
High-Risk Human Papillomavirus Infection in Lung Cancer: Mechanisms and Perspectives
by
 ,
,
Julio C. Osorio
1,
Felipe Candia-Escobar
1,
Alejandro H. Corvalán
2,
Gloria M. Calaf
3 and
Francisco Aguayo
4,* 1
Laboratorio de Oncovirología, Programa de Virología, Instituto de Ciencias Biomédicas (ICBM), Facultad de Medicina, Universidad de Chile, Santiago 8380000, Chile
2
Advanced Center for Chronic Diseases (ACCDiS), Pontificia Universidad Católica de Chile, Santiago 8320000, Chile
3
Instituto de Alta Investigación, Universidad de Tarapacá, Arica 1000000, Chile
4
Universidad de Tarapacá, Arica 1000000, Chile
*
Author to whom correspondence should be addressed.
Biology 2022, 11(12), 1691; https://doi.org/10.3390/biology11121691
Submission received: 15 October 2022
/
Revised: 8 November 2022
/
Accepted: 16 November 2022
/
Published: 23 November 2022
(This article belongs to the Section Cancer Biology)
Abstract
:Simple Summary
A subset of human papillomaviruses (HPVs), so-called high-risk (HR)-HPVs are the causal agents of cervical, anogenital and a group of head and neck carcinomas. Additionally, HR-HPVs have been detected in extragenital tumors including in lung cancer, though their role in this heterogeneous group of malignancies remains controversial. In this review, we address the epidemiological and experimental studies regarding the role of HR-HPV in lung cancer, worldwide, and we propose potential mechanisms. The evidence suggests that HR-HPVs are involved in the development of a variable subset of lung carcinomas in both smoker and non-smoker subjects.
Abstract
Lung cancer is a very prevalent and heterogeneous group of malignancies, and most of them are etiologically associated with tobacco smoking. However, viral infections have been detected in lung carcinomas, with high-risk human papillomaviruses (HR-HPVs) being among them. The role of HR-HPVs in lung cancer has been considered to be controversial. This issue is due to the highly variable presence of this virus in lung carcinomas worldwide, and the low viral load frequently that is detected. In this review, we address the epidemiological and mechanistic findings regarding the role of HR-HPVs in lung cancer. Some mechanisms of HR-HPV-mediated lung carcinogenesis have been proposed, including (i) HPV works as an independent carcinogen in non-smoker subjects; (ii) HPV cooperates with carcinogenic compounds present in tobacco smoke; (iii) HPV promotes initial alterations being after cleared by the immune system through a “hit and run” mechanism. Additional research is warranted to clarify the role of HPV in lung cancer.
1. Introduction
Lung cancer is the main cause of cancer deaths around the world, with there having been 1.8 million deaths in 2020 and an estimated nearly 2 million cases by 2022 [1]. Lung cancer is associated with multiple etiological factors including environmental, lifestyle and/or genetic ones [2]. Although this cancer is a heterogeneous disease, tobacco smoke is the most important etiological factor in most of the populations around the world [3]. Due to its heterogeneity, it can be sorted into two main groups with subsequent subclassifications: small-cell lung carcinomas (SCLCs) represent near of 15% of the lung cancer cases, with there being a tendency for this to be decreasing in all the populations [4]. SCLCs are characterized by a neuroendocrine origin, aggressivity and a poor outcome [5]. Non-small-cell lung carcinomas (NSCLCs) are the most common type of lung malignancy, contributing to ~85% of cases, and it is subclassified into three groups: squamous cell carcinoma (SQC), adenocarcinoma (AdC) and large cell carcinoma (LCC) [6].
A plethora of persistent viral infections have been detected in lung carcinomas worldwide, including high-risk human papillomaviruses (HR-HPVs) [7], Merkel cell polyomavirus (MCPyV) [8], Jaagsiekte Sheep Retrovirus (JSRV) [9], John Cunningham Virus (JCV) [10], and Epstein–Barr virus (EBV) [11]. However, the role of these viruses in lung cancer has not been clarified because the very variable viral presence of them in the populations, them having a low viral load and there being some bias in the detection methods. In addition, a high percentage of lung cancer is etiologically associated with tobacco smoking, which suggest that the viruses could have an oncogenic role in non-smokers. HR-HPVs have been detected in significant percentages of lung carcinomas worldwide, although the etiological role of this malignancy remains enigmatic. Due to HPV infections not being a sufficient condition for carcinogenesis, we addressed its potential cooperation with tobacco smoke. We focused on epidemiological and mechanistic evidence regarding a potential role of HR-HPVs in lung cancer.
2. Human Papillomavirus: Classification, Structure and Replication Cycle
Human papillomaviruses (HPVs) are members of the Papillomaviridae family which includes five genera: alpha-HPV (α-HPV), beta-HPV (β-HPV), gamma-HPV (γ-HPV), mu-HPV and nu-HPV [12]. The β-HPV, γ-HPV, mu-HPV and nu-HPV infect the cutaneous epithelia, while α-HPV infects both the mucous and cutaneous epithelia [13]. The α-HPV includes the high-risk (HR)-HPV, intermediate-risk (IR-HPV) and low-risk (LR)-HPV genotypes [14]. The HR-HPVs can be subdivided as carcinogenic (Group 1), probably carcinogenic (Group 2a) and possibly carcinogenic (Group 2b) by the International Agency for Research on Cancer (IARC). HPV consists of a non-enveloped particle of 55 nm in diameter with an icosahedral symmetry [15], whose genome is made of double-stranded DNA with about 8,000 nucleotides, and it holds eight open reading frames (ORFs), encoding for six early and two late proteins [16]. Furthermore, the non-coding long control region (LCR), located between the L1 and E6 genes regulates the viral gene expression program, and it is currently divided into three segments: the 5′ segment, the central segment and the 3′ segment [17,18]. Cellular transcription factors including Ying-yang 1(YY1), Nuclear-factor 1(NF1), Activator protein 1 (AP1), Glucocorticoid receptor (GR) and Progesterone receptor (PR), among others, can bind to the cognate site in this region for viral gene expression regulation. Additionally, viral E2 protein binding to cognate sites inside the LCR stimulate or to suppress the viral transcriptional activity with effects depending on different HPV types and variants [19,20,21]. The E region encodes all the non-structural E1, E2, E4, E5, E6 and E7 proteins, with them having major functions in viral replication and cell transformation [22]. On the other hand, the L region encodes for the major (L1) and minor (L2) structural proteins. The E2 gene encodes for a protein that can regulate the expression levels of the viral gene products [23]. Indeed, depending on the binding sites that are occupied by E2 in the LCR, it acts as a transcriptional repressor or activator [24]. Additionally, E2 recruits E1, a protein with helicase activity, at the viral replication origin for DNA replication [25,26], and finally, it transfers the viral genome to the daughter cells during host cell division [27]. The E4 gene encodes for the most abundant viral proteins, with it having functions in viral genome amplification and viral release [28]. The E5 gene encodes for an oncogenic protein that contributes to the productive state of the viral cycle and tumor progression [29], with an important role in the epidermal growth factor receptor (EGFR) activation and immune evasion [30]. Additionally, the E5 protein shows different host cellular targets that affect EGFR regulation mainly through the endosomal acidification process or by disrupting the EGFR ubiquitination in human foreskin keratinocytes [31]. In addition, the E5 protein has effects on the heavy chain of human histocompatibility antigen (HLA) and can interfere with the antigen presentation, which would derive from HR-HPV immune evasion [32]. E6 and E7 are known to be involved in cell cycle dysregulation, and they are responsible for viral genome replication [33]. The E6 and E7 oncogene expression by the episomal HR-HPV can contribute to tumor lesion progression [34]. The E6 oncogene mediates cell transformation, in part, by forming a complex with cellular E3 ligase E6-Association Protein (E6AP) to target p53 for degradation by the ubiquitin proteasome pathway [35]. Further, E6 increases the hTERT activity and inhibits interferon regulatory factor-3 transcriptional activity [36]. On the other hand, E7 is a small, dimeric protein that can bind and promote pRB degradation, which causes premature E2F releasing [37]. In addition, E7 mediates the activation of cyclin E and cyclin A, which are required for malignant transformation [38,39]. Additional interactions between the E6/E7 proteins and host partners are also involved in carcinogenesis [40].
HPV is an epitheliotropic virus, and the infectious cycle occurs in the stratified squamous epithelium [41]. In the cervical cells, HPV infects the basal epithelial cells of the squamocolumnar junctions through a microlesion in the host’s skin or mucosa, gaining direct access to the target cells [42,43,44]. Firstly, HPV binds to the heparan sulfate proteoglycans (HSPGs) which is located on the surface of the epithelial cells or basal lamina [45]. It has been established that after the HPV cell attachment, conformational changes occur in the capsid due to the proteolytic cleavage of the L2 protein [46], and cell entry is achieved by an endocytosis-mediated mechanism [47]. A virion rupture is accomplished due to the acidification of the endosome, revealing an L2-viral DNA complex [48] that is transported by actin microfilaments towards the Golgi apparatus [49] and nucleus [50]. The nuclear entry requires mitosis that allows the rupture of the nuclear membrane, thus facilitating the viral DNA association with chromatin [50]. After its entry into the nucleus, the viral genome stabilizes as an episome that is attached to the host genome through the E2 viral protein [51]. The transcription starts from the early promoter and occurs only from one viral DNA strand [52]. Most HPV transcripts are polycistronic [53], and the generated pre-ribonucleic acid (RNA) messengers (mRNA) are spliced into smaller mRNA pieces encoding different viral proteins [16,54]. During early infection, all of the early viral proteins (E1, E2 and E4–E7) are expressed [55]. The early polyadenylation signal (pAe) is blocked by E2, allowing there to be longer reads of the viral genome, ending at the late polyadenylation signal (pAl) and then expressing late mRNAs [56]. Most HPV infections are cleared by the immune system from 1 to 2 years [57], despite persistent HPV infections being a prerequisite for the development of a high-grade precancerous lesion [58]. Viral genome integration allows for E6 and E7 overexpression, which causes cell cycle deregulation and increases the genetic instability [59,60].
3. Epidemiology of HPV in Lung Cancer
Syrjänen (1972) described for the first time the presence of a condyloma-type lesion with the presence of koilocytosis in a bronchial SQC. This description turned out to be very similar to reports of cervical cancer lesions [61]. Additionally, Syrjänen (1980) described 104 bronchial SQCs, in which three different types of condylomatous lesions (papillomatous, flat and endophytic) were identified. Furthermore, the presence of a condyloma-type lesion with the presence of koilocytosis was reported [62]. Stremlau et al. (1985) reported one anaplastic carcinoma in the lung that contained HPV16 genotypes [63]. In 1989, Syrjänen et al. discovered the presence of HPV6/16 genotypes in bronchial SQCs by conducting in situ DNA hybridization (ISH) [64]. During the 1990s, different European countries reported HPV detections in lung carcinomas at different frequencies. In France, Béjui-Thivolet et al. (1990) reported HPV in seven out of forty-three (16%) tumor specimens by using the same method [65], while Thomas et al. (1995) found HPV in five out of thirty-one (16%) cases by using a nested polymerase chain reaction (PCR) [66]. In Greece, Noutsou et al. (1996), reported an HPV presence in 15 out of 99 (15%) lung carcinomas by using PCR [67]. Conversely, in Germany, Welt et al. (1997) did not detect HPV in 38 specimens by using ISH/PCR [68]. In Greece, Papadopoulou et al. (1998) found HPV in 36 out of 52 (69%) lung carcinomas by using PCR/Southern blotting (SB). Interestingly, HPV16/18 were the most prevalent genotypes (37.9%) [69]. However, in the same country, Gorgoulis et al. (1998) reported the absence of HPV in 91 lung SQCs by using PCR/ISH. [70]. In Norway, Henning et al. (1998) found HPV in 37 out of 75 (49%) lung carcinomas from women by using PCR/ISH [71]. In Asia, different HPV frequencies in lung carcinomas were reported in the same decade. In Beijing in the Republic of China, Xing et al. (1993) found HPV in seven out of forty-nine (14.3%) tumor samples by using multiplex PCR [72], though Szabó et al. (1994) reported the absence of HPVs (6, 11, 16, 18, 31, 33, 52b and 58) in 47 lung cancers from Japan by using PCR [73], and Tsuhako et al. (1998) detected HPV in 19 out of 207 (9%) lung carcinomas by using PCR and non-isotopic ISH in the same country [74]. Liu et al. (1994) found five out of forty-nine (10%) HPV-positive lung carcinomas from China by using PCR/ISH [75]. In the same country, Hu et al. (1997), found HPV in 16 out of 50 (32%) lung carcinomas by using PCR/dot-blot hybridization [76]. In the US, two studies were reported in the 1990s. Yousem et al. (1992), detected HPV in seven out of fifty-eight (12.1%) lung cancers [77], and Bolhmeyer et al. (1998) reported an HPV presence in six out of thirty-four (18%) lung carcinomas by using PCR. HPV18 was detected in 6% of the samples (2/34) [78]. During the 2000s, variable frequencies of HPV in lung carcinomas were found. In France, Clavel et al. (2000) found HPV in five out of one hundred and eighty-five (2.7%) samples by the a Hybrid Capture II assay (HCA) [79], while in Poland, Miasko et al. (2001) reported an HPV presence in four out of forty (10%) NSCLCs [80]. In Turkey, Kaya et al. (2001) detected HPV in three out of twenty-six (11.5%) cases (primary SQC) by using NISH [81], and Zafer et al. (2004) found HPV in two out of forty (5%) lung carcinomas by using ISH, PCR and SB [82]. In France, Brouchet et al. (2005) reported no HPV presence in 122 specimens by using IHC/ISH [83], and Coissard et al. (2005) found HPV in four out of two hundred and eighteen (2%) lung tumors by using reverse line blotting (RLB), though the E6 mRNA was undetectable [84]. In Italy, Ciotti et al. (2006) found HPV in eight out of thirty-eight (21%) NSCLCs by observing the E6/E7 expression [85], and Giuliani et al. (2007) found HPV in 10 out of 78 (13%) lung carcinomas by using PCR and RFLP. Interestingly, the E6 and E7 transcripts were expressed in nine samples [86].
In Asia, the HPV frequency in the lung cancer samples were relatively higher than they were in other regions of the world. For instance, in Taiwan, Cheng et al. (2001) found HPV in 77 out of 141 (54.6%) lung carcinomas and in 16 out of 60 (26.7%) non-cancer control samples [87]. Additionally, Hsu et al. (2009) found the HPV16 E6 oncoprotein in 49 out of 217 (22.6%) and HPV18 E6 in 31 out 217 (14.3%) patients with stage I NSCLC by using immunohistochemistry (IHC) [88]. In China, Yu et al. (2009) found HPV in 43 out of 109 (39%) lung carcinomas by using INNO-LIPA PCR and reverse transcriptase (RT)-PCR [89], while Xu et al. (2009) reported an HPV16/18 presence in 32 out 44 of (73%) SQCs by using ISH. Integrated forms of HPV were found in twenty-three (52.27%) and episomal forms were found in nine (20.45%) of the cases [90]. In the same country, Zhang et al. (2009) reported an HPV16 (E6 and E7 oncogenes and L1 gene) presence in 18 out of 104 (17.3%) lung carcinomas by using PCR/sequencing [91]. In addition, Fei et al. (2006) found HPV in 32% of the 73 lung tumors by using ISH [92], and Wang et al. (2008) reported an HPV prevalence in 23 out of 313 (39.2%) fresh lung tumor specimens by using PCR and NISH [93]. In Okinawa in Japan (2000), Miyagi et al. reported an HPV presence in 78 out of 434 (18%) surgically resected lung tumors by using PCR/SB [94]. In Seoul in Korea, Park et al. (2007) reported an HPV presence in 58 out of 112 (52%) NSCLCs. HPV16, 18, and 33 were detected in 12 (10.7%), 11 (9.8%), and 37 (33.0%) of the cases, respectively [95]. In Tehran in Iran, Nadji et al. (2007) found HPV in 37 out of 141 (26%) lung carcinomas by using nested PCR [96]. In Singapore, Lim et al. (2009) reported no HPV presence in 110 patients with adenocarcinoma by using ISH [97]. In Latin America, some studies have detected HPV in lung carcinomas. Castillo et al. (2006) reported an HPV presence in 10 out of 36 (28%) of tumors which were collected from Colombia, Mexico and Peru by using PCR/SB [98], while Aguayo et al. (2007) detected the HPV presence in 20 out of 69 (29%) lung carcinomas from Chile by using PCR/SB. HPV16 was found in 11 cases (16%) [99].
In Europe after 2010, a high level of variation in the HPV frequency in lung cancer patients has been reported. In Croatia, Branica et al. (2010) reported the HPV (16, 18 and 33 genotype) presence in three out of eighty-four (3.6%) bronchial aspirates of lung carcinoma patients by using PCR [100]. In Italy, Carpagnano et al. (2011) reported an HPV presence in 12 out of 89 (13.5%) exhaled breath condensates (EBC) of lung cancer patients by using PCR/pyrosequencing [101]. In Finland, Syrjänen et al. (2012) found HPV in four out of seventy-seven (5,2%) lung carcinomas by using HPV genotyping with the Luminex-based Multimetrix. Three specimens were HPV16-positive, and one case was coinfected with HPV6/HPV16 [102]. In Italy, Galvan et al. (2012) reported absence of HPV in 100 lung carcinomas by using PCR and hybridization using specific probes [103]. In Greece, Sarchianaki et al. (2014) found HPV in 19 out of 200 (9.5%) lung carcinomas by using qPCR. The HPV genotypes more frequently detected were HPV16 (42.1%) and HPV11 (15.8%) [104]. In Greece, Argyri et al. (2017) found HPV E6/E7 mRNA in two out of sixty-seven (3%) lung tissues by using PCR and Real-time nucleic acid sequence-based amplification (NASBA). E6/E7 mRNA was not found in any of the tissue samples [105]. In Copenhagen in Denmark, Shikova et al. (2017) reported an HPV16/18 presence in 33 out of 132 (25%) lung carcinomas by using PCR with GP5+/6+ primers and a type-specific (TS) primers for HPV16/18. When the HPV was analyzed by conducting a consensus PCR, only five out of one hundred and thirty-two (3.8%) samples were HPV-positive [106]. In the Czech Republic, Jaworek et al. (2020) did not detect HPV in 80 primary NSCLCs by using qPCR [107]. In Bordeaux, France, Chaussade et al. (2022) reported HPV incidence rate ratios (IRR) of 1.8 [1.4–2.2] in a cohort of HIV-positive patients with lung cancer (incidence rates for 100 000 people per year) [108]. In Badalona, Spain, Sirena et al. (2022) found HPV in 23 out of 41 (56%) lung carcinomas by using qPCR. Furthermore, the HR-HPV types were detected in 16 out of 41 samples (39%, 95% CI 26–54%), and HPV16 was the most prevalent genotype [13/16 (81.3%, 95% CI 57.0-93%] [109].
After 2010 in Asia, the HPV frequency in the lung cancer samples were relatively higher than they were in other regions of the world. In Kagoshima in Japan, Baba et al. (2010) found HPV in nine out of thirty (30%) AdCs and in two out of twenty-seven (7%) SQCs by using a PCR/INNO-LiPA assay. This difference was statistically significant (p = 0.044). Interestingly, in 20 additional specimens from patients who were treated with gefitinib, HR-HPV was found in six out of eight (75%) lung AdCs from patients with a complete or partial response to gefitinib, and it was not detected in the twelve patients that did not respond to gefitinib [110]. In the same country, Iwakawa et al. (2010) reported absence of HPV 16/18/33 in 297 lung AdCs by using multiplex PCR [111]. Additionally, Aguayo et al. (2010) found HPV-16 in eight out of sixty (13%) of lung carcinomas from China, Pakistan and Papua New Guinea by using RT-qPCR. Additionally, HPV16 was detected in eight out of eighteen (44%) SQCs [112]. In Japan, Goto et al. (2011) found HPV in 20 out of 304 (6.6%) of lung cancer samples by using PCR/ISH. The HPV16/18 genotypes were present in the most (75.7%) of the patients with lung cancer [113]. In Iran, Jafari et al. (2013) found HPV in nine out of fifty (18%) lung SQCs by using nested PCR/sequencing [114]. In China, Yu et al. (2013) found HPV16/18 in 44% of the lung cancers by using PCR, the INNO-LIPA genotyping system and SB. An HPV infection was more prevalent in the SQCs (59.8%) when they were compared to the AdCs (17.5%). HPV16/18 were the most frequently detected type [115]. In China, Fan et al. (2015) reported an HPV presence in 22 out of 262 (8.4%) lung carcinomas by using PCR, ISH (p53 and p16 expressions) and a reverse dot blot. The HPV infection rates in the SQC cases were significantly higher than they were in the AdC cases (12.69 versus 3.91%) [116]. In China, Yu et al. (2015) found HPV in 100 out of 180 (55.6%) lung carcinomas by using PCR and IHC. HPV16 was detected in 67 out of 180 (37.22%) cases, and HPV18 was detected in 56 out of 180 (31.11%) cases [117]. In Iraq, Al-Shabbani (2015) reported an HPV presence in 30 out of 50 (60%) lung carcinomas by using ISH. HPV16 and HPV18 were detected in 32% and 28% of the samples, respectively [118]. In Hefei in the Republic of China, Li et al. (2016) found HPV in 27 out of 95 (28.4%) advanced-lung AdCs by performing the PCR amplification of a fragment of the HPV L1 gene [119]. In Fuzhou in the Republic of China, Xiong et al. (2016) reported HPV presence in seven out of eighty-three (8.4%) lung carcinomas by using PCR and reverse hybridization [120]. In Fuzhou in the Republic of China, He F et al. (2020) found HPV in 13 out of 140 (9.3%) lung cancer tissues by using PCR amplification (L1 primers) and specific probe reverse hybridization [121]. In Tehran-Iran, Rezaei et al. (2020) found HPV in 54 out of 102 (52.9%) lung cancers by using PCR for the L1 and E7 genes and by genotyping by INNO-LiPA [122]. In Iran, Hussen et al. reported an HPV presence in 61 out of 109 (56%) lung cancer tissues by using PCR and RLB [123]. In China, Wu et al. (2021) detected the presence of HPV DNA in 16 out of 100 (16%) patients with NSCLC by using RT-qPCR [124]. In Shenyang, Republic of China, Zou et al. (2021) found HPV in 183 out of 310 (59%) lung carcinomas by using qPCR. Furthermore, the expression levels of E6 mRNA and E7 mRNA in the SCLC group were significantly higher than those in benign cell group [125]. In Taiwan, Huang et al. (2022) reported an HPV incidence rate of 39.44 (37.47–41.52) (crude incidence rate, per 100,000 people per year) in lung cancer patients. Furthermore, it was concluded that an HPV infection was associated with the occurrence of adenocarcinoma of the lungs in both men and women (1.714; 1.572–1.870) [126].
After 2010, new studies were reported in America. In Mexico, Badillo-Almaraz et al. (2013) reported an HPV presence in 16 out of 39 (41%) lung cancer tissues by using PCR [127]. In USA, Joh et al., (2010) reported an HPV presence in five out of thirty (16.7%) lung carcinomas by using PCR and DNA sequencing. Only HPV16 and HPV11 were identified [8]. In the same country, Koshiol et al. (2011) reported no HPV presence in 399 lung carcinomas by using RT-qPCR [128]. In Canada, Yanagawa et al., 2013, reported HPV incidences in five out of three hundred and thirty-six (1.5%) lung cancers by using ISH and PCR [129], while Chang et al. (2015) reported negative results in 196 lung cancer samples by conducting ISH, an HR-HPV E6/E7 RNA detection and p16 IHC [130]. In the USA, Colombara et al. (2015) evaluated the HPV antibodies in 200 lung cancer cases and matched them to the controls. There was no evidence for a positive association between an HPV16 or 18 infection and the incidence of lung cancer [131]. In Brazil, de Oliveira et al. (2018) found HPV in 33 out of 63 (52%) lung carcinomas by using PCR, genotyping and IHC for E6 and E7. HPV16 was present in 27 out of 33 (81%) cases, and HPV18 was present in six out of thirty-three (19%) cases [132], while Silva et al. (2019) did not find HPV in 77 NSCLC patients by using PCR [133]. Table 1 shows the frequency of HPV detection worldwide since 1972.
4. HR-HPV-Mediated Lung Carcinogenesis: Potential Mechanisms
It has been suggested that both the natural and the iatrogenic squamous–columnar junctions (SCJs), which are present in the upper respiratory tree, are the predilected entry site of HPV in this anatomical region [7]. Interestingly, this is in line with a recent meta-analysis which showed that HPV is most frequently detected in lung SQCs than in AdCs worldwide [134]. Despite the molecular mechanisms of HR-HPV-mediated cervical and head and neck carcinogenesis having been widely studied [135], those which may be related to lung cancer are not clear. However, the studies suggest that the HR-HPV genome integration with the subsequent E6 and E7 overexpression are important events [99,136], with a subsequent p53 and pRB downregulation occurring, which in turn results in loss of apoptosis and cell proliferation, respectively [137]. HPV integration into the host genome is a random event that is not part of the normal HPV life cycle and whose mechanisms have not been completely understood. Indeed, the integration sites into the host genome have been mapped in cervical and head and neck cancer [138,139], although according to our knowledge, the studies addressing HPV integration sites in lung cancer are lacking. HPV genome integration can alter the expression levels of the genes near the integration sites. These altered genes in the “hotspots” show diverse roles including angiogenesis, cellular differentiation, migration, invasion, proliferation, and regulation of cell death, among others [140]. Of note, HPV integration is facilitated by repair processes that are activated in the cells with chromosomal instability, which is a hallmark of human cancer [141,142]. The “looping” model of HPV integration is the most accepted one. In this model, HPV integration is mediated by DNA replication and recombination, resulting in DNA concatemers, such as those which occur in SiHa and CasKi cervical cancer cells [143,144].
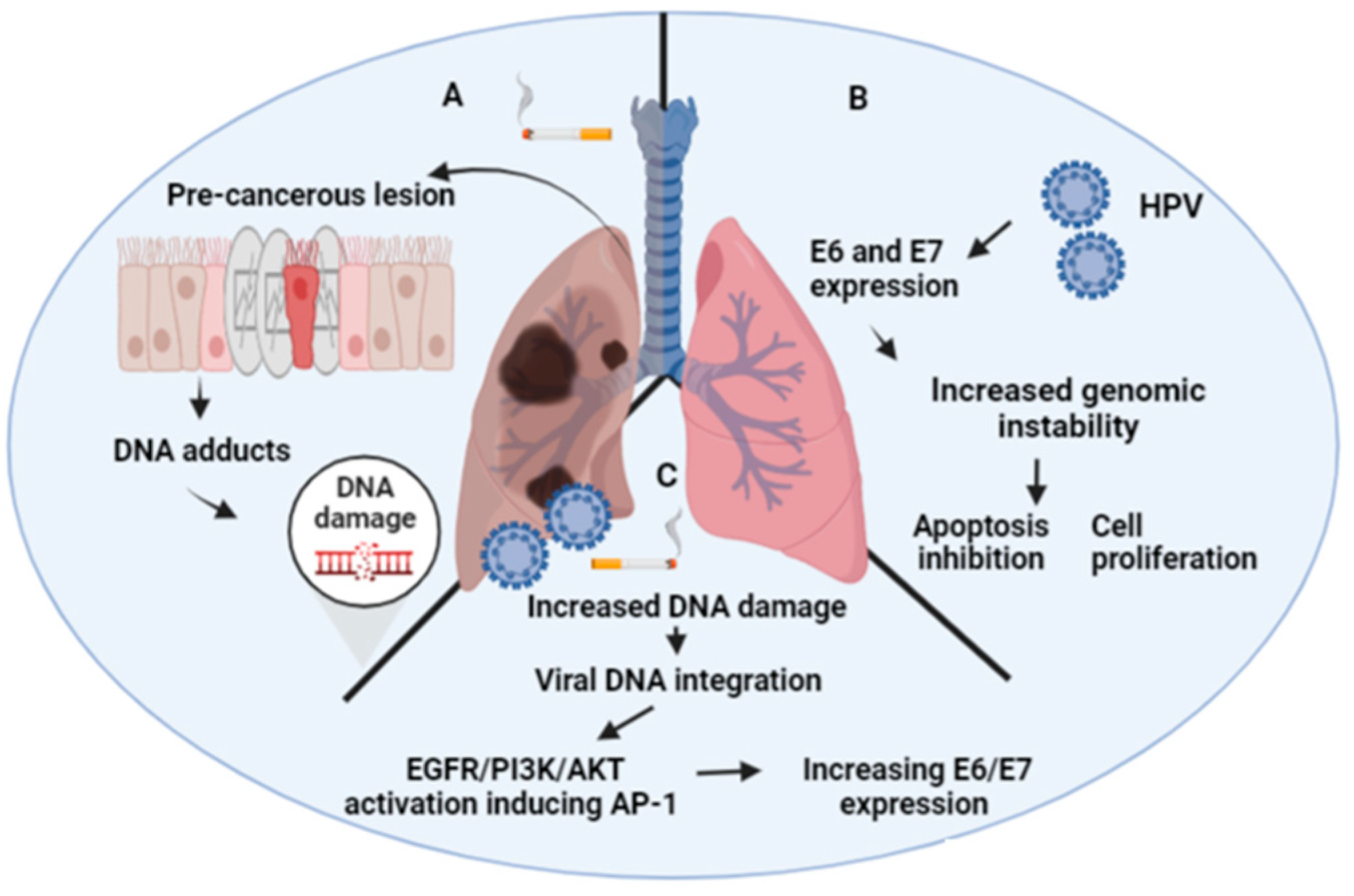
Tobacco smoke is the most important carcinogen involved in lung carcinogenesis worldwide [3]. In this context, the role of HPV needs to be clarified (Figure 1). Some groups in Asia have suggested that HPV works as a carcinogen in non-smoker subjects (Figure 1) [145]. Regarding these data, the signaling pathways have been characterized, and the potential biomarkers have been suggested. For instance, a frequent HR-HPV presence has been found in non-smoker, Taiwanese female lung cancers. Additionally, a significant increase in CDKN2A (p16) promoter hypermethylation was found in this group when it was compared to the non-smoker male lung cancers, suggesting that HR-HPV is potentially involved in this epigenetic alteration. Consecutively, it was demonstrated that this effect may be linked with the expression of the DNA methyltransferase 3b (DNMT3b) protein. Interestingly, it has been described an important role for the E6 oncoprotein in lung cancer. Indeed, E6 expression in lung tumors have shown to be associated with the tissue inhibitor of metalloproteinase 3 (TIMP-3) loss by promoter hypermethylation, thus inducing interleukin 6 production (IL-6). In addition, the expression of PD-L1 by the E6 oncoprotein through the ERK-C/EBPβ-TLR4-NF-κB signaling pathway promotes tumor growth and the invasiveness of lung carcinomas [146]. Of note, E6 can promote a reduction of microRNA-184, conferring cisplatin resistance in lung cancer via increasing Bcl-2 [147]. The same effect is promoted through cIAP2 upregulation via the EGFR/PI3K/AKT pathway by E6 in HPV16/18-positive lung cancer subjects [148]. Moreover, the induction of FOXM1 by the E6 oncoprotein through the MZF1/NKX2-1 axis may be involved in HR-HPV-mediated lung cancer progression and poor outcomes in HPV-positive patients [149]. An additional effect of E6, but not of E7, is to inhibit the antitumor activity of LKB1, a serine-threonine protein kinase, in lung cancer cells by downregulating the expression of kinesin family member 7 (KIF7) [150].
Cheng YW et al. showed that the HPV E6-induced promoter hypermethylation of the XRCC3 and XRCC5 DNA repair genes promoted increased benzopyrene (B[a]P)-induced DNA adducts, in turn, contributing to lung tumorigenesis. B[a]P is a polycyclic aromatic hydrocarbon (PAH) that is a recognized as a class I carcinogen that is present in tobacco, industrial exhaust, and environmental contamination. Additionally, arsenic [151], radon [152] and others environmental factors are etiologically related to lung cancer. For instance, it is known that tobacco smoking and second-hand smoke are etiologically related to 70–90% of lung cancer cases worldwide, though this percentage varies depending on the histological type and the sociodemographic factors that are involved [153,154]. In fact, tobacco smoke is a class I carcinogen whose oncogenic mechanisms and involved signaling pathways have been extensively understood in the past years [155]. Whether environmental compounds such as tobacco smoke can cooperate with HR-HPV for lung tumorigenesis is a controversial topic. Interestingly, smoker women who are infected with HR-HPV are more susceptible to cervical cancer when they are compared to non-smokers [156]. However, such a relationship has not been established in lung or head and neck cancers. Our group addressed a potential cooperation between HR-HPV and the cigarette smoke components in the models of lung epithelial cells. Additionally, we previously proposed the possibility that HR-HPV can cooperate with tobacco smoke for lung carcinogenesis using in vitro approaches. Muñoz et al. suggested that tobacco smoke increases the tumorigenic properties of E6/E7-expressing lung cells [157]. Additionally, our team demonstrated that tobacco smoke can activate the HPV16 early (p97) promoter in the lung epithelial cells, thus increasing the levels of the E6 and E7 oncoproteins. These oncoproteins can cooperate with tobacco smoke to increase the DNA damage in the lung epithelial cells [158]. In addition, other studies have established the molecular mechanisms of cooperation between HPV and tobacco in different cell contexts. In fact, Wei et al. reported that tobacco smoke extracts increase the E6/E7 levels only when the virus is found in an episomal state in the cervical cells, suggesting that tobacco smoke affects the HPV gene expression only in preneoplastic lesions before cancer development [159]. Local immunosuppressive effects, leading to the persistence of an HPV infection has been suggested [160,161,162]. Molecular alterations in HPV-associated lung cancers are summarized in Figure 2.
Importantly, the viral load in lung tumors can shed light in respect to its role in this malignancy. Indeed, the very low viral load in lung carcinomas (less than 1 copy/cell) suggest the possibility that HPV is a mere bystander in the clinical samples. However, we cannot deny the possibility of a “hit and run” mechanism, by which the viral infection is involved in the initial events in carcinogenesis, and then the virus is cleared as it is no longer required for the cancer progression. Indeed, previous evidence shows that HPV can work by this “hit and run” mechanism [163,164,165]. Future research that is focused on lung preneoplastic lesions can elucidate this possibility.
5. Conclusions
An etiological role of HR-HPV in a subset of lung cancers including both AdCs and SQCs is plausible. However, there is a high variability in HPV detection rates among different countries, and moreover, in the same countries (from 0 to 100%). Probably, the factors related to the differential sensitivity among the detection methods can account for these differences because we lack a gold standard method for HPV detection in human tissues. Additionally, ethnic, lifestyle and sociodemographic factors can be involved in explaining such differences. The molecular mechanisms by which HPV promotes lung cancer are not fully known. As in cervical cancer, HR-HPV E6/E7 overexpression by HPV genome integration is an important event, though the completion of additional studies is necessary to address the consequences of such events for lung epithelial cell transformation. Thus, the analysis of some viral parameters such as the HPV copy number and the viral physical status in the lung clinical specimens is warranted in future studies. Because a “hit and run” mechanism cannot be denied, studies including the preneoplastic lesions of lung cancer will be valuable for the further characterization of this virus in this malignancy. As an HR-HPV infection is not a sufficient condition for carcinogenesis, the role of additional co-factors such as xenobiotics, including environmental factors (tobacco, arsenic, pollution, etc.) which can potentially cooperate with HPV for lung tumorigenesis remains an interesting point for future research.
Author Contributions
Conceptualization, J.C.O. and F.A.; writing—original draft preparation, J.C.O. and F.A.; writing—review and editing, J.C.O., F.A., F.C.-E., A.H.C. and G.M.C.; supervision, F.A. All authors have read and agreed to the published version of the manuscript.
Funding
Fondecyt # 1221033 (F.A.); Fondecyt # 1200656 (G.M.C.); Fondecyt Postdoctoral Grant # 3220486 (J.C.O.); Conicyt-Fondap # 15130011 (A.H.C.).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sharma, R. Mapping of global, regional and national incidence, mortality and mortality-to-incidence ratio of lung cancer in 2020 and 2050. Int. J. Clin. Oncol. 2022, 27, 665–675. [Google Scholar] [CrossRef]
- Mbemi, A.; Khanna, S.; Njiki, S.; Yedjou, C.; Tchounwou, P. Impact of Gene–Environment Interactions on Cancer Development. Int. J. Environ. Res. Public Health 2020, 17, 8089. [Google Scholar] [CrossRef]
- Levin, M.L.; Goldstein, H.; Gerhardt, P.R. Cancer and tobacco smoking; a preliminary report. J. Am. Med. Assoc. 1950, 143, 336–338. [Google Scholar] [CrossRef]
- Rudin, C.M.; Brambilla, E.; Faivre-Finn, C.; Sage, J. Small-cell lung cancer. Nat. Rev. Dis. Prim. 2021, 7, 3. [Google Scholar] [CrossRef]
- Stovold, R.; Blackhall, F.; Meredith, S.; Hou, J.; Dive, C.; White, A. Biomarkers for small cell lung cancer: Neuroendocrine, epithelial and circulating tumour cells. Lung Cancer 2012, 76, 263–268. [Google Scholar] [CrossRef]
- Molina, J.R.; Yang, P.; Cassivi, S.D.; Schild, S.E.; Adjei, A.A. Non-Small Cell Lung Cancer: Epidemiology, Risk Factors, Treatment, and Survivorship. Mayo Clin. Proc. 2008, 83, 584–594. [Google Scholar] [CrossRef]
- Syrjänen, K.J. HPV infections and lung cancer. J. Clin. Pathol. 2002, 55, 885–891. [Google Scholar] [CrossRef] [Green Version]
- Joh, J.; Jenson, A.B.; Moore, G.D.; Rezazedeh, A.; Slone, S.P.; Ghim, S.-J.; Kloecker, G.H. Human papillomavirus (HPV) and Merkel cell polyomavirus (MCPyV) in non small cell lung cancer. Exp. Mol. Pathol. 2010, 89, 222–226. [Google Scholar] [CrossRef]
- Palmarini, M.; Sharp, J.M.; Heras, M.D.L.; Fan, H. Jaagsiekte Sheep Retrovirus Is Necessary and Sufficient To Induce a Contagious Lung Cancer in Sheep. J. Virol. 1999, 73, 6964–6972. [Google Scholar] [CrossRef] [Green Version]
- Zheng, H.; Aziz, H.A.; Nakanishi, Y.; Masuda, S.; Saito, H.; Tsuneyama, K.; Takano, Y. Oncogenic role of JC virus in lung cancer. J. Pathol. 2007, 212, 306–315. [Google Scholar] [CrossRef]
- Becnel, D.; Abdelghani, R.; Nanbo, A.; Avilala, J.; Kahn, J.; Li, L.; Lin, Z. Pathogenic Role of Epstein–Barr Virus in Lung Cancers. Viruses 2021, 13, 877. [Google Scholar] [CrossRef]
- Gheit, T. Mucosal and Cutaneous Human Papillomavirus Infections and Cancer Biology. Front. Oncol. 2019, 9, 355. [Google Scholar] [CrossRef] [Green Version]
- Bzhalava, D.; Guan, P.; Franceschi, S.; Dillner, J.; Clifford, G. A systematic review of the prevalence of mucosal and cutaneous human papillomavirus types. Virology 2013, 445, 224–231. [Google Scholar] [CrossRef] [Green Version]
- Graham, S.V. The human papillomavirus replication cycle, and its links to cancer progression: A comprehensive review. Clin. Sci. 2017, 131, 2201–2221. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, E.; Freese, U.K.; Gissmann, L.; Mayer, W.; Roggenbuck, B.; Stremlau, A.; Hausen, H.Z. Structure and transcription of human papillomavirus sequences in cervical carcinoma cells. Nature 1985, 314, 111–114. [Google Scholar] [CrossRef]
- Zheng, Z.-M. Papillomavirus genome structure, expression, and post-transcriptional regulation. Front. Biosci. 2006, 11, 2286–2302. [Google Scholar] [CrossRef] [Green Version]
- Graham, S.V. Human papillomavirus: Gene expression, regulation and prospects for novel diagnostic methods and antiviral therapies. Futur. Microbiol. 2010, 5, 1493–1506. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, A.L.; Caodaglio, A.S.; Sichero, L. Regulation of HPV transcription. Clinics 2018, 73, e486s. [Google Scholar] [CrossRef]
- Bletsa, G.; Zagouri, F.; Amoutzias, G.D.; Nikolaidis, M.; Zografos, E.; Markoulatos, P.; Tsakogiannis, D. Genetic variability of the HPV16 early genes and LCR. Present and future perspectives. Expert Rev. Mol. Med. 2021, 23, e19. [Google Scholar] [CrossRef]
- López-Saavedra, A.; González-Maya, L.; Ponce-De-León, S.; García-Carrancá, A.; Mohar, A.; Lizano, M. Functional implication of sequence variation in the long control region and E2 gene among human papillomavirus type 18 variants. Arch. Virol. 2009, 154, 747–754. [Google Scholar] [CrossRef]
- Warowicka, A.; Broniarczyk, J.; Węglewska, M.; Kwaśniewski, W.; Goździcka-Józefiak, A. Dual Role of YY1 in HPV Life Cycle and Cervical Cancer Development. Int. J. Mol. Sci. 2022, 23, 3453. [Google Scholar] [CrossRef] [PubMed]
- Doorbar, J.; Egawa, N.; Griffin, H.; Kranjec, C.; Murakami, I. Human papillomavirus molecular biology and disease association. Rev. Med. Virol. 2015, 25 (Suppl. 1), 2–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stubenrauch, F.; Colbert, A.M.E.; Laimins, L.A. Transactivation by the E2 Protein of Oncogenic Human Papillomavirus Type 31 Is Not Essential for Early and Late Viral Functions. J. Virol. 1998, 72, 8115–8123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishimura, A.; Ono, T.; Ishimoto, A.; Dowhanick, J.J.; Frizzell, M.A.; Howley, P.; Sakai, H. Mechanisms of Human Papillomavirus E2-Mediated Repression of Viral Oncogene Expression and Cervical Cancer Cell Growth Inhibition. J. Virol. 2000, 74, 3752–3760. [Google Scholar] [CrossRef] [Green Version]
- Hughes, F.J.; Romanos, M.A. E1 protein of human papillomavirus is a DNA helicase/ATPase. Nucleic Acids Res. 1993, 21, 5817–5823. [Google Scholar] [CrossRef] [Green Version]
- DeSmet, M.; Kanginakudru, S.; Rietz, A.; Wu, W.-H.; Roden, R.; Androphy, E.J. The Replicative Consequences of Papillomavirus E2 Protein Binding to the Origin Replication Factor ORC2. PLoS Pathog. 2016, 12, e1005934. [Google Scholar] [CrossRef] [Green Version]
- Sekhar, V.; McBride, A.A. Phosphorylation Regulates Binding of the Human Papillomavirus Type 8 E2 Protein to Host Chromosomes. J. Virol. 2012, 86, 10047–10058. [Google Scholar] [CrossRef] [Green Version]
- Doorbar, J. The E4 protein; structure, function and patterns of expression. Virology 2013, 445, 80–98. [Google Scholar] [CrossRef] [Green Version]
- DiMaio, D.; Petti, L.M. The E5 proteins. Virology 2013, 445, 99–114. [Google Scholar] [CrossRef]
- Venuti, A.; Paolini, F.; Nasir, L.; Corteggio, A.; Roperto, S.; Campo, M.S.; Borzacchiello, G. Papillomavirus E5: The smallest oncoprotein with many functions. Mol. Cancer 2011, 10, 140. [Google Scholar] [CrossRef]
- Kim, S.-H.; Juhnn, Y.-S.; Kang, S.; Park, S.-W.; Sung, M.-W.; Bang, Y.-J.; Song, Y.-S. Human papillomavirus 16 E5 up-regulates the expression of vascular endothelial growth factor through the activation of epidermal growth factor receptor, MEK/ ERK1,2 and PI3K/Akt. Cell Mol. Life Sci. 2006, 63, 930–938. [Google Scholar] [CrossRef] [PubMed]
- Ashrafi, G.H.; Haghshenas, M.R.; Marchetti, B.; O’Brien, P.M.; Campo, M.S. E5 protein of human papillomavirus type 16 selectively downregulates surface HLA class I. Int. J. Cancer 2004, 113, 276–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yugawa, T.; Kiyono, T. Molecular mechanisms of cervical carcinogenesis by high-risk human papillomaviruses: Novel functions of E6 and E7 oncoproteins. Rev. Med. Virol. 2009, 19, 97–113. [Google Scholar] [CrossRef] [PubMed]
- Melsheimer, P.; Vinokurova, S.; Wentzensen, N.; Bastert, G.; Doeberitz, M.V.K. DNA Aneuploidy and Integration of Human Papillomavirus Type 16 E6/E7 Oncogenes in Intraepithelial Neoplasia and Invasive Squamous Cell Carcinoma of the Cervix Uteri. Clin. Cancer Res. 2004, 10, 3059–3063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malecka, K.A.; Fera, D.; Schultz, D.C.; Hodawadekar, S.; Reichman, M.; Donover, P.S.; Murphy, M.E.; Marmorstein, R. Identification and Characterization of Small Molecule Human Papillomavirus E6 Inhibitors. ACS Chem. Biol. 2014, 9, 1603–1612. [Google Scholar] [CrossRef]
- Veldman, T.; Liu, X.; Yuan, H.; Schlegel, R. Human papillomavirus E6 and Myc proteins associate in vivo and bind to and cooperatively activate the telomerase reverse transcriptase promoter. Proc. Natl. Acad. Sci. USA 2003, 100, 8211–8216. [Google Scholar] [CrossRef] [Green Version]
- Scheffner, M.; Whitaker, N.J. Human papillomavirus-induced carcinogenesis and the ubiquitin–proteasome system. Semin. Cancer Biol. 2003, 13, 59–67. [Google Scholar] [CrossRef]
- Martin, L.G.; Demers, G.W.; Galloway, D.A. Disruption of the G 1 /S Transition in Human Papillomavirus Type 16 E7-Expressing Human Cells Is Associated with Altered Regulation of Cyclin E. J. Virol. 1998, 72, 975–985. [Google Scholar] [CrossRef] [Green Version]
- Zerfass, K.; Schulze, A.; Spitkovsky, D.; Friedman, V.; Henglein, B.; Jansen-Dürr, P. Sequential activation of cyclin E and cyclin A gene expression by human papillomavirus type 16 E7 through sequences necessary for transformation. J. Virol. 1995, 69, 6389–6399. [Google Scholar] [CrossRef] [Green Version]
- Narisawa-Saito, M.; Kiyono, T. Basic mechanisms of high-risk human papillomavirus-induced carcinogenesis: Roles of E6 and E7 proteins. Cancer Sci. 2007, 98, 1505–1511. [Google Scholar] [CrossRef]
- Gupta, S.; Kumar, P.; Das, B.C. HPV: Molecular pathways and targets. Curr. Probl. Cancer 2018, 42, 161–174. [Google Scholar] [CrossRef] [PubMed]
- Doorbar, J.; Griffin, H. Refining our understanding of cervical neoplasia and its cellular origins. Papillomavirus Res. 2019, 7, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Beutner, K.R.; Tyring, S. Human Papillomavirus and Human Disease. Am. J. Med. 1997, 102, 9–15. [Google Scholar] [CrossRef]
- Cubie, H.A. Diseases associated with human papillomavirus infection. Virology 2013, 445, 21–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafti-Keramat, S.; Handisurya, A.; Kriehuber, E.; Meneguzzi, G.; Slupetzky, K.; Kirnbauer, R. Different Heparan Sulfate Proteoglycans Serve asCellular Receptors for HumanPapillomaviruses. J. Virol. 2003, 77, 13125–13135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, R.M.; Lowy, D.R.; Schiller, J.T.; Day, P.M. Cleavage of the papillomavirus minor capsid protein, L2, at a furin consensus site is necessary for infection. Proc. Natl. Acad. Sci. USA 2006, 103, 1522–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spoden, G.; Freitag, K.; Husmann, M.; Boller, K.; Sapp, M.; Lambert, C.; Florin, L. Clathrin- and Caveolin-Independent Entry of Human Papillomavirus Type 16—Involvement of Tetraspanin-Enriched Microdomains (TEMs). PLoS ONE 2008, 3, e3313. [Google Scholar] [CrossRef] [Green Version]
- DiGiuseppe, S.; Bienkowska-Haba, M.; Guion, L.G.M.; Keiffer, T.R.; Sapp, M. Human Papillomavirus Major Capsid Protein L1 Remains Associated with the Incoming Viral Genome throughout the Entry Process. J. Virol. 2017, 91. [Google Scholar] [CrossRef] [Green Version]
- Yang, R.; Iv, W.H.Y.; Viscidi, R.P.; Roden, R.B.S. Interaction of L2 with ॆ-Actin Directs Intracellular Transport of Papillomavirus and Infection. J. Biol. Chem. 2003, 278, 12546–12553. [Google Scholar] [CrossRef] [Green Version]
- Pyeon, D.; Pearce, S.M.; Lank, S.M.; Ahlquist, P.; Lambert, P.F. Establishment of Human Papillomavirus Infection Requires Cell Cycle Progression. PLOS Pathog. 2009, 5, e1000318. [Google Scholar] [CrossRef]
- Fisher, C. Recent Insights into the Control of Human Papillomavirus (HPV) Genome Stability, Loss, and Degradation. J. Clin. Med. 2015, 4, 204–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Liu, H.; Ge, H.; Ajiro, M.; Sharma, N.R.; Meyers, C.; Morozov, P.; Tuschl, T.; Klar, A.; Court, D.; et al. Viral DNA Replication Orientation and hnRNPs Regulate Transcription of the Human Papillomavirus 18 Late Promoter. mBio 2017, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longworth, M.S.; Laimins, L.A. Pathogenesis of Human Papillomaviruses in Differentiating Epithelia. Microbiol. Mol. Biol. Rev. 2004, 68, 362–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mole, S.; Faizo, A.; Hernandez-Lopez, H.; Griffiths, M.; Stevenson, A.; Roberts, S.; Graham, S.V. Human papillomavirus type 16 infection activates the host serine arginine protein kinase 1 (SRPK1)—Splicing factor axis. J. Gen. Virol. 2020, 101, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, N.; Castellsagué, X.; de González, A.B.; Gissmann, L. Chapter 1: HPV in the etiology of human cancer. Vaccine 2006, 24 (Suppl. 3), S1–S10. [Google Scholar] [CrossRef]
- Johansson, C.; Somberg, M.; Li, X.; Winquist, E.B.; Fay, J.; Ryan, F.; Pim, D.; Banks, L.; Schwartz, S. HPV-16 E2 contributes to induction of HPV-16 late gene expression by inhibiting early polyadenylation. EMBO J. 2012, 31, 3212–3227. [Google Scholar] [CrossRef]
- Ault, K.A. Epidemiology and Natural History of Human Papillomavirus Infections in the Female Genital Tract. Infect. Dis. Obstet. Gynecol. 2006, 2006, 40470. [Google Scholar] [CrossRef]
- Park, T.W.; Fujiwara, H.; Wright, T.C. Molecular biology of cervical cancer and its precursors. Cancer 1995, 76, 1902–1913. [Google Scholar] [CrossRef]
- Duensing, S.; Münger, K. Mechanisms of genomic instability in human cancer: Insights from studies with human papillomavirus oncoproteins. Int. J. Cancer 2003, 109, 157–162. [Google Scholar] [CrossRef]
- Doorbar, J. Molecular biology of human papillomavirus infection and cervical cancer. Clin. Sci. 2006, 110, 525–541. [Google Scholar] [CrossRef]
- Syrjänen, K.J. Condylomatous Changes in Neoplastic Bronchial Epithelium. Report of a case. Respiration 1979, 38, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Syrjänen, K.J. Epithelial Lesions Suggestive of a Condylomatous Origin Found Closely Associated with Invasive Bronchial Squamous Cell Carcinomas. Respiration 1980, 40, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Stremlau, A.; Gissmann, L.; Ikenberg, H.; Stark, M.; Bannasch, P.; Hausen, H.Z. Human papillomavirus type 16 related DNA in an anaplastic carcinoma of the lung. Cancer 1985, 55, 1737–1740. [Google Scholar] [CrossRef]
- Syrjänen, K.; Syrjänen, S.; Kellokoski, J.; Kärjä, J.; Mäntyjärvi, R. Human papillomavirus (HPV) type 6 and 16 DNA sequences in bronchial squamous cell carcinomas demonstrated by in situ DNA hybridization. Lung 1989, 167, 33–42. [Google Scholar] [CrossRef]
- Béjui-Thivolet, F.; Liagre, N.; Chignol, M.C.; Chardonnet, Y.; Patricot, L.M. Detection of human papillomavirus DNA in squamous bronchial metaplasia and squamous cell carcinomas of the lung by in situ hybridization using biotinylated probes in paraffin-embedded specimens. Hum. Pathol. 1990, 21, 111–116. [Google Scholar] [CrossRef]
- Thomas, P.; De Lamballerie, X.; Garbe, L.; Douagui, H.; Kleisbauer, J.P. Detection of human papillomavirus DNA in primary lung carcinoma by nested polymerase chain reaction. Cell. Mol. Biol. 1995, 41, 1093–1097. [Google Scholar]
- Noutsou, A.; Koffa, M.; Ergazaki, M.; Siafakas, N.; Spandidos, D. Detection of human papilloma virus (HPV) and K-ras mutations in human lung carcinomas. Int. J. Oncol. 1996, 8, 1089–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welt, A.; Hummel, M.; Niedobitek, G.; Stein, H. Human papillomavirus infection is not associated with bronchial carcinoma: Evaluation by in situ hybridization and the polymerase chain reaction. J. Pathol. 1997, 181, 276–280. [Google Scholar] [CrossRef]
- Papadopoulou, K.; Labropoulou, V.; Davaris, P.; Mavromara, P.; Tsimara-Papastamatiou, H. Detection of human papillomaviruses in squamous cell carcinomas of the lung. Virchows Arch. 1998, 433, 49–54. [Google Scholar] [CrossRef]
- Gorgoulis, V.G.; Zacharatos, P.; Kotsinas, A.; Kyroudi, A.; Rassidakis, A.N.; A Ikonomopoulos, J.; Barbatis, C.; Herrington, C.S.; Kittas, C. Human papilloma virus (HPV) is possibly involved in laryngeal but not in lung carcinogenesis. Hum. Pathol. 1999, 30, 274–283. [Google Scholar] [CrossRef]
- Hennig, E.M.; Suo, Z.; Karlsen, F.; Holm, R.; Thoresen, S.; Nesland, J.M. HPV positive bronchopulmonary carcinomas in women with previous high-grade cervical intraepithelial neoplasia (CIN III). Acta Oncol. 1999, 38, 639–648. [Google Scholar] [PubMed]
- Xing, L.Q.; Liu, H.R.; Si, J.Y. Detection of human papillomavirus DNA in squamous cell carcinomas of the lung by multiple polymerase chain reaction. Zhonghua jie he he hu xi za zhi = Zhonghua jiehe he huxi zazhi = Chin. J. Tuberc. Respir. Dis. 1993, 16, 275–277, 319. [Google Scholar]
- Szabó, I.; Sepp, R.; Nakamoto, K.; Maeda, M.; Sakamoto, H.; Uda, H. Human papillomavirus not found in squamous and large cell lung carcinomas by polymerase chain reaction. Cancer 1994, 73, 2740–2744. [Google Scholar] [CrossRef]
- Tsuhako, K.; Nakazato, I.; Hirayasu, T.; Sunakawa, H.; Iwamasa, T. Human papillomavirus DNA in adenosquamous carcinoma of the lung. J. Clin. Pathol. 1998, 51, 741–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.R.; Xing, L.Q.; Si, J.Y. A study of human papillary virus infection by in situ hybridization and histopathology in squamous cell carcinoma of the lung. Zhonghua bing li xue za zhi = Chin. J. Pathol. 1994, 23, 299–301. [Google Scholar]
- Hu, K.; Li, Q.; Yang, J.; Hu, S. Detection of human papillomavirus types 16, 18 DNA related sequences in bronchogenic carcinoma. Zhonghua Shi Yan He Lin Chuang Bing Du Xue Za Zhi 1997, 11, 147–149. [Google Scholar]
- Yousem, S.A.; Ohori, N.P.; Sonmez-Alpan, E. Occurrence of Human Papillomavirus DNA in Primary Lung Neoplasms. Cancer 1992, 69, 693–697. [Google Scholar] [CrossRef]
- Bohlmeyer, T.; Le, T.N.; Shroyer, A.L.; Markham, N.; Shroyer, K.R. Detection of Human Papillomavirus in Squamous Cell Carcinomas of the Lung by Polymerase Chain Reaction. Am. J. Respir. Cell Mol. Biol. 1998, 18, 265–269. [Google Scholar] [CrossRef]
- Clavel, C.E.; Nawrocki, B.; Bosseaux, B.; Poitevin, G.; Putaud, I.C.; Mangeonjean, C.C.; Monteau, M.; Birembaut, P.L. Detection of human papillomavirus DNA in bronchopulmonary carcinomas by hybrid capture II: A study of 185 tumors. Cancer 2000, 88, 1347–1352. [Google Scholar] [CrossRef]
- Miąsko, A.; Niklińska, W.; Nikliński, J.; Chyczewska, E.; Naumnik, W.; Chyczewski, L. Detection of human papillomavirus in non-small cell lung carcinoma by polymerase chain reaction. Folia Histochem. Cytobiol. 2001, 39, 127–128. [Google Scholar]
- Kaya, H.; Kotiloğlu, E.; Inanli, S.; Ekicioğlu, G.; Bozkurt, S.U.; Tutkun, A.; Küllü, S. Prevalence of human papillomavirus (HPV) DNA in larynx and lung carcinomas. Pathologica 2001, 93, 531–534. [Google Scholar] [PubMed]
- Zafer, E.; Ergun, M.A.; Alver, G.; Sahin, F.I.; Yavuzer, S.; Ekmekci, A. Detection and Typing of Human Papillomavirus in Non-Small Cell Lung Cancer. Respiration 2004, 71, 88–90. [Google Scholar] [CrossRef] [PubMed]
- Brouchet, L.; Valmary, S.; Dahan, M.; Didier, A.; Galateau-Salle, F.; Brousset, P.; Degano, B. Detection of oncogenic virus genomes and gene products in lung carcinoma. Br. J. Cancer 2005, 92, 743–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coissard, C.J.; Besson, G.; Polette, M.C.; Monteau, M.; Birembaut, P.L.; Clavel, C.E. Prevalence of human papillomaviruses in lung carcinomas: A study of 218 cases. Mod. Pathol. 2005, 18, 1606–1609. [Google Scholar] [CrossRef] [Green Version]
- Ciotti, M.; Giuliani, L.; Ambrogi, V.; Ronci, C.; Benedetto, A.; Mineo, T.C.; Syrjänen, K.; Favalli, C. Detection and expression of human papillomavirus oncogenes in non-small cell lung cancer. Oncol. Rep. 2006, 16, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, L.; Jaxmar, T.; Casadio, C.; Gariglio, M.; Manna, A.; D’Antonio, D.; Syrjanen, K.; Favalli, C.; Ciotti, M. Detection of oncogenic viruses (SV40, BKV, JCV, HCMV, HPV) and p53 codon 72 polymorphism in lung carcinoma. Lung Cancer 2007, 57, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.W.; Chiou, H.L.; Sheu, G.T.; Hsieh, L.L.; Chen, J.T.; Chen, C.Y.; Su, J.M.; Lee, H. The association of human papillomavirus 16/18 infection with lung cancer among nonsmoking Taiwanese women. Cancer Res. 2001, 61, 2799–2803. [Google Scholar]
- Hsu, N.Y.; Cheng, Y.W.; Chan, I.P.; Ho, H.C.; Chen, C.Y.; Hsu, C.P.; Lin, M.H.; Chou, M.C. Association between expression of human papillomavirus 16/18 E6 oncoprotein and survival in patients with stage I non-small cell lung cancer. Oncol. Rep. 2009, 21, 81–87. [Google Scholar]
- Yu, Y.; Yang, A.; Hu, S.; Yan, H. Correlation of HPV-16/18 infection of human papillomavirus with lung squamous cell carcinomas in Western China. Oncol. Rep. 2009, 21, 1627–1632. [Google Scholar]
- Xu, Y.; Cheng, B.; Pan, H.; Wu, A.; Zhang, L. The Relationship between the Status of Human Papillomavirus 16/18 Infection and the Expression of Bcl-2 and Bax in Squamous Cell Carcinomas of the Lung. Zhongguo Fei Ai Za Zhi 2009, 12, 849–852. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, T.; Han, M.; Yang, Z.H.; Liu, L.X.; Chen, Y.; Zhang, L.; Hu, H.Z.; Xi, M.R. Variation of human papillomavirus 16 in cervical and lung cancers in Sichuan, China. Acta Virol. 2010, 54, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Fei, Y.; Yang, J.; Hsieh, W.-C.; Wu, J.-Y.; Wu, T.-C.; Goan, Y.-G.; Lee, H.; Cheng, Y.-W. Different Human Papillomavirus 16/18 Infection in Chinese Non-Small Cell Lung Cancer Patients Living in Wuhan, China. Jpn. J. Clin. Oncol. 2006, 36, 274–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, C.; Wang, Y.; Wang, A.; Jiang, R.; Pan, H.; Huang, B.; Lu, Y. Human papillomavirus type 16 and 18 infection is associated with lung cancer patients from the central part of China. Oncol. Rep. 1994, 20, 333–339. [Google Scholar] [CrossRef] [Green Version]
- Miyagi, J.; Tsuhako, K.; Kinjo, T.; Iwamasa, T.; Hirayasu, T. Recent striking changes in histological differentiation and rate of human papillomavirus infection in squamous cell carcinoma of the lung in Okinawa, a subtropical island in southern Japan. J. Clin. Pathol. 2000, 53, 676–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, M.S.; Chang, Y.S.; Shin, J.H.; Kim, D.J.; Chung, K.Y.; Shin, D.H.; Moon, J.W.; Kang, S.M.; Hahn, C.H.; Kim, Y.S.; et al. The Prevalence of Human Papillomavirus Infection in Korean Non-Small Cell Lung Cancer Patients. Yonsei Med. J. 2007, 48, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nadji, S.A.; Mokhtari-Azad, T.; Mahmoodi, M.; Yahyapour, Y.; Naghshvar, F.; Torabizadeh, J.; Ziaee, A.A.; Nategh, R. Relationship between lung cancer and human papillomavirus in north of Iran, Mazandaran province. Cancer Lett. 2007, 248, 41–46. [Google Scholar] [CrossRef]
- Lim, W.-T.; Chuah, K.L.; Leong, S.S.; Tan, E.H.; Toh, C.K. Assessment of human papillomavirus and Epstein-Barr virus in lung adenocarcinoma. Oncol. Rep. 2009, 21, 971–975. [Google Scholar] [CrossRef] [Green Version]
- Castillo, A.; Aguayo, F.; Koriyama, C.; Shuyama, K.; Akiba, S.; Herrera-Goepfert, R.; Carrascal, E.; Klinge, G.; Sánchez, J.; Eizuru, Y. Human papillomavirus in lung carcinomas among three Latin American countries. Oncol. Rep. 2006, 15, 883–888. [Google Scholar] [CrossRef]
- Aguayo, F.; Castillo, A.; Koriyama, C.; Higashi, M.; Itoh, T.; Capetillo, M.; Shuyama, K.; Corvalan, A.; Eizuru, Y.; Akiba, S. Human papillomavirus-16 is integrated in lung carcinomas: A study in Chile. Br. J. Cancer 2007, 97, 85–91. [Google Scholar] [CrossRef]
- Branica, B.V.; Smojver-Jezek, S.; Juros, Z.; Grgić, S.; Srpak, N.; Mitrecić, D.; Gajović, S. Detection of human papillomaviruses type 16, 18 and 33 in bronchial aspirates of lung carcinoma patients by polymerase chain reaction: A study of 84 cases in Croatia. Coll. Antropol. 2010, 34, 159–162. [Google Scholar]
- Carpagnano, G.E.; Koutelou, A.; Natalicchio, M.I.; Martinelli, D.; Ruggieri, C.; Di Taranto, A.; Antonetti, R.; Carpagnano, F.; Barbaro, M.P.F. HPV in exhaled breath condensate of lung cancer patients. Br. J. Cancer 2011, 105, 1183–1190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Syrjänen, K.; Silvoniemi, M.; Salminen, E.; Vasankari, T.; Syrjänen, S. Detection of human papillomavirus genotypes in bronchial cancer using sensitive multimetrix assay. Anticancer Res. 2012, 32, 625–631. [Google Scholar] [PubMed]
- Galvan, A.; Noci, S.; Taverna, F.; Lombardo, C.; Franceschi, S.; Pastorino, U.; Dragani, T.A. Testing of human papillomavirus in lung cancer and non-tumor lung tissue. BMC Cancer 2012, 12, 512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarchianaki, E.; Derdas, S.P.; Ntaoukakis, M.; Vakonaki, E.; Lagoudaki, E.D.; Lasithiotaki, I.; Sarchianaki, A.; Koutsopoulos, A.; Symvoulakis, E.K.; Spandidos, D.A.; et al. Detection and genotype analysis of human papillomavirus in non-small cell lung cancer patients. Tumor Biol. 2013, 35, 3203–3209. [Google Scholar] [CrossRef] [PubMed]
- Argyri, E.; Tsimplaki, E.; Marketos, C.; Politis, G.; Panotopoulou, E. Investigating the role of human papillomavirus in lung cancer. Papillomavirus Res. 2016, 3, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Shikova, E.; Ivanova, Z.; Alexandrova, D.; Shindov, M.; Lekov, A. Human papillomavirus prevalence in lung carcinomas in Bulgaria. Microbiol. Immunol. 2017, 61, 427–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaworek, H.; Koudelakova, V.; Slavkovsky, R.; Drabek, J.; Hajduch, M. The absence of high-risk human papillomavirus in Czech non-small cell lung cancer cases. Biomed. Pap. 2020, 164, 71–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaussade, H.; Le Marec, F.; Coureau, G.; Leleux, O.; Neau, D.; Lazaro, E.; Amadeo, B.; Duffau, P.; Ferrand, H.; Courtault, C.; et al. Incidence of lung and human papilloma virus-associated malignancies in HIV-infected patients. AIDS 2021, 36, 665–673. [Google Scholar] [CrossRef]
- Sirera, G.; Videla, S.; Saludes, V.; Castellà, E.; Sanz, C.; Ariza, A.; Clotet, B.; Martró, E. Prevalence of HPV-DNA and E6 mRNA in lung cancer of HIV-infected patients. Sci. Rep. 2022, 12, 13196. [Google Scholar] [CrossRef]
- Koriyama, C.; Baba, M.; Castillo, A.; Yanagi, M.; Matsumoto, H.; Natsugoe, S.; Shuyama, K.Y.; Khan, N.; Higashi, M.; Itoh, T.; et al. Human papillomavirus is frequently detected in gefitinib-responsive lung adenocarcinomas. Oncol. Rep. 2010, 23, 1085–1092. [Google Scholar] [CrossRef]
- Iwakawa, R.; Kohno, T.; Enari, M.; Kiyono, T.; Yokota, J. Prevalence of human papillomavirus 16/18/33 infection and p53 mutation in lung adenocarcinoma. Cancer Sci. 2010, 101, 1891–1896. [Google Scholar] [CrossRef] [PubMed]
- Aguayo, F.; Anwar, M.; Koriyama, C.; Castillo, A.; Sun, Q.; Morewaya, J.; Eizuru, Y.; Akiba, S. Human papillomavirus-16 presence and physical status in lung carcinomas from Asia. Infect. Agents Cancer 2010, 5, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goto, A.; Li, C.-P.; Ota, S.; Niki, T.; Ohtsuki, Y.; Kitajima, S.; Yonezawa, S.; Koriyama, C.; Akiba, S.; Uchima, H.; et al. Human papillomavirus infection in lung and esophageal cancers: Analysis of 485 Asian cases. J. Med. Virol. 2011, 83, 1383–1390. [Google Scholar] [CrossRef] [PubMed]
- Jafari, H.; Gharemohammadlou, R.; Fakhrjou, A.; Ebrahimi, A.; Nejati-Koshki, K.; Nadri, M.; Sakhinia, E. Genotyping of Human Papillomavirus and TP53 Mutaions at Exons 5 to 7 in Lung Cancer Patients from Iran. BioImpacts 2013, 3, 135–140. [Google Scholar] [CrossRef]
- Yu, Y.; Yang, A.; Hu, S.; Zhang, J.; Yan, H. Significance of human papillomavirus 16/18 infection in association with p53 mutation in lung carcinomas. Clin. Respir. J. 2012, 7, 27–33. [Google Scholar] [CrossRef]
- Fan, X.; Yu, K.; Wu, J.; Shao, J.; Zhu, L.; Zhang, J. Correlation between squamous cell carcinoma of the lung and human papillomavirus infection and the relationship to expression of p53 and p16. Tumor Biol. 2014, 36, 3043–3049. [Google Scholar] [CrossRef]
- Yu, Y.; Liu, X.; Yang, Y.; Zhao, X.; Xue, J.; Zhang, W.; Yang, A. Effect of FHIT loss and p53 mutation on HPV-infected lung carcinoma development. Oncol. Lett. 2015, 10, 392–398. [Google Scholar] [CrossRef] [Green Version]
- Al-Shabbani, N. Detection of Human Papilloma Virus (Type 16 and 18) in Cytological Samples in Patients with Lung Cancer. An Evaluation by Chromogenic In Situ Hybridization Technique. Redox Biol. 2015, 5, 416. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Deng, F.; Qian, L.-T.; Meng, S.-P.; Zhang, Y.; Shan, W.-L.; Zhang, X.-L.; Wang, B.-L. Association between human papillomavirus and EGFR mutations in advanced lung adenocarcinoma. Oncol. Lett. 2016, 12, 1953–1958. [Google Scholar] [CrossRef]
- Xiong, W.M.; He, F.; Xiao, R.D.; Yu, T.T.; Zhang, X.; Liu, Z.Q.; Xu, Q.P.; Cai, L. Association between human papillomavirus infection and lung cancer. Zhonghua Liu Xing Bing Xue Za Zhi 2016, 37, 1658–1661. [Google Scholar]
- He, F.; Xiong, W.; Yu, F.; Xiao, R.; Ye, H.; Li, W.; Liu, Z.; Hu, Z.; Cai, L. Human papillomavirus infection maybe not associated with primary lung cancer in the Fujian population of China. Thorac. Cancer 2020, 11, 561–569. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, M.; Mostafaei, S.; Aghaei, A.; Hosseini, N.; Darabi, H.; Nouri, M.; Etemadi, A.; Neill, A.O.; Nahand, J.S.; Mirzaei, H.; et al. The association between HPV gene expression, inflammatory agents and cellular genes involved in EMT in lung cancer tissue. BMC Cancer 2020, 20, 916. [Google Scholar] [CrossRef] [PubMed]
- Hussen, B.M.; Ahmadi, G.; Marzban, H.; Azar, M.E.F.; Sorayyayi, S.; Karampour, R.; Nahand, J.S.; Hidayat, H.J.; Moghoofei, M. The role of HPV gene expression and selected cellular MiRNAs in lung cancer development. Microb. Pathog. 2020, 150, 104692. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Yin, Q.; Zhou, Y.-L.; He, L.; Zou, Z.-Q.; Dai, X.-Y.; Xia, W. Evaluation of microRNAs as potential biomarkers in circulating HPV-DNA-positive non-small cell lung cancer patients. Cancer Biol. Ther. 2021, 22, 136–148. [Google Scholar] [CrossRef]
- Zou, D.-J.; Zhao, Y.-B.; Yang, J.-H.; Xu, H.-T.; Li, Q.-C.; Wu, G.-P. Expression and Significance of HPV16 E6/E7 mRNAs in the Bronchial Brush and TBNA Cells of Patients with Small Cell Lung Cancer. Technol. Cancer Res. Treat. 2021, 20. [Google Scholar] [CrossRef]
- Huang, J.-Y.; Lin, C.; Tsai, S.C.-S.; Lin, F.C.-F. Human Papillomavirus Is Associated With Adenocarcinoma of Lung: A Population-Based Cohort Study. Front. Med. 2022, 9, 932196. [Google Scholar] [CrossRef]
- Badillo-Almaraz, I.; Zapata-Benavides, P.; Saavedra-Alonso, S.; Zamora-Avila, D.; Reséndez-Pérez, D.; Tamez-Guerra, R.; Herrera-Esparza, R.; Rodríguez-Padilla, C. Human Papillomavirus 16/18 Infections in Lung Cancer Patients in Mexico. Intervirology 2013, 56, 310–315. [Google Scholar] [CrossRef]
- Koshiol, J.; Rotunno, M.; Gillison, M.L.; Van Doorn, L.-J.; Chaturvedi, A.K.; Tarantini, L.; Song, H.; Quint, W.G.V.; Struijk, L.; Goldstein, A.M.; et al. Assessment of Human Papillomavirus in Lung Tumor Tissue. JNCI J. Natl. Cancer Inst. 2011, 103, 501–507. [Google Scholar] [CrossRef]
- Yanagawa, N.; Wang, A.; Kohler, D.; Santos, G.D.C.; Sykes, J.; Xu, J.; Pintilie, M.; Tsao, M. Human papilloma virus genome is rare in North American non-small cell lung carcinoma patients. Lung Cancer 2013, 79, 215–220. [Google Scholar] [CrossRef]
- Chang, S.Y.; Keeney, M.; Law, M.; Donovan, J.; Aubry, M.-C.; Garcia, J. Detection of human papillomavirus in non–small cell carcinoma of the lung. Hum. Pathol. 2015, 46, 1592–1597. [Google Scholar] [CrossRef]
- Colombara, D.V.; Manhart, L.E.; Carter, J.J.; Hawes, S.E.; Weiss, N.S.; Hughes, J.P.; Barnett, M.J.; Goodman, G.E.; Smith, J.S.; Qiao, Y.-L.; et al. Prior human polyomavirus and papillomavirus infection and incident lung cancer: A nested case–control study. Cancer Causes Control 2015, 26, 1835–1844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Oliveira, T.H.A.; Amaral, C.M.D.; Marcos, B.D.F.S.; Nascimento, K.C.G.; Rios, A.C.D.M.; Quixabeira, D.C.A.; Muniz, M.T.C.; Neto, J.D.C.S.; de Freitas, A.C. Presence and activity of HPV in primary lung cancer. J. Cancer Res. Clin. Oncol. 2018, 144, 2367–2376. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.M.; Mariano, V.S.; Pastrez, P.R.A.; Pinto, M.C.; Nunes, E.M.; Sichero, L.; Villa, L.L.; Scapulatempo-Neto, C.; Syrjanen, K.J.; Longatto-Filho, A. Human papillomavirus is not associated to non-small cell lung cancer: Data from a prospective cross-sectional study. Infect. Agents Cancer 2019, 14, 18. [Google Scholar] [CrossRef] [PubMed]
- Karnosky, J.; Dietmaier, W.; Knuettel, H.; Freigang, V.; Koch, M.; Koll, F.; Zeman, F.; Schulz, C. HPV and lung cancer: A systematic review and meta-analysis. Cancer Rep. 2021, 4, e1350. [Google Scholar] [CrossRef] [PubMed]
- Mittal, S.; Banks, L. Molecular mechanisms underlying human papillomavirus E6 and E7 oncoprotein-induced cell transformation. Mutat. Res. Mutat. Res. 2017, 772, 23–35. [Google Scholar] [CrossRef]
- Aguayo, F.C.M.; González, C.; Gheit, T.; Tommasino, M.; Corvalán, A. Role of HPV-16 physical status (episomal/integrated) in lung cancer from Chile. In Proceedings of the American Society for Virology, 29th Annual Meeting, Bozeman, MT, USA, 17–21 July 2010. [Google Scholar]
- Szymonowicz, E.A.K.A.; Chen, J. Biological and clinical aspects of HPV-related cancers. Cancer Biol. Med. 2020, 17, 864–878. [Google Scholar] [CrossRef]
- Pinatti, L.; Walline, H.; Carey, T. Human Papillomavirus Genome Integration and Head and Neck Cancer. J. Dent. Res. 2017, 97, 691–700. [Google Scholar] [CrossRef]
- Bodelon, C.; Untereiner, M.E.; Machiela, M.J.; Vinokurova, S.; Wentzensen, N. Genomic characterization of viral integration sites in HPV-related cancers. Int. J. Cancer 2016, 139, 2001–2011. [Google Scholar] [CrossRef]
- Oyervides-Muñoz, M.A.; Pérez-Maya, A.A.; Rodríguez-Gutiérrez, H.F.; Gómez-Macias, G.S.; Fajardo, O.R.; Trevino, V.; Barrera-Saldaña, H.A.; Garza-Rodríguez, M.L. Understanding the HPV integration and its progression to cervical cancer. Infect. Genet. Evol. 2018, 61, 134–144. [Google Scholar] [CrossRef]
- Senapati, R.; Senapati, N.N.; Dwibedi, B. Molecular mechanisms of HPV mediated neoplastic progression. Infect. Agents Cancer 2016, 11, 59. [Google Scholar] [CrossRef]
- Wentzensen, N.; Vinokurova, S.; Doeberitz, M.V.K. Systematic Review of Genomic Integration Sites of Human Papillomavirus Genomes in Epithelial Dysplasia and Invasive Cancer of the Female Lower Genital Tract. Cancer Res. 2004, 64, 3878–3884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akagi, K.; Li, J.; Broutian, T.R.; Padilla-Nash, H.; Xiao, W.; Jiang, B.; Rocco, J.W.; Teknos, T.N.; Kumar, B.; Wangsa, D.; et al. Genome-wide analysis of HPV integration in human cancers reveals recurrent, focal genomic instability. Genome Res. 2013, 24, 185–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, F.; Cao, M.; Shi, Q.; Chen, H.; Wang, Y.; Li, X. Integration of the full-length HPV16 genome in cervical cancer and Caski and Siha cell lines and the possible ways of HPV integration. Virus Genes 2015, 50, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-C.; Chen, J.-H.; Richard, K.; Chen, P.-Y.; Christiani, D.C. Lung adenocarcinoma and human papillomavirus infection. Cancer 2004, 101, 1428–1436. [Google Scholar] [CrossRef]
- Chen, M.; Wang, Y.; Wang, L.; Shen, C.; Chen, C.; Lee, H. PD-L1 expressed from tumor cells promotes tumor growth and invasion in lung cancer via modulating TGF-β1/SMAD4 expression. Thorac. Cancer 2022, 13, 1322–1332. [Google Scholar] [CrossRef] [PubMed]
- Tung, M.-C.; Lin, P.-L.; Cheng, Y.-W.; Wu, D.-W.; Yeh, S.-D.; Chen, C.-Y.; Lee, H. Reduction of microRNA-184 by E6 oncoprotein confers cisplatin resistance in lung cancer via increasing Bcl-2. Oncotarget 2016, 7, 32362–32374. [Google Scholar] [CrossRef] [Green Version]
- Wu, H.-H.; Wu, J.-Y.; Cheng, Y.-W.; Chen, C.-Y.; Lee, M.-C.; Goan, Y.-G.; Lee, H. cIAP2 Upregulated by E6 Oncoprotein via Epidermal Growth Factor Receptor/Phosphatidylinositol 3-Kinase/AKT Pathway Confers Resistance to Cisplatin in Human Papillomavirus 16/18–Infected Lung Cancer. Clin. Cancer Res. 2010, 16, 5200–5210. [Google Scholar] [CrossRef] [Green Version]
- Chen, P.-M.; Cheng, Y.-W.; Wang, Y.-C.; Wu, T.-C.; Chen, C.-Y.; Lee, H. Up-Regulation of FOXM1 by E6 Oncoprotein through the MZF1/NKX2-1 Axis Is Required for Human Papillomavirus–Associated Tumorigenesis. Neoplasia 2014, 16, 961–971. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Wu, M.; Gu, N.; Xu, H.; Li, Q.; Wu, G. Human papillomavirus 16 (HPV 16) E6 but not E7 inhibits the antitumor activity of LKB1 in lung cancer cells by downregulating the expression of KIF7. Thorac. Cancer 2020, 11, 3175–3180. [Google Scholar] [CrossRef]
- Wei, S.; Zhang, H.; Tao, S. A review of arsenic exposure and lung cancer. Toxicol. Res. 2019, 8, 319–327. [Google Scholar] [CrossRef]
- Riudavets, M.; de Herreros, M.G.; Besse, B.; Mezquita, L. Radon and Lung Cancer: Current Trends and Future Perspectives. Cancers 2022, 14, 3142. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Mengersen, K.; Tong, S.; Kimlin, M.; Zhou, M.; Hu, W. Global, regional, and national burden of lung cancer and its attributable risk factors, 1990 to 2017. Cancer 2020, 126, 4220–4234. [Google Scholar] [CrossRef] [PubMed]
- Jedrychowski, W.; Becher, H.; Basa-Cierpialek, Z.; Gomola, K. Effect of tobacco smoking on various histological types of lung cancer. J. Cancer Res. Clin. Oncol. 1992, 118, 276–282. [Google Scholar] [CrossRef]
- Stading, R.; Gastelum, G.; Chu, C.; Jiang, W.; Moorthy, B. Molecular mechanisms of pulmonary carcinogenesis by polycyclic aromatic hydrocarbons (PAHs): Implications for human lung cancer. Semin. Cancer Biol. 2021, 76, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Moutinho, J.A. Smoking and Cervical Cancer. ISRN Obstet. Gynecol. 2011, 2011, 847684. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, J.P.; González, C.; Parra, B.; Corvalan, A.; Tornesello, M.L.; Eizuru, Y.; Aguayo, F. Functional Interaction between Human Papillomavirus Type 16 E6 and E7 Oncoproteins and Cigarette Smoke Components in Lung Epithelial Cells. PLoS ONE 2012, 7, e38178. [Google Scholar] [CrossRef]
- Peña, N.; Carrillo, D.; Muñoz, J.P.; Chnaiderman, J.; Urzua, U.; León, O.; Tornesello, M.L.; Corvalan, A.; Rifo, R.S.; Aguayo, F. Tobacco Smoke Activates Human Papillomavirus 16 p97 Promoter and Cooperates with High-Risk E6/E7 for Oxidative DNA Damage in Lung Cells. PLoS ONE 2015, 10, e0123029. [Google Scholar] [CrossRef] [Green Version]
- Wei, L.; Griego, A.M.; Chu, M.; Ozbun, M.A. Tobacco exposure results in increased E6 and E7 oncogene expression, DNA damage and mutation rates in cells maintaining episomal human papillomavirus 16 genomes. Carcinogenesis 2014, 35, 2373–2381. [Google Scholar] [CrossRef] [Green Version]
- Miller, L.G.; Goldstein, G.; Murphy, M.; Ginns, L.C. Reversible Alterations in Immunoregulatory T Cells in Smoking. Analysis by monoclonal antibodies and flow cytometry. Chest 1982, 82, 526–529. [Google Scholar] [CrossRef]
- Ferson, M.; Edwards, A.; Lind, A.; Milton, G.W.; Hersey, P. Low natural killer-cell activity and immunoglobulin levels associated with smoking in human subjects. Int. J. Cancer 1979, 23, 603–609. [Google Scholar] [CrossRef]
- Holt, P.G.; Keast, D. Environmentally induced changes in immunological function: Acute and chronic effects of inhalation of tobacco smoke and other atmospheric contaminants in man and experimental animals. Bacteriol. Rev. 1977, 41, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Iwasaka, T.; Hayashi, Y.; Yokoyama, M.; Hara, K.; Matsuo, N.; Sugimori, H. ‘Hit and run’ oncogenesis by human papillomavirus type 18 DNA. Acta Obstet. Gynecol. Scand. 1992, 71, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Viarisio, D.; Müller-Decker, K.; Accardi, R.; Robitaille, A.; Dürst, M.; Beer, K.; Jansen, L.; Flechtenmacher, C.; Bozza, M.; Harbottle, R.; et al. Beta HPV38 oncoproteins act with a hit-and-run mechanism in ultraviolet radiation-induced skin carcinogenesis in mice. PLoS Pathog. 2018, 14, e1006783. [Google Scholar] [CrossRef] [PubMed]
- Kostov, S.; Dzhenkov, D.; Metodiev, D.; Kornovski, Y.; Slavchev, S.; Ivanova, Y.; Yordanov, A. A case of human papillomavirus infection and vulvar cancer in a young patient—“Hit and run” theory. Gynecol. Oncol. Rep. 2021, 36, 100760. [Google Scholar] [CrossRef]
Figure 1.
Tobacco smoke and HPV in lung cancer. (A) Tobacco smoking is the most important independent etiological factor of lung cancer. (B) HPV can be related to lung cancer as an independent carcinogen in non-smoker subjects. (C) HPV can cooperate with tobacco smoke for lung tumorigenesis. Designed using BioRender.
Figure 1.
Tobacco smoke and HPV in lung cancer. (A) Tobacco smoking is the most important independent etiological factor of lung cancer. (B) HPV can be related to lung cancer as an independent carcinogen in non-smoker subjects. (C) HPV can cooperate with tobacco smoke for lung tumorigenesis. Designed using BioRender.

Figure 2.
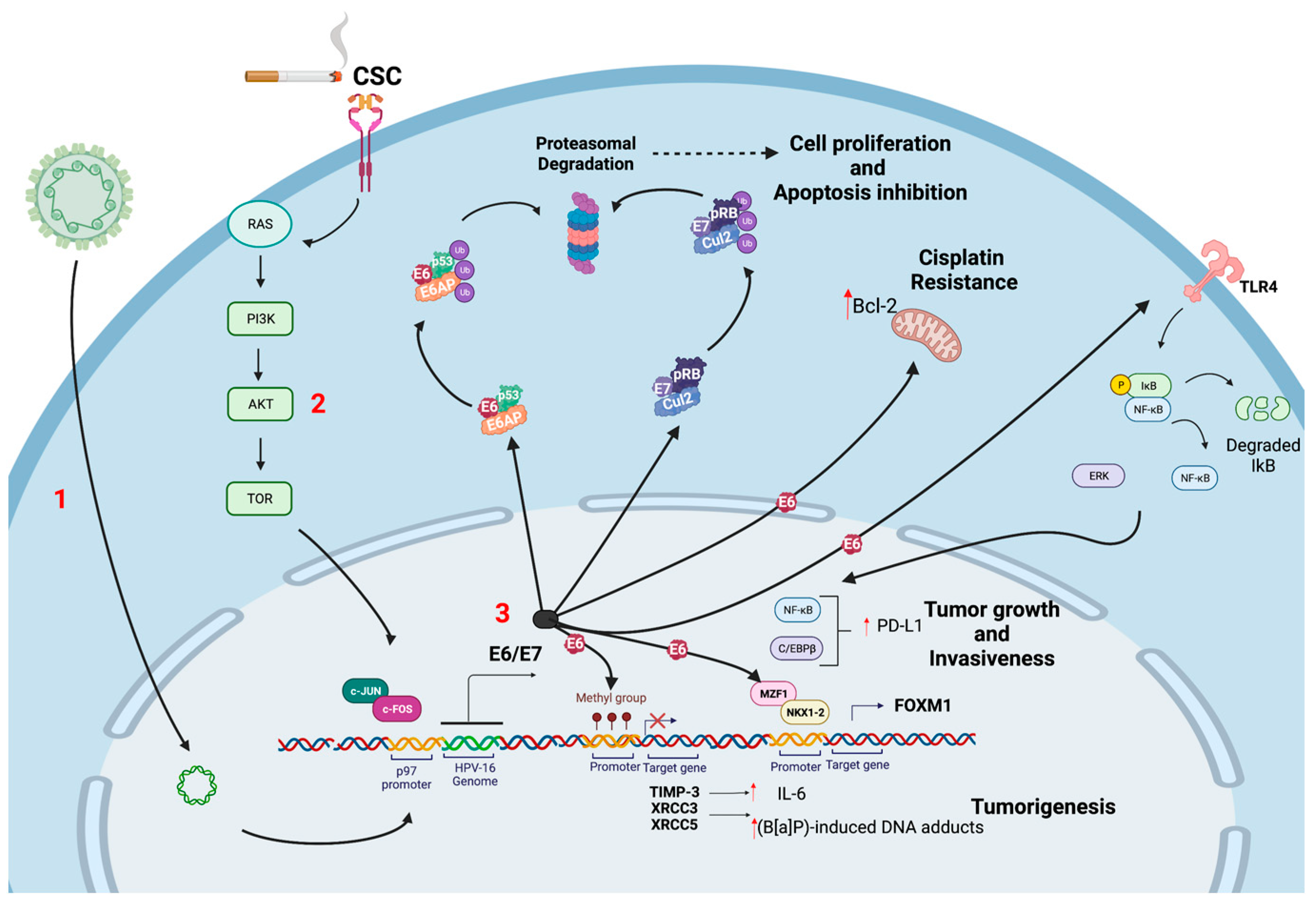
Molecular alterations in HPV-associated lung cancer. (1) HR-HPV infection and viral genome integration leads to E2 ORF disruption, resulting in early promoter (p97 in HPV16) activation (2) CSC can activate PI3K/Akt/mTOR signaling pathway, thus cooperating for increased HPV early promoter activation and E6/E7 overexpression; (3) HR-HPV E6/E7 oncoproteins induce p53 and pRB ubiquitination and degradation, in turn, promoting apoptosis inhibition and cell proliferation. In addition, HR-HPV E6 promote increased Bcl-2 levels and cisplatin resistance, the expression of PD-L1 through the ERK-C/EBPβ-TLR4-NF-κB signaling pathway, thus increasing tumor growth and invasiveness; induction of FOXM1 by E6 oncoprotein through the MZF1/NKX2-1 axis and the E6-induced promoter hypermethylation of the XRCC3 and XRCC5 DNA repair genes that increase tumorigenesis. Created using BioRender.
Figure 2.
Molecular alterations in HPV-associated lung cancer. (1) HR-HPV infection and viral genome integration leads to E2 ORF disruption, resulting in early promoter (p97 in HPV16) activation (2) CSC can activate PI3K/Akt/mTOR signaling pathway, thus cooperating for increased HPV early promoter activation and E6/E7 overexpression; (3) HR-HPV E6/E7 oncoproteins induce p53 and pRB ubiquitination and degradation, in turn, promoting apoptosis inhibition and cell proliferation. In addition, HR-HPV E6 promote increased Bcl-2 levels and cisplatin resistance, the expression of PD-L1 through the ERK-C/EBPβ-TLR4-NF-κB signaling pathway, thus increasing tumor growth and invasiveness; induction of FOXM1 by E6 oncoprotein through the MZF1/NKX2-1 axis and the E6-induced promoter hypermethylation of the XRCC3 and XRCC5 DNA repair genes that increase tumorigenesis. Created using BioRender.


{kind=link}
{kind=link}
Table 1.
HPV frequency in lung cancer cases.
| Tumor Types | Total | HPV (+) | (%) | HPV Genotype | HPV Gene | Methods | Country | Year | Ref |
|---|---|---|---|---|---|---|---|---|---|
| SQC | 1 | Condiloma | 100 | - | Histological changes | Finland | 1972 | [61] | |
| SQC | 100 | -Condiloma | 6 | - | Histological changes | Finland | 1980 | [62] | |
| -Endophytic condyloma | 4 | ||||||||
| -Flat type condyloma | 26 | ||||||||
| Anaplastic carcinoma in the lung | 24 | HPV 16 DNA | 4.2 | - | DNA hybridizing | Germany | 1985 | [63] | |
| SQC | 131 | 9 | 6.9 | 6, 11, 16, 18, and 30 | - | ISH | Finland | 1989 | [64] |
| Squamous bronchial metaplasia, SQC | 43 | 7 | 16 | 6, 11, 16 and 18 | - | ISH | France | 1990 | [65] |
| SQC, AdC, SCLC, Large cell undifferentiated carcinoma, bronchioloalveolar carcinoma | 58 | 7 | 12.1 | 6, 11, 16, 18, 31, 33, 35 | - | ISH | USA | 1992 | [77] |
| SQC | 49 | 7 | 14.3 | 6,11 | - | PCR | Republic of China | 1993 | [72] |
| SQC, SCLC | 47 | 0 | 0 | - | - | PCR | Japan | 1994 | [73] |
| SQC | 49 | 7 | 14.3 | 6, 11 | - | PCR | Republic of China | 1994 | [75] |
| 5 | 10.2 | ISH | |||||||
| SQC, AdC, Neuro-endocrine cancers. | 31 | 5 | 16.1 | 6, 11, 16 | - | PCR | France | 1995 | [66] |
| SQC, AdC, SCLC, SCC, adenosquamous carcinomas | 99 | 14 | 15 | 11, 16, 18, 33 | - | PCR | Greece | 1996 | [67] |
| SQC, SCC | 38 | 0 | 0 | - | - | ISH | Germany | 1997 | [68] |
| SQC, AdC, SCC | 50 | 16 | 32 | 16, 18 | - | PCR, dot-blot hybridization | Republic of China | 1997 | [76] |
| SQC | 34 | 2 | 6 | 18 | - | PCR, SBH | USA | 1998 | [78] |
| SQC | 52 | 32 | 69 | 6, 11, 16, 18 | - | PCR, SBH | Greece | 1998 | [69] |
| SQC, AdC | 207 | 18 | 9 | 6, 11, 16, 18 | E6,E7 | NISH | Japan | 1998 | [74] |
| SQC, AdC, oat cell carcinomas, LCC, anaplastic carcinoma | 75 | 37 | 49 | 6, 11, 16, 18 | - | PCR, ISH | Norway | 1998 | [71] |
| SQC | 91 | 0 | 0 | - | - | PCR, ISH | Greece | 1998 | [70] |
| SQC, AdC | 185 | 5 | 2,7 | 16, 31, 33 | - | HCA | France | 2000 | [79] |
| SQC | 434 | 80 | 18 | 6, 11, 16, 18 | E6,E7 | PCR, SBH | Japan | 2000 | [94] |
| NSCLC | 40 | 4 | 10 | - | - | - | Poland | 2001 | [80] |
| SQC, AdC | 141 | 77 | 54.6 | 16, 18 | L1 | Nested PCR, ISH | Republic of China | 2001 | [87] |
| SQC | 26 | 3 | 11.5 | 6, 11, 16, 18 | - | NISH | Turkey | 2001 | [81] |
| SQC, AdC, SCLC | 40 | 2 | 5 | 18 | L1 | ISH, PCR, SBH, dot blotting | Turkey | 2004 | [82] |
| SQC | 122 | 0 | 0 | - | - | ISH | France | 2005 | [83] |
| SQC, AdC, Bronchioalveolar carcinomas | 218 | 4 | 2 | 16 | L1, E6 | PCR | France | 2005 | [84] |
| SQC, AdC, SCC | 36 | 10 | 28 | 16, 18, 33 | L1 | PCR, SBH | Japan | 2006 | [98] |
| SQC, AdC | 73 | 23 | 32 | 16, 18 | - | ISH | Republic of China | 2006 | [92] |
| NSCLC | 38 | 8 | 21 | 16, 18, 31 | E6, E7 | RT-PCR | Italy | 2006 | [85] |
| NSCLC | 112 | 58 | 52 | 16, 18, 33 | E6 | PCR | Korea | 2007 | [95] |
| LCLC, AdC, SQC, LCC, SCLC | 141 | 33 | 26 | 6, 11, 16, 18, 26, 31 | L1 | Nested PCR | Iran | 2007 | [96] |
| AdC, SQC | 69 | 20 | 29 | 16, 18, 31, 33, 45, 59 | L1, E6 | PCR, SBH, IHC | Chile | 2007 | [99] |
| AdC, SQC, LCC | 78 | 10 | 13 | 6, 16, 31 | E6, E7 | PCR, RFLP | Italy | 2007 | [86] |
| AdC, SQC | 313 | 138 | 39.1 | 16, 18 | E6, E7 | NISH | Republic of China | 2008 | [93] |
| AdC, SQC | 217 | 80 | 37 | 16, 18 | E6 | IHC | Republic of China | 2009 | [88] |
| AdC | 110 | 0 | 0 | - | - | ISH | Republic of Singapore | 2009 | [97] |
| AdC, SQC | 109 | 43 | 39 | 16, 18 | L1, E6, E2 | INNO-LIPA PCR, RT-PCR | Republic of China | 2009 | [89] |
| SQC | 44 | 32 | 73 | 16, 18 | - | ISH | Republic of China | 2009 | [90] |
| NSCLC | 104 | 18 | 17.3 | 16 | L1, E6, E7 | RT-PCR, PCR | Republic of China | 2009 | [91] |
| AdC, SQC, LCC, SCLC | 84 | 3 | 3.6 | 16, 18, 33 | E6 | PCR | Croatia | 2010 | [100] |
| AdC, SQC | 57 | 11 | 19.3 | 6, 16, 18, 33 | L1, E6, E2 | RT-PCR, PCR | Japan | 2010 | [110] |
| AdC | 297 | 0 | 0 | 16, 18, 33 | L1, E1, E6, E7 | Multiplex PCR, Nested PCR | Japan | 2010 | [111] |
| AdC, SQC, SCLC | 59 | 8 | 13 | 16 | L1, E6, E2 | qRT-PCR, SBH | Japan | 2010 | [112] |
| AdC, SQC | 30 | 5 | 16.7 | 16, 11 | L1 | PCR, DNA sequencing | USA | 2010 | [8] |
| AdC, SQC, LCC, SCLC | 399 | 0 | 0 | - | E6, E7 | qRT-PCR | USA | 2011 | [128] |
| AdC, SQC | 304 | 20 | 6.6 | 6, 11, 16, 18 | L1 | PCR, ISH | Japan | 2011 | [113] |
| AdC, SQC, SCLC | 89 | 13 | 13.5 | 16, 30, 31, 39 | E1 | PCR, pyrosequencing analysis | Italy | 2011 | [101] |
| AdC, SQC | 77 | 4 | 5.2 | 6,16 | L1 | Luminex-based Multimetrix | Finland | 2012 | [102] |
| AdC, SQC | 100 | 0 | 0 | - | L1 | PCR, ISH | Italy | 2012 | [103] |
| SQC | 50 | 9 | 18 | 6, 18 | L1 | Nested PCR | Iran | 2013 | [114] |
| AdC, SQC | 39 | 16 | 41 | 16, 18 | L1 | PCR, ISH | Mexico | 2013 | [127] |
| AdC, SQC | 170 | 75 | 44 | 16, 18 | E6 | PCR, INNO-LIPA, SBH | Republic of China | 2013 | [115] |
| AdC, SQC | 336 | 5 | 1.5 | 16 | L1 | PCR, ISH | Canada | 2013 | [129] |
| AdC, SQC | 200 | 19 | 9.5 | 16, 11 | L1 | qRT-PCR | Greece | 2014 | [104] |
| AdC, SQC | 262 | 22 | 8.4 | 16,18,31 | - | PCR, ISH, reverse dot blot | Republic of China | 2015 | [116] |
| AdC, SQC, SCLC | 180 | 100 | 55.6 | 16, 18 | L1 | PCR and immunohistochemistry | Republic of China | 2015 | [117] |
| SQC | 50 | 30 | 60 | 16, 18 | - | ISH | Iraq | 2015 | [118] |
| AdC, SQC | 196 | 0 | 0 | - | E6, E7 | DNA-ISH, RNA-ISH | Canada | 2015 | [130] |
| AdC, SQC, LCC, SCLC | 200 | 5 | 2.5 | 16 | L1, | Antibody assays | USA | 2015 | [131] |
| 16 | 8.5 | E6, | |||||||
| 4 | 2 | E7 | |||||||
| AdC | 95 | 27 | 28.4 | 16, 18, 33, 58 | L1 | PCR | Republic of China | 2016 | [119] |
| NSCLC | 83 | 7 | 8.4 | - | L1 | Reverse hybridization | Republic of China | 2016 | [120] |
| AdC, SQC, SCLC | 67 | 2 | 3 | 16, 53 | E6, E7 | NASBA | Greece | 2017 | [105] |
| AdC, SQC | 132 | 33 | 25 | 16, 18 | L1 | PCR | Denmark | 2017 | [106] |
| AdC, SQC, LCC | 63 | 33 | 52 | 16, 18 | E6, E7 | PCR | Brazil | 2018 | [132] |
| AdC, SQC | 77 | 0 | 0 | - | E7 | Multiplex PCR, RT-PCR | Brazil | 2019 | [133] |
| AdC, SQC, LCC | 140 | 13 | 9.3 | 16, 18, 35, 42, 44, 51 | L1 | PCR, Reverse hybridization | Republic of China | 2020 | [121] |
| AdC, SQC, LCC | 80 | 0 | 0 | - | E6 | qPCR | Czech Republic | 2020 | [107] |
| AdC, SQC, SCLC | 102 | 54 | 52.9 | 16 | L1, E2, E6, E7 | PCR, INNO-LiPA | Iran | 2020 | [122] |
| AdC, SQC, SCLC | 109 | 56 | 51.4 | 6, 11, 16, 18, 33 | L1, E,2, E6, E7 | PCR, INNO-LiPA | Iran | 2021 | [123] |
| AdC, SQC | 100 | 16 | 16 | 16 | L1 | PCR | Republic of China | 2021 | [124] |
| SCLC, SQC, AdC | 310 | 183 | 59 | - | E6, E7 | qRT-PCR | Republic of China | 2021 | [125] |
| AdC, SQC, NSCLC, SCLC | 41 | 23 | 56 | 16,18,33, 56,58 | L1, E6 | RT-PCR | Spain | 2022 | [109] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Osorio, J.C.; Candia-Escobar, F.; Corvalán, A.H.; Calaf, G.M.; Aguayo, F. High-Risk Human Papillomavirus Infection in Lung Cancer: Mechanisms and Perspectives. Biology 2022, 11, 1691. https://doi.org/10.3390/biology11121691
AMA Style
Osorio JC, Candia-Escobar F, Corvalán AH, Calaf GM, Aguayo F. High-Risk Human Papillomavirus Infection in Lung Cancer: Mechanisms and Perspectives. Biology. 2022; 11(12):1691. https://doi.org/10.3390/biology11121691
Chicago/Turabian StyleOsorio, Julio C., Felipe Candia-Escobar, Alejandro H. Corvalán, Gloria M. Calaf, and Francisco Aguayo. 2022. "High-Risk Human Papillomavirus Infection in Lung Cancer: Mechanisms and Perspectives" Biology 11, no. 12: 1691. https://doi.org/10.3390/biology11121691
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.