
Do Repeated Sprints Affect the Biceps Femoris Long Head Architecture in Football Players with and without an Injury History?—A Retrospective Study

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Dynamometry
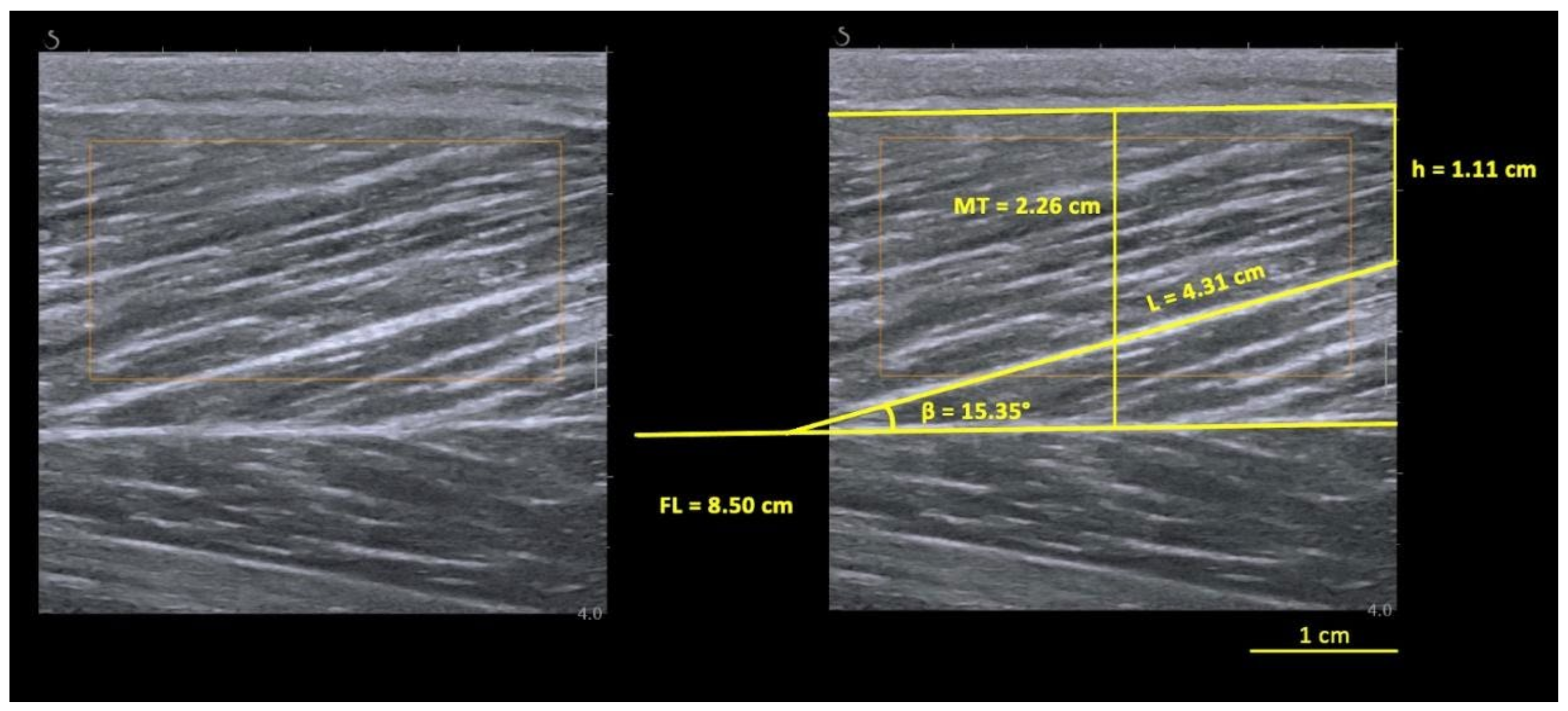
2.2. BFlh Architecture Assessment
2.3. Protocol
2.4. Data Processing
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gabbe, B.J.; Bennell, K.L.; Finch, C.F.; Wajswelner, H.; Orchard, J.W. Predictors of Hamstring Injury at the Elite Level of Australian Football. Scand. J. Med. Sci. Sport. 2006, 16, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Gabbe, B.; Finch, C.; Wajswelner, H.; Bennell, K. Australian Football: Injury Profile at the Community Level. J. Sci. Med. Sport 2002, 5, 149–160. [Google Scholar] [CrossRef] [PubMed]
- Feeley, B.T.; Kennelly, S.; Barnes, R.P.; Muller, M.S.; Kelly, B.T.; Rodeo, S.A.; Warren, R.F. Epidemiology of National Football League Training Camp Injuries from 1998 to 2007. Am. J. Sport. Med. 2008, 36, 1597–1603. [Google Scholar] [CrossRef] [PubMed]
- Brooks, J.H.M.; Fuller, C.W.; Kemp, S.P.T.; Reddin, D.B. Incidence, Risk, and Prevention of Hamstring Muscle Injuries in Professional Rugby Union. Am. J. Sport. Med. 2006, 34, 1297–1306. [Google Scholar] [CrossRef] [PubMed]
- Henderson, G.; Barnes, C.A.; Portas, M.D. Factors Associated with Increased Propensity for Hamstring Injury in English Premier League Soccer Players. J. Sci. Med. Sport 2010, 13, 397–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Injury Incidence and Injury Patterns in Professional Football: The UEFA Injury Study. Br. J. Sport. Med. 2011, 45, 553–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woods, C.; Hawkins, R.D.; Maltby, S.; Hulse, M.; Thomas, A.; Hodson, A. Football Association Medical Research Programme The Football Association Medical Research Programme: An Audit of Injuries in Professional Football—Analysis of Hamstring Injuries. Br. J. Sport. Med. 2004, 38, 36–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekstrand, J.; Hägglund, M.; Waldén, M. Epidemiology of Muscle Injuries in Professional Football (soccer). Am. J. Sport. Med. 2011, 39, 1226–1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hägglund, M.; Waldén, M.; Ekstrand, J. Risk Factors for Lower Extremity Muscle Injury in Professional Soccer: The UEFA Injury Study. Am. J. Sport. Med. 2013, 41, 327–335. [Google Scholar] [CrossRef] [Green Version]
- Heiderscheit, B.C.; Sherry, M.A.; Silder, A.; Chumanov, E.S.; Thelen, D.G. Hamstring Strain Injuries: Recommendations for Diagnosis, Rehabilitation, and Injury Prevention. J. Orthop. Sport. Phys. Ther. 2010, 40, 67–81. [Google Scholar] [CrossRef]
- Ekstrand, J. Keeping Your Top Players on the Pitch: The Key to Football Medicine at a Professional Level. Br. J. Sport. Med. 2013, 47, 723–724. [Google Scholar] [CrossRef] [Green Version]
- Green, B.; Bourne, M.N.; van Dyk, N.; Pizzari, T. Recalibrating the Risk of Hamstring Strain Injury (HSI): A 2020 Systematic Review and Meta-Analysis of Risk Factors for Index and Recurrent Hamstring Strain Injury in Sport. Br. J. Sport. Med. 2020, 54, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Girard, O.; Mendez-Villanueva, A.; Bishop, D. Repeated-Sprint Ability—Part I: Factors Contributing to Fatigue. Sport. Med. 2011, 41, 673–694. [Google Scholar] [CrossRef]
- Askling, C.M.; Tengvar, M.; Saartok, T.; Thorstensson, A. Acute First-Time Hamstring Strains during High-Speed Running: A Longitudinal Study Including Clinical and Magnetic Resonance Imaging Findings. Am. J. Sport. Med. 2007, 35, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Timmins, R.G.; Bourne, M.N.; Shield, A.J.; Williams, M.D.; Lorenzen, C.; Opar, D.A. Short Biceps Femoris Fascicles and Eccentric Knee Flexor Weakness Increase the Risk of Hamstring Injury in Elite Football (soccer): A Prospective Cohort Study. Br. J. Sport. Med. 2016, 50, 1524–1535. [Google Scholar] [CrossRef] [PubMed]
- Porter, K.; Opar, D.; Williams, M.; Shield, A. Biceps Femoris Fascicle Length Is Shorter in a Previously Hamstring Injured Athlete. J. Sci. Med. Sport 2012, 15, S152. [Google Scholar] [CrossRef]
- Timmins, R.G.; Shield, A.J.; Williams, M.D.; Lorenzen, C.; Opar, D.A. Biceps Femoris Long Head Architecture: A Reliability and Retrospective Injury Study. Med. Sci. Sport. Exerc. 2015, 47, 905–913. [Google Scholar] [CrossRef] [Green Version]
- Kellis, E.; Galanis, N.; Kapetanos, G.; Natsis, K. Architectural Differences between the Hamstring Muscles. J. Electromyogr. Kinesiol. 2012, 22, 520–526. [Google Scholar] [CrossRef]
- Lieber, R.L.; Fridén, J. Functional and Clinical Significance of Skeletal Muscle Architecture. Muscle Nerve 2000, 23, 1647–1666. [Google Scholar] [CrossRef]
- Butterfield, T.A. Eccentric Exercise in Vivo: Strain-Induced Muscle Damage and Adaptation in a Stable System. Exerc. Sport Sci. Rev. 2010, 38, 51–60. [Google Scholar] [CrossRef]
- Silder, A.; Thelen, D.G.; Heiderscheit, B.C. Effects of Prior Hamstring Strain Injury on Strength, Flexibility, and Running Mechanics. Clin. Biomech. 2010, 25, 681–686. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Askling, C.; Saartok, T.; Thorstensson, A. Type of Acute Hamstring Strain Affects Flexibility, Strength, and Time to Return to Pre-Injury Level. Br. J. Sport. Med. 2006, 40, 40–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Askling, C.M.; Tengvar, M.; Saartok, T.; Thorstensson, A. Acute First-Time Hamstring Strains during Slow-Speed Stretching: Clinical, Magnetic Resonance Imaging, and Recovery Characteristics. Am. J. Sport. Med. 2007, 35, 1716–1724. [Google Scholar] [CrossRef]
- Kwah, L.K.; Pinto, R.Z.; Diong, J.; Herbert, R.D. Reliability and Validity of Ultrasound Measurements of Muscle Fascicle Length and Pennation in Humans: A Systematic Review. J. Appl. Physiol. 2013, 114, 761–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wisdom, K.M.; Delp, S.L.; Kuhl, E. Use It or Lose It: Multiscale Skeletal Muscle Adaptation to Mechanical Stimuli. Biomech. Model. Mechanobiol. 2015, 14, 195–215. [Google Scholar] [CrossRef]
- Guex, K.; Degache, F.; Morisod, C.; Sailly, M.; Millet, G.P. Hamstring Architectural and Functional Adaptations following Long vs. Short Muscle Length Eccentric Training. Front. Physiol. 2016, 7, 340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silder, A.; Whittington, B.; Heiderscheit, B.; Thelen, D.G. Identification of Passive Elastic Joint Moment-Angle Relationships in the Lower Extremity. J. Biomech. 2007, 40, 2628–2635. [Google Scholar] [CrossRef] [Green Version]
- Pimenta, R.; Blazevich, A.J.; Freitas, S.R. Biceps Femoris Long-Head Architecture Assessed Using Different Sonographic Techniques. Med. Sci. Sport. Exerc. 2018, 50, 2584–2594. [Google Scholar] [CrossRef]
- Berg, H.E.; Tedner, B.; Tesch, P.A. Changes in Lower Limb Muscle Cross-Sectional Area and Tissue Fluid Volume after Transition from Standing to Supine. Acta Physiol. Scand. 1993, 148, 379–385. [Google Scholar] [CrossRef]
- Kositsky, A.; Gonçalves, B.A.M.; Stenroth, L.; Barrett, R.S.; Diamond, L.E.; Saxby, D.J. Reliability and Validity of Ultrasonography for Measurement of Hamstring Muscle and Tendon Cross-Sectional Area. Ultrasound Med. Biol. 2020, 46, 55–63. [Google Scholar] [CrossRef]
- Franchi, M.V.; Fitze, D.P.; Raiteri, B.J.; Hahn, D.; Spörri, J. Ultrasound-Derived Biceps Femoris Long Head Fascicle Length: Extrapolation Pitfalls. Med. Sci. Sport. Exerc. 2020, 52, 233–243. [Google Scholar] [CrossRef] [Green Version]
- Ishøi, L.; Thorborg, K.; Hölmich, P.; Krommes, K. Sprint Performance In Football (Soccer) Players With And Without A Previous Hamstring Strain Injury: An Explorative Cross-Sectional Study. Int. J. Sport. Phys. Ther. 2020, 15, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Reurink, G.; Goudswaard, G.J.; Moen, M.H.; Weir, A.; Verhaar, J.A.N.; Bierma-Zeinstra, S.M.A.; Maas, M.; Tol, J.L. Rationale, Secondary Outcome Scores and 1-Year Follow-up of a Randomised Trial of Platelet-Rich Plasma Injections in Acute Hamstring Muscle Injury: The Dutch Hamstring Injection Therapy Study. Br. J. Sport. Med. 2015, 49, 1206–1212. [Google Scholar] [CrossRef] [PubMed]
- Maniar, N.; Shield, A.J.; Williams, M.D.; Timmins, R.G.; Opar, D.A. Hamstring Strength and Flexibility after Hamstring Strain Injury: A Systematic Review and Meta-Analysis. Br. J. Sport. Med. 2016, 50, 909–920. [Google Scholar] [CrossRef] [PubMed]
- Chumanov, E.S.; Heiderscheit, B.C.; Thelen, D.G. The Effect of Speed and Influence of Individual Muscles on Hamstring Mechanics during the Swing Phase of Sprinting. J. Biomech. 2007, 40, 3555–3562. [Google Scholar] [CrossRef]
- Baumert, P.; Temple, S.; Stanley, J.M.; Cocks, M.; Strauss, J.A.; Shepherd, S.O.; Drust, B.; Lake, M.J.; Stewart, C.E.; Erskine, R.M. Neuromuscular Fatigue and Recovery after Strenuous Exercise Depends on Skeletal Muscle Size and Stem Cell Characteristics. Sci. Rep. 2021, 11, 7733. [Google Scholar] [CrossRef]
- Reeves, N.D.; Narici, M.V. Behavior of Human Muscle Fascicles during Shortening and Lengthening Contractions in Vivo. J. Appl. Physiol. 2003, 95, 1090–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sant, G.L.; Le Sant, G.; Ates, F.; Brasseur, J.-L.; Nordez, A. Elastography Study of Hamstring Behaviors during Passive Stretching. PLoS ONE 2015, 10, e0139272. [Google Scholar]
- Bourne, M.N.; Williams, M.D.; Opar, D.A.; Al Najjar, A.; Kerr, G.K.; Shield, A.J. Impact of Exercise Selection on Hamstring Muscle Activation. Br. J. Sport. Med. 2017, 51, 1021–1028. [Google Scholar] [CrossRef] [Green Version]
- Bourne, M.N.; Timmins, R.G.; Opar, D.A.; Pizzari, T.; Ruddy, J.D.; Sims, C.; Williams, M.D.; Shield, A.J. An Evidence-Based Framework for Strengthening Exercises to Prevent Hamstring Injury. Sport. Med. 2018, 48, 251–267. [Google Scholar] [CrossRef]
- Evangelidis, P.E.; Shan, X.; Otsuka, S.; Yang, C.; Yamagishi, T.; Kawakami, Y. Hamstrings Load Bearing in Different Contraction Types and Intensities: A Shear-Wave and B-Mode Ultrasonographic Study. PLoS ONE 2021, 16, e0251939. [Google Scholar] [CrossRef] [PubMed]
- Frisk, R.F.; Lorentzen, J.; Barber, L.; Nielsen, J.B. Characterization of Torque Generating Properties of Ankle Plantar Flexor Muscles in Ambulant Adults with Cerebral Palsy. Eur. J. Appl. Physiol. 2019, 119, 1127–1136. [Google Scholar] [CrossRef]
- Gao, F.; Zhang, L.-Q. Altered Contractile Properties of the Gastrocnemius Muscle Poststroke. J. Appl. Physiol. 2008, 105, 1802–1808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, N.G.; Falvo, M.J.; Damiano, D.L. Rapid Force Generation Is Impaired in Cerebral Palsy and Is Related to Decreased Muscle Size and Functional Mobility. Gait Posture 2012, 35, 154–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreau, N.G.; Holthaus, K.; Marlow, N. Differential Adaptations of Muscle Architecture to High-Velocity versus Traditional Strength Training in Cerebral Palsy. Neurorehabil. Neural Repair 2013, 27, 325–334. [Google Scholar] [CrossRef] [PubMed]
- De Lima-E-Silva, F.X.; de Lima-E-Silva, F.X.; Oliveira, G.S.; Medeiros, T.M.; Dornelles, M.P.; Ribeiro-Alvares, J.B.A.; Baroni, B.M. Flexibility, Strength, and Fascicle Length of Football Players with and without History of Hamstring Strain Injury in the Prior Season. Sci. Med. Footb. 2020, 4, 322–328. [Google Scholar] [CrossRef]
- Ribeiro-Alvares, J.B.; Dornelles, M.P.; Fritsch, C.G.; de Lima-E-Silva, F.X.; Medeiros, T.M.; Severo-Silveira, L.; Marques, V.B.; Baroni, B.M. Prevalence of Hamstring Strain Injury Risk Factors in Professional and Under-20 Male Football (Soccer) Players. J. Sport Rehabil. 2020, 29, 339–345. [Google Scholar] [CrossRef]
- Gonçalves, B.A.M.; Meinders, E.; Saxby, D.J.; Barrett, R.S.; Bourne, M.N.; Diamond, L.E. Repeated Sprints Alter Mechanical Work Done by Hip and Knee, but Not Ankle, Sagittal Moments. J. Sci. Med. Sport 2021, 24, 939–944. [Google Scholar] [CrossRef]
- Butterfield, T.A.; Herzog, W. Quantification of Muscle Fiber Strain during in Vivo Repetitive Stretch-Shortening Cycles. J. Appl. Physiol. 2005, 99, 593–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubo, K.; Ikebukuro, T. Changes in Joint, Muscle, and Tendon Stiffness Following Repeated Hopping Exercise. Physiol Rep 2019, 7, e14237. [Google Scholar] [CrossRef]
- Freitas, S.R.; Marmeleira, J.; Valamatos, M.J.; Blazevich, A.; Mil-Homens, P. Ultrasonographic Measurement of the Biceps Femoris Long-Head Muscle Architecture. J. Ultrasound Med. 2018, 37, 977–986. [Google Scholar] [CrossRef] [PubMed]
- Lee Dow, C.; Timmins, R.G.; Ruddy, J.D.; Williams, M.D.; Maniar, N.; Hickey, J.T.; Bourne, M.N.; Opar, D.A. Prediction of Hamstring Injuries in Australian Football Using Biceps Femoris Architectural Risk Factors Derived From Soccer. Am. J. Sport. Med. 2021, 49, 3687–3695. [Google Scholar] [CrossRef] [PubMed]
- Ferber, R.; Davis, I.M.; Williams, D.S., 3rd. Gender Differences in Lower Extremity Mechanics during Running. Clin. Biomech. 2003, 18, 350–357. [Google Scholar] [CrossRef]
- Willson, J.D.; Petrowitz, I.; Butler, R.J.; Kernozek, T.W. Male and Female Gluteal Muscle Activity and Lower Extremity Kinematics during Running. Clin. Biomech. 2012, 27, 1052–1057. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Injured Players vs. Healthy Controls | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PRE SPRINT | POST SPRINT | Instant (Pre vs. Post) | Injury (Injured vs. Control) | Instant × Injury Interaction | |||||||
| Injured | Control | Injured | Control | p | η2p | p | η2p | p | η2p | ||
| REST | FL (cm) | 7.40 ± 0.98 | 8.20 ± 0.80 | 7.02 ± 1.20 | 8.29 ± 1.38 | 0.298 | 0.039 | 0.014 | 0.196 | 0.103 | 0.092 |
| PA (°) | 21.35 ± 2.67 | 18.47 ± 2.32 | 22.91 ± 3.09 | 18.65 ± 3.00 | 0.011 | 0.208 | 0.002 | 0.307 | 0.041 | 0.141 | |
| MT (cm) | 2.61 ± 0.28 | 2.58 ± 0.30 | 2.66 ± 0.26 | 2.60 ± 0.33 | 0.208 | 0.056 | 0.707 | 0.005 | 0.619 | 0.009 | |
| ACTIVE | FL (cm) | 6.36 ± 1.21 | 7.89 ± 0.96 | 6.22 ± 1.13 | 7.86 ± 0.83 | 0.504 | 0.015 | <0.001 | 0.413 | 0.677 | 0.006 |
| PA (°) | 25.04 ± 3.34 | 20.28 ± 2.97 | 24.68 ± 4.06 | 20.60 ± 2.70 | 0.971 | <0.001 | <0.001 | 0.368 | 0.492 | 0.016 | |
| MT (cm) | 2.62 ± 0.27 | 2.69 ± 0.30 | 2.54 ± 0.24 | 2.73 ± 0.26 | 0.476 | 0.017 | 0.173 | 0.061 | 0.036 | 0.138 | |
| PT (N⋅m) | 141.17 ± 43.90 | 149.39 ± 35.45 | 132.54 ± 37.18 | 136.64 ± 32.27 | <0.001 | 0.399 | 0.642 | 0.007 | 0.397 | 0.024 | |
| Injured vs. Contralateral Limbs | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| PRE SPRINT | POST SPRINT | Instant (Pre vs. Post) | Injury (Injured vs. Healthy) | Instant × Injury Interaction | |||||||
| Injured | Contralateral | Injured | Contralateral | p | η2p | p | η2p | p | η2p | ||
| REST | FL (cm) | 7.40 ± 0.98 | 9.14 ± 2.18 | 7.02 ± 1.20 | 8.36 ± 1.88 | <0.001 | 0.799 | 0.012 | 0.519 | 0.394 | 0.082 |
| PA (°) | 21.35 ± 2.67 | 18.81 ± 4.22 | 22.91 ± 3.09 | 20.14 ± 3.62 | 0.001 | 0.732 | 0.006 | 0.582 | 0.834 | 0.005 | |
| MT (cm) | 2.61 ± 0.28 | 2.77 ± 0.24 | 2.66 ± 0.26 | 2.75 ± 0.24 | 0.646 | 0.024 | 0.088 | 0.289 | 0.250 | 0.144 | |
| ACTIVE | FL (cm) | 6.36 ± 1.21 | 7.73 ± 2.57 | 6.22 ± 1.13 | 7.60 ± 1.84 | 0.543 | 0.035 | 0.039 | 0.332 | 0.989 | <0.001 |
| PA (°) | 25.04 ± 3.34 | 22.06 ± 4.28 | 24.68 ± 4.06 | 21.23 ± 3.46 | 0.454 | 0.052 | 0.018 | 0.412 | 0.691 | 0.015 | |
| MT (cm) | 2.62 ± 0.27 | 2.70 ± 0.40 | 2.54 ± 0.24 | 2.60 ± 0.35 | 0.073 | 0.263 | 0.371 | 0.073 | 0.685 | 0.016 | |
| PT (N⋅m) | 141.17 ± 43.90 | 141.44 ± 36.59 | 132.54 ± 37.18 | 133.76 ± 35.53 | 0.017 | 0.419 | 0.857 | 0.003 | 0.735 | 0.011 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pimenta, R.; Antunes, H.; Lopes, T.; Veloso, A. Do Repeated Sprints Affect the Biceps Femoris Long Head Architecture in Football Players with and without an Injury History?—A Retrospective Study. Biology 2023, 12, 96. https://doi.org/10.3390/biology12010096
Pimenta R, Antunes H, Lopes T, Veloso A. Do Repeated Sprints Affect the Biceps Femoris Long Head Architecture in Football Players with and without an Injury History?—A Retrospective Study. Biology. 2023; 12(1):96. https://doi.org/10.3390/biology12010096
Chicago/Turabian StylePimenta, Ricardo, Hugo Antunes, Tomás Lopes, and António Veloso. 2023. "Do Repeated Sprints Affect the Biceps Femoris Long Head Architecture in Football Players with and without an Injury History?—A Retrospective Study" Biology 12, no. 1: 96. https://doi.org/10.3390/biology12010096