
Enhanced Antitumor Efficacy of PhAc-ALGP-Dox, an Enzyme-Activated Doxorubicin Prodrug, in a Panel of THOP1-Expressing Patient-Derived Xenografts of Soft Tissue Sarcoma

 ,
,  ,
,  , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient-Derived Sarcoma Xenograft Models
2.2. Drugs and Reagents
2.3. Experimental Setup
2.3.1. CBR-049 and CBR-050 vs. Doxo
2.3.2. CBR-049 vs. Doxo and Aldoxo
2.4. Histological Assessment
2.5. Statistics
3. Results
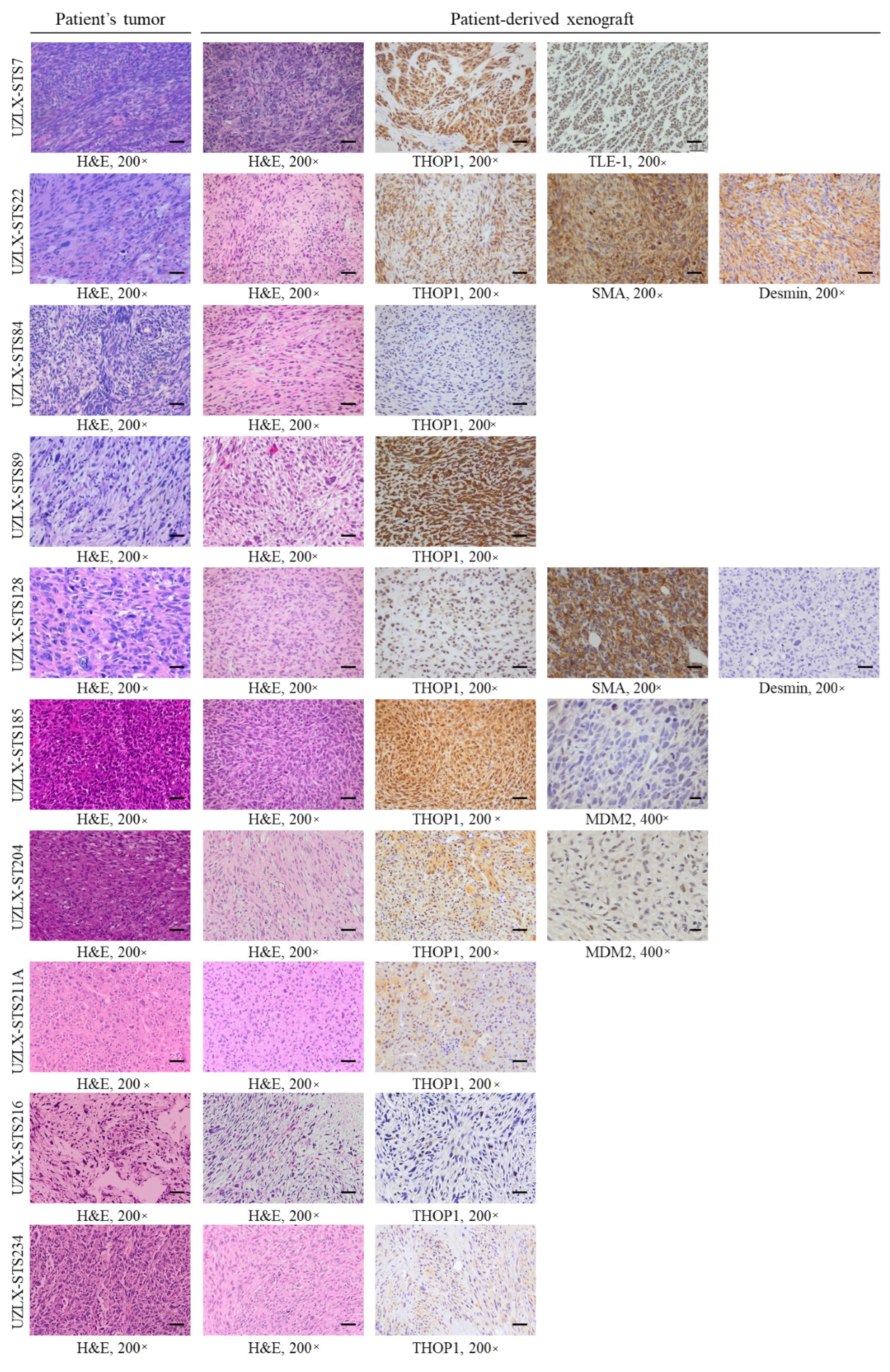
3.1. Characterization of the Selected STS Xenograft Models
3.2. CBR-049 and CBR-050 vs. Doxo
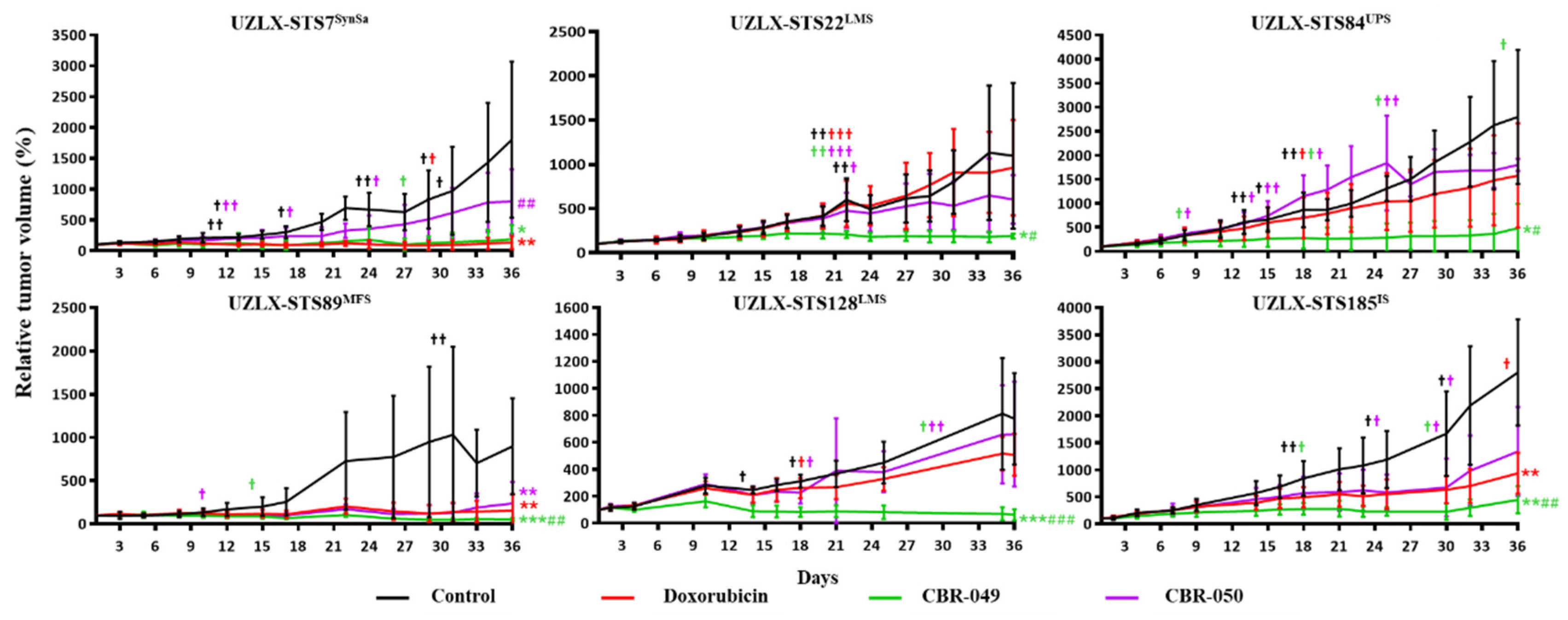
3.2.1. Tumor Volume Evaluation
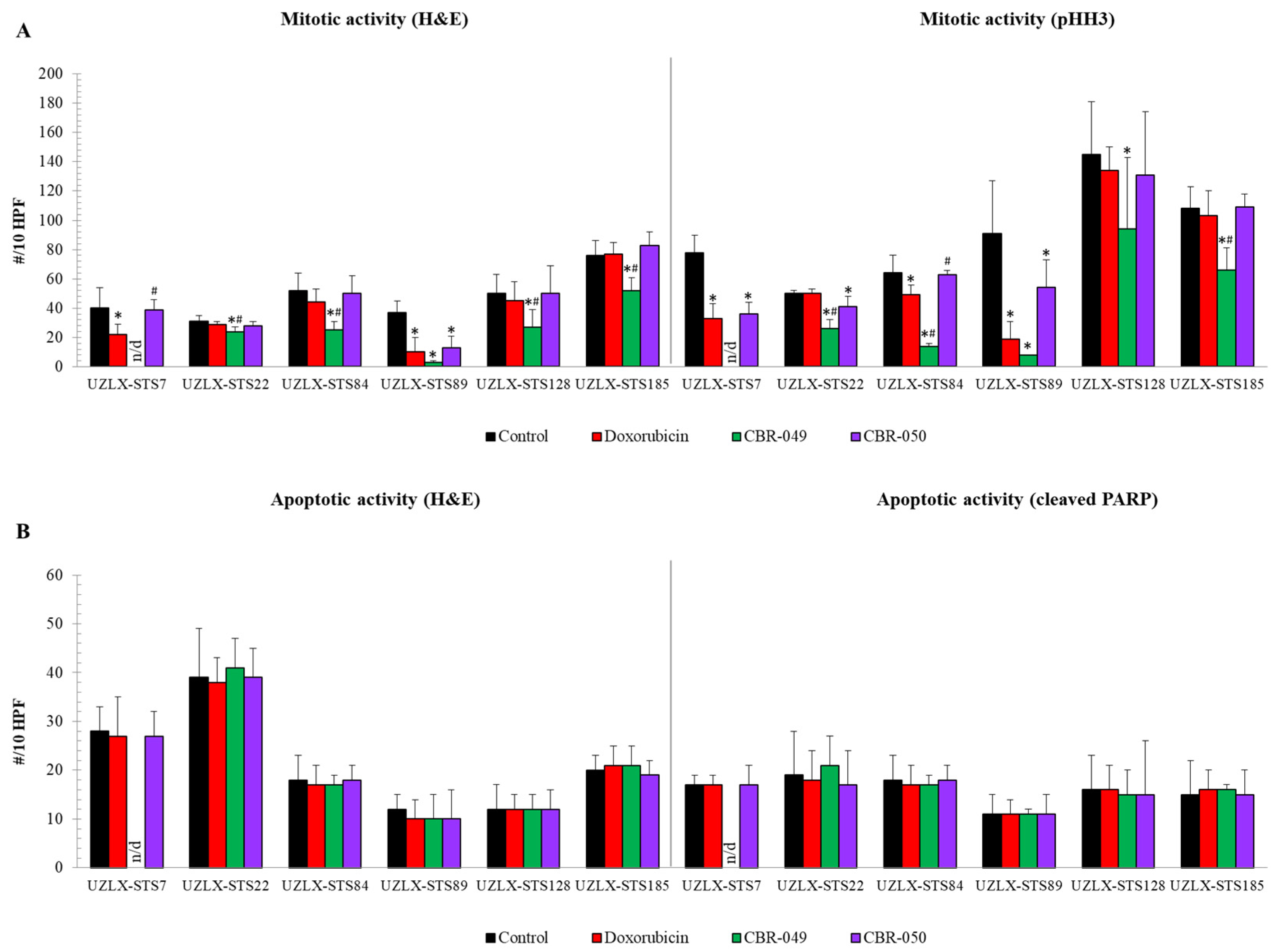
3.2.2. Histological Assessment
3.3. CBR-049 vs. Doxo and Aldoxo
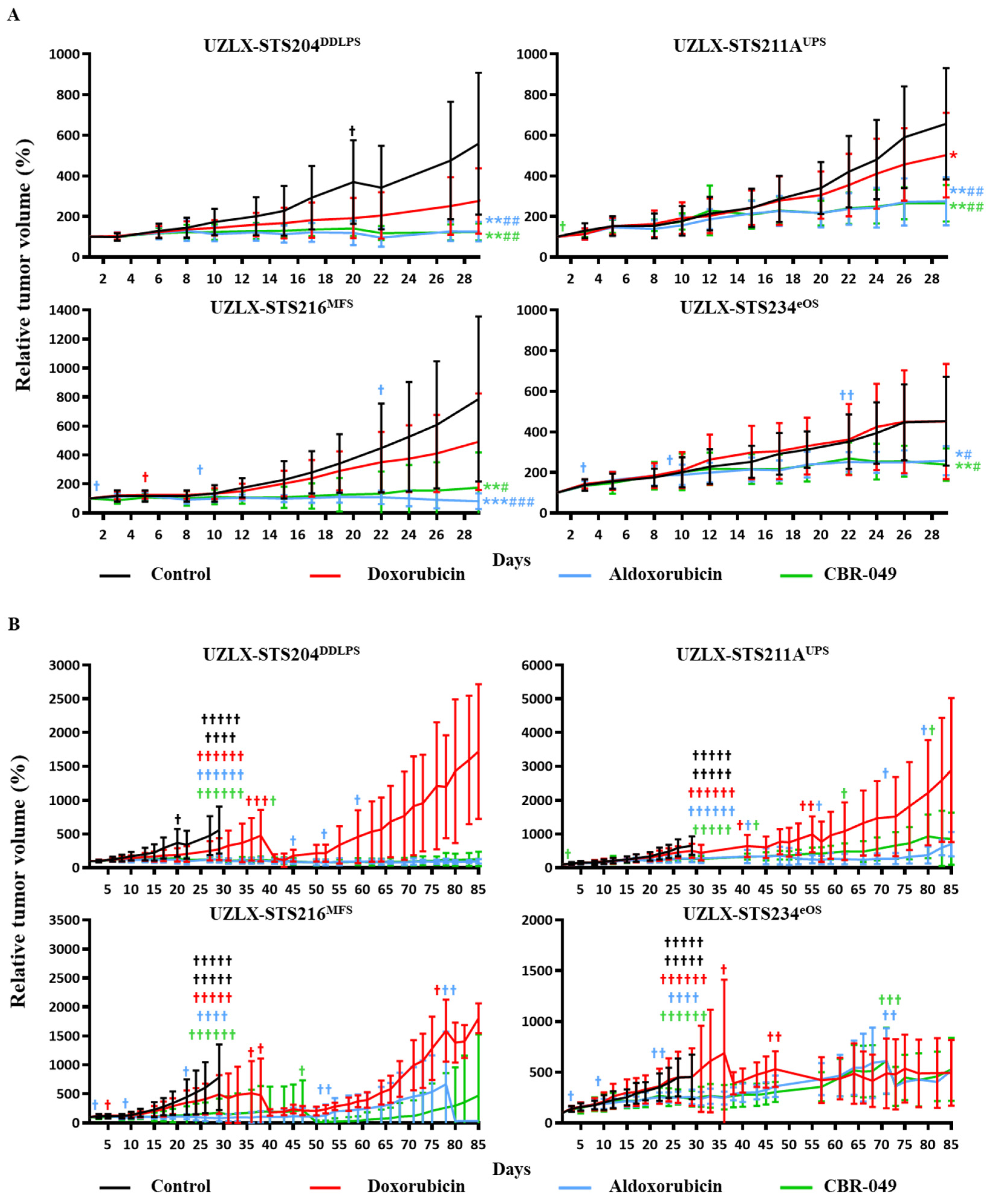
3.3.1. Tumor Volume Evaluation
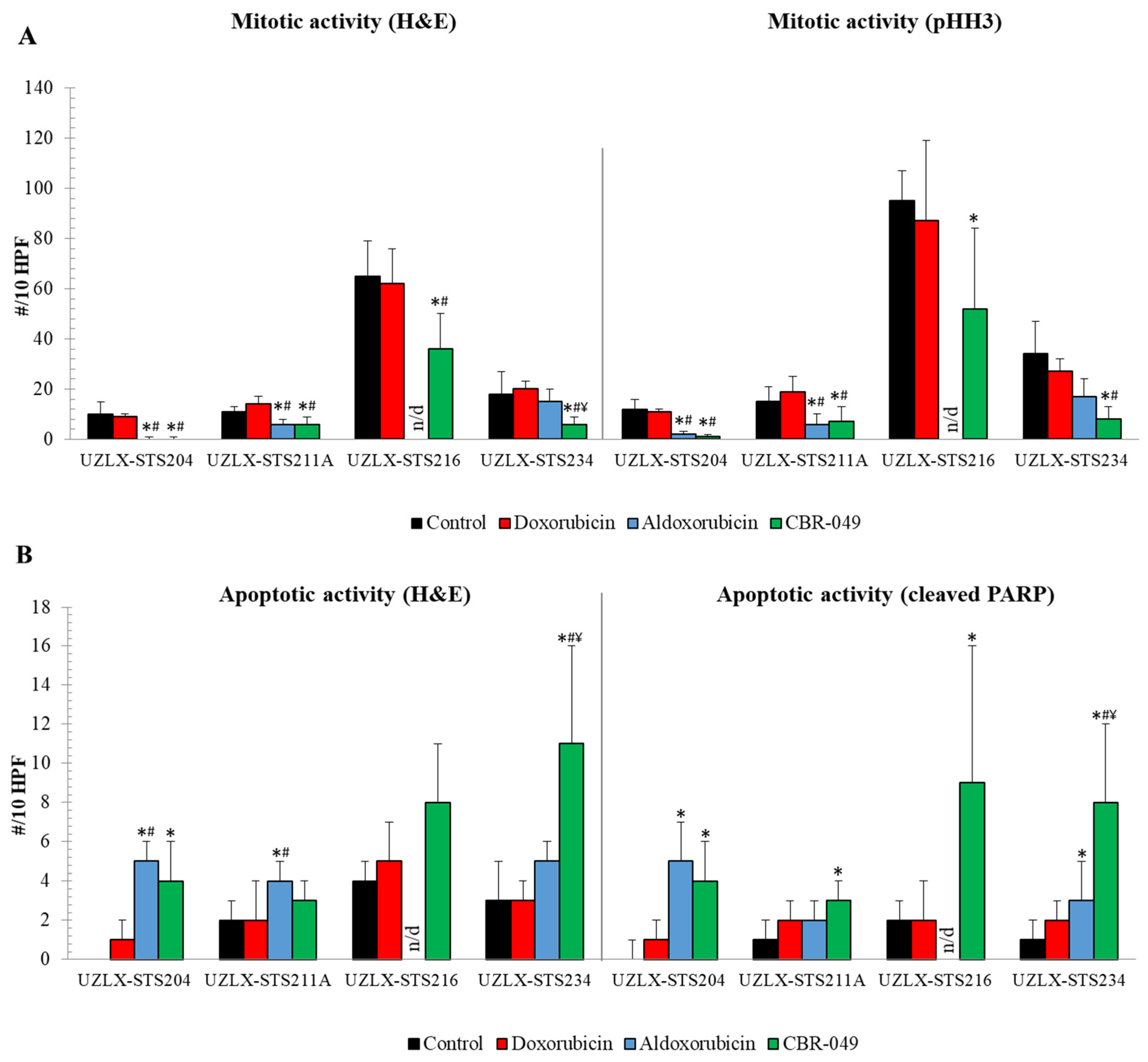
3.3.2. Histological Assessment
3.4. THOP1 Expression and Tumor Growth Delay
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schöffski, P.; Cornillie, J.; Wozniak, A.; Li, H.; Hompes, D. Soft Tissue Sarcoma: An Update on Systemic Treatment Options for Patients with Advanced Disease. Oncol. Res. Treat. 2014, 37, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Clark, M.A.; Fisher, C.; Judson, I.; Thomas, J.M. Soft-Tissue Sarcomas in Adults. N. Engl. J. Med. 2005, 353, 701–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamin, R.S.; Wiernik, P.H.; Bachur, N.R. Adriamycin: A new effective agent in the therapy of disseminated sarcomas. Med. Pediatr. Oncol. 1975, 1, 63–76. [Google Scholar] [CrossRef] [PubMed]
- Judson, I.; Verweij, J.; Gelderblom, H.; Hartmann, J.T.; Schöffski, P.; Blay, J.-Y.; Kerst, J.M.; Sufliarsky, J.; Whelan, J.; Hohenberger, P.; et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: A randomised controlled phase 3 trial. Lancet Oncol. 2014, 15, 415–423. [Google Scholar] [CrossRef]
- Ryan, C.W.; Merimsky, O.; Agulnik, M.; Blay, J.-Y.; Schuetze, S.M.; Van Tine, B.A.; Jones, R.L.; Elias, A.D.; Choy, E.; Alcindor, T.; et al. PICASSO III: A Phase III, Placebo-Controlled Study of Doxorubicin with or without Palifosfamide in Patients with Metastatic Soft Tissue Sarcoma. J. Clin. Oncol. 2016, 34, 3898–3905. [Google Scholar] [CrossRef]
- Seddon, B.; Strauss, S.J.; Whelan, J.; Leahy, M.; Woll, P.; Cowie, F.; Rothermundt, C.; Wood, Z.; Benson, C.; Ali, N.; et al. Gemcitabine and docetaxel versus doxorubicin as first-line treatment in previously untreated advanced unresectable or metastatic soft-tissue sarcomas (GeDDiS): A randomised controlled phase 3 trial. Lancet Oncol. 2017, 18, 1397–1410. [Google Scholar] [CrossRef] [Green Version]
- Tap, W.D.; Papai, Z.; Van Tine, B.A.; Attia, S.; Ganjoo, K.N.; Jones, R.L.; Schuetze, S.; Reed, D.; Chawla, S.P.; Riedel, R.F.; et al. Doxorubicin plus evofosfamide versus doxorubicin alone in locally advanced, unresectable or metastatic soft-tissue sarcoma (TH CR-406/SARC021): An international, multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2017, 18, 1089–1103. [Google Scholar] [CrossRef]
- Tacar, O.; Sriamornsak, P.; Dass, C.R. Doxorubicin: An update on anticancer molecular action, toxicity and novel drug delivery systems. J. Pharm. Pharmacol. 2013, 65, 157–170. [Google Scholar] [CrossRef]
- Bull, F.E.; Von Hoff, D.D.; Balcerzak, S.P.; Stephens, R.L.; Panettiere, F.J. Phase II trial of mitoxantrone in advanced sarco-mas: A Southwest Oncology Group study. Cancer Treat. Rep. 1985, 69, 231–233. [Google Scholar] [PubMed]
- Nielsen, O.S.; Dombernowsky, P.; Mouridsen, H.T.; Crowther, D.; Verweij, J.; Buesa, J.; Steward, W.P.; Daugaard, S.; Van Glabbeke, M.; Kirkpatrick, A.E.; et al. High-dose epirubicin is not an alternative to standard-dose doxorubicin in the treatment of advanced soft tissue sarcomas. A study of the EORTC soft tissue and bone sarcoma group. Br. J. Cancer 1998, 78, 1634–1639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Judson, I.; Radford, J.; Harris, M.; Blay, J.-Y.; van Hoesel, Q.; le Cesne, A.; van Oosterom, A.; Clemons, M.; Kamby, C.; Hermans, C.; et al. Randomised phase II trial of pegylated liposomal doxorubicin (DOXIL®/CAELYX®) versus doxorubicin in the treatment of advanced or metastatic soft tissue sarcoma: A study by the EORTC Soft Tissue and Bone Sarcoma Group. Eur. J. Cancer 2001, 37, 870–877. [Google Scholar] [CrossRef]
- Lebrecht, D.; Geist, A.; Ketelsen, U.-P.; Haberstroh, J.; Setzer, B.; Kratz, F.; Walker, U.A. The 6-maleimidocaproyl hydrazone derivative of doxorubicin (DOXO-EMCH) is superior to free doxorubicin with respect to cardiotoxicity and mitochondrial damage. Int. J. Cancer 2006, 120, 927–934. [Google Scholar] [CrossRef]
- Unger, C.; Häring, B.; Medinger, M.; Drevs, J.; Steinbild, S.; Kratz, F.; Mross, K. Phase I and Pharmacokinetic Study of the (6-Maleimidocaproyl) Hydrazone Derivative of Doxorubicin. Clin. Cancer Res. 2007, 13, 4858–4866. [Google Scholar] [CrossRef] [Green Version]
- Chawla, S.P.; Ganjoo, K.N.; Schuetze, S.; Papai, Z.; Van Tine, B.A.; Choy, E.; Liebner, D.A.; Agulnik, M.; Chawla, S.; Wieland, S.; et al. Phase III study of aldoxorubicin vs investigators’ choice as treatment for relapsed/refractory soft tissue sarcomas. J. Clin. Oncol. 2017, 35, 11000. [Google Scholar] [CrossRef]
- Casazza, A.; Van Helleputte, L.; Van Renterghem, B.; Pokreisz, P.; De Geest, N.; De Petrini, M.; Janssens, T.; Pellens, M.; Diricx, M.; Riera-Domingo, C.; et al. PhAc-ALGP-Dox, a novel anti-cancer prodrug with targeted activation and improved therapeutic index. Mol. Cancer Ther. 2022. published online ahead of print, 11 February 2022. [Google Scholar] [CrossRef] [PubMed]
- Ravel, D.; Dubois, V.; Quinonero, J.; Meyer-Losic, F.; Delord, J.; Rochaix, P.; Nicolazzi, C.; Ribes, F.; Mazerolles, C.; Assouly, E.; et al. Preclinical Toxicity, Toxicokinetics, and Antitumoral Efficacy Studies of DTS-201, a Tumor-Selective Peptidic Prodrug of Doxorubicin. Clin. Cancer Res. 2008, 14, 1258–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dohi, O.; Ohtani, H.; Hatori, M.; Sato, E.; Hosaka, M.; Nagura, H.; Itoi, E.; Kokubun, S. Histogenesis-specific expression of fibroblast activation protein and dipeptidylpeptidase-IV in human bone and soft tissue tumours. Histopathology 2009, 55, 432–440. [Google Scholar] [CrossRef] [Green Version]
- Deniz, K.; Çoban, G.; Okten, T. Anti-CD10 (56C6) expression in soft tissue sarcomas. Pathol. Res. Pract. 2012, 208, 281–285. [Google Scholar] [CrossRef]
- Cornillie, J.; Wozniak, A.; Pokreisz, P.; Casazza, A.; Vreys, L.; Wellens, J.; Vanleeuw, U.; Gebreyohannes, Y.K.; Debiec-Rychter, M.; Sciot, R.; et al. In vivo antitumoral efficacy of PhAc-ALGP-doxorubicin, an enzyme-activated doxorubicin prodrug, in patient-derived soft tissue sarcoma xenograft models. Mol. Cancer Ther. 2017, 16, 1566–1575. [Google Scholar] [CrossRef] [Green Version]
- Cornillie, J.; Wozniak, A.; Li, H.; Wang, Y.; Boeckx, B.; Gebreyohannes, Y.K.; Wellens, J.; Vanleeuw, U.; Hompes, D.; Stas, M.; et al. Establishment and Characterization of Histologically and Molecularly Stable Soft-tissue Sarcoma Xenograft Models for Biological Studies and Preclinical Drug Testing. Mol. Cancer Ther. 2019, 18, 1168–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornillie, J.; Wozniak, A.; Van Renterghem, B.; Van Winkel, N.; Wellens, J.; Gebreyohannes, Y.K.; Debiec-Rychter, M.; Sciot, R.; Hompes, D.; Schöffski, P. Assessment of the platelet-derived growth factor receptor alpha antibody olaratumab in a panel of patient-derived soft tissue sarcoma xenografts. BMC Cancer 2019, 19, 724. [Google Scholar] [CrossRef] [PubMed]
- Demetri, G.D.; von Mehren, M.; Jones, R.L.; Hensley, M.L.; Schuetze, S.M.; Staddon, A.; Milhem, M.; Elias, A.; Ganjoo, K.; Tawbi, H.; et al. Efficacy and Safety of Trabectedin or Dacarbazine for Metastatic Liposarcoma or Leiomyosarcoma After Failure of Conventional Chemotherapy: Results of a Phase III Randomized Multicenter Clinical Trial. J. Clin. Oncol. 2016, 34, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Schöffski, P.; Chawla, S.; Maki, R.G.; Italiano, A.; Gelderblom, H.; Choy, E.; Grignani, G.; Camargo, V.; Bauer, S.; Rha, S.Y.; et al. Eribulin versus dacarbazine in previously treated patients with advanced liposarcoma or leiomyosarcoma: A randomised, open-label, multicentre, phase 3 trial. Lancet 2016, 387, 1629–1637. [Google Scholar] [CrossRef]
- Van der Graaf, W.T.; Blay, J.-Y.; Chawla, S.P.; Kim, D.-W.; Bui-Nguyen, B.; Casali, P.G.; Schöffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2012, 379, 1879–1886. [Google Scholar] [CrossRef]
- Al Shoyaib, A.; Archie, S.R.; Karamyan, V.T. Intraperitoneal Route of Drug Administration: Should it Be Used in Experimental Animal Studies? Pharm. Res. 2019, 37, 12. [Google Scholar] [CrossRef]
- Ener, R.A.; Meglathery, S.B.; Styler, M. Extravasation of systemic hemato-oncological therapies. Ann. Oncol. 2004, 15, 858–862. [Google Scholar] [CrossRef]
- Kratz, F.; Ehling, G.; Kauffmann, H.-M.; Unger, C. Acute and repeat-dose toxicity studies of the (6-maleimidocaproyl)hydrazone derivative of doxorubicin (DOXO-EMCH), an albumin-binding prodrug of the anticancer agent doxorubicin. Hum. Exp. Toxicol. 2007, 26, 19–35. [Google Scholar] [CrossRef]
- Marrero, L.; Wyczechowska, D.; Musto, A.E.; Wilk, A.; Vashistha, H.; Zapata, A.; Walker, C.; Velasco-Gonzalez, C.; Parsons, C.; Wieland, S.; et al. Therapeutic Efficacy of Aldoxorubicin in an Intracranial Xenograft Mouse Model of Human Glioblastoma. Neoplasia 2014, 16, 874–882. [Google Scholar] [CrossRef] [Green Version]
- Chawla, S.P.; Papai, Z.; Mukhametshina, G.; Sankhala, K.; Vasylyev, L.; Fedenko, A.; Khamly, K.; Ganjoo, K.; Nagarkar, R.; Wieland, S.; et al. First-Line Aldoxorubicin vs Doxorubicin in Metastatic or Locally Advanced Unresectable Soft-Tissue Sarcoma: A Phase 2b Randomized Clinical Trial. JAMA Oncol. 2015, 1, 1272. [Google Scholar] [CrossRef] [Green Version]
- Hidalgo, M.; Amant, F.; Biankin, A.V.; Budinská, E.; Byrne, A.T.; Caldas, C.; Clarke, R.B.; De Jong, S.; Jonkers, J.; Mælandsmo, G.M.; et al. Patient-Derived Xenograft Models: An Emerging Platform for Translational Cancer Research. Cancer Discov. 2014, 4, 998–1013. [Google Scholar] [CrossRef] [Green Version]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Van Renterghem, B.; Wozniak, A.; Tarantola, L.; Casazza, A.; Wellens, J.; Nysen, M.; Vanleeuw, U.; Lee, C.-J.; Reyns, G.; Sciot, R.; et al. Enhanced Antitumor Efficacy of PhAc-ALGP-Dox, an Enzyme-Activated Doxorubicin Prodrug, in a Panel of THOP1-Expressing Patient-Derived Xenografts of Soft Tissue Sarcoma. Biomedicines 2022, 10, 862. https://doi.org/10.3390/biomedicines10040862
Van Renterghem B, Wozniak A, Tarantola L, Casazza A, Wellens J, Nysen M, Vanleeuw U, Lee C-J, Reyns G, Sciot R, et al. Enhanced Antitumor Efficacy of PhAc-ALGP-Dox, an Enzyme-Activated Doxorubicin Prodrug, in a Panel of THOP1-Expressing Patient-Derived Xenografts of Soft Tissue Sarcoma. Biomedicines. 2022; 10(4):862. https://doi.org/10.3390/biomedicines10040862
Chicago/Turabian StyleVan Renterghem, Britt, Agnieszka Wozniak, Ludovica Tarantola, Andrea Casazza, Jasmien Wellens, Madita Nysen, Ulla Vanleeuw, Che-Jui Lee, Geert Reyns, Raf Sciot, and et al. 2022. "Enhanced Antitumor Efficacy of PhAc-ALGP-Dox, an Enzyme-Activated Doxorubicin Prodrug, in a Panel of THOP1-Expressing Patient-Derived Xenografts of Soft Tissue Sarcoma" Biomedicines 10, no. 4: 862. https://doi.org/10.3390/biomedicines10040862