
Incretin Hormone Secretion in Women with Polycystic Ovary Syndrome: Roles of Obesity, Insulin Sensitivity and Treatment with Metformin and GLP-1s
 , ,
, ,  , , , ,
, , , , 
Abstract
:1. Introduction
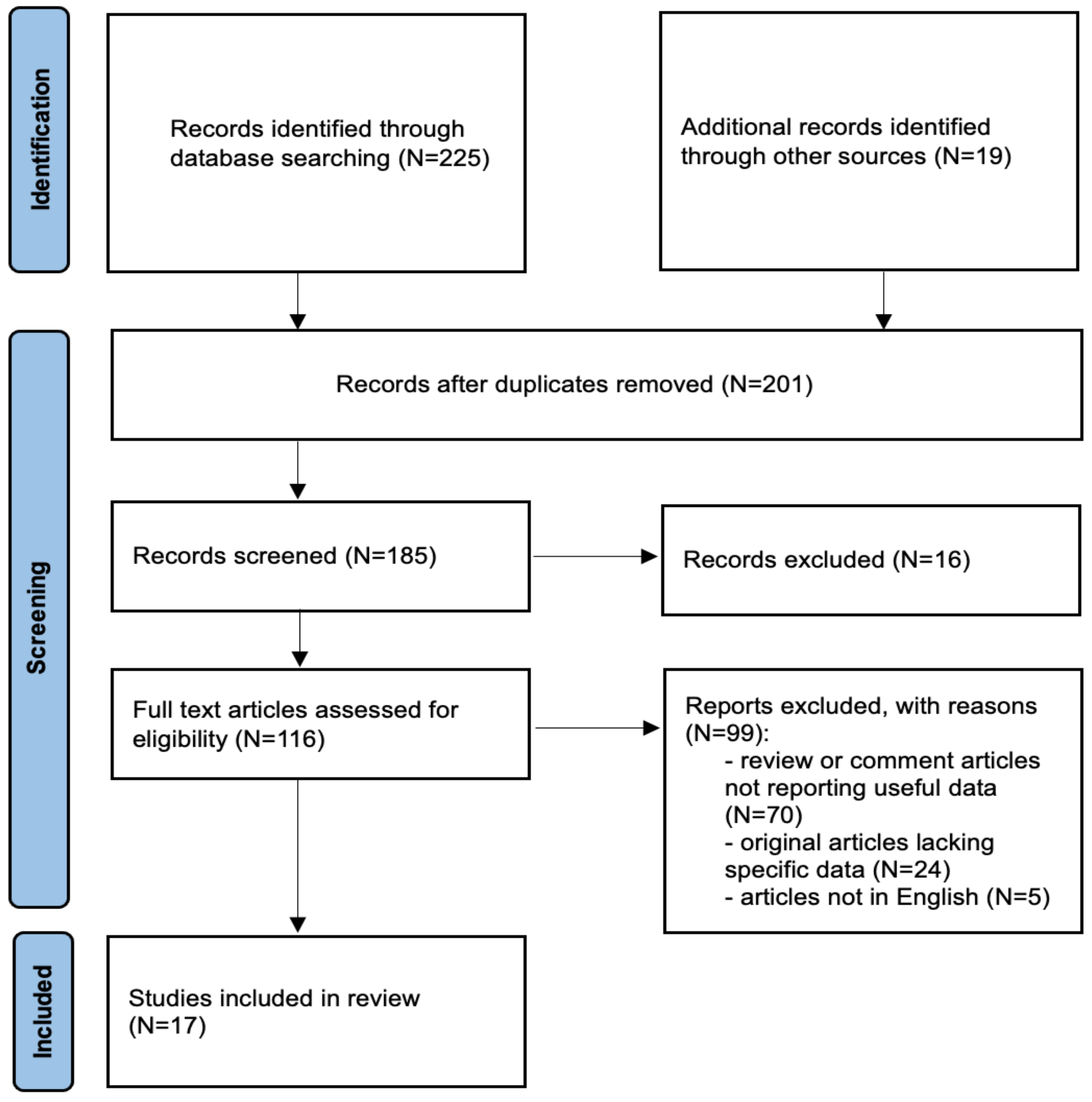
2. Materials and Methods
3. Results
3.1. PCOS: Definition and Current Pathophysiological Considerations
3.2. Metabolic and Fertility Consequences of PCOS
3.3. Specific Role of Obesity and Insulin Resistance in PCOS
3.4. Metformin: A Final Solution for All Patients with PCOS?
3.5. GLP-1 Receptor Agonists: Current Knowledge on Their Therapeutic Potential in PCOS
4. Discussion
Key Findings and Future Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Anekwe, C.V.; Jarrell, A.R.; Townsend, M.J.; Gaudier, G.I.; Hiserodt, J.M.; Stanford, F.C. Socioeconomics of Obesity. Curr. Obes. Rep. 2020, 9, 272–279. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide Trends in Body-Mass Index, Underweight, Overweight, and Obesity from 1975 to 2016: A Pooled Analysis of 2416 Population-Based Measurement Studies in 128.9 Million Children, Adolescents, and Adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [PubMed]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.-P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. Obesity and Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef] [PubMed]
- Chadt, A.; Scherneck, S.; Joost, H.-G.; Al-Hasani, H. Molecular Links between Obesity and Diabetes: “Diabesity”. In Endotext; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Dixon, A.E.; Peters, U. The Effect of Obesity on Lung Function. Expert. Rev. Respir. Med. 2018, 12, 755–767. [Google Scholar] [CrossRef] [PubMed]
- The Lancet Diabetes Endocrinology. The Obesity-Cancer Link: Of Increasing Concern. Lancet Diabetes Endocrinol. 2020, 8, 175. [Google Scholar] [CrossRef] [PubMed]
- Alsannan, B.; Laganà, A.S.; Alhermi, J.; Almansoor, S.; Ayed, A.; Venezia, R.; Etrusco, A. Prevalence of overactive bladder among overweight and obese women: A prospective cross-sectional cohort study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2024, 295, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Vurbic, D.; Harder, V.S.; Redner, R.R.; Lopez, A.A.; Phillips, J.K.; Higgins, S.T. Co-Occurring Obesity and Smoking among U.S. Women of Reproductive Age: Associations with Educational Attainment and Health Biomarkers and Outcomes. Prev. Med. 2015, 80, 60–66. [Google Scholar] [CrossRef]
- Crosbie, E.J.; Kitson, S.J.; McAlpine, J.N.; Mukhopadhyay, A.; Powell, M.E.; Singh, N. Endometrial Cancer. Lancet 2022, 399, 1412–1428. [Google Scholar] [CrossRef]
- Pomian, A.; Lisik, W.; Kosieradzki, M.; Barcz, E. Obesity and Pelvic Floor Disorders: A Review of the Literature. Med. Sci. Monit. 2016, 22, 1880–1886. [Google Scholar] [CrossRef]
- Ramlau-Hansen, C.H.; Thulstrup, A.M.; Nohr, E.A.; Bonde, J.P.; Sørensen, T.I.A.; Olsen, J. Subfecundity in Overweight and Obese Couples. Hum. Reprod. 2007, 22, 1634–1637. [Google Scholar] [CrossRef]
- Snider, A.P.; Wood, J.R. Obesity Induces Ovarian Inflammation and Reduces Oocyte Quality. Reproduction 2019, 158, R79–R90. [Google Scholar] [CrossRef]
- Bergant, G.; Abdulkhalikova, D.; Šuštaršič, A.; Peterlin, B.; Vrtačnik Bokal, E.; Maver, A.; Videmšek, M.; Burnik Papler, T. Expression of Markers of Endometrial Receptivity in Obese Infertile PCOS Women before and after the Weight Loss Program-A Preliminary Study. Cells 2022, 12, 164. [Google Scholar] [CrossRef] [PubMed]
- van der Steeg, J.W.; Steures, P.; Eijkemans, M.J.C.; Habbema, J.D.F.; Hompes, P.G.A.; Burggraaff, J.M.; Oosterhuis, G.J.E.; Bossuyt, P.M.M.; van der Veen, F.; Mol, B.W.J. Obesity Affects Spontaneous Pregnancy Chances in Subfertile, Ovulatory Women. Hum. Reprod. 2008, 23, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Practice Committee of the American Society for Reproductive Medicine. Obesity and Reproduction: A Committee Opinion. Fertil. Steril. 2021, 116, 1266–1285. [Google Scholar] [CrossRef]
- Zehravi, M.; Maqbool, M.; Ara, I. Polycystic Ovary Syndrome and Infertility: An Update. Int. J. Adolesc. Med. Health 2021, 34, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 Consensus on Diagnostic Criteria and Long-Term Health Risks Related to Polycystic Ovary Syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [Google Scholar] [CrossRef]
- Legro, R.S. Obesity and PCOS: Implications for Diagnosis and Treatment. Semin. Reprod. Med. 2012, 30, 496–506. [Google Scholar] [CrossRef]
- Legro, R.S.; Hansen, K.R.; Diamond, M.P.; Steiner, A.Z.; Coutifaris, C.; Cedars, M.I.; Hoeger, K.M.; Usadi, R.; Johnstone, E.B.; Haisenleder, D.J.; et al. Effects of Preconception Lifestyle Intervention in Infertile Women with Obesity: The FIT-PLESE Randomized Controlled Trial. PLoS Med. 2022, 19, e1003883. [Google Scholar] [CrossRef]
- Han, Y.; Li, Y.; He, B. GLP-1 Receptor Agonists versus Metformin in PCOS: A Systematic Review and Meta-Analysis. Reprod. Biomed. Online 2019, 39, 332–342. [Google Scholar] [CrossRef]
- Teede, H.J.; Tay, C.T.; Laven, J.; Dokras, A.; Moran, L.J.; Piltonen, T.T.; Costello, M.F.; Boivin, J.; Redman, L.M.; Boyle, J.A.; et al. Recommendations from the 2023 International Evidence-Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome†. Hum. Reprod. 2023, 38, 1655–1679. [Google Scholar] [CrossRef]
- Tak, Y.J.; Lee, S.Y. Anti-Obesity Drugs: Long-Term Efficacy and Safety: An Updated Review. World J. Men’s Health 2021, 39, 208–221. [Google Scholar] [CrossRef] [PubMed]
- Benham, J.L.; Goldberg, A.; Teede, H.; Tay, C.T. Polycystic Ovary Syndrome: Associations with Cardiovascular Disease. Climacteric 2023, 27, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, B.O.; Knochenhauer, E.S.; Azziz, R. Impact of Obesity on the Risk for Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2008, 93, 162–168. [Google Scholar] [CrossRef]
- Legro, R.S. Diabetes Prevalence and Risk Factors in Polycystic Ovary Syndrome. Obstet. Gynecol. Clin. N. Am. 2001, 28, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Pinborg, A.; Gaarslev, C.; Hougaard, C.O.; Nyboe Andersen, A.; Andersen, P.K.; Boivin, J.; Schmidt, L. Influence of Female Bodyweight on IVF Outcome: A Longitudinal Multicentre Cohort Study of 487 Infertile Couples. Reprod. Biomed. Online 2011, 23, 490–499. [Google Scholar] [CrossRef]
- Maheshwari, A.; Stofberg, L.; Bhattacharya, S. Effect of Overweight and Obesity on Assisted Reproductive Technology—A Systematic Review. Hum. Reprod. Update 2007, 13, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Dunaif, A.; Segal, K.R.; Shelley, D.R.; Green, G.; Dobrjansky, A.; Licholai, T. Evidence for Distinctive and Intrinsic Defects in Insulin Action in Polycystic Ovary Syndrome. Diabetes 1992, 41, 1257–1266. [Google Scholar] [CrossRef]
- Diamanti-Kandarakis, E.; Dunaif, A. Insulin Resistance and the Polycystic Ovary Syndrome Revisited: An Update on Mechanisms and Implications. Endocr. Rev. 2012, 33, 981–1030. [Google Scholar] [CrossRef]
- Apridonidze, T.; Essah, P.A.; Iuorno, M.J.; Nestler, J.E. Prevalence and Characteristics of the Metabolic Syndrome in Women with Polycystic Ovary Syndrome. J. Clin. Endocrinol. Metab. 2005, 90, 1929–1935. [Google Scholar] [CrossRef]
- Nestler, J.E.; Jakubowicz, D.J.; de Vargas, A.F.; Brik, C.; Quintero, N.; Medina, F. Insulin Stimulates Testosterone Biosynthesis by Human Thecal Cells from Women with Polycystic Ovary Syndrome by Activating Its Own Receptor and Using Inositolglycan Mediators as the Signal Transduction System. J. Clin. Endocrinol. Metab. 1998, 83, 2001–2005. [Google Scholar] [CrossRef]
- Munir, I.; Yen, H.-W.; Geller, D.H.; Torbati, D.; Bierden, R.M.; Weitsman, S.R.; Agarwal, S.K.; Magoffin, D.A. Insulin Augmentation of 17α-Hydroxylase Activity Is Mediated by Phosphatidyl Inositol 3-Kinase But Not Extracellular Signal-Regulated Kinase-1/2 in Human Ovarian Theca Cells. Endocrinology 2004, 145, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.-K.; Sallinen, K.; Anttila, L.; Mä, M.; Luo, C.; Pö, P.; Nen, L.; Erkkola, R. Expression of Insulin-Receptor Substrate-1 and-2 in Ovaries from Women with Insulin Resistance and from Controls. Fertil. Steril. 2000, 74, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Sekar, N.; Garmey, J.C.; Veldhuis, J.D. Mechanisms Underlying the Steroidogenic Synergy of Insulin and Luteinizing Hormone in Porcine Granulosa Cells: Joint Amplification of Pivotal Sterol-Regulatory Genes Encoding the Low-Density Lipoprotein (LDL) Receptor, Steroidogenic Acute Regulatory (stAR) Protein and Cytochrome P450 Side-Chain Cleavage (P450scc) Enzyme. Mol. Cell. Endocrinol. 2000, 159, 25–35. [Google Scholar] [CrossRef] [PubMed]
- Willis, D.; Mason, H.; Gilling-Smith, C.; Franks, S. Modulation by Insulin of Follicle-Stimulating Hormone and Luteinizing Hormone Actions in Human Granulosa Cells of Normal and Polycystic Ovaries. J. Clin. Endocrinol. Metab. 1996, 81, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Rice, S.; Christoforidis, N.; Gadd, C.; Nikolaou, D.; Seyani, L.; Donaldson, A.; Margara, R.; Hardy, K.; Franks, S. Impaired Insulin-Dependent Glucose Metabolism in Granulosa-Lutein Cells from Anovulatory Women with Polycystic Ovaries. Hum. Reprod. 2005, 20, 373–381. [Google Scholar] [CrossRef] [PubMed]
- Curat, C.A.; Wegner, V.; Sengenès, C.; Miranville, A.; Tonus, C.; Busse, R.; Bouloumié, A. Macrophages in Human Visceral Adipose Tissue: Increased Accumulation in Obesity and a Source of Resistin and Visfatin. Diabetologia 2006, 49, 744–747. [Google Scholar] [CrossRef] [PubMed]
- Weisberg, S.P.; McCann, D.; Desai, M.; Rosenbaum, M.; Leibel, R.L.; Ferrante, A.W. Obesity Is Associated with Macrophage Accumulation in Adipose Tissue. J. Clin. Investig. 2003, 112, 1796–1808. [Google Scholar] [CrossRef]
- Lumeng, C.N.; Deyoung, S.M.; Saltiel, A.R. Macrophages Block Insulin Action in Adipocytes by Altering Expression of Signaling and Glucose Transport Proteins. Am. J. Physiol. Endocrinol. Metab. 2007, 292, E166–E174. [Google Scholar] [CrossRef]
- Ardawi, M.S.M.; Rouzi, A.A. Plasma Adiponectin and Insulin Resistance in Women with Polycystic Ovary Syndrome. Fertil. Steril. 2005, 83, 1708–1716. [Google Scholar] [CrossRef]
- Komorowski, A.S.; Hughes, L.; Sarkar, P.; Aaby, D.A.; Kumar, A.; Kalra, B.; Legro, R.S.; Boots, C.E. Anti-müllerian hormone level predicts ovulation in women with polycystic ovary syndrome treated with clomiphene and metformin. Fertil. Steril. 2023. [Google Scholar] [CrossRef]
- Pea, J.; Bryan, J.; Wan, C.; Oldfield, A.L.; Ganga, K.; Carter, F.E.; Johnson, L.M.; Lujan, M.E. Ultrasonographic criteria in the diagnosis of polycystic ovary syndrome: A systematic review and diagnostic meta-analysis. Hum. Reprod. Update 2023, 30, 109–130. [Google Scholar] [CrossRef] [PubMed]
- Escobar-Morreale, H.F.; Villuendas, G.; Botella-Carretero, J.I.; Alvarez-Blasco, F.; Sanchón, R.; Luque-Ramírez, M.; San Millán, J.L. Adiponectin and Resistin in PCOS: A Clinical, Biochemical and Molecular Genetic Study. Hum. Reprod. 2006, 21, 2257–2265. [Google Scholar] [CrossRef] [PubMed]
- Diamanti-Kandarakis, E.; Katsikis, I.; Piperi, C.; Kandaraki, E.; Piouka, A.; Papavassiliou, A.G.; Panidis, D. Increased Serum Advanced Glycation End-Products Is a Distinct Finding in Lean Women with Polycystic Ovary Syndrome (PCOS). Clin. Endocrinol. 2008, 69, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; Zhou, M.; Zhou, G.; Zhu, Q.; Li, W. Effect of Metformin on Adiponectin in PCOS: A Meta-Analysis and a Systematic Review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 267, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Etrusco, A.; Laganà, A.S.; Chiantera, V.; Buzzaccarini, G.; Unfer, V. Myo-Inositol in Assisted Reproductive Technology from Bench to Bedside. Trends Endocrinol. Metab. 2023, 35, 74–83. [Google Scholar] [CrossRef]
- Moreira-Pinto, B.; Costa, L.; Felgueira, E.; Fonseca, B.M.; Rebelo, I. Low Doses of Resveratrol Protect Human Granulosa Cells from Induced-Oxidative Stress. Antioxidants 2021, 10, 561. [Google Scholar] [CrossRef]
- Sanchez-Garrido, M.A.; Tena-Sempere, M. Metabolic Dysfunction in Polycystic Ovary Syndrome: Pathogenic Role of Androgen Excess and Potential Therapeutic Strategies. Mol. Metab. 2020, 35, 100937. [Google Scholar] [CrossRef]
- Rosenfield, R.L.; Ehrmann, D.A. The Pathogenesis of Polycystic Ovary Syndrome (PCOS): The Hypothesis of PCOS as Functional Ovarian Hyperandrogenism Revisited. Endocr. Rev. 2016, 37, 467–520. [Google Scholar] [CrossRef]
- Kim, J.J.; Choi, Y.M. Dyslipidemia in Women with Polycystic Ovary Syndrome. Obstet. Gynecol. Sci. 2013, 56, 137–142. [Google Scholar] [CrossRef]
- Vitale, S.G.; Fulghesu, A.M.; Mikuš, M.; Watrowski, R.; D’Alterio, M.N.; Lin, L.-T.; Shah, M.; Reyes-Muñoz, E.; Sathyapalan, T.; Angioni, S. The Translational Role of miRNA in Polycystic Ovary Syndrome: From Bench to Bedside—A Systematic Literature Review. Biomedicines 2022, 10, 1816. [Google Scholar] [CrossRef]
- Geng, X.; Zhao, J.; Huang, J.; Li, S.; Chu, W.; Wang, W.-S.; Chen, Z.-J.; Du, Y. Lnc-MAP3K13-7:1 Inhibits Ovarian GC Proliferation in PCOS via DNMT1 Downregulation-Mediated CDKN1A Promoter Hypomethylation. Mol. Ther. 2021, 29, 1279–1293. [Google Scholar] [CrossRef] [PubMed]
- Barber, T.M.; Hanson, P.; Weickert, M.O.; Franks, S. Obesity and Polycystic Ovary Syndrome: Implications for Pathogenesis and Novel Management Strategies. Clin. Med. Insights Reprod. Health 2019, 13, 1179558119874042. [Google Scholar] [CrossRef]
- Hoeger, K.M.; Dokras, A.; Piltonen, T. Update on PCOS: Consequences, Challenges, and Guiding Treatment. J. Clin. Endocrinol. Metab. 2021, 106, e1071–e1083. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, A.E.; Udesen, P.B.; Maciag, G.; Geiger, J.; Saliani, N.; Januszewski, A.S.; Jiang, G.; Ma, R.C.; Hardikar, A.A.; Wissing, M.L.M.; et al. Hyperandrogenism and Metabolic Syndrome Are Associated with Changes in Serum-Derived microRNAs in Women with Polycystic Ovary Syndrome. Front. Med. 2019, 6, 242. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Qiao, J. Association of Insulin Resistance and Elevated Androgen Levels with Polycystic Ovarian Syndrome (PCOS): A Review of Literature. J. Healthc. Eng. 2022, 2022, 9240569. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.; Deeks, A.; Moran, L. Polycystic ovary syndrome: A complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010, 8, 41. [Google Scholar] [CrossRef] [PubMed]
- Baskind, N.E.; Balen, A.H. Hypothalamic–pituitary, ovarian and adrenal contributions to polycystic ovary syndrome. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 37, 80–97. [Google Scholar] [CrossRef]
- Moore, A.M.; Campbell, R.E. Polycystic ovary syndrome: Understanding the role of the brain. Front. Neuroendocr. 2017, 46, 1–14. [Google Scholar] [CrossRef]
- Zuo, T.; Zhu, M.; Xu, W. Roles of Oxidative Stress in Polycystic Ovary Syndrome and Cancers. Oxidative Med. Cell. Longev. 2016, 2016, 8589318. [Google Scholar] [CrossRef]
- Hernández-Jiménez, J.L.; Barrera, D.; Espinoza-Simón, E.; González, J.; Ortíz-Hernández, R.; Escobar, L.; Echeverría, O.; Torres-Ramírez, N. Polycystic ovarian syndrome: Signs and feedback effects of hyperandrogenism and insulin resistance. Gynecol. Endocrinol. 2022, 38, 2–9. [Google Scholar] [CrossRef]
- Stepto, N.; Cassar, S.; Joham, A.E.; Hutchison, S.K.; Harrison, C.L.; Goldstein, R.F.; Teede, H.J. Women with polycystic ovary syndrome have intrinsic insulin resistance on euglycaemic-hyperinsulaemic clamp. Hum. Reprod. 2013, 28, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.S.; Giacobini, P. New insights into anti-Müllerian hormone role in the hypothalamic–pituitary–gonadal axis and neuroendocrine development. Cell. Mol. Life Sci. 2021, 78, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Dewailly, D.; Robin, G.; Peigne, M.; Decanter, C.; Pigny, P.; Catteau-Jonard, S. Interactions between androgens, FSH, anti-Müllerian hormone and estradiol during folliculogenesis in the human normal and polycystic ovary. Hum. Reprod. Update 2016, 22, 709–724. [Google Scholar] [CrossRef] [PubMed]
- Jiang, N.-X.; Zhao, W.-J.; Shen, H.-R.; Du, D.; Li, X.-L. Hyperinsulinemia impairs decidualization via Akt-NR4A1 signaling: New insight into polycystic ovary syndrome (pcos)-related infertility. J. Ovarian Res. 2024, 17, 31. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Peng, C.; Cao, G.; Li, W.; Hou, L. Tai chi for overweight/obese adolescent and young women with polycystic ovary syndrome: Study protocol for a randomized controlled trial. Trials 2018, 19, 512. [Google Scholar] [CrossRef] [PubMed]
- Madusudhanan, R.R.; Nambisan, B.; Brahmanandan, M.; Radha, S. Study on the Prevalence and Characteristics of Metabolic Syndrome in Women of Reproductive Age Group with Polycystic Ovarian Syndrome. J. South Asian Fed. Obstet. Gynaecol. 2016, 9, 341–347. [Google Scholar] [CrossRef]
- Ng, N.Y.H.; Jiang, G.; Cheung, L.P.; Zhang, Y.; Tam, C.H.T.; Luk, A.O.Y.; Quan, J.; Lau, E.S.H.; Yau, T.T.L.; Chan, M.H.M.; et al. Progression of glucose intolerance and cardiometabolic risk factors over a decade in Chinese women with polycystic ovary syndrome: A case-control study. PLoS Med. 2019, 16, e1002953. [Google Scholar] [CrossRef]
- Amato, M.C.; Vesco, R.; Vigneri, E.; Ciresi, A.; Giordano, C. Hyperinsulinism and polycystic ovary syndrome (PCOS): Role of insulin clearance. J. Endocrinol. Investig. 2015, 38, 1319–1326. [Google Scholar] [CrossRef]
- Costello, M.F.; Misso, M.L.; Balen, A.; Boyle, J.; Devoto, L.; Garad, R.M.; Hart, R.; Johnson, L.; Jordan, C.; Legro, R.S.; et al. A brief update on the evidence supporting the treatment of infertility in polycystic ovary syndrome. Aust. N. Z. J. Obstet. Gynaecol. 2019, 59, 867–873. [Google Scholar] [CrossRef]
- Huddleston, H.G.; Dokras, A. Diagnosis and treatment of polycystic ovary syndrome. JAMA 2022, 327, 274–275. [Google Scholar] [CrossRef]
- Carmina, E.; Lobo, R.A. Comparing lean and obese PCOS in different PCOS phenotypes: Evidence that the body weight is more important than the rotterdam phenotype in influencing the metabolic status. Diagnostics 2022, 12, 2313. [Google Scholar] [CrossRef] [PubMed]
- Cioana, M.; Deng, J.; Nadarajah, A.; Hou, M.; Qiu, Y.; Chen, S.S.; Rivas, A.; Banfield, L.; Alfaraidi, H.; Alotaibi, A.; et al. Prevalence of polycystic ovary syndrome in patients with pediatric type 2 diabetes: A systematic review and meta-analysis. JAMA Netw. Open 2022, 5, e2147454. [Google Scholar] [CrossRef] [PubMed]
- Nikolettos, K.; Nikolettos, N.; Vlahos, N.; Pagonopoulou, O.; Asimakopoulos, B. Role of leptin, adiponectin, and kisspeptin in polycystic ovarian syndrome pathogenesis. Minerva Obstet. Gynecol. 2022, 75, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Nautiyal, H.; Imam, S.S.; Alshehri, S.; Ghoneim, M.M.; Afzal, M.; Alzarea, S.I.; Güven, E.; Al-Abbasi, F.A.; Kazmi, I. Polycystic Ovarian Syndrome: A Complex Disease with a Genetics Approach. Biomedicines 2022, 10, 540. [Google Scholar] [CrossRef] [PubMed]
- Boshku, A.A.; Panova, D.I.; Ivanovska, B.Z. Adiponectin as a serum marker of adipose tissue dysfunction in women with polycystic ovary syndrome: Correlation with indicators of metabolic disturbances. Acta Endocrinol. 2018, 14, 346–352. [Google Scholar]
- Shirazi, F.K.H.; Khodamoradi, Z.; Jeddi, M. Insulin resistance and high molecular weight adiponectin in obese and non-obese patients with Polycystic Ovarian Syndrome (PCOS). BMC Endocr. Disord. 2021, 21, 45. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Xie, Y.-J.; Liu, Y.-T.; Long, S.-L.; Mo, Z.-C. Polycystic ovarian syndrome: Correlation between hyperandrogenism, insulin resistance and obesity. Clin. Chim. Acta 2020, 502, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Cassar, S.; Misso, M.L.; Hopkins, W.G.; Shaw, C.S.; Teede, H.; Stepto, N.K. Insulin resistance in polycystic ovary syndrome: A systematic review and meta-analysis of euglycaemic–hyperinsulinaemic clamp studies. Hum. Reprod. 2016, 31, 2619–2631. [Google Scholar] [CrossRef]
- Di Segni, C.; Silvestrini, A.; Fato, R.; Bergamini, C.; Guidi, F.; Raimondo, S.; Meucci, E.; Romualdi, D.; Apa, R.; Lanzone, A.; et al. Plasmatic and Intracellular Markers of Oxidative Stress in Normal Weight and Obese Patients with Polycystic Ovary Syndrome. Exp. Clin. Endocrinol. Diabetes 2017, 125, 506–513. [Google Scholar] [CrossRef]
- Özer, A.; Bakacak, M.; Kiran, H.; Ercan, O.; Kostu, B.; Pektas, M.K.; Kilinç, M.; Aslan, F. Increased oxidative stress is associated with insulin resistance and infertility in polycystic ovary syndrome. Ginekol. Pol. 2016, 87, 733–738. [Google Scholar] [CrossRef]
- Delitala, A.; Capobianco, G.; Delitala, G.; Cherchi, P.L.; Dessole, S. Polycystic ovary syndrome, adipose tissue and metabolic syndrome. Arch. Gynecol. Obstet. 2017, 296, 405–419. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zheng, Y.; Guo, Y.; Lai, Z. The Effect of Low Carbohydrate Diet on Polycystic Ovary Syndrome: A Meta-Analysis of Randomized Controlled Trials. Int. J. Endocrinol. 2019, 2019, 4386401. [Google Scholar] [CrossRef] [PubMed]
- Jia, L.-Y.; Feng, J.-X.; Li, J.-L.; Liu, F.-Y.; Xie, L.-Z.; Luo, S.-J.; Han, F.-J. The Complementary and Alternative Medicine for Polycystic Ovary Syndrome: A Review of Clinical Application and Mechanism. Evid.-Based Complement. Altern. Med. 2021, 2021, 5555315. [Google Scholar] [CrossRef] [PubMed]
- Shirvani-Rad, S.; Tabatabaei-Malazy, O.; Mohseni, S.; Hasani-Ranjbar, S.; Soroush, A.-R.; Hoseini-Tavassol, Z.; Ejtahed, H.-S.; Larijani, B. Probiotics as a Complementary Therapy for Management of Obesity: A Systematic Review. Evid.-Based Complement. Altern. Med. 2021, 2021, 6688450. [Google Scholar] [CrossRef]
- Ortega, I.; A Villanueva, J.; Wong, D.H.; Cress, A.B.; Sokalska, A.; Stanley, S.D.; Duleba, A.J. Resveratrol potentiates effects of simvastatin on inhibition of rat ovarian theca-interstitial cells steroidogenesis. J. Ovarian Res. 2014, 7, 21. [Google Scholar] [CrossRef] [PubMed]
- Crandall, J.P.; Oram, V.; Trandafirescu, G.; Reid, M.; Kishore, P.; Hawkins, M.; Cohen, H.W.; Barzilai, N. Pilot Study of Resveratrol in Older Adults with Impaired Glucose Tolerance. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2012, 67, 1307–1312. [Google Scholar] [CrossRef] [PubMed]
- Salvatore, T.; Pafundi, P.C.; Morgillo, F.; Di Liello, R.; Galiero, R.; Nevola, R.; Marfella, R.; Monaco, L.; Rinaldi, L.; Adinolfi, L.E.; et al. Metformin: An Old Drug against Old Age and Associated Morbidities. Diabetes Res. Clin. Pract. 2020, 160, 108025. [Google Scholar] [CrossRef]
- Bugianesi, E.; Gentilcore, E.; Manini, R.; Natale, S.; Vanni, E.; Villanova, N.; David, E.; Rizzetto, M.; Marchesini, G. A Randomized Controlled Trial of Metformin versus Vitamin E or Prescriptive Diet in Nonalcoholic Fatty Liver Disease. Am. J. Gastroenterol. 2005, 100, 1082–1090. [Google Scholar] [CrossRef]
- Zhou, J.; Massey, S.; Story, D.; Li, L. Metformin: An Old Drug with New Applications. Int. J. Mol. Sci. 2018, 19, 2863. [Google Scholar] [CrossRef]
- Luo, T.; Nocon, A.; Fry, J.; Sherban, A.; Rui, X.; Jiang, B.; Xu, X.J.; Han, J.; Yan, Y.; Yang, Q.; et al. AMPK Activation by Metformin Suppresses Abnormal Extracellular Matrix Remodeling in Adipose Tissue and Ameliorates Insulin Resistance in Obesity. Diabetes 2016, 65, 2295–2310. [Google Scholar] [CrossRef]
- Preiss, D.; Sattar, N.; Harborne, L.; Norman, J.; Fleming, R. The Effects of 8 Months of Metformin on Circulating GGT and ALT Levels in Obese Women with Polycystic Ovarian Syndrome. Int. J. Clin. Pract. 2008, 62, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Tu, M.; Huang, Y.; Liu, Y.; Zhang, D. Association of Metformin with Pregnancy Outcomes in Women with Polycystic Ovarian Syndrome Undergoing In Vitro Fertilization: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2020, 3, e2011995. [Google Scholar] [CrossRef] [PubMed]
- Lagana, A.S.; Barbaro, L.; Pizzo, A. Evaluation of ovarian function and metabolic factors in women affected by polycystic ovary syndrome after treatment with D-Chiro-Inositol. Arch. Gynecol. Obstet. 2015, 291, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Tao, T.; Zhang, Y.; Zhu, Y.C.; Fu, J.R.; Wang, Y.Y.; Cai, J.; Ma, J.Y.; Xu, Y.; Gao, Y.N.; Sun, Y.; et al. Exenatide, Metformin, or Both for Prediabetes in PCOS: A Randomized, Open-Label, Parallel-Group Controlled Study. J. Clin. Endocrinol. Metab. 2021, 106, e1420–e1432. [Google Scholar] [CrossRef] [PubMed]
- Oppelt, P.G.; Mueller, A.; Jentsch, K.; Kronawitter, D.; Reissmann, C.; Dittrich, R.; Beckmann, M.W.; Cupisti, S. The effect of metformin treatment for 2 years without caloric restriction on endocrine and metabolic parameters in women with polycystic ovary syndrome. Exp. Clin. Endocrinol. Diabetes 2010, 118, 633–637. [Google Scholar] [CrossRef] [PubMed]
- Glueck, C.J.; Pranikoff, J.; Aregawi, D.; Wang, P. Prevention of gestational diabetes by metformin plus diet in patients with polycystic ovary syndrome. Fertil. Steril. 2008, 89, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Cui, P.; Jiang, H.Y.; Guo, Y.R.; Pishdari, B.; Hu, M.; Feng, Y.; Billig, H.; Shao, R. Reversing the reduced level of endometrial GLUT4 expression in polycystic ovary syndrome: A mechanistic study of metformin action. Am. J. Transl. Res. 2015, 7, 574–586. [Google Scholar]
- Liu, J.; Zhao, Y.; Chen, L.; Li, R.; Ning, Y.; Zhu, X. Role of metformin in functional endometrial hyperplasia and polycystic ovary syndrome involves the regulation of MEG3/miR223/GLUT4 and SNHG20/miR4486/GLUT4 signaling. Mol. Med. Rep. 2022, 26, 218. [Google Scholar] [CrossRef]
- Frías, J.P.; Guja, C.; Hardy, E.; Ahmed, A.; Dong, F.; Öhman, P.; Jabbour, S.J. Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with type 2 diabetes inadequately controlled with metformin monotherapy (DURATION-8): A 28 week, multicentre, double-blind, phase 3, randomised control. Lancet Diabetes Endocrinol. 2016, 4, 1004–1016. [Google Scholar] [CrossRef]
- Feng, L.; Lin, X.F.; Wan, Z.H.; Hu, D.; Du, Y.K. Efficacy of metformin on pregnancy complications in women with polycystic ovary syndrome: A meta-analysis. Gynecol. Endocrinol. 2015, 31, 833–839. [Google Scholar] [CrossRef]
- Szczesnowicz, A.; Szeliga, A.; Niwczyk, O.; Bala, G.; Meczekalski, B. Do GLP-1 Analogs Have a Place in the Treatment of PCOS? New Insights and Promising Therapies. J. Clin. Med. 2023, 12, 5915. [Google Scholar] [CrossRef] [PubMed]
- Rubino, D.M.; Greenway, F.L.; Khalid, U.; O’Neil, P.M.; Rosenstock, J.; Sørrig, R.; Wadden, T.A.; Wizert, A.; Garvey, W.T.; STEP 8 Investigators. Effect of Weekly Subcutaneous Semaglutide vs. Daily Liraglutide on Body Weight in Adults with Overweight or Obesity without Diabetes: The STEP 8 Randomized Clinical Trial. JAMA 2022, 327, 138–150. [Google Scholar] [CrossRef] [PubMed]
- Jensterle, M.; Goricar, K.; Janez, A. Metformin as an initial adjunct to low-dose liraglutide enhances the weight-decreasing potential of liraglutide in obese polycystic ovary syndrome: Randomized control study. Exp. Ther. Med. 2016, 11, 1194–1200. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, G.; de Alteriis, G.; Muscogiuri, G.; Barrea, L.; Verde, L.; Zumbolo, F.; Colao, A.; Savastano, S. Liraglutide and polycystic ovary syndrome: Is it only a matter of body weight? J. Endocrinol. Investig. 2023, 46, 1761–1774. [Google Scholar] [CrossRef] [PubMed]
- Frøssing, S.; Nylander, M.; Kistorp, C.; Skouby, S.O.; Faber, J. Effect of liraglutide on atrial natriuretic peptide, adrenomedullin, and copeptin in PCOS. Endocr. Connect. 2018, 7, 115–123. [Google Scholar] [CrossRef]
- Salamun, V.; Jensterle, M.; Janez, A.; Vrtacnik Bokal, E. Liraglutide increases IVF pregnancy rates in obese PCOS women with poor response to first-line reproductive treatments: A pilot randomized study. Eur. J. Endocrinol. 2018, 179, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zhang, Y.; Zheng, S.Y.; Lin, R.; Xie, Y.J.; Chen, H.; Zheng, Y.; Liu, E.; Chen, L.; Yan, J.; et al. Efficacy of exenatide on weight loss, metabolic parameters and pregnancy in overweight/obese polycystic ovary syndrome. Clin. Endocrinol. 2017, 87, 767–774. [Google Scholar] [CrossRef]
- Lyu, X.; Lyu, T.; Wang, X.; Zhu, H.; Pan, H.; Wang, L.; Yang, H.; Gong, F. The antiobesity effect of GLP-1 receptor agonists alone or in combination with metformin in overweight /obese women with polycystic ovary syndrome: A systematic review and meta-analysis. Int. J. Endocrinol. 2021, 2021, 6616693. [Google Scholar] [CrossRef]
- Lee, J.; Hong, S.-W.; Kim, M.-J.; Moon, S.J.; Kwon, H.; Park, S.E.; Rhee, E.-J.; Lee, W.-Y. Glucagon-like peptide receptor agonist inhibits angiotensin II-induced proliferation and migration in vascular smooth muscle cells and ameliorates phosphate-induced vascular smooth muscle cells calcification. Diabetes Metab. J. 2024, 48, 83–96. [Google Scholar] [CrossRef]
- Wong, C.K.; McLean, B.A.; Baggio, L.L.; Koehler, J.A.; Hammoud, R.; Rittig, N.; Yabut, J.M.; Seeley, R.J.; Brown, T.J.; Drucker, D.J. Central glucagon-like peptide 1 receptor activation inhibits toll-like receptor agonist-induced inflammation. Cell Metab. 2024, 36, 130–143.e5. [Google Scholar] [CrossRef]
- Zhang, Y.; Lin, Y.; Li, G.; Yuan, Y.; Wang, X.; Li, N.; Xiong, C.; Yang, Y.; Ma, Y.; Zhang, Z.; et al. Glucagon-like peptide-1 receptor agonists decrease hyperinsulinemia and hyperandrogenemia in dehydroepiandrosterone-induced polycystic ovary syndrome mice and are associated with mitigating inflammation and inducing browning of white adipose tissue. Biol. Reprod. 2023, 108, 945–959. [Google Scholar] [CrossRef]
- Jensterle, M.; Ferjan, S.; Ležaič, L.; Sočan, A.; Goričar, K.; Zaletel, K.; Janez, A. Semaglutide delays 4-hour gastric emptying in women with polycystic ovary syndrome and obesity. Diabetes Obes. Metab. 2023, 25, 975–984. [Google Scholar] [CrossRef]
- Jensterle, M.; Ferjan, S.; Vovk, A.; Battelino, T.; Rizzo, M.; Janež, A. SEMAGLUTIDE reduces fat accumulation in the tongue: A randomized single-blind, pilot study. Diabetes Res. Clin. Pract. 2021, 178, 108935. [Google Scholar] [CrossRef]
- Li, R.; Mai, T.; Zheng, S.; Zhang, Y. Effect of metformin and exenatide on pregnancy rate and pregnancy outcomes in overweight or obese infertility PCOS women: Long-term follow-up of an RCT. Arch. Gynecol. Obstet. 2022, 306, 1711–1721. [Google Scholar] [CrossRef]


{kind=link}
| Phenotypes | Hyperandrogenism | Ovulatory Dysfunction | Polycystic Ovarian Morphology |
|---|---|---|---|
| A | + | + | + |
| B | + | + | - |
| C | + | - | + |
| D | - | + | + |
| Factor | Abnormality in PCOS | Result |
|---|---|---|
| FSH | Decreased secretion → relative deficiency | Inadequate follicular stimulation |
| LH | Hypersecretion | Hyperandrogenemia, follicle growth interruption |
| Insulin | Hypersecretion → decreased glucose tolerance → insulin resistance | Hyperandrogenemia, follicle growth interruption |
| Androgens | Hypersecretion | Abnormal gonadotropin secretion, follicle growth interruption |
| Estrogens | Hypersecretion | Suppression of FSH secretion, increased LH secretion |
| Inhibin B | Hypersecretion | Suppression of FSH secretion |
| Apoptosis | Reduced | Increased number of small follicles included in steroidogenesis |
| Growth factors | Abnormal expression | Abnormal apoptosis (EGF/TGF-α), follicle growth interruption (TGF-β), increase secretion of granulosa lutein cells (VEGF), suppression of estrogen synthesis (IGF-1), excessive androgen production (IGFBP-1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Etrusco, A.; Mikuš, M.; D’Amato, A.; Barra, F.; Planinić, P.; Goluža, T.; Buzzaccarini, G.; Marušić, J.; Tešanović, M.; Laganà, A.S. Incretin Hormone Secretion in Women with Polycystic Ovary Syndrome: Roles of Obesity, Insulin Sensitivity and Treatment with Metformin and GLP-1s. Biomedicines 2024, 12, 653. https://doi.org/10.3390/biomedicines12030653
Etrusco A, Mikuš M, D’Amato A, Barra F, Planinić P, Goluža T, Buzzaccarini G, Marušić J, Tešanović M, Laganà AS. Incretin Hormone Secretion in Women with Polycystic Ovary Syndrome: Roles of Obesity, Insulin Sensitivity and Treatment with Metformin and GLP-1s. Biomedicines. 2024; 12(3):653. https://doi.org/10.3390/biomedicines12030653
Chicago/Turabian StyleEtrusco, Andrea, Mislav Mikuš, Antonio D’Amato, Fabio Barra, Petar Planinić, Trpimir Goluža, Giovanni Buzzaccarini, Jelena Marušić, Mara Tešanović, and Antonio Simone Laganà. 2024. "Incretin Hormone Secretion in Women with Polycystic Ovary Syndrome: Roles of Obesity, Insulin Sensitivity and Treatment with Metformin and GLP-1s" Biomedicines 12, no. 3: 653. https://doi.org/10.3390/biomedicines12030653