
Impact of Chronic Exposure to Endometriosis on Perinatal Outcomes: Establishment of a Mouse Model
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
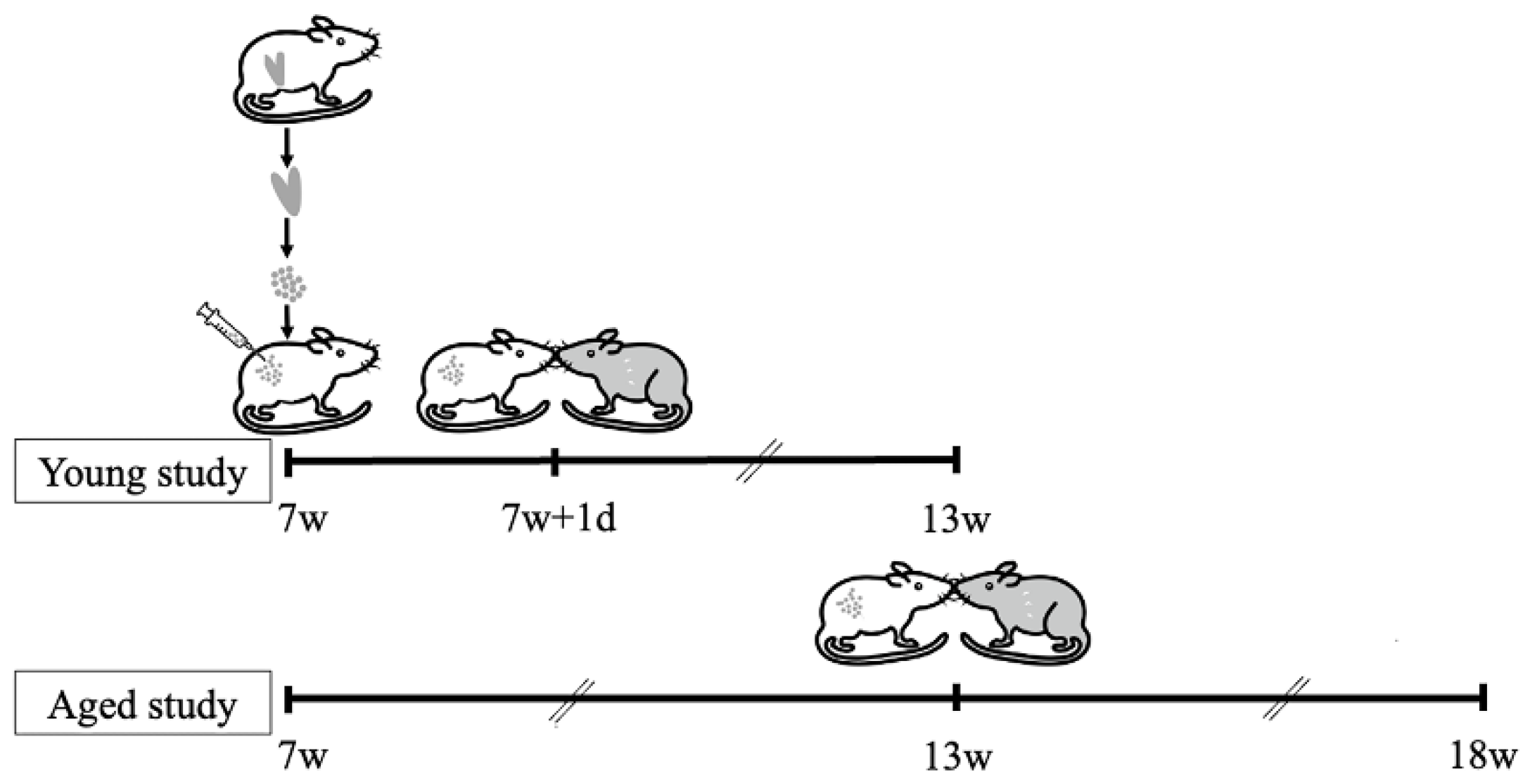
2.1. Establishment of Endometriosis Mouse Model
2.2. Establishment of Pregnancy Mouse Model
2.3. Fertility Analysis
2.4. Perinatal Outcome Analysis
2.5. Statistical Analysis
3. Results
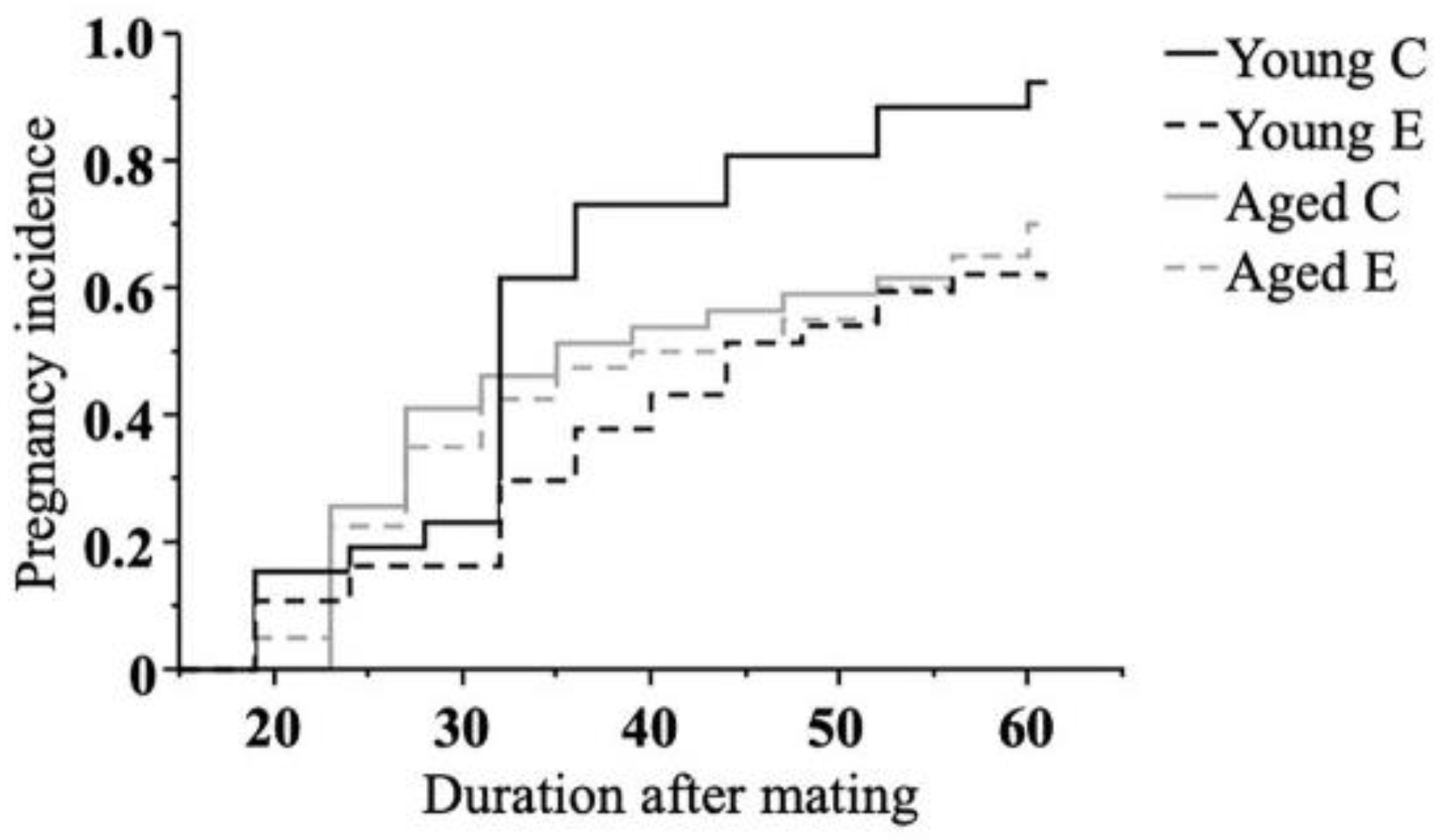
3.1. Effect of Endometriosis on Fertility
3.2. Effect of Endometriosis on the Onset of Labor
3.3. Effect of Endometriosis on Neonatal Outcome
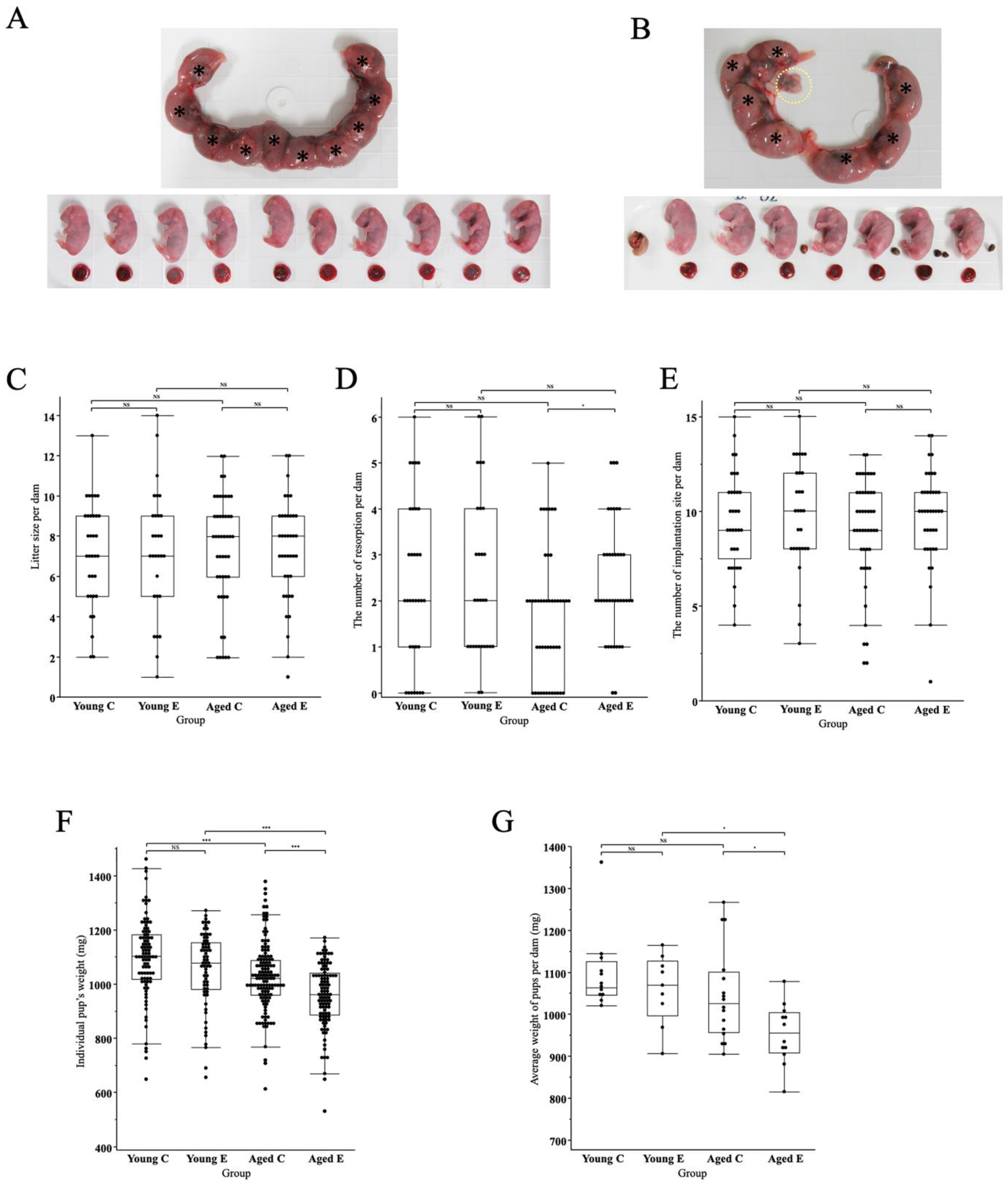
3.3.1. Morphological Changes of Pups and Placenta
3.3.2. Litter Size
3.3.3. Pups’ Body Weight
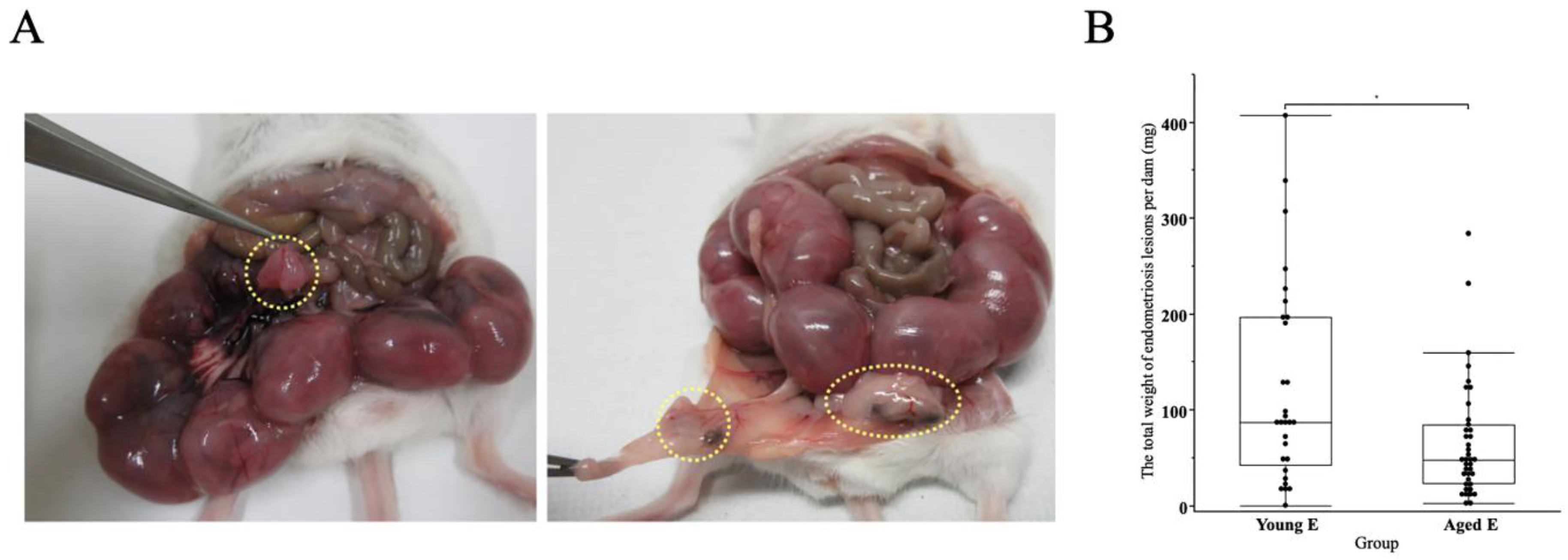
3.4. Presence of Endometriosis Lesions in Both Endometriosis Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zondervan, K.T.; Becker, C.M.; Koga, K.; Missmer, S.A.; Taylor, R.N.; Vigano, P. Endometriosis. Nat. Rev. Dis. Prim. 2018, 4, 9. [Google Scholar] [CrossRef] [PubMed]
- Lalani, S.; Choudhry, A.J.; Firth, B.; Bacal, V.; Walker, M.; Wen, S.W.; Singh, S.; Amath, A.; Hodge, M.; Chen, I. Endometriosis and adverse maternal, fetal and neonatal outcomes, a systematic review and meta-analysis. Hum. Reprod. 2018, 33, 1854–1865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takemura, Y.; Osuga, Y.; Fujimoto, A.; Oi, N.; Tsutsumi, R.; Koizumi, M.; Yano, T.; Taketani, Y. Increased risk of placenta previa is associated with endometriosis and tubal factor infertility in assisted reproductive technology pregnancy. Gynecol. Endocrinol. 2013, 29, 113–115. [Google Scholar] [CrossRef]
- Fujii, T.; Wada-Hiraike, O.; Nagamatsu, T.; Harada, M.; Hirata, T.; Koga, K.; Fujii, T.; Osuga, Y. Assisted reproductive technology pregnancy complications are significantly associated with endometriosis severity before conception: A retrospective cohort study. Reprod. Biol. Endocrinol. 2016, 14, 73. [Google Scholar] [CrossRef] [Green Version]
- Li, L.P.; Li, Z.M.; Wang, Z.Z.; Cheng, Y.F.; He, D.M.; Chen, G.; Cao, B.N.; Zou, Y.; Luo, Y. A novel nude mouse model for studying the pathogenesis of endometriosis. Exp. Ther. Med. 2022, 24, 498. [Google Scholar] [CrossRef]
- Nothnick, W.B.; Graham, A. Dissecting the miR-451a-Mif Pathway in Endometriosis Pathophysiology Using a Syngeneic Mouse Model: Temporal Expression of Lesion Mif Receptors, Cd74 and Cxcr4. Biomedicines 2022, 10, 1699. [Google Scholar] [CrossRef]
- Ramirez-Pavez, T.N.; Martinez-Esparza, M.; Ruiz-Alcaraz, A.J.; Marin-Sanchez, P.; Machado-Linde, F.; Garcia-Penarrubia, P. The Role of Peritoneal Macrophages in Endometriosis. Int. J. Mol. Sci. 2021, 22, 10792. [Google Scholar] [CrossRef]
- Lagana, A.S.; Garzon, S.; Franchi, M.; Casarin, J.; Gullo, G.; Ghezzi, F. Translational animal models for endometriosis research: A long and windy road. Ann. Transl. Med. 2018, 6, 431. [Google Scholar] [CrossRef]
- Zhao, M.; Zhang, M.; Yu, Q.; Fei, W.; Li, T.; Zhu, L.; Yao, Y.; Zheng, C.; Zhang, X. Hyaluronic Acid-Modified Nanoplatforms as a Vector for Targeted Delivery of Autophagy-Related Gene to the Endometriotic Lesions in Mice. Front. Bioeng. Biotechnol. 2022, 10, 918368. [Google Scholar] [CrossRef]
- Huang, S.; Xiao, F.; Guo, S.W.; Zhang, T. Tetramethylpyrazine Retards the Progression and Fibrogenesis of Endometriosis. Reprod. Sci. 2022, 29, 1170–1187. [Google Scholar] [CrossRef]
- Hoorsan, H.; Simbar, M.; Tehrani, F.R.; Fathi, F.; Mosaffa, N.; Riazi, H.; Akradi, L.; Nasseri, S.; Bazrafkan, S. The effectiveness of antioxidant therapy (vitamin C) in an experimentally induced mouse model of ovarian endometriosis. Womens Health 2022, 18, 17455057221096218. [Google Scholar] [CrossRef] [PubMed]
- Vernon, M.W.; Wilson, E.A. Studies on the surgical induction of endometriosis in the rat. Fertil. Steril. 1985, 44, 684–694. [Google Scholar] [CrossRef]
- Barragán, J.C.; Brotons, J.; Ruiz, J.A.; Acién, P. Experimentally induced endometriosis in rats: Effect on fertility and the effects of pregnancy and lactation on the ectopic endometrial tissue. Fertil. Steril. 1992, 58, 1215–1219. [Google Scholar] [CrossRef]
- Cummings, A.M.; Metcalf, J.L. Effect of surgically induced endometriosis on pregnancy and effect of pregnancy and lactation on endometriosis in mice. Proc. Soc. Exp. Biol. Med. 1996, 212, 332–337. [Google Scholar] [CrossRef]
- Stilley, J.A.; Woods-Marshall, R.; Sutovsky, M.; Sutovsky, P.; Sharpe-Timms, K.L. Reduced fecundity in female rats with surgically induced endometriosis and in their daughters: A potential role for tissue inhibitors of metalloproteinase 1. Biol. Reprod. 2009, 80, 649–656. [Google Scholar] [CrossRef]
- Bilotas, M.A.; Olivares, C.N.; Ricci, A.G.; Baston, J.I.; Bengochea, T.S.; Meresman, G.F.; Baranao, R.I. Interplay between Endometriosis and Pregnancy in a Mouse Model. PLoS ONE 2015, 10, e0124900. [Google Scholar] [CrossRef]
- Treatment of pelvic pain associated with endometriosis: A committee opinion. Fertil. Steril. 2014, 101, 927–935. [CrossRef]
- Sasamoto, N.; Ngo, L.; Vitonis, A.F.; Dillon, S.T.; Missmer, S.A.; Libermann, T.A.; Terry, K.L. Circulating proteomic profiles associated with endometriosis in adolescents and young adults. Hum. Reprod. 2022, 37, 2042–2053. [Google Scholar] [CrossRef]
- Mansfield, C.B.; Lenobel, D.; McCracken, K.; Hewitt, G.; Appiah, L.C. Impact of Pelvic Floor Physical Therapy on Function in Adolescents and Young Adults with Biopsy Confirmed Endometriosis at a Tertiary Children’s Hospital: A Case Series. J. Pediatr. Adolesc. Gynecol. 2022, in press. [CrossRef]
- Rasp, E.; Saavalainen, L.; But, A.; Gissler, M.; Harkki, P.; Heikinheimo, O.; Rono, K. Surgically confirmed endometriosis in adolescents in Finland-A register-based cross-sectional cohort study. Acta Obstet. Gynecol. Scand. 2022, 101, 1065–1107. [Google Scholar] [CrossRef]
- OECD. Age of Mothers at Childbirth and Age-Specific Fertility; OECD: Paris, France, 2022.
- Takeuchi, A.; Koga, K.; Tokita, Y.; Matsumoto, T.; Satake, E.; Taguchi, A.; Makabe, T.; Miyashita, M.; Takamura, M.; Harada, M.; et al. The effects of tokishakuyakusan, a traditional Japanese medicine (kampo), ferulic acid and paeoniflorin, on human endometriotic stromal cells and peritoneal macrophages. J. Reprod. Immunol. 2020, 139, 103104. [Google Scholar] [CrossRef] [PubMed]
- Satake, E.; Koga, K.; Takamura, M.; Izumi, G.; Elsherbini, M.; Taguchi, A.; Makabe, T.; Takeuchi, A.; Harada, M.; Hirata, T.; et al. The roles of polymorphonuclear myeloid-derived suppressor cells in endometriosis. J. Reprod. Immunol. 2021, 148, 103371. [Google Scholar] [CrossRef] [PubMed]
- Borisova, A.V.; Konnon, S.R.D.; Tosto, V.; Gerli, S.; Radzinsky, V.E. Obstetrical complications and outcome in patients with endometriosis. J. Matern. Fetal. Neonatal. Med. 2020, 35, 2663–2677. [Google Scholar] [CrossRef]
- Hirata, Y.; Katsukura, Y.; Henmi, Y.; Ozawa, R.; Shimazaki, S.; Kurosawa, A.; Torii, Y.; Takahashi, H.; Iwata, H.; Kuwayama, T.; et al. Advanced maternal age induces fetal growth restriction through decreased placental inflammatory cytokine expression and immune cell accumulation in mice. J. Reprod. Dev. 2021, 67, 257–264. [Google Scholar] [CrossRef]
- Zullo, F.; Spagnolo, E.; Saccone, G.; Acunzo, M.; Xodo, S.; Ceccaroni, M.; Berghella, V. Endometriosis and obstetrics complications: A systematic review and meta-analysis. Fertil. Steril. 2017, 108, 667–672 e665. [Google Scholar] [CrossRef] [Green Version]
- Pinheiro, R.L.; Areia, A.L.; Pinto, M.A.; Donato, H. Advanced Maternal Age: Adverse Outcomes of Pregnancy, A Meta-Analysis. Acta Med. Port. 2019, 32, 219–226. [Google Scholar] [CrossRef] [Green Version]
- Saccone, G.; Gragnano, E.; Ilardi, B.; Marrone, V.; Strina, I.; Venturella, R.; Berghella, V.; Zullo, F. Maternal and perinatal complications according to maternal age: A systematic review and meta-analysis. Int. J. Gynaecol. Obstet. 2022, 159, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Lean, S.C.; Heazell, A.E.P.; Dilworth, M.R.; Mills, T.A.; Jones, R.L. Placental Dysfunction Underlies Increased Risk of Fetal Growth Restriction and Stillbirth in Advanced Maternal Age Women. Sci. Rep. 2017, 7, 9677. [Google Scholar] [CrossRef] [PubMed]
- Kuivasaari-Pirinen, P.; Raatikainen, K.; Hippeläinen, M.; Heinonen, S. Adverse Outcomes of IVF/ICSI Pregnancies Vary Depending on Aetiology of Infertility. ISRN Obstet. Gynecol. 2012, 2012, 451915. [Google Scholar] [CrossRef] [Green Version]
- Conti, N.; Cevenini, G.; Vannuccini, S.; Orlandini, C.; Valensise, H.; Gervasi, M.T.; Ghezzi, F.; Di Tommaso, M.; Severi, F.M.; Petraglia, F. Women with endometriosis at first pregnancy have an increased risk of adverse obstetric outcome. J. Matern. Fetal. Neonatal. Med. 2015, 28, 1795–1798. [Google Scholar] [CrossRef]
- Exacoustos, C.; Lauriola, I.; Lazzeri, L.; De Felice, G.; Zupi, E. Complications during pregnancy and delivery in women with untreated rectovaginal deep infiltrating endometriosis. Fertil. Steril. 2016, 106, 1129–1135.e1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mannini, L.; Sorbi, F.; Noci, I.; Ghizzoni, V.; Perelli, F.; Di Tommaso, M.; Mattei, A.; Fambrini, M. New adverse obstetrics outcomes associated with endometriosis: A retrospective cohort study. Arch. Gynecol. Obstet. 2017, 295, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Horton, J.; Sterrenburg, M.; Lane, S.; Maheshwari, A.; Li, T.C.; Cheong, Y. Reproductive, obstetric, and perinatal outcomes of women with adenomyosis and endometriosis: A systematic review and meta-analysis. Hum. Reprod. Update 2019, 25, 592–632. [Google Scholar] [CrossRef] [PubMed]
- Leader, J.; Bajwa, A.; Lanes, A.; Hua, X.; Rennicks White, R.; Rybak, N.; Walker, M. The Effect of Very Advanced Maternal Age on Maternal and Neonatal Outcomes: A Systematic Review. J. Obstet. Gynaecol. Can. 2018, 40, 1208–1218. [Google Scholar] [CrossRef]
- Bulletti, C.; Coccia, M.E.; Battistoni, S.; Borini, A. Endometriosis and infertility. J. Assist. Reprod. Genet. 2010, 27, 441–447. [Google Scholar] [CrossRef]
- Macer, M.L.; Taylor, H.S. Endometriosis and infertility: A review of the pathogenesis and treatment of endometriosis-associated infertility. Obstet. Gynecol. Clin. N. Am. 2012, 39, 535–549. [Google Scholar] [CrossRef] [Green Version]
- Akande, V.A.; Hunt, L.P.; Cahill, D.J.; Jenkins, J.M. Differences in time to natural conception between women with unexplained infertility and infertile women with minor endometriosis. Hum. Reprod. 2004, 19, 96–103. [Google Scholar] [CrossRef] [Green Version]
- Isono, W.; Wada-Hiraike, O.; Akino, N.; Terao, H.; Harada, M.; Hirata, T.; Hirota, Y.; Koga, K.; Fujii, T.; Osuga, Y. The efficacy of non-assisted reproductive technology treatment might be limited in infertile patients with advanced endometriosis in their 30s. J. Obstet. Gynaecol. Res. 2019, 45, 368–375. [Google Scholar] [CrossRef]
- Yang, X.; Huang, R.; Cai, M.; Liang, X. Endometriosis has no negative impact on outcomes of in vitro fertilisation in women with poor ovarian response. BJOG 2016, 123 (Suppl. S3), 76–81. [Google Scholar] [CrossRef]
- Flurkey, K.; Brandvain, Y.; Klebanov, S.; Austad, S.N.; Miller, R.A.; Yuan, R.; Harrison, D.E. PohnB6F1, A Cross of Wild and Domestic Mice That Is a New Model of Extended Female Reproductive Life Span. J. Gerontol. Ser. A 2007, 62, 1187–1198. [Google Scholar] [CrossRef]
- Garratt, M.; Try, H.; Smiley, K.O.; Grattan, D.R.; Brooks, R.C. Mating in the absence of fertilization promotes a growth-reproduction versus lifespan trade-off in female mice. Proc. Natl. Acad. Sci. USA 2020, 117, 15748–15754. [Google Scholar] [CrossRef] [PubMed]
- Habib, N.; Buzzaccarini, G.; Centini, G.; Moawad, G.; Ceccaldi, P.-F.; Gitas, G.; Alkatout, I.; Gullo, G.; Terzic, S.; Sleiman, Z. Impact of lifestyle and diet on endometriosis: A fresh look to a busy corner. Menopausal Rev. 2022, 21, 124–132. [Google Scholar] [CrossRef] [PubMed]
- D’Anna, R.; Santamaria, A.; Giorgianni, G.; Vaiarelli, A.; Gullo, G.; Di Bari, F.; Benvenga, S. Myo-inositol and melatonin in the menopausal transition. Gynecol. Endocrinol. 2017, 33, 279–282. [Google Scholar] [CrossRef] [PubMed]
- D’Anna, R.; Corrado, F.; Loddo, S.; Gullo, G.; Giunta, L.; Di Benedetto, A. Myoinositol plus alpha-lactalbumin supplementation, insulin resistance and birth outcomes in women with gestational diabetes mellitus: A randomized, controlled study. Sci. Rep. 2021, 11, 8866. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Young C | Young E | Aged C | Aged E | |
|---|---|---|---|---|
| Total # of dam | 33 | 29 | 47 | 39 |
| # of dam delivered before dpc18 | 0 | 2 | 0 | 1 |
| % of dam delivered before dpc18 | 0 | 6.9 | 0 | 2.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elsherbini, M.; Koga, K.; Maki, E.; Kumasawa, K.; Satake, E.; Taguchi, A.; Makabe, T.; Takeuchi, A.; Izumi, G.; Takamura, M.; et al. Impact of Chronic Exposure to Endometriosis on Perinatal Outcomes: Establishment of a Mouse Model. Biomedicines 2022, 10, 2627. https://doi.org/10.3390/biomedicines10102627
Elsherbini M, Koga K, Maki E, Kumasawa K, Satake E, Taguchi A, Makabe T, Takeuchi A, Izumi G, Takamura M, et al. Impact of Chronic Exposure to Endometriosis on Perinatal Outcomes: Establishment of a Mouse Model. Biomedicines. 2022; 10(10):2627. https://doi.org/10.3390/biomedicines10102627
Chicago/Turabian StyleElsherbini, Mohammed, Kaori Koga, Eiko Maki, Keiichi Kumasawa, Erina Satake, Ayumi Taguchi, Tomoko Makabe, Arisa Takeuchi, Gentaro Izumi, Masashi Takamura, and et al. 2022. "Impact of Chronic Exposure to Endometriosis on Perinatal Outcomes: Establishment of a Mouse Model" Biomedicines 10, no. 10: 2627. https://doi.org/10.3390/biomedicines10102627