
A Scoping Review on the Use of Non-Invasive Brain Stimulation Techniques for Persistent Post-Concussive Symptoms

 , , , , and
, , , , and
Abstract
:1. Introduction
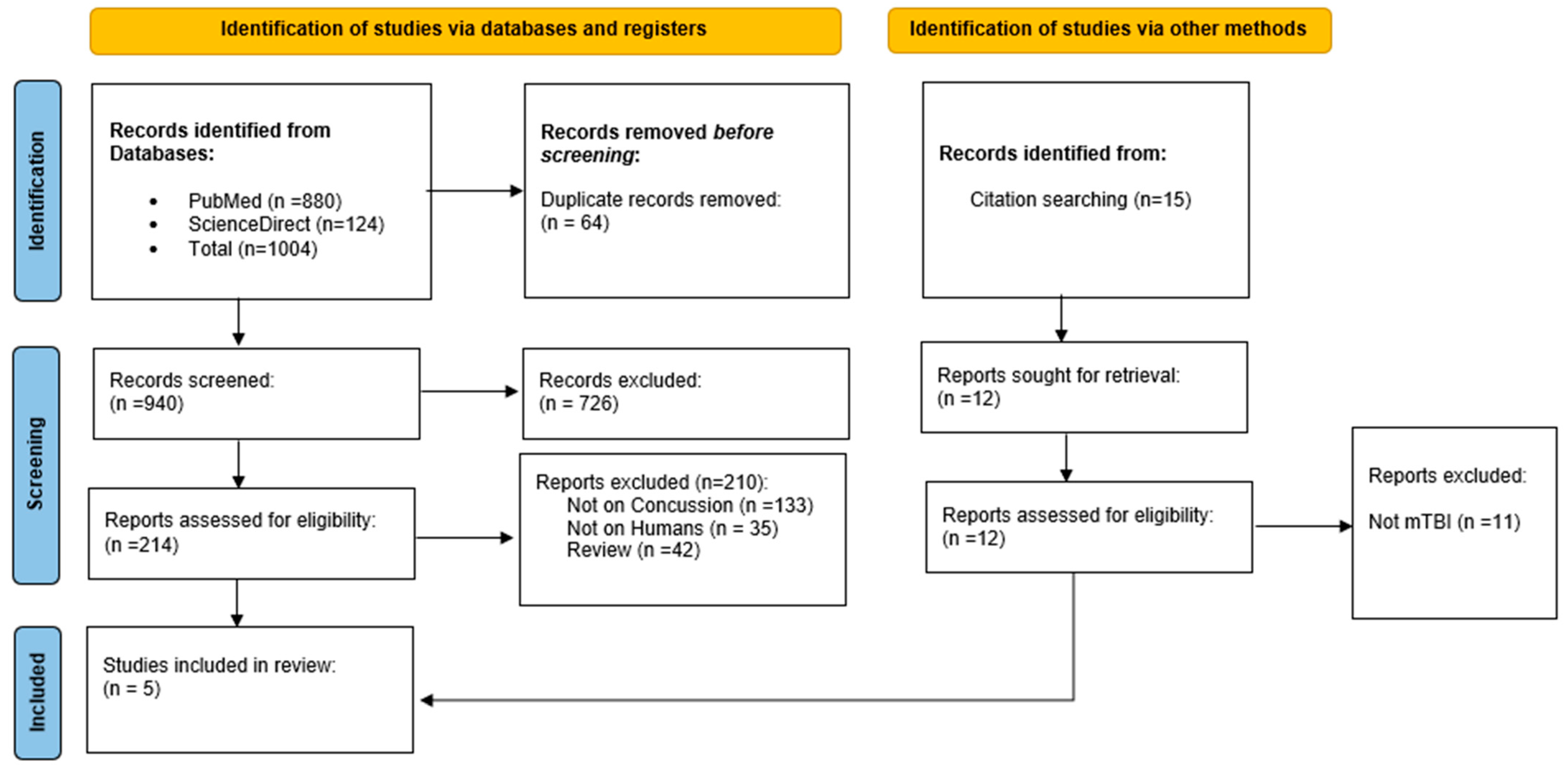
2. Search Methodology
3. Results
3.1. Cognitive Symptoms
3.2. Headache
3.3. Psychological Symptoms
3.4. PPCS—General Symptoms
4. Discussion
4.1. Which Post-Concussion Symptoms Were Investigated, and Which Ones Remain Unexplored?
4.2. What Are the Main Targeted Brain Areas?
4.3. What Is the Optimal NIBS Technique for Managing PPCS?
4.4. What Is the Existing Evidence in Other TBI Populations?
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Dewan, M.C.; Rattani, A.; Gupta, S.; Baticulon, R.E.; Hung, Y.-C.; Punchak, M.; Agrawal, A.; Adeleye, A.O.; Shrime, M.G.; Rubiano, A.M.; et al. Estimating the Global Incidence of Traumatic Brain Injury. J. Neurosurg. 2018, 130, 1080–1097. [Google Scholar] [CrossRef] [PubMed]
- Woodrow, R.E.; Winzeck, S.; Luppi, A.I.; Kelleher-Unger, I.R.; Spindler, L.R.B.; Wilson, J.T.L.; Newcombe, V.F.J.; Coles, J.P.; CENTER-TBI MRI Substudy Participants and Investigators; Amrein, K.; et al. Acute Thalamic Connectivity Precedes Chronic Post-Concussive Symptoms in Mild Traumatic Brain Injury. Brain 2023, 146, 3484–3499. [Google Scholar] [CrossRef] [PubMed]
- Giza, C.C.; Hovda, D.A. The New Neurometabolic Cascade of Concussion. Neurosurgery 2014, 75, S24–S33. [Google Scholar] [CrossRef]
- Hiploylee, C.; Dufort, P.A.; Davis, H.S.; Wennberg, R.A.; Tartaglia, M.C.; Mikulis, D.; Hazrati, L.N.; Tator, C.H. Longitudinal Study of Postconcussion Syndrome: Not Everyone Recovers. J. Neurotrauma 2017, 34, 1511–1523. [Google Scholar] [CrossRef]
- Tator, C.H.; Davis, H.S.; Dufort, P.A.; Tartaglia, M.C.; Davis, K.D.; Ebraheem, A.; Hiploylee, C. Postconcussion Syndrome: Demographics and Predictors in 221 Patients. J. Neurosurg. 2016, 125, 1204. [Google Scholar] [CrossRef]
- Mayer, A.R.; Quinn, D.K.; Master, C.L. The Spectrum of Mild Traumatic Brain Injury: A Review. Neurology 2017, 89, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Audrit, H.; Beauchamp, M.H.; Tinawi, S.; Laguë-Beauvais, M.; de Guise, E. Development and Description of SAAM Intervention: A Brief, Multidimensional and Psycho-Educational Intervention for Adults with Mild Traumatic Brain Injury. Ann. Phys. Rehabil. Med. 2021, 64, 101424. [Google Scholar] [CrossRef]
- Patricios, J.S.; Schneider, K.J.; Dvorak, J.; Ahmed, O.H.; Blauwet, C.; Cantu, R.C.; Davis, G.A.; Echemendia, R.J.; Makdissi, M.; McNamee, M.; et al. Consensus Statement on Concussion in Sport: The 6th International Conference on Concussion in Sport–Amsterdam, October 2022. Br. J. Sports Med. 2023, 57, 695–711. [Google Scholar] [CrossRef]
- Putukian, M.; Purcell, L.; Schneider, K.J.; Black, A.M.; Burma, J.S.; Chandran, A.; Boltz, A.; Master, C.L.; Register-Mihalik, J.K.; Anderson, V.; et al. Clinical Recovery from Concussion–Return to School and Sport: A Systematic Review and Meta-Analysis. Br. J. Sports Med. 2023, 57, 798–809. [Google Scholar] [CrossRef]
- Schneider, K.J.; Critchley, M.L.; Anderson, V.; Davis, G.A.; Debert, C.T.; Feddermann-Demont, N.; Gagnon, I.; Guskiewicz, K.M.; Hayden, K.A.; Herring, S.; et al. Targeted Interventions and Their Effect on Recovery in Children, Adolescents and Adults Who Have Sustained a Sport-Related Concussion: A Systematic Review. Br. J. Sports Med. 2023, 57, 771–779. [Google Scholar] [CrossRef]
- Leddy, J.J.; Burma, J.S.; Toomey, C.M.; Hayden, A.; Davis, G.A.; Babl, F.E.; Gagnon, I.; Giza, C.C.; Kurowski, B.G.; Silverberg, N.D.; et al. Rest and Exercise Early after Sport-Related Concussion: A Systematic Review and Meta-Analysis. Br. J. Sports Med. 2023, 57, 762–770. [Google Scholar] [CrossRef]
- Martens, G.; Khosravi, M.H.; Lejeune, N.; Kaux, J.-F.; Thibaut, A. Gender Specificities in Sleep Disturbances Following Mild Traumatic Brain Injury: A Preliminary Study. Brain Sci. 2023, 13, 323. [Google Scholar] [CrossRef]
- Quatman-Yates, C.C.; Hunter-Giordano, A.; Shimamura, K.K.; Landel, R.; Alsalaheen, B.A.; Hanke, T.A.; McCulloch, K.L.; Altman, R.D.; Beattie, P.; Berz, K.E.; et al. Physical Therapy Evaluation and Treatment After Concussion/Mild Traumatic Brain Injury: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability and Health From the Academy of Orthopaedic Physical Therapy of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2020, 50, CPG1–CPG73. [Google Scholar] [CrossRef]
- Kesikburun, S. Non-Invasive Brain Stimulation in Rehabilitation. Turk. J. Phys. Med. Rehabil. 2022, 68, 1–8. [Google Scholar] [CrossRef]
- Mortaheb, S.; Filippini, M.M.; Kaux, J.F.; Annen, J.; Lejeune, N.; Martens, G.; Calderón, M.A.F.; Laureys, S.; Thibaut, A. Neurophysiological Biomarkers of Persistent Post-Concussive Symptoms: A Scoping Review. Front. Neurol. 2021, 12, 687197. [Google Scholar] [CrossRef]
- Zhou, Y.; Milham, M.P.; Lui, Y.W.; Miles, L.; Reaume, J.; Sodickson, D.K.; Grossman, R.I.; Ge, Y. Default-Mode Network Disruption in Mild Traumatic Brain Injury. Radiology 2012, 265, 882–892. [Google Scholar] [CrossRef]
- Sours, C.; Kinnison, J.; Padmala, S.; Gullapalli, R.P.; Pessoa, L. Altered Segregation between Task-Positive and Task-Negative Regions in Mild Traumatic Brain Injury. Brain Imaging Behav. 2018, 12, 697–709. [Google Scholar] [CrossRef]
- Fox, M.D.; Snyder, A.Z.; Vincent, J.L.; Corbetta, M.; Van Essen, D.C.; Raichle, M.E. The Human Brain Is Intrinsically Organized into Dynamic, Anticorrelated Functional Networks. Proc. Natl. Acad. Sci. USA 2005, 102, 9673–9678. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A.; Paulus, W. Excitability Changes Induced in the Human Motor Cortex by Weak Transcranial Direct Current Stimulation. J. Physiol. 2000, 527, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Santos Ferreira, I.; Teixeira Costa, B.; Lima Ramos, C.; Lucena, P.; Thibaut, A.; Fregni, F. Searching for the Optimal tDCS Target for Motor Rehabilitation. J. NeuroEng. Rehabil. 2019, 16, 90. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, J.-P.; Antal, A.; Ayache, S.S.; Benninger, D.H.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; De Ridder, D.; Ferrucci, R.; Langguth, B.; et al. Evidence-Based Guidelines on the Therapeutic Use of Transcranial Direct Current Stimulation (tDCS). Clin. Neurophysiol. 2017, 128, 56–92. [Google Scholar] [CrossRef] [PubMed]
- du Plessis, S.; Oni, I.K.; Lapointe, A.P.; Campbell, C.; Dunn, J.F.; Debert, C.T. Treatment of Persistent Postconcussion Syndrome With Repetitive Transcranial Magnetic Stimulation Using Functional Near-Infrared Spectroscopy as a Biomarker of Response: Protocol for a Randomized Controlled Clinical Trial. JMIR Res. Protoc. 2022, 11, e31308. [Google Scholar] [CrossRef] [PubMed]
- Stilling, J.; Paxman, E.; Mercier, L.; Gan, L.S.; Wang, M.; Amoozegar, F.; Dukelow, S.P.; Monchi, O.; Debert, C. Treatment of Persistent Post-Traumatic Headache and Post-Concussion Symptoms Using Repetitive Transcranial Magnetic Stimulation: A Pilot, Double-Blind, Randomized Controlled Trial. J. Neurotrauma 2020, 37, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Study Quality Assessment Tools|NHLBI, NIH. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 2 February 2024).
- Silverberg, N.D.; Iverson, G.L.; Cogan, A.; Dams-O-Connor, K.; Delmonico, R.; Graf, M.J.P.; Iaccarino, M.A.; Kajankova, M.; Kamins, J.; McCulloch, K.L.; et al. The American Congress of Rehabilitation Medicine Diagnostic Criteria for Mild Traumatic Brain Injury. Arch. Phys. Med. Rehabil. 2023, 104, 1343–1355. [Google Scholar] [CrossRef] [PubMed]
- Quinn De Launay, K.; Cheung, S.T.; Riggs, L.; Reed, N.; Beal, D.S. The Effect of Transcranial Direct Current Stimulation on Cognitive Performance in Youth with Persistent Cognitive Symptoms Following Concussion: A Controlled Pilot Study. Brain Inj. 2022, 36, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.; Shukla, S.; Fallah, A.; Song, D.; Lin, L.; Golshan, S.; Tsai, A.; Jak, A.; Polston, G.; Lee, R. Repetitive Transcranial Magnetic Stimulation in Managing Mild Traumatic Brain Injury-Related Headaches. Neuromodul. J. Int. Neuromodul. Soc. 2016, 19, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.; Metzger-Smith, V.; He, Y.; Cordero, J.; Ehlert, B.; Song, D.; Lin, L.; Shahrokh, G.; Tsai, A.; Vaninetti, M.; et al. Left Dorsolateral Prefrontal Cortex rTMS in Alleviating MTBI Related Headaches and Depressive Symptoms. Neuromodul. J. Int. Neuromodul.Soc. 2018, 21, 390–401. [Google Scholar] [CrossRef]
- Moussavi, Z.; Suleiman, A.; Rutherford, G.; Ranjbar Pouya, O.; Dastgheib, Z.; Zhang, W.; Salter, J.; Wang, X.; Mansouri, B.; Lithgow, B. A Pilot Randomised Double-Blind Study of the Tolerability and Efficacy of Repetitive Transcranial Magnetic Stimulation on Persistent Post-Concussion Syndrome. Sci. Rep. 2019, 9, 5498. [Google Scholar] [CrossRef]
- Cunningham, J.; Broglio, S.P.; O’Grady, M.; Wilson, F. History of Sport-Related Concussion and Long-Term Clinical Cognitive Health Outcomes in Retired Athletes: A Systematic Review. J. Athl. Train. 2020, 55, 132–158. [Google Scholar] [CrossRef]
- McInnes, K.; Friesen, C.L.; MacKenzie, D.E.; Westwood, D.A.; Boe, S.G. Mild Traumatic Brain Injury (mTBI) and Chronic Cognitive Impairment: A Scoping Review. PLoS ONE 2017, 12, e0174847. [Google Scholar] [CrossRef]
- Bigler, E.D. Neuropsychology and Clinical Neuroscience of Persistent Post-Concussive Syndrome. J. Int. Neuropsychol. Soc. JINS 2008, 14, 1–22. [Google Scholar] [CrossRef]
- Arnold, M. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd Edition. Cephalalgia Int. J. Headache 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Capi, M.; Pomes, L.M.; Andolina, G.; Curto, M.; Martelletti, P.; Lionetto, L. Persistent Post-Traumatic Headache and Migraine: Pre-Clinical Comparisons. Int. J. Environ. Res. Public. Health 2020, 17, 2585. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Care Services; Board on Health Sciences Policy; Committee on Accelerating Progress in Traumatic Brain Injury Research and Care; Matney, C.; Bowman, K.; Berwick, D. (Eds.) Traumatic Brain Injury: A Roadmap for Accelerating Progress; National Academies Press: Cambridge, MA, USA, 2022. [Google Scholar]
- Silverberg, N.D.; Mikolić, A. Management of Psychological Complications Following Mild Traumatic Brain Injury. Curr. Neurol. Neurosci. Rep. 2023, 23, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Kreitzer, N.; Ancona, R.; McCullumsmith, C.; Kurowski, B.G.; Foreman, B.; Ngwenya, L.B.; Adeoye, O. The Effect of Antidepressants on Depression after Traumatic Brain Injury: A Meta-Analysis. J. Head Trauma Rehabil. 2019, 34, E47. [Google Scholar] [CrossRef]
- Chen, C.-L.; Lin, M.-Y.; Huda, M.H.; Tsai, P.-S. Effects of Cognitive Behavioral Therapy for Adults with Post-Concussion Syndrome: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Psychosom. Res. 2020, 136, 110190. [Google Scholar] [CrossRef]
- McCrory, P.; Meeuwisse, W.; Dvořák, J.; Aubry, M.; Bailes, J.; Broglio, S.; Cantu, R.C.; Cassidy, D.; Echemendia, R.J.; Castellani, R.J.; et al. Consensus statement on concussion in sport—The 5th international conference on concussion in sport held in Berlin, October 2016. Br. J. Sports Med. 2017, 51, 838–847. [Google Scholar] [CrossRef]
- King, N.S.; Crawford, S.; Wenden, F.J.; Moss, N.E.G.; Wade, D.T. The Rivermead Post Concussion Symptoms Questionnaire: A Measure of Symptoms Commonly Experienced after Head Injury and Its Reliability. J. Neurol. 1995, 242, 587–592. [Google Scholar] [CrossRef]
- Charest, J.; Marois, A.; Bastien, C.H. Can a tDCS treatment enhance subjective and objective sleep among student-athletes? J. Ach. 2021, 69, 378–389. [Google Scholar] [CrossRef]
- Herrero Babiloni, A.; Bellemare, A.; Beetz, G.; Vinet, S.-A.; Martel, M.O.; Lavigne, G.J.; De Beaumont, L. The Effects of Non-Invasive Brain Stimulation on Sleep Disturbances among Different Neurological and Neuropsychiatric Conditions: A Systematic Review. Sleep Med. Rev. 2021, 55, 101381. [Google Scholar] [CrossRef]
- Thibaut, A.; Schiff, N.D. New Therapeutic Options for the Treatment of Patients with Disorders of Consciousness: The Field of Neuromodulation. In Coma and Disorders of Consciousness; Schnakers, C., Laureys, S., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 207–223. ISBN 978-3-319-55964-3. [Google Scholar]
- D’Esposito, M.; Detre, J.A.; Alsop, D.C.; Shin, R.K.; Atlas, S.; Grossman, M. The Neural Basis of the Central Executive System of Working Memory. Nature 1995, 378, 279–281. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Li, X.-X.; Wei, S.; Zhao, D.; Ding, J.; Xu, Y.; Yu, C.; Chen, Z.; Zhou, D.-S.; Yuan, T.-F. Orbitofrontal Cortex-Hippocampus Potentiation Mediates Relief for Depression: A Randomized Double-Blind Trial and TMS-EEG Study. Cell Rep. Med. 2023, 4, 101060. [Google Scholar] [CrossRef] [PubMed]
- Safiai, N.I.M.; Mohamad, N.A.; Basri, H.; Mat, L.N.I.; Hoo, F.K.; Rashid, A.M.A.; Khan, A.H.K.Y.; Loh, W.C.; Baharin, J.; Fernandez, A.; et al. High-Frequency Repetitive Transcranial Magnetic Stimulation at Dorsolateral Prefrontal Cortex for Migraine Prevention: A Protocol for a Systematic Review of Controlled Trials. PLoS ONE 2021, 16, e0251528. [Google Scholar] [CrossRef]
- Pearson, K. Motor Systems. Curr. Opin. Neurobiol. 2000, 10, 649–654. [Google Scholar] [CrossRef]
- Bhattacharjee, S.; Kashyap, R.; Abualait, T.; Annabel Chen, S.-H.; Yoo, W.-K.; Bashir, S. The Role of Primary Motor Cortex: More Than Movement Execution. J. Mot. Behav. 2021, 53, 258–274. [Google Scholar] [CrossRef] [PubMed]
- Madore, M.R.; Kozel, F.A.; Williams, L.M.; Green, L.C.; George, M.S.; Holtzheimer, P.E.; Yesavage, J.A.; Philip, N.S. Prefrontal Transcranial Magnetic Stimulation for Depression in US Military Veterans—A Naturalistic Cohort Study in the Veterans Health Administration. J. Affect. Disord. 2022, 297, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Carmi, L.; Tendler, A.; Bystritsky, A.; Hollander, E.; Blumberger, D.M.; Daskalakis, J.; Ward, H.; Lapidus, K.; Goodman, W.; Casuto, L.; et al. Efficacy and Safety of Deep Transcranial Magnetic Stimulation for Obsessive-Compulsive Disorder: A Prospective Multicenter Randomized Double-Blind Placebo-Controlled Trial. Am. J. Psychiatry 2019, 176, 931–938. [Google Scholar] [CrossRef] [PubMed]
- Philip, N.S.; Ridout, S.J.; Albright, S.E.; Sanchez, G.; Carpenter, L.L. 5-Hz Transcranial Magnetic Stimulation for Comorbid Posttraumatic Stress Disorder and Major Depression. J. Trauma. Stress 2016, 29, 93–96. [Google Scholar] [CrossRef]
- Martin, D.M.; Liu, R.; Alonzo, A.; Green, M.; Loo, C.K. Use of Transcranial Direct Current Stimulation (tDCS) to Enhance Cognitive Training: Effect of Timing of Stimulation. Exp. Brain Res. 2014, 232, 3345–3351. [Google Scholar] [CrossRef]
- Yao, X.; Cui, L.; Wang, J.; Feng, W.; Bao, Y.; Xie, Q. Effects of Transcranial Direct Current Stimulation with Virtual Reality on Upper Limb Function in Patients with Ischemic Stroke: A Randomized Controlled Trial. J. Neuroeng. Rehabil. 2020, 17, 73. [Google Scholar] [CrossRef]
- Silverberg, N.D.; Otamendi, T. Advice to Rest for More Than 2 Days After Mild Traumatic Brain Injury Is Associated with Delayed Return to Productivity: A Case-Control Study. Front. Neurol. 2019, 10, 362. [Google Scholar] [CrossRef]
- Leddy, J.J.; Master, C.L.; Mannix, R.; Wiebe, D.J.; Grady, M.F.; Meehan, W.P.; Storey, E.P.; Vernau, B.T.; Brown, N.J.; Hunt, D.; et al. Early Targeted Heart Rate Aerobic Exercise versus Placebo Stretching for Sport-Related Concussion in Adolescents: A Randomised Controlled Trial. Lancet Child Adolesc. Health 2021, 5, 792–799. [Google Scholar] [CrossRef]
- Worts, P.R.; Mason, J.R.; Burkhart, S.O.; Sanchez-Gonzalez, M.A.; Kim, J.-S. The Acute, Systemic Effects of Aerobic Exercise in Recently Concussed Adolescent Student-Athletes: Preliminary Findings. Eur. J. Appl. Physiol. 2022, 122, 1441–1457. [Google Scholar] [CrossRef]
- Hutchison, M.G.; Di Battista, A.P.; Lawrence, D.W.; Pyndiura, K.; Corallo, D.; Richards, D. Randomized Controlled Trial of Early Aerobic Exercise Following Sport-Related Concussion: Progressive Percentage of Age-Predicted Maximal Heart Rate versus Usual Care. PLoS ONE 2022, 17, e0276336. [Google Scholar] [CrossRef]
- Gondoh, Y.; Sensui, H.; Kinomura, S.; Fukuda, H.; Fujimoto, T.; Masud, M.; Nagamatsu, T.; Tamaki, H.; Takekura, H. Effects of Aerobic Exercise Training on Brain Structure and Psychological Well-Being in Young Adults. J. Sports Med. Phys. Fit. 2009, 49, 129–135. [Google Scholar]
- Leddy, J.J.; Kozlowski, K.; Fung, M.; Pendergast, D.R.; Willer, B. Regulatory and Autoregulatory Physiological Dysfunction as a Primary Characteristic of Post Concussion Syndrome: Implications for Treatment. NeuroRehabilitation 2007, 22, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Clausen, M.; Pendergast, D.R.; Willer, B.; Leddy, J. Cerebral Blood Flow during Treadmill Exercise Is a Marker of Physiological Postconcussion Syndrome in Female Athletes. J. Head Trauma Rehabil. 2016, 31, 215–224. [Google Scholar] [CrossRef] [PubMed]
- Shirvani, S.; Davoudi, M.; Shirvani, M.; Koleini, P.; Hojat Panah, S.; Shoshtari, F.; Omidi, A. Comparison of the Effects of Transcranial Direct Current Stimulation and Mindfulness-Based Stress Reduction on Mental Fatigue, Quality of Life and Aggression in Mild Traumatic Brain Injury Patients: A Randomized Clinical Trial. Ann. Gen. Psychiatry 2021, 20, 33. [Google Scholar] [CrossRef] [PubMed]
- Quinn, D.K.; Upston, J.; Jones, T.; Brandt, E.; Story-Remer, J.; Fratzke, V.; Wilson, J.K.; Rieger, R.; Hunter, M.A.; Gill, D.; et al. Cerebral Perfusion Effects of Cognitive Training and Transcranial Direct Current Stimulation in Mild-Moderate TBI. Front. Neurol. 2020, 11, 545174. [Google Scholar] [CrossRef] [PubMed]
- Quinn, D.K.; Story-Remer, J.; Brandt, E.; Fratzke, V.; Rieger, R.; Wilson, J.K.; Gill, D.; Mertens, N.; Hunter, M.; Upston, J.; et al. Transcranial Direct Current Stimulation Modulates Working Memory and Prefrontal-Insula Connectivity after Mild-Moderate Traumatic Brain Injury. Front. Hum. Neurosci. 2022, 16, 1026639. [Google Scholar] [CrossRef]
- Rao, V.; Bechtold, K.; McCann, U.; Roy, D.; Peters, M.; Vaishnavi, S.; Yousem, D.; Mori, S.; Yan, H.; Leoutsakos, J.; et al. Low-Frequency Right Repetitive Transcranial Magnetic Stimulation for the Treatment of Depression After Traumatic Brain Injury: A Randomized Sham-Controlled Pilot Study. J. Neuropsychiatry Clin. Neurosci. 2019, 31, 306–318. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, S.H.; Trapp, N.T.; Hacker, C.D.; Laumann, T.O.; Kandala, S.; Hong, X.; Trillo, L.; Shahim, P.; Leuthardt, E.C.; Carter, A.R.; et al. Repetitive Transcranial Magnetic Stimulation with Resting-State Network Targeting for Treatment-Resistant Depression in Traumatic Brain Injury: A Randomized, Controlled, Double-Blinded Pilot Study. J. Neurotrauma 2019, 36, 1361–1374. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author [Reference] | Design | Patients | Target | Outcome Measure | Stimulation Protocol | Sham Protocol | Outcomes |
|---|---|---|---|---|---|---|---|
| De Launay et al. [26] | Double-blind, sham-controlled clinical trial | N = 12 with cognitive PPCSs | Left DLPFC | Cognitive symptoms (working memory): Dual N-Back WMT | Three sessions of anodal tDCS for 20 min at 1.5 mA | Three sessions of sham tDCS for 20 min at 1.5 mA | -No changes in reaction times in both sham and active groups -Improved N2 and N3 level accuracy in active tDCS |
| Leung et al. [27] | Single-blind, sham-controlled clinical trial | N = 24 with post-concussion chronic headache | Left Motor Cortex | Headaches: daily headache diary | Three sessions of rTMS: 2000 pulses (20 trains of 100 pulses at 10 Hz) in one week | Three sessions of sham rTMS: 2000 pulses (20 trains of 100 pulses at 10 Hz) in one week | -Reduced intensity of persistent headache and debilitating headache exacerbation score in active rTMS |
| Leung et al. [28] | Single-blind, sham-controlled clinical trial | N = 29 with persistent concussion-related headaches (mTBI-HA) | Left DLPFC | Depression: HRSD Headaches: VAS | Four sessions of active rTMS (20 trains of 100 pulses at 10 Hz) | Four sessions of sham rTMS (over treatment area) | -Improved HRSD level in active rTMS -Reduced intensity of persistent headache and debilitating headache exacerbation score in active rTMS in both one- and four-week assessments |
| Moussavi et al. [29] | Randomized, double-blind, sham-controlled trial | N = 18 with PPCS and depression in two groups: short and long durations of symptoms | Left DLPFC | General PPCS: RPQ Depression: MADRS | 13 treatment sessions of low- frequency rTMS within three weeks (25 trains of 30 pulses at 20 Hz) | 13 treatment sessions of low-frequency rTMS within three weeks | -Decreased RPQ3 and MADRS in both active and sham treatment in group with short duration of symptoms -Decreased RPQ13 in active group with short duration of symptoms -Non-significant decrease in RPQ3 and 13 for patients with long duration of symptoms -No MADRS improvement for patients with long duration of symptoms |
| Stilling et al. [23] | Randomized, double-blind, sham-controlled trial | N = 20 patients with PTH and PPCS | Left DLPFC | Headaches: daily headache diary + HIT-6 HIT-Depression: PHQ-9 | 10 sessions of rTMS: 10 trains of 60 pulses at 10 Hz in two weeks | 10 sessions of sham rTMS in two weeks | -Non-significant decreased headache severity in both active and sham groups -Significant decrease in depression in active group |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khosravi, M.H.; Louras, M.; Martens, G.; Kaux, J.-F.; Thibaut, A.; Lejeune, N. A Scoping Review on the Use of Non-Invasive Brain Stimulation Techniques for Persistent Post-Concussive Symptoms. Biomedicines 2024, 12, 450. https://doi.org/10.3390/biomedicines12020450
Khosravi MH, Louras M, Martens G, Kaux J-F, Thibaut A, Lejeune N. A Scoping Review on the Use of Non-Invasive Brain Stimulation Techniques for Persistent Post-Concussive Symptoms. Biomedicines. 2024; 12(2):450. https://doi.org/10.3390/biomedicines12020450
Chicago/Turabian StyleKhosravi, Mohammad Hossein, Mélanie Louras, Géraldine Martens, Jean-François Kaux, Aurore Thibaut, and Nicolas Lejeune. 2024. "A Scoping Review on the Use of Non-Invasive Brain Stimulation Techniques for Persistent Post-Concussive Symptoms" Biomedicines 12, no. 2: 450. https://doi.org/10.3390/biomedicines12020450