
Breastfeeding at Any Cost? Adverse Effects of Breastfeeding Pain on Mother–Infant Behavior

1
The Department of Psychology, The Hebrew University of Jerusalem, Jerusalem 9190501, Israel
2
Criminology Department, Bar-Ilan University, Ramat Gan 5290002, Israel
*
Author to whom correspondence should be addressed.
Biology 2023, 12(5), 636; https://doi.org/10.3390/biology12050636
Submission received: 18 March 2023
/
Revised: 11 April 2023
/
Accepted: 19 April 2023
/
Published: 22 April 2023
(This article belongs to the Special Issue Neural and Behavioural Mechanisms Underlying Human Bonding)
Abstract
:Simple Summary
Breastfeeding is encouraged worldwide due to its nutritional and bonding benefits, but more attention needs to be given to the potential psychological challenges it poses to new mothers. This study investigated whether breastfeeding pain relates to mothers’ and infants’ bonding behavior. Seventy-one mothers with varying levels of breastfeeding pain were videotaped with their infants during face-to-face interactions. We found that mothers with severe breastfeeding pain express less affect and less infant-directed gaze during interactive moments of engagement and play than mothers with no or moderate pain. Infants of mothers experiencing pain also express less affect and more mother-directed gaze than those of mothers not experiencing pain. These findings suggest that maternal pain can interfere with the behaviors of both mothers and infants, potentially impacting development and bonding. Since the mother–infant dyad is a codependent allostatic unit, the allostatic challenges of one partner can influence both partners. Therefore, nutritional advances should be considered along with additional allostatic consequences of breastfeeding to ensure the well-being of both mothers and infants.
Abstract
Breast milk is considered the ideal infant nutrition, and medical organizations encourage breastfeeding worldwide. Moreover, breastfeeding is often perceived as a natural and spontaneous socio-biological process and one of the fundamental roles of new mothers. While breastfeeding is beneficial, little scientific consideration has been given to its potential psychological challenges. Here, we investigate the phenomenon of breastfeeding pain in mothers and its association with maternal and infant behavioral regulation. During the postpartum weeks, the mother–infant dyad can be considered one allostatic unit directed at infant regulation and development. We hypothesize that pain comprises an allostatic challenge for mothers and will thus impair the capacity for dyadic regulation. To test this, we recruited 71 mothers with varying levels of breastfeeding pain and videotaped them with their infants (2–35 weeks old) during spontaneous face-to-face interactions. We quantified the individual differences in dyadic regulation by behaviorally coding the second-by-second affective expressions for each mother and infant throughout their interactions. We tested the extent to which breastfeeding pain alters affect regulation during mother–infant interactions. We discovered that mothers with severe breastfeeding pain express less affective expressions and less infant-directed gaze during interactive moments of engagement and play than mothers with no or moderate pain. Moreover, infants of mothers experiencing pain during breastfeeding express less affective expressions and more mother-directed gaze while interacting with their mothers than infants of mothers who are not in pain. This demonstrates that the allostatic challenge of maternal pain interferes with the behavioral regulation of both mothers and infants. Since the mother–infant dyad is a codependent allostatic unit, the allostatic challenges of one partner can impact the dyad and thus potentially impact child development, bonding, and mother and infant well-being. The challenges of breastfeeding should be considered in addition to the nutritional advances.
Keywords:
breastfeeding; bonding; maternal behavior; infant behavior; affect; regulation; ARCS; allostasis1. Introduction
Breast milk is widely considered the ideal nutrition for infants, advancing the health of both infants and mothers and promoting infant development [1]. For example, breast milk proteins decrease the risk of obesity, adiposity [2], and diabetes [3]. More extended periods of breastfeeding reduce the prevalence of Crohn’s disease [4], augment the infant’s immune system [5], and reduces cases of allergies and asthma [6]. Moreover, breastfeeding affects infants’ neural function [7] and anatomy. Infants exclusively breastfed for at least three months showed increased brain white matter in frontal cortical regions [8,9]. Breastfeeding is also associated with improved social and cognitive development [10], intelligence [11], memory [12], and language in infants [13]. Breastfeeding is advantageous for mothers too, and is associated with a reduced risk of breast cancer and diabetes [14,15]. Furthermore, some studies associate breastfeeding with improved maternal mood [16], sleep [17], maternal care [18], and mother–infant bonding [19,20,21]. Consequently, all major medical organizations recommend breastfeeding as a significant source of infant nutrition for at least one year [22,23,24,25].
Currently, most studies on breastfeeding have focused on the benefits for the infant and mother [26,27]. Yet, despite such consensual recommendations, women often choose not to breastfeed throughout their first postpartum year. While most women in the United States and Europe initiate breastfeeding, many mothers wean the infant within the first few postpartum weeks [27]. In 2019–2020, 83.9% of American women reported starting breastfeeding, yet only 25.8% continued breastfeeding exclusively after six months [28]. Shorter durations of breastfeeding were associated with psychological hardship, lower self-efficacy, and lower self-confidence [29]. In addition, a negative experience of breastfeeding is associated with symptoms of depression [30], a sense of struggle and loneliness [27], altered maternal mood, and sleep disturbances [31].
One of the main reasons to stop breastfeeding is pain [32]. Breastfeeding pain affects up to 68% of breastfeeding mothers [33,34] and is perceived as highly distressing [35]. Much research addressed breastfeeding pain, mainly concerning ankyloglossia (or tongue-tie) [36,37]. This research tested the effects of pain on breastfeeding quality [31,38] and breastfeeding outcomes [39,40,41]. Motivated to improve the feeding outcome and the maternal experience [34,42,43], several studies addressed the treatments for breastfeeding pain involving medication [44,45] or frenotomy [43,46]. While this research is mainly directed toward the outcome of feeding, no study we know addresses the effects of breastfeeding pain on the mother–infant relationship.
Pain can modulate and be modulated by social interactions. Positive social interactions alleviate pain [47,48,49,50,51,52], whereas negative social relations are associated with increased pain [49,50,51,53,54,55]. The opposite direction is also evident: pain can impact social behavior toward an individual in pain by eliciting prosocial behaviors in both humans and rodents [47,48,53,56]. Pain can also change the social tendencies of the individual in pain. At a physiological level, chronic pain promotes an allostatic load [57,58] characterized by neuroendocrine dysregulation, fatigue, and impaired mental and physical performance, which can adversely impact social interactions [59,60,61,62]. Specifically, pain was demonstrated to alter the expressions and regulation of affect [50,63,64]. Given the importance of expression and regulation of affect during social interactions, pain can interfere with the ability to interact, which is particularly relevant in the mother–infant bond.
At the beginning of life, the mother–infant relations focus on the infant’s survival and regulation. The newborn infant depends entirely on the mother (or the primary caregiver) to regulate most fundamental physiological processes [65,66,67,68,69,70]. This process is called Allostasis and refers to the ongoing adjustment of an individual’s internal milieu necessary for survival, growth, and reproduction [71,72,73,74]. To regulate the infant’s allostasis, mothers must be attuned to their infant’s behavioral cues and constantly address them to correct even subtle allostatic disturbances [75]. Accordingly, adjusted maternal care is essential for optimal child well-being and development [76,77,78].
Affect expressions and gaze are key behavioral features exchanged during social interactions [79,80]. Mothers attune their affective expressions to moments of mutual gaze [81,82] when infants are engaged in the interaction [83]. Consequently, with development, infants increase the duration of visual fixation on the mother’s face and express more affect during an interaction [84]. Infants’ positive and negative affective expressions indicate their regulation [85]. Accordingly, mothers tend to be sensitive and responsive to the infants’ affective expressions [85,86,87], resulting in the mutual facial coupling of affective expressions [84,88]. This positive feedback loop of gaze and facial expressions is essential for the infants’ affective development [75], teaching infants to synchronize and regulate their affect during social interactions. In this sense, mutual gaze and affective facial expressions are essential for mothers to infer the infant’s allostatic needs, provide attuned allostatic care, and promote infants’ learning and development [89,90].
Regulating infants through attuned interactions is demanding for mothers and requires heightened availability and resources [91]. Mothers must be attentive and constantly adjust their behavior to notice and address every subtle allostatic cue the infant communicates [86]. Such a demanding process is susceptible to regulatory challenges posed to the mother herself, such as pain, illness, and psychopathology [92,93]. Pain is a regulatory challenge that depletes physiological and psychological resources [94,95]. Moreover, the consistent presence of pain or the expectancy of pain reduces engagement in different activities and increases a sense of helplessness [94,96,97]. Breastfeeding takes hours throughout the day, especially in the first months of life [98]. If painful, breastfeeding can be a source of ongoing pain and pain expectancy. Mothers who experience pain in every feeding struggle while breastfeeding, and continuously dread the next feeding, increasing the allostatic load.
Here, we test whether breastfeeding pain adversely affects mothers’ and infants’ behavior during free interaction. We hypothesize that since pain is an allostatic challenge for mothers, breastfeeding pain will adversely impact the mothers’ behavioral regulation of infants. Specifically, we predict that mothers who suffer from breastfeeding pain will show altered affective expressions during interactions and be less responsive to infant cues. Moreover, since infant affective communication is contingent on maternal affective communication [99,100,101,102,103,104], we further predict that infants of mothers with breastfeeding pain will demonstrate altered affective communication during interactions.
2. Methods
2.1. Participants
A total of 71 mother–infant dyads participated in the study: 50 dyads where the mothers were experiencing varying levels of breastfeeding pain (from no pain to severe pain) and a control group of 21 non-breastfeeding mothers. Mothers with breastfeeding pain were recruited through a lactation consultant, while other mothers were recruited from an early childhood center or through an ad post on Facebook. Mothers’ ages ranged from 22 to 39 years. Infants’ ages ranged from 2 to 35 weeks (breastfeeding pain: = 12.02 weeks, = 8.88; no pain: = 13.40 weeks, = 8.97; not breastfeeding: = 17.96 weeks, = 9.47). In our cohort, the maternal income level ranged from lower than average (10% of mothers) to somewhat lower than average (19% of mothers) to average (17% of mothers) to slightly higher than average (37% of mothers) to higher than average (17% of mothers). The maternal relationship statuses were in a relationship (12% of mothers), married (83% of mothers), or single (5% of mothers). Infants were born via vaginal delivery (82% of mothers), cesarean section (14% of mothers), or vacuum extraction delivery (4% of mothers). The mean number of children in the household was 1.56 children (sd = 0.92), with a mean of 3.11 rooms (sd = 0.71). The mean years of education were 17.18 years (sd = 1.39). The target sample size was assessed with power analysis (G*Power software [105]). Since no research had addressed this question, a moderate effect size was estimated based on previous studies that reported a moderate to high correlation between maternal emotional pain and maternal bonding behavior (r values ranging between 0.31 and 0.873) [106,107,108]. Therefore, given a power of 0.95 and estimated moderate effect size in a linear regression of 0.35 for the correlation between breastfeeding pain and maternal behavior, the target sample size was 50 dyads with breastfeeding mothers. After collecting the data, we excluded one mother from the “breastfeeding without pain” group since she reported having prior breastfeeding pain. Therefore, the results include only 19 breastfeeding mothers with no breastfeeding pain. The Institution Review Board approved the study, and mothers signed an informed consent form before participating. Families were remunerated for their participation.
2.2. Procedures
Mothers experiencing breastfeeding pain were recruited through lactation consultants, who asked mothers experiencing pain to participate in the research. Mothers without pain or mothers not breastfeeding were recruited through social media. Participation included questionnaires and a video recording of a two-minute free interaction with the infant. Videos were captured in the families’ homes or their local community center. Trained research personnel filmed the interaction based on our previous research [83,85,109,110]. Mothers were instructed to freely interact with their infants as usual, without any restrictions, specific toys, or guidelines; the videos did not include breastfeeding. This setting represents natural mother–infant interactions [111,112], allowing each mother to determine her setup, interaction choices, and tendencies without constraints. The free mother–infant interactions were then imported to the lab and behaviorally coded and analyzed by trained personnel using the Affect Regulation Coding Scheme (ARCS) [113].
2.3. Behavior
2.3.1. ARCS—Affect Regulation Coding Scheme
Using the ARCS, trained coders coded the mothers’ and infants’ second-by-second affective expressions during the interactions.
The ARCS is a coding scheme that enables us to trace the valence, expression intensity, and gaze separately for mothers and infants for each second of the interaction. Valence represents the moment-by-moment valence of facial expression: positive, neutral, or negative. Expression intensity represents the changing effort of the facial expression, ranging from no facial effort to strong effort. Gaze and attention trace the mothers’ and infants’ gaze and attention, ranging from an unfocused gaze to a directed gaze to switching glances (Table 1).
2.3.2. Inter-Rater Reliability
The inter-rater reliability was conducted for each variable separately based on 10–12% of the interactions [85,114,115,116,117]. Krippendorff’s alpha test was used to estimate the inter-rater reliability between coders, given its accuracy in assessing the level of agreement between raters for categorical variables of multiple levels [118]. The inter-rater reliability score for maternal behavior was Krippendorff’s α = 0.835 and for the infant behavior, Krippendorff’s α = 0.855, which is considered moderate to high [118] (see Supplementary Anaysis S1, Table S1 for reliability scores of each variable).
After the initial coding, we used an in-house toolbox using MATLAB R2016a (The MathWorks, Natick, MA, USA) and Python (version 3.7) to compute the mean and dynamic changes in the three variables of valence, expression intensity, and gaze during the interaction. The scores were calculated as such:
- General Valence: averaged 120 s of the interaction ().
- General Expression Intensity: averaged 120 s of the interaction ().
- The average duration in focused gaze: the average time mothers maintained focused gaze. = the number of focused gaze events across the interaction.
For more information on the ARCS and its implementation, email the corresponding author.
2.4. Breastfeeding Pain
2.4.1. Breastfeeding Questionnaire: Mothers Completed a Questionnaire about Their Current Breastfeeding Pain Experience. Scores Started from 0 (No Pain at All) and Gradually Increased to 10 (Extremely Intense and Unbearable Pain)
We divided all breastfeeding mothers into three groups, a priory defined by the questionnaire score:
- No pain: N = 19, questionnaire score of 0. These mothers reported that they had not experienced any breastfeeding pain since the second postnatal week.
- Moderate pain: N = 16, questionnaire score of 1–4.
- Severe pain: N = 14, questionnaire score of 5–10.
- Additionally, we recruited 21 mothers who were not breastfeeding as a control group.
2.4.2. Computing the Association between Breastfeeding Pain and Maternal Behaviors
We tested the correlation between the degree of breastfeeding pain and three maternal behaviors:
- Duration of directed gaze;
- Expressed valence;
- Affective expression intensity.
We applied two analyses:
- (1)
- A Pearson correlation between the degree of breastfeeding pain and the three maternal behavior variables while controlling for infants’ age. Given the three dependent variables, Bonferroni correction for multiple hypotheses was applied.
- (2)
- A one-way ACNOVA to test the group differences in the three maternal behaviors across the four groups (no pain = 19, moderate pain = 16, severe pain = 14, not breastfeeding = 21) while controlling for infants’ age. We further calculated group differences using post hoc LSD.
2.4.3. Maternal Behavior during Infant Engagement and Distress across Pain Groups
The ARCS provides second-by-second measures of dyadic affect, which enables us to assess in a dynamic way how maternal behavior unfolds during specific events of infant affective regulation. Maternal behavior was evaluated during two types of infant regulatory events: engagement in play and distress.
Infant Engagement: Events of infant engagement were defined as infants transitioning from neutral to positive valence. We determined all events where infants transitioned from neutral to positive valence across all the free interaction videos and aligned them in time (153 events).
Infant Distress: Events of infant distress were defined as infants transitioning from neutral to negative valence. We located all events where infants transitioned from neutral to negative valence across all the free interaction videos and aligned them in time (123 events).
Maternal valence, intensity, and gaze were averaged across all participants for a given second during events of engagement and distress (separately) and compared between pain groups with repeated-measure ANCOVA. A repeated-measure general linear model (ANCOVA) was conducted to test the temporal changes in maternal valence and expression intensity across the four breastfeeding groups while controlling for infant age differences (five groups X seven time points). We further calculated specific differences using the post hoc LSD.
2.4.4. Computing the Association between Breastfeeding Pain and Infant Behaviors
We tested the correlation between the degree of breastfeeding pain and three infant behaviors:
- Duration of directed gaze;
- Expressed valence;
- Affective expression intensity.
We applied two types of analyses:
- (1)
- A Pearson correlation between the degree of breastfeeding pain and the three maternal behavior variables while controlling for infants’ age.
- (2)
- A one-way ANCOVA to test the group differences in the three maternal behaviors across the four breastfeeding groups (no pain = 19, moderate pain = 16, severe pain = 14, not breastfeeding = 21) while controlling for infants’ age. We further calculated group differences using the post hoc LSD.
3. Results
3.1. The Association between Maternal Breastfeeding Pain and Maternal Behaviors
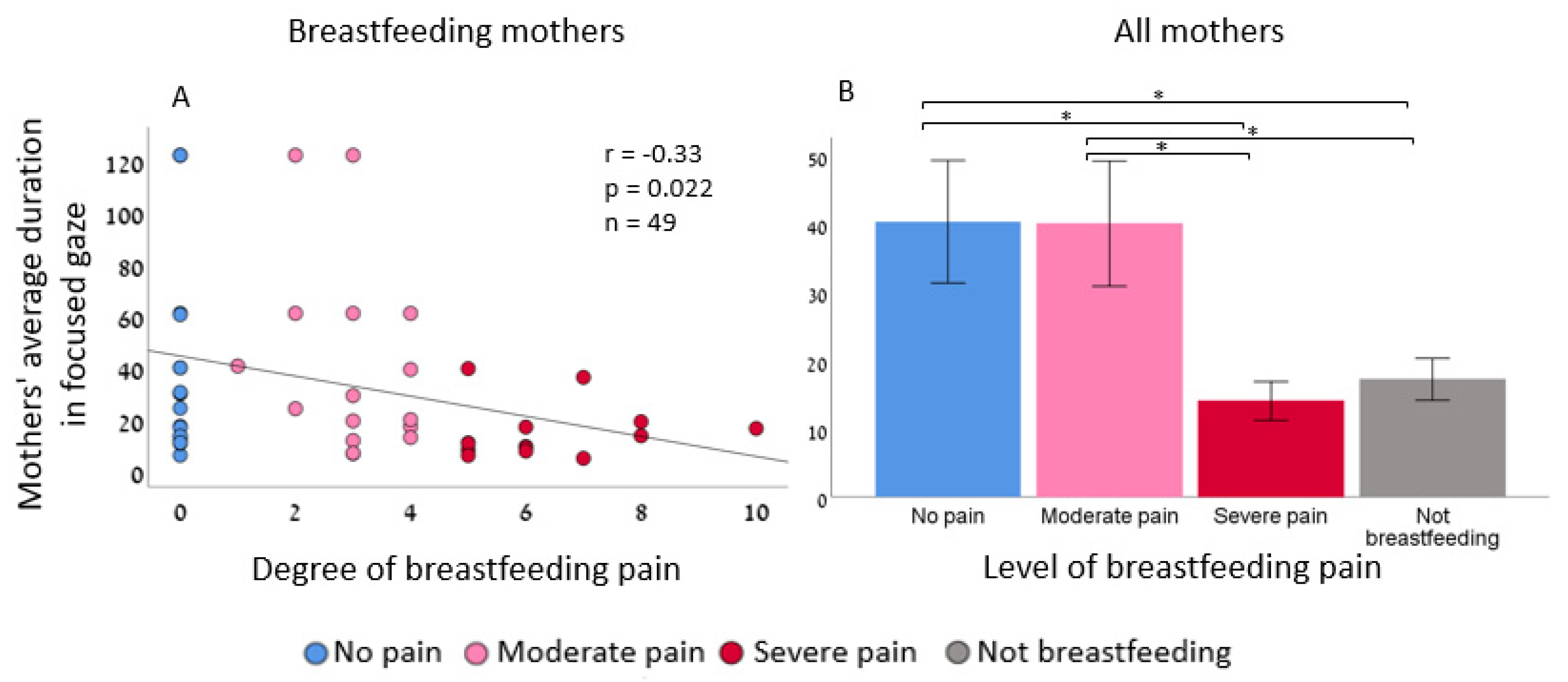
Mothers with severe pain maintained a less focused gaze compared to mothers with no pain or with moderate pain (Pearson r = −0.33, p = 0.022 two-tailed, n = 49, 95% CI [−0.49, −0.15]) (Figure 1A), one-way ANCOVA, F (3,65) = 3.91, p = 0.013, η2 = 0.15 (Figure 1B)). There was no significant association between the degree of breastfeeding pain and affect intensity (Pearson r = −0.14, p 0.337 two-tailed, n = 49, CI [−0.39, 0.16]) or with valence (Pearson r = −0.025, p = 0.868 two-tailed, n = 49, 95% CI [−0.25, 0.29]) (Supplementary Figure S1). Given the three dependent variables, Bonferroni correction for multiple hypotheses testing yielded a p-value of 0.016, and the effect remained marginally significant (p = 0.02). However, when including only mothers who experienced pain in the analysis, the correlation was higher (Pearson r = −0.47, p = 0.011 two-tailed, n = 30, 95% CI [−0.65, −0.25]).
3.2. The Effect of Breastfeeding Pain on Maternal Affective Reactivity during Infant Engagement and Distress
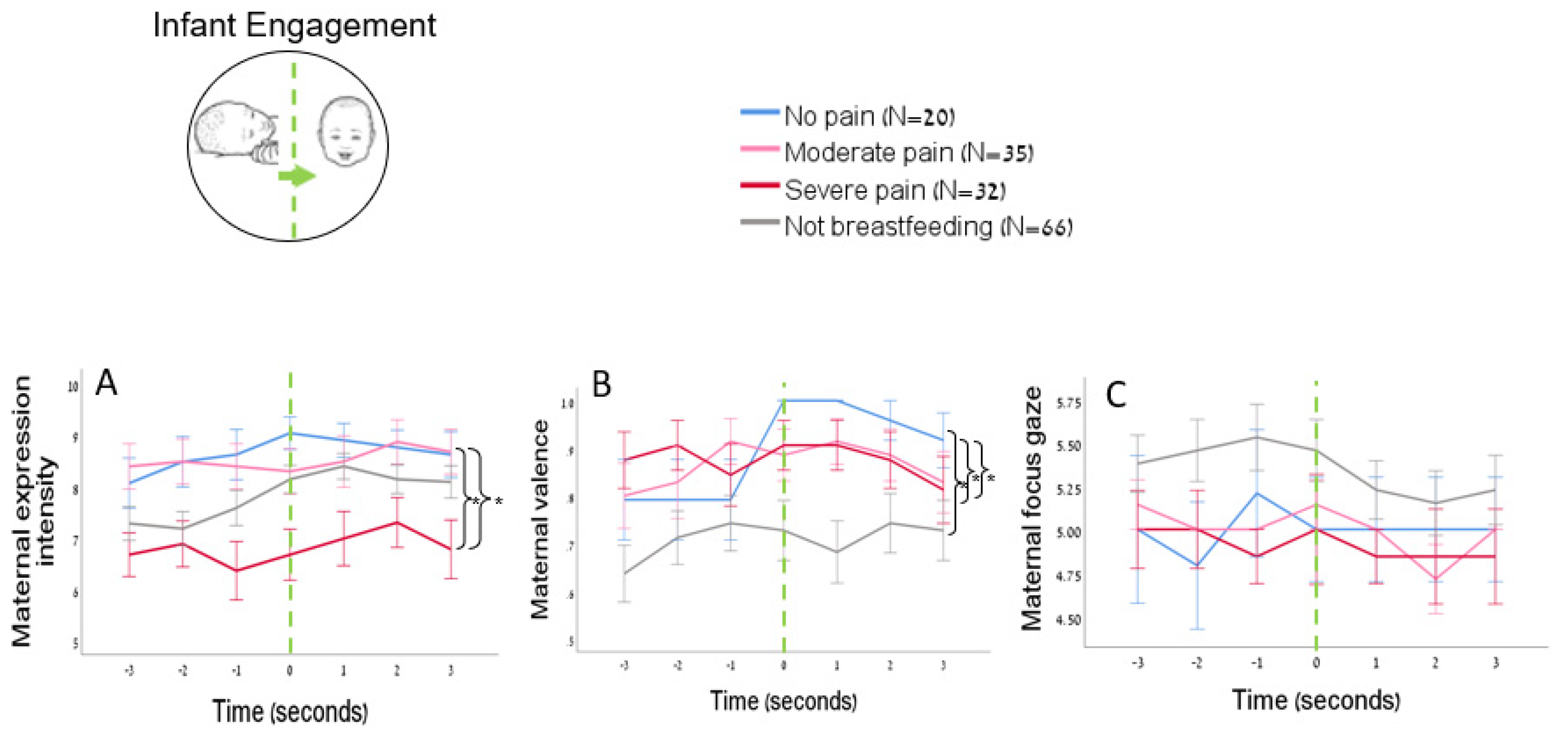
Maternal affective expression during infant engagement: There was a significant group effect of pain on maternal affective expressions during events of infant engagement, where infants transition from neutral to positive valence (Mix ANCOVA, F(3,148) = 4.98, p = 0.003, η2 = 0.092). Post hoc LSD analyses showed that mothers who experienced severe breastfeeding pain displayed less intense facial expressions while interacting with their infant in positive engagements events compared to mothers with no breastfeeding pain (Cohen’s d = −0.91, p = 0.007, 95% CI [−3.43, −0.39]) and mothers with moderate breastfeeding pain (Cohen’s d = −0.80, p = 0.005, 95% CI [−3.01, −0.40]) (Figure 2A).
Maternal valence during infant engagement: There was a significant group effect on maternal valence (Mix ANCOVA, F(3,148) = 5.85, p = 0.001, η2 = 0.11). Post hoc LSD analyses showed that mothers who did not breastfeed demonstrated less positive valence compared to mothers with no breastfeeding pain (Cohen’s d = −0.77, p = 0.003, 95% CI [−0.35, −0.07]), mothers with moderate pain (Cohen’s d = −0.63, p = 0.003, 95% CI [−0.29, −0.06]), and mothers with severe pain (Cohen’s d = 0.70, p = 0.001, 95% CI [−0.32, −0.08]) (Figure 2B).
Maternal gaze during infant engagement: There was no significant group effect of pain on maternal gaze during events of infant engagement (Mix ANCOVA, F(3,148) = 2.57, p = 0.0561).
There was no significant group effect of pain on maternal behavior during events of infant distress in any of the dependent variables: expression intensity: Mix ANCOVA, F(3, 118) = 0.75, p = 0.525; valence: Mix ANCOVA, F (3,118) = 0.25, p = 858; gaze: Mix ANCOVA, F (3,118) = 267, p = 0.51 (Figure 2C).
3.3. The Association between Maternal Breastfeeding Pain and Infant Behaviors
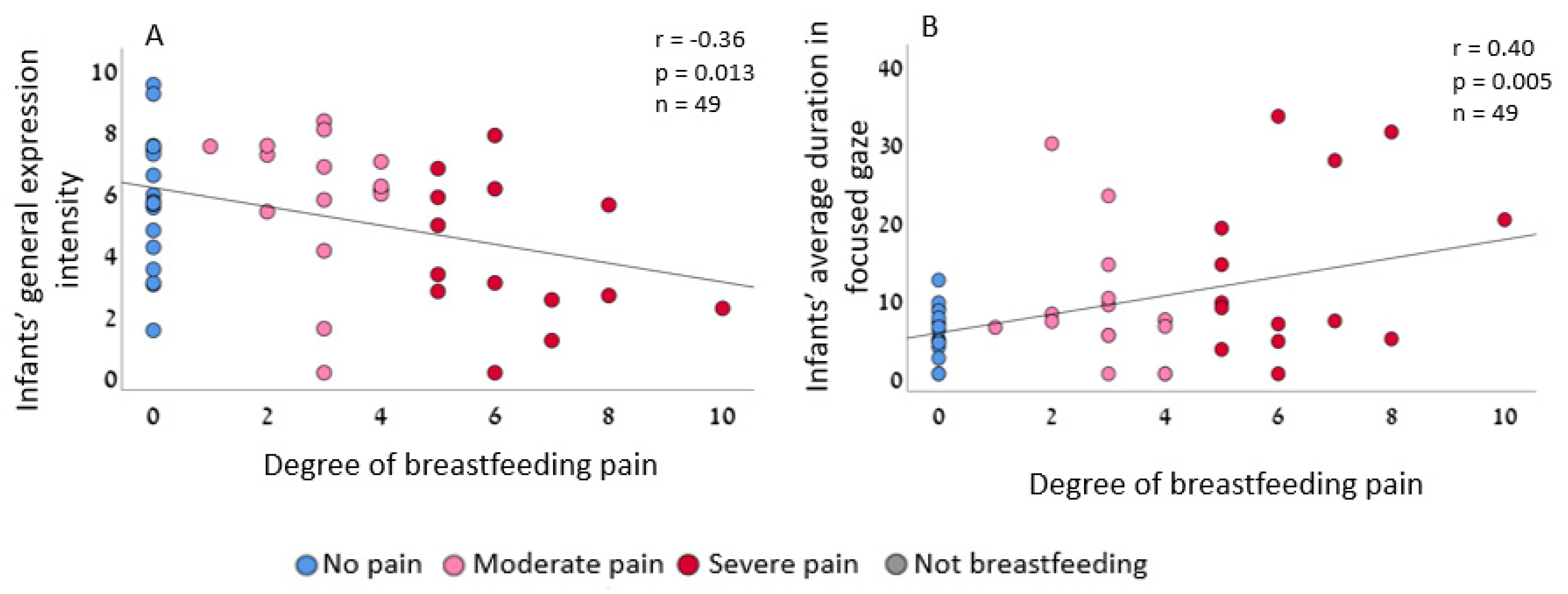
Next, we tested the effect of maternal breastfeeding pain on infants’ affective expression and gaze. Interestingly, infants of mothers with severe pain expressed weaker affective expressions during mother–infant interaction (Figure 3A) and maintained longer focused gaze during mother–infant interaction (Figure 3B). There was no significant association between maternal pain and infants’ expressed valence (Pearson r = 0.25, p = 0.089; two-tailed, n = 49, 95% CI [−0.035, 0.459]). Given the three dependent variables Bonferroni correction for multiple hypothesis testing is applied, p = 0.016, and the effect remained significant.
4. Discussion
The current research demonstrates that severe breastfeeding pain is associated with altered behavior of both mothers and infants during an interaction. Mothers with severe breastfeeding pain maintain a less focused gaze and communicate weaker positive affective expressions during infants’ engagement and play than mothers with no pain or moderate pain. Breastfeeding pain is also associated with infants’ behavior, as infants express weaker facial expressions and maintain a longer focused gaze compared to infants of mothers with no pain or moderate pain. This suggests that an allostatic challenge to mothers, such as pain, can interfere with the behavioral mechanism of affective communication in early childhood and is thus a potential risk factor for child development and mother–infant well-being.
Pain can lead to disengagement in social interactions [96,97]. Here, we found that in mothers, this was evident only during playful moments. There is a differential effect of pain on maternal response to the infant’s distress and play: mothers suffering from breastfeeding pain were less responsive during infant engagement and play. They expressed positive valence with significantly less intensity. However, breastfeeding pain did not affect maternal response during the infant’s distress. Infants communicate distress to signal allostatic challenges [85]. This highlights that infants’ allostatic signals priorly guide maternal behavior, and only when infants do not communicate distress do maternal allostatic challenges play a role in driving behavior. This also signifies the methodological need to separately inspect positive and negative moments of interactions, which is a central feature of the ARCS method.
Mothers with severe pain had difficulty maintaining a focused gaze during face-to-face interactions. This suggests that severe breastfeeding pain interferes with the mother’s ability to fully engage with her infant while interacting. Maternal gaze is a fundamental component of maternal-sensitive responding during a face-to-face interaction [90], which enables mothers to signal availability, establish mutual engagement, and regulate infant arousal [89,90]. Thus, this behavioral alternation can have downstream effects on infants’ behavior.
Accordingly, maternal pain affects both maternal behavior and infant behavior: infants of mothers with pain demonstrated less affective expressions during interactions. Infants are highly sensitive to adult faces, notably the caregiver gaze [119]. During face-to-face interactions, mothers typically attune to and complement the infant’s expressions with exaggerated mimicry, which in turn enhances the infant’s social communication [101]. In contrast, when parents look away during a face-to-face interaction, infants’ affective cues decline [120]. This suggests that the effect of maternal breastfeeding pain on reduced infant affective expressions could result from an altered maternal responsivity during an engagement. Future research is needed to test this on a larger sample.
While mothers in pain maintain a less focused gaze, infants of mothers with severe breastfeeding pain hold a longer focused gaze compared to infants of mothers with no or moderate pain. Gaze behavior is one of the earliest regulatory channels infants develop- through their gaze, infants control the amount and type of stimulation they perceive [91,121]. In cases of “reduced maternal feedback, such as the “still face” paradigm [122] or cases of maternal depression [123], infants often respond with an increased gaze, seeking social engagement [124]. Like depression and the “still face” experience, breastfeeding pain is associated with reduced maternal responsivity and gaze. This may elicit the infant’s increased gaze as an approach-seeking compensation mechanism to gain more information and engage the unengaged mother during interactions.
The current research has some limitations. Studying human mothers and infants does not allow for an experimental inducement of pain or other allostatic challenges or to test their causal effect on maternal and infant behavior. Future research in larger samples of both human and non-human animals that directly test the impact of allostatic interference on mothers and infants is needed to establish the role of mutual allostasis regulation in the mother–infant dyad. Moreover, this research did not include longitudinal developmental assessments of breastfeeding under severe pain on the long-term mother–infant bond and infant development.
Breastfeeding has many benefits, including promoting close mother–infant contact and social-emotional development [19,125]. Moreover, breastfeeding can enhance maternal behaviors, such as gazing at the infant and more affectionate responses [126]. Since breastfeeding is seen as essential in creating an intimate and close relationship between the mother and her infant [127], women likely feel pressured to breastfeed even under severe pain. However, here we demonstrate that breastfeeding under pain may pose adverse outcomes to both mothers and infants. Given the allostatic codependence between mothers and infants, optimal care, well-being, and child development depend on the allostasis of both mothers and infants.
5. Conclusions
This research demonstrates the potential negative impact of severe breastfeeding pain on the mother–infant dyad. The findings suggest that maternal pain can lead to disengagement during playful interactions, resulting in altered affective communication and reduced maternal gaze, which in turn can affect infant behavior. Optimal care, well-being, and child development depend on the allostasis of both mothers and infants; breastfeeding under severe pain may pose adverse outcomes. These findings highlight the importance of addressing maternal pain during breastfeeding to promote care and development. Future research is needed to explore the long-term impact of maternal pain and additional allostatic challenges on the mother–infant bond and infant development.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/biology12050636/s1. Table S1. The average inter-rater reliability between coders, using Krippendorff’s alpha test. Analysis S1. Confirming the consistency of each measurement across the interaction. Figure S1. The association between maternal breastfeeding pain and maternal expression intensity and valence. (A) Partial Pearson correlation between the degree of breastfeeding pain and maternal expression intensity while controlling for infants’ age. (B) Maternal expression intensity in the four pain groups, one-way ANCOVA, F (3,65) = 0.291 p = 0.832. (C) Partial Pearson’s correlation between the degree of breastfeeding pain and maternal valence while controlling for infants’ age. (D) Maternal valence in the four pain groups, one-way ANCOVA, F (3,65) = 0.844 p = 0.475.
Author Contributions
M.A.—writing, methodology, analysis, graph preparation. M.I.—conceptualization, writing, data collection, analysis, graph preparation. N.k.S.—data analysis. S.A.—conceptualization, writing, analysis, graph preparation, supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by internal funding.
Institutional Review Board Statement
The Institution Review Board of the Hebrew University approved the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
ARCS method and implementation can become freely available for research use by emailing the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- León-Cava, N.; Lutter, C.; Ross, J.; Martin, L. Quantifying the Benefits of Breastfeeding: A Summary of the Evidence; Pan American Health Organization: Washington, DC, USA, 2002. [Google Scholar]
- Koletzko, B.; Demmelmair, H.; Grote, V.; Totzauer, M. Optimized protein intakes in term infants support physiological growth and promote long-term health. Semin. Perinatol. 2019, 43, 151153. [Google Scholar] [CrossRef] [PubMed]
- Horta, B.L.; de Lima, N.P. Breastfeeding and Type 2 Diabetes: Systematic Review and Meta-Analysis. Curr. Diab. Rep. 2019, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Lochhead, P.; Ko, Y.; Claggett, B.; Leong, R.W.; Ananthakrishnan, A.N. Systematic review with meta-analysis: Breastfeeding and the risk of Crohn’s disease and ulcerative colitis. Aliment. Pharmacol. Ther. 2017, 46, 780–789. [Google Scholar] [CrossRef] [PubMed]
- Jackson, K.M.; Nazar, A.M. Breastfeeding, the Immune Response, and Long-term Health. J. Osteopath. Med. 2006, 106, 203–207. [Google Scholar]
- Lodge, C.J.; Tan, D.J.; Lau, M.X.Z.; Dai, X.; Tham, R.; Lowe, A.J.; Bowatte, G.; Allen, K.J.; Dharmage, S.C. Breastfeeding and asthma and allergies: A systematic review and meta-analysis. Acta Paediatr. 2015, 104, 38–53. [Google Scholar] [CrossRef]
- Jing, H.; Gilchrist, J.M.; Badger, T.M.; Pivik, R.T. A longitudinal study of differences in electroencephalographic activity among breastfed, milk formula-fed, and soy formula-fed infants during the first year of life. Early Hum. Dev. 2010, 86, 119–125. [Google Scholar] [CrossRef]
- Deoni, S.; Dean, D.; Joelson, S.; O’Regan, J.; Schneider, N. Early nutrition influences developmental myelination and cognition in infants and young children. NeuroImage 2018, 178, 649–659. [Google Scholar] [CrossRef]
- Deoni, S.C.; Dean III, D.C.; Piryatinsky, I.; O’Muircheartaigh, J.; Waskiewicz, N.; Lehman, K.; Han, M.; Dirks, H. Breastfeeding and early white matter development: A cross-sectional study. NeuroImage 2013, 82, 77–86. [Google Scholar] [CrossRef]
- Kramer, M.S.; Aboud, F.; Mironova, E.; Vanilovich, I.; Platt, R.W.; Matush, L.; Igumnov, S.; Fombonne, E.; Bogdanovich, N.; Ducruet, T.; et al. Breastfeeding and Child Cognitive Development: New Evidence From a Large Randomized Trial. Arch. Gen. Psychiatry 2008, 65, 578–584. [Google Scholar] [CrossRef]
- Mortensen, E.L.; Michaelsen, K.F.; Sanders, S.A.; Reinisch, J.M. The Association Between Duration of Breastfeeding and Adult Intelligence. JAMA 2002, 287, 2365–2371. [Google Scholar] [CrossRef]
- Leventakou, V.; Roumeliotaki, T.; Koutra, K.; Vassilaki, M.; Mantzouranis, E.; Bitsios, P.; Kogevinas, M.; Chatzi, L. Breastfeeding duration and cognitive, language and motor development at 18 months of age: Rhea mother–child cohort in Crete, Greece. J. Epidemiol. Community Health. 2015, 69, 232–239. [Google Scholar] [CrossRef]
- Mahurin Smith, J. Breastfeeding and language outcomes: A review of the literature. J. Commun. Disord. 2015, 57, 29–40. [Google Scholar] [CrossRef]
- González-Jiménez, E.; García, P.A.; Aguilar, M.J.; Padilla, C.A.; Álvarez, J. Breastfeeding and the prevention of breast cancer: A retrospective review of clinical histories. J. Clin. Nurs. 2014, 23, 2397–2403. [Google Scholar] [CrossRef]
- Section on Breastfeeding. Breastfeeding and the use of human milk. Pediatrics 2005, 115, 496–506. [Google Scholar] [CrossRef]
- Alimi, R.; Azmoude, E.; Moradi, M.; Zamani, M. The Association of Breastfeeding with a Reduced Risk of Postpartum Depression: A Systematic Review and Meta-Analysis. Breastfeed. Med. 2022, 17, 290–296. [Google Scholar] [CrossRef]
- Doan, T.; Gardiner, A.; Gay, C.L.; Lee, K.A. Breast-feeding Increases Sleep Duration of New Parents. J. Perinat. Neonatal Nurs. 2007, 21, 200–206. [Google Scholar] [CrossRef]
- Krol, K.M.; Grossmann, T. Psychological effects of breastfeeding on children and mothers. Bundesgesundheitsblatt Gesundh. Gesundh. 2018, 61, 977–985. [Google Scholar] [CrossRef]
- Kim, P.; Feldman, R.; Mayes, L.C.; Eicher, V.; Thompson, N.; Leckman, J.F.; Swain, J.E. Breastfeeding, brain activation to own infant cry, and maternal sensitivity. J. Child. Psychol. Psychiatry 2011, 52, 907–915. [Google Scholar] [CrossRef]
- Linde, K.; Lehnig, F.; Nagl, M.; Kersting, A. The association between breastfeeding and attachment: A systematic review. Midwifery 2020, 81, 102592. [Google Scholar] [CrossRef]
- Peñacoba, C.; Catala, P. Associations Between Breastfeeding and Mother–Infant Relationships: A Systematic Review. Breastfeed. Med. 2019, 14, 616–629. [Google Scholar] [CrossRef]
- Bibbins-Domingo, K.; Grossman, D.C.; Curry, S.J.; Davidson, K.W.; Epling, J.W.; García, F.A.; Kemper, A.R.; Krist, A.H.; Kurth, A.E.; Landefeld, C.S.; et al. Primary Care Interventions to Support Breastfeeding: US Preventive Services Task Force Recommendation Statement. JAMA 2016, 316, 1688. [Google Scholar] [CrossRef] [PubMed]
- Dieterich, C.M.; Felice, J.P.; O’Sullivan, E.; Rasmussen, K.M. Breastfeeding and Health Outcomes for the Mother-Infant Dyad. Pediatr. Clin. N. Am. 2013, 60, 31–48. [Google Scholar] [CrossRef] [PubMed]
- Kramer, M.S.; Kakuma, R. The optimal duration of exclusive breastfeeding. Trop. Doct. 2012, 321. [Google Scholar] [CrossRef] [PubMed]
- Westerfield, K.L.; Koenig, K.; Oh, R.C. Breastfeeding: Common Questions and Answers. Am. Fam. Physician 2018, 98, 368–373. [Google Scholar] [PubMed]
- World Health Organization. Report of the Expert Consultation of the Optimal Duration of Exclusive Breastfeeding; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Palmér, L.; Carlsson, G.; Mollberg, M.; Nyström, M. Severe breastfeeding difficulties: Existential lostness as a mother—Women’s lived experiences of initiating breastfeeding under severe difficulties. Int. J. Qual. Stud. Health Well-Being 2012, 7, 10846. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Results: Breastfeeding Rates|Breastfeeding|CDC 2021. Available online: https://www.cdc.gov/breastfeeding/data/nis_data/results.html (accessed on 8 November 2021).
- De Jager, E.; Broadbent, J.; Fuller-Tyszkiewicz, M.; Nagle, C.; McPhie, S.; Skouteris, H. A longitudinal study of the effect of psychosocial factors on exclusive breastfeeding duration. Midwifery 2015, 31, 103–111. [Google Scholar] [CrossRef]
- Watkins, S.; Meltzer-Brody, S.; Zolnoun, D.; Stuebe, A. Early Breastfeeding Experiences and Postpartum Depression. Obstet. Gynecol. 2011, 118, 214–221. [Google Scholar] [CrossRef]
- McClellan, H.L.; Hepworth, A.R.; Garbin, C.P.; Rowan, M.K.; Deacon, J.; Hartmann, P.E.; Geddes, D.T. Nipple Pain during Breastfeeding with or without Visible Trauma. J. Hum. Lact. 2012, 28, 511–521. [Google Scholar] [CrossRef]
- Hauck, Y.L.; Fenwick, J.; Dhaliwal, S.S.; Butt, J. A Western Australian Survey of Breastfeeding Initiation, Prevalence and Early Cessation Patterns. Matern. Child Health J. 2011, 15, 260–268. [Google Scholar] [CrossRef]
- Henderson, A.; Stamp, G.; Pincombe, J. Postpartum Positioning and Attachment Education for Increasing Breastfeeding: A Randomized Trial. Birth 2001, 28, 236–242. [Google Scholar] [CrossRef]
- Strong, G.D. Provider Management and Support for Breastfeeding Pain. J. Obstet. Gynecol. Neonatal Nurs. 2011, 40, 753–764. [Google Scholar] [CrossRef]
- Jackson, J.C.; Watts, J.; Henry, T.R.; List, J.M.; Forkel, R.; Mucha, P.J.; Greenhill, S.J.; Gray, R.D.; Lindquist, K.A. Emotion semantics show both cultural variation and universal structure. Science 2019, 366, 1517–1522. [Google Scholar] [CrossRef]
- Ballard, J.L.; Auer, C.E.; Khoury, J.C. Ankyloglossia: Assessment, Incidence, and Effect of Frenuloplasty on the Breastfeeding Dyad. Pediatrics 2002, 110, e63. [Google Scholar] [CrossRef]
- Webb, A.N.; Hao, W.; Hong, P. The effect of tongue-tie division on breastfeeding and speech articulation: A systematic review. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 635–646. [Google Scholar] [CrossRef]
- Ghaheri, B.A.; Cole, M.; Fausel, S.C.; Chuop, M.; Mace, J.C. Breastfeeding improvement following tongue-tie and lip-tie release: A prospective cohort study. Laryngoscope 2017, 127, 1217–1223. [Google Scholar] [CrossRef]
- Hill, R.R.; Lyons, K.S.; Kelly-Weeder, S.; Pados, B.F. Effect of Frenotomy on Maternal Breastfeeding Symptoms and the Relationship Between Maternal Symptoms and Problematic Infant Feeding. Glob. Pediatr. Health 2022, 9, 2333794X2110728. [Google Scholar] [CrossRef]
- Hill, R.R.; Richard, M.A.; Pados, B.F. Breastfeeding Symptoms with Tongue- and Lip-Tie. MCN Am. J. Matern. Nurs. 2023, 48, 17–23. [Google Scholar] [CrossRef]
- Jackson, K.T.; Dennis, C.-L. Lanolin for the treatment of nipple pain in breastfeeding women: A randomized controlled trial: An RCT evaluating lanolin for nipple pain. Matern. Child Nutr. 2017, 13, e12357. [Google Scholar] [CrossRef]
- Niazi, A.; Baradaran Rahimi, V.; Askari, N.; Rahmanian-Devin, P.; Askari, V.R. Topical treatment for the prevention and relief of nipple fissure and pain in breastfeeding women: A systematic review. Adv. Integr. Med. 2021, 8, 312–321. [Google Scholar] [CrossRef]
- Srinivasan, A.; Dobrich, C.; Mitnick, H.; Feldman, P. Ankyloglossia in Breastfeeding Infants: The Effect of Frenotomy on Maternal Nipple Pain and Latch. Breastfeed. Med. 2006, 1, 216–224. [Google Scholar] [CrossRef]
- Dalal, P.G. The Need to Treat Maternal Pain in the Breastfeeding Mother: Are Opioids Safe? Pain Med. 2015, 16, 630–631. [Google Scholar] [CrossRef] [PubMed]
- Ghaheri, B.A.; Cole, M.; Mace, J.C. Revision Lingual Frenotomy Improves Patient-Reported Breastfeeding Outcomes: A Prospective Cohort Study. J. Hum. Lact. 2018, 34, 566–574. [Google Scholar] [CrossRef] [PubMed]
- O’Callahan, C.; Macary, S.; Clemente, S. The effects of office-based frenotomy for anterior and posterior ankyloglossia on breastfeeding. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 827–832. [Google Scholar] [CrossRef] [PubMed]
- Hadjistavropoulos, T.; Craig, K.D.; Duck, S.; Cano, A.; Goubert, L.; Jackson, P.L.; Mogil, J.S.; Rainville, P.; Sullivan, M.J.; Williams, A.C.D.C.; et al. A biopsychosocial formulation of pain communication. Psychol. Bull. 2011, 137, 910–939. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.J.; Tuttle, A.H.; Mogil, J.S. The Interaction Between Pain and Social Behavior in Humans and Rodents. In Behavioral Neurobiology of Chronic Pain; Taylor, B.K., Finn, D.P., Eds.; Springer: Berlin/Heidelberg, Germany, 2014; pp. 233–250. [Google Scholar]
- Nicolardi, V.; Panasiti, M.S.; D’Ippolito, M.; Pecimo, G.L.; Aglioti, S.M. Pain perception during social interactions is modulated by self-related and moral contextual cues. Sci. Rep. 2020, 10, 41. [Google Scholar] [CrossRef]
- Reicherts, P.; Gerdes, A.B.M.; Pauli, P.; Wieser, M.J. On the mutual effects of pain and emotion: Facial pain expressions enhance pain perception and vice versa are perceived as more arousing when feeling pain. PAIN® 2013, 154, 793–800. [Google Scholar] [CrossRef]
- Rivera, N.V.; Parmelee, P.A.; Smith, D.M. The impact of social interactions and pain on daily positive and negative affect in adults with osteoarthritis of the knee. Aging Ment. Health 2020, 24, 8–14. [Google Scholar] [CrossRef]
- Schenk, L.; Krimmel, S.R.; Colloca, L. Observe to get pain relief: Current evidence and potential mechanisms of socially-learned pain modulation. PAIN 2017, 158, 2077–2081. [Google Scholar] [CrossRef]
- Eisenberger, N.I. The neural bases of social pain: Evidence for shared representations with physical pain. Psychosom. Med. 2012, 74, 126–135. [Google Scholar] [CrossRef]
- Krahé, C.; Springer, A.; Weinman, J.; Fotopoulou, A. The Social Modulation of Pain: Others as Predictive Signals of Salience—A Systematic Review. Front. Hum. Neurosci. 2013, 7, 386. [Google Scholar] [CrossRef]
- Zhang, M.; Zhang, Y.; Kong, Y. Interaction between social pain and physical pain. Brain Sci. Adv. 2019, 5, 265–273. [Google Scholar] [CrossRef]
- Mogil, J.S. Social modulation of and by pain in humans and rodents. PAIN 2015, 156, S35. [Google Scholar] [CrossRef]
- Sibille, K.T.; McBeth, J.; Smith, D.; Wilkie, R. Allostatic load and pain severity in older adults: Results from the English Longitudinal Study of Ageing. Exp. Gerontol. 2017, 88, 51–58. [Google Scholar] [CrossRef]
- Slade, G.D.; Sanders, A.E.; By, K. Role of Allostatic Load in Sociodemographic Patterns of Pain Prevalence in the, U.S. Population. J. Pain 2012, 13, 666–675. [Google Scholar] [CrossRef]
- Chapman, C.R.; Gavrin, J. Suffering: The contributions of persistent pain. Lancet 1999, 353, 2233–2237. [Google Scholar] [CrossRef]
- Heinrichs, M.; Gaab, J. Neuroendocrine mechanisms of stress and social interaction: Implications for mental disorders. Curr. Opin. Psychiatry 2007, 20, 158. [Google Scholar] [CrossRef]
- Neff, A.J.; Lee, Y.; Metts, C.L.; Wong, A.W.K. Ecological Momentary Assessment of Social Interactions: Associations With Depression, Anxiety, Pain, and Fatigue in Individuals With Mild Stroke. Arch. Phys. Med. Rehabil. 2021, 102, 395–405. [Google Scholar] [CrossRef]
- Ziegler, T.E.; Crockford, C. Neuroendocrine control in social relationships in non-human primates: Field based evidence. Horm. Behav. 2017, 91, 107–121. [Google Scholar] [CrossRef]
- Koechlin, H.; Coakley, R.; Schechter, N.; Werner, C.; Kossowsky, J. The role of emotion regulation in chronic pain: A systematic literature review. J. Psychosom. Res. 2018, 107, 38–45. [Google Scholar] [CrossRef]
- Lumley, M.A.; Cohen, J.L.; Borszcz, G.S.; Cano, A.; Radcliffe, A.M.; Porter, L.S.; Schubiner, H.; Keefe, F.J. Pain and emotion: A biopsychosocial review of recent research. J. Clin. Psychol. 2011, 67, 942–968. [Google Scholar] [CrossRef]
- Atzil, S.; Gao, W.; Fradkin, I.; Barrett, L.F. Growing a social brain. Nat. Hum. Behav. 2018, 2, 624–636. [Google Scholar] [CrossRef] [PubMed]
- Atzil, S.; Barrett, L.F. Social regulation of allostasis: Commentary on “Mentalizing homeostasis: The social origins of interoceptive inference” by Fotopoulou and Tsakiris. Neuropsychoanalysis 2017, 19, 29–33. [Google Scholar] [CrossRef]
- Feldman, R.; Eidelman, A.I.; Sirota, L.; Weller, A. Comparison of Skin-to-Skin (Kangaroo) and Traditional Care: Parenting Outcomes and Preterm Infant Development. Pediatrics 2002, 110, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Feldman, R.; Magori-Cohen, R.; Galili, G.; Singer, M.; Louzoun, Y. Mother and infant coordinate heart rhythms through episodes of interaction synchrony. Infant. Behav. Dev. 2011, 34, 569–577. [Google Scholar] [CrossRef]
- Hofer, M.A. Hidden Regulators in Attachment, Separation, and Loss. Monogr. Soc. Res. Child Dev. 1994, 59, 192–207. [Google Scholar] [CrossRef]
- Shenfield, T.; Trehub, S.E.; Nakata, T. Maternal Singing Modulates Infant Arousal. Psychol. Music 2003, 31, 365–375. [Google Scholar] [CrossRef]
- McEWEN, B.S. Stress, Adaptation, and Disease: Allostasis and Allostatic Load. Ann. N. Y Acad. Sci. 1998, 840, 33–44. [Google Scholar] [CrossRef]
- Schulkin, J. Allostasis, Homeostasis, and the Costs of Physiological Adaptation; Cambridge University Press: Cambridge, UK, 2004. [Google Scholar]
- Sterling, P. Allostasis: A model of predictive regulation. Physiol. Behav. 2012, 106, 5–15. [Google Scholar] [CrossRef]
- Sterling, P.; Eyer, J. Allostasis: A new paradigm to explain arousal pathology. In Handbook of Life Stress, Cognition and Health; John Wiley & Sons: Oxford, UK, 1988; pp. 629–649. [Google Scholar]
- Atzil, S.; Gendron, M. Bio-behavioral synchrony promotes the development of conceptualized emotions. Curr. Opin. Psychol. 2017, 17, 162–169. [Google Scholar] [CrossRef]
- Agostini, A.; Rizzello, F.; Ravegnani, G.; Gionchetti, P.; Tambasco, R.; Straforini, G.; Ercolani, M.; Campieri, M. Adult Attachment and Early Parental Experiences in Patients With Crohn’s Disease. Psychosomatics 2010, 51, 208–215. [Google Scholar] [CrossRef]
- Entringer, S.; Buss, C.; Wadhwa, P.D. Prenatal stress and developmental programming of human health and disease risk: Concepts and integration of empirical findings. Curr. Opin. Endocrinol. Diabetes Obes. 2010, 17, 507–516. [Google Scholar] [CrossRef]
- Feldman, R. Parent–Infant Synchrony: Biological Foundations and Developmental Outcomes. Curr. Dir. Psychol. Sci. 2007, 16, 340–345. [Google Scholar] [CrossRef]
- Feldman, R. Parent–infant synchrony and the construction of shared timing; physiological precursors, developmental outcomes, and risk conditions. J. Child Psychol. Psychiatry 2007, 48, 329–354. [Google Scholar] [CrossRef]
- Northrup, J.B.; Iverson, J.M. The development of mother–infant coordination across the first year of life. Dev. Psychol. 2020, 56, 221–236. [Google Scholar] [CrossRef] [PubMed]
- Feldman, R.; Eidelman, A.I. Parent-Infant Synchrony and the Social-Emotional Development of Triplets. Dev. Psychol. 2004, 40, 1133–1147. [Google Scholar] [CrossRef]
- Northrup, J.B.; Iverson, J.M. Multimodal coordination of vocal and gaze behavior in mother–infant dyads across the first year of life. Infancy 2020, 25, 952–972. [Google Scholar] [CrossRef]
- Atzil, S.; Touroutoglou, A.; Rudy, T.; Salcedo, S.; Feldman, R.; Hooker, J.M.; Dickerson, B.C.; Catana, C.; Barrett, L.F. Dopamine in the medial amygdala network mediates human bonding. Proc. Natl. Acad. Sci. USA 2017, 114, 2361–2366. [Google Scholar] [CrossRef]
- Lavelli, M.; Fogel, A. Developmental Changes in the Relationship Between the Infant’s Attention and Emotion During Early Face-to-Face Communication: The 2-Month Transition. Dev. Psychol. 2005, 41, 265–280. [Google Scholar] [CrossRef]
- Zeevi, L.; Irani, M.; Catana, C.; Feldman Barrett, L.; Atzil, S. Maternal Dopamine Encodes Affective Signals of Human Infants. Soc. Cogn. Affect. Neurosci. 2021, 17, 503–509. [Google Scholar] [CrossRef]
- Alan, F. Developing through Relationships: Origins of Communication, Self, and Culture. In The Origins of Communication, Self, and Culture; Harvester Wheatsheaf: Hemel Hempstead CITy, UK, 1933. [Google Scholar]
- Hiraoka, D.; Ooishi, Y.; Mugitani, R.; Nomura, M. Differential Effects of Infant Vocalizations on Approach-Avoidance Postural Movements in Mothers. Front. Psychol. 2019, 10, 1378. [Google Scholar] [CrossRef]
- Jonsson, C.O.; Clinton, D.N.; Fahrman, M.; Mazzaglia, G.; Novak, S.; Sörhus, K. How do mothers signal shared feeling-states to their infants? An investigation of affect attunement and imitation during the first year of life. Scand. J. Psychol. 2001, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Slee, P.T. The Nature of Mother-Infant Gaze Patterns during Interaction as a Function of Emotional Expression. J. Am. Acad. Child Psychiatry 1984, 23, 385–391. [Google Scholar] [CrossRef] [PubMed]
- Beebe, B.; Jaffe, J.; Markese, S.; Buck, K.; Chen, H.; Cohen, P.; Bahrick, L.; Andrews, H.; Feldstein, S. The origins of 12-month attachment: A microanalysis of 4-month mother-infant interaction. Attach. Hum. Dev. 2010, 12, 3–141. [Google Scholar] [CrossRef] [PubMed]
- Dennis, C.L.; Ross, L. Relationships Among Infant Sleep Patterns, Maternal Fatigue, and Development of Depressive Symptomatology. Birth 2005, 32, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Shorey, S.; Chee, C.Y.I.; Ng, E.D.; Chan, Y.H.; Tam, W.W.S.; Chong, Y.S. Prevalence and incidence of postpartum depression among healthy mothers: A systematic review and meta-analysis. J. Psychiatr. Res. 2018, 104, 235–248. [Google Scholar] [CrossRef]
- Slomian, J.; Honvo, G.; Emonts, P.; Reginster, J.-Y.; Bruyère, O. Consequences of maternal postpartum depression: A systematic review of maternal and infant outcomes. Womens Health 2019, 15, 1745506519844044. [Google Scholar] [CrossRef]
- Solberg Nes, L.; Roach, A.R.; Segerstrom, S.C. Executive Functions, Self-Regulation, and Chronic Pain: A Review. Ann. Behav. Med. 2009, 37, 173–183. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Bratslavsky, E.; Muraven, M.; Tice, D.M. Ego depletion: Is the active self a limited resource? J. Personal. Soc. Psychol. 1998, 74, 1252–1265. [Google Scholar] [CrossRef]
- Zautra, A.J.; Hamilton, N.A.; Burke, H.M. Comparison of stress responses in women with two types of chronic pain: Fibromyalgia and osteoarthritis. Cogn. Ther. Res. 1999, 23, 209–230. [Google Scholar] [CrossRef]
- Callahan, C.D. Stress, coping, and personality hardiness in patients with temporomandibular disorders. Rehabil. Psychol. 2000, 45, 38–48. [Google Scholar] [CrossRef]
- Hörnell, A.; Aarts, C.; Kylberg, E.; Hofvander, Y.; Gebre-Medhin, M. Breastfeeding patterns in exclusively breastfed infants: A longitudinal prospective study in Uppsala, Sweden. Acta Paediatr. 1999, 88, 203–211. [Google Scholar] [CrossRef]
- Laurent, H.K.; Ablow, J.C. The missing link: Mothers’ neural response to infant cry related to infant attachment behaviors. Infant. Behav. Dev. 2012, 35, 761–772. [Google Scholar] [CrossRef]
- Little, E.E.; Legare, C.H.; Carver, L.J. Mother–Infant Physical Contact Predicts Responsive Feeding among, U.S. Breastfeeding Mothers. Nutrients 2018, 10, 1251. [Google Scholar] [CrossRef]
- Murray, L.; De Pascalis, L.; Bozicevic, L.; Hawkins, L.; Sclafani, V.; Ferrari, P.F. The functional architecture of mother-infant communication, and the development of infant social expressiveness in the first two months. Sci. Rep. 2016, 6, 39019. [Google Scholar] [CrossRef]
- Pechtel, P.; Murray, L.M.M.; Brumariu, L.E.; Lyons-Ruth, K. Reactivity, regulation, and reward responses to infant cues among mothers with and without psychopathology: An fMRI review. Transl. Dev. Psychiatry 2013, 1, 19673. [Google Scholar] [CrossRef]
- White-Traut, R.; Norr, K.F.; Fabiyi, C.; Rankin, K.M.; Li, Z.; Liu, L. Mother–infant interaction improves with a developmental intervention for mother–preterm infant dyads. Infant Behav. Dev. 2013, 36, 694–706. [Google Scholar] [CrossRef]
- Young, K.S.; Parsons, C.E.; Stein, A.; Vuust, P.; Craske, M.G.; Kringelbach, M.L. The neural basis of responsive caregiving behaviour: Investigating temporal dynamics within the parental brain. Behav. Brain Res. 2017, 325, 105–116. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Kumar, R.; Hipwell, A.E. Development of a Clinical Rating Scale to Assess Mother-Infant Interaction in a Psychiatric Mother and Baby Unit. Br. J. Psychiatry 1996, 169, 18–26. [Google Scholar] [CrossRef]
- Taylor, A.; Atkins, R.; Kumar, R.; Adams, D.; Glover, V. A new Mother-to-Infant Bonding Scale: Links with early maternal mood. Arch. Women’s Ment. Health 2005, 8, 45–51. [Google Scholar] [CrossRef]
- Tietz, A.; Zietlow, A.-L.; Reck, C. Maternal bonding in mothers with postpartum anxiety disorder: The crucial role of subclinical depressive symptoms and maternal avoidance behaviour. Arch. Women’s Ment. Health 2014, 17, 433–442. [Google Scholar] [CrossRef] [PubMed]
- Atzil, S.; Hendler, T.; Feldman, R. Specifying the Neurobiological Basis of Human Attachment: Brain, Hormones, and Behavior in Synchronous and Intrusive Mothers. Neuropsychopharmacology 2011, 36, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Atzil, S.; Hendler, T.; Zagoory-Sharon, O.; Winetraub, Y.; Feldman, R. Synchrony and Specificity in the Maternal and the Paternal Brain: Relations to Oxytocin and Vasopressin. J. Am. Acad. Child Acad. Psychiatry 2012, 51, 798–811. [Google Scholar] [CrossRef] [PubMed]
- Belsky, J. Mother-Infant Interaction at Home and in the Laboratory: A Comparative Study. J. Genet. Psychol. 1980, 137, 37–47. [Google Scholar] [CrossRef]
- Gardner, F. Methodological Issues in the Direct Observation of Parent–Child Interaction: Do Observational Findings Reflect. the Natural Behavior of Participants? Clin. Child Fam. Psychol. Rev. 2000, 3, 185–198. [Google Scholar] [CrossRef]
- Abu Salih, M.; Abargil, M.; Badarneh, S.; klein Selle, N.; Irani, M.; Atzil, S. Evidence for cultural differences in affect during mother–infant interactions. Sci. Rep. 2023, 13, 4831. [Google Scholar] [CrossRef]
- Feldman, R.; Gordon, I.; Zagoory-Sharon, O. Maternal and paternal plasma, salivary, and urinary oxytocin and parent–infant synchrony: Considering stress and affiliation components of human bonding. Dev. Sci. 2011, 14, 752–761. [Google Scholar] [CrossRef]
- Pratt, M.; Zeev-Wolf, M.; Goldstein, A.; Feldman, R. Exposure to early and persistent maternal depression impairs the neural basis of attachment in preadolescence. Prog. Neuropsychopharmacol. Biol. Psychiatry 2019, 93, 21–30. [Google Scholar] [CrossRef]
- Viaux-Savelon, S.; Dommergues, M.; Rosenblum, O.; Bodeau, N.; Aidane, E.; Philippon, O.; Mazet, P.; Vibert-Guigue, C.; Vauthier-Brouzes, D.; Feldman, R.; et al. Prenatal Ultrasound Screening: False Positive Soft Markers May Alter Maternal Representations and Mother-Infant Interaction. PLoS ONE. 2012, 7, e30935. [Google Scholar] [CrossRef]
- Atzil, S.; Hendler, T.; Feldman, R. The brain basis of social synchrony. Soc. Cogn. Affect. Neurosci. 2014, 9, 1193–1202. [Google Scholar] [CrossRef]
- Hayes, A.F.; Krippendorff, K. Answering the Call for a Standard Reliability Measure for Coding Data. Commun. Methods Meas. 2007, 1, 77–89. [Google Scholar] [CrossRef]
- Johnson, M.H.; Senju, A.; Tomalski, P. The two-process theory of face processing: Modifications based on two decades of data from infants and adults. Neurosci. Biobehav. Rev. 2015, 50, 169–179. [Google Scholar] [CrossRef]
- Hains, S.M.J.; Muir, D.W. Infant Sensitivity to Adult Eye Direction. Child Dev. 1996, 67, 1940–1951. [Google Scholar] [CrossRef]
- Stern, D.N. A Micro-Analysis of Mother-Infant Interaction: Behavior Regulating Social Contact Between a Mother and her 3 1/2-Month-Old Twins. J. Am. Acad. Child Psychiatry 1971, 10, 501–517. [Google Scholar] [CrossRef]
- Mesman, J.; van IJzendoorn, M.H.; Bakermans-Kranenburg, M.J. The many faces of the Still-Face Paradigm: A review and meta-analysis. Dev. Rev. 2009, 29, 120–162. [Google Scholar] [CrossRef]
- Tronick, E.Z. Emotions and emotional communication in infants. Am. Psychol. 1989, 44, 112–119. [Google Scholar] [CrossRef]
- Hane, A.A.; LaCoursiere, J.N.; Mitsuyama, M.; Wieman, S.; Ludwig, R.J.; Kwon, K.Y.; Browne, J.V.; Austin, J.; Myers, M.M.; Welch, M.G. The Welch Emotional Connection Screen: Validation of a brief mother–infant relational health screen. Acta Paediatr. 2019, 108, 615–625. [Google Scholar] [CrossRef]
- Feldman, R.; Eidelman, A.I. Direct and indirect effects of breast milk on the neurobehavioral and cognitive development of premature infants. Dev. Psychobiol. 2003, 43, 109–119. [Google Scholar] [CrossRef]
- Lavelli, M.; Poli, M. Early mother-infant interaction during breast- and bottle-feeding. Infant Behav. Dev. 1998, 21, 667–683. [Google Scholar] [CrossRef]
- Papp, L.M.; Papp, L.M. Longitudinal associations between breastfeeding and observed mother–child interaction qualities in early childhood. Child Care Health Dev. 2014, 40, 740–746. [Google Scholar] [CrossRef]
Figure 1.
Mothers with severe breastfeeding pain maintain a less focused gaze during face-to-face interaction with the infant. (A) Partial Pearson’s correlation between the degree of breastfeeding pain and mothers’ average time spent in focused gaze revealed a significant correlation after controlling for infants’ age differences. (B) Maternal-focused gaze was significantly different across the four breastfeeding groups. Post hoc LSD showed that mothers with severe pain maintained a less focused gaze compared to mothers with no breastfeeding pain (Cohen’s d = −0.94, p = 0.010, 95% CI [−46.65, −6.73]) and mothers with moderate pain (Cohen’s d = −0.92, p = 0.015, 95% CI [−46.74, −5.29]). Interestingly, mothers who do not breastfeed maintain a less focused gaze compared to mothers with no pain (Cohen’s d = −0.73, p = 0.024, 95% CI [−39.44, −2.81]) and mothers with moderate pain (Cohen’s d = −0.70, p = 0.038, 95% CI [−39.77, −1.13]), * p < 0.05.
Figure 1.
Mothers with severe breastfeeding pain maintain a less focused gaze during face-to-face interaction with the infant. (A) Partial Pearson’s correlation between the degree of breastfeeding pain and mothers’ average time spent in focused gaze revealed a significant correlation after controlling for infants’ age differences. (B) Maternal-focused gaze was significantly different across the four breastfeeding groups. Post hoc LSD showed that mothers with severe pain maintained a less focused gaze compared to mothers with no breastfeeding pain (Cohen’s d = −0.94, p = 0.010, 95% CI [−46.65, −6.73]) and mothers with moderate pain (Cohen’s d = −0.92, p = 0.015, 95% CI [−46.74, −5.29]). Interestingly, mothers who do not breastfeed maintain a less focused gaze compared to mothers with no pain (Cohen’s d = −0.73, p = 0.024, 95% CI [−39.44, −2.81]) and mothers with moderate pain (Cohen’s d = −0.70, p = 0.038, 95% CI [−39.77, −1.13]), * p < 0.05.

Figure 2.
Mothers with severe breastfeeding pain demonstrated weaker affective expressions during playful interactions with the infant. The X axis represents time, where events of positive infant engagement in play are temporally aligned on “0” and marked by the dashed green line. (A) Mothers with severe breastfeeding pain (in red) were less expressive during positive interactions with their infants than mothers with no and moderate breastfeeding pain. (B) Mothers with no breastfeeding pain (in blue) were more responsive to the infant when they engaged in play by shifting up their positive valence just before the infants shifted up their positive valence. (C) Pain did not affect the maternal gaze during events of infant engagement, * p < 0.05.
Figure 2.
Mothers with severe breastfeeding pain demonstrated weaker affective expressions during playful interactions with the infant. The X axis represents time, where events of positive infant engagement in play are temporally aligned on “0” and marked by the dashed green line. (A) Mothers with severe breastfeeding pain (in red) were less expressive during positive interactions with their infants than mothers with no and moderate breastfeeding pain. (B) Mothers with no breastfeeding pain (in blue) were more responsive to the infant when they engaged in play by shifting up their positive valence just before the infants shifted up their positive valence. (C) Pain did not affect the maternal gaze during events of infant engagement, * p < 0.05.

Figure 3.
Infants of mothers with severe breastfeeding pain expressed weaker affective expressions and maintained a longer focused gaze during mother–infant interactions. (A) There was a significant association between the degree of maternal breastfeeding pain and infant expression intensity (Pearson r = −0.36, p = 0.013 two-tailed, n = 49, 95% CI [−0.58, −0.08]). (B) A significant association existed between the degree of maternal breastfeeding pain and infants’ focused gaze (Pearson r = 0.4, p = 0.005 two-tailed, 95% CI [0.125, 0.632]).
Figure 3.
Infants of mothers with severe breastfeeding pain expressed weaker affective expressions and maintained a longer focused gaze during mother–infant interactions. (A) There was a significant association between the degree of maternal breastfeeding pain and infant expression intensity (Pearson r = −0.36, p = 0.013 two-tailed, n = 49, 95% CI [−0.58, −0.08]). (B) A significant association existed between the degree of maternal breastfeeding pain and infants’ focused gaze (Pearson r = 0.4, p = 0.005 two-tailed, 95% CI [0.125, 0.632]).


{kind=link}
{kind=link}
{kind=link}
Table 1.
ARCS—Affect Regulation Coding System. Trained coders coded the second-by-second social signals of valence, the intensity of the affective expression, and the gaze during free interaction. Each variable was coded separately for each mother and infant per second.
Table 1.
ARCS—Affect Regulation Coding System. Trained coders coded the second-by-second social signals of valence, the intensity of the affective expression, and the gaze during free interaction. Each variable was coded separately for each mother and infant per second.
| Behavioral Coding | Coding Values |
|---|---|
| Valence | Negative/Neutral/Positive |
| The intensity of affective expression | No facial effort |
| Mild facial effort | |
| Strong facial effort | |
| Gaze | Unfocused gaze |
| Directed gaze | |
| Glancing |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Abargil, M.; Irani, M.; klein Selle, N.; Atzil, S. Breastfeeding at Any Cost? Adverse Effects of Breastfeeding Pain on Mother–Infant Behavior. Biology 2023, 12, 636. https://doi.org/10.3390/biology12050636
AMA Style
Abargil M, Irani M, klein Selle N, Atzil S. Breastfeeding at Any Cost? Adverse Effects of Breastfeeding Pain on Mother–Infant Behavior. Biology. 2023; 12(5):636. https://doi.org/10.3390/biology12050636
Chicago/Turabian StyleAbargil, Maayan, Merav Irani, Nathalie klein Selle, and Shir Atzil. 2023. "Breastfeeding at Any Cost? Adverse Effects of Breastfeeding Pain on Mother–Infant Behavior" Biology 12, no. 5: 636. https://doi.org/10.3390/biology12050636
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.