

Understanding the Impact of COVID-19 on Angioplasty Service and Outcome of Patients Treated for Chronic Limb-Threatening Ischaemia: A Single-Centre Retrospective Cohort Study
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting and Patients
2.2. Patient Assessment and Procedure Planning
2.3. Day-Case Criteria and Procedure Preparation
2.4. Peri- and Post-Procedural Management
2.5. Clinical Outcome Assessment
2.6. Statistical Analyses
3. Results
3.1. Baseline and Procedural Characteristics
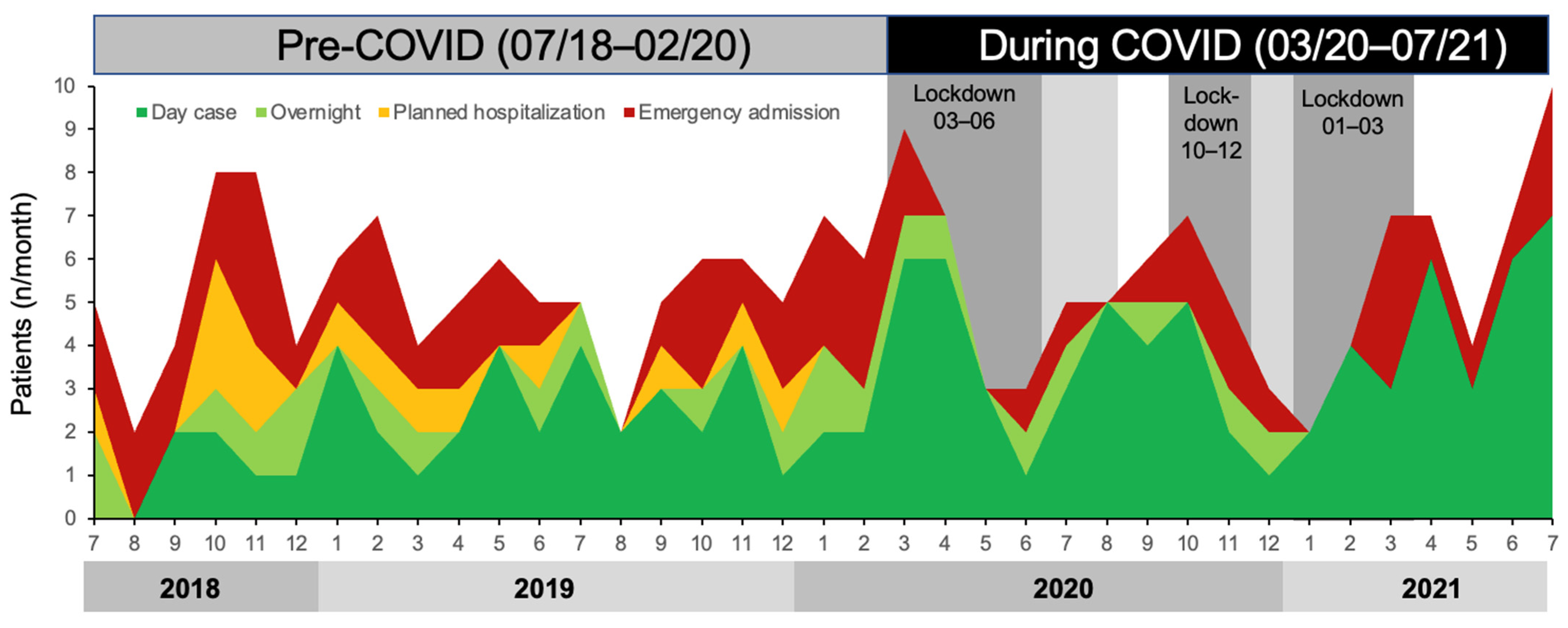
3.2. COVID-19-Related Changes in Angioplasty Service
3.3. Effect of COVID-19 on 30-Day and 1-Year Outcomes
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Song, P.; Rudan, D.; Zhu, Y.; Fowkes, F.J.I.; Rahimi, K.; Fowkes, F.G.R.; Rudan, I. Global, regional, and national prevalence and risk factors for peripheral artery disease in 2015: An updated systematic review and analysis. Lancet Glob. Health 2019, 7, e1020–e1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behrendt, C.A.; Thomalla, G.; Rimmele, D.L.; Petersen, E.L.; Twerenbold, R.; Debus, E.S.; Kolbel, T.; Blankenberg, S.; Schmidt-Lauber, C.; Peters, F.; et al. Editor’s Choice—Prevalence of Peripheral Arterial Disease, Abdominal Aortic Aneurysm, and Risk Factors in the Hamburg City Health Study: A Cross Sectional Analysis. Eur. J. Vasc. Endovasc. Surg. 2023, 65, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Stoberock, K.; Kaschwich, M.; Nicolay, S.S.; Mahmoud, N.; Heidemann, F.; Rieß, H.C.; Debus, E.S.; Behrendt, C.-A. The interrelationship between diabetes mellitus and peripheral arterial disease—A systematic review. Vasa 2021, 50, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Ireland, Vascular Society of Great Britain and Ireland. Peripheral Arterial Disease-Quality Improvement Framework. 2019. Available online: https://www.vascularsociety.org.uk/_userfiles/pages/files/Newsletters/PAD%20QIF%20April%202019(1).pdf (accessed on 1 July 2023).
- Reinecke, H.; Unrath, M.; Freisinger, E.; Bunzemeier, H.; Meyborg, M.; Luders, F.; Gebauer, K.; Roeder, N.; Berger, K.; Malyar, N.M. Peripheral arterial disease and critical limb ischaemia: Still poor outcomes and lack of guideline adherence. Eur. Heart J. 2015, 36, 932–938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigvant, B.; Lundin, F.; Wahlberg, E. The Risk of Disease Progression in Peripheral Arterial Disease is Higher than Expected: A Meta-Analysis of Mortality and Disease Progression in Peripheral Arterial Disease. Eur. J. Vasc. Endovasc. Surg. 2016, 51, 395–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prompers, L.; Huijberts, M.; Apelqvist, J.; Jude, E.; Piaggesi, A.; Bakker, K.; Edmonds, M.; Holstein, P.; Jirkovska, A.; Mauricio, D.; et al. High prevalence of ischaemia, infection and serious comorbidity in patients with diabetic foot disease in Europe. Baseline results from the Eurodiale study. Diabetologia 2007, 50, 18–25. [Google Scholar] [CrossRef] [Green Version]
- Frank, U.; Nikol, S.; Belch, J.; Boc, V.; Brodmann, M.; Carpentier, P.H.; Chraim, A.; Canning, C.; Dimakakos, E.; Gottsater, A.; et al. ESVM Guideline on peripheral arterial disease. Vasa 2019, 48, 1–79. [Google Scholar] [CrossRef] [Green Version]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Bjorck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries Endorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [CrossRef] [Green Version]
- Hinchliffe, R.J.; Brownrigg, J.R.; Andros, G.; Apelqvist, J.; Boyko, E.J.; Fitridge, R.; Mills, J.L.; Reekers, J.; Shearman, C.P.; Zierler, R.E.; et al. Effectiveness of revascularization of the ulcerated foot in patients with diabetes and peripheral artery disease: A systematic review. Diabetes Metab. Res. Rev. 2016, 32 (Suppl. 1), 136–144. [Google Scholar] [CrossRef]
- Rodway, A.; Stafford, M.; Wilding, S.; Ntagiantas, N.; Patsiogiannis, V.; Allan, C.; Field, B.; Clark, J.; Casal, F.P.; Pankhania, A.; et al. Day case angioplasty in a secondary care setting-initial experience. Vasa 2021, 50, 202–208. [Google Scholar] [CrossRef]
- Rodway, A.D.; Cheal, D.; Allan, C.; Pazos-Casal, F.; Hanna, L.; Field, B.C.T.; Pankhania, A.; Aston, P.J.; Skene, S.S.; Maytham, G.D.; et al. Ankle Doppler for Cuffless Ankle Brachial Index Estimation and Peripheral Artery Disease Diagnosis Independent of Diabetes. J. Clin. Med. 2023, 12, 97. [Google Scholar] [CrossRef] [PubMed]
- Conte, M.S.; Bradbury, A.W.; Kolh, P.; White, J.V.; Dick, F.; Fitridge, R.; Mills, J.L.; Ricco, J.B.; Suresh, K.R.; Murad, M.H.; et al. Global Vascular Guidelines on the Management of Chronic Limb-Threatening Ischemia. Eur. J. Vasc. Endovasc. Surg. 2019, 58, S1–S109.e33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heiss, C.; Olinic, D.M.; Belch, J.J.F.; Brodmann, M.; Mazzolai, L.; Stanek, A.; Madaric, J.; Krentz, A.; Schlager, O.; Lichtenberg, M.; et al. Management of chronic peripheral artery disease patients with indication for endovascular revascularization. Vasa 2022, 51, 121–137. [Google Scholar] [CrossRef]
- Bradbury, A.W.; Moakes, C.A.; Popplewell, M.; Meecham, L.; Bate, G.R.; Kelly, L.; Chetter, I.; Diamantopoulos, A.; Ganeshan, A.; Hall, J.; et al. A vein bypass first versus a best endovascular treatment first revascularisation strategy for patients with chronic limb threatening ischaemia who required an infra-popliteal, with or without an additional more proximal infra-inguinal revascularisation procedure to restore limb perfusion (BASIL-2): An open-label, randomised, multicentre, phase 3 trial. Lancet 2023, 401, 1798–1809. [Google Scholar] [CrossRef]
- Farber, A.; Menard, M.T.; Conte, M.S.; Kaufman, J.A.; Powell, R.J.; Choudhry, N.K.; Hamza, T.H.; Assmann, S.F.; Creager, M.A.; Cziraky, M.J.; et al. Surgery or Endovascular Therapy for Chronic Limb-Threatening Ischemia. N. Engl. J. Med. 2022, 387, 2305–2316. [Google Scholar] [CrossRef] [PubMed]
- Thieme, M.; Krankenberg, H.; Schilling, T.; Betge, S.; Korosoglou, G.; Rammos, C.; Vosseler, M.; Espinola-Klein, C.; Heilmeier, B.; Muller, O.J.; et al. Endovascular interventions in outpatient care. Vasa 2023, 52, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Korosoglou, G.; Blessing, E.; Grozinger, G.; Teichgraber, U.; Schmidt, A.; Zeller, T. Endovascular therapy or surgery for chronic limb threatening ischemia? Vasa 2023, 52, 214–217. [Google Scholar] [CrossRef]
- Meza-Torres, B.; Cunningham, S.G.; Heiss, C.; Joy, M.; Feher, M.; Leese, G.P.; de Lusignan, S.; Carinci, F. Adherence to General Diabetes and Foot Care Processes, with Prompt Referral, Are Associated with Amputation-Free Survival in People with Type 2 Diabetes and Foot Ulcers: A Scottish National Registry Analysis. J. Diabetes Res. 2022, 2022, 7414258. [Google Scholar] [CrossRef]
- Kendirci, M.; Sahiner, I.T.; Sezikli, I.; Akin, M.; Yasti, A.C. Effects of the COVID-19 pandemic on the management of diabetic foot ulcers: Experiences from a dedicated diabetic foot care center. Wounds 2022, 34, 146–150. [Google Scholar] [CrossRef]
- Mariet, A.S.; Benzenine, E.; Bouillet, B.; Verges, B.; Quantin, C.; Petit, J.M. Impact of the COVID-19 Epidemic on hospitalization for diabetic foot ulcers during lockdown: A French nationwide population-based study. Diabet. Med. 2021, 38, e14577. [Google Scholar] [CrossRef]
- de Mestral, C.; Gomez, D.; Wilton, A.S.; Lee, D.S.; Albalawi, Z.; Austin, P.C.; Jacob-Brassard, J.; Urbach, D.R.; Al-Omran, M.; Baxter, N.N. A Population-Based Analysis of Diabetes-Related Care Measures, Foot Complications, and Amputation During the COVID-19 Pandemic in Ontario, Canada. JAMA Netw. Open 2022, 5, e2142354. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre-COVID-19 | During COVID-19 | p | |
|---|---|---|---|
| 07/2018–02/2020 | 03/2020–07/2021 | ||
| n (n) | 106 | 94 | |
| Sex (m/f) | 61/45 | 66/28 | |
| Day case-based outpatients | 56 | 75 | <0.001 |
| - Same day discharge (n) | 41 | 68 | 0.009 |
| - Overnight (n) | 15 | 7 | 0.009 |
| Hospitalised (n) | 50 | 19 | <0.001 |
| - Planned urgent hospitalisation (n) | 14 | 0 | 0.010 |
| - Emergency admission (n) | 36 | 19 | 0.010 |
| Time to procedure (d) | 19 ± 18 | 15 ± 13 | 0.129 |
| - daycases (d) | 25 ± 20 | 18 ± 13 | 0.009 |
| - daycases ≤ 14 days | 39% | 64% | 0.291 |
| - hospitalised (d) | 11 ± 13 | 5 ± 6 | 0.018 |
| - hospitalised ≤ 5 days | 44% | 63% | 0.291 |
| Age (years) | 75 ± 12 | 74 ± 10 | 0.310 |
| Haemoglobin (mg/dL) | 119 ± 20 | 124 ± 20 | 0.060 |
| Leucocytes (/dL) | 9.5 ± 4.0 | 10.3 ± 10.2 | 0.475 |
| Platelets (/dL) | 323 ± 127 | 288 ± 116 | 0.052 |
| Estimated glomerular filtration rate (mL/min) | 55 ± 19 | 64 ± 23 | 0.004 |
| Total cholesterol (mg/dl) | 4.1 ± 1.1 | 4.4 ± 1.2 | 0.196 |
| Low-density lipoprotein cholesterol (mg/dL) | 2.0 ± 0.9 | 2.2 ± 1.0 | 0.195 |
| High-density lipoprotein cholesterol (mg/dL) | 1.4 ± 0.4 | 1.3 ± 0.4 | 0.194 |
| Triglycerides (mg/dL) | 1.5 ± 0.8 | 1.8 ± 0.9 | 0.031 |
| International Normalized Ratio | 1.2 ± 0.4 | 1.2 ± 0.4 | 0.342 |
| HbA1c (mmol/mol) | 43 ± 8 | 56 ± 23 | 0.072 |
| Systolic blood pressure (mmHg) | 147 ± 22 | 151 ± 21 | 0.242 |
| Diastolic blood pressure (mmHg) | 82 ± 13 | 83 ± 11 | 0.637 |
| Fontaine III (n) | 10 | 13 | 0.318 |
| Fontaine IV (n) | 96 | 80 | 0.318 |
| Baseline ankle brachial pressure index | 0.43 ± 0.28 | 0.44 ± 0.21 | 0.831 |
| Ulcer known since (d) | 138 ± 147 | 187 ± 323 | 0.258 |
| Diabetes mellitus (n) | 64 | 61 | 0.562 |
| Type 1 (n) | 11 | 3 | |
| Type 2 (n) | 53 | 58 | |
| Chronic kidney disease (n) | 59 | 51 | 0.849 |
| Arterial hypertension (n) | 88 | 83 | 0.267 |
| Coronary artery disease (n) | 45 | 38 | 0.821 |
| Chronic heart failure (n) | 19 | 20 | 0.548 |
| Stroke (n) | 7 | 15 | 0.035 |
| Cancer (n) | 10 | 14 | 0.235 |
| Chronic lung disease (n) | 26 | 24 | 0.836 |
| Atrial fibrillation (n) | 28 | 25 | 0.973 |
| Smoker (n) | 17 | 22 | 0.067 |
| Ex-Smoker (n) | 81 | 60 | |
| Oral anticoagulation (n) | 31 | 29 | 0.396 |
| Warfarin (n) | 16 | 5 | |
| Rivaroxaban (n) | 6 | 7 | |
| Apixaban (n) | 9 | 15 | |
| Metformin (n) | 28 | 44 | 0.002 |
| Insulin (n) | 36 | 27 | 0.457 |
| Aspirin (n) | 48 | 32 | 0.119 |
| Clopidogrel (n) | 42 | 32 | 0.418 |
| Rivaroxaban 2.5 mg BID (n) | 4 | 4 | |
| Statin (n) | 54 | 71 | <0.001 |
| Ezetimibe (n) | 0 | 0 | |
| PCSK9 (n) | 1 | 1 | |
| Angiotensin-converting enzyme inhibitor/Angiotensin receptor blocker (n) | 57 | 62 | 0.145 |
| Beta blocker (n) | 34 | 39 | 0.236 |
| Diuretic (n) | 2 | 0 | 0.325 |
| Calcium channel blocker (n) | 26 | 19 | 0.382 |
| Pre-COVID-19 | During COVID-19 | p | |
|---|---|---|---|
| 07/2018–02/2020 | 03/2020–07/2021 | ||
| Iliac (n) | 10 | 14 | |
| Femoral (n) | 67 | 55 | |
| Popliteal (n) | 34 | 42 | |
| Crural (n) | 63 | 47 | |
| Number treated levels (n [1/2/3/4]) | 49/41/14/2 | 43/31/18/1 | |
| Recanalisation (n) | 87 | 79 | |
| Total lesion length (mm) | 141 ± 97 | 253 ± 158 | <0.001 |
| Stenting (n patients) | 55 | 53 | |
| Bare metal stents (n implanted) | 49 | 45 | |
| Drug eluting stents (n implanted) | 36 | 39 | |
| Total stent length (mm) | 135 ± 95 | 87 ± 82 | 0.005 |
| Drug coated balloons (n patients) | 18 | 49 | |
| Total length drug-coated balloon (mm) | 157 ± 98 | 163 ± 123 | 0.815 |
| Fluoroscopy time (s) | 1294 ± 1010 | 1398 ± 756 | 0.450 |
| Contrast volume (mL) | 89 ± 40 | 97 ± 37 | 0.187 |
| Technical success | 92% | 91% | 0.593 |
| Post procedure ankle brachial pressure index | 0.81 ± 0.19 | 0.87 ± 0.20 | 0.045 |
| Delta ankle brachial pressure index (post-baseline) | 0.37 ± 0.31 | 0.42 ± 0.22 | 0.210 |
| Increased ankle brachial pressure index (increased/unchanged/decreased) | 91%/6%/3% | 96%/3%/1% | 0.183 |
| Minor procedure related complication (n) | 5 | 3 | 0.594 |
| Minor | 5% | 3% | |
| Spurious aneurysm (n) | 0 | 0 | |
| AV fistula (n) | 0 | 0 | |
| Hematoma (n) | 5 | 3 | |
| Major/Life threatening (n) | 0 | 0 | |
| Length of stay (d, (IQR)) | 36 (46) | 25 (36) | <0.001 |
| All | Pre-COVID-19 | During COVID-19 | p (Log Rank Mantel-Cox) | |
|---|---|---|---|---|
| Events | 07/2018–02/2020 | 03/2020–07/2021 | ||
| 30-day wound healing | 11 (7%) | 5 (6%) | 6 (9%) | 0.911 |
| Day cases | 11 (12%) | 5 (12%) | 6 (12%) | 0.911 |
| Hospitalised | 0 | 0 | 0 | |
| p (log rank Mantel-Cox) | 0.010 | 0.024 | 0.169 | |
| 30-day mortality | 9 (4%) | 4 (4%) | 5 (6%) | 0.558 |
| Day cases | 4 (4%) | 1 (2%) | 3 (1%) | 0.451 |
| Hospitalised | 5 (7%) | 3 (6%) | 2 (10%) | 0.538 |
| p (log rank Mantel-Cox) | 0.230 | 0.333 | 0.294 | |
| 30-day amputation | 2 (1%) | 0 | 2 (3%) | 0.212 |
| Day cases | 2 (2%) | 0 | 2 (4%) | 0.212 |
| Hospitalised | 0 | 0 | 0 | |
| p (log rank Mantel-Cox) | 0.287 | 0.469 | ||
| 30-day target lesion revascularisation | 4 (2%) | 2 (2%) | 2 (2%) | 0.734 |
| Day cases | 2 (2%) | 1 (2%) | 1 (1%) | 0.866 |
| Hospitalised | 2 (3%) | 1 (2%) | 1 (5%) | 0.461 |
| p (log rank Mantel-Cox) | 0.568 | 0.866 | 0.488 |
| All | Pre-COVID-19 | During COVID-19 | p (Log Rank Mantel-Cox) | ||||
|---|---|---|---|---|---|---|---|
| 07/2018–02/2020 | 03/2020–07/2021 | ||||||
| Events (n) | Median (95%CI) | Events (n) | Median (95%CI) | Events (n) | Median (95%CI) | ||
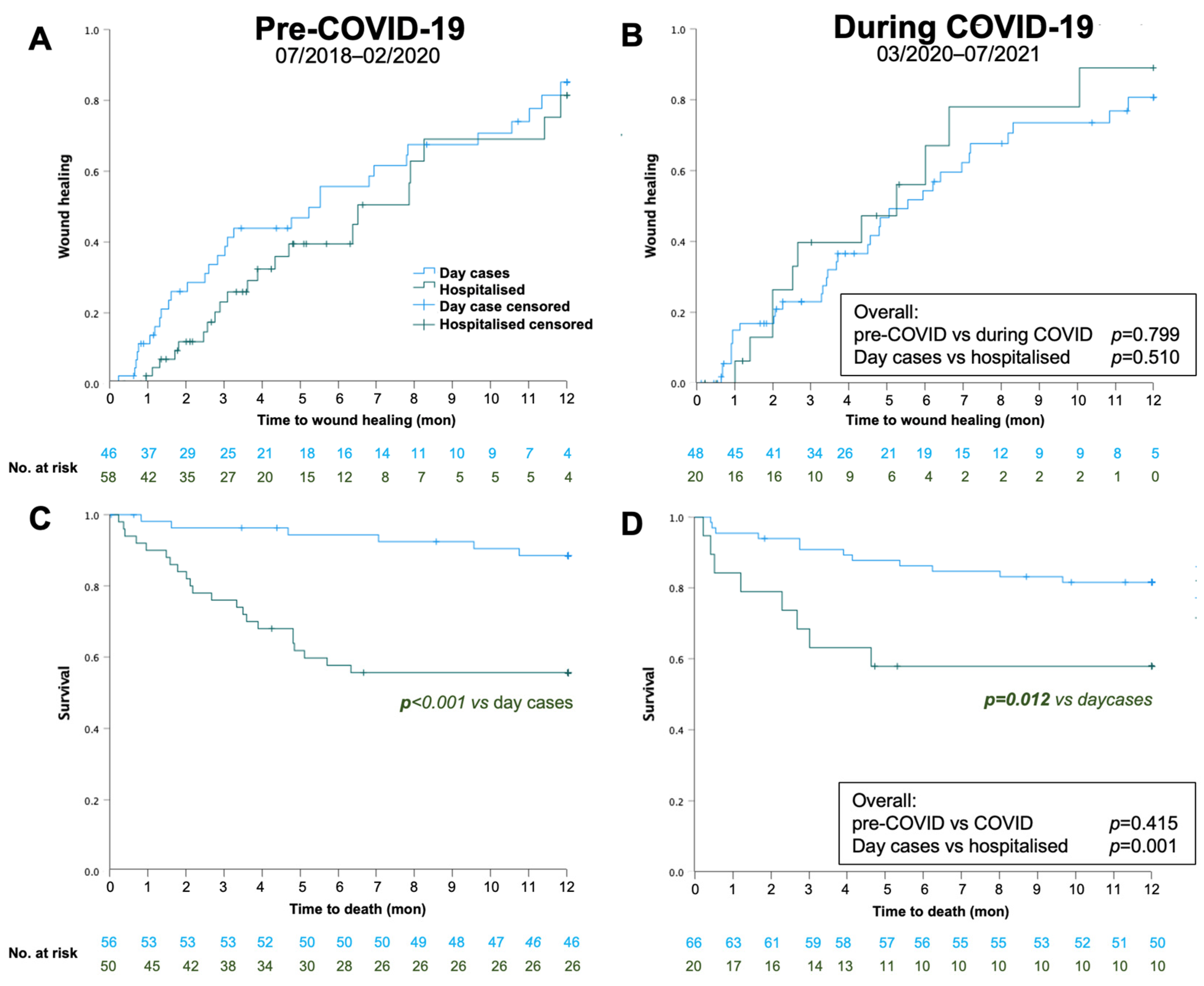
| 1-year wound healing | 98 (83%) | 169 (132, 205) | 52 (83%) | 194 (141, 247) | 46 (83%) | 160 (114, 206) | 0.746 |
| Day cases | 65 (83%) | 168 (129, 207) | 31 (85%) | 168 (75, 261) | 34 (81%) | 169 (119, 219) | 0.666 |
| Hospitalised | 33 (84%) | 194 (139, 249) | 21 (81%) | 198 (123, 273) | 12 (90%) | 160 (31, 289) | 0.234 |
| p (log rank Mantel-Cox) | 0.609 | 0.248 | 0.493 | ||||
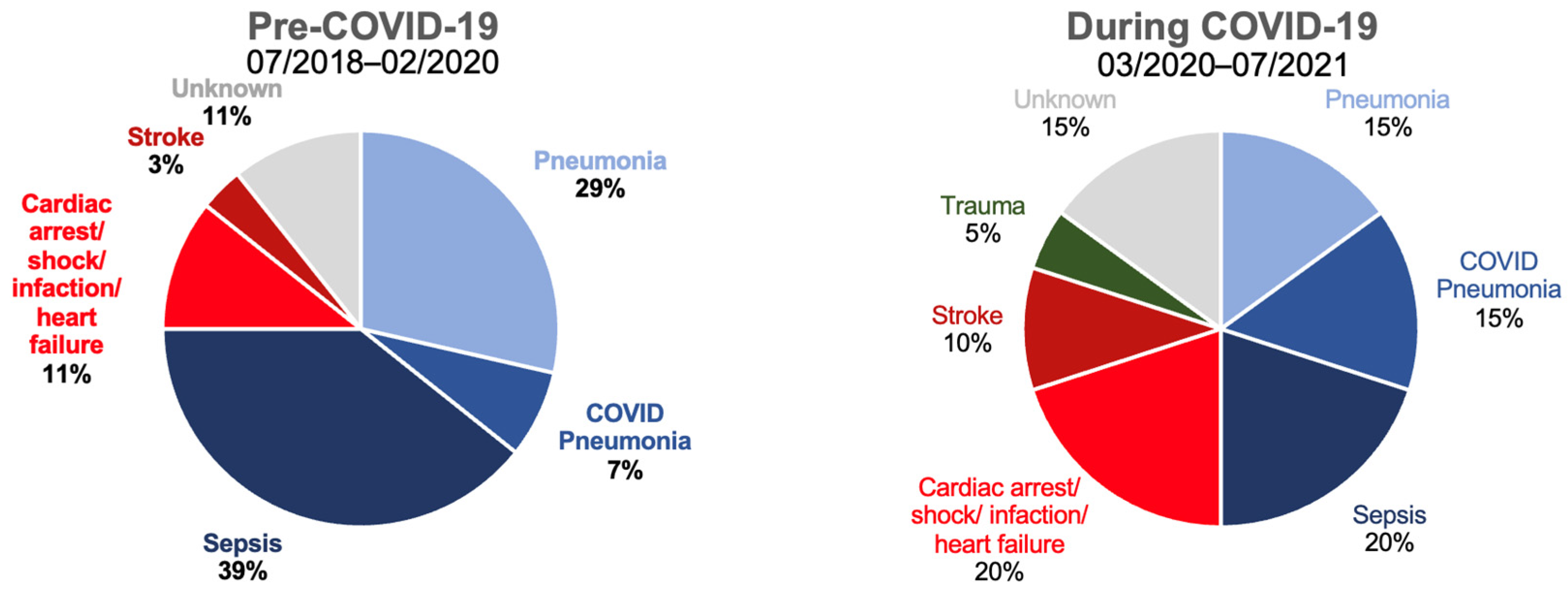
| 1-year mortality | 47 (25%) | 297 (280, 315) | 27 (26%) | 294 (271, 318) | 20 (24%) | 300 (274, 326) | 0.381 |
| Day cases | 17 (14%) | 330 (314, 347) | 5 (10%) | 343 (323, 362) | 12 (18%) | 319 (294, 344) | 0.268 |
| Hospitalised | 30 (43%) | 239 (205, 274) | 22 (44%) | 241 (202, 281) | 8 (40%) | 235 (166, 305) | 0.913 |
| p (log rank Mantel-Cox) | <0.001 | <0.001 | 0.012 | ||||
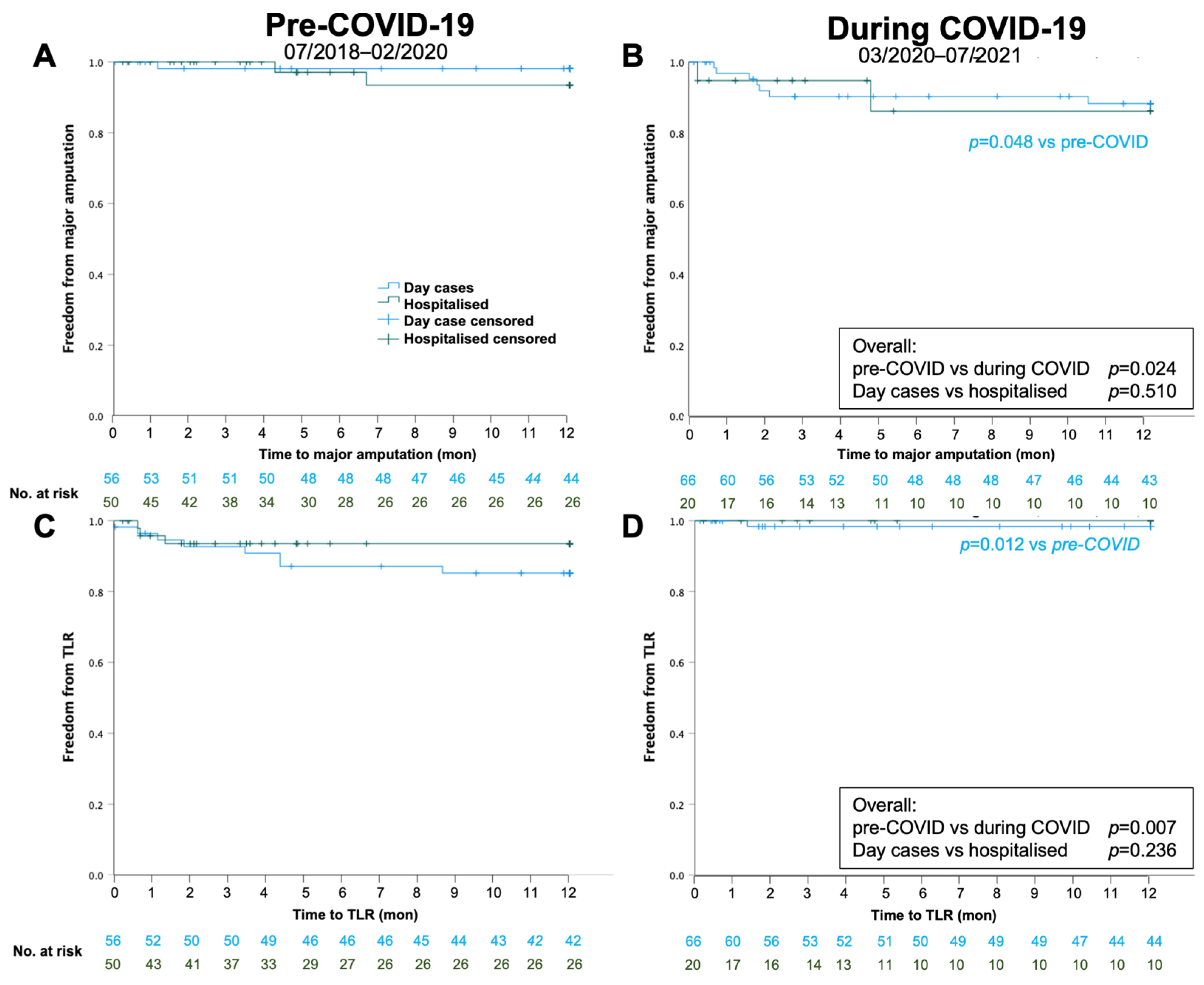
| 1-year amputation | 12 (7%) | 346 (335,357) | 3 (3%) | 357 (347, 366) | 9 (12%) | 332 (311, 353) | 0.024 |
| Day cases | 8 (7%) | 345 (331, 359) | 1 (2%) | 359 (347, 371) | 7 (12%) | 333 (309, 357) | 0.048 |
| Hospitalised | 4 (8%) | 346 (327, 364) | 2 (7%) | 352 (335, 369) | 2 (13%) | 327 (278, 376) | 0.271 |
| p (log rank Mantel-Cox) | 0.510 | 0.360 | 0.873 | ||||
| 1-year TLR | 12 (7%) | 345 (333, 356) | 11 (12%) | 1 (1%) | 0.007 | ||
| Day cases | 9 (8%) | 343 (328, 357) | 8 (15%) | 1 (2%) | 0.012 | ||
| Hospitalised | 3 (5%) | 349 (332, 367) | 3 (6%) | 0 | 0.309 | ||
| p (log rank Mantel-Cox) | 0.236 | 0.272 | 0.617 | ||||
| Hazard Ratio (95% CI) | p | |
|---|---|---|
| Age | 1.05 (1.01, 1.08) | 0.014 |
| Male sex | 0.95 (0.48, 1.89) | 0.894 |
| Hospitalised | 4.50 (1.94, 10.40) | <0.001 |
| ABPI baseline | 1.10 (0.32, 3.76) | 0.884 |
| Time to procedure | 1.00 (0.97, 10.3) | 0.879 |
| During COVID-19 | 1.35 (0.70, 2.63) | 0.369 |
| Diabetes mellitus | 1.14 (0.50, 2.59) | 0.749 |
| Coronary artery disease | 1.99 (1.02, 3.91) | 0.044 |
| Statin | 1.52 (0.73, 3.14) | 0.259 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodway, A.D.; Harris, J.; Hanna, L.; Allan, C.; Casal, F.P.; Giltinan, C.; Dehghan-Nayeri, A.; Santos, A.; Whyte, M.B.; Ntagiantas, N.; et al. Understanding the Impact of COVID-19 on Angioplasty Service and Outcome of Patients Treated for Chronic Limb-Threatening Ischaemia: A Single-Centre Retrospective Cohort Study. Biomedicines 2023, 11, 2034. https://doi.org/10.3390/biomedicines11072034
Rodway AD, Harris J, Hanna L, Allan C, Casal FP, Giltinan C, Dehghan-Nayeri A, Santos A, Whyte MB, Ntagiantas N, et al. Understanding the Impact of COVID-19 on Angioplasty Service and Outcome of Patients Treated for Chronic Limb-Threatening Ischaemia: A Single-Centre Retrospective Cohort Study. Biomedicines. 2023; 11(7):2034. https://doi.org/10.3390/biomedicines11072034
Chicago/Turabian StyleRodway, Alexander D., Jenny Harris, Lydia Hanna, Charlotte Allan, Felipe Pazos Casal, Ciara Giltinan, Ali Dehghan-Nayeri, Andre Santos, Martin B. Whyte, Nikolaos Ntagiantas, and et al. 2023. "Understanding the Impact of COVID-19 on Angioplasty Service and Outcome of Patients Treated for Chronic Limb-Threatening Ischaemia: A Single-Centre Retrospective Cohort Study" Biomedicines 11, no. 7: 2034. https://doi.org/10.3390/biomedicines11072034