
The Role of Immunoglobulin G (IgG), IgA and IgE—Antibodies against Helicobacter pylori in the Development of Oxidative Stress in Patients with Chronic Gastritis


Abstract
:1. Introduction
2. Materials and Methods
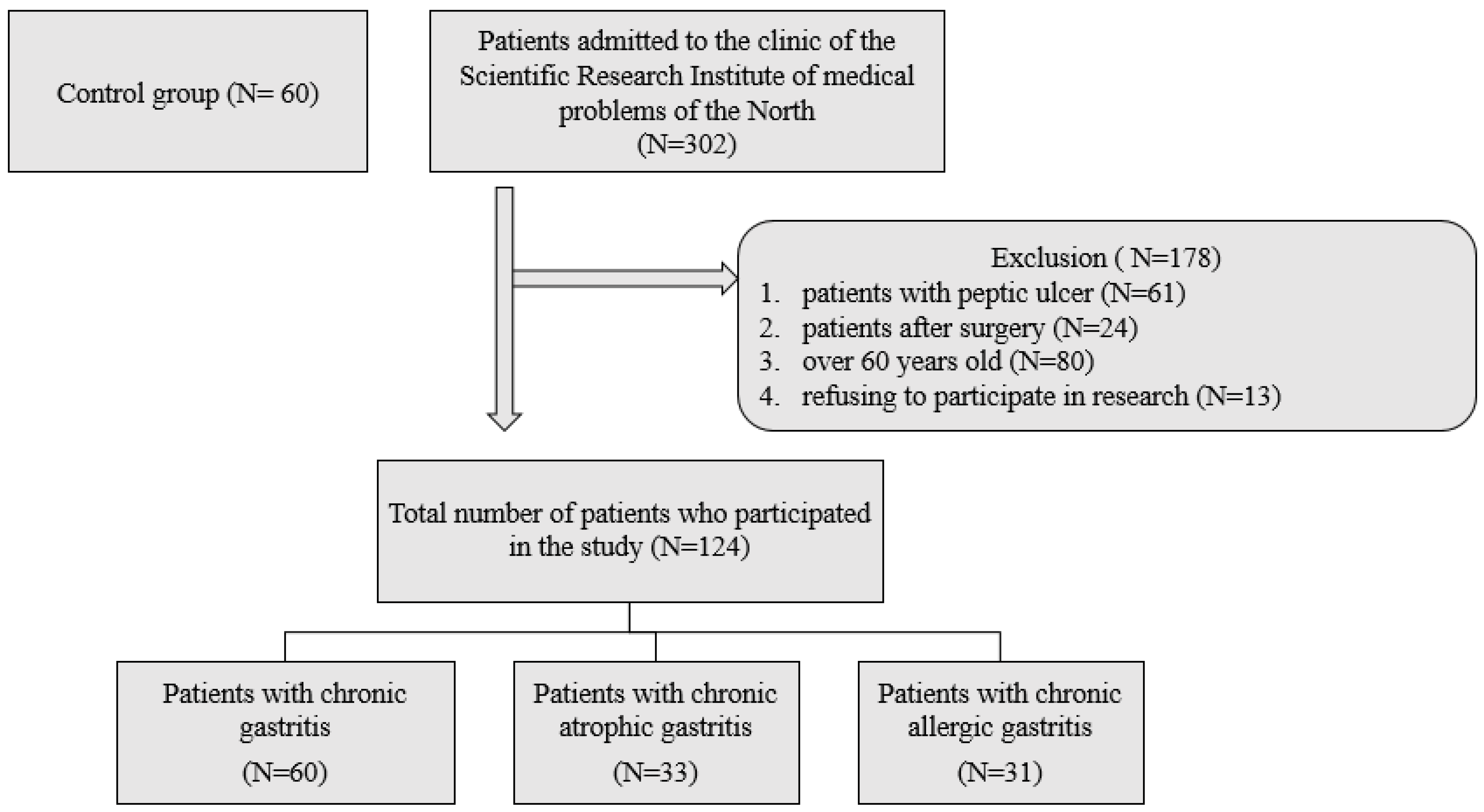
2.1. Subjects
2.2. Endoscopic Examination of the Stomach, Histological Examination, Testing for Helicobacter pylori and Sampling of Gastric Juice
2.3. Collection of Gastric Juice and Measurement of Its pH
2.4. Determination of Serum Indicators of Pepsinogens
2.5. Serum IgA, IgG, IgM, IgE Levels
2.6. Lipid Peroxidation and Antioxidants
2.6.1. Determination of the Content of Diene Conjugates
2.6.2. Determination of Malondialdehyde Content
2.6.3. Determination of the Amount of Reduced Glutathione
2.6.4. Determination of Glutathione-S-Transferase Activity
2.6.5. Determination of Glutathione Peroxidase Activity
2.6.6. Determination of Superoxide Dismutase Activity
2.6.7. Determination of Catalase Activity
2.6.8. Definition Oxidative Stress Ratio (OSR)
2.7. Statistical Analysis
3. Results
3.1. Baseline Patient Data
3.2. Distribution of Chronic Gastritis according to the Specifics of the Humoral Response to H. pylori Infection
3.3. Indicators of Lipid Peroxidation–AOD in Chronic Gastritis, Depending on the Specific Humoral Response to H. pylori Infection
3.3.1. The State of the System “Lipid Peroxidation–Antioxidant Defense System” in Various Types of Chronic Gastritis in the Presence of a Serum Response against H. pylori in the Form of “IgG > IgA”
3.3.2. The State of the System “Lipid Peroxidation–Antioxidant Defense System” in Various Types of Chronic Gastritis in the Presence of a Serum Response against H. pylori in the Form of “Low Concentrations of IgG and IgA”
3.3.3. The State of the System “Lipid Peroxidation–Antioxidant Defense System” in Various Types of Chronic Gastritis in the Presence of a Serum Response against H. pylori in the Form of an Increase in IgE
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Aguilar, G.R.; Ayala, G.; Fierros-Zarate, G. Helicobacter pylori: Recent advances in the study of its pathogenicity and prevention. Salud Publica Mex. 2001, 43, 237–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, H.J.; Yu, L.Z.; Bai, J.F.; Peng, Y.S.; Sun, G.; Zhao, H.L.; Miu, K.; Lu, X.Z.; Zhang, X.Y.; Zhao, Z.Q. Multiple genetic alterations and behavior of cellular biology in gastric cancer and other gastric mucosal lesions: H. pylori infection, histological types and staging. World J. Gastroenterol. 2000, 6, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, X.Q.; Lin, S.R. Research of Helicobacter pylori infection in precancerous gastric lesions. World J. Gastroenterol. 2000, 6, 428–429. [Google Scholar] [CrossRef] [PubMed]
- Prinz, C.; Schoniger, M.; Rad, R.; Becker, I.; Keiditsch, E.; Wagenpfeil, S.; Classen, M.; Rosch, T.; Schepp, W.; Gerhard, M. Key importance of the Helicobacter pylori adherence factor blood group antigen binding adhesin during chronic gastric inflammation. Cancer Res. 2001, 61, 1903–1909. [Google Scholar] [PubMed]
- Zhu, Y.; Lin, J.; Li, D.; Du, Q.; Qian, K.; Wu, Q.; Zheng, S. Helicobacter pylori antigen and its IgG, IgA-type specific immunocomplexes in sera from patients with Helicobacter pylori infection. Chin. Med. J. 2002, 115, 381–383. [Google Scholar] [PubMed]
- Futagami, S.; Takahashi, H.; Norose, Y.; Kobayashi, M. Systemic and local immune responses against Helicobacter pylori urease in patients with chronic gastritis: Distinct IgA and IgG productive sites. Gut 1998, 43, 168–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, H.; Chaturvedi, R.; Cheng, Y.; Bussiere, F.I.; Asim, M.; Yao, M.D.; Potosky, D.; Meltzer, S.J.; Rhee, J.G.; Kim, S.S.; et al. Spermine oxidation induced by Helicobacter pylori results in apoptosis and DNA damage: Implications for gastric carcinogenesis. Cancer Res. 2004, 64, 8521–8525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domellof, L. Reversal of gastric atrophy after Helicobacter pylori eradication: Is it possible or not? Am. J. Gastroenterol. 1998, 93, 1407–1408. [Google Scholar] [CrossRef] [PubMed]
- Meining, A.; Stolte, M. Close correlation of intestinal metaplasia and corpus gastritis in patients infected with Helicobacter pylori. Z. Für Gastroenterol. 2022, 40, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, G.; Faundez, G.; Troncoso, M.; Navarrete, P.; Toledo, M.S. Immunoglobulin G antibody response to infection with coccoid forms of Helicobacter pylori. Clin. Vaccine Immunol. 2002, 9, 1067–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drake, I.M.; Davies, M.J.; Mapstone, N.P.; Dixon, M.F.; Schorah, C.J.; White, K.L.; Chalmers, D.M.; Axon, A.T. Ascorbic acid may protect against human gastric cancer by scavenging mucosal oxygen radicals. Carcinogenesis 1996, 17, 559–562. [Google Scholar] [CrossRef] [PubMed]
- Na, H.K.; Woo, J.H. Helicobacter pylori Induces Hypermethylation of CpG Islands Through Upregulation of DNA Methyltransferase: Possible Involvement of Reactive Oxygen/Nitrogen Species. J. Cancer Prev. 2014, 19, 259–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yanaka, A. Sulforaphane enhances protection and repair of gastric mucosa against oxidative stress in vitro, and demonstrates anti-inflammatory effects on Helicobacter pylori-infected gastric mucosae in mice and human subjects. Curr. Pharm. Des. 2011, 17, 1532–1540. [Google Scholar] [CrossRef] [PubMed]
- Posselt, G.; Backert, S.; Wessler, S. The functional interplay of Helicobacter pylori factors with gastric epithelial cells induces a multi-step process in pathogenesis. Cell Commun. Signal. 2013, 11, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, R.; Asim, M.; Romero–Gallo, J.; Barry, D.P.; Hoge, S.; de Sablet, T.; Delgado, A.G.; Wroblewski, L.E.; Piazuelo, M.B.; Yan, F.; et al. Spermine oxidase mediates the gastric cancer risk associated with Helicobacter pylori CagA. Gastroenterology 2011, 141, 1696–1708.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaturvedi, R.; Cheng, Y.; Asim, M.; Bussière, F.I.; Xu, H.; Gobert, A.P.; Hacker, A.; Casero Robert, A., Jr.; Wilson, K.T. Induction of polyamine oxidase 1 by Helicobacter pylori causes macrophage apoptosis by hydrogen peroxide release and mitochondrial membrane depolarization. J. Biol. Chem. 2004, 279, 40161–40173. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | CG, N = 60 | CAG, N = 33 | CALG, N = 31 | p Value |
|---|---|---|---|---|
| Age, yr | 47.54 ± 12.65 | 57.3 ± 9.65 | 49.87 ± 8.34 | 0.414 |
| Body mass index, kg/m2 | 23.78 ± 2.62 | 22.41 ± 2.45 | 22.31 ± 3.68 | 0.237 |
| Alcohol consumption 1. Never 2. Past 3. Current | 0.468 | |||
| 10 (15.3) | 8 (10.9) | 4 (13.8) | ||
| 7 (17.4) | 6 (20.7) | 3 (11.8) | ||
| 43 (71.7) | 19 (65.5) | 24 (82.4) | ||
| Smoking 1. Never 2. Past 3. Current | 0.842 | |||
| 6 (34.8) | 6 (29.4) | 12 (41.4) | ||
| 20 (43.5) | 7 (47.1) | 11 (37.9) | ||
| 34 (21.7) | 20 (23.5) | 8 (20.7) | ||
| pH value of gastric juice | 3.23 ± 1.99 | 4.54 ± 2.23 | 2.46 ± 1.73 | 0.003 |
| Serum pepsinogen content | N = 56 | N = 29 | N = 30 | |
| Pepsinogen I, ng/mL | 56.48 ± 89.13 | 93.16 ± 147.33 | 66.33 ± 93.25 | 0.133 |
| Pepsinogen II, ng/mL | 19.32 ± 28.44 | 34.80 ± 41.62 | 27.56 ± 38.67 | 0.068 |
| Pepsinogen I/II ratio | 3.68 ± 1.79 | 3.06 ± 1.61 | 3.49 ± 1.36 | 0.232 |
| H. pylori | CG | CAG | CALG | Total |
|---|---|---|---|---|
| Total number of patients | 60 | 33 | 31 | 124 |
| The presence of antibodies (%/abs.) | 78%/47 | 91%/30 | 83%/25 | 102 |
| Absence of antibodies, (%/abs.) | 22%/13 | 9%/3 | 17%/6 | 22 |
| Serum Response Against H. pylori | CG | CAG | CALG | Total |
|---|---|---|---|---|
| IgG > IgA, (%/abs.) | 75%/35 | 60%/18 | 5%/1 | 54 |
| Low concentrations of IgG, IgA, (%/abs.) | 15%/7 | 27%/8 | 4%/1 | 16 |
| IgE, (%/abs.) | 10%/5 | 13%/4 | 91%/23 | 32 |
| Indicators | Control Group, N = 43 (1) | CG, N = 47 (2) | CAG, N = 30 (3) | CALG, N = 25 (4) | ||||
|---|---|---|---|---|---|---|---|---|
| Me | Q1–Q3 | Me | Q1–Q3 | Me | Q1–Q3 | Me | Q1–Q3 | |
| DC, µmol/L | 1.15 | 0.88–1.38 | 1.4 | 1.97–2.78 | 2.8 | 1.43–1.98 | 3.16 | 3.12–3.53 |
| p1–2 = 0.02 | p1–3 < 0.001 | p1–4 < 0.001; p2–4 < 0.001; p3–4 < 0.001 | ||||||
| MDA, µmol/1 g protein | 1.6 | 0.96–2.24 | 2.1 | 1.42–2.8 | 2.5 | 1.6–2.9 | 3.3 | 2.6–4.7 |
| p1–2 = 0.01 | p1–3 < 0.001 | p1–4 < 0.001; p2–4 < 0.001; p3–4 < 0.001 | ||||||
| SOD, U/min/1 g protein | 204.41 | 151.05–250.3 | 187.6 | 141.6–213.3 | 191.3 | 157.7–210.2 | 218.3 | 200.3–243.4 |
| p1–3 = 0.01 | p1–4 < 0.001; p2–4 < 0.001; p3–4 < 0.001 | |||||||
| CAT, µmol/s/1 g protein | 0.2 | 0.16–0.39 | 0.18 | 0.12–0.29 | 0.25 | 0.19–0.43 | 0.36 | 0.27–0.64 |
| p1–3 = 0.03 | p1–4 < 0.001; p2–4 < 0.001 | |||||||
| GST, mmol/min/1 g protein | 41.3 | 37.7–42.64 | 50.2 | 24.9–51.7 | 54.2 | 55.1–70.3 | 68.6 | 56.3–74.6 |
| p1–3 = 0.04 | p1–4 < 0.001; p2–4 < 0.001 | |||||||
| GPO, µmol/1 g protein | 107.9 | 81.19–126.38 | 105.02 | 68.9–122.1 | 118.6 | 132.1–176.5 | 147.4 | 138.1–194.4 |
| p1–3 = 0.04 | p1–4 = 0.01; p2–4 = 0.01 | |||||||
| Indicators | Control Group, N = 43 (1) | CG, N = 47 (2) | CAG, N = 30 (3) | CALG, N = 25 (4) | ||||
|---|---|---|---|---|---|---|---|---|
| Me | Q1–Q3 | Me | Q1–Q3 | Me | Q1–Q3 | Me | Q1–Q3 | |
| DC, µmol/L | 1.15 | 0.88–1.38 | 1.38 | 1.43–1.98 | 2.4 | 1.97–2.78 | 3.16 | 3.12–3.53 |
| p1–3 < 0.001; p2–3 = 0.001 | p1–4 < 0.001; p2–4 < 0.001; p3–4 < 0.001 | |||||||
| MDA, µmol/1 g protein | 1.6 | 0.96–2.24 | 2.4 | 1.9–3.1 | 3.1 | 2.9–4.8 | 4.8 | 3.6–6.7 |
| p1–3 < 0.001; p2–3 = 0.03 | p1–4 < 0.001; p2–4 < 0.001; p3–4 < 0.001 | |||||||
| SOD, U/min/1 g protein | 204.41 | 151.05–250.3 | 198.3 | 186.1–213.1 | 192.1 | 175–20.2 | 185.3 | 174.1–205.1 |
| p1–3 = 0.03 | p1–4 < 0.001; p2–4 = 0.01 | |||||||
| CAT, µmol/s/1 g protein | 0.2 | 0.16–0.39 | 0.19 | 0.13–0.2 | 0.15 | 0.12–0.22 | 0.14 | 0.12–0.24 |
| p1–2 = 0.04 | p1–3 < 0.001; p2–3 = 0.03 | p1–4 < 0.001; p2–4 = 0.01 | ||||||
| GST, mmol/min/1 g protein | 41.3 | 37.7–42.64 | 39.1 | 26.8–47.7 | 34.2 | 29.1–40.3 | 33.6 | 26.3–44.6 |
| p1–3 = 0.01 | p1–4 < 0.001; p2–4 = 0.001 | |||||||
| GPO, µmol/1 g protein | 107.9 | 81.19–126.38 | 109.3 | 91.3–117.3 | 98.6 | 89.1–106.5 | 97.4 | 91.1–104.4 |
| p1–3 = 0.001 | p1–4 < 0.001; p2–4 = 0.01 | |||||||
| Indicators | Control Group, N = 43 (1) | CG, N = 47 (2) | CAG, N = 30 (3) | CALG, N = 25 (4) | ||||
|---|---|---|---|---|---|---|---|---|
| Me | Q1–Q3 | Me | Q1–Q3 | Me | Q1–Q3 | Me | Q1–Q3 | |
| DC, µmol/L | 1.15 | 0.88–1.38 | 1.7 | 1.43–1.98 | 2.9 | 2.71–3.08 | 3.98 | 3.52–4.03 |
| p1–2 = 0.02 | p1–3 < 0.001; p2–3 = 0.003 | p1–4 < 0.001; p2–4 < 0.001; p3–4 < 0.001 | ||||||
| MDA, µmol/1 g protein | 1.6 | 0.96–2.24 | 2.6 | 1.9–3.3 | 3.8 | 3.3–4.8 | 5.1 | 4.6–7.7 |
| p1–2 = 0.02 | p1–3 < 0.001; p2–3 = 0.001 | p1–4 < 0.001; p2–4 < 0.001; p3–4 < 0.001 | ||||||
| SOD, U/min/1 g protein | 204.41 | 151.05–250.3 | 215.3 | 207.2–252.4 | 224.3 | 219.1–257.6 | 281.2 | 240.4–298.5 |
| p1–2 = 0.04 | p1–3 < 0.001; p2–3 = 0.03 | p1–4 < 0.001; p2–4 < 0.001; p3–4 < 0.001 | ||||||
| CAT, µmol/s/1 g protein | 0.2 | 0.16–0.39 | 0.6 | 0.41–0.72 | 1.01 | 0.82–1.12 | 1.23 | 0.97–1.44 |
| p1–2 = 0.01 | p1–3 < 0.001; p2–3 = 0.04 | p1–4 < 0.001; p2–4 < 0.001; p3–4 < 0.001 | ||||||
| GST, mmol/min/1 g protein | 41.3 | 37.7–42.64 | 53.5 | 46.8–67.7 | 64.2 | 55.1–87.3 | 78.6 | 61.3–94.6 |
| p1–3 < 0.001; p2–3 = 0.004 | p1–4 < 0.001; p2–4 < 0.001 | |||||||
| GPO µmol/1 g protein | 107.9 | 81.19–126.38 | 104.3 | 91.3–117.3 | 127.6 | 114.1–146.5 | 137.4 | 128.1–154.4 |
| p1–3 = 0.01; p2–3 = 0.004 | p1–4 < 0.001; p2–4 < 0.001 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Smirnova, O.V.; Sinyakov, A.A.; Kasparov, E.V. The Role of Immunoglobulin G (IgG), IgA and IgE—Antibodies against Helicobacter pylori in the Development of Oxidative Stress in Patients with Chronic Gastritis. Biomedicines 2022, 10, 2053. https://doi.org/10.3390/biomedicines10082053
Smirnova OV, Sinyakov AA, Kasparov EV. The Role of Immunoglobulin G (IgG), IgA and IgE—Antibodies against Helicobacter pylori in the Development of Oxidative Stress in Patients with Chronic Gastritis. Biomedicines. 2022; 10(8):2053. https://doi.org/10.3390/biomedicines10082053
Chicago/Turabian StyleSmirnova, Olga Valentinovna, Alexander Alexandrovich Sinyakov, and Eduard Vilyamovich Kasparov. 2022. "The Role of Immunoglobulin G (IgG), IgA and IgE—Antibodies against Helicobacter pylori in the Development of Oxidative Stress in Patients with Chronic Gastritis" Biomedicines 10, no. 8: 2053. https://doi.org/10.3390/biomedicines10082053