
Elastodontic Devices in Orthodontics: An In-Vitro Study on Mechanical Deformation under Loading

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
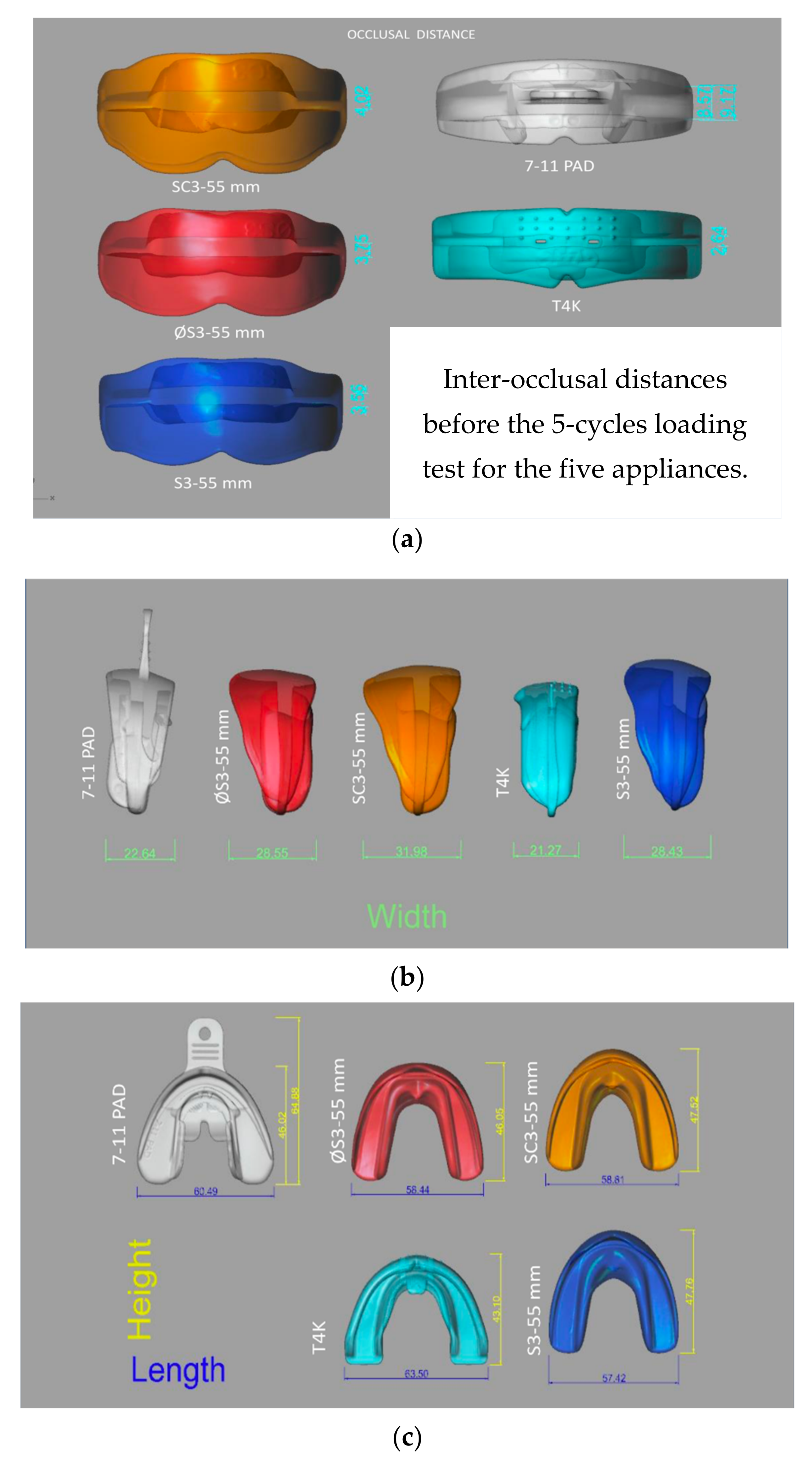
- -A.M.C.O.P. (Micerium, Genova, Italy) in red color (Ref. ΦS3–55 mm).
- -A.M.C.O.P. in orange color (Ref. SC3–55 mm).
- -A.M.C.O.P. in blue color (Ref. S3–55 mm).
- -HealthyStart (Ortho-Tain, Winnetka, IL, USA) (Ref. 7–11 PAD).
- -T4K phase 1(Myofuncional Research Co., Helensvale, Australia) (Ref. T4K).
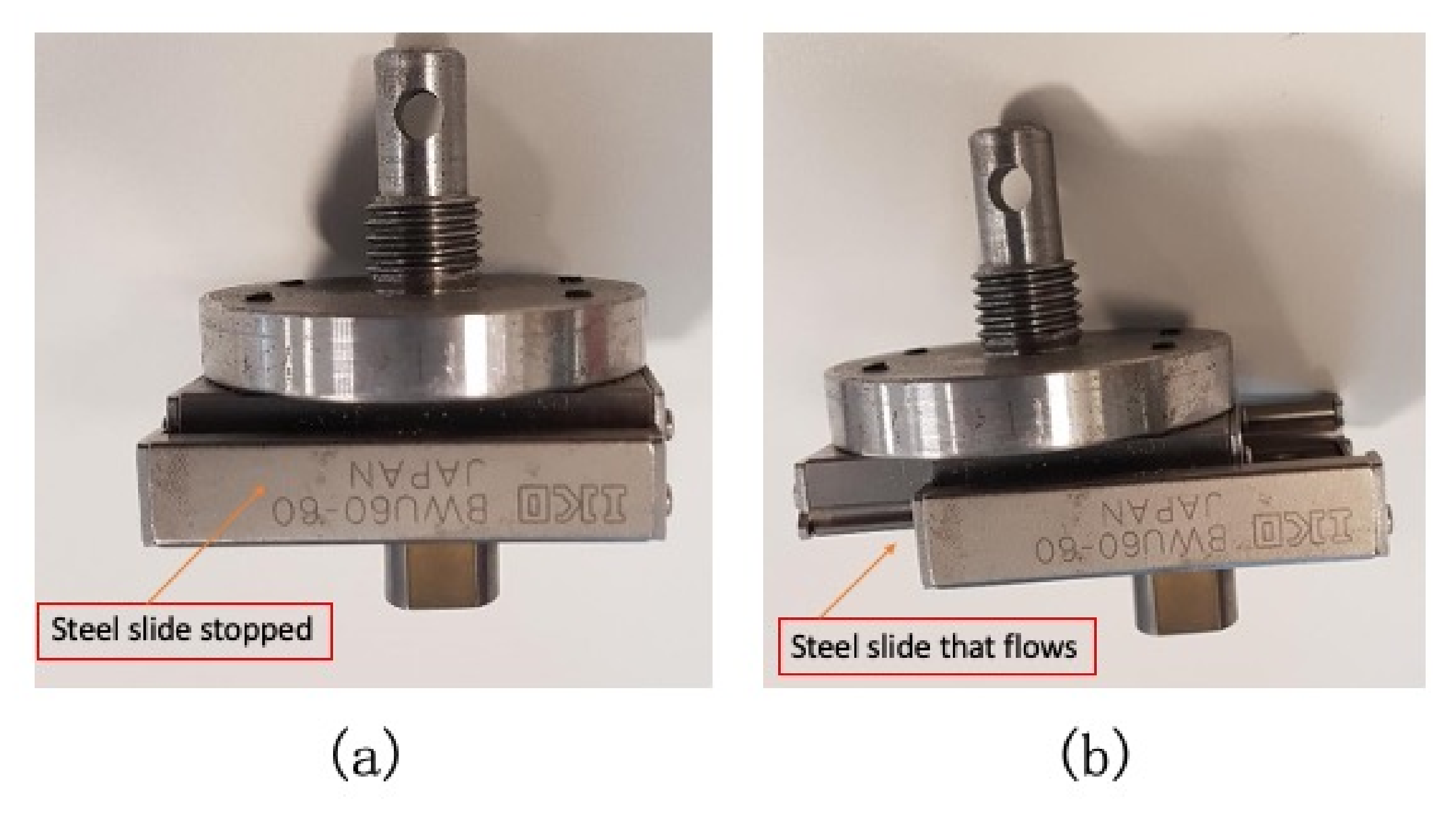
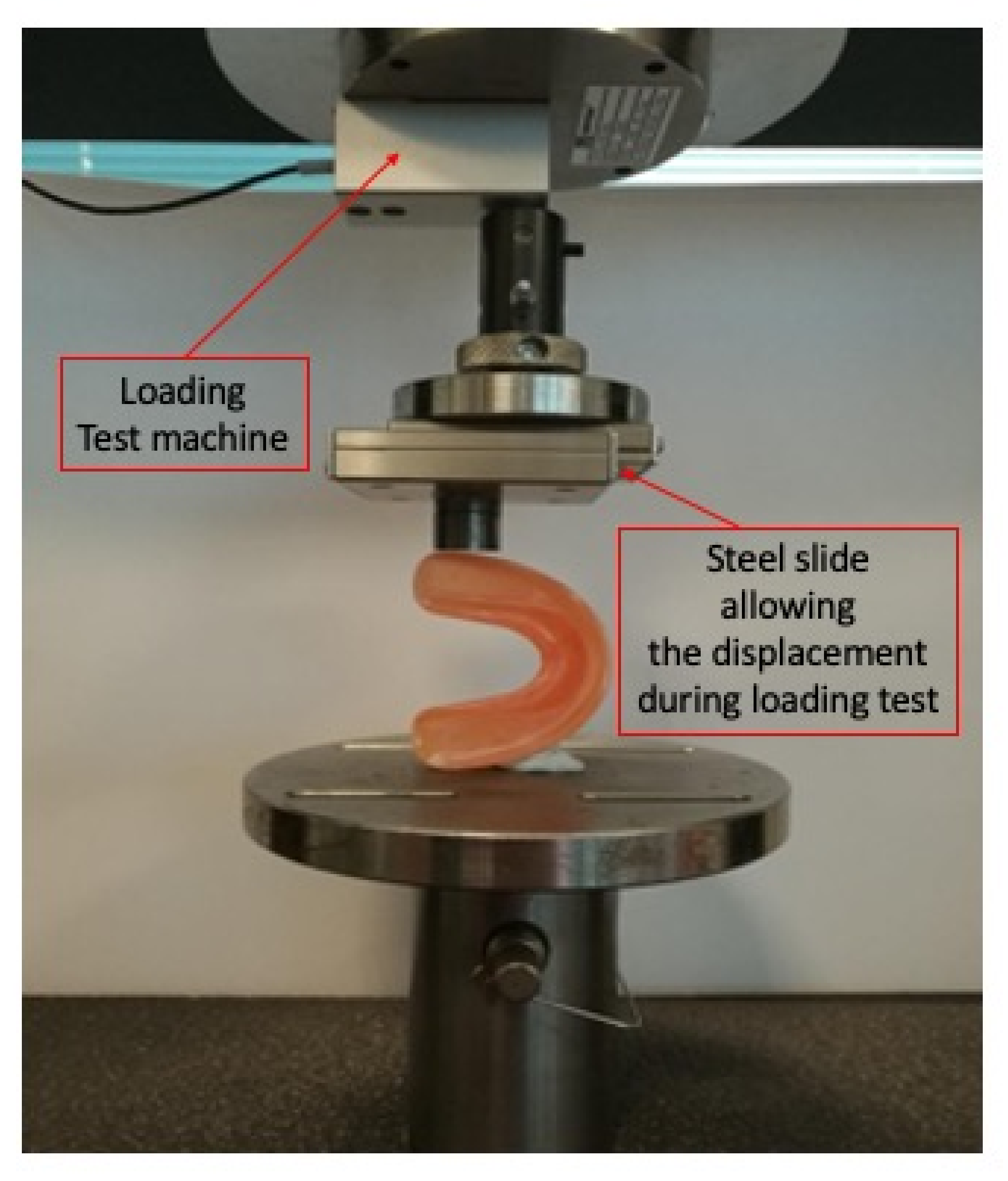
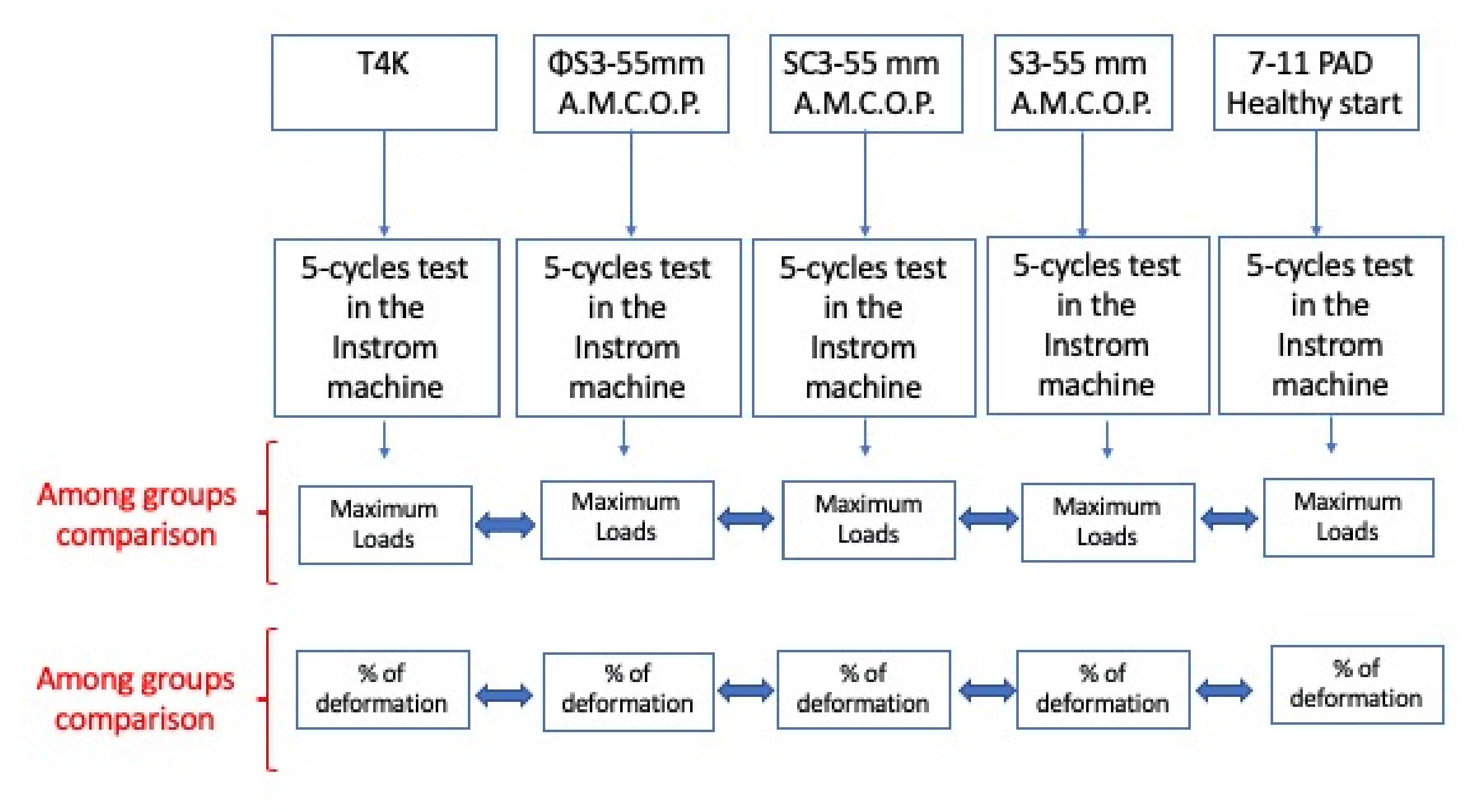
2.1. The Mechanical Tests
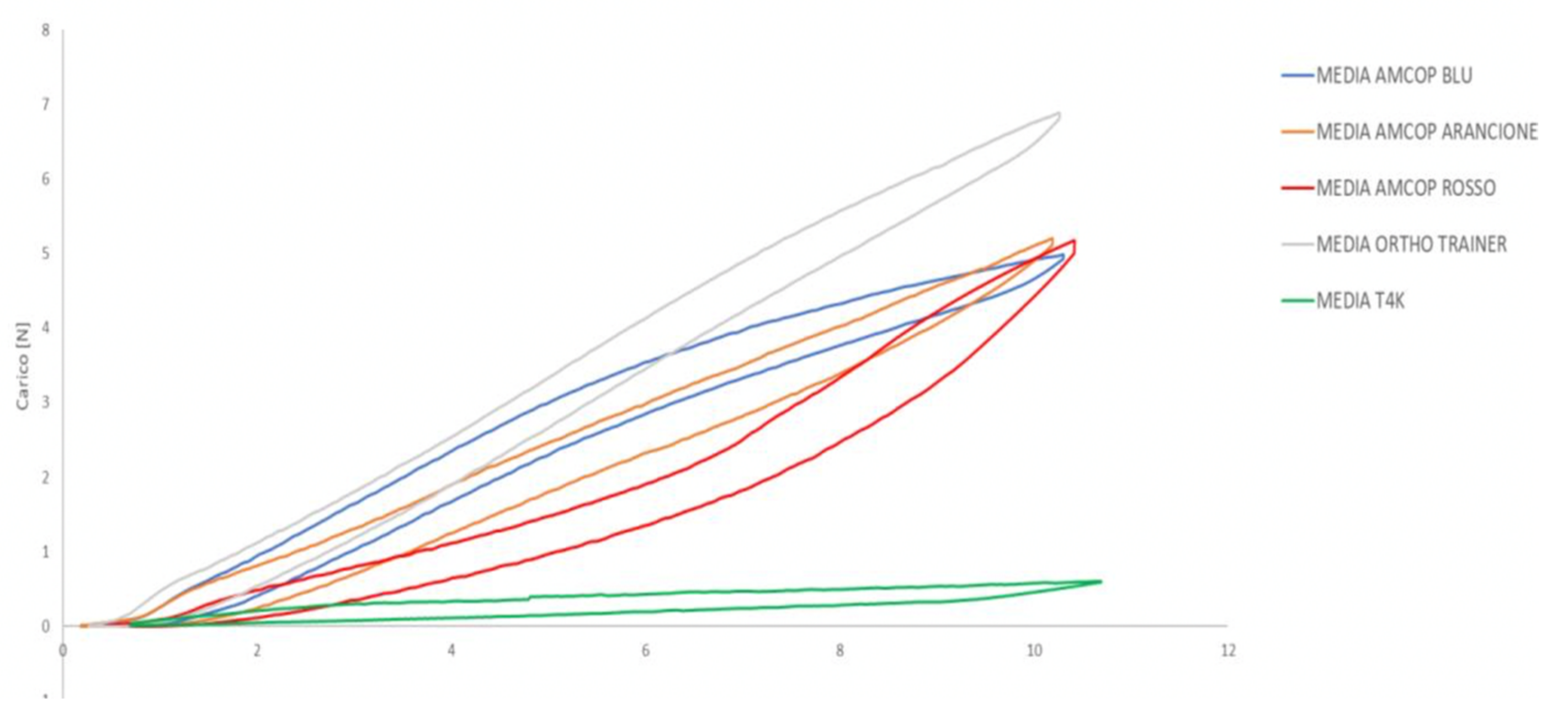
2.2. The Maximum Compression Loads
2.3. The Plastic Deformation under Loading
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Graber, T.M.; Chung, D.D.; Aoba, J.T. Dentofacial orthopedics versus orthodontics. J. Am. Dent. Assoc. 1967, 75, 1145–1166. [Google Scholar] [CrossRef] [PubMed]
- Wishney, M.; Darendeliler, M.A.; Dalci, O. Myofunctional therapy and prefabricated functional appliances: An overview of the history and evidence. Aust. Dent. J. 2019, 64, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Migliaccio, S.; Aprile, V.; Zicari, S.; Grenci, A. Eruption guidance appliance: A review. Eur. J. Paediatr. Dent. 2014, 15. [Google Scholar]
- Keski-Nisula, K.; Hernesniemi, R.; Heiskanen, M.; Keski-Nisula, L.; Varrela, J. Orthodontic intervention in the early mixed dentition: A prospective, controlled study on the effects of the eruption guidance appliance. Am. J. Orthod. Dentofac. Orthop. 2008, 133, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Tecco, S.; Epifania, E.; Festa, F. An electromyographic evaluation of bilateral symmetry of masticatory, neck and trunk muscles activity in patients wearing a positioner. J. Oral Rehabil. 2008, 35, 433–439. [Google Scholar] [CrossRef]
- Bergersen, E.O. The eruption guidance myofunctional appliances: How it works, how to use it. Funct. Orthod. 1984, 1, 28–29; 31–35. [Google Scholar]
- Quinzi, V.; Nota, A.; Caggiati, E.; Saccomanno, S.; Marzo, G.; Tecco, S. Short-Term Effects of a Myofunctional Appliance on Atypical Swallowing and Lip Strength: A Prospective Study. J. Clin. Med. 2020, 9, 2652. [Google Scholar] [CrossRef]
- Skomro, P. Aparat ortodontyczny z elastomeru silikonowego w ocenie klinicznej i opinii pacjentów po leczeniu niektórych wad zgryzu [Orthodontic appliance made from silicone elastomer, evaluated clinically and from patient opinions after treatment for malocclusion]. Ann. Acad. Med. Stetin. 2000, 46, 293–304. [Google Scholar]
- Laganà, G.; Cozza, P. Interceptive therapy with elastodontic appliance: Case report. Ann. Stomatol. 2011, 1, 22–28. [Google Scholar]
- Janson, G.; Nakamura, A.; Chiqueto, K.; Castro, R.; de Freitas, M.R.; Henriques, J.F.C. Treatment stability with the eruption guidance appliance. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 717–728. [Google Scholar] [CrossRef]
- Montenegro, V.; Inchingolo, A.D.; Malcangi, G.; Limongelli, L.; Marinelli, G.; Coloccia, G.; Laudadio, C.; Patano, A.; Inchingolo, F.; Bordea, I.R.; et al. Compliance of children with removable functional appliance with microchip integrated during COVID-19 pandemic: A systematic review. J. Biol. Regul. Homeost. Agents. 2021, 35, 365–377. [Google Scholar] [CrossRef]
- Patano, A.; Cirulli, N.; Beretta, M.; Plantamura, P.; Inchingolo, A.; Inchingolo, A.; Bordea, I.; Malcangi, G.; Marinelli, G.; Scarano, A.; et al. Education Technology in Orthodontics and Paediatric Dentistry during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6056. [Google Scholar] [CrossRef]
- Ramirez-Yañez, G.; Sidlauskas, A.; Junior, E.; Fluter, J. Dimensional Changes in Dental Arches After Treatment with a Prefabricated Functional Appliance. J. Clin. Pediatr. Dent. 2007, 31, 279–283. [Google Scholar] [CrossRef]
- Zhang, X.; He, J.-M.; Zheng, W.-Y. Comparison of rapid maxillary expansion and pre-fabricated myofunctional appliance for the management of mouth breathers with Class II malocclusion. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 16–23. [Google Scholar]
- Fichera, G.; Martina, S.; Palazzo, G.; Musumeci, R.; Leonardi, R.; Isola, G.; Giudice, A.L. New Materials for Orthodontic Interceptive Treatment in Primary to Late Mixed Dentition. A Retrospective Study Using Elastodontic Devices. Materials 2021, 14, 1695. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Di Pede, C.; et al. The Efficacy of a New AMCOP® Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview. Int. J. Environ. Res. Public Health 2022, 19, 988. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Ceci, S.; Patano, A.; Inchingolo, A.M.; Montenegro, V.; Di Pede, C.; Malcangi, G.; Marinelli, G.; Coloccia, G.; Garibaldi, M.; et al. Elastodontic Therapy of Hyperdivergent Class II Patients Using AMCOP® Devices: A Retrospective Study. Appl. Sci. 2022, 12, 3259. [Google Scholar] [CrossRef]
- Cardarelli, F.; Patano, A.; Montenegro, V.; Malcangi, G.; Coloccia, G.; Inchingolo, A.D.; Marinelli, G.; Laudadio, C.; Dipalma, G.; Di Venere, D.; et al. Elastodontic therapy un nuovo approccio alla terapia ortodontica funzionale. Il Dent. Mod. 2021, 4, 48–63. [Google Scholar]
- Elhamouly, Y.; El-Housseiny, A.A.; Ismail, H.A.; El Habashy, L.M. Myofunctional Trainer versus Twin Block in Developing Class II Division I Malocclusion: A Randomized Comparative Clinical Trial. Dent. J. 2020, 8, 44. [Google Scholar] [CrossRef]
- Idris, G.; Hajeer, M.Y.; Al-Jundi, A. Soft- and hard-tissue changes following treatment of Class II division 1 malocclusion with Activator versus Trainer: A randomized controlled trial. Eur. J. Orthod. 2018, 41, 21–28. [Google Scholar] [CrossRef]
- Warunek, S.P.; Sorenson, S.E.; Cunat, J.J.; Green, L.J. Physical and mechanical properties of elastomers in orthodontic positioners. Am. J. Orthod. Dentofac. Orthop. 1989, 95, 388–400. [Google Scholar] [CrossRef]
- Quinn, R.S.; Yoshikawa, D.K. A reassessment of force magnitude in orthodontics. Am. J. Orthod. 1985, 88, 252–260. [Google Scholar] [CrossRef]
- Tecco, S.; Farronato, G.; Salini, V.; Di Meo, S.; Filippi, M.R.; Festa, F.; D’Attilio, M. Evaluation of Cervical Spine Posture After Functional Therapy with FR-2: A Longitudinal Study. CRANIO® 2005, 23, 53–66. [Google Scholar] [CrossRef]
- Jamari, J.; Ammarullah, M.I.; Santoso, G.; Sugiharto, S.; Supriyono, T.; Prakoso, A.T.; Basri, H.; van der Heide, E. Computational Contact Pressure Prediction of CoCrMo, SS 316L and Ti6Al4V Femoral Head against UHMWPE Acetabular Cup under Gait Cycle. J. Funct. Biomater. 2022, 13, 64. [Google Scholar] [CrossRef]
- Bergersen, E.O.; Stevens-Green, B.; Rosellini, E. Efficacy of Preformed Sleep and Habit Appliances to Modify Symptoms of Sleep-Disordered Breathing and Oral Habits in Children with Focus on Resolution of Mouth Breathing. Compend. Contin. Educ. Dent. 2022, 43, e9–e12. [Google Scholar]
- Collett, A.R.; Cook, W.D.; West, V.C. Mechanical properties of some polymer materials used for tooth positioners. Aust. Dent. J. 1994, 39, 298–305. [Google Scholar] [CrossRef]
- Wong, A.K. Orthodontic elastic materials. Angle Orthod. 1976, 46, 196–205. [Google Scholar] [CrossRef]
- Mummolo, S.; Tieri, M.; Nota, A.; Caruso, S.; Darvizeh, A.; Albani, F.; Gatto, R.; Marzo, G.; Marchetti, E.; Quinzi, V.; et al. Salivary concentrations of Streptococcus mutans and Lactobacilli during an orthodontic treatment. An observational study comparing fixed and removable orthodontic appliances. Clin. Exp. Dent. Res. 2019, 6, 181–187. [Google Scholar] [CrossRef] [Green Version]
- Di Venere, D.; Pettini, F.; Nardi, G.M.; Laforgia, A.; Stefanachi, G.; Notaro, V.; Rapone, B.; Grassi, F.R.; Corsalini, M. Correlation between parodontal indexes and orthodontic retainers: Prospective study in a group of 16 patients. Oral Implant. 2017, 10, 78–86. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| The Maximum Compression Loads (N) | Maximum Deformation (mm) | |
|---|---|---|
| A.M.C.O.P. blu color (S3–55 mm) | 5.85 | 10.004 |
| A.M.C.O.P. orange color (SC3–55 mm) | 5.33 | 10.004 |
| A.M.C.O.P. red color (ΦS3–55 mm) | 5.81 | 10.004 |
| HealthyStart (Ortho-Tain) (7–11 PAD) | 7.56 | 10.004 |
| Trainer for Kids (T4K) | 0.7 | No data * |
| Percentage of Deformation (%) | |
|---|---|
| A.M.C.O.P. blu color (S3–55 mm) | 1.29 |
| A.M.C.O.P. orange color (SC3–55 mm) | 1.41 |
| A.M.C.O.P. red color (ΦS3–55 mm) | 1.75 |
| HealthyStart (Ortho-Tain) (7–11 PAD) | 0.97 |
| Trainer for Kids (T4K) | 2.55 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quinzi, V.; Gallusi, G.; Carli, E.; Pepe, F.; Rastelli, E.; Tecco, S. Elastodontic Devices in Orthodontics: An In-Vitro Study on Mechanical Deformation under Loading. Bioengineering 2022, 9, 282. https://doi.org/10.3390/bioengineering9070282
Quinzi V, Gallusi G, Carli E, Pepe F, Rastelli E, Tecco S. Elastodontic Devices in Orthodontics: An In-Vitro Study on Mechanical Deformation under Loading. Bioengineering. 2022; 9(7):282. https://doi.org/10.3390/bioengineering9070282
Chicago/Turabian StyleQuinzi, Vincenzo, Gianni Gallusi, Elisabetta Carli, Francesca Pepe, Elena Rastelli, and Simona Tecco. 2022. "Elastodontic Devices in Orthodontics: An In-Vitro Study on Mechanical Deformation under Loading" Bioengineering 9, no. 7: 282. https://doi.org/10.3390/bioengineering9070282