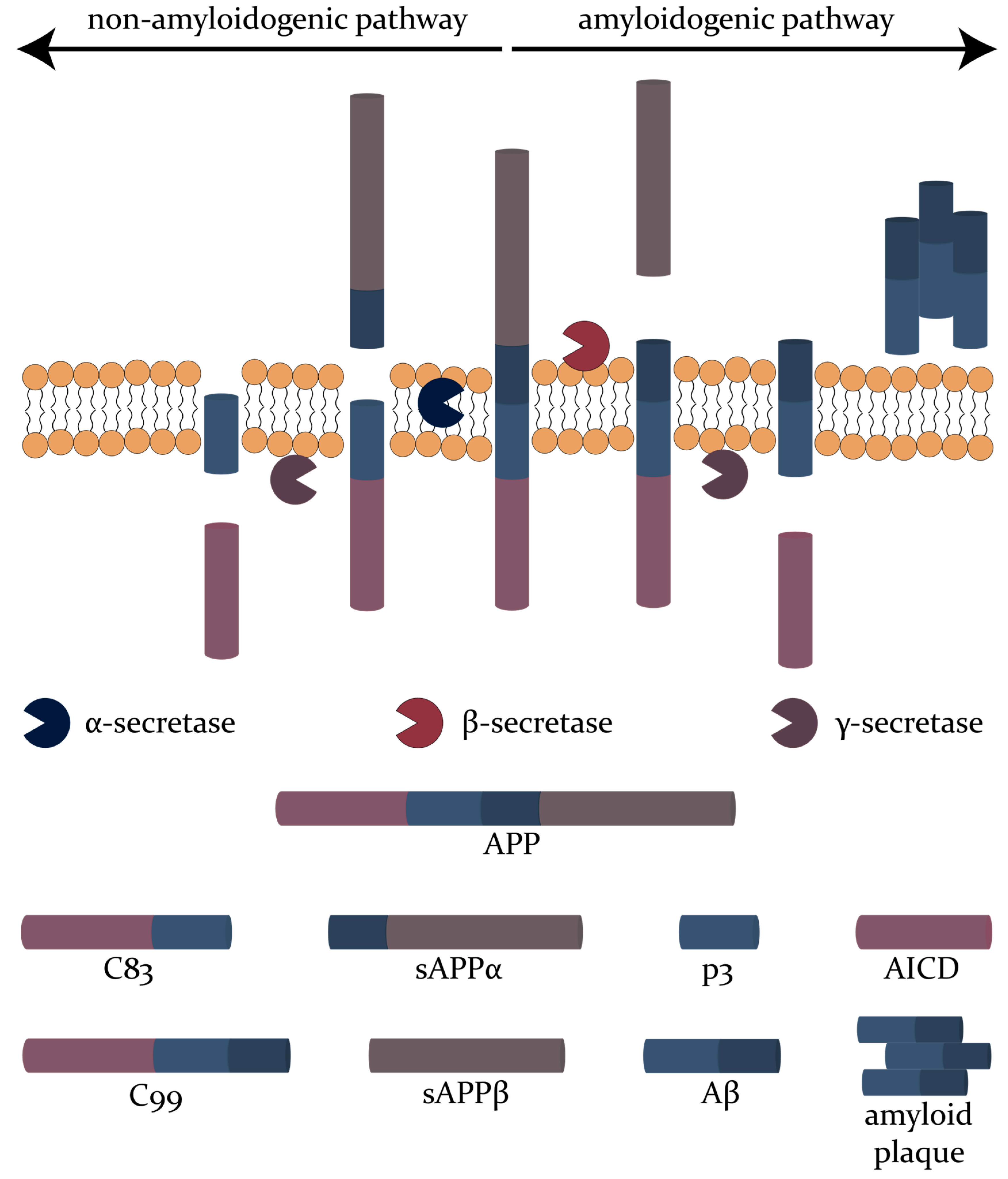{kind=link}
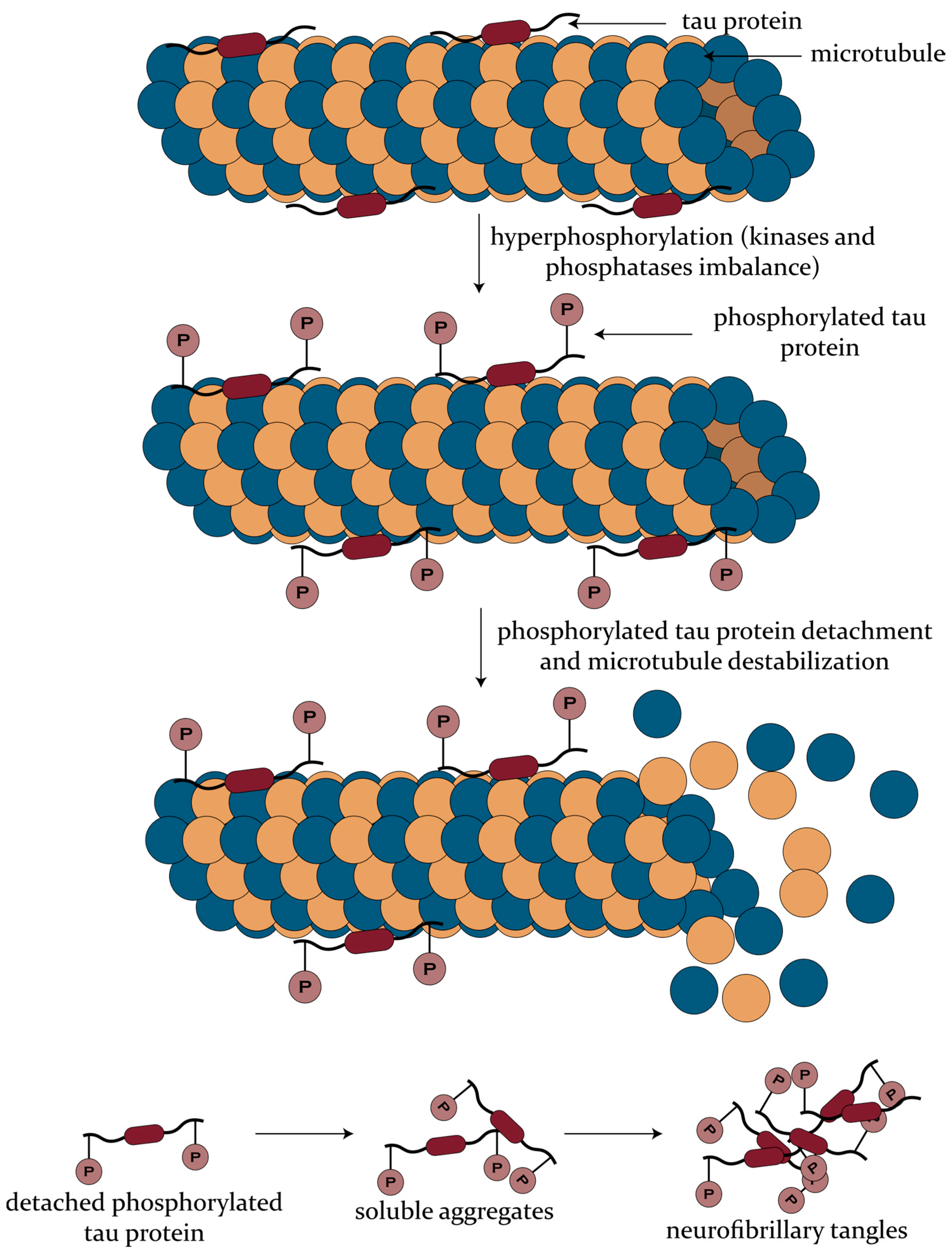{kind=link}
Table 1.
The major changes of the identified CSF biomarkers for AD and the associated mechanisms of pathology.
Table 1.
The major changes of the identified CSF biomarkers for AD and the associated mechanisms of pathology.
| Mechanism of AD Pathology | CSF Biomarker | Change in AD Pathology | Sensitivity | Specificity | References |
|---|---|---|---|---|---|
| Aβ plaque deposition | Aβ42 | ↓ | 0.69–0.81 | 0.44–0.89 | [43,97,98,99,100] |
| Aβ40 | - | 0.72 | 0.39 | [98,101] | |
| Aβ38 | - | 0.63 | 0.56 | [98,101] | |
| Aβ42/Aβ40 | ↑ | 0.81–0.93 | 0.60–1 | [45,97,98,99] | |
| Aβ42/Aβ38 | ↑ | 0.92 | 0.89 | [101] | |
| tau pathology | T-tau | ↑↑ | 0.74–0.77 | 0.70–0.75 | [97,100] |
| P-tau | ↑ | 0.66–0.73 | 0.63–0.82 | [97,100] | |
| neuronal injury | NFL | ↑ | 0.81 | 0.79 | [100] |
| synaptic dysfunction and/or loss | neurogranin | ↑ | 0.73 | 0.84 | [102] |
| BACE1 | ↑ | 0.87 | 0.63 | [103] | |
| synaptotagmin | ↑ | n.r. | n.r. | [69,76] | |
| SNAP-25 | ↑ | n.r. | n.r. | [69,76] | |
| GAP-43 | ↑ | n.r. | n.r. | [69,76] | |
| synaptophysin | ↑ | n.r. | n.r. | [69,76] | |
| neuroinflammation | sTREM2 | ↑ | n.r. | n.r. | [82,83] |
| YKL-40 | ↑ | 0.77–0.85 | 0.81–0.84 | [80,86,87,104] |
n.r.—not reported; ↓—decrease; ↑—increase; ↑↑—high increase.
Table 2.
The major changes of the identified blood biomarkers for AD and the associated mechanisms of pathology.
Table 2.
The major changes of the identified blood biomarkers for AD and the associated mechanisms of pathology.
| Mechanism of AD Pathology | Blood Biomarker | Change in AD Pathology | Sensitivity | Specificity | References |
|---|---|---|---|---|---|
| Aβ plaque deposition | Aβ42 | ↓ | 0.82 | 0.77 | [35,132,133] |
| Aβ40 | ↓ | n.r. | n.r. | [133] | |
| Aβ42/Aβ40 | ↓ | 0.75 | 0.77 | [35,132,133] | |
| tau pathology | T-tau | ↑ | 0.62 | 0.54 | [134] |
| P-tau | ↑ | n.r. | n.r. | [135] | |
| GSK-3β | ↑ | n.r. | n.r. | [105,118] | |
| DYRK1A | ↓ | n.r. | n.r. | [105,122] | |
| neuronal injury | NFL | ↑ | 0.86 | 0.76 | [136] |
| inflammation | IL-1, IL-4, IL-6, and IL-10 | ↑ | n.r. | n.r. | [105] |
| cytokine I-309 | ↑ | n.r. | n.r. | [105] | |
| interferon-γ | ↑ | n.r. | n.r. | [105] | |
| TNF-α | ↑ | n.r. | n.r. | [105] | |
| apoptosis | clusterin | ↑ | 0.76 | 0.63 | [105,137] |
n.r.—not reported; ↓—decrease; ↑—increase.
Table 3.
The major changes of the identified saliva biomarkers for AD and the associated mechanisms of pathology.
Table 3.
The major changes of the identified saliva biomarkers for AD and the associated mechanisms of pathology.
| Mechanism of AD Pathology | Saliva Biomarker | Change in AD Pathology | Sensitivity | Specificity | References |
|---|---|---|---|---|---|
| Aβ plaque deposition | Aβ42 | ↑ | 0.16 | 0.93 | [148,149,150,169] |
| Aβ40 | - | n.r. | n.r. | [148,149] | |
| acetylcholinesterase | ↓ | n.r. | n.r. | [139,148,151,170] | |
| tau pathology | T-tau | ↑ | n.r. | n.r. | [152,153,171] |
| P-tau | ↑ | n.r. | n.r. | [152,153] | |
| P-tau/T-tau | ↑ | 0.73–0.83 | 0.30–0.50 | [152,153] | |
| inflammation | lactoferrin | ↓ | 1 | 0.98 | [168] |
n.r.—not reported; ↓—decrease; ↑—increase.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Bălașa, A.F.; Chircov, C.; Grumezescu, A.M. Body Fluid Biomarkers for Alzheimer’s Disease—An Up-To-Date Overview. Biomedicines 2020, 8, 421. https://doi.org/10.3390/biomedicines8100421
AMA Style
Bălașa AF, Chircov C, Grumezescu AM. Body Fluid Biomarkers for Alzheimer’s Disease—An Up-To-Date Overview. Biomedicines. 2020; 8(10):421. https://doi.org/10.3390/biomedicines8100421
Chicago/Turabian StyleBălașa, Adrian Florian, Cristina Chircov, and Alexandru Mihai Grumezescu. 2020. "Body Fluid Biomarkers for Alzheimer’s Disease—An Up-To-Date Overview" Biomedicines 8, no. 10: 421. https://doi.org/10.3390/biomedicines8100421
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.