
Synchronous Breast and Cervical Carcinoma: A Genetic Point of View

Abstract
:1. Introduction
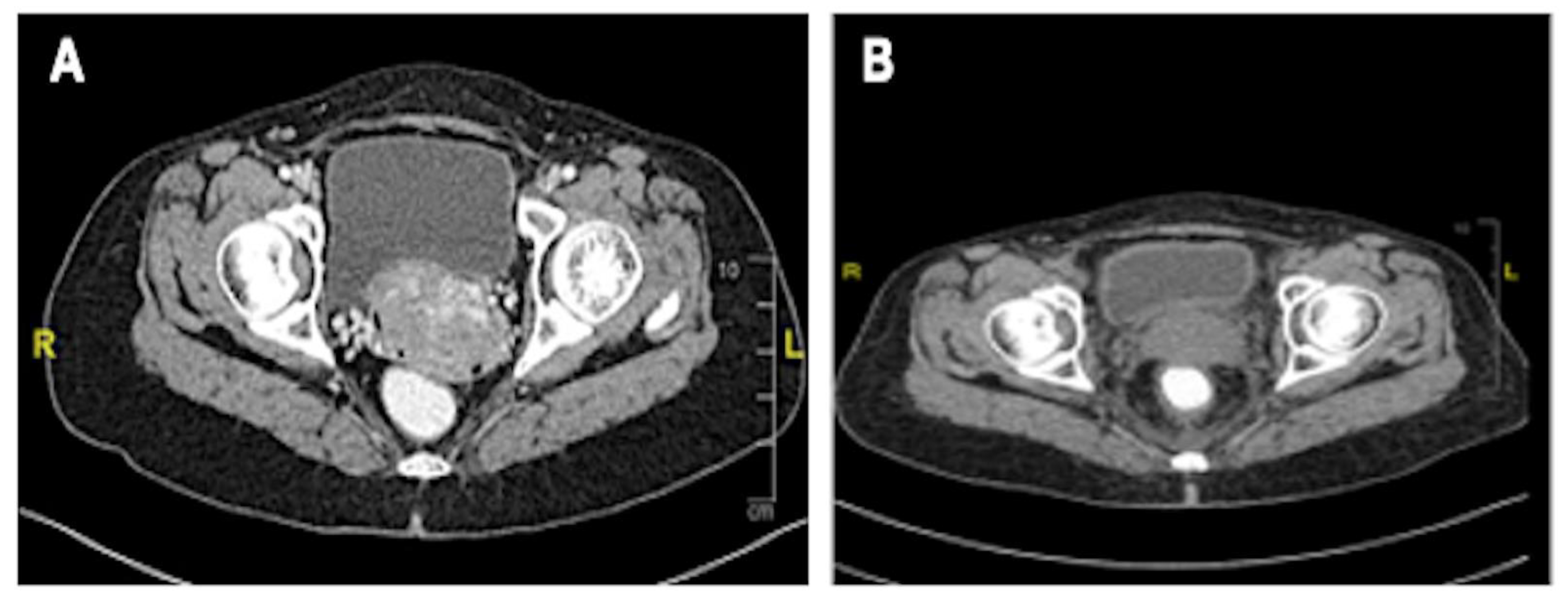
2. Case Presentation
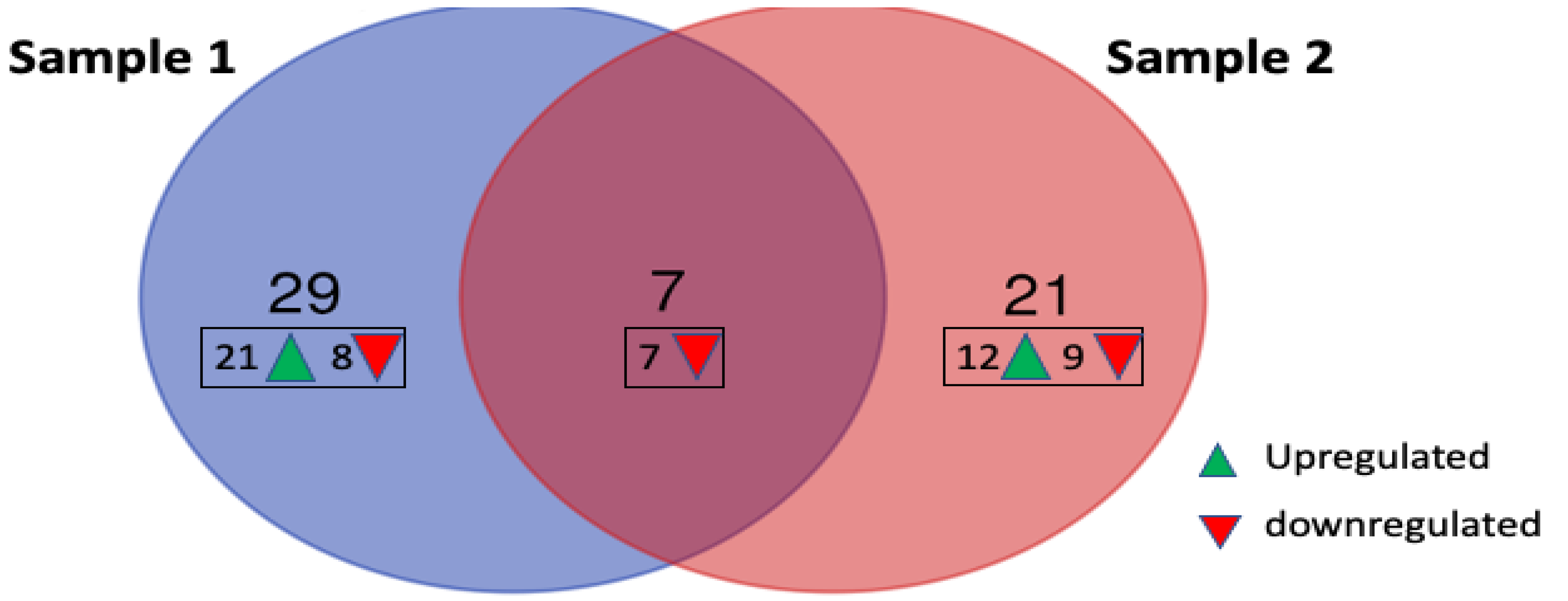
3. Gene Expression Profiling
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thouvenot, A.; Bizet, Y.; Baccar, L.S.; Lamuraglia, M. Primary breast cancer relapse as metastasis to the cervix uteri: A case report. Mol. Clin. Oncol. 2018, 9, 96–97. [Google Scholar] [CrossRef] [PubMed]
- Jin, L.; Han, B.; Siegel, E.; Cui, Y.; Giuliano, A.; Cui, X. Breast cancer lung metastasis: Molecular biology and therapeutic implications. Cancer Biol. Ther. 2018, 19, 858–868. [Google Scholar] [CrossRef] [PubMed]
- Cholmondeley, K.; Callan, L.; Sangle, N.; D’Souza, D. Metastatic cervical adenocarcinoma to the breast: A case report and literature review. Gynecol. Oncol. Rep. 2019, 28, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Padegaonkar, A.; Chadha, P.; Shetty, A. A rare case of synchronous cervical and breast carcinoma. Indian J. Surg. Oncol. 2018, 9, 622–623. [Google Scholar] [CrossRef] [PubMed]
- Azizah, A.M.; Hashimah, B.; Nirmal, K.; Siti Zubaidah, A.R.; Puteri, N.A.; Nabihah, A.; Sukumaran, R.; Balqis, B.; Nadia, S.M.R.; Sharifah, S.S.S.; et al. Malaysia National Cancer Registry Report (MNCR) 2012-2016; National Cancer Institute: Putrajaya, Wilayah, 2019; pp. 1–116. [Google Scholar]
- Norsa’adah, B.; Rampal, K.G.; Rahmah, M.A.; Naing, N.N.; Biswal, B.M. Diagnosis delay of breast cancer and its associated factors in Malaysian women. BMC Cancer 2011, 11, 141. [Google Scholar] [CrossRef] [PubMed]
- Meechan, G.; Collins, J.; Petrie, K.J. The relationship of symptoms and psychological factors to delay in seeking medical care for breast symptoms. Prev. Med. 2003, 36, 374–378. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Breast Cancer; Version 3; National Comprehensive Cancer Network: Plymouth Meeting, PA, USA, 2020. [Google Scholar]
- Goldhirsch, A.; Winer, E.P.; Coates, A.S.; Gelber, R.D.; Piccart-Gebhart, M.; Thürlimann, B.; Senn, H.J.; Albain, K.S.; André, F.; Bergh, J.; et al. Personalizing the treatment of women with early breast cancer: Highlights of the St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2013. Ann. Oncol. 2013, 24, 2206–2223. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Breast Cancer; Version 4; National Comprehensive Cancer Network: Plymouth Meeting, PA, USA, 2022. [Google Scholar]
- Robert, N.J.; Denduluri, N. Patient case lessons: Endocrine management of advanced breast cancer. Clin. Breast Cancer 2018, 18, 192–204. [Google Scholar] [CrossRef]
- Mallik, D.; Ravi, B.; Kumar, N.; Chattopadhyay, D.; Syed, A.; Joshi, P. Invasive ductal carcinoma of breast and squamous cell carcinoma of anterior chest wall—A rare collision. Clin. Case Rep. 2020, 8, 1618–1621. [Google Scholar] [CrossRef] [PubMed]
- Chemoradiotherapy for Cervical Cancer Meta-Analysis Collaboration. Reducing uncertainties about the effects of chemoradiotherapy for cervical cancer: Individual patient data meta-analysis. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef]
- Liu, R.; Wang, X.; Tian, J.H.; Yang, K.; Wang, J.; Jiang, L.; Hao, X.Y. High dose rate versus low dose rate intracavity brachytherapy for locally advanced uterine cervix cancer. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- Kokka, F.; Bryant, A.; Brockbank, E.; Powell, M.; Oram, D. Hysterectomy with radiotherapy or chemotherapy or both for women with locally advanced cervical cancer. Cochrane Database Syst. Rev. 2015, 7, CD010260. [Google Scholar] [CrossRef]
- Kristiansen, G.; Sammar, M.; Altevogt, P. Tumour biological aspects of CD24, a mucin-like adhesion molecule. J. Mol. Histol. 2004, 35, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Kim, S.H.; Lee, E.S.; Kim, Y.S. CD24 overexpression in cancer development and progression: A meta-analysis. Oncol. Rep. 2009, 22, 1149–1156. [Google Scholar]
- Fang, X.; Zheng, P.; Tang, J.; Liu, Y. CD24: From A to, Z. Cell. Mol. Immunol. 2010, 7, 100–103. [Google Scholar] [CrossRef]
- Kwon, M.J.; Han, J.; Seo, J.H.; Song, K.; Jeong, H.M.; Choi, J.-S.; Kim, Y.J.; Lee, S.-H.; Choi, Y.-L.; Shin, Y.K. CD24 Overexpression is associated with poor prognosis in Luminal A and triple-negative breast cancer. PLoS ONE 2015, 10, e0139112. [Google Scholar] [CrossRef]
- Kaipparettu, B.A.; Malik, S.; Konduri, S.D.; Liu, W.; Rokavec, M.; van der Kuip, H.; Hoppe, R.; Hammerich-Hille, S.; Fritz, P.; Schroth, W.; et al. Estrogen-mediated downregulation of CD24 in breast cancer cells. Int. J. Cancer 2008, 123, 66–72. [Google Scholar] [CrossRef]
- Kluz, P.N.; Kolb, R.; Xie, Q.; Borcherding, N.; Liu, Q.; Luo, Y.; Kim, M.C.; Wang, L.; Zhang, Y.; Li, W.; et al. Cancer cell-intrinsic function of CD177 in attenuating β-catenin signaling. Oncogene 2020, 39, 2877–2889. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.C.; Borcherding, N.; Ahmed, K.K.; Voigt, A.P.; Vishwakarma, A.; Kolb, R.; Kluz, P.N.; Pandey, G.; De, U.; Drashansky, T.; et al. CD177 modulates the function and homeostasis of tumor-infiltrating regulatory T cells. Nat. Commun. 2021, 12, 5764. [Google Scholar] [CrossRef]
- Li, K.; Du, Y.; Wei, D.Q.; Zhang, F. CEBPE expression is an independent prognostic factor for acute myeloid leukemia. J. Transl. Med. 2019, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- Aegerter, H.; Smole, U.; Heyndrickx, I.; Verstraete, K.; Savvides, S.N.; Hammad, H.; Lambrecht, B.N. Charcot–Leyden crystals and other protein crystals driving type 2 immunity and allergy. Curr. Opin. Immunol. 2021, 72, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Zhao, T.; Su, Z.; Li, Y.; Zhang, X.; You, Q. Chitinase-3 like-protein-1 function and its role in diseases. Signal Transduct. Target. Ther. 2020, 5, 201. [Google Scholar] [CrossRef]
- Qiu, Q.C.; Wang, L.; Jin, S.S.; Liu, G.F.; Liu, J.; Ma, L.; Mao, R.F.; Ma, Y.Y.; Zhao, N.; Chen, M.; et al. CHI3L1 promotes tumor progression by activating TGF-β signaling pathway in hepatocellular carcinoma. Sci. Rep. 2018, 8, 15029. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhang, S.; Wang, Q.; Zhang, X. Tumor-recruited M2 macrophages promote gastric and breast cancer metastasis via M2 macrophage-secreted CHI3L1 protein. J. Hematol. Oncol. 2017, 10, 36. [Google Scholar] [CrossRef] [PubMed]
- Rusak, A.; Jablonska, K.; Piotrowska, A.; Grzegrzolka, J.; Nowak, A.; Wojnar, A.; Dziegiel, P. The role of CHI3L1 expression in angiogenesis in invasive ductal breast carcinoma. Anticancer Res. 2018, 38, 3357–3366. [Google Scholar] [CrossRef]
- Xu, D.; Lu, W. Defensins: A double-edged sword in host immunity. Front. Immunol. 2020, 11, 764. [Google Scholar] [CrossRef]
- Ganz, T. Defensins and host defense. Science 1999, 286, 420–421. [Google Scholar] [CrossRef]
- Kohli, M.; Young, C.Y.; Tindall, D.J.; Nandy, D.; McKenzie, K.M.; Bevan, G.H.; Donkena, K.V. Whole blood defensin mRNA expression is a predictive biomarker of docetaxel response in castration-resistant prostate cancer. OncoTargets Ther. 2015, 8, 1915–1922. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Gene | Annotation |
|---|---|---|
| Downregulated Genes | ||
| 1 | * CHI3L1 | chitinase-3 like-protein-1 |
| 2 | * EPB42 | erythrocyte membrane protein band 4.2, transcript variant 1 |
| 3 | MS4A3 | membrane spanning 4-domains A3 |
| 4 | GYPB | glycophorin B (MNS blood group) |
| 5 | * PF4 | platelet factor 4 |
| 6 | ALAS2 | 5′-aminolevulinate synthase 2 |
| 7 | FOXO4 | Homo sapiens forkhead box O4 |
| 8 | CA1 | carbonic anhydrase I |
| 9 | * COL18A1 | Homo sapiens collagen type XVIII alpha 1 chain |
| 10 | SNCA | Homo sapiens synuclein alpha, transcript variant 3 |
| 11 | * DEFA1 | Homo sapiens defensin, alpha 1 |
| 12 | MYLK | myosin light chain kinase |
| 13 | * CAMP | cathelicidin antimicrobial peptide |
| 14 | * F2RL1 | Homo sapiens coagulation factor II (thrombin) receptor-like 1 |
| 15 | FKBP1B | FK506 binding protein 1B |
| Upregulated Genes | ||
| 1 | CST3 | Homo sapiens cystatin C |
| 2 | CD3G | CD3g molecule |
| 3 | PARP | Homo sapiens poly(ADP-ribose) polymerase 1 |
| 4 | CENPF | centromere protein F |
| 5 | EZH2 | enhancer of zeste 2 polycomb repressive complex 2 subunit |
| 6 | ENO1 | Homo sapiens enolase 1, (alpha) |
| 7 | FCN1 | Homo sapiens ficolin 1 |
| 8 | PCNA | proliferating cell nuclear antigen |
| 9 | CDK6 | cyclin dependent kinase 6 |
| 10 | HP | Haptoglobin |
| 11 | CD5 | CD5 molecule |
| 12 | PDCD5 | Homo sapiens programmed cell death 5 |
| 13 | PEBP1 | Homo sapiens phosphatidylethanolamine binding protein 1 |
| 14 | FEN1 | flap structure-specific endonuclease 1 |
| 15 | MIF | macrophage migration inhibitory factor |
| 16 | LYZ | Homo sapiens lysozyme |
| 17 | CXCR3 | C-X-C motif chemokine receptor 3 |
| 18 | SQLE | squalene epoxidase |
| 19 | MIER2 | MIER family member 2 |
| 20 | ASGR2 | asialoglycoprotein receptor 2 |
| 21 | VCAN | Homo sapiens versican, transcript variant 1 |
| No. | Gene | Annotation |
|---|---|---|
| Downregulated Genes | ||
| 1 | * CHI3L1 | chitinase-3 like-protein-1 |
| 2 | * DEFA1 | Homo sapiens defensin, alpha 1 |
| 3 | * PF4 | platelet factor 4 |
| 4 | ANXA3 | annexin A3 |
| 5 | MMP9 | matrix metallopeptidase 9 |
| 6 | CD177 | CD177 molecule |
| 7 | * CAMP | cathelicidin antimicrobial peptide |
| 8 | * F2RL1 | Homo sapiens coagulation factor II (thrombin) receptor-like 1 |
| 9 | EPB42 | erythrocyte membrane protein band 4.2, transcript variant 1 |
| 10 | * DEFA4 | Homo sapiens defensin, alpha 4, corticostatin |
| 11 | LRG1 | leucine rich alpha-2-glycoprotein 1 |
| 12 | * COL18A1 | collagen type XVIII alpha 1 chain |
| 13 | IL1R2 | Homo sapiens interleukin 1 receptor, type II, transcript variant 2 |
| 14 | TREM1 | Homo sapiens triggering receptor expressed on myeloid cells 1, transcript variant 2 |
| 15 | NAMPT | nicotinamide phosphoribosyltransferase |
| 16 | S100A8 | S100 calcium binding protein A8 |
| Upregulated Genes | ||
| 1 | ISG15 | ISG15 ubiquitin-like modifier |
| 2 | COL9A2 | collagen type IX alpha 2 chain |
| 3 | SOCS1 | Homo sapiens suppressor of cytokine signaling 1 |
| 4 | IL2R | Homo sapiens interleukin 2 receptor |
| 5 | CSF1 | colony stimulating factor 1 (macrophage) |
| 6 | C3AR1 | complement component 3a receptor 1 |
| 7 | FGFR2 | fibroblast growth factor receptor 2 |
| 8 | P2RY14 | Homo sapiens purinergic receptor P2Y, G-protein coupled, 14 |
| 9 | EEF2K | Homo sapiens eukaryotic elongation factor 2 kinase |
| 10 | CEBPE | CCAAT/enhancer binding protein, epsilon |
| 11 | CD24 | Homo sapiens CD24 molecule |
| 12 | CLC | Homo sapiens Charcot-Leyden crystal protein |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yahya, M.M.; Ismail, M.P.; Ramanathan, S.; Kadir, M.N.; Azhar, A.; Ibrahim, N.B.C.; Wee, C.L.; Mohd Amin, Z.; Tham, S.K.; Mat-Sharani, S.; et al. Synchronous Breast and Cervical Carcinoma: A Genetic Point of View. Biomedicines 2023, 11, 525. https://doi.org/10.3390/biomedicines11020525
Yahya MM, Ismail MP, Ramanathan S, Kadir MN, Azhar A, Ibrahim NBC, Wee CL, Mohd Amin Z, Tham SK, Mat-Sharani S, et al. Synchronous Breast and Cervical Carcinoma: A Genetic Point of View. Biomedicines. 2023; 11(2):525. https://doi.org/10.3390/biomedicines11020525
Chicago/Turabian StyleYahya, Maya Mazuwin, Mohd Pazudin Ismail, Shogeta Ramanathan, Muhammad Nashriq Kadir, Azzahra Azhar, Noorul Balqis Che Ibrahim, Chee Lee Wee, Zahiah Mohd Amin, Seng Kong Tham, Shuhaila Mat-Sharani, and et al. 2023. "Synchronous Breast and Cervical Carcinoma: A Genetic Point of View" Biomedicines 11, no. 2: 525. https://doi.org/10.3390/biomedicines11020525