
Activation Capacity of the Intrinsic Musculature of the Foot in Handball Athletes with Chronic Ankle Instability

 , ,
, ,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
2.3. Outcome Measures
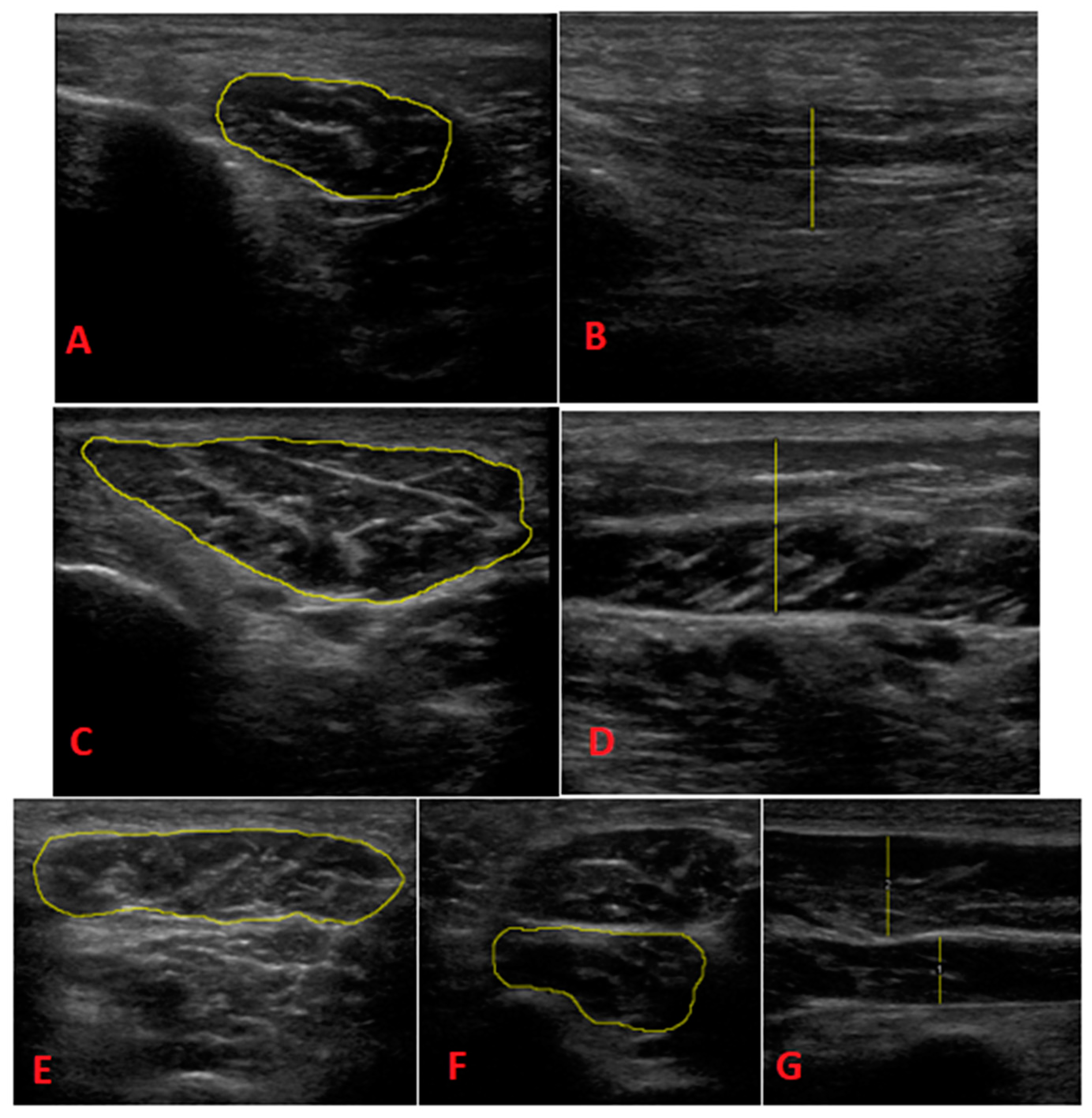
2.3.1. Ultrasound Morphology
- -
- FHB: Each patient was assessed in the prone decubitus position. We placed the probe longitudinally into the first MT (slightly oblique posterolateral direction). We then performed a proximal sweep to locate the thickest portion of the muscle belly, which was distal to the base of the first MT. The image was taken to measure the thickness.
- -
- AbH: Each patient was assessed in the supine position with slight external rotation of the hip and slight knee flexion. We placed the probe into the medial tuberosity of the calcaneus toward the scaphoid tubercle. Normally, the area of greatest thickness is located 1–2 cm proximal to the scaphoid tubercle. A longitudinal image was taken to determine thickness and a transverse image was taken to determine CSA.
- -
- AbDM: Each patient was assessed in the prone position. We located the insertion of the muscle in the lateral calcaneal tubercle and oriented the probe toward the tuberosity of the 5th MT. Normally, the area of greatest thickness is located near the calcaneocuboid joint, which was found before the tendon appeared. Longitudinal acquisition was performed to measure thickness and transverse acquisition was performed to determine CSA.
- -
- QP: Each patient was assessed in the prone position. The quadratus plantaris was located deep in the flexor digitorum brevis. We then located the talus-calcaneus-scaphoid joint and used the longitudinal probe to align in the direction of the muscle fibers, looking for the area of greatest thickness in the muscle belly, which is usually found proximal to the spring ligament. We then measured the thickness in the longitudinal section and measured CSA in the transverse section.
- -
- FDB: Each patient was assessed in prone position. We drew a line between the medial calcaneal tubercle and the third toe. We placed the probe in a longitudinal position relative to this line, which extended from the insertion in the calcaneus, and we performed distal sweeping until locating the area of greatest thickness in the muscle belly, before dividing it into 4 fascicles. The image was longitudinally taken to determine the thickness in the longitudinal section and transversely taken to determine the thickness in the ASC.
- -
- Heel fat pad morphology: The longitudinal section was measured at the calcaneus level and in the area of greatest thickness of the heel fat pad [21]. Measurements were first taken without compression and then taken with compression. The distance between the skin and the plantar fascia (heel fat) was measured. The compressibility index was calculated by dividing the thickness in compression by the thickness without compression. The measurements of the heel fat thickness were also determined using Image J 2.0 software (National Institutes of Health, Bethesda, MD, USA), as was the intrinsic musculature determined via the foot assessment.
- -
- Abdominal wall thickness: A bilateral ultrasound assessment was performed at rest (at the end of a relaxed exhalation) and at the contraction (homolateral hip flexion with the knee extended) of the abdominal wall thickness muscles and the inter-rectus distance. Three points were recorded: the anterolateral abdominal wall (thickness of the EO, IO and TrA), the anterior abdominal wall (rectus abdominis thickness) and the anterior abdominal wall 2 (inter-straight distance).
- -
- Anterolateral abdominal wall: Each patient was assessed in the supine position with a slight flexion of the hips and knees, with a cushion placed in the popliteal fossa. We transversally placed the probe at the level of the mid-axillary line at the midpoint between the lower edge of the costal grid and the iliac crest. In this way, we measured the thicknesses of the EO, IO and TrA.
- -
- Anterior abdominal wall: Each subject was assessed in the supine position with slight flexion of the hips and knees, with a cushion placed in the popliteal fossa. We transversely place the probe at the level of the umbilicus and laterally to the midline. In this image, we can see the transverse section of the rectus abdominis, of which we measured the thickness.
- -
- Anterior abdominal wall 2: Each subject was assessed in the supine position with hips and knees flexed, with a cushion placed in the popliteal fossa. We transversely placed the probe on the midline, which was just proximal to the umbilicus. In this image, we measured the inter-rectal distance. This distance was calculated from one muscle belly to the other, i.e., the connective tissue was included in the distance (the limits of the inter-rectus distance would be the muscle bellies themselves).
2.3.2. Foot Functionality: Bristol Foot Score Questionnaire
2.3.3. Toe Flexor Strength
2.3.4. Psychological Outcome Measures
2.4. Procedure
2.5. Statistical Analysis
3. Results
Descriptive Data Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Åman, M.; Forssblad, M.; Henriksson-Larsén, K. Incidence and severity of reported acute sports injuries in 35 sports using insurance registry data. Scand. J. Med. Sci. Sports 2015, 26, 451–462. [Google Scholar] [CrossRef] [PubMed]
- Engebretsen, L.; Soligard, T.; Steffen, K. Sports injuries and illnesses during the London Summer Olympic Games 2012. Br. J. Sports Med. 2013, 47, 407–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bere, T.; Alonso, J.M.; Wangensteen, A.; Bakken, A.; Eirale, C.; Dijkstra, H.P.; Ahmed, H.; Bahr, R.; Poppvic, N. Injury and illness surveillance during the 24th Men’s Handball World Championship 2015 in Qatar. Br. J. Sports Med. 2015, 49, 1151–1156. [Google Scholar] [CrossRef] [PubMed]
- Tabben, M.; Landreau, P.; Chamari, K.; Juin, G.; Ahmed, H.; Farooq, A.; Bahr, R.; Popovic, N. Age, player position and 2 min suspensions were associated with match injuries during the 2017 Men’s Handball World Championship (France). Br. J. Sports Med. 2018, 53, 436–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giroto, N.; Junior, L.C.H.; Gomes, M.R.C.; Lopes, A.D. Incidence and risk factors of injuries in Brazilian elite handball players: A prospective cohort study. Scand. J. Med. Sci. Sports 2015, 27, 195–202. [Google Scholar] [CrossRef]
- Rafnsson, E.T.; Valdimarsson, Ö.; Sveinsson, T.; Árnason, Á. Injury Pattern in Icelandic Elite Male Handball Players. Clin. J. Sport Med. 2019, 29, 232–237. [Google Scholar] [CrossRef]
- Yde, J.; Nielsen, A.B. Sports injuries in adolescents′ ball games: Soccer, handball and basketball. Br. J. Sports Med. 1990, 24, 51–54. [Google Scholar] [CrossRef] [Green Version]
- Fong, D.T.-P.; Hong, Y.; Chan, L.-K.; Yung, P.S.-H.; Chan, K.-M. A Systematic Review on Ankle Injury and Ankle Sprain in Sports. Sports Med. 2007, 37, 73–94. [Google Scholar] [CrossRef] [Green Version]
- Junge, A.; Engebretsen, L.; Mountjoy, M.L.; Alonso, J.M.; Renström, P.A.F.H.; Aubry, M.J.; Dvorak, J. Sports Injuries During the Summer Olympic Games 2008. Am. J. Sports Med. 2009, 37, 2165–2172. [Google Scholar] [CrossRef] [PubMed]
- Langevoort, G.; Myklebust, G.; Dvorak, J.; Junge, A. Handball injuries during major international tournaments. Scand. J. Med. Sci. Sports 2007, 17, 400–407. [Google Scholar] [CrossRef]
- Seil, R.; Rupp, S.; Tempelhof, S.; Kohn, D. Sports injuries in team handball. A one-year prospective study of sixteen men’s senior teams of a superior nonprofessional level. Am. J. Sports Med. 1998, 26, 681–687. [Google Scholar] [CrossRef]
- Nielsen, A.B.; Yde, J. An Epidemiologic and Traumatologic Study of Injuries in Handball. Int. J. Sports Med. 1988, 9, 341–344. [Google Scholar] [CrossRef]
- Soysa, A.; Hiller, C.; Refshauge, K.; Burns, J. Importance and challenges of measuring intrinsic foot muscle strength. J. Foot Ankle Res. 2012, 5, 1–14. Available online: http://www.jfootankleres.com/content/5/1/29 (accessed on 31 May 2023). [CrossRef] [PubMed] [Green Version]
- Mickle, K.J.; Nester, C.J.; Crofts, G.; Steele, J.R. Reliability of ultrasound to measure morphology of the toe flexor muscles. J. Foot Ankle Res. 2013, 6, 12. Available online: http://www.jfootankleres.com/content/6/1/12 (accessed on 31 May 2023). [CrossRef] [PubMed] [Green Version]
- Romero-Morales, C.; Martín-Llantino, P.J.; Calvo-Lobo, C.; Almazán-Polo, J.; López-López, D.; de la Cruz-Torres, B.; Palomo-López, P.; Rodríguez-Sanz, D. Intrinsic foot muscles morphological modifications in patients with Achilles tendinopathy: A novel case-control research study. Phys. Ther. Sport 2019, 40, 208–212. [Google Scholar] [CrossRef]
- Calvo-Lobo, C.; Useros-Olmo, A.I.; Almazán-Polo, J.; Becerro-De-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Palomo-López, P.; Rodríguez-Sanz, D.; López-López, D. Rehabilitative ultrasound imaging of the bilateral intrinsic plantar muscles and fascia in post-stroke survivors with hemiparesis: A case-control study. Int. J. Med Sci. 2018, 15, 907–914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angin, S.; Crofts, G.; Mickle, K.J.; Nester, C.J. Ultrasound evaluation of foot muscles and plantar fascia in pes planus. Gait Posture 2014, 40, 48–52. [Google Scholar] [CrossRef] [Green Version]
- Mickle, K.J.; Angin, S.; Crofts, G.; Nester, C.J. Effects of Age on Strength and Morphology of Toe Flexor Muscles. J. Orthop. Sports Phys. Ther. 2016, 46, 1065–1070. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int. J. Surg. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]
- Gribble, P.A.; Delahunt, E.; Bleakley, C.M.; Caulfield, B.; Docherty, C.L.; Fong, D.T.-P.; Fourchet, F.; Hertel, J.; Hiller, C.E.; Kaminski, T.W.; et al. Selection Criteria for Patients With Chronic Ankle Instability in Controlled Research: A Position Statement of the International Ankle Consortium. J. Athl. Train. 2014, 49, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Falsetti, P.; Frediani, B.; Acciai, C.; Baldi, F.; Filippou, G.; Galeazzi, M.; Marcolongo, R. Ultrasonography and magnetic resonance imaging of heel fat pad inflammatory-oedematous lesions in rheumatoid arthritis. Scand. J. Rheumatol. 2006, 35, 454–458. [Google Scholar] [CrossRef]
- Riskowski, J.L.; Hagedorn, T.J.; Hannan, M.T. Measures of foot function, foot health and foot pain. Arthritis Care Res. 2011, 63, 229–239. [Google Scholar] [CrossRef] [PubMed]
- Spink, M.; Fotoohabadi, M.R.; Menz, H. Foot and Ankle Strength Assessment Using Hand-Held Dynamometry: Reliability and Age-Related Differences. Gerontology 2010, 56, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. Test Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W.F. Comparison of Beck Depression Inventories-IA and-II in Psychiatric Outpatients. J. Pers. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-It; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Gómez-Pérez, L.; López-Martínez, A.E.; Ruiz-Párraga, G.T. Psychometric Properties of the Spanish Version of the Tampa Scale for Kinesiophobia (TSK). J. Pain 2011, 12, 425–435. [Google Scholar] [CrossRef]
- Miller, R.P.; Kori, S.H. The Tampa Scale; Tampa Fla: Georgia, MX, USA, 1991. [Google Scholar]
- Kori, S.H.; Miller, R.P.; Todd, D.D. Kinesiophobia: A new view of chronic pain behaviour. Pain Manag. 1990, 3, 35–43. [Google Scholar]
- lbañez, M.L.; Ortet, G.; Moro, M. Adaptación al castellano de la versión reducida cuestionario revisado de personalidad de Eysenck (EPQ-RA). Análisis y Modificación de Conducta 1999, 25, 849–864. [Google Scholar]
- Eysenck, H.J.; Eysenck, B.G. Cuestionario Revisado de Personalidad de Eysenck EPQ-R; TEA Ediciones: Madrid, Spain, 1997. [Google Scholar]
- Cárdenas, M.; Arancibia, H. Potencia estadística y cálculo del tamaño del efecto en G*Power. Salud Soc. 2014, 5, 210–224. [Google Scholar] [CrossRef] [Green Version]
- Dominguez-Lara, S. Magnitud del efecto para pruebas de normalidad en investigación en salud. Investig. En Educ. Médica 2018, 7, 92–93. [Google Scholar] [CrossRef]
- Fraser, J.J.; Koldenhoven, R.; Hertel, J. Ultrasound Measures of Intrinsic Foot Muscle Size and Activation Following Lateral Ankle Sprain and Chronic Ankle Instability. J. Sport Rehabil. 2021, 30, 1008–1018. [Google Scholar] [CrossRef]
- Feger, M.A.; Snell, S.; Handsfield, G.G.; Blemker, S.S.; Wombacher, E.; Fry, R.; Hart, J.M.; Saliba, S.A.; Park, J.S.; Hertel, J. Diminished Foot and Ankle Muscle Volumes in Young Adults with Chronic Ankle Instability. Orthop. J. Sports Med. 2016, 4, 2325967116653719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.-R.; Choi, Y.-E. Effects of a 6-week intrinsic foot muscle exercise program on the functions of intrinsic foot muscle and dynamic balance in patients with chronic ankle instability. J. Exerc. Rehabil. 2019, 15, 709–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wikstrom, E.A.; Song, K. Generic and psychological patient-reported deficits in those with chronic ankle instability: A cross sectional study. Phys. Ther. Sport 2019, 40, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, K.; Arab, A.M.; Abdollahi, I.; López-López, D.; Calvo-Lobo, C. Electromiography comparison of distal and proximal lower limb muscle activity patterns during external perturbation in subjects with and without functional ankle instability. Hum. Mov. Sci. 2017, 55, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Fraser, J.J.; Koldenhoven, R.M.; Jaffri, A.H.; Park, J.S.; Saliba, S.F.; Hart, J.M.; Hertel, J. Foot impairments contribute to functional limitation in individuals with ankle sprain and chronic ankle instability. Knee Surg. Sports Traumatol. Arthrosc. 2018, 28, 1600–1610. [Google Scholar] [CrossRef]
- Lee, E.; Cho, J.; Lee, S. Short-Foot Exercise Promotes Quantitative Somatosensory Function in Ankle Instability: A Randomized Controlled Trial. Experiment 2019, 25, 618–626. [Google Scholar] [CrossRef]
- Hertel, J.; Corbett, R.O. An Updated Model of Chronic Ankle Instability. J. Athl. Train. 2019, 54, 572–588. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, T.; Takabayashi, T.; Kudo, S.; Edama, M. The prevalence of chronic ankle instability and its relationship to foot arch characteristics in female collegiate athletes. Phys. Ther. Sport 2020, 46, 162–168. [Google Scholar] [CrossRef]
- Mei-Dan, O.; Kahn, G.; Zeev, A.; Rubin, A.; Constantini, N.; Even, A.; Nyska, M.; Mann, G. The Medial Longitudinal Arch as a Possible Risk Factor for Ankle Sprains: A Prospective Study in 83 Female Infantry Recruits. Foot Ankle Int. 2005, 26, 180–183. [Google Scholar] [CrossRef]
- Young, C.C.; Niedfeldt, M.W.; Morris, G.A.; Eerkes, K.J. Clinical Examination of the Foot and Ankle. Prim. Care 2005, 32, 105–132. [Google Scholar] [CrossRef]
- Abe, T.; Tayashiki, K.; Nakatani, M.; Watanabe, H. Relationships of ultrasound measures of intrinsic foot muscle cross-sectional area and muscle volume with maximum toe flexor muscle strength and physical performance in young adults. J. Phys. Ther. Sci. 2016, 28, 14–19. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Rodríguez, R.; Valle-Estévez, S.; Fraile-García, P.A.; Martínez-Nova, A.; Gómez-Martín, B.; Escamilla-Martínez, E. Modification of Pronated Foot Posture after a Program of Therapeutic Exercises. Int. J. Environ. Res. Public Health 2020, 17, 8406. [Google Scholar] [CrossRef] [PubMed]
- Ozmen, T.; Aydogmus, M. Effect of core strength training on dynamic balance and agility in adolescent badminton players. J. Bodyw. Mov. Ther. 2015, 20, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.; Kim, Y.; Choi, M. Kinetic Effects of 6 Weeks’ Pilates or Balance Training in College Soccer Players with Chronic Ankle Instability. Int. J. Environ. Res. Public Health 2022, 19, 12903. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Group | Mean | Sx | Maximum | Minimum | Significance | d |
|---|---|---|---|---|---|---|---|
| BFS | Control | 21.083 | 6.501 | 35 | 15 | 0.007 * | 1.404 |
| Case | 31.875 | 8.709 | 48 | 20 | |||
| FPI | Control | 3.083 | 3.704 | 7 | −3 | 1.000 | 0.020 |
| Case | 3.000 | 4.309 | 8 | −6 | |||
| BMI | Control | 24.980 | 2.418 | 28 | 21 | 1.000 | 0.268 |
| Case | 25.763 | 3.332 | 33 | 23 | |||
| HALLUX F. | Control | 138.849 | 55.277 | 272.13 | 72.6 | 0.069 | 0.658 |
| Case | 169.565 | 36.019 | 216.73 | 128.73 | |||
| TOES F. | Control | 128.162 | 38.779 | 197.4 | 76.2 | 0.115 | 0.903 |
| Case | 162.920 | 38.183 | 219.53 | 115 | |||
| SENSE F. | Control | 1.293 | 3.496 | 9.29 | −2.37 | 0.970 | 0.201 |
| Case | 0.643 | 2.927 | 6.59 | −3.53 | |||
| THICKNESS AbH | Control | 1.035 | 0.018 | 1.073 | 1.012 | 0.734 | 0.419 |
| Case | 1.048 | 0.04 | 1.108 | 1.003 | |||
| CSA AbH | Control | 1.055 | 0.028 | 1.093 | 1.016 | 0.910 | 0.148 |
| Case | 1.059 | 0.026 | 1.107 | 1.031 | |||
| THICKNESS AbDM | Control | 1.072 | 0.050 | 1.178 | 0.998 | 0.851 | 0.209 |
| Case | 1.086 | 0.080 | 1.261 | 1.006 | |||
| CSA AbDM | Control | 1.137 | 0.122 | 1.384 | 0.996 | 1.000 | 0.048 |
| Case | 1.131 | 0.126 | 1.408 | 1.015 | |||
| THICKNESS QP | Control | 1.092 | 0.081 | 1.262 | 1.009 | 0.157 | 0.729 |
| Case | 1.024 | 0.104 | 1.141 | 0.781 | |||
| CSA QP | Control | 1.149 | 0.088 | 1.304 | 1.017 | 0.473 | 0.377 |
| Case | 1.116 | 0.087 | 1.280 | 0.979 | |||
| THICKNESS FDB | Control | 1.097 | 0.047 | 1.188 | 1.029 | 0.384 | 0.080 |
| Case | 1.091 | 0.095 | 1.304 | 0.990 | |||
| CSA FDB | Control | 1.053 | 0.026 | 1.102 | 1.015 | 0.910 | 0.299 |
| Case | 1.071 | 0.081 | 1.229 | 0.990 | |||
| HEEL FAT | Control | 0.699 | 0.067 | 0.797 | 0.596 | 0.427 | 0.422 |
| Case | 0.674 | 0.050 | 0.758 | 0.606 | |||
| IRD | Control | 0.112 | 0.213 | 0.718 | −0.136 | 0.792 | 0 |
| Case | 0.112 | 0.124 | 0.377 | −0.004 | |||
| RA R | Control | 1.054 | 0.053 | 1.177 | 0.995 | 0.157 | 0.480 |
| Case | 1.079 | 0.051 | 1.164 | 1.019 | |||
| RA L | Control | 1.063 | 0.040 | 1.145 | 1.016 | 0.734 | 0.118 |
| Case | 1.067 | 0.026 | 1.107 | 1.018 | |||
| TrA R | Control | 1.112 | 0.093 | 1.259 | 0.984 | 0.734 | 0.242 |
| Case | 1.137 | 0.112 | 1.374 | 1.035 | |||
| TrA L | Control | 1.125 | 0.126 | 1.404 | 1.008 | 0.851 | 0.240 |
| Case | 1.097 | 0.106 | 1.234 | 0.947 | |||
| IO R | Control | 1.125 | 0.125 | 1.329 | 0.918 | 0.624 | 0.510 |
| Case | 1.077 | 0.045 | 1.145 | 1.015 | |||
| IO L | Control | 1.122 | 0.094 | 1.261 | 0.988 | 0.238 | 0.719 |
| Case | 1.065 | 0.061 | 1.141 | 0.944 | |||
| EO R | Control | 0.898 | 0.118 | 1.074 | 0.631 | 0.343 | 0.457 |
| Case | 0.947 | 0.095 | 1.124 | 0.850 | |||
| EO L | Control | 0.923 | 0.080 | 1.039 | 0.771 | 0.851 | 0.210 |
| Case | 0.958 | 0.221 | 1.297 | 0.661 | |||
| EPQ-RA Neuroticism | Control | 1.500 | 1.168 | 3 | 0 | 0.521 | 0.346 |
| Case | 1.125 | 0.991 | 2 | 0 | |||
| EPQ-RA Psychoticism | Control | 1.083 | 0.793 | 2 | 0 | 0.792 | 0.270 |
| Case | 1.375 | 1.302 | 4 | 0 | |||
| EPQ-RA Extraversion | Control | 3.750 | 2.050 | 6 | 0 | 0.624 | 0,267 |
| Case | 4.250 | 1.669 | 6 | 2 | |||
| EPQ-RA Sincerity | Control | 4.333 | 1.614 | 6 | 1 | 0.157 | 0.659 |
| Case | 3.250 | 1.669 | 6 | 1 | |||
| TSK-11 Avoidance | Control | 13.917 | 2.712 | 18 | 10 | 0.208 | 0.578 |
| Case | 12.125 | 3.441 | 17 | 9 | |||
| TSK-11 Harm | Control | 9.250 | 1.765 | 13 | 7 | 0.734 | 0.056 |
| Case | 9.375 | 2.615 | 14 | 5 | |||
| BD I-II | Control | 11.083 | 8.185 | 27 | 2 | 1.000 | 0.036 |
| Case | 11.375 | 7.963 | 26 | 4 | |||
| STAI T/A | Control | 26.750 | 5.496 | 35 | 17 | 0.521 | 0.141 |
| Case | 26.000 | 5.127 | 34 | 21 | |||
| STAI S/A | Control | 28.000 | 6.551 | 39 | 17 | 0.208 | 0.738 |
| Case | 23.875 | 4.422 | 29 | 17 |
| Foot Ultrasound Morphology Variables Correlations | r | Sig. (n = 20) | φ |
|---|---|---|---|
| BMI-SENSE F | 0.568 | 0.009 ** | 0.753 |
| BMI-IRD | −0.510 | 0.022 * | 0.714 |
| FPI-TrA R | 0.600 | 0.005 ** | 0.774 |
| FPI-IO L | 0.514 | 0.020 * | 0.716 |
| BFS-HALLUX F | 0.494 | 0.027 * | 0.702 |
| HALLUX F-TOES F | 0.916 | 0.000 ** | 0.957 |
| TOES F-CSA QP | 0.451 | 0.046 * | 0.671 |
| SENSE F-CSA AbDM | −0.510 | 0.022 * | 0.714 |
| SENSE F-IRD | −0.459 | 0.042 * | 0.677 |
| THICKNESS AbH-CSA AbH | 0.498 | 0.025 * | 0.705 |
| THICKNESS AbH-IO L | −0.540 | 0.014 * | 0.734 |
| CSA AbDM-TrA L | 0.508 | .0.022 * | 0.712 |
| CSA QP-RA R | −0.505 | 0.023 * | 0.710 |
| THICKNESS FDB-HEEL FAT | −0.498 | 0.026 * | 0.705 |
| CSA FDB-RA L | −0.525 | 0.017 * | 0.724 |
| HEEL FAT-TrA L | 0.559 | 0.010 * | 0.747 |
| EO R-EO L | 0.589 | 0.006 * | 0.767 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-García, D.; Llamas-Ramos, R.; Calvo-Lobo, C.; Rodríguez-Sanz, D.; San Antolín-Gil, M.; Cabanillas-García, J.L.; Sánchez-Gómez, M.C.; Llamas-Ramos, I. Activation Capacity of the Intrinsic Musculature of the Foot in Handball Athletes with Chronic Ankle Instability. Biomedicines 2023, 11, 2115. https://doi.org/10.3390/biomedicines11082115
García-García D, Llamas-Ramos R, Calvo-Lobo C, Rodríguez-Sanz D, San Antolín-Gil M, Cabanillas-García JL, Sánchez-Gómez MC, Llamas-Ramos I. Activation Capacity of the Intrinsic Musculature of the Foot in Handball Athletes with Chronic Ankle Instability. Biomedicines. 2023; 11(8):2115. https://doi.org/10.3390/biomedicines11082115
Chicago/Turabian StyleGarcía-García, Daniel, Rocío Llamas-Ramos, César Calvo-Lobo, David Rodríguez-Sanz, Marta San Antolín-Gil, Juan Luis Cabanillas-García, Mari Cruz Sánchez-Gómez, and Inés Llamas-Ramos. 2023. "Activation Capacity of the Intrinsic Musculature of the Foot in Handball Athletes with Chronic Ankle Instability" Biomedicines 11, no. 8: 2115. https://doi.org/10.3390/biomedicines11082115