
Short-Term Outcomes and Efficacy of Percutaneous Deep Vein Arterialization for No-Option Critical Limb Ischemia: A Systematic Review and Meta-Analysis
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
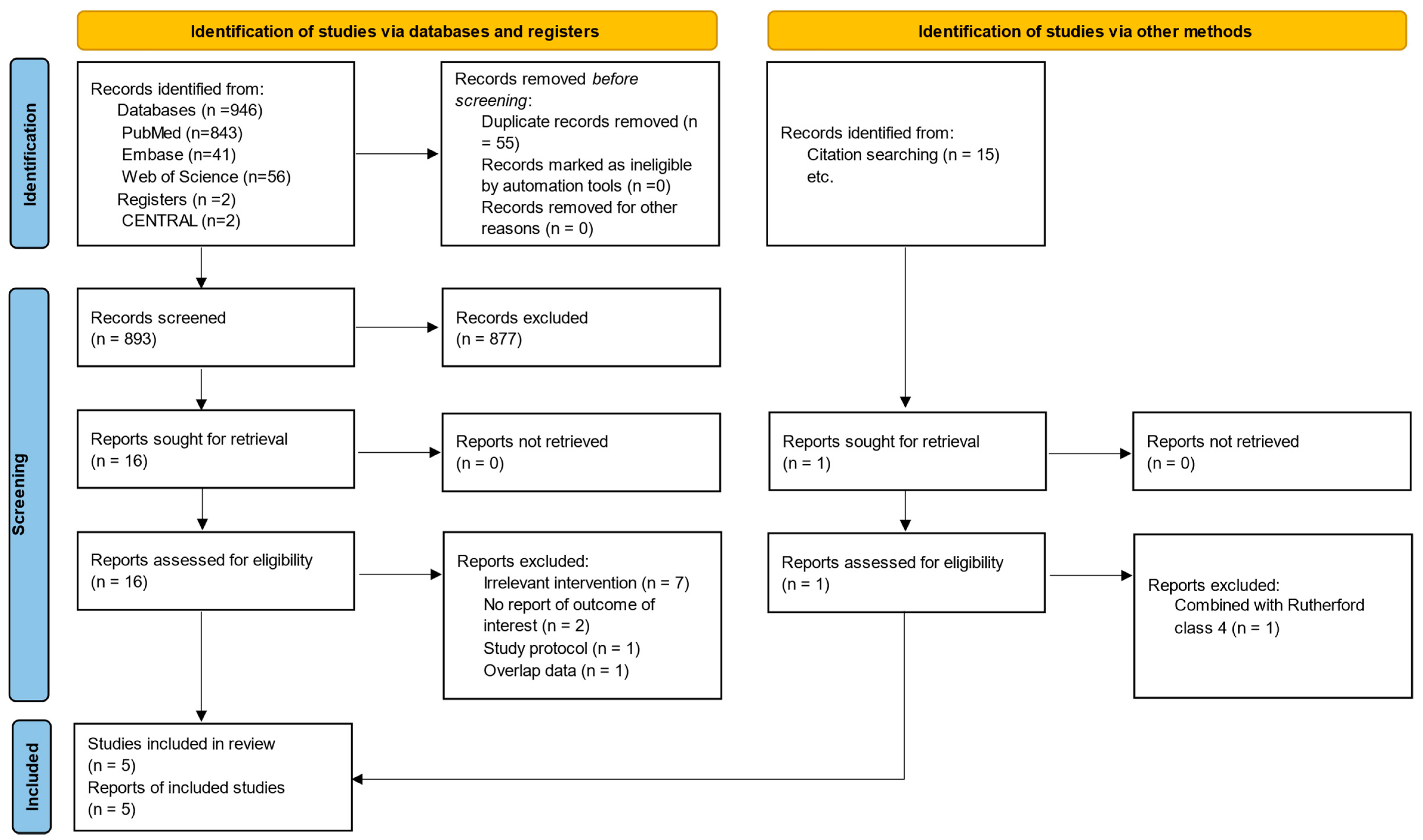
2.1. Search Strategy and Eligibility Criteria
2.2. Data Extraction and Quality Assessment
2.3. Statistical Analysis
3. Results
3.1. Study Design
3.2. Study Population
3.3. Risk of Bias Assessment
3.4. Outcomes
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Nehler, M.R.; Duval, S.; Diao, L.; Annex, B.H.; Hiatt, W.R.; Rogers, K.; Zakharyan, A.; Hirsch, A.T. Epidemiology of peripheral arterial disease and critical limb ischemia in an insured national population. J. Vasc. Surg. 2014, 60, 686–695.e2. [Google Scholar] [CrossRef]
- Hirsch, A.T.; Haskal, Z.J.; Hertzer, N.R.; Bakal, C.W.; Creager, M.A.; Halperin, J.L.; Hiratzka, L.F.; Murphy, W.R.C.; Olin, J.W.; Puschett, J.B.; et al. ACC/AHA 2005 Practice Guidelines for the Management of Patients with Peripheral Arterial Disease (Lower Extremity, Renal, Mesenteric, and Abdominal Aortic). Circulation 2006, 113, e463–e654. [Google Scholar] [CrossRef]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; Mills, J.L.; Ricco, J.-B.; Suresh, K.R.; Murad, M.H.; et al. Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. Eur. J. Vasc. Endovasc. Surg. 2019, 58, S1–S109.e33. [Google Scholar] [CrossRef]
- Duff, S.; Mafilios, M.S.; Bhounsule, P.; Hasegawa, J.T. The burden of critical limb ischemia: A review of recent literature. Vasc. Health Risk Manag. 2019, 15, 187–208. [Google Scholar] [CrossRef]
- Wong, K.L.; Nather, A.; Liang, S.; Chang, Z.; Wong, T.T.; Lim, C.T. Clinical outcomes of below knee amputations in diabetic foot patients. Ann. Acad. Med. Singap. 2013, 42, 388–394. [Google Scholar] [CrossRef]
- Benoit, E.; O’Donnell, T.F.; Kitsios, G.D.; Iafrati, M.D. Improved amputation-free survival in unreconstructable critical limb ischemia and its implications for clinical trial design and quality measurement. J. Vasc. Surg. 2012, 55, 781–789. [Google Scholar] [CrossRef]
- Schreve, M.A.; Ünlü, Ç.; Kum, S.; Tan, Y.K. Surgical and endovascular venous arterialization: Ready to take the “desert” by storm? J. Cardiovasc. Surg. 2017, 58, 402–408. [Google Scholar] [CrossRef]
- Halstead, A.E.; Vaughan, R.T. Arteriovenous anastomosis in the treatment of gangrene of the extremities. Trans. Am. Surg. Ass. 1911, 29, 265–315. [Google Scholar]
- Kum, S.; Tan, Y.K.; Schreve, M.A.; Ferraresi, R.; Varcoe, R.L.; Schmidt, A.; Scheinert, D.; Mustapha, J.A.; Lim, D.M.; Ho, D.; et al. Midterm Outcomes from a Pilot Study of Percutaneous Deep Vein Arterialization for the Treatment of No-Option Critical Limb Ischemia. J. Endovasc. Ther. 2017, 24, 619–626. [Google Scholar] [CrossRef]
- Shishehbor, M.H.; Powell, R.J.; Montero-Baker, M.F.; Dua, A.; Martinez-Trabal, J.L.; Bunte, M.C.; Lee, A.C.; Mugglin, A.S.; Mills, J.L.; Farber, A.; et al. Transcatheter Arterialization of Deep Veins in Chronic Limb-Threatening Ischemia. N. Engl. J. Med. 2023, 388, 1171–1180. [Google Scholar] [CrossRef]
- Nakama, T.; Ichihashi, S.; Ogata, K.; Kojima, S.; Muraishi, M.; Obunai, K.; Watanabe, H. Twelve-Month Clinical Outcomes of Percutaneous Deep Venous Arterialization with Alternative Techniques and Ordinary Endovascular Therapy Devices for Patients with Chronic Limb-Threatening Ischemia: Results of the DEPARTURE Japan Study. Cardiovasc. Interv. Radiol. 2022, 45, 622–632. [Google Scholar] [CrossRef]
- Yan, Q.; Prasla, S.; Carlisle, D.C.; Rajesh, A.; Treffalls, J.; Davies, M.G. Deep Venous Arterialization for Chronic Limb Threatening Ischemia in Atherosclerosis Patients—A Meta-Analysis. Ann. Vasc. Surg. 2022, 81, 1–21. [Google Scholar] [CrossRef]
- Matthew, J.P.; Joanne, E.M.; Patrick, M.B.; Isabelle, B.; Tammy, C.H.; Cynthia, D.M.; Larissa, S.; Jennifer, M.T.; Elie, A.A.; Sue, E.B.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Schmidt, A.; Schreve, M.A.; Huizing, E.; Del Giudice, C.; Branzan, D.; Unlu, C.; Varcoe, R.L.; Ferraresi, R.; Kum, S. Midterm Outcomes of Percutaneous Deep Venous Arterialization with a Dedicated System for Patients with No-Option Chronic Limb-Threatening Ischemia: The ALPS Multicenter Study. J. Endovasc. Ther. 2020, 27, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Miranda, J.A.; Pallister, Z.; Sharath, S.; Ferrer, L.; Chung, J.; Lepow, B.; Mills, J.L.; Montero-Baker, M. Early experience with venous arterialization for limb salvage in no-option patients with chronic limb-threatening ischemia. J. Vasc. Surg. 2022, 76, 987–996.e3. [Google Scholar] [CrossRef]
- Fashandi, A.Z.; Mehaffey, J.H.; Hawkins, R.B.; Kron, I.L.; Upchurch, G.R., Jr.; Robinson, W.P. Major adverse limb events and major adverse cardiac events after contemporary lower extremity bypass and infrainguinal endovascular intervention in patients with claudication. J. Vasc. Surg. 2018, 68, 1817–1823. [Google Scholar] [CrossRef] [PubMed]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Bowden, J.; Tierney, J.F.; Copas, A.J.; Burdett, S. Quantifying, displaying and accounting for heterogeneity in the meta-analysis of RCTs using standard and generalised Q statistics. BMC Med. Res. Methodol. 2011, 11, 41. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Sutton, A.J.; Duval, S.J.; Tweedie, R.L.; Abrams, K.R.; Jones, D.R. Empirical assessment of effect of publication bias on meta-analyses. BMJ 2000, 320, 1574–1577. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Clair, D.G.; Mustapha, J.A.; Shishehbor, M.H.; Schneider, P.A.; Henao, S.; Bernardo, N.N.; Deaton, D.H. PROMISE I: Early feasibility study of the LimFlow System for percutaneous deep vein arterialization in no-option chronic limb-threatening ischemia: 12-month results. J. Vasc. Surg. 2021, 74, 1626–1635. [Google Scholar] [CrossRef]
- Alexandrescu, V.; Ngongang, C.; Vincent, G.; Ledent, G.; Hubermont, G. Deep calf veins arterialization for inferior limb preservation in diabetic patients with extended ischaemic wounds, unfit for direct arterial reconstruction: Preliminary results according to an angiosome model of perfusion. Cardiovasc. Revasc. Med. 2011, 12, 10–19. [Google Scholar] [CrossRef]
- Schreve, M.A.; Minnee, R.C.; Bosma, J.; Leijdekkers, V.J.; Idu, M.M.; Vahl, A.C. Comparative study of venous arterialization and pedal bypass in a patient cohort with critical limb ischemia. Ann. Vasc. Surg. 2014, 28, 1123–1127. [Google Scholar] [CrossRef]
- Schreve, M.A.; Lichtenberg, M.; Ünlü, Ç.; Branzan, D.; Schmidt, A.; van den Heuvel, D.A.F.; Blessing, E.; Brodmann, M.; Cabane, V.; Lin, W.T.Q.; et al. PROMISE international; a clinical post marketing trial investigating the percutaneous deep vein arterialization (LimFlow) in the treatment of no-option chronic limb ischemia patient. CVIR Endovasc. 2019, 2, 26. [Google Scholar] [CrossRef]
- Mutirangura, P.; Ruangsetakit, C.; Wongwanit, C.; Sermsathanasawadi, N.; Chinsakchai, K. Pedal bypass with deep venous arterialization: The therapeutic option in critical limb ischemia and unreconstructable distal arteries. Vascular 2011, 19, 313–319. [Google Scholar] [CrossRef]
- Huizing, E.; Schreve, M.A.; Kum, S.; Papageorgiou, G.; de Vries, J.P.M.; de Borst, G.J.; Ünlü, Ç. Development of a Prediction Model for the Occurrence of Stenosis or Occlusion after Percutaneous Deep Venous Arterialization. Diagnostics 2021, 11, 1008. [Google Scholar] [CrossRef]
- Djoric, P.; Zeleskov-Djoric, J.; Stanisavljevic, D.M.; Markovic, Z.D.; Zivkovic, V.; Vuletic, M.; Djuric, D.; Jakovljevic, V. Distal venous arterialization and reperfusion injury: Focus on oxidative status. Eur. Surg. Res. 2012, 48, 200–207. [Google Scholar] [CrossRef]
- Satam, K.; Aboian, E.; Huttler, J.; Zhuo, H.; Zhang, Y.; Tonnessen, B.; Cardella, J.; Guzman, R.J.; Ochoa Chaar, C.I. Eligibility of Patients with Chronic Limb Threatening Ischemia for Deep Venous Arterialization. Ann. Vasc. Surg. 2022, 86, 260–267. [Google Scholar] [CrossRef]
- Ferraresi, R.; Casini, A.; Losurdo, F.; Caminiti, M.; Ucci, A.; Longhi, M.; Schreve, M.; Lichtenberg, M.; Kum, S.; Clerici, G. Hybrid Foot Vein Arterialization in No-Option Patients With Critical Limb Ischemia: A Preliminary Report. J. Endovasc. Ther. 2019, 26, 7–17. [Google Scholar] [CrossRef]
- Taylor, R.S.; Belli, A.M.; Jacob, S. Distal venous arterialisation for salvage of critically ischaemic inoperable limbs. Lancet 1999, 354, 1962–1965. [Google Scholar] [CrossRef]
- Engelke, C.; Morgan, R.A.; Quarmby, J.W.; Taylor, R.S.; Belli, A.M. Distal venous arterialization for lower limb salvage: Angiographic appearances and interventional procedures. Radiographics 2001, 21, 1239–1248; discussion 1248–1250. [Google Scholar] [CrossRef]
- Schreve, M.A.; Huizing, E.; Kum, S.; de Vries, J.P.M.; de Borst, G.J.; Ünlü, Ç. Volume Flow and Peak Systolic Velocity of the Arteriovenous Circuit in Patients after Percutaneous Deep Venous Arterialization. Diagnostics 2020, 10, 760. [Google Scholar] [CrossRef]
- Saab, F.A.; Mustapha, J.A.; Ansari, M.; Pupp, G.; Madassery, K.; N’Dandu, Z.; Wiechmann, B.N.; Bernstein, R.; Mize, A.; Pliagas, G. Percutaneous Deep Venous Arterialization: Treatment of Patients with End-Stage Plantar Disease. J. Am. Coll. Cardiol. 2022, 1, 100437. [Google Scholar] [CrossRef]
- Spiliopoulos, S.; Davoutis, E.; Arkoudis, N.-A.; Sritharan, K.; Lechareas, S. Percutaneous Deep Venous Arterialization for Limb Salvage in No Option Patients with Chronic Limb-Threatening Ischemia. J. Clin. Med. 2023, 12, 7324. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Ye, P.; Chen, Y.; Li, Y.; Cai, C.; Lv, P. The current state of endovascular intervention for critical limb ischemia: A systematic review. Vasc. Investig. Ther. 2021, 4, 46–53. [Google Scholar] [CrossRef]
- Baser, O.; Verpillat, P.; Gabriel, S.; Wanf, L. Prevalence, incidence, and outcomes of critical limb ischemia in the US Medicare population. Vasc. Dis. Manag. 2013, 10, 26–36. [Google Scholar]
- Ho, V.T.; Gologorsky, R.; Kibrik, P.; Chandra, V.; Prent, A.; Lee, J.; Dua, A. Open, percutaneous, and hybrid deep venous arterialization technique for no-option foot salvage. J. Vasc. Surg. 2020, 71, 2152–2160. [Google Scholar] [CrossRef] [PubMed]
- Ucci, A.; Perini, P.; Freyrie, A.; Schreve, M.A.; Ünlü, Ç.; Huizing, E.; van den Heuvel, D.A.; Kum, S.; Shishehbor, M.H.; Ferraresi, R. Endovascular and Surgical Venous Arterialization for No-Option Patients with Chronic Limb-Threatening Ischemia: A Systematic Review and Meta-Analysis. J. Endovasc. Ther. 2023; Online ahead of print. [Google Scholar] [CrossRef]
- Mohammad Hassan, M.; Shahnaz, S.; Samir, H.; Fateh, B. Methodological quality and synthesis of case series and case reports. BMJ Evid.-Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef]
- Ghare, M.I.; Cody Pietras, B.A.; Tirziu, D.; Parise, H.; White, R.; Altin, S.E.; Nagpal, S.; Lansky, A. Outcomes among Patients with Chronic Critical Limb Ischemia with No Revascularization Option: Systematic Review and Meta-Analysis. J. Crit. Limb Ischem. 2021, 1, E85–E92. [Google Scholar]
- Cangiano, G.; Corvino, F.; Giurazza, F.; De Feo, E.M.; Fico, F.; Palumbo, V.; Amodio, F.; Silvestre, M.; Corvino, A.; Niola, R. Percutaneous Deep Foot Vein Arterialization IVUS-Guided in No-Option Critical Limb Ischemia Diabetic Patients. Vasc. Endovasc. Surg. 2021, 55, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Yunir, E.; Wisman, B.A.; Antono, D.; Mansjoer, A.; Sarumpaet, A.; Iswati, E.; Rosana, M.; Tahapary, D.L.; Tarigan, T.J.E.; Soewondo, P. Factors Affecting Mortality of Critical Limb Ischemia 1 Year after Endovascular Revascularization in Patients with Type 2 Diabetes Mellitus. Rev. Diabet. Stud. 2022, 18, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Kotov, A.; Blasche, D.A.; Peters, F.; Pospiech, P.; Rother, U.; Stavroulakis, K.; Remig, J.; Schmidt-Lauber, C.; Zeller, T.; Görtz, H.; et al. The Impact of Chronic Kidney Disease on Mid-Term Outcomes after Revascularisation of Peripheral Arterial Occlusive Disease: Results from a Prospective Cohort Study. J. Clin. Med. 2022, 11, 4750. [Google Scholar] [CrossRef] [PubMed]
- Janiaud, P.; Agarwal, A.; Tzoulaki, I.; Theodoratou, E.; Tsilidis, K.K.; Evangelou, E.; Ioannidis, J.P.A. Validity of Observational Evidence on Putative Risk and Protective Factors: Appraisal of 3744 Meta-analyses on 57 Topics. BMC Med. 2021, 19, 157. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Study Design | No. of Patients | Follow-Up ± SD (Months) | Mean Age ± SD (Years) | Rutherford Class 5/6 | Outcomes |
|---|---|---|---|---|---|---|---|---|
| Shishehbor et al. [10] | 2023 | United States | Prospective observational | 105 | 6 ± 0 | 69.29 ± 10.13 | 68/37 | Technical and procedural success, limb salvage at 30 days and 6 months, overall survival and AFS at 6 months, MALEs, wound healing, reintervention |
| Miranda et al. [15] | 2022 | United States | Prospective observational | 21 | 7.13 ± 2.32 | 68.14 ± 5.29 | 12/9 | Technical success; limb salvage at 6 months and 1 year; overall survival at 30 days, 6 months and 1 year; MALEs; wound healing; reintervention |
| Clair et al. [22] | 2021 | United States | Prospective observational | 32 | 13.9 ± 10.05 | 71 ± 14 | 28/4 | Technical and procedural success; limb salvage, overall survival and AFS at 30 days, 6 months and 1 year; wound healing; reintervention |
| Nakama et al. [11] | 2021 | Japan | Retrospective observational | 18 | 7.94 ± 4.84 | 75.5 ± 8.5 | 6/12 | Technical and procedural success; limb salvage, overall survival and AFS at 30 days, 6 months and 1 year; MALEs; wound healing |
| Schmidt et al. [14] | 2020 | The Netherlands, Germany, France, Singapore | Retrospective observational | 32 | 35.26 ± 11.37 | 67 ± 14 | 23/9 | Technical success, limb salvage, overall survival and AFS at 30 days, 6 months and 1 year; wound healing; reintervention |
| Patient Characteristics | No. of Studies | No. of Patients (%) |
|---|---|---|
| Male gender | 5 | 143 (69) |
| History of smoking | 4 | 93 (45) |
| Diabetes mellitus | 5 | 156 (75) |
| Hypertension | 5 | 186 (89) |
| Chronic kidney disease | 5 | 97 (47) |
| Rutherford classification | 5 | |
| 5 | 137 (66) | |
| 6 | 71 (34) | |
| WIfI * score | 4 | |
| 0 | 0 (0) | |
| 1 | 10 (5) | |
| 2 | 25 (12) | |
| 3 | 67 (32) |
| Shishehbor, 2023 [10] | Miranda, 2022 [15] | Clair, 2021 [22] | Nakama, 2021 [11] | Schmidt, 2020 [14] | |
|---|---|---|---|---|---|
| 1. A clearly stated aim | 2 | 2 | 2 | 2 | 2 |
| 2. Inclusion of consecutive patients | 2 | 2 | 2 | 2 | 2 |
| 3. Prospective collection of data | 2 | 2 | 2 | 1 | 1 |
| 4. Endpoints appropriate to the aim of the study | 2 | 2 | 2 | 2 | 2 |
| 5. Unbiased assessment of the study endpoint | 0 | 0 | 0 | 0 | 0 |
| 6. Follow-up period appropriate to the aim of the study | 2 | 2 | 2 | 2 | 2 |
| 7. Loss to follow up less than 5% | 2 | 0 | 1 | 2 | 2 |
| 8. Prospective calculation of the study size | 1 | 1 | 1 | 1 | 1 |
| 9. Additional criteria in the case of comparative study | |||||
| 10. An adequate control group | NA | NA | NA | NA | NA |
| 11. Contemporary groups | NA | NA | NA | NA | NA |
| 12. Baseline equivalence of groups | NA | NA | NA | NA | NA |
| 13. Adequate statistical analyses | NA | NA | NA | NA | NA |
| MINORS total score | 13 | 11 | 12 | 12 | 12 |
| Outcome | No. of Estimates | Summary Rate (95% CI) | Z-Value | |
|---|---|---|---|---|
| Procedural success | 3 | 0.740 (0.665–0.803) | 5.666 | 0.00% (0.409) |
| 30-day overall survival | 4 | 0.961 (0.894–0.986) | 5.868 | 0.00% (0.763) |
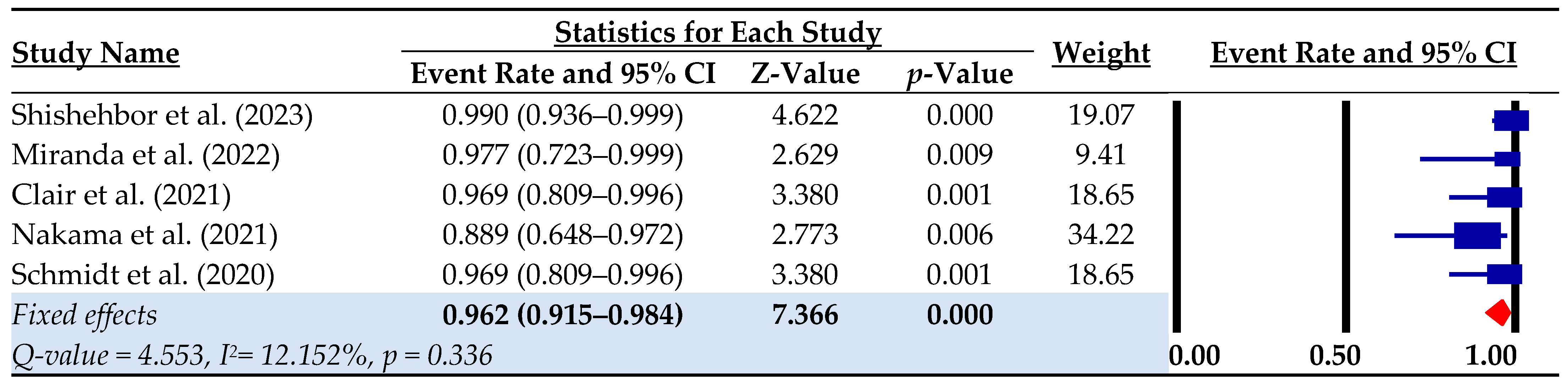
| 6-month overall survival | 5 | 0.900 (0.850–0.934) | 9.360 | 0.00% (0.872) |
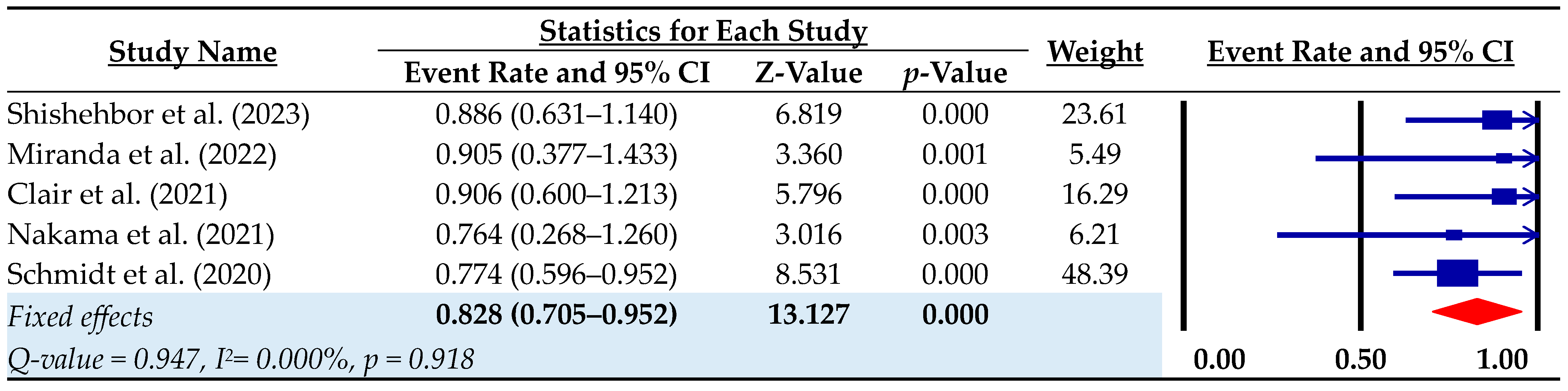
| 1-year overall survival | 4 | 0.851 (0.765–0.909) | 6.098 | 0.00% (0.543) |
| 30-day limb salvage | 4 | 0.904 (0.850–0.941) | 8.551 | 34.57% (0.205) |
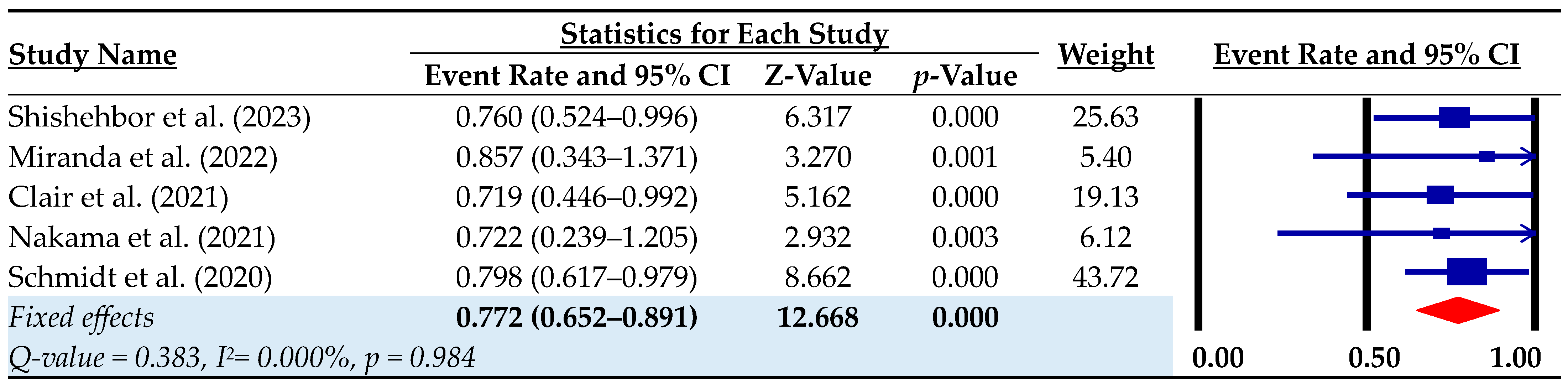
| 6-month limb salvage | 5 | 0.771 (0.708–0.824) | 7.238 | 0.00% (0.508) |
| 1-year limb salvage | 4 | 0.767 (0.674–0.840) | 5.026 | 0.00% (0.633) |
| 30-day amputation-free survival | 3 | 0.878 (0.780–0.936) | 5.453 | 31.76% (0.231) |
| 6-month amputation-free survival | 4 | 0.687 (0.616–0.751) | 4.884 | 44.20% (0.146) |
| 1-year amputation-free survival | 3 | 0.656 (0.545–0.752) | 2.722 | 25.97% (0.259) |
| Primary patency | 2 | 0.308 (0.218–0.397) | 6.714 | 0.00% (0.360) |
| Primary assisted patency * | 1 | – | – | – |
| Secondary patency * | 1 | – | – | – |
| Change in Rutherford class * | 1 | – | – | – |
| MALE during follow-up | 3 | 0.537 (0.373–0.700) | 6.423 | 0.00% (0.760) |
| MACE during follow-up * | 1 | – | – | – |
| Complete wound healing during follow-up | 5 | 0.534 (0.303–0.765) | 4.529 | 78.53% (0.001) |
| Reintervention during follow-up | 4 | 0.467 (0.371–0.563) | 9.568 | 45.95% (0.136) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roustazadeh, R.; Gombert, A.; Krabbe, J.; Jacobs, M.; Doukas, P. Short-Term Outcomes and Efficacy of Percutaneous Deep Vein Arterialization for No-Option Critical Limb Ischemia: A Systematic Review and Meta-Analysis. Biomedicines 2024, 12, 318. https://doi.org/10.3390/biomedicines12020318
Roustazadeh R, Gombert A, Krabbe J, Jacobs M, Doukas P. Short-Term Outcomes and Efficacy of Percutaneous Deep Vein Arterialization for No-Option Critical Limb Ischemia: A Systematic Review and Meta-Analysis. Biomedicines. 2024; 12(2):318. https://doi.org/10.3390/biomedicines12020318
Chicago/Turabian StyleRoustazadeh, Roshanak, Alexander Gombert, Julia Krabbe, Michael Jacobs, and Panagiotis Doukas. 2024. "Short-Term Outcomes and Efficacy of Percutaneous Deep Vein Arterialization for No-Option Critical Limb Ischemia: A Systematic Review and Meta-Analysis" Biomedicines 12, no. 2: 318. https://doi.org/10.3390/biomedicines12020318