
Is the Development of Ascites in Alcoholic Liver Patients Influenced by Specific KIR/HLA Gene Profiles?

 ,
,  ,
, 
Abstract
:1. Introduction
2. Patients and Methods
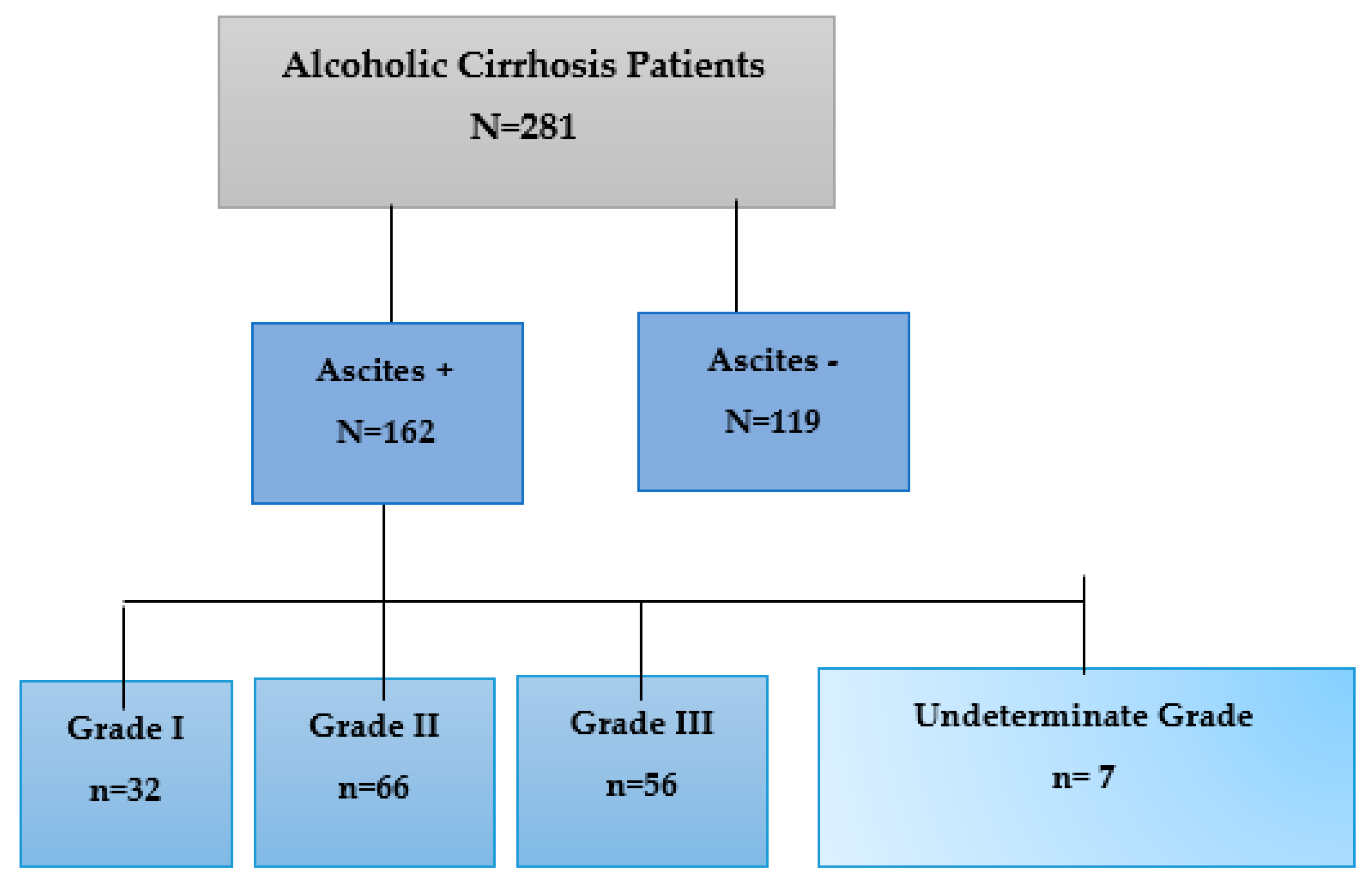
2.1. Patient Enrollment
2.2. Diagnostic Criteria of Alcohol Cirrhosis
2.3. Ascites Diagnosis
2.4. Biochemical Parameters Analyzed in AC Patients with and without Ascites
2.5. KIR and HLA Typing
2.6. Statistical Analysis
3. Results
3.1. Sociodemographic and Clinical Characteristics
3.2. Biochemical Characteristics of the AC Patient with and without Ascites
3.3. Analysis of KIR Genes in AC Patients with and without Ascites
3.3.1. Analysis of the Inhibitory KIR (iKIR) Gene Frequencies in AC Patients with and without Ascites
3.3.2. Analysis of the Frequencies of aKIR Genes in AC Patients with and without Ascites
3.4. Analysis of KIR Genes in AC Patients with Different Ascites Degrees
3.4.1. Analysis of the Frequencies of iKIR Genes in AC Patients with Different Ascites Degrees
3.4.2. Analysis of the Frequencies of aKIR Genes in AC Patients with Different Degrees of Ascites
3.5. Analysis of the Frequency of Epitopes and HLA-C Genotypes in AC Patients with Different Degrees of Ascites
3.6. Analysis of KIR Gene Combinations and Their Corresponding HLA-C Ligands
Analysis of KIR Genotypes and Their HLA-C Ligands in AC Patients with Ascites
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anstee, Q.M.; Seth, D.; Day, C.P. Genetic Factors That Affect Risk of Alcoholic and Nonalcoholic Fatty Liver Disease. Gastroenterology 2016, 150, 1728.e7–1744.e7. [Google Scholar] [CrossRef] [PubMed]
- Arroyo, V. Pathophysiology, diagnosis and treatment of ascites in cirrhosis. Ann. Hepatol. 2002, 1, 72–79. [Google Scholar] [CrossRef]
- Arroyo, V.; Gines, P.; Gerbes, A.L.; Dudley, F.J.; Gentilini, P.; Laffi, G.; Reynolds, T.B.; Ring-Larsen, H.; Schölmerich, J. Special Article Definition and Diagnostic Criteria of Refractory Ascites and Hepatorenal Syndrome in Cirrhosis. Hepatology 1996, 23, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Bamias, A.; Tsiatas, M.; Kafantari, E.; Liakou, C.; Rodolakis, A.; Voulgaris, Z.; Vlahos, G.; Papageorgiou, T.; Tsitsilonis, O.; Bamia, C.; et al. Significant differences of lymphocytes isolated from ascites of patients with ovarian cancer compared to blood and tumor lymphocytes. Association of CD3+CD56+ cells with platinum resistance. Gynecol. Oncol. 2007, 106, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Bamias, A.; Koutsoukou, V.; Terpos, E.; Tsiatas, M.L.; Liakos, C.; Tsitsilonis, O.; Rodolakis, A.; Voulgaris, Z.; Vlahos, G.; Papageorgiou, T.; et al. Correlation of NK T-like CD3+CD56+ cells and CD4+CD25+(hi) regulatory T cells with VEGF and TNFα in ascites from advanced ovarian cancer: Association with platinum resistance and prognosis in patients receiving first-line, platinum-based chemotherapy. Gynecol. Oncol. 2008, 108, 421–427. [Google Scholar] [CrossRef]
- Barquera, R.; Zuñiga, J. Consortium for the Analysis of the Diversity and Evolution of Latinamerica View Project Immunogenetic Characterization of Central American Populations View Project. 2008. Available online: www.iner.gob.mx (accessed on 26 January 2023).
- Ursu, L.; Calenic, B.; Diculescu, M.; Dima, A.; Constantinescu, I. HLA Alleles and KIR Genes in Romanian Patients with Chronic Hepatitis C. J. Gastrointestin. Liver Dis. 2020, 29, 595–601. [Google Scholar] [CrossRef]
- Campillo, J.A.; Legaz, I.; López-Álvarez, M.R.; Bolarín, J.M.; Heras, B.L.; Muro, M.; Minguela, A.; Moya-Quiles, M.R.; Blanco-García, R.; Martínez-Banaclocha, H.; et al. KIR gene variability in cutaneous malignant melanoma: Influence of KIR2D/HLA-C pairings on disease susceptibility and prognosis. Immunogenetics 2013, 65, 333–343. [Google Scholar] [CrossRef]
- Características Clínicas De Los Pacientes Con Cirrosis Internados En El Servicio De Clínica Médica|Revista Argentina De Medicina. (n.d.). Available online: http://www.revistasam.com.ar/index.php/RAM/article/view/261 (accessed on 5 May 2023).
- Cárdenas, A.; Arroyo, V. Mechanisms of water and sodium retention in cirrhosis and the pathogenesis of ascites. Best Pract. Res. Clin. Endocrinol. Metab. 2003, 17, 607–622. [Google Scholar] [CrossRef]
- Cárdenas, A.; Bataller, R.; Arroyo, V. Mechanisms of Ascites Formation. Clin. Liver Dis. 2000, 4, 447–465. [Google Scholar] [CrossRef]
- Choudhary, N.S.; Duseja, A. Genetic and epigenetic disease modifiers: Non-alcoholic fatty liver disease (NAFLD) and alcoholic liver disease (ALD). Transl. Gastroenterol. Hepatol. 2021, 6, 2. [Google Scholar] [CrossRef]
- Chuang, W.-L.; Liu, H.-W.; Chang, W.-Y.; Chen, S.-C.; Hsieh, M.-Y.; Wang, L.-Y. Natural killer cell activity in patients with liver cirrhosis relative to severity of liver damage. Dig. Dis. Sci. 1991, 36, 299–302. [Google Scholar] [CrossRef] [PubMed]
- Colonna, M.; Borsellino, G.; Falco, M.; Ferrara, G.B.; Strominger, J.L. HLA-C is the inhibitory ligand that determines dominant resistance to lysis by NK1- and NK2-specific natural killer cells. Proc. Natl. Acad. Sci. USA 1993, 90, 12000–12004. [Google Scholar] [CrossRef] [PubMed]
- Complications of Cirrhosis, an Issue of Clinics in Liver Disease, E-Book—Google Libros. (n.d.). Available online: https://books.google.es/books?hl=es&lr=&id=84cpEAAAQBAJ&oi=fnd&pg=PP1&dq=At+this+last+stage+of+alcoholic+cirrhosis,+patients+suffer+complications+associated+with+portal+hypertension,+including+ascites,+spontaneous+bacterial+peritonitis+(SBP),+hepatic+encephalopathy+(HE),+hepatorenal+syndrome,+portopulmonary+hypertension,+or+var&ots=_h1hq9PR35&sig=OeTLGYnvRXVFveOP1mnSLnbwSDs#v=onepage&q&f=false (accessed on 5 May 2023).
- Del Campo, J.A.; Gallego-Durán, R.; Gallego, P.; Grande, L. Genetic and Epigenetic Regulation in Nonalcoholic Fatty Liver Disease (NAFLD). Int. J. Mol. Sci. 2018, 19, 911. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Peña, R.; Vidal-Castiñeira, J.R.; Moro-García, M.A.; Alonso-Arias, R.; Castro-Santos, P. Significant association of the KIR2DL3/HLA-C1 genotype with susceptibility to Crohn’s disease. Hum. Immunol. 2016, 77, 104–109. [Google Scholar] [CrossRef]
- Dumitrescu, R.G. Alcohol-induced epigenetic changes in cancer. Methods Mol. Biol. 2018, 1856, 157–172. [Google Scholar]
- EBSCOhost|87336999|Austrian Consensus on the Definition and Treatment of Portal Hypertension and Its Complications (Billroth II). (n.d.). Available online: https://eds.s.ebscohost.com/abstract?site=eds&scope=site&jrnl=00435325&AN=87336999&h=EkZoak1pq0P%2Bc%2B%2FW9MZp0Qm8MgzhuVVLxmJa8%2BhhJcWfTkKznvKSeeY6qBFTuRA0aYj3aRsH6Gu4vhBwbMC90w%3D%3D&crl=c&resultLocal=ErrCrlNoResults&resultNs=Ehost&crlhashurl=login.aspx%3Fdirect%3Dtrue%26profile%3Dehost%26scope%3Dsite%26authtype%3Dcrawler%26jrnl%3D00435325%26AN%3D87336999 (accessed on 5 May 2023).
- Salerno, F.; Angeli, P.; Bernardi, M.; Laffi, G.; Riggio, O.; Salvagnini, M. Clinical practice guidelines for the management of cirrhotic patients with ascites. Committee on Ascites of the Italian Association for the Study of the Liver. Ital. J. Gastroenterol. Hepatol. 1999, 31, 626–634. [Google Scholar]
- Franco, S.; Horneros, J.; Soldevila, L.; Ouchi, D.; Galván-Femenía, I.; de Cid, R.; Tenesa, M.; Bechini, J.; Perez, R.; Llibre, J.M.; et al. Single nucleotide polymorphisms in PNPLA3, ADAR-1 and IFIH1 are associated with advanced liver fibrosis in patients co-infected with HIV-1//hepatitis C virus. AIDS 2021, 35, 2497–2502. [Google Scholar] [CrossRef]
- Gambino, C.M.; Di Bona, D.; Aiello, A.; Carru, C.; Duro, G.; Guggino, G.; Ferrante, A.; Zinellu, A.; Caruso, C.; Candore, G.; et al. HLA-C1 ligands are associated with increased susceptibility to systemic lupus erythematosus. Hum. Immunol. 2018, 79, 172–177. [Google Scholar] [CrossRef]
- Gao, B.; Radaeva, S. Natural killer and natural killer T cells in liver fibrosis. Biochim. Biophys. Acta (BBA)-Mol. Basis Dis. 2013, 1832, 1061–1069. [Google Scholar] [CrossRef]
- García-León, J.A.; Pinto-Medel, M.J.; García-Trujillo, L.; López-Gómez, C.; Oliver-Martos, B.; Prat-Arrojo, I.; Marín-Bañasco, C.; Suardíaz-García, M.; Maldonado-Sanchez, R.; Fernández-Fernández, Ó.; et al. Killer cell immunoglobulin-like receptor genes in Spanish multiple sclerosis patients. Mol. Immunol. 2011, 48, 1896–1902. [Google Scholar] [CrossRef]
- Buey, L.G.; Mateos, F.G.; Moreno-Otero, R. Cirrosis hepática. Med.-Programa Form. Médica Contin. Acreditado 2012, 11, 625–633. [Google Scholar] [CrossRef]
- Ginès, P.; Angeli, P.; Lenz, K.; Møller, S.; Moore, K.; Moreau, R.; Hayes, P. EASL clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. J. Hepatol. 2010, 53, 397–417. [Google Scholar] [CrossRef]
- Gourraud, P.-A.; Meenagh, A.; Cambon-Thomsen, A.; Middleton, D. Linkage disequilibrium organization of the human KIR superlocus: Implications for KIR data analyses. Immunogenetics 2010, 62, 729–740. [Google Scholar] [CrossRef] [PubMed]
- Heidelbaugh, J.J.; Bruderly, M. Cirrhosis and Chronic Liver Failure: Part I. Diagnosis and Evaluation. Am. Fam. Physician 2006, 74, 756–762. [Google Scholar]
- Hiby, S.E.; Apps, R.; Sharkey, A.M.; Farrell, L.E.; Gardner, L.; Mulder, A.; Claas, F.H.; Walker, J.J.; Redman, C.C.; Morgan, L.; et al. Maternal activating KIRs protect against human reproductive failure mediated by fetal HLA-C2. J. Clin. Investig. 2010, 120, 4102–4110. [Google Scholar] [CrossRef]
- Hochreuter, M.Y.; Dall, M.; Treebak, J.T.; Barrès, R. MicroRNAs in non-alcoholic fatty liver disease: Progress and perspectives. Mol. Metab. 2022, 65, 101581. [Google Scholar] [CrossRef]
- Hollenbach, J.A.; Pando, M.J.; Caillier, S.J.; Gourraud, P.A.; Oksenberg, J.R. The killer immunoglobulin-like receptor KIR3DL1 in combination with HLA-Bw4 is protective against multiple sclerosis in African Americans. Genes Immun. 2016, 17, 199–202. [Google Scholar] [CrossRef]
- Hou, W.; Sanyal, A.J. Ascites: Diagnosis and Management. Med. Clin. N. Am. 2009, 93, 801–817. [Google Scholar] [CrossRef]
- Hou, Y.-F.; Zhang, Y.-C.; Jiao, Y.-L.; Wang, L.-C.; Li, J.-F.; Pan, Z.-L.; Yang, Q.-R.; Sun, H.-S.; Zhao, Y.-R. Disparate distribution of activating and inhibitory killer cell immunoglobulin-like receptor genes in patients with systemic lupus erythematosus. Lupus 2010, 19, 20–26. [Google Scholar] [CrossRef]
- Morales Penalva, R. Ascitis y encefalopatía, causas de muerte y supervivencia del paciente por cirrosis alcohólica y su influencia inmunológica. Proy. Investig. 2022. Available online: https://digitum.um.es/digitum/handle/10201/117508 (accessed on 1st August 2023).
- Jeong, W.I.; Park, O.; Gao, B. Abrogation of the Antifibrotic Effects of Natural Killer Cells/Interferon-γ Contributes to Alcohol Acceleration of Liver Fibrosis. Gastroenterology 2008, 134, 248–258. [Google Scholar] [CrossRef]
- Jiao, Y.-L.; Ma, C.-Y.; Wang, L.-C.; Cui, B.; Zhang, J.; You, L.; Chen, Z.-J.; Li, J.-F.; Zhao, Y.-R. Polymorphisms of KIRs gene and HLA-C alleles in patients with ankylosing spondylitis: Possible association with susceptibility to the disease. J. Clin. Immunol. 2008, 28, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Kawaratani, H.; Fukui, H.; Yoshiji, H. Treatment for cirrhotic ascites. Hepatol. Res. 2017, 47, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Khakoo, S.I.; Thio, C.L.; Martin, M.P.; Brooks, C.R.; Gao, X.; Astemborski, J.; Cheng, J.; Goedert, J.J.; Vlahov, D.; Hilgartner, M.; et al. HLA and NK cell inhibitory receptor genes in resolving hepatitis C virus infection. Science 2004, 305, 872–874. [Google Scholar] [CrossRef] [PubMed]
- Legaz, I.; Bolarín, J.M.; Navarro, E.; Campillo, J.A.; Moya, R.; Pérez-Cárceles, M.D.; Luna, A.; Osuna, E.; Miras, M.; Muro, M.; et al. KIR2DL2/S2 and KIR2DS5 in alcoholic cirrhotic patients undergoing liver transplantation. Arch. Med. Sci. 2021, 17, 764–774. [Google Scholar] [CrossRef] [PubMed]
- Legaz, I.; López-Álvarez, M.R.; Campillo, J.A.; Moya-Quiles, M.R.; Bolarín, J.M.; de la Peña, J.; Salgado, G.; Gimeno, L.; García-Alonso, A.M.; Muro, M.; et al. KIR gene mismatching and KIR/C ligands in liver transplantation: Consequences for short-term liver allograft injury. Transplantation 2013, 95, 1037–1044. [Google Scholar] [CrossRef]
- Legaz, I.; Navarro-Noguera, E.; Bolarín, J.M.; García-Alonso, A.M.; Maldonado, A.L.; Mrowiec, A.; Campillo, J.A.; Gimeno, L.; Moya-Quiles, R.; Álvarez-López, M.d.R.; et al. Epidemiology, Evolution, and Long-Term Survival of Alcoholic Cirrhosis Patients Submitted to Liver Transplantation in Southeastern Spain. Alcohol. Clin. Exp. Res. 2016, 40, 794–805. [Google Scholar] [CrossRef]
- Legaz, I.; Noguera, E.N.; Bolarín, J.M.; Campillo, J.A.; Moya, R.; Luna, A.; Miras, M.; Minguela, A.; Álvarez-López, M.R.; Muro, M. Patient Sex in the Setting of Liver Transplant in Alcoholic Liver Disease. Exp. Clin. Transplant. 2018, 17, 355–362. [Google Scholar] [CrossRef]
- Li, J.-T.; Guo, C.; Li, M.-L.; Wei, Y.-Q.; Hou, Y.-F.; Jiao, Y.-L.; Zhao, Y.-R.; Sun, H.; Xu, J.; Cao, M.-F.; et al. Killer Cell Immunoglobulin-Like Receptor Genes and their HLA-C Ligands in Hashimoto Thyroiditis in a Chinese Population. Endocr. Pract. 2016, 22, 935–940. [Google Scholar] [CrossRef]
- Lutz, P.; Jeffery, H.C.; Jones, N.; Birtwistle, J.; Kramer, B.; Nattermann, J.; Spengler, U.; Strassburg, C.P.; Adams, D.H.; Oo, Y.H. NK cells in ascites from liver disease patients display a particular phenotype and take part in antibacterial immune response. Front. Immunol. 2019, 10, 462029. [Google Scholar] [CrossRef]
- Maclaren, R. Management of Cirrhosis and Associated Complications Learning Objectives. J. Pharm. Pract. 2009, 22, 290–309. [Google Scholar] [CrossRef]
- Mahmoudi, M.; Fallahian, F.; Sobhani, S.; Ghoroghi, S.; Jamshidi, A.; Poursani, S.; Dolati, M.; Hosseinpour, Z.; Gharibdoost, F. Analysis of killer cell immunoglobulin-like receptors (KIRs) and their HLA ligand genes polymorphisms in Iranian patients with systemic sclerosis. Clin. Rheumatol. 2017, 36, 853–862. [Google Scholar] [CrossRef] [PubMed]
- Moretta, A.; Vitale, M.; Bottino, C.; Orengo, A.M.; Morelli, L.; Augugliaro, R.; Barbaresi, M.; Ciccone, E.; Moretta, L. P58 molecules as putative receptors for major histocompatibility complex (MHC) class I molecules in human natural killer (NK) cells. Anti-p58 antibodies reconstitute lysis of MHC class I-protected cells in NK clones displaying different specificities. J. Exp. Med. 1993, 178, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Mu, T.; Peng, L.; Xie, X.; He, H.; Shao, Q.; Wang, X.; Zhang, Y. Single Nucleotide Polymorphism of Genes Associated with Metabolic Fatty Liver Disease. J. Oncol. 2022, 2022, 9282557. [Google Scholar] [CrossRef]
- Murray, K.F.; Carithers, R.L. AASLD practice guidelines: Evaluation of the patient for liver transplantation. Hepatology 2005, 41, 1407–1432. [Google Scholar] [CrossRef]
- Nham, T.; Poznanski, S.M.; Fan, I.Y.; Shenouda, M.M.; Chew, M.V.; Lee, A.J.; Vahedi, F.; Karimi, Y.; Butcher, M.; Lee, D.A.; et al. Ex vivo-expanded NK cells from blood and ascites of ovarian cancer patients are cytotoxic against autologous primary ovarian cancer cells. Cancer Immunol. Immunother. 2018, 67, 575–587. [Google Scholar] [CrossRef] [PubMed]
- Parolini, F.; Biswas, P.; Serena, M.; Sironi, F.; Muraro, V.; Guizzardi, E.; Cazzoletti, L.; Scupoli, M.T.; Gibellini, D.; Ugolotti, E.; et al. Stability and Expression Levels of HLA-C on the Cell Membrane Modulate HIV-1 Infectivity. J. Virol. 2018, 92, 10–1128. [Google Scholar] [CrossRef]
- Rajagopalan, S.; Long, E.O. Understanding how combinations of HLA and KIR genes influence disease. J. Exp. Med. 2005, 201, 1025. [Google Scholar] [CrossRef]
- Rizzo, R.; Gentili, V.; Casetta, I.; Caselli, E.; De Gennaro, R.; Granieri, E.; Cassai, E.; Di Luca, D.; Rotola, A. Altered natural killer cells’ response to herpes virus infection in multiple sclerosis involves KIR2DL2 expression. J. Neuroimmunol. 2012, 251, 55–64. [Google Scholar] [CrossRef]
- Rizzo, R.; Gentili, V.; Rotola, A.; Bortolotti, D.; Cassai, E.; Di Luca, D. Implication of HLA-C and KIR Alleles in Human Papillomavirus Infection and Associated Cervical Lesions. Viral Immunol. 2014, 27, 468–470. [Google Scholar] [CrossRef]
- Roberts, C.H.; Molina, S.; Makalo, P.; Joof, H.; Harding-Esch, E.M.; Burr, S.E.; Mabey, D.C.W.; Bailey, R.L.; Burton, M.J.; Holland, M.J. Conjunctival Scarring in Trachoma Is Associated with the HLA-C Ligand of KIR and Is Exacerbated by Heterozygosity at KIR2DL2/KIR2DL3. PLoS Neglected Trop. Dis. 2014, 8, e2744. [Google Scholar] [CrossRef] [PubMed]
- Salerno, F.; Guevara, M.; Bernardi, M.; Moreau, R.; Wong, F.; Angeli, P.; Garcia-Tsao, G.; Lee, S.S. Refractory ascites: Pathogenesis, definition and therapy of a severe complication in patients with cirrhosis. Liver Int. 2010, 30, 937–947. [Google Scholar] [CrossRef] [PubMed]
- Salvoza, N.C.; Klinzing, D.C.; Gopez-Cervantes, J.; Baclig, M.O. Association of Circulating Serum miR-34a and miR-122 with Dyslipidemia among Patients with Non-Alcoholic Fatty Liver Disease. PLoS ONE 2016, 11, e0153497. [Google Scholar] [CrossRef]
- Sayaf, K.; Gabbia, D.; Russo, F.P.; De Martin, S. The Role of Sex in Acute and Chronic Liver Damage. Int. J. Mol. Sci. 2022, 23, 10654. [Google Scholar] [CrossRef]
- Serena, M.; Parolini, F.; Biswas, P.; Sironi, F.; Miranda, A.B.; Zoratti, E.; Scupoli, M.T.; Ziglio, S.; Valenzuela-Fernandez, A.; Gibellini, D.; et al. HIV-1 Env associates with HLA-C free-chains at the cell membrane modulating viral infectivity. Sci. Rep. 2017, 7, 40037. [Google Scholar] [CrossRef]
- Shi, J.; Zhao, J.; Zhang, X.; Cheng, Y.; Hu, J.; Li, Y.; Zhao, X.; Shang, Q.; Sun, Y.; Tu, B.; et al. Activated hepatic stellate cells impair NK cell anti-fibrosis capacity through a TGF-β-dependent emperipolesis in HBV cirrhotic patients. Sci. Rep. 2017, 7, srep44544. [Google Scholar] [CrossRef]
- Stephens, C.; Moreno-Casares, A.; López-Nevot, M.; García-Cortés, M.; Medina-Cáliz, I.; Hallal, H.; Soriano, G.; Roman, E.; Ruiz-Cabello, F.; Romero-Gomez, M.; et al. Killer immunoglobulin-like receptor profiles are not associated with risk of amoxicillin-clavulanate-induced liver injury in Spanish patients. Front. Pharmacol. 2016, 7, 280. [Google Scholar] [CrossRef]
- Stickel, F.; Moreno, C.; Hampe, J.; Morgan, M.Y. The genetics of alcohol dependence and alcohol-related liver disease. J. Hepatol. 2017, 66, 195–211. [Google Scholar] [CrossRef] [PubMed]
- Thiruchelvam-Kyle, L.; Hoelsbrekken, S.E.; Saether, P.C.; Bjørnsen, E.G.; Pende, D.; Fossum, S.; Daws, M.R.; Dissen, E. The Activating Human NK Cell Receptor KIR2DS2 Recognizes a β2-Microglobulin–Independent Ligand on Cancer Cells. J. Immunol. 2017, 198, 2556–2567. [Google Scholar] [CrossRef]
- Tonetti, C.R.; de Souza-Araújo, C.N.; Yoshida, A.; da Silva, R.F.; Alves, P.C.M.; Mazzola, T.N.; Derchain, S.; Fernandes, L.G.R.; Guimarães, F. Ovarian cancer-associated ascites have high proportions of cytokine-responsive CD56bright NK cells. Cells 2021, 10, 1702. [Google Scholar] [CrossRef]
- Umemura, T.; Joshita, S.; Saito, H.; Wakabayashi, S.-I.; Kobayashi, H.; Yamashita, Y.; Sugiura, A.; Yamazaki, T.; Ota, M. Investigation of the Effect of KIR–HLA Pairs on Hepatocellular Carcinoma in Hepatitis C Virus Cirrhotic Patients. Cancers 2021, 13, 3267. [Google Scholar] [CrossRef] [PubMed]
- Van den Besselaar, A.M.H.P. Precision and accuracy of the international normalized ratio in oral anticoagulant control. Haemostasis 1996, 26 (Suppl. 4), 248–265. [Google Scholar] [CrossRef] [PubMed]
- Varela-Rey, M.; Woodhoo, A.; Martinez-Chantar, M.L.; Mato, J.M.; Lu, S.C. Alcohol, DNA Methylation, and Cancer. Alcohol Res. Curr. Rev. 2013, 35, 25. [Google Scholar]
- WHO. Global Status Report on Alcohol and Health 2018; World Health Organisation: Geneva, Switzerland, 2018; p. 478. Available online: https://www.who.int/publications/i/item/9789241565639 (accessed on 25 March 2023).
- Yamada, H.; Suzuki, K.; Ichino, N.; Ando, Y.; Sawada, A.; Osakabe, K.; Sugimoto, K.; Ohashi, K.; Teradaira, R.; Inoue, T.; et al. Associations between circulating microRNAs (miR-21, miR-34a, miR-122 and miR-451) and non-alcoholic fatty liver. Clin. Chim. Acta 2013, 424, 99–103. [Google Scholar] [CrossRef]
- Yang, M.; Vanderwert, E.; Kimchi, E.T.; Staveley-O’Carroll, K.F.; Li, G. The Important Roles of Natural Killer Cells in Liver Fibrosis. Biomedicines 2023, 11, 1391. [Google Scholar] [CrossRef]


{kind=link}
| n (%) | Mean Age (Years ± SEM) | ||
|---|---|---|---|
| Total patients | 281 (92.7) | 53.63 ± 0.495 | |
| Ascites * | + | 162 (57.7) | 53.91 ± 0.644 |
| − | 119 (42.3) | 53.24 ± 0.775 | |
| Grade of Ascites | I | 32 (20.7) | 53.22 ± 1.381 |
| II | 66 (43.2) a | 52.73 ± 1.001 | |
| III | 56 (36.1) | 56.21 ± 1.074 | |
| Male AC Patients | Grade of Ascites | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameter | Normal Values | Total Patients N = 281 | Ascites + N = 162 | Ascites − N = 119 | P1 | Grade I N = 91 | Grade II N = 190 | Grade III N = 190 | P2 |
| Creatinine (mg/dL) | 0.7–1.2 | 228 * | 155 | 73 | 30 | 64 | 55 | ||
| 1.09 ± 0.75 ** | 1.14 ± 0.81 | 0.99 ± 0.61 | 0.161 | 1.01 ± 0.26 | 1.11 ± 1.05 | 1.25 ± 0.74 | 0.413 | ||
| Albumin (g/dL) | 3.5–5.2 | 174 | 118 | 56 | 21 | 53 | 39 | ||
| 3.46 ± 0.66 | 3.34 ± 0.62 | 3.69 ± 0.68 | 0.139 | 3.46 ± 0.65 | 3.28 ± 0.60 | 3.40 ± 0.63 | 0.455 | ||
| Bilirubin total (mg/dL) | 0.05–1.2 | 180 | 124 | 56 | 25 | 52 | 41 | ||
| 3.15 ± 4.15 | 3.33 ± 4.00 | 2.74 ± 4.47 | 0.378 | 2.62 ± 1.78 | 2.87 ± 2.39 | 4.42 ± 6.14 | 0.3785 | ||
| AST (U/L) | 5–40 | 172 | 119 | 53 | 20 | 52 | 41 | ||
| 97.44 ±189.61 | 88.15 ± 101.21 | 118.30 ± 307.14 | 0.337 | 62.10 ± 47.54 | 102.36 ± 128.92 | 84.34 ± 83.10 | 0.114 | ||
| ALT (U/L) | 5–41 | 174 | 120 | 54 | 21 | 52 | 41 | ||
| 74.35 ± 158.57 | 66.60 ± 100.49 | 91.55 ± 242.83 | 0.338 | 72.90 ± 168.28 | 69.50 ± 89.13 | 60.43 ± 73.56 | 0.877 | ||
| AP (U/L) | 40–130 | 163 | 112 | 51 | 20 | 49 | 37 | ||
| 175.28 ± 114.61 | 176.41 ± 110.41 | 162.80 ± 124.45 | 0.015 | 155.65 ± 62.95 | 178.12 ± 121.85 | 163.32 ± 88.39 | 0.655 | ||
| GGT (U/L) | 10–71 | 161 | 111 | 50 | 19 | 50 | 37 | ||
| 103.07 ± 91.75 | 99.90 ± 95.66 | 110.10 ± 82.88 | 0.5156 | 75.42 ± 58.33 | 108.06 ± 92.82 | 93.13 ± 104.53 | 0.405 | ||
| INR | 0.9–1.2 | 215 | 148 | 67 | 30 | 59 | 55 | ||
| 1.44 ± 0.35 | 1.46 ± 0.34 | 1.38 ± 0.38 | 0.125 | 1.38 ± 0.20 | 1.42 ± 0.22 | 1.55 ± 0.46 | 0.038 | ||
| Male AC Patients | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Controls N = 319 | Total AC Patients N = 281 | Ascites − N = 119 | Ascites + N = 162 | ||||||
| KIR Gene * | P/A | n (%) | n (%) | P1 | n (%) | n (%) | P2 | P3 | P4 |
| iKIRs | |||||||||
| 2DL1 (S1-) | + | 197 (61.8) | 160 (56.9) | 0.244 | 64 (53.8) | 96 (59.3) | 0.155 | 0.622 | 0.394 |
| − | 122 (38.2) | 121 (43.1) | 55 (46.2) | 66 (40.7) | |||||
| 2DL2 | + | 202 (63.3) | 149 (53.0) | 0.013 a | 64 (53.8) | 85 (52.5) | 0.079 | 0.024 b | 0.904 |
| − | 117 (36.7) | 132 (47) | 55 (46.2) | 77 (47.5) | |||||
| 2DL3 | + | 279 (87.5) | 249 (88.6) | 0.707 | 106 (89.1) | 143 (88.3) | 0.743 | 0.883 | 1.000 |
| − | 40 (12.5) | 32 (11.4) | 13 (10.9) | 19 (11.7) | |||||
| 2DL5 | + | 170 (53.3) | 158 (56.2) | 0.511 | 70 (58.8) | 88 (54.3) | 0.322 | 0.847 | 0.468 |
| − | 149 (46.7) | 123 (43.8) | 49 (41.2) | 74 (45.7) | |||||
| 3DL1 | + | 304 (95.3) | 268 (95.4) | 1.000 | 117 (98.3) | 151 (93.2) | 0.174 | 0.394 | 0.048 c |
| − | 15 (4.7) | 13 (4.6) | 2 (1.7) | 11 (6.8) | |||||
| Male AC Patients | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Controls N = 319 | Total Patients N = 281 | Ascites − N = 119 | Ascites + N = 162 | ||||||
| KIR Gene * | P/A | n (%) | n (%) | P1 | n (%) | n (%) | P2 | P3 | P4 |
| aKIRs | |||||||||
| 2DS1 (L1+) | + | 119 (37.3) | 119 (42.3) | 0.211 | 55 (46.2) | 64 (39.5) | 0.100 | 0.691 | 0.274 |
| − | 200 (62.7) | 162 (57.7) | 64 (53.8) | 98 (60.5) | |||||
| 2DS2 (L2+) | + | 201 (63.0) | 146 (52.0) | 0.006 a | 62 (52.1) | 84 (51.9) | 0.048 c | 0.024 e | 1.000 |
| − | 118 (37.0) | 135 (48) | 57 (47.9) | 78 (48.1) | |||||
| 2DS3 | + | 107 (33.5) | 93 (33.1) | 0.931 | 41 (34.5) | 52 (32.1) | 0.910 | 0.838 | 0.702 |
| − | 212 (66.5) | 188 (66.9) | 78 (65.5) | 110 (67.9) | |||||
| 2DS4 | + | 305 (95.6) | 266 (94.7) | 0.704 | 115 (96.6) | 151 (93.2) | 0.790 | 0.281 | 0.285 |
| − | 14 (4.4) | 15 (5.3) | 4 (3.4) | 11 (6.8) | |||||
| 2DS5 | + | 86 (27.0) | 99 (35.2) | 0.033 b | 47 (39.5) | 52 (32.1) | 0.014 d | 0.243 | 0.209 |
| − | 233 (73.0) | 182 (64.8) | 72 (60.5) | 110 (67.9) | |||||
| 3DS1 | + | 129 (40.4) | 132 (47.0) | 0.117 | 60 (50.4) | 72 (44.4) | 0.066 | 0.434 | 0.335 |
| − | 190 (59.6) | 149 (53.0) | 59 (49.6) | 90 (55.6) | |||||
| Male AC Patients | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Grade of Ascites | |||||||||||||
| Controls N = 319 | Total Patients N = 281 | Grade I N = 32 | Grade II N = 66 | Grade III N = 56 | |||||||||
| KIR Gene * | P/A | n (%) | n (%) | P1 | n (%) | n (%) | n (%) | P2 | P3 | P4 | P5 | P6 | P7 |
| iKIRs | |||||||||||||
| 2DL1 (S1-) | + | 197 (61.8) | 160 (56.9) | 0.244 | 16 (50) | 41 (62.1) | 34 (60.7) | 0.281 | 0.375 | 1.000 | 0.254 | 1.000 | 0.883 |
| − | 122 (38.2) | 121 (43.1) | 16 (50) | 25 (37.9) | 22 (39.3) | ||||||||
| 2DL2 | + | 202 (63.3) | 149 (53.0) | 0.013 a | 14 (43.8) | 34 (51.5) | 29 (51.8) | 0.523 | 0.512 | 1.000 | 0.036 b | 0.095 | 0.104 |
| − | 117 (36.7) | 132 (47) | 18 (56.3) | 32 (48.5) | 27 (48.2) | ||||||||
| 2DL3 | + | 279 (87.5) | 249 (88.6) | 0.707 | 26 (81.3) | 61 (92.4) | 51 (91.1) | 0.169 | 0.198 | 1.000 | 0.406 | 0.299 | 0.655 |
| − | 40 (12.5) | 32 (11.4) | 6 (18.8) | 5 (7.6) | 5 (8.9) | ||||||||
| 2DL5 | + | 170 (53.3) | 158 (56.2) | 0.511 | 18 (56.3) | 36 (54.5) | 30 (53.6) | 1.000 | 0.828 | 1.000 | 0.853 | 0.893 | 1.000 |
| − | 149 (46.7) | 123 (43.8) | 14 (43.8) | 30 (45.5) | 26 (46.4) | ||||||||
| 3DL1 | + | 304 (95.3) | 268 (95.4) | 1.000 | 28 (87.5) | 63 (95.5) | 52 (92.9) | 0.211 | 0.455 | 0.702 | 0.083 | 1.000 | 0.504 |
| − | 15 (4.7) | 13 (4.6) | 4 (12.5) | 3 (4.5) | 4 (7.1) | ||||||||
| Male AC Patients | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Grade of Ascites | |||||||||||||
| Controls N = 319 | Total Patients N = 281 | Grade I N = 32 | Grade II N = 66 | Grade III N = 56 | |||||||||
| KIR Gene * | P/A | n (%) | n (%) | P1 | n (%) | n (%) | n (%) | P2 | P3 | P4 | P5 | P6 | P7 |
| aKIRs | |||||||||||||
| 2DS1 (L1+) | + | 119 (37.3) | 119 (42.3) | 0.211 | 15 (46.9) | 25 (37.9) | 21 (37.5) | 0.511 | 0.500 | 1.000 | 0.341 | 1.000 | 1.000 |
| − | 200 (62.7) | 162 (57.7) | 17 (53.1) | 41 (62.1) | 35 (62.5) | ||||||||
| 2DS2 (L2+) | + | 201 (63.0) | 146 (52.0) | 0.006 a | 14 (43.8) | 34 (51.5) | 28 (50) | 0.523 | 0.659 | 1.000 | 0.037 c | 0.096 | 0.075 |
| − | 118 (37.0) | 135 (48) | 18 (56.3) | 32 (48.5) | 28 (50) | ||||||||
| 2DS3 | + | 107 (33.5) | 93 (33.1) | 0.931 | 14 (43.8) | 18 (27.3) | 17 (30.4) | 0.114 | 0.249 | 0.841 | 0.249 | 0.387 | 0.758 |
| − | 212 (66.5) | 188 (66.9) | 18 (56.3) | 48 (72.7) | 39 (69.6) | ||||||||
| 2DS4 | + | 305 (95.6) | 266 (94.7) | 0.704 | 28 (87.5) | 63 (95.5) | 52 (92.9) | 0.211 | 0.455 | 0.702 | 0.070 | 1.000 | 0.325 |
| − | 14 (4.4) | 15 (5.3) | 4 (12.5) | 3 (4.5) | 4 (7.1) | ||||||||
| 2DS5 | + | 86 (27.0) | 99 (35.2) | 0.033 b | 10 (31.3) | 23 (34.8) | 17 (30.4) | 0.821 | 1.000 | 0.700 | 0.678 | 0.230 | 0.627 |
| − | 233 (73.0) | 182 (64.8) | 22 (68.8) | 43 (65.2) | 39 (69.6) | ||||||||
| 3DS1 | + | 129 (40.4) | 132 (47.0) | 0.117 | 16 (50) | 29 (43.9) | 24 (42.9) | 0.667 | 0.657 | 1.000 | 0.347 | 0.680 | 0.769 |
| − | 190 (59.6) | 149 (53.0) | 16 (50) | 37 (56.1) | 32 (57.1) | ||||||||
| Male AC Patients | ||||||||
|---|---|---|---|---|---|---|---|---|
| Controls | Total Patients | Ascites − | Ascites + | |||||
| N = 314 | N = 272 | N = 113 | N = 159 | |||||
| Epitope HLA-C | n (%) | n (%) | P1 | n (%) | n (%) | P2 | P3 | P4 |
| C1+ | 266 (84.7) | 208 (76.5) | 0.015 a | 85 (75.2) | 123 (77.4) | 0.031 c | 0.056 | 0.772 |
| C1− | 48 (15.3) | 64 (23.5) | 28 (24.8) | 36 (22.6) | ||||
| C2+ | 213 (67.8) | 190 (69.9) | 0.655 | 72 (63.7) | 118 (74.2) | 0.485 | 0.168 | 0.081 |
| C2− | 101 (32.2) | 82 (30.1) | 41 (36.3) | 41 (36.3) | ||||
| Genotype HLA-C | ||||||||
| C1C1 | 101 (32.2) | 82 (30.1) | 0.655 | 41 (36.3) | 41 (25.8) | 0.485 | 0.168 | 0.081 |
| C1C2 | 165 (52.5) | 126 (46.3) | 0.137 | 44 (38.9) | 82 (51.6) | 0.016 d | 0.846 | 0.048 f |
| C2C2 | 48 (15.3) | 64 (23.5) | 0.015 b | 28 (24.8) | 36 (22.6) | 0.031 e | 0.056 | 0.772 |
| Grade I N = 32 | Grade II N = 65 | Grade III N = 55 | ||||
|---|---|---|---|---|---|---|
| Epitope HLA-C | n (%) | n (%) | n (%) | P1 | P2 | P3 |
| C1+ | 23 (71.9) | 50 (76.9) | 45 (81.8) | 0.622 | 0.295 | 0.653 |
| C1− | 9 (28.1) | 15 (23.1) | 10 (18.2) | |||
| C2+ | 23 (71.9) | 51 (78.5) | 40 (72.7) | 0.612 | 1.000 | 0.524 |
| C2− | 9 (28.1) | 14 (21.5) | 15 (27.3) | |||
| Genotype HLA-C | ||||||
| C1C1 | 9 (28.1) | 14 (21.5) | 15 (27.3) | 0.612 | 1.000 | 1.000 |
| C1C2 | 14 (43.8) | 36 (55.4) | 30 (54.5) | 0.388 | 0.388 | 1.000 |
| C2C2 | 9 (28.1) | 15 (23.1) | 10 (18.2) | 0.622 | 0.622 | 0.653 |
| Controls N = 319 | Patient Totals N = 281 | Ascites − N = 119 | Ascites + N = 213 | Grade I N = 32 | Grade II N = 66 | Grade III N = 56 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| KIR Genes | HLA-I Ligand | n (%) | n (%) | P1 | n (%) | n (%) | P2 | n (%) | n (%) | n (%) | P3 | P4 | P5 |
| iKIRs | |||||||||||||
| KIR2DL1+/S1− | C2+ | 221 (67.6) | 188 (70.1) | 0.530 | 71 (63.4) | 117 (75.0) | 0.043 | 23 (76.7) | 51 (78.5) | 40 (72.7) | 0.105 | 0.144 | 1.000 |
| C2− | 1 (25.0) | 2 (50.0) | 0 (0) | 2 (66.7) | 2 (100.0) | 0 (0) | 0 (0) | ||||||
| KIR2DL2+ | C1+ | 167 (83.5) | 109 (76.2) | 0.099 | 46 (76.7) | 63 (75.9) | 1.000 | 9 (64.3) | 27 (77.1) | 22 (78.6) | 0.710 | 0.402 | 0.516 |
| C1− | 15 (12.9) | 30 (23.3) | 14 (26.4) | 16 (21.1) | 4 (22.2) | 8 (25.8) | 4 (14.8) | ||||||
| KIR2DL3+ | C1+ | 235 (85.1) | 183 (75.9) | 0.010 a | 75 (75.0) | 108 (76.6) | 0.879 | 18 (69.2) | 46 (76.7) | 41 (80.4) | 1.000 | 0.317 | 0.497 |
| C1− | 7 (17.5) | 6 (19.4) | 3 (23.1) | 3 (16.7) | 1 (16.7) | 2 (33.3) | 0 (0) | ||||||
| KIR3DL1+ | Bw4+ | 231 (76.0) | 201 (75.0) | 0.846 | 87 (74.4) | 114 (75.5) | 0.887 | 21 (75.0) | 47 (73.4) | 40 (76.9) | 0.647 | 0.610 | 1.000 |
| Bw4– | 7 (46.7) | 7 (53.8) | 0 (0) | 7 (63.6) | 2 (50.0) | 3 (100.0) | 2 (50.0) | ||||||
| aKIRs | |||||||||||||
| KIR2DS1+ | C2+ | 78 (67.2) | 81 (70.4) | 0.670 | 32 (61.5) | 49 (77.8) | 0.067 | 10 (66.7) | 21 (84.0) | 17 (81.0) | 1.000 | 0.734 | 0.598 |
| C2− | 64 (32.0) | 48 (30.6) | 21 (34.4) | 27 (28.1) | 4 (23.5) | 10 (24.4) | 11 (32.4) | ||||||
| C2+ | 206 (68.0) | 178 (69.3) | 0.784 | 70 (64.2) | 108 (730) | 0.136 | 19 (67.9) | 49 (77.8) | 37 (72.5) | 1.000 | 1.000 | 0.437 | |
| C2− | 5 (38.5) | 3 (20.0) | 2 (50.0) | 1 (9.1) | 0 (0) | 0 (0) | 1 (25.0) | ||||||
| KIR2DS4+ | |||||||||||||
| C1+ | 257 (84.8) | 196 (76.3) | 0.013 b | 82 (75.2) | 114 (77.0) | 0.768 | 20 (71.4) | 47 (74.6) | 42 (82.4) | 0.309 | 1.000 | 0.478 | |
| C1− | 2 (15.4) | 3 (20.0) | 1 (25.0) | 2 (18.2) | 1 (25.0) | 0 (0) | 1 (25.0) | ||||||
| C1+ | 70 (84.3) | 70 (72.9) | 0.072 | 31 (70.5) | 39 (75.0) | 0.651 | 8 (80.0) | 17 (70.8) | 12 (70.6) | 0.517 | 0.467 | 1.000 | |
| C1− | 35 (15.0) | 38 (21.6) | 15 (21.7) | 23 (21.5) | 7 (31.8) | 9 (21.4) | 5 (13.2) | ||||||
| KIR2DS5+ | |||||||||||||
| C2+ | 56 (67.5) | 71 (74.0) | 0.410 | 30 (68.2) | 41 (78.8) | 0.253 | 8 (80.0) | 19 (79.2) | 14 (82.4) | 0.509 | 1.000 | 0.403 | |
| C2− | 75 (32.2) | 57 (32.4) | 27 (39.1) | 30 (28.0) | 7 (31.8) | 9 (21.4) | 12 (31.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Legaz, I.; Morales, R.; Bolarín, J.M.; Collados-Ros, A.; Pons, J.A.; Muro, M. Is the Development of Ascites in Alcoholic Liver Patients Influenced by Specific KIR/HLA Gene Profiles? Biomedicines 2023, 11, 2405. https://doi.org/10.3390/biomedicines11092405
Legaz I, Morales R, Bolarín JM, Collados-Ros A, Pons JA, Muro M. Is the Development of Ascites in Alcoholic Liver Patients Influenced by Specific KIR/HLA Gene Profiles? Biomedicines. 2023; 11(9):2405. https://doi.org/10.3390/biomedicines11092405
Chicago/Turabian StyleLegaz, Isabel, Raquel Morales, José Miguel Bolarín, Aurelia Collados-Ros, José Antonio Pons, and Manuel Muro. 2023. "Is the Development of Ascites in Alcoholic Liver Patients Influenced by Specific KIR/HLA Gene Profiles?" Biomedicines 11, no. 9: 2405. https://doi.org/10.3390/biomedicines11092405