


Temporary Occlusion of Common Carotid Arteries Does Not Evoke Total Inhibition in the Activity of Corticospinal Tract Neurons in Experimental Conditions
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
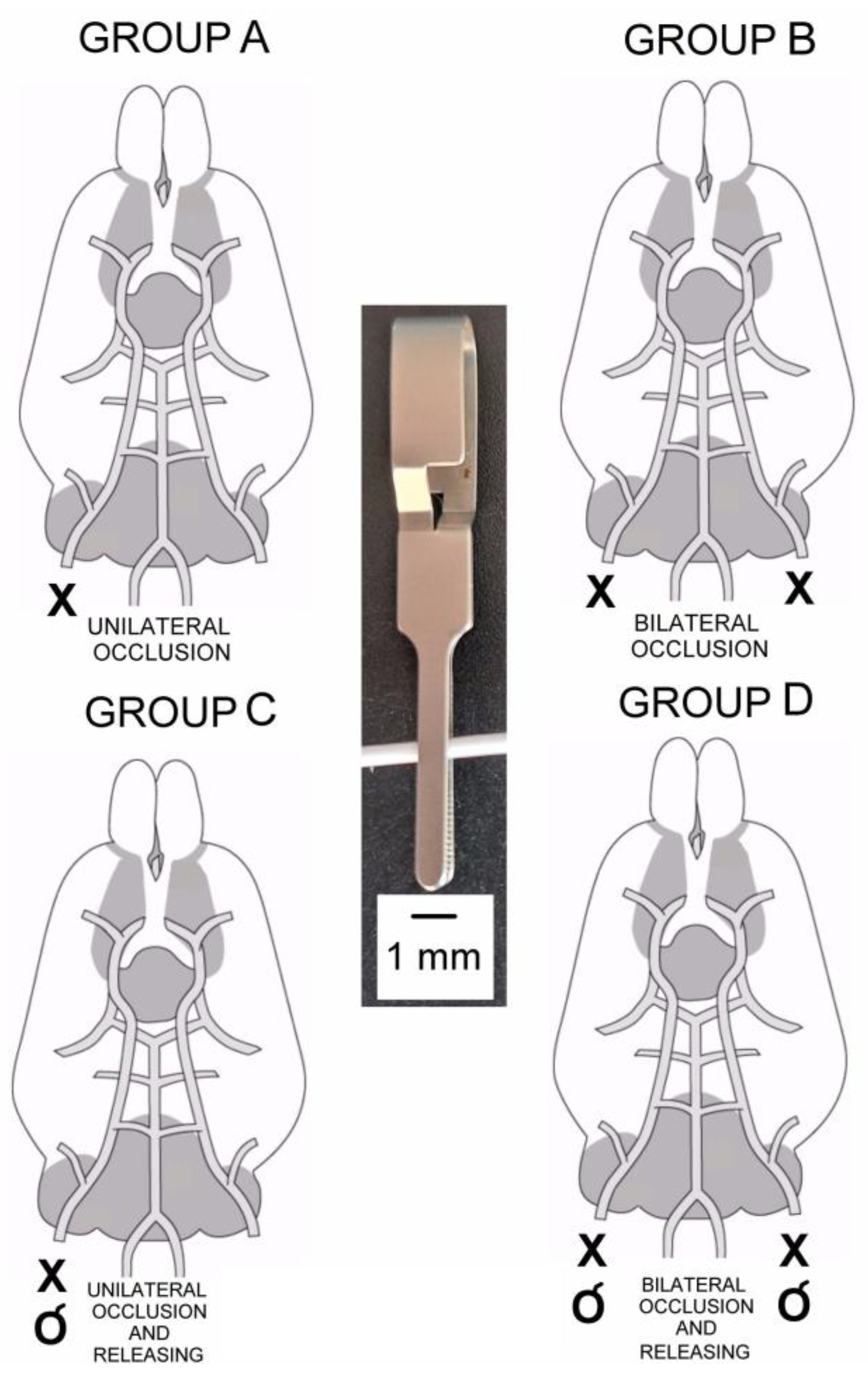
2.1. Animals and Study Design
2.2. Anesthesia and Surgical Procedures
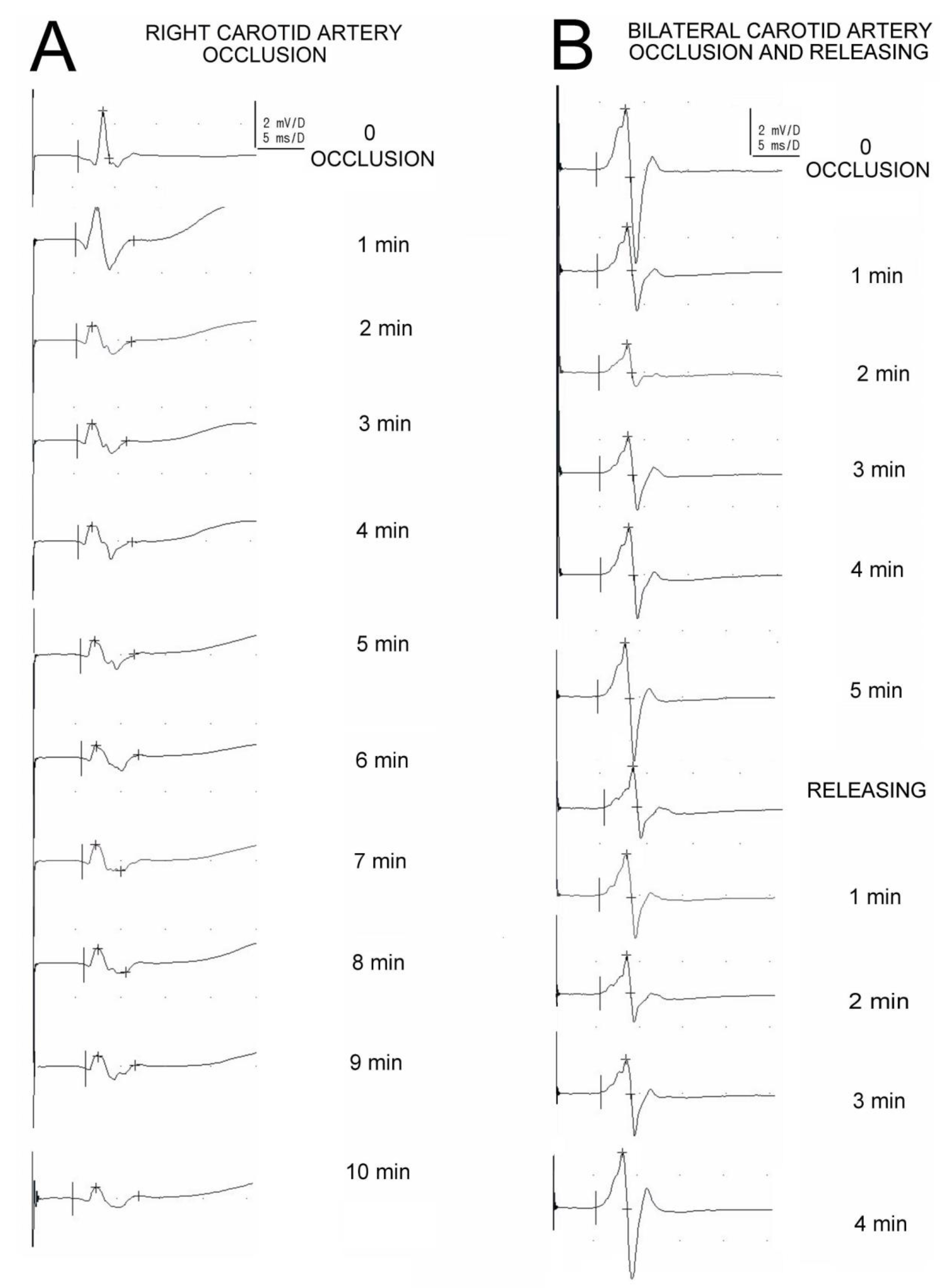
2.3. Electrophysiological Recordings
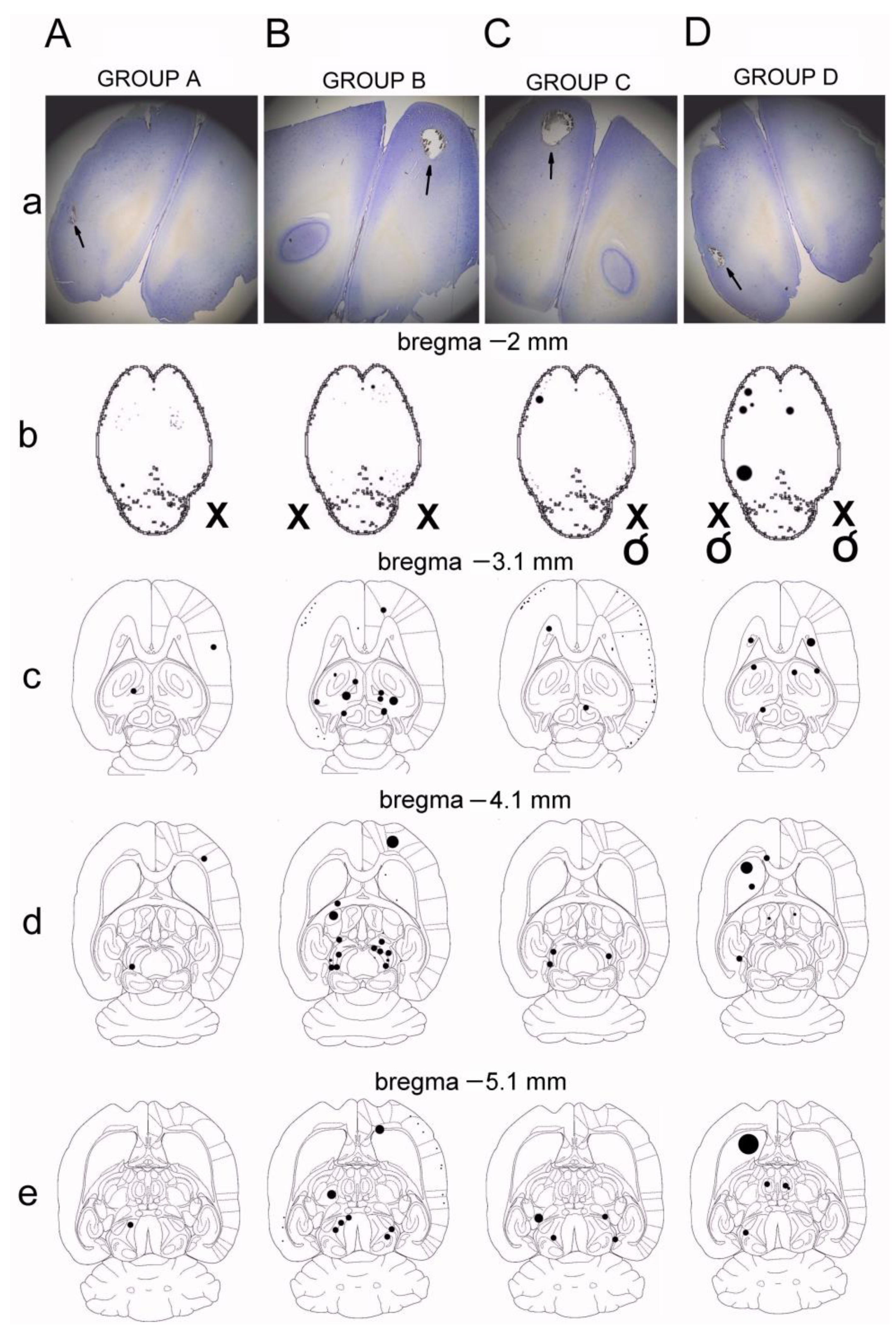
2.4. Histological Verification of Ischemia
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Lopez, A.D. Mortality by cause for eight regions of the world: Global Burden of Disease Study. Lancet 1997, 349, 1269–1276. [Google Scholar] [CrossRef] [PubMed]
- Foerch, C.; Sitzer, M.; Steinmetz, H.; Neumann-Haefelin, T. Arbeitsgruppe Schlaganfall Hessen. Future demographic trends decrease the proportion of ischemic stroke patients receiving thrombolytic therapy: A call to set-up therapeutic studies in the very old. Stroke 2009, 40, 1900–1902. [Google Scholar] [CrossRef]
- Khaja, A.M.; Grotta, J.C. Established treatments for acute ischaemic stroke. Lancet 2007, 369, 319–330. [Google Scholar] [CrossRef]
- Hossmann, K.A. Pathophysiology and therapy of experimental stroke. Cell Mol. Neurobiol. 2006, 26, 1057–1083. [Google Scholar] [CrossRef] [PubMed]
- Sashadri, S.; Beiser, A.; Kelly-Hayes, M.; Kase, C.S.; Au, R.; Kannel, W.B.; Wolf, P.A. The lifetime risk of stroke: Estimates from the Framingham Study. Stroke 2006, 37, 345–350. [Google Scholar] [CrossRef]
- Hossmann, K.A. Cerebral ischemia: Models methods and outcomes. Neuropharmacology 2008, 55, 257–270. [Google Scholar] [CrossRef]
- Woodruff, T.M.; Thundyil, J.; Tang, S.-H.; Sobey, C.; Taylor, S.M. Pathophysiology, treatment and animal and cellular models of human ischemic stroke. Mol. Neurodegener. 2011, 6, 11. [Google Scholar] [CrossRef]
- Harukuni, I.; Bhardwaj, A. Mechanism of brain injury after global cerebral ischemia. Neurol. Clin. 2006, 24, 1–21. [Google Scholar] [CrossRef]
- Ward, N.S. Mechanisms underlying recovery of motor function after stroke. Postgrad. Med. J. 2005, 81, 510–514. [Google Scholar] [CrossRef]
- Macdonell, R.A.; Donnan, G.A.; Bladin, P.F. A comparison of somatosensory evoked and motor evoked potentials in stroke. Ann. Neurol. 1989, 25, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Feys, H.; Van Hees, J.; Bruyninckx, F.; Mercelis, R.; De Weerdt, W. Value of somatosensory and motor evoked potentials in predicting arm recovery after a stroke. J. Neurol. Neurosurg. Psych. 2000, 68, 323–331. [Google Scholar] [CrossRef]
- Rossini, P.M.; Pauri, F. Transcranial magnetic stimulation in stroke. In Magnetic Stimulation in Clinical Neurophysiology; Hallett, M., Chakroverty, S., Eds.; Elsevier, Butterworth Heinemann: Philadelphia, PA, USA, 2005; pp. 239–252. [Google Scholar]
- Nascimbeni, A.; Gaffuri, A.; Imazio, P. Motor evoked potentials: Prognostic value in motor recovery after stroke. Fund. Neurol. 2006, 21, 199–203. [Google Scholar]
- Vang, C.; Dunbabin, D.; Kilpatrick, D. Correlation between functional and electrophysiological recovery in acute ischemic stroke. Stroke 1999, 30, 2126–2130. [Google Scholar] [CrossRef] [PubMed]
- D’Olhaberriague, L.; Espadaler Gamissans, J.M.; Marrugat, J.; Valls, A.; Oliveras Ley, C.; Seoane, J.L. Transcranial magnetic stimulation as a prognostic tool in stroke. J. Neurol. Sci. 1997, 147, 73–80. [Google Scholar] [CrossRef]
- Catano, A.; Houa, M.; Caroyer, J.M.; Ducarne, H.; Noel, P. Magnetic transcranial stimulation in acute stroke: Early excitation threshold and functional prognosis. Electroencephalogr. Clin. Neurophysiol. 1996, 101, 233–239. [Google Scholar] [CrossRef]
- Timmerhuis, T.P.J.; Hageman, G.; Oosterloo, S.J.; Rozeboom, A.R. The prognostic value of cortical magnetic stimulation in acute middle cerebral artery infraction compared of other parameters. Clin. Neurol. Neurosurg. 1996, 98, 231–236. [Google Scholar] [CrossRef]
- Weber, M.; Eisen, A.A. Magnetic stimulation of central and peripheral nervous systems. Muscle Nerve 2002, 25, 160–175. [Google Scholar] [CrossRef]
- Simpson, R.K.; Baskin, D.S. Early component changes in corticomotor evoked potentials following experimental stroke. Stroke 1987, 18, 1141–1147. [Google Scholar] [CrossRef]
- Shao, Y. Cortical evoked potential changes in a rat model of acute ischemic stroke. Detection of somatosensory evoked potential and motor evoked potential. Neural. Regener. Res. 2010, 5, 550–554. [Google Scholar]
- North American Symptomatic Carotid Endarterectomy Trial Collaborators. Beneficial effect of carotied endarterectomy in symptomatic patients with high-grade carotid stenosis. N. Eng. J. Med. 1991, 325, 445–453. [Google Scholar]
- Dougherty, J.H.; Levy, D.E.; Rawlinson, D.G.; Ruff, R.; Weksler, B.B.; Plum, F. Experimental cerebral ischemia produced by extracranial vascular injury: Protection with indomethacin and prostacyclin. Neurology 1982, 32, 970–974. [Google Scholar] [CrossRef] [PubMed]
- Garcia, J.H. Experimental ischemic stroke: A review. Stroke 1984, 15, 5–14. [Google Scholar] [CrossRef]
- Canazza, A.; Minati, L.; Boffano, C.; Parati, E.; Binks, S. Experimental models of brain ischemia: A review of techniques, magnetic resonance imaging, and investigational cell-based therapies. Front. Neurol. 2014, 5, 19. [Google Scholar] [CrossRef] [PubMed]
- Kety, S.S. The Cerebral Circulation. In Handbook of Physiology; Field, J., Magoun, H.W., Hall, V.E., Eds.; American Physiological Society: Bethesda, MD, USA, 1960. [Google Scholar]
- Longa, E.Z.; Weinstein, P.R.; Carlson, S.; Cummins, R. Reversible middle cerebral artery occlusion without craniotomy in rats. Stroke 1989, 20, 84–91. [Google Scholar] [CrossRef]
- Kamida, T.; Fujiki, M.; Hori, S.; Isono, M. Conduction pathways of motor evoked potentials following transcranial magnetic stimulation: A rodent study using a “figure-8” coil. Muscle Nerve 1998, 21, 722–731. [Google Scholar] [CrossRef]
- Hovey, C.; Jalinous, R. The Guide to Magnetic Stimulation; The Magstim Company Limited: Whiteland, UK, 2006. [Google Scholar]
- Czarnecki, P.; Huber, J.; Szukała, A.; Górecki, M.; Romanowski, L. The Usefulness of Motor Potentials Evoked Transvertebrally at Lumbar Levels for the Evaluation of Peroneal Nerve Regeneration after Experimental Repair in Rats. J. Pers. Med. 2023, 13, 438. [Google Scholar] [CrossRef]
- Ferreira, R.; Oliveirall, A.R.; de Barros Filholl, T.E. Standardization of motor evoked potential captivation technique in rats through transcranial electric stimulus. Acta Ortoped Bras. 2005, 13, 112–114. [Google Scholar] [CrossRef]
- Nielsen, J.B.; Perez, M.A.; Oudega, M.; Enriquez- Denton, M.; Aimonetti, J.M. Evaluation of transcranial magnetic stimulation for investigation transmission in descending motor tracts in the rat. Eur. J. Neurosci. 2007, 25, 805–814. [Google Scholar] [CrossRef]
- Linden, R.D.; Zhang, Y.P.; Darlene, A.; Burke, A.; Matthew, A.; Hunt, A.; Harping, J.E.; Shields, C.B. Magnetic motor evoked potentials monitoring in the rat. J. Neurosurg. 1999, 91, 205–210. [Google Scholar] [CrossRef]
- Paxinos, G.; Watson, C. The Rat Brain in Stereotaxic Coordinates; Elsevier: Amsterdam, The Netherlands, 1997; ISBN 9780123919496. [Google Scholar]
- Pellegrino, L.J.; Pellegrino, A.S.; Cushman, A.J. A Stereotaxic Atlas of the Rat Brain, 2nd ed.; Plenum Press: New York, NY, USA, 1979. [Google Scholar]
- Garcia, J.; Yoshida, Y.; Chem, H.; Li, Y.; Zahang, Z.G.; Lian, J.; Chen, S.; Chopp, M. Progression form ischemic injury to infract following middle cerebral artery occlusion in the rat. Am. J. Pathol. 1993, 142, 623–635. [Google Scholar] [PubMed]
- Kakinohana, M.; Nakamura, S.; Fuchigami, T.; Sugahara, K. Transcranial motor-evoked potentials monitoring can detect spinal cord ischemia more rapidly than spinal cord-evoked potentials monitoring during aortic occlusion in rats. Eur. Spine J. 2007, 16, 787–793. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.P.; Shields, L.B.E.; Zhang, Y.; Pei, J.; Hu, X.-M.; Hoskin, R.; Cai, J.; Qiu, M.S. Use of magnetic stimulation to elicit motor evoked potentials, somatosensory evoked potentials and H reflex in no-sedated rodents. J. Neurosci. Meth. 2007, 165, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Arac, N.; Sagduyu, A.; Binai, S.; Ertekin, C. Prognostic value of transcranial magnetic stimulation in acute stroke. Stroke 1994, 25, 2183–2186. [Google Scholar] [CrossRef]
- Escudero, J.V.; Rancho, J.; Bautista, D.; Escudero, M.; Lopez-Trigo, J. Prognostic value of motor evoked potential obtained by transcranial magnetic brain stimulation in motor function in patients with acute ischemic stroke. Stroke 1998, 29, 1854–1859. [Google Scholar] [CrossRef] [PubMed]
- George, M.S.; Nahas, Z.; Kozel, F.A.; Li, X.; Denslow, S.; Yamanaka, K.; Mishory, A.; Foust, M.J.; Bohning, D.E. Mechanisms and state of art of transcranial magnetic stimulation. J. ECT 2000, 18, 170–181. [Google Scholar] [CrossRef]
- Rösler, K.M. Transcranial magnetic brain stimulation: A tool to investigate central motor pathways. News Physiol. Sci. 2001, 16, 297–302. [Google Scholar] [CrossRef]
- Michel-Flutot, P.; Jesus, I.; Mansart, A.; Bonay, M.; Lee, K.Z.; Auré, K.; Vinit, S. Evaluation of Gastrocnemius Motor Evoked Potentials Induced by Trans-Spinal Magnetic Stimulation Following Tibial Nerve Crush in Rats. Biology 2022, 11, 1834. [Google Scholar] [CrossRef]
- Fishback, A.S.; Shields, C.B.; Linden, R.D.; Zhang, Y.P.; Burke, D. The effects of propofol on rat transcranial magnetic motor evoked potentials. Neurosurgery 1995, 37, 969–974. [Google Scholar] [CrossRef]
- Konrad, P.E.; Tacker, W.A.; Levy, W.J.; Reedy, D.P.; Cook, J.R.; Greddes, L.A. Motor evoked potentials in dog: Effects of global ischemia on spinal cord and peripheral nerve signals. Neurosurgery 1987, 20, 117–124. [Google Scholar] [CrossRef]
- Mathew, P.; Bullock, R.; Graham, D.I.; Maxwell, W.L.; Teasdale, G.M.; McCulloch, J. A new experimental model of contusion in the rat. Histopathological analysis and temporal patterns of cerebral blood flow disturbances. J. Neurosurg. 1996, 85, 860–870. [Google Scholar] [CrossRef] [PubMed]
- Nagasawa, H.; Kogure, K. Correlation between cerebral blood flow and histologic in a new model of middle cerebral artery occlusion. Stroke 1989, 20, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Carmichael, S.T. Rodent models of focal stroke: Size, mechanism, and purpose. NeuroRx J. Am. Soc. Exp. NeuroTherapeutics 2005, 2, 396–409. [Google Scholar] [CrossRef] [PubMed]
- Seitz, R.J.; Bütefisch, C.M.; Kleiser, R.; Hömberg, V. Reorganization of cerebral circuits in human ischemic brain disease. Restor. Neurol. Neurosci. 2004, 22, 207–229. [Google Scholar] [PubMed]
- Pennisi, G.; Rapisarda, G.; Bella, R.; Calabrese, V.; Maertens de Noordhout, A.; Delwaide, P.J. Prognostic value for hand motor recovery absence of response to early transcranial magnetic stimulation in ischemic stroke potentials. Stroke 1999, 30, 2666–2670. [Google Scholar] [CrossRef]
- Ciobanu, O.; Elena Sandu, R.; Tudor Balseanu, A.; Zavaleanu, A.; Gresita, A.; Petcu, E.B.; Uzoni, A.; Popa-Wagner, A. Caloric restriction stabilizes body weight and accelerates behavioral recovery in aged rats after focal ischemia. Aging Cell 2017, 16, 1394–1403. [Google Scholar] [CrossRef]
- Arboix, A.; Cabeza, N.; García-Eroles, L.; Massons, J.; Oliveres, M.; Targa, C.; Balcells, M. Relevance of transient ischemic attack to early neurological recovery after nonlacunar ischemic stroke. Cerebrovasc. Dis. 2004, 18, 304–311. [Google Scholar] [CrossRef]
- Rudilosso, S.; Rodríguez-Vázquez, A.; Urra, X.; Arboix, A. The Potential Impact of Neuroimaging and Translational Research on the Clinical Management of Lacunar Stroke. Int. J. Mol. Sci. 2022, 23, 1497. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
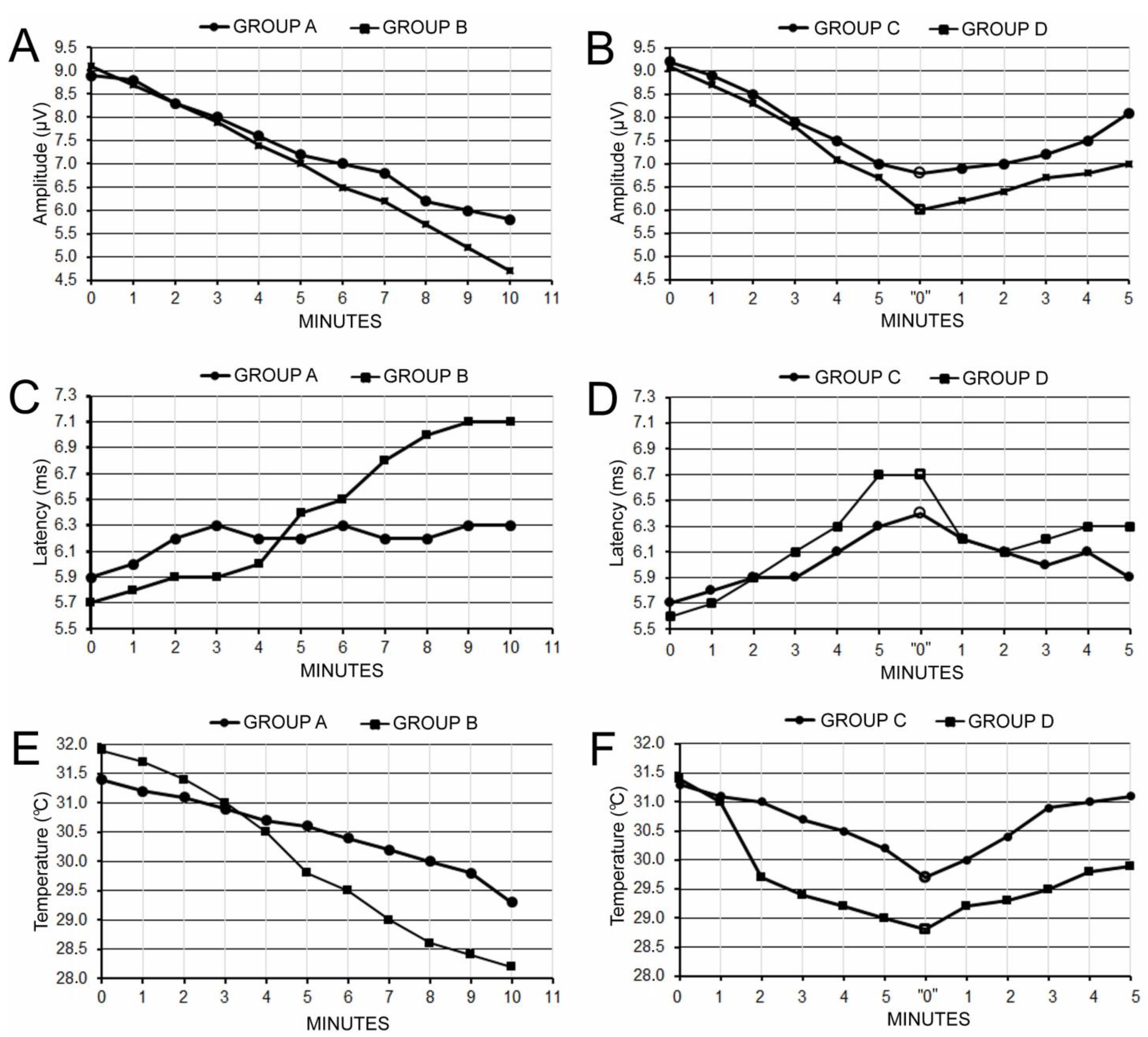
| Amplitude (µV), % of Change | |||||||||||||
| Duration of Ischemia after Carotid Artery Occlusion (min) | |||||||||||||
| Control | Animals Groups | Before | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| 9.2 ± 1.3 (N = 4) | A (N = 10) | 8.9 ± 1.1 | 8.8 ± 1.0 | 8.3 ± 0.9 | 8.0 ± 1.1 | 7.6 ± 0.9 | 7.2 ± 1.2 | 7.0 ± 1.1 | 6.8 ± 0.9 | 6.2 ± 1.0 | 6.0 ± 1.2 | 5.8 ± 1.1 | |
| −100% | −1.20% | −6.80% | −10.10% | −14.60% | −19.10% | −20.30% | −23.60% | −30.30% | −32.60% | −34.80% | |||
| B (N = 11) | 9.1 ± 1.3 | 8.7 ± 1.0 | 8.3 ± 0.7 | 7.9 ± 0.8 | 7.4 ± 0.9 | 7.0 ± 1.0 | 6.5 ± 1.1 | 6.2 ± 0.9 | 5.7 ± 1.1 | 5.2 ± 1.0 | 4.7 ± 0.9 | ||
| −100% | −4.40% | −8.80% | −13.20% | −18.70% | −23.10% | −28.60% | −31.90% | −37.40% | −42.90% | −48.40% | |||
| Occlusion duration (min) | Occlusion releasing duration (min) | ||||||||||||
| Animals Groups | Before | 1 | 2 | 3 | 4 | 5 | “0” | 1 | 2 | 3 | 4 | 5 | |
| C (N = 10) | 9.2 ± 1.2 | 8.9 ± 1.0 | 8.5 ± 1.0 | 7.9 ± 1.0 | 7.5 ± 0.8 | 7.0 ± 1.0 | 6.8 ± 0.9 | 6.9 ± 1.0 | 7.0 ± 0.9 | 7.2 ± 1.2 | 7.5 ± 1.1 | 8.1 ± 1.1 | |
| −100% | −3.30% | −7.60% | −14.10% | −18.50% | −23.90% | −26.10% | −25.00% | −23.90% | −21.70% | −18.40% | −11.90% | ||
| D (N = 11) | 9.1 ± 1.3 | 8.7 ± 0.9 | 8.3 ± 0.9 | 7.8 ± 1.0 | 7.1 ± 1.0 | 6.7 ± 0.7 | 6.0 ± 1.1 | 6.2 ± 1.1 | 6.4 ± 0.8 | 6.7 ± 3.1 | 6.8 ± 0.8 | 7.0 ± 0.9 | |
| −100% | −4.40% | −8.80% | −14.30% | −21.90% | −26.30% | −34.10% | −31.80% | −10.90% | −11.00% | −25.20% | −23.00% | ||
| Latency (ms) | |||||||||||||
| 5.8 ± 0.8 (N = 4) | Duration of Ischemia After Carotid Artery Occlusion (min) | ||||||||||||
| Animals Groups | Before | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | ||
| A (N = 10) | 5.9 ± 0.8 | 6.0 ± 0.8 | 6.2 ± 0.6 | 6.3 ± 0.9 | 6.2 ± 0.5 | 6.2 ± 0.9 | 6.3 ± 0.7 | 6.2 ± 0.7 | 6.2 ± 0.7 | 6.3 ± 0.7 | 6.3 ± 0.8 | ||
| B (N = 11) | 5.7 ± 0.7 | 5.8 ± 0.7 | 5.9 ± 0.8 | 5.9 ± 0.7 | 6.0 ± 0.7 | 6.4 ± 0.5 | 6.5 ± 0.8 | 6.8 ± 0.8 | 7.0 ± 0.9 | 7.1 ± 0.9 | 7.1 ± 0.8 | ||
| Occlusion duration (min) | Occlusion releasing duration (min) | ||||||||||||
| Animals Groups | Before | 1 | 2 | 3 | 4 | 5 | “0” | 1 | 2 | 3 | 4 | 5 | |
| C (N = 10) | 5.7 ± 0.4 | 5.8 ± 0.8 | 5.9 ± 0.6 | 5.9 ± 0.4 | 6.1 ± 0.4 | 6.3 ± 0.4 | 6.4 ± 0.4 | 6.2 ± 0.4 | 6.1 ± 0.5 | 6.0 ± 0.5 | 6.1 ± 0.4 | 5.9 ± 0.6 | |
| D (N = 11) | 5.6 ± 0.7 | 5.7 ± 0.5 | 5.9 ± 0.6 | 6.1 ± 0.6 | 6.3 ± 0.6 | 6.7 ± 0.6 | 6.7 ± 0.5 | 6.2 ± 0.5 | 6.1 ± 0.5 | 6.2 ± 0.4 | 6.3 ± 0.4 | 6.3 ± 0.5 | |
| Temperature (°C) | |||||||||||||
| 31.6 ± 1.1 (N = 4) | Duration of Ischemia after Carotid Artery Occlusion (min) | ||||||||||||
| Animals Groups | Before | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | ||
| A (N = 10) | 31.4 ± 1.0 | 31.2 ± 1.2 | 31.1 ± 1.2 | 30.9 ± 1.2 | 30.7 ± 1.1 | 30.6 ± 1.1 | 30.4 ± 0.9 | 30.2 ± 1.1 | 30.0 ± 1.2 | 29.8 ± 1.1 | 29.3 ± 1.1 | ||
| B (N = 11) | 31.9 ± 1.2 | 31.7 ± 1.3 | 31.4 ± 1.2 | 31.0 ± 1.3 | 30.5 ± 0.9 | 29.8 ± 1.2 | 29.5 ± 0.9 | 29.0 ± 1.1 | 28.6 ± 1.0 | 28.4 ± 1.2 | 28.2 ± 1.2 | ||
| Occlusion duration (min) | Occlusion releasing duration (min) | ||||||||||||
| Before | 1 | 2 | 3 | 4 | 5 | “0” | 1 | 2 | 3 | 4 | 5 | ||
| C (N = 10) | 31.3 ± 1.2 | 31.1 ± 1.2 | 31.0 ± 1.0 | 30.7 ± 0.9 | 30.5 ± 1.0 | 30.2 ± 1.0 | 29.7 ± 1.2 | 30.0 ± 1.1 | 30.4 ± 1.0 | 30.9 ± 0.9 | 31.0 ± 1.1 | 31.1 ± 1.0 | |
| D (N = 11) | 31.4 ± 0.9 | 31.0 ± 0.9 | 29.7 ± 1.0 | 29.4 ± 1.0 | 29.2 ± 1.0 | 29.0 ± 1.1 | 28.8 ± 0.9 | 29.2 ± 1.0 | 29.3 ± 0.9 | 29.5 ± 0.9 | 29.8 ± 0.9 | 29.9 ± 0.9 | |
| Observation Periods (Minutes) | Group A | Group B | Group C | Group D | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Amplitude | Latency | Temperature | Amplitude | Latency | Temperature | Amplitude | Latency | Temperature | Amplitude | Latency | Temperature | |
| “0” vs. 5th | 0.06 | 0.05 | 0.05 | 0.06 | 0.04 | 0.04 | 0.04 | 0.05 | 0.05 | 0.03 | 0.04 | 0.04 |
| “0” vs. 10th | 0.01 | 0.05 | 0.03 | 0.009 | 0.03 | 0.02 | 0.05 | 0.07 | 0.07 | 0.04 | 0.05 | 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szymankiewicz-Szukała, A.; Huber, J.; Czarnecki, P.; Wiertel-Krawczuk, A.; Dąbrowski, M. Temporary Occlusion of Common Carotid Arteries Does Not Evoke Total Inhibition in the Activity of Corticospinal Tract Neurons in Experimental Conditions. Biomedicines 2023, 11, 1287. https://doi.org/10.3390/biomedicines11051287
Szymankiewicz-Szukała A, Huber J, Czarnecki P, Wiertel-Krawczuk A, Dąbrowski M. Temporary Occlusion of Common Carotid Arteries Does Not Evoke Total Inhibition in the Activity of Corticospinal Tract Neurons in Experimental Conditions. Biomedicines. 2023; 11(5):1287. https://doi.org/10.3390/biomedicines11051287
Chicago/Turabian StyleSzymankiewicz-Szukała, Agnieszka, Juliusz Huber, Piotr Czarnecki, Agnieszka Wiertel-Krawczuk, and Mikołaj Dąbrowski. 2023. "Temporary Occlusion of Common Carotid Arteries Does Not Evoke Total Inhibition in the Activity of Corticospinal Tract Neurons in Experimental Conditions" Biomedicines 11, no. 5: 1287. https://doi.org/10.3390/biomedicines11051287