
Histological and Immunohistochemical Analysis of the Effects of Topical Melatonin Treatment Associated with Collagen Sponge and rhBMP-2 Protein on Bone Remodeling

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
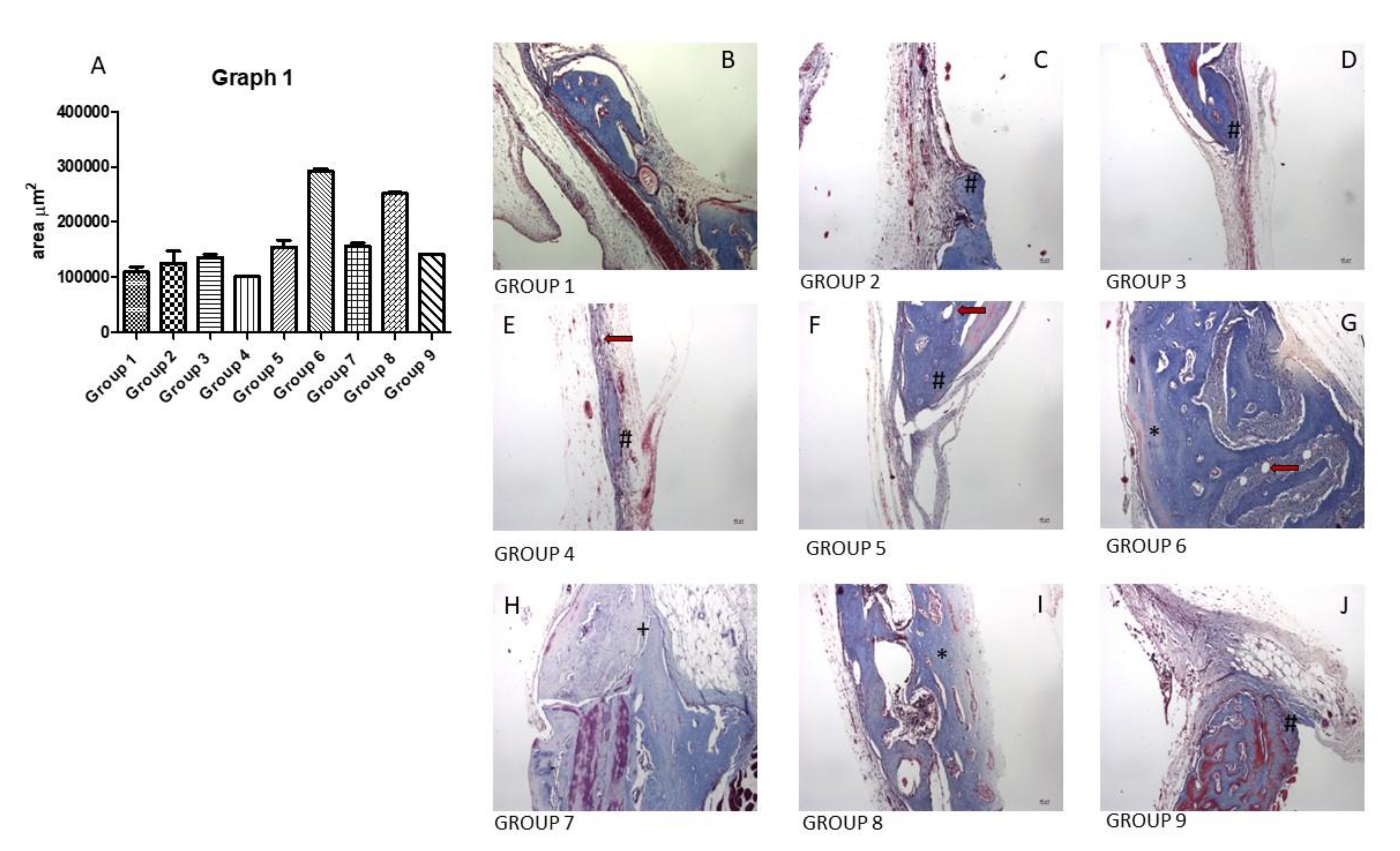
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lei, H.; Gui, L.; Xiao, R. The effect of anticoagulants on the quality and biological efficacy of platelet-rich plasma. Clin. Biochem. 2009, 42, 1452–1460. [Google Scholar] [CrossRef] [PubMed]
- Pandi-Perumal, S.R.; Srinivasan, V.; Maestroni, G.J.; Cardinali, D.P.; Poeggeler, B.; Hardeland, R. Melatonin, Nature’s most versatile biological signal? FEBS J. 2006, 273, 2813–2838. [Google Scholar] [CrossRef] [PubMed]
- Zawilska, J.B.; Skene, D.J.; Arendt, J. Physiology and pharmacology of melatonin in relation to biological rhythms. Pharm. Rep. 2009, 61, 383–410. [Google Scholar] [CrossRef]
- Lima, F.B.; Machado, U.F.; Bartol, I.; Seraphim, P.M.; Sumida, D.H.; Moraes, S.M.; Hell, N.S.; Okamoto, M.M.; Saad, M.J.; Carvalho, C.R.; et al. Pinealectomy causes glucose intolerance and decreases adipose cell responsiveness to insulin in rats. Am. J. Physiol. 1998, 275, 934–941. [Google Scholar] [CrossRef]
- Conti, A.; Conconi, S.; Hertens, E.; Skwarlo-Sonta, K.; Markowska, M.; Maestroni, J.M. Evidence for melatonin synthesis in mouse and human bone marrow cells. J. Pineal. Res. 2000, 28, 193–202. [Google Scholar] [CrossRef] [PubMed]
- Hardeland, R.; Madrid, J.A.; Tan, D.X.; Reiter, R.J. Melatonin, the circadian multioscillator system and health, the need for detailed analyses of peripheral melatonin signaling. J. Pineal. Res. 2012, 52, 139–166. [Google Scholar] [CrossRef] [PubMed]
- Greenspan Sl Dresner-Pollak, R.; Parker, R.A.; London, D.; Ferguson, L. Diurnal variation of bone mineral turnover in elderly men and women. Calcif. Tissue Int. 1997, 60, 419–423. [Google Scholar] [CrossRef]
- Ostrowska, Z.; Kos-Kudla, B.; Marek, B.; Kajdaniuk, D. Influence of lighting conditions on daily rhythm of bone metabolism in rats and possible involvement of melatonin and other hormones in this process. Endocr. Regul. 2003, 37, 163–174. [Google Scholar]
- Koyama, H.; Nakade, O.; Takada, Y.; Kaku, T.; Lau, K.H. Melatonin at pharmacologic doses increases bone mass by suppressing resorption through down-regulation of the RANKL-mediated osteoclast formation and activation. J. Bone Min. Res. 2002, 17, 1219–1229. [Google Scholar] [CrossRef]
- Nakade, O.; Koyama, H.; Ariji, H.; Yajima, A.; Kaku, T. Melatonin stimulates proliferation and type Isynthesis in human bone cells in vitro. J. Pineal Res. 1999, 27, 106–110. [Google Scholar] [CrossRef]
- Roth, J.A.; Kim, B.G.; Lin, W.L.; Cho, M.I. Melatonin promotes osteoblast differentiation and bone formation. J. Biol. Chem. 1999, 274, 22041–22047. [Google Scholar] [CrossRef] [PubMed]
- Satomura, K.; Tobiume, S.; Tokuyama, R.; Yamasaki, Y.; Kudoh, K.; Maeda, E.; Nagayama, M. Melatonin at pharmacological doses enhances human osteoblastic differentiation in vitro and promotes mouse cortical bone formation in vivo. J. Pineal. Res. 2007, 42, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Park, K.H.; Kang, J.W.; Lee, E.M.; Kim, J.S.; Rhee, Y.H.; Kim, M.; Jeong, S.J.; Park, Y.G.; Kim, S.H. Melatonin promotes osteoblastic differentiation through the BMP/ERK/Wnt signaling pathways. J. Pineal Res. 2011, 51, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Su, P.; Xu, C.; Chen, C.; Liang, A.; Du, K.; Peng, Y.; Huang, D. Melatonin inhibits adipogenesis and enhances osteogenesis of human mesenchymal stem cells by suppressing PPAR-gamma expression and enhancing Runx2 expression. J. Pineal. Res. 2010, 49, 364–372. [Google Scholar] [CrossRef]
- Cutando, A.; Arana, C.; Gómez-Moreno, G.; Escames, G.; López, A.; Ferrera MJReiter, R.J.; Acu-a-Castroviejo, D. Local application of melatonin into alveolar sockets of beagle dogs reduces tooth removal-induced oxidative stress. J. Periodontol. 2007, 78, 576–583. [Google Scholar] [CrossRef] [Green Version]
- Mediero, A.; Wilder, T.; Perez-Aso, M.; Cronstein, B.N. Direct or indirect stimulation of adenosine A2A receptors enhances bone regeneration as well as bone morphogenetic protein-2. FASEB J. 2015, 29, 1577–1590. [Google Scholar] [CrossRef] [Green Version]
- Ripamonti, U.; Reddi, A.H. Periodontal regeneration, potential role of bone morphogenetic proteins. J. Periodontal. Res. 1994, 29, 225–235. [Google Scholar] [CrossRef]
- Issa, J.P.M.; Defino, H.L.A.; Coutinho-Netto, J.; Volpon, J.B.; Regalo, S.C.H.; Siéssere, S.; Tiossi, R. Evaluation of rhBMP-2 and natural late as potential osteogenic proteins in critical size defects by histomorphometric methods. Anat. Record. 2010, 293, 794–801. [Google Scholar] [CrossRef]
- Siéssere, S.; Sousa, L.G.; Issa, J.P.M.; Iyomasa, M.M.; Pitol, D.L.; Barbosa, A.P.A.; Semprini, M.; Sebald, W.; Bentley, M.V.; Regalo, S.C.H. Application of low-level laser irradiation (LLLI) and rhBMP-2 in critical bone defect of ovariectomized rats, histomorphometric evaluation. Photomed. Laser Surg. 2011, 29, 453–458. [Google Scholar] [CrossRef]
- Issa, J.P.; Gonzaga, M.; Kotake, B.G.; de Lucia, C.; Ervolino, E.; Iyomasa, M. Bone repair of critical size defects treated with autogenic, allogenic, or xenogenic bone grafts alone or in combination with rhBMP-2. Clin. Oral. Impl. Res. 2016, 27, 558–566. [Google Scholar] [CrossRef]
- Wikesjö, U.M.E.; Qahash, M.; Polimeni, G.; Susin, C.; Shanaman, R.H.; Rohrer, M.D.; Wozney, J.M.; Salão, J. Alveolar ridge augmentation using implants coated with recombinant human bone morReferências, phogenetic protein-2, histologic observations. J. Clin. Periodontol. 2008, 35, 1001–1010. [Google Scholar] [CrossRef] [PubMed]
- Kotake, B.G.; Salzedas, L.M.; Ervolino, E.; Calzzani, R.A.; Sebald, W.; Issa, J.P.M. Bone Recuperation After rhBMP-2 Insertion in Alcoholic Animals-Experimental Study. Curr. Pharm. Des. 2015, 21, 3557–3564. [Google Scholar] [CrossRef] [PubMed]
- Schindeler, A.; McDonald, M.M.; Bokko, P.; Little, D.G. Bone remodeling during fracture repair the cellular picture. Semin. Cell Dev. Biol. 2008, 19, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Turri, A.; Elgali, I.; Vazirisani, F.; Johansson, A.; Emanuelsson, L.; Dahlin, C.; Thomsen, P.; Omar, O. Guided bone regeneration is promoted by the molecular events in the membrane compartment. Biomaterials 2016, 84, 167–183. [Google Scholar] [CrossRef] [Green Version]
- Gruber, R.; Stadlinger, B.; Terheyden, H. Cell-to-cell communication in guided bone regeneration, molecular and cellular mechanisms. Clin. Oral Implant. Res. 2017, 28, 1139–1146. [Google Scholar] [CrossRef]
- Haas, R.; Haidvogl, D.; Donath, K.; Watzek, G. Freeze-dried homogeneous and heterogeneous bone for sinus augmentation in sheep. Part I, histological findings. Clin. Oral Implant. Res. 2012, 13, 396–404. [Google Scholar] [CrossRef]
- Gómez-Moreno, G.; Aguilar-Salvatierra, A.; Boquete-Castro, A.; Guardia, J.; Piattelli, A.; Perrotti, V. Outcomes of topical applications of melatonin in implant dentistry. Implant. Dent. 2015, 24, 25–30. [Google Scholar] [CrossRef]
- Ramírez-Fernández, M.P.; Calvo-Guirado, J.L.; De-Val, J.E.M.S.; Delgado-Ruiz, R.A.; Negri, B.; Pardo-Zamora, G. Melatonin promotes angiogenesis during repair of bone defects, A radiological and histomorphometric study in rabbit tibiae. Clin. Oral Investig. 2013, 17, 147–158. [Google Scholar] [CrossRef]
- Cutando, A.; Gómez-Moreno, G.; Arana, C.; Munoz, L.; Lopez-Pena, M.; Stephenson, J. Melatonin stimulates osteointegration of dental implants. J. Pineal. Res. 2008, 45, 174–179. [Google Scholar] [CrossRef]
- Hankenson, K.D.; Zimmerman, G.; Marcucio, R. Biological perspectives of delayed fracture healing. Injury 2014, 45 (Suppl. 2), S8–S15. [Google Scholar] [CrossRef] [Green Version]
- Hollinger, J.O.; Kleinschmidt, J.C. The critical size defect as an experimental model to test bone repair materials. J. Craniofac. Surg. 1990, 1, 60–68. [Google Scholar]
- Gonzaga, M.G.; Dos Santos Kotake, B.G.; de Figueiredo, F.A.T.; Feldman, S.; Ervolino, E.; Dos Santos, M.C.G.; Issa, J.P.M. Effectiveness of rhBMP-2 association to autogenous, allogeneic, and heterologous bone grafts. Microsc. Res. Tech. 2019, 82, 689–695. [Google Scholar] [CrossRef] [PubMed]
- Burg, K.J.; Porter, S.; Kellam, J.F. Biomaterial developments for bone tissue engineering. Biomaterials 2000, 21, 2347–2359. [Google Scholar] [CrossRef]
- Polo-Corrales, L.; Latorre-Esteves, M.; Ramirez-Vick, J.E. Scaffold design for bone regeneration. J. Nanosci. Nanotechnol. 2014, 14, 15–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grgurevic, L.; Erjavec, I.; Gupta, M.; Pecin, M.; Bordukalo-Niksic, T.; Stokovic, N.; Vnuk, D.; Farkas, V.; Capak, H.; Milosevic, M.; et al. Autologous blood coagulum containing rhBMP6 induces new bone formation to promote anterior lumbar interbody fusion (ALIF) and posterolateral lumbar fusion (PLF) of spine in sheep. Bone 2020, 138, 115448. [Google Scholar] [CrossRef] [PubMed]
- Basaloglu, H.K.; Turgut, M.; Şirin, C.; Uyanikgil, Y.; Demirci, B.; Cetin, E.O. The influence of functional pinealectomy and exogenous melatonin application on healing of burr hole in adult rat calvaria: A histological and immunohistochemical study. Folia Morphol. 2022, 81, 271–279. [Google Scholar] [CrossRef]
- Shino, H.; Hasuike, A.; Arai, Y.; Honda, M.; Isokawa, K.; Sato, S. Melatonin enhances vertical bone augmentation in rat calvaria secluded spaces. Med. Oral Patol Oral Cir. Bucal. 2016, 21, e122–e126. [Google Scholar] [CrossRef]
- Liu, P.I.; Chang, A.C.; Lai, J.L.; Lin, T.H.; Tsai, C.H.; Chen, P.C.; Jiang, Y.J.; Lin, L.W.; Huang, W.C.; Yang, S.F.; et al. Melatonin interrupts osteoclast functioning and suppresses tumor-secreted RANKL expression, implications for bone metastases. Oncogene 2021, 40, 1503–1515. [Google Scholar] [CrossRef]
- Wang, E.A.; Rosen, V.; D’Alessandro, J.S.; Bauduy, M.; Cordes, P.; Harada, T.; Israel, D.I.; Hewick, R.M.; Kerns, K.M.; LaPan, P.; et al. Recombinant human bone morphogenetic protein induces bone formation. Proc. Natl. Acad. Sci. USA 1990, 87, 2220–2224. [Google Scholar] [CrossRef] [Green Version]
- Simpson, H. Bone consolidation is enhanced by rhBMP-2 in a rabbit model of distraction osteogenesis. J. Orthop. Res. 2002, 20, 779–788. [Google Scholar]
- Croteau, S.; Rauch, F.; Silvestri, A.; Hamdy, R.C. Bone morphogenetic proteins in orthopedics: From basic science to clinical practice. Orthopedics 1999, 22, 686–697. [Google Scholar] [PubMed]
- Elgali, I.; Omar, O.; Dahlin, C.; Thomsen, P. Guided bone regeneration: Materials and biological mechanisms revisited. Eur. J. Oral. Sci. 2017, 125, 315–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Urban, I.A.; Monje, A. Guided Bone Regeneration in Alveolar Bone Reconstruction. Oral. Maxillofac. Surg. Clin. N. Am. 2019, 31, 331–338. [Google Scholar] [CrossRef]
- Schenk, R.K.; Buser, D.; Hardwick, W.R.; Dahlin, C. Healing pattern of bone regeneration in membrane-protected defects, a histologic study in the canine mandible. Int. J. Oral. Maxillofac. Implant. 1994, 9, 13–29. [Google Scholar]
- Jung, R.E.; Glauser, R.; Schärer, P.; Hämmerle, C.H.; Sailer, H.F.; Weber, F.E. Effect of rhBMP-2 on guided bone regeneration in humans. Clin. Oral. Implant. Res. 2003, 14, 556–568. [Google Scholar] [CrossRef]
- Schorn, L.; Sproll, C.; Ommerborn, M.; Naujoks, C.; Kübler, N.R.; Depprich, R. Vertical bone regeneration using rhBMP-2 and VEGF. Head Face Med. 2017, 13, 11. [Google Scholar] [CrossRef] [Green Version]
- Wikesjö, U.M.; Qahash, M.; Thomson, R.C.; Cook, A.D.; Rohrer, M.D.; Wozney, J.M.; Hardwick, W.R. rhBMP-2 significantly enhances guided bone regeneration. Clin. Oral. Implant. Res. 2004, 15, 194–204. [Google Scholar] [CrossRef]
- Cicciù, M.; Fiorillo, L.; Cervino, G.; Habal, M.B. Bone Morophogenetic Protein Application as Grafting Materials for Bone Regeneration in Craniofacial Surgery: Current Application and Future Directions. J. Craniofac. Surg. 2021, 32, 787–793. [Google Scholar] [CrossRef]
- Boden, S.D.; Zdeblick, T.A.; Sandhu, H.S.; Heim, S.E. The use of rhBMP-2 in interbody fusion cages. Definitive evidence of osteoinduction in humans, a preliminary report. Spine 2000, 25, 376–381. [Google Scholar] [CrossRef]
- Talwar, R.; Di Silvio, L.; Hughes, F.J.; King, G.N. Effects of carrier release kinetics on bone morphogenetic protein-2-induced periodontal regeneration in vivo. J. Clin. Periodontol. 2001, 28, 340–347. [Google Scholar] [CrossRef]
- Wozney, J.M.; Rosen, V.; Celeste, A.J.; Mitsock, L.M.; Whitters, M.J.; Kriz, R.W.; Hewick, R.M.; Wang, E.A. Novel regulators of bone formation, molecular clones and activities. Science 1988, 242, 1528–1534. [Google Scholar] [CrossRef] [PubMed]
- Toriumi, D.M.; Kotler, H.S.; Luxenberg, D.P.; Holtrop, M.E.; Wang, E.A. Mandibular reconstruction with a recombinant bone-inducing factor. Functional, histologic, and biomechanical evaluation. Arch. Otolaryngol. Head Neck Surg. 1991, 117, 1101–1112. [Google Scholar] [CrossRef] [PubMed]
- Sampath, T.K.; Reddi, A.H. Dissociative extraction and reconstitution of extracellular matrix components involved in local bone differentiation. Proc. Natl. Acad. Sci. USA 1981, 78, 7599–7603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burkus, J.K.; Gornet, M.F.; Schuler, T.C.; Kleeman, T.J.; Zdeblick, T.A. Six-year outcomes of anterior lumbar interbody arthrodesis with use of interbody fusion cages and recombinant human bone morphogenetic protein-2. JBJS 2009, 91, 1181–1189. [Google Scholar] [CrossRef]
- Carlevaro, M.F.; Cermelli, S.; Cancedda, R. Descalzi Cancedda Vascular endothelial growth factor (VEGF) in cartilage neovascularization and chondrocyte differentiation, auto-paracrine role during endochondral bone formation. J. Cell Sci. 2000, 113, 59–69. [Google Scholar] [CrossRef]
- Street, J.; Bao, M.; de Guzman, L.; Bunting, S.; Peale, F.V., Jr.; Ferrara, N.; Steinmetz, H.; Hoeffel, J.; Cleland, J.L.; Daugherty, A.; et al. Vascular endothelial growth factor stimulates bone repair by promoting angiogenesis and bone turnover. Proc. Natl. Acad. Sci. USA 2002, 99, 9656–9661. [Google Scholar] [CrossRef] [Green Version]
- Coates, P. Bone turnover markers. Aust. Fam. Physician 2013, 42, 285–287. [Google Scholar]
- Chen, W.; Chen, X.; Chen, A.C.; Shi, Q.; Pan, G.; Pei, M.; Yang, H.; Liu, T.; He, F. Melatonin restores the osteoporosis-impaired osteogenic potential of bone marrow mesenchymal stem cells by preserving SIRT1-mediated intracellular antioxidant properties. Free Radic Biol. Med. 2020, 146, 92–106. [Google Scholar] [CrossRef]
- Kesemenli, C.C.; Necmioğlu, S. The role of melatonin as a link between head injury and enhanced osteogenesis. Med. Hypotheses 2005, 65, 605–606. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Treatments |
|---|---|
| Group 1 | blood clot |
| Group 2 | blood clot + Scaffold |
| Group 3 | blood clot + Scaffold + Melatonin 1 µg |
| Group 4 | blood clot + Scaffold + Melatonin 10 µg |
| Group 5 | blood clot + Scaffold + Melatonin 100 µg |
| Group 6 | blood clot + Scaffold + Melatonin 1 µg + rhBMP-2 |
| Group 7 | blood clot + Scaffold + Melatonin 10 µg + rhBMP-2 |
| Group 8 | blood clot + Scaffold + Melatonin 100 µg + rhBMP-2 |
| Group 9 | blood clot + Scaffold + rhBMP-2 |
| Group 1 | Group 2 | Group 3 | Group 4 | Group 5 | Group 6 | Group 7 | Group 8 | Group 9 | |
|---|---|---|---|---|---|---|---|---|---|
| OPG | ++++ | + | +++ | +++ | +++ | ++++ | ++ | ++++ | +++ |
| CD31 | + | + | + | + | + | + | + | + | + |
| IL1β | ++ | ++ | ++ | +++ | ++ | ++ | ++ | ++ | ++ |
| IL6 | +++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ |
| IL10 | +++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ | +++ |
| Osteocalcin | +++ | + | ++ | ++ | ++ | +++ | +++ | +++ | +++ |
| Osteoprogeterin | ++++ | ++ | ++ | ++ | ++ | ++++ | +++ | ++++ | ++++ |
| RUNX2 | ++ | + | ++ | ++ | ++ | +++ | ++ | +++ | +++ |
| TRAP | ++ | + | ++ | ++ | ++ | ++ | ++ | ++ | ++ |
| VEGF | ++ | ++ | ++ | ++ | ++ | ++ | +++ | ++ | ++ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montarele, L.F.; Pitol, D.L.; Pereira, B.F.; Feldman, S.; Fazan, V.P.S.; Issa, J.P.M. Histological and Immunohistochemical Analysis of the Effects of Topical Melatonin Treatment Associated with Collagen Sponge and rhBMP-2 Protein on Bone Remodeling. Biomolecules 2022, 12, 1738. https://doi.org/10.3390/biom12121738
Montarele LF, Pitol DL, Pereira BF, Feldman S, Fazan VPS, Issa JPM. Histological and Immunohistochemical Analysis of the Effects of Topical Melatonin Treatment Associated with Collagen Sponge and rhBMP-2 Protein on Bone Remodeling. Biomolecules. 2022; 12(12):1738. https://doi.org/10.3390/biom12121738
Chicago/Turabian StyleMontarele, Leticia Ferreira, Dimitrius Leonardo Pitol, Bruno Fiorelini Pereira, Sara Feldman, Valéria Paula Sassoli Fazan, and João Paulo Mardegan Issa. 2022. "Histological and Immunohistochemical Analysis of the Effects of Topical Melatonin Treatment Associated with Collagen Sponge and rhBMP-2 Protein on Bone Remodeling" Biomolecules 12, no. 12: 1738. https://doi.org/10.3390/biom12121738