

Corneal Sub-Basal Nerve Plexus Regeneration Pattern following Implantable Collamer Lens Implantation for Myopia: A Prospective Longitudinal In Vivo Confocal Microscopy Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Patients
2.2. Study Protocol
2.3. Confocal Microscopy and Image Analysis
2.4. Surgical Methodology
2.5. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sandoval, H.P.; Donnenfeld, E.D.; Kohnen, T.; Lindstrom, R.L.; Potvin, R.; Tremblay, D.M.; Solomon, K.D. Modern laser in situ keratomileusis outcomes. J. Cataract. Refract. Surg. 2016, 42, 1224–1234. [Google Scholar] [CrossRef]
- Chen, X.; Wang, X.; Xu, Y.; Cheng, M.; Han, T.; Niu, L.; Wang, X.; Zhou, X. Five-year outcomes of EVO implantable collamer lens implantation for the correction of high myopia and super high myopia. Eye Vis. 2021, 8, 40. [Google Scholar] [CrossRef]
- Toda, I. Dry Eye After LASIK. Investig. Ophthalmol. Vis. Sci. 2018, 59, DES109–DES115. [Google Scholar] [CrossRef]
- Tamimi, A.; Sheikhzadeh, F.; Ezabadi, S.G.; Islampanah, M.; Parhiz, P.; Fathabadi, A.; Poudineh, M.; Khanjani, Z.; Pourmontaseri, H.; Orandi, S.; et al. Post-LASIK dry eye disease: A comprehensive review of management and current treatment options. Front. Med. 2023, 10, 1057685. [Google Scholar] [CrossRef] [PubMed]
- Solomon, R.; Donnenfeld, E.D.; Perry, H.D. The effects of LASIK on the ocular surface. Ocul. Surf. 2004, 2, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Ambrósio RJr Tervo, T.; Wilson, S.E. LASIK-associated dry eye and neurotrophic epitheliopathy: Pathophysiology and strategies for prevention and treatment. J. Refract. Surg. 2008, 24, 396–407. [Google Scholar]
- Ganesh, S.; Brar, S.; Pawar, A. Matched population comparison of visual outcomes and patient satisfaction between 3 modalities for the correction of low to moderate myopic astigmatism. Clin. Ophthalmol. 2017, 11, 1253–1263. [Google Scholar] [CrossRef] [PubMed]
- Gjerdrum, B.; Gundersen, K.G.; Lundmark, P.O.; Potvin, R.; Aakre, B.M. Prevalence of signs and symptoms of dry eye disease 5 to 15 after refractive surgery. Clin. Ophthalmol. 2020, 14, 269–279. [Google Scholar] [CrossRef]
- Rosenberg, M.E.; Tervo, T.M.; Petroll, W.M.; Vesaluoma, M.H. In vivo confocal microscopy of patients with corneal recurrent erosion syndrome or epithelial basement membrane dystrophy. Ophthalmology 2000, 107, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Efron, N. Contact lens-induced changes in the anterior eye as observed in vivo with the confocal microscope. Prog. Retin. Eye Res. 2007, 26, 398–436. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, B.; Irkec, M.; Mocan, M.C. In vivo confocal microscopic findings in posterior polymorphous corneal dystrophy. Cornea 2013, 32, 1237–1242. [Google Scholar] [CrossRef]
- Giannaccare, G.; Bernabei, F.; Pellegrini, M.; Guaraldi, F.; Turchi, F.; Torrazza, C.; Senni, C.; Scotto, R.; Sindaco, D.; Di Cello, L.; et al. Bilateral morphometric analysis of corneal sub-basal nerve plexus in patients undergoing unilateral cataract surgery: A preliminary in vivo confocal microscopy study. Br. J. Ophthalmol. 2021, 105, 174–179. [Google Scholar] [CrossRef]
- Pacaud, D.; Romanchuk, K.G.; Tavakoli, M.; Gougeon, C.; Virtanen, H.; Ferdousi, M.; Nettel-Aguirre, A.; Mah, J.K.; Malik, R.A. The Reliability and Reproducibility of Corneal Confocal Microscopy in Children. Investig. Opthalmol. Vis. Sci. 2015, 56, 5636–5640. [Google Scholar] [CrossRef] [PubMed]
- Takhar, J.S.; Joye, A.S.D.; Lopez, S.E.O.; Marneris, A.G.D.; Tsui, E.; Seitzman, G.D.; Keenan, J.D.; Gonzales, J.A. Validation of a Novel Confocal Microscopy Imaging Protocol with Assessment of Reproducibility and Comparison of Nerve Metrics in Dry Eye Disease Compared with Controls. Cornea 2021, 40, 603–612. [Google Scholar] [CrossRef] [PubMed]
- Wei, Q.; Zhou, X.; Chang, W.; Jiang, R.; Zhou, X.; Yu, Z. Retinal and Choroidal Changes following Implantable Collamer Lens V4c Implantation in High Myopia Patients-A 1-Year Follow-Up Study. Diagnostics 2023, 13, 3097. [Google Scholar] [CrossRef]
- Kowtharapu, B.S.; Stahnke, T.; Wree, A.; Guthoff, R.F.; Stachs, O. Corneal epithelial and neuronal interactions: Role in wound healing. Exp. Eye Res. 2014, 125, 53–61. [Google Scholar] [CrossRef]
- Versura, P.; Giannaccare, G.; Pellegrini, M.; Sebastiani, S.; Campos, E.C. Neurotrophic keratitis: Current challenges and future prospects. Eye Brain 2018, 10, 37–45. [Google Scholar] [CrossRef]
- Saad, S.; Abdelmassih, Y.; Saad, R.; Guindolet, D.; el Khoury, S.; Doan, S.; Cochereau, I.; Gabison, E.E. Neurotrophic keratitis: Frequency, etiologies, clinical management and outcomes. Ocul. Surf. 2020, 18, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Moilanen, J.A.; Vesaluoma, M.H.; Müller, L.J.; Tervo, T.M. Long-term corneal morphology after PRK by in vivo confocal microscopy. Investig. Opthalmol. Vis. Sci. 2003, 44, 1064–1069. [Google Scholar] [CrossRef] [PubMed]
- Erie, J.C.; McLaren, J.W.; Hodge, D.O.; Bourne, W.M. Recovery of corneal subbasal nerve density after PRK and LASIK. Am. J. Ophthalmol. 2005, 140, 1059–1064. [Google Scholar] [CrossRef]
- Linna, T.; Tervo, T. Real-time confocal microscopic observations on human corneal nerves and wound healing after excimer laser photorefractive keratectomy. Curr. Eye Res. 1997, 16, 640–649. [Google Scholar] [CrossRef]
- Lee, B.H.; McLaren, J.W.; Erie, J.C.; Hodge, D.O.; Bourne, W.M. Reinnervation in the cornea after LASIK. Investig. Ophthalmol. Vis. Sci. 2002, 43, 3660–3664. [Google Scholar]
- Linna, T.U.; Vesaluoma, M.H.; Pérez-Santonja, J.J.; Petroll, W.M.; Alió, J.L.; Tervo, T.M. Effect of myopic LASIK on corneal sensitivity and morphology of subbasal nerves. Investig. Ophthalmol. Vis. Sci. 2000, 41, 393–397. [Google Scholar]
- Darwish, T.; Brahma, A.; O’Donnell, C.; Efron, N. Subbasal nerve fiber regeneration after LASIK and LASEK assessed by noncontact esthesiometry and in vivo confocal microscopy: Prospective study. J. Cataract. Refract. Surg. 2007, 33, 1515–1521. [Google Scholar] [CrossRef] [PubMed]
- Hou, C.; Li, J.; Li, J.; Peng, H.; Wang, Q. In vivo confocal microscopy of sub-basal corneal nerves and corneal densitometry after three kinds of refractive procedures for high myopia. Int. Ophthalmol. 2023, 43, 925–935. [Google Scholar] [CrossRef] [PubMed]
- Hamrah, P.; Seyed-Razavi, Y.; Yamaguchi, T. Translational Immunoimaging and Neuroimaging Demonstrate Corneal Neuroimmune Crosstalk. Cornea 2016, 35 (Suppl. S1), S20–S24. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.K.; Kim, K.W.; Ryu, J.S.; Jeong, H.J.; Lee, S.M.; Kim, M.K. Bilateral Effect of the Unilateral Corneal Nerve Cut on Both Ocular Surface and Lacrimal Gland. Investig. Opthalmol. Vis. Sci. 2019, 60, 430–441. [Google Scholar] [CrossRef] [PubMed]
- Mastropasqua, L.; Nubile, M.; Lanzini, M.; Carpineto, P.; Ciancaglini, M.; Pannellini, T.; Di Nicola, M.; Dua, H.S. Epithelial dendritic cell distribution in normal and inflamed human cornea: In vivo confocal microscopy study. Am. J. Ophthalmol. 2006, 142, 736–744. [Google Scholar] [CrossRef] [PubMed]
- Villani, E.; Garoli, E.; Termine, V.; Pichi, F.; Ratiglia, R.; Nucci, P. Corneal Confocal Microscopy in Dry Eye Treated with Corticosteroids. Optom. Vis. Sci. 2015, 92, e290–e295. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Shigeno, Y.; Sato, E.A.; Ibrahim, O.M.A.; Saiki, M.; Negishi, K.; Ogawa, Y.; Dogru, M.; Tsubota, K. The evaluation of the treatment response in obstructive meibomian gland disease by in vivo laser confocal microscopy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2009, 247, 821–829. [Google Scholar] [CrossRef]
- Parissi, M.; Karanis, G.; Randjelovic, S.; Germundsson, J.; Poletti, E.; Ruggeri, A.; Utheim, T.P.; Lagali, N. Standardized baseline human corneal subbasal nerve density for clinical investigations with laser-scanning in vivo confocal microscopy. Investig. Opthalmol. Vis. Sci. 2013, 54, 7091–7102. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.-C.; So, W.; Wong, N.Q.; Tan, H.; Lin, M.Y.; Lee, I.Y.; Mehta, J. Diabetic corneal neuropathy as a surrogate marker for diabetic peripheral neuropathy. Neural Regen. Res. 2022, 17, 2172–2178. [Google Scholar] [CrossRef] [PubMed]
- Belmonte, C.; Acosta, M.C.; Gallar, J. Neural basis of sensation in intact and injured corneas. Exp. Eye Res. 2004, 78, 513–525. [Google Scholar] [CrossRef] [PubMed]
- Sitompul, R.; Sancoyo, G.S.; Hutauruk, J.A.; Gondhowiardjo, T.D. Sensitivity change in cornea and tear layer due to incision difference on cataract surgery with either manual small-incision cataract surgery or phacoemulsification. Cornea 2008, 27 (Suppl. S1), S13–S18. [Google Scholar] [CrossRef]
- Kim, J.H.; Chung, J.L.; Kang, S.Y.; Kim, S.W.; Seo, K.Y. Change in Corneal Sensitivity and Corneal Nerve after Cataract Surgery. Cornea 2009, 28, S20–S25. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Total or Mean (Range) |
|---|---|
| No. of patients | 37 |
| No. of eyes (right/left) | 37 (23/14) |
| Gender (n, male/female) | 8/29 |
| Age (yrs) | 26.6 ± 5.4 (17~41) |
| Spherical equivalent refraction (D) | −10.04 ± 2.70 (−16.75~−5.0) |
| Best-corrected visual acuity (logMAR) | 0.03 ± 0.07 (−0.07~0.30) |
| Axial length (mm) | 27.43 ± 1.4 (24.81~30.34) |
| Central corneal thickness (μm) | 517.76 ± 29.2 (469~630) |
| Anterior chamber depth (mm) | 3.32 ± 0.36 (2.69~4.25) |
| Lens thickness (mm) | 3.71 ± 0.25 (3.21~4.23) |
| Corneal endothelial cell density (cell/mm2) | 2998.82 ± 255.11 (2607~3653) |
| Anterior chamber volume (mm3) | 200.47 ± 34.1 (136~279) |
| Parameter | Before Surgery | After Surgery | p * | |||||
|---|---|---|---|---|---|---|---|---|
| Day 1 | Week 1 | Month 1 | Month 3 | Month 6 | Month 12 | |||
| Eyes (n) | 37 | 36 | 29 | 22 | 27 | 12 | 12 | |
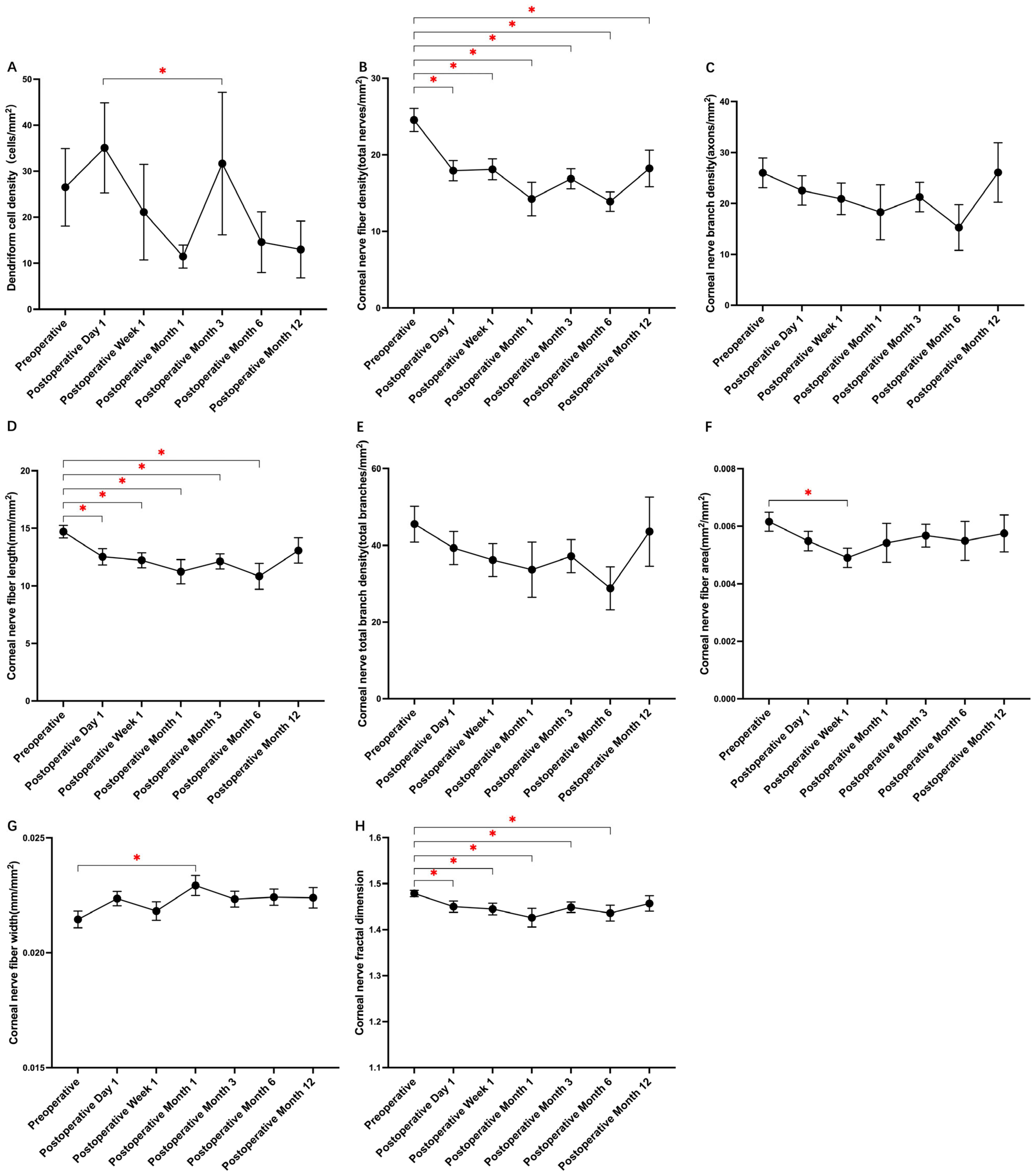
| DC density (number/mm2) | 26.52 ± 50.6 | 35.07 ± 57.8 | 21.12 ± 55.0 | 11.46 ± 10.3 | 31.65 ± 84.9 | 14.58 ± 18.6 | 12.98 ± 21.4 | 0.008 |
| CNFD (total nerves/mm2) | 24.55 ± 9.1 | 17.93 ± 7.7 | 18.11 ± 7.3 | 14.23 ± 9.0 | 16.87 ± 7.1 | 13.89 ± 3.6 | 18.22 ± 8.3 | 0.000 |
| CNBD (axons/mm2) | 26.01 ± 17.5 | 22.54 ± 17.0 | 20.90 ± 16.7 | 18.29 ± 22.2 | 21.27 ± 15.6 | 15.27 ± 12.7 | 26.08 ± 20.2 | 0.366 |
| CNFL (mm/mm2) | 14.71 ± 3.2 | 12.54 ± 4.2 | 12.23 ± 3.5 | 11.24 ± 4.3 | 12.14 ± 3.6 | 10.84 ± 3.2 | 13.09 ± 3.8 | 0.000 |
| CTBD (total branches/mm2) | 45.52 ± 27.9 | 39.31 ± 25.5 | 36.18 ± 23.0 | 33.66 ± 29.7 | 37.19 ± 23.3 | 28.82 ± 15.8 | 43.55 ± 31.2 | 0.373 |
| CNFA (mm2/mm2) | 0.0062 ± 0.002 | 0.0055 ± 0.002 | 0.0049 ± 0.002 | 0.0054 ± 0.003 | 0.0057 ± 0.002 | 0.0055 ± 0.002 | 0.0058 ± 0.002 | 0.043 |
| CNFW (mm/mm2) | 0.0215 ± 0.002 | 0.0224 ± 0.002 | 0.0218 ± 0.002 | 0.0229 ± 0.002 | 0.0223 ± 0.002 | 0.0224 ± 0.001 | 0.0224 ± 0.002 | 0.045 |
| CNFrD | 1.479 ± 0.04 | 1.450 ± 0.07 | 1.445 ± 0.07 | 1.426 ± 0.08 | 1.449 ± 0.06 | 1.436 ± 0.05 | 1.457 ± 0.06 | 0.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, Q.; Ding, X.; Chang, W.; Zhou, X.; Jiang, R.; Zhou, X.; Yu, Z. Corneal Sub-Basal Nerve Plexus Regeneration Pattern following Implantable Collamer Lens Implantation for Myopia: A Prospective Longitudinal In Vivo Confocal Microscopy Study. Biomedicines 2024, 12, 555. https://doi.org/10.3390/biomedicines12030555
Wei Q, Ding X, Chang W, Zhou X, Jiang R, Zhou X, Yu Z. Corneal Sub-Basal Nerve Plexus Regeneration Pattern following Implantable Collamer Lens Implantation for Myopia: A Prospective Longitudinal In Vivo Confocal Microscopy Study. Biomedicines. 2024; 12(3):555. https://doi.org/10.3390/biomedicines12030555
Chicago/Turabian StyleWei, Qiaoling, Xuan Ding, Weiteng Chang, Xianjin Zhou, Rui Jiang, Xingtao Zhou, and Zhiqiang Yu. 2024. "Corneal Sub-Basal Nerve Plexus Regeneration Pattern following Implantable Collamer Lens Implantation for Myopia: A Prospective Longitudinal In Vivo Confocal Microscopy Study" Biomedicines 12, no. 3: 555. https://doi.org/10.3390/biomedicines12030555