
The Impact of Clinical Prognosis of Viral Hepatitis in Head and Neck Cancer Patients Receiving Concurrent Chemoradiotherapy
 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
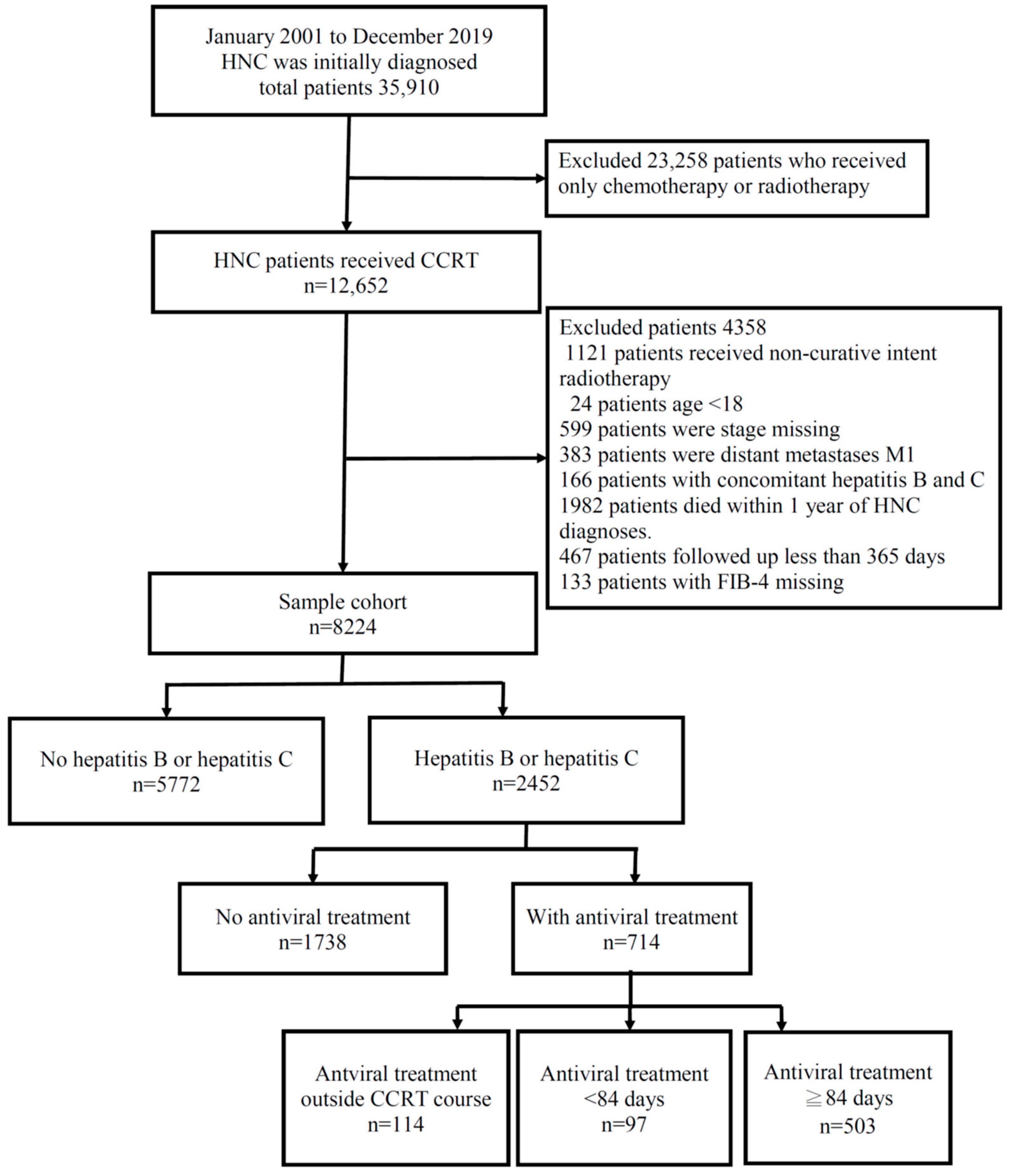
2.1. Patient Recruitment
2.2. Study Design and Subjects
2.3. Treatment
2.4. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of Patients Diagnosed with HNC
3.2. Univariate and Multivariate Analyses of Predictive Variables for HNC Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mei, M.; Chen, Y.H.; Meng, T.; Qu, L.H.; Zhang, Z.Y.; Zhang, X. Comparative efficacy and safety of radiotherapy/cetuximab versus radiotherapy/chemotherapy for locally advanced head and neck squamous cell carcinoma patients: A systematic review of published, primarily non-randomized, data. Ther. Adv. Med. Oncol. 2020, 12, 1758835920975355. [Google Scholar] [CrossRef] [PubMed]
- Chow, L.Q.M. Head and Neck Cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef] [PubMed]
- Sindhu, S.K.; Bauman, J.E. Current Concepts in Chemotherapy for Head and Neck Cancer. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Lazzari, G.; De Cillis, M.A.; Buccoliero, G.; Silvano, G. Competing Morbidities In Advanced Head And Neck Squamous Cell Carcinoma Concurrent Chemoradiotherapy: A Strong Implication Of A Multidisciplinary Team Approach. Cancer Manag. Res. 2019, 11, 9771–9782. [Google Scholar] [CrossRef] [PubMed]
- Ganem, D.; Prince, A.M. Hepatitis B virus infection—Natural history and clinical consequences. N. Engl. J. Med. 2004, 350, 1118–1129. [Google Scholar] [CrossRef]
- Lok, A.S.; Lai, C.L.; Wu, P.C.; Wong, V.C.; Yeoh, E.K.; Lin, H.J. Hepatitis B virus infection in Chinese families in Hong Kong. Am. J. Epidemiol. 1987, 126, 492–499. [Google Scholar] [CrossRef]
- Paul, S.; Saxena, A.; Terrin, N.; Viveiros, K.; Balk, E.M.; Wong, J.B. Hepatitis B Virus Reactivation and Prophylaxis During Solid Tumor Chemotherapy: A Systematic Review and Meta-analysis. Ann. Intern. Med. 2016, 164, 30–40. [Google Scholar] [CrossRef]
- Li, Y.R.; Chen, W.C.; Tsai, W.L.; Cheng, J.S.; Tsay, F.W.; Kao, S.S.; Chen, H.C.; Hsu, P.I. Severe acute exacerbation of HCV infection in cancer patients who undergo chemotherapy without antiviral prophylaxis. J. Viral Hepat. 2020, 27, 873–879. [Google Scholar] [CrossRef]
- Lok, A.S.; McMahon, B.J. Chronic hepatitis B: Update 2009. Hepatology 2009, 50, 661–662. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of chronic hepatitis B. J. Hepatol. 2009, 50, 227–242. [Google Scholar] [CrossRef]
- Chen, W.C.; Cheng, J.S.; Chiang, P.H.; Tsay, F.W.; Chan, H.H.; Chang, H.W.; Yu, H.C.; Tsai, W.L.; Lai, K.H.; Hsu, P.I. A Comparison of Entecavir and Lamivudine for the Prophylaxis of Hepatitis B Virus Reactivation in Solid Tumor Patients Undergoing Systemic Cytotoxic Chemotherapy. PLoS ONE 2015, 10, e0131545. [Google Scholar] [CrossRef] [PubMed]
- Jang, T.Y.; Liang, P.C.; Liu, T.W.; Wei, Y.J.; Yeh, M.L.; Hsu, C.T.; Hsu, P.Y.; Lin, Y.H.; Hsieh, M.H.; Huang, C.I.; et al. Genotype distribution, clinical characteristics, and racial differences observed in chronic hepatitis C patients in Pingtung, Taiwan. J. Chin. Med. Assoc. 2021, 84, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.L.; Kao, J.H. Perspectives and control of hepatitis B virus infection in Taiwan. J. Formos. Med. Assoc. 2015, 114, 901–909. [Google Scholar] [CrossRef]
- Yu, M.L.; Chen, P.J.; Dai, C.Y.; Hu, T.H.; Huang, C.F.; Huang, Y.H.; Hung, C.H.; Lin, C.Y.; Liu, C.H.; Liu, C.J.; et al. 2020 Taiwan consensus statement on the management of hepatitis C: Part (I) general population. J. Formos. Med. Assoc. 2020, 119, 1019–1040. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H. Comparative study on three algorithms of the ICD-10 Charlson comorbidity index with myocardial infarction patients. J. Prev. Med. Public Health 2010, 43, 42–49. [Google Scholar] [CrossRef]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef]
- Torres, H.A.; Davila, M. Reactivation of hepatitis B virus and hepatitis C virus in patients with cancer. Nat. Rev. Clin. Oncol. 2012, 9, 156–166. [Google Scholar] [CrossRef]
- Torres, H.A.; Hosry, J.; Mahale, P.; Economides, M.P.; Jiang, Y.; Lok, A.S. Hepatitis C virus reactivation in patients receiving cancer treatment: A prospective observational study. Hepatology 2018, 67, 36–47. [Google Scholar] [CrossRef]
- Hwang, J.P.; Somerfield, M.R.; Alston-Johnson, D.E.; Cryer, D.R.; Feld, J.J.; Kramer, B.S.; Sabichi, A.L.; Wong, S.L.; Artz, A.S. Hepatitis B Virus Screening for Patients With Cancer Before Therapy: American Society of Clinical Oncology Provisional Clinical Opinion Update. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 2212–2220. [Google Scholar] [CrossRef]
- Zheng, S.H.; Zhou, S.; Wang, G.N.; Huang, Z.L.; Liu, S.R.; Chen, C.; Tao, Y.L.; Chang, H.; Ding, S.R.; Liao, R.N.; et al. Prognostic value of hepatitis B viral infection in patients with nasopharyngeal carcinoma in the intensity-modulated radiotherapy era. Transl. Cancer Res. 2021, 10, 4624–4635. [Google Scholar] [CrossRef] [PubMed]
- Nobles, J.; Wold, C.; Fazekas-May, M.; Gilbert, J.; Friedlander, P.L. Prevalence and epidemiology of hepatitis C virus in patients with squamous cell carcinoma of the head and neck. Laryngoscope 2004, 114, 2119–2122. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.; Shang, Z. Burden of oral cancer in Asia from 1990 to 2019: Estimates from the Global Burden of Disease 2019 study. PLoS ONE 2022, 17, e0265950. [Google Scholar] [CrossRef] [PubMed]
- Weng, J.J.; Wei, J.Z.; Li, M.; Lu, J.L.; Qin, Y.D.; Jiang, H.; Qu, S.H. Effects of hepatitis B virus infection and antiviral therapy on the clinical prognosis of nasopharyngeal carcinoma. Cancer Med. 2020, 9, 541–551. [Google Scholar] [CrossRef]
- Shih, C.A.; Chen, W.C.; Yu, H.C.; Cheng, J.S.; Lai, K.H.; Hsu, J.T.; Chen, H.C.; Hsu, P.I. Risk of Severe Acute Exacerbation of Chronic HBV Infection Cancer Patients Who Underwent Chemotherapy and Did Not Receive Anti-Viral Prophylaxis. PLoS ONE 2015, 10, e0132426. [Google Scholar] [CrossRef]
- Li, Y.R.; Hu, T.H.; Chen, W.C.; Hsu, P.I.; Chen, H.C. Screening and prevention of hepatitis C virus reactivation during chemotherapy. World J. Gastroenterol. 2021, 27, 5181–5188. [Google Scholar] [CrossRef]
- Zhang, C.; Wu, J.; Xu, J.; Xu, J.; Xian, J.; Xue, S.; Ye, J. Association between Aspartate Aminotransferase-to-Platelet Ratio Index and Hepatocellular Carcinoma Risk in Patients with Chronic Hepatitis: A Meta-Analysis of Cohort Study. Dis. Markers 2019, 2019, 2046825. [Google Scholar] [CrossRef]
- Zhang, Y.; Wang, R.; Yang, X. FIB-4 index serves as a noninvasive prognostic biomarker in patients with hepatocellular carcinoma: A meta-analysis. Medicine 2018, 97, e13696. [Google Scholar] [CrossRef]
- Xu, K.; Shi, M.; Zhang, W.; Shi, Y.; Dong, Q.; Shen, X.; Chen, X.; Lin, J. Preoperative Fibrosis-4 (FIB-4) Evaluation May Be Helpful to Evaluate Prognosis of Gastric Cancer Patients Undergoing Operation: A Retrospective Study. Front. Oncol. 2021, 11, 655343. [Google Scholar] [CrossRef]
- Chang, K.P.; Lee, C.C.; Su, Y.C.; Han, M.L.; Kung, T.H.; Chang, H.J. Correlation between liver cirrhosis and risk of death from oral cancer: Taiwan cohort study. J. Laryngol. Otol. 2016, 130, 565–570. [Google Scholar] [CrossRef]
- Pinter, M.; Trauner, M.; Peck-Radosavljevic, M.; Sieghart, W. Cancer and liver cirrhosis: Implications on prognosis and management. ESMO Open 2016, 1, e000042. [Google Scholar] [CrossRef] [PubMed]
- Boje, C.R.; Dalton, S.O.; Primdahl, H.; Kristensen, C.A.; Andersen, E.; Johansen, J.; Andersen, L.J.; Overgaard, J. Evaluation of comorbidity in 9388 head and neck cancer patients: A national cohort study from the DAHANCA database. Radiother. Oncol. 2014, 110, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.J.; Kim, D.Y.; Lee, J.H.; Roh, J.L.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Prognostic value of total tumor volume in advanced-stage laryngeal and hypopharyngeal carcinoma. J. Surg. Oncol. 2013, 108, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.T.; Chiu, T.J.; Huang, T.L.; Chien, C.Y.; Fang, F.M. Impact of comorbidity on survival for locally advanced head and neck cancer patients treated by radiotherapy or radiotherapy plus chemotherapy. Chang Gung Med. J. 2010, 33, 283–291. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total Patient n = 8224 | No Hepatitis B or C n = 5772 | Hepatitis B or C without Antiviral Treatment in CCRT Course n = 1852 | Hepatitis B or C with Antiviral Treatment in CCRT Course n = 600 | p-Value |
|---|---|---|---|---|---|
| Age | |||||
| <52 y/o | 4037 | 2808 (48.7%) | 888 (48.0%) | 341 (56.8%) | 0.0004 |
| ≥52 y/o | 4187 | 2964 (51.4%) | 964 (52.1%) | 259 (43.2%) | |
| Gender | |||||
| Male | 7243 | 5021 (87.0%) | 1683 (90.1%) | 539 (89.8%) | <0.0001 |
| Female | 981 | 751 (13.0%) | 169 (9.1%) | 61 (10.2%) | |
| Primary site | |||||
| Oral | 2599 | 1848 (30.0%) | 661 (33.0%) | 140 (23.3%) | <0.0001 |
| Oropharynx | 1321 | 881 (15.3%) | 349 (18.8%) | 91 (15.2%) | |
| Hypopharynx | 1111 | 741 (12.8%) | 274 (14.8%) | 96 (16.0%) | |
| Larynx | 498 | 342 (5.9%) | 126 (6.8%) | 30 (5%) | |
| Others | 2695 | 1960 (34.0%) | 492 (26.6%) | 243 (40.5%) | |
| T stage | |||||
| 1 | 1152 | 783 (13.6%) | 270 (14.6%) | 99 (16.5%) | 0.0688 |
| 2 | 2129 | 1505 (26.1%) | 468 (25.3%) | 156 (26.0%) | |
| 3 | 1428 | 977 (16.9%) | 332 (17.9%) | 119 (19.8%) | |
| 4 | 3515 | 2507 (43.4%) | 782 (42.2%) | 226 (37.7%) | |
| N stage | |||||
| 0 | 1748 | 1201 (20.8%) | 436 (23.5%) | 111 (18.5%) | 0.0022 |
| 1 | 1899 | 1349 (23.4%) | 403 (21.8%) | 147 (24.5%) | |
| 2 | 3712 | 2618 (45.4%) | 838 (45.3%) | 256 (42.7%) | |
| 3 | 865 | 604 (10.5%) | 175 (9.5%) | 86 (14.3%) | |
| AJCC stage of cancer | |||||
| I and II | 1415 | 981 (17.0%) | 328 (17.7%) | 106 (17.7%) | 0.6332 |
| III | 1631 | 1140 (19.8%) | 377 (20.4%) | 114 (19.0%) | |
| IVA | 3825 | 2686 (46.5%) | 867 (46.8%) | 272 (45.3%) | |
| IVB | 1353 | 965 (16.7%) | 280 (15.1%) | 108 (18.0%) | |
| CCI | |||||
| 0–5 | 8143 | 5743 (99.5%) | 1808 (97.6%) | 592 (98.7%) | <0.0001 |
| ≥6 | 81 | 29 (0.5%) | 44 (2.38%) | 8 (1.3%) | |
| APRI score | |||||
| <2 | 8124 | 5751 (99.6%) | 1790 (96.7%) | 583 (97.2%) | <0.0001 |
| ≥2 | 100 | 21 (0.4%) | 62 (3.4%) | 17 (2.8%) | |
| FIB-4 score | |||||
| <3.25 | 7869 | 5651 (97.9%) | 1664 (89.9%) | 554 (92.3%) | <0.0001 |
| ≥3.25 | 355 | 121 (2.1%) | 188 (10.1%) | 46 (7.7%) | |
| Variables | Total Patient n = 8224 | Hazard Ratio | |||
|---|---|---|---|---|---|
| Univariates | p-Value | Multivariates | p-Value | ||
| Age | |||||
| <52 y/o | 4037 | Ref. | <0.0001 | Ref. | 0.0982 |
| ≥52 y/o | 4187 | 1.19 (1.11–1.28) | 1.06 (0.99–1.15) | ||
| Gender | |||||
| Male | 7243 | Ref. | <0.0001 | Ref. | <0.0001 |
| Female | 981 | 0.46 (0.40–0.53) | 0.64 (0.55–0.75) | ||
| Primary site | |||||
| Oral | 2599 | Ref. | Ref. | ||
| Oropharynx | 1321 | 1.11 (1.00–1.23) | 0.0491 | 1.11 (1.00–1.23) | 0.0554 |
| Hypopharynx | 1111 | 1.32 (1.19–1.47) | <0.0001 | 1.25 (1.13–1.39) | <0.0001 |
| Larynx | 498 | 0.93 (0.80–1.09) | 0.394 | 1.08 (0.92–1.26) | 0.360 |
| Others | 2695 | 0.46 (0.41–0.51) | <0.0001 | 0.57 (0.52–0.64) | <0.0001 |
| T stage | |||||
| 1 | 1152 | Ref. | Ref. | ||
| 2 | 2129 | 1.67 (1.43–1.94) | <0.0001 | 1.30 (1.12–1.52) | 0.008 |
| 3 | 1428 | 1.98 (1.70–2.32) | <0.0001 | 1.66 (1.42–1.95) | <0.001 |
| 4 | 3515 | 2.77 (2.41–3.18) | <0.0001 | 2.06 (1.78–2.39) | <0.001 |
| N stage | |||||
| 0 | 1748 | Ref. | Ref. | ||
| 1 | 1899 | 0.73 (0.64-.082) | <0.0001 | 1.00 (0.88–1.13) | 0.9763 |
| 2 | 3712 | 1.28 (1.16–1.41) | <0.0001 | 1.31 (1.19–1.45) | <0.0001 |
| 3 | 865 | 1.47 (1.28–1.68) | <0.0001 | 2.09 (1.81–2.40) | <0.0001 |
| AJCC stage of cancer | |||||
| I and II | 1415 | Ref. | Ref. | ||
| III | 1631 | 1.20 (1.03–1.39) | 0.0177 | 1.22 (1.06–1.42) | 0.0075 |
| IVA | 3825 | 2.19 (1.93–2.47) | <0.0001 | 1.73 (1.53–1.96) | <0.0001 |
| IVB | 1353 | 2.80 (2.44–3.22) | <0.0001 | 2.53 (2.20–2.90) | <0.0001 |
| CCI | |||||
| 0–5 | 8143 | Ref. | <0.0001 | Ref. | <0.0001 |
| ≥6 | 81 | 2.19 (1.62–2.97) | 2.18 (1.61–2.95) | ||
| APRI score | |||||
| <2 | 8124 | Ref. | 0.0002 | Ref. | 0.0044 |
| ≥2 | 100 | 1.68 (1.28–2.21) | 1.49 (1.13–1.97) | ||
| FIB-4 score | |||||
| <3.25 | 7869 | Ref. | <0.0001 | Ref. | <0.0001 |
| ≥3.25 | 355 | 2.04 (1.77–2.36) | 1.82 (1.57–2.11) | ||
| Viral hepatitis | |||||
| No viral hepatitis | 5772 | Ref. | Ref. | ||
| Viral hepatitis without antiviral treatment in CCRT course | 1852 | 1.02 (0.94–1.11) | 0.638 | 0.90 (0.92–0.98) | 0.0172 |
| Viral hepatitis with antiviral treatment in CCRT course | 600 | 0.90 (0.78–1.05) | 0.196 | 0.90 (0.78–1.05) | 0.194 |
| Variables | Total Patient n = 2452 | Hazard Ratio | |||
|---|---|---|---|---|---|
| Univariates | p-Value | Multivariate | p-Value | ||
| Age | |||||
| <52 y/o | 1129 | Ref. | 0.0947 | Ref. | 0.627 |
| ≥52 y/o | 1153 | 1.12 (0.98–1.28) | 1.03 (0.90–1.18) | ||
| Gender | |||||
| Male | 2222 | Ref. | <0.0001 | Ref. | 0.0159 |
| Female | 230 | 0.44 (0.32–0.60) | 0.67 (0.49–0.93) | ||
| Primary site | |||||
| Oral | 751 | Ref. | Ref. | ||
| Oropharynx | 440 | 1.18 (0.98–1.41) | 0.0832 | 1.18 (0.98–1.42) | 0.0768 |
| Hypopharynx | 370 | 1.54 (1.28–1.86) | <0.0001 | 1.57 (1.30–1.89) | <0.0001 |
| Larynx | 156 | 1.05 (0.79–1.39) | 0.7324 | 1.20 (0.91–1.60) | 0.1995 |
| Others | 735 | 0.48 (0.39–0.58) | <0.0001 | 0.60 (0.48–0.74) | <0.0001 |
| T stage | |||||
| 1 | 369 | Ref. | Ref. | ||
| 2 | 624 | 1.52 (1.17–1.98) | 0.0016 | 1.12 (0.86–1.47) | 0.4046 |
| 3 | 451 | 1.99 (1.53–2.60) | <0.0001 | 1.60 (1.22–2.09) | 0.0007 |
| 4 | 1008 | 2.43 (1.91–3.09) | <0.0001 | 1.82 (1.41–2.33) | <0.001 |
| N stage | |||||
| 0 | 547 | Ref. | Ref. | ||
| 1 | 550 | 0.72 (0.58–0.90) | 0.0040 | 0.98 (0.78–1.23) | 0.8698 |
| 2 | 1094 | 1.27 (1.07–1.50) | 0.0072 | 1.31 (1.10–1.56) | 0.0025 |
| 3 | 261 | 1.66 (1.30–2.11) | <0.0001 | 2.30 (1.80–2.95) | <0.0001 |
| AJCC stage of cancer | |||||
| I and II | 434 | Ref. | Ref. | ||
| III | 491 | 1.27 (0.97–1.65) | 0.0778 | 1.27 (0.98–1.66) | 0.0729 |
| IVA | 1139 | 2.19 (1.75–2.72) | <0.0001 | 1.79 (1.43–2.24) | <0.0001 |
| IVB | 388 | 2.87 (2.44–3.68) | <0.0001 | 2.73 (2.12–3.51) | <0.0001 |
| CCI | |||||
| 0–5 | 2400 | Ref. | 0.0008 | Ref. | 0.0028 |
| ≥6 | 52 | 1.96 (1.32–2.89) | 1.83 (1.23–2.71) | ||
| APRI score | |||||
| <2 | 2373 | Ref. | 0.0001 | Ref. | 0.0013 |
| ≥2 | 79 | 1.83 (1.35–2.46) | 1.65 (1.22–2.23) | ||
| FIB-4 score | |||||
| <3.25 | 2218 | Ref. | <0.0001 | Ref. | <0.0001 |
| ≥3.25 | 234 | 2.12 (1.76–2.54) | 1.84 (1.52–2.21) | ||
| Viral hepatitis | |||||
| Viral hepatitis without antiviral treatment in CCRT course | 1852 | Ref. | Ref. | ||
| Viral hepatitis with antiviral treatment < 84 days in CCRT course | 97 | 0.91 (0.65–1.29) | 0.598 | 1.07 (0.76–1.51) | 0.6977 |
| Viral hepatitis with antiviral treatment ≥ 84 days in CCRT course | 503 | 0.88 (0.74–1.06) | 0.1723 | 0.96 (0.80–1.15) | 0.6804 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Y.-M.; Luo, S.-D.; Wu, C.-N.; Wu, S.-C.; Chen, W.-C.; Yang, Y.-H.; Chiu, T.-J. The Impact of Clinical Prognosis of Viral Hepatitis in Head and Neck Cancer Patients Receiving Concurrent Chemoradiotherapy. Biomedicines 2023, 11, 2946. https://doi.org/10.3390/biomedicines11112946
Wang Y-M, Luo S-D, Wu C-N, Wu S-C, Chen W-C, Yang Y-H, Chiu T-J. The Impact of Clinical Prognosis of Viral Hepatitis in Head and Neck Cancer Patients Receiving Concurrent Chemoradiotherapy. Biomedicines. 2023; 11(11):2946. https://doi.org/10.3390/biomedicines11112946
Chicago/Turabian StyleWang, Yu-Ming, Sheng-Dean Luo, Ching-Nung Wu, Shao-Chun Wu, Wei-Chih Chen, Yao-Hsu Yang, and Tai-Jan Chiu. 2023. "The Impact of Clinical Prognosis of Viral Hepatitis in Head and Neck Cancer Patients Receiving Concurrent Chemoradiotherapy" Biomedicines 11, no. 11: 2946. https://doi.org/10.3390/biomedicines11112946