
Detection of Aortic Valve Opening and Estimation of Pre-Ejection Period in Forcecardiography Recordings

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
- Peak of atrial systole (AS);
- Mitral valve closure (MC);
- Isovolumic movement (IM);
- Aortic valve opening (AO);
- Isotonic contraction (IC);
- Peak of rapid systolic ejection (RE);
- Aortic valve closure (AC);
- Mitral valve opening (MO);
- Peak of rapid systolic filling (RF);
2. Materials and Methods
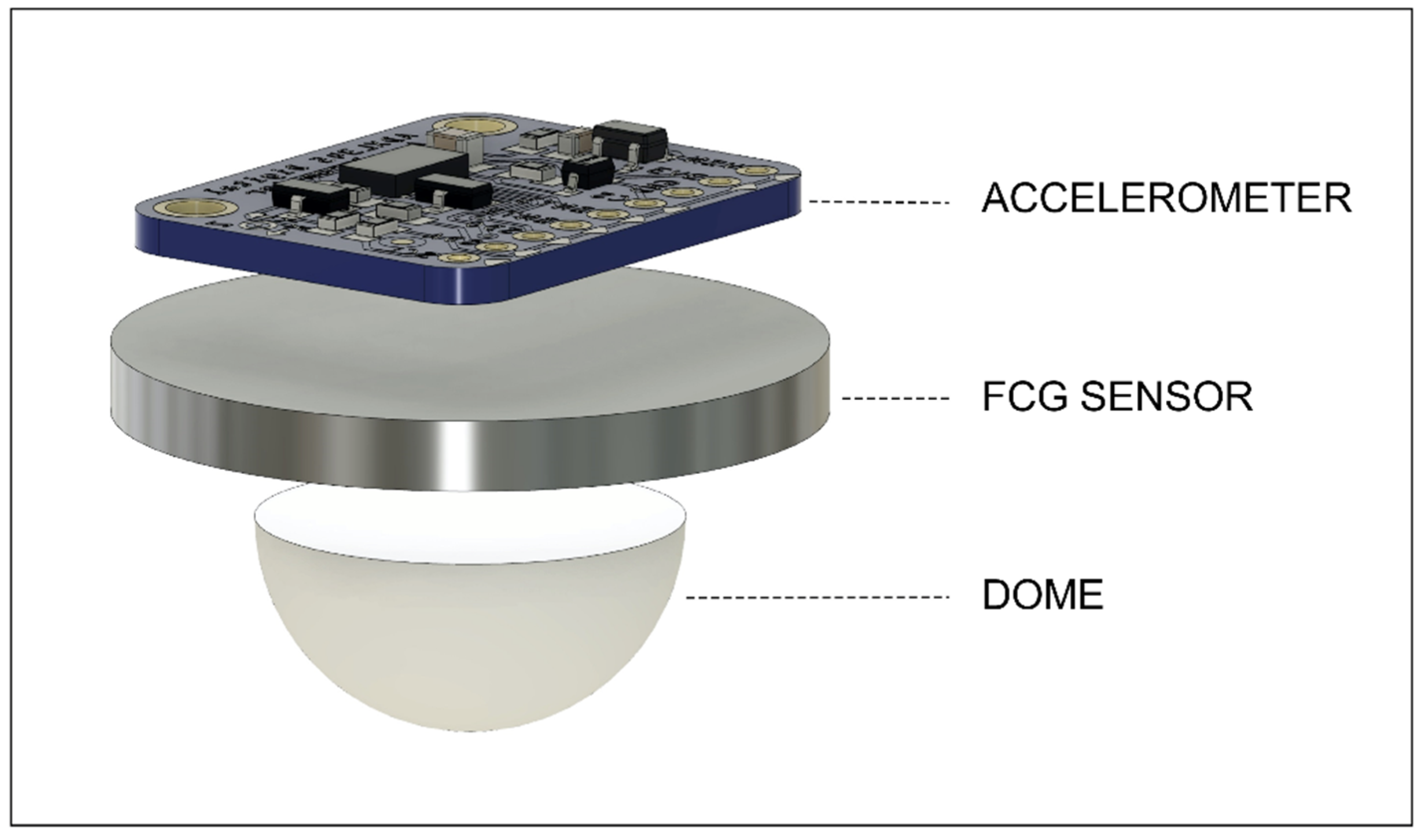
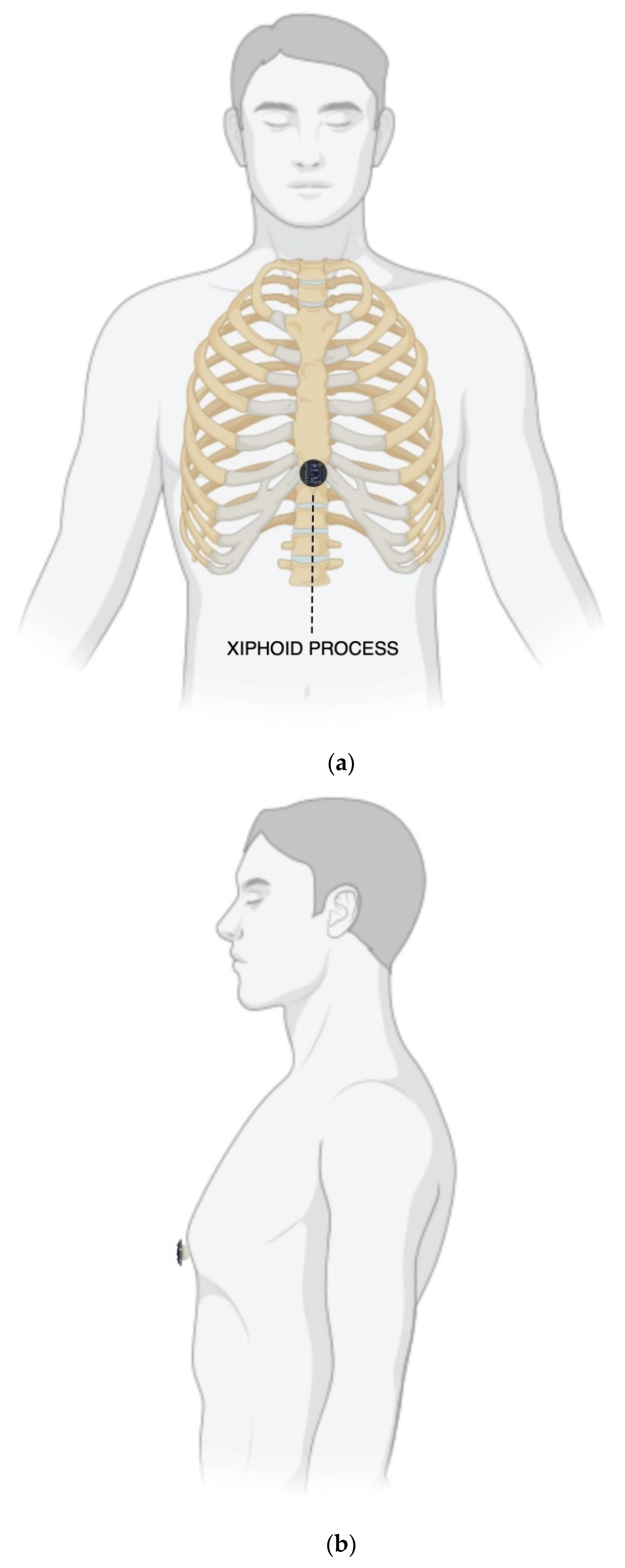
2.1. Measurement Setup and Protocol
2.2. Signal Processing
2.3. Morphological Comparison between FCG and SCG Signals
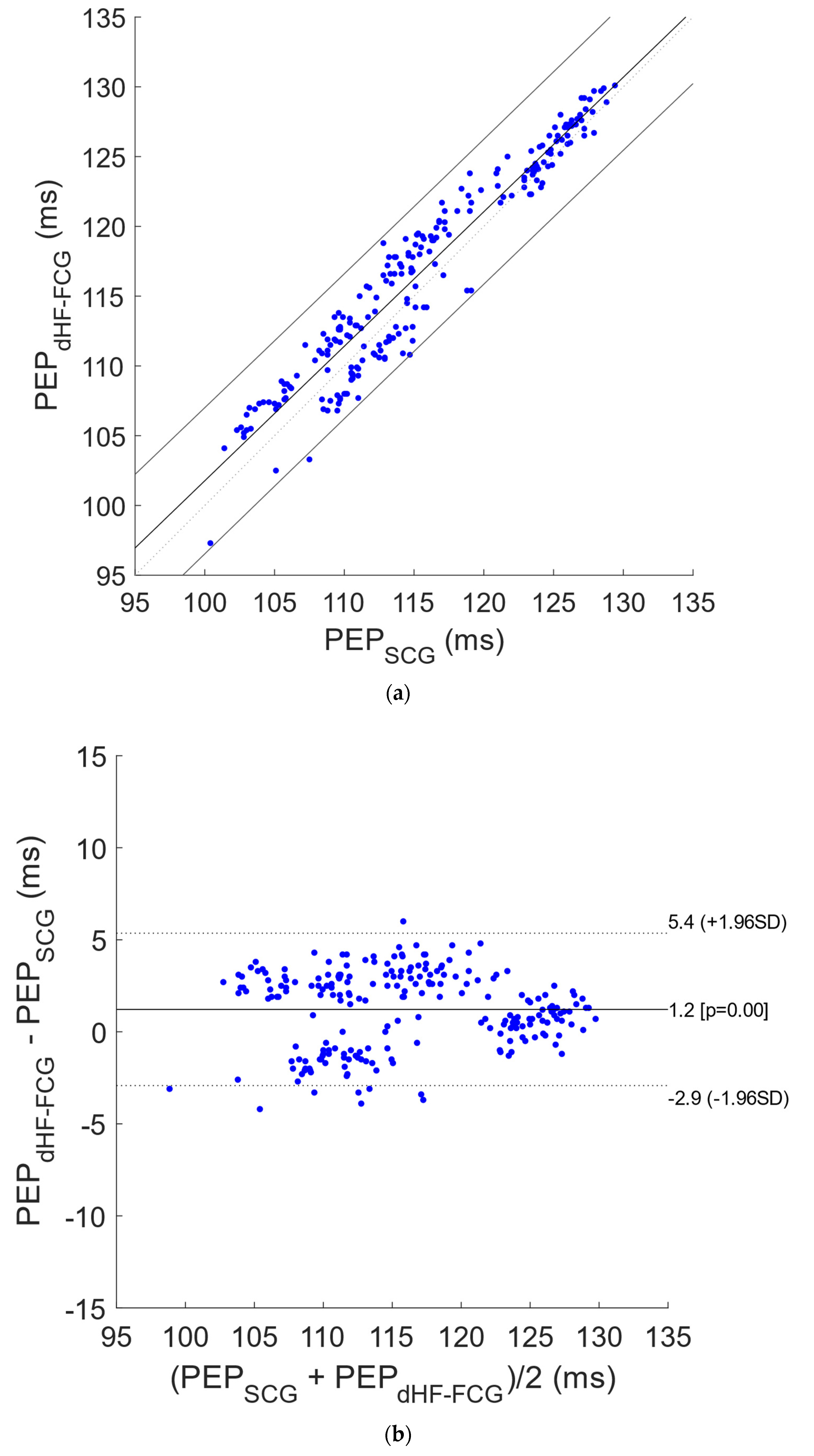
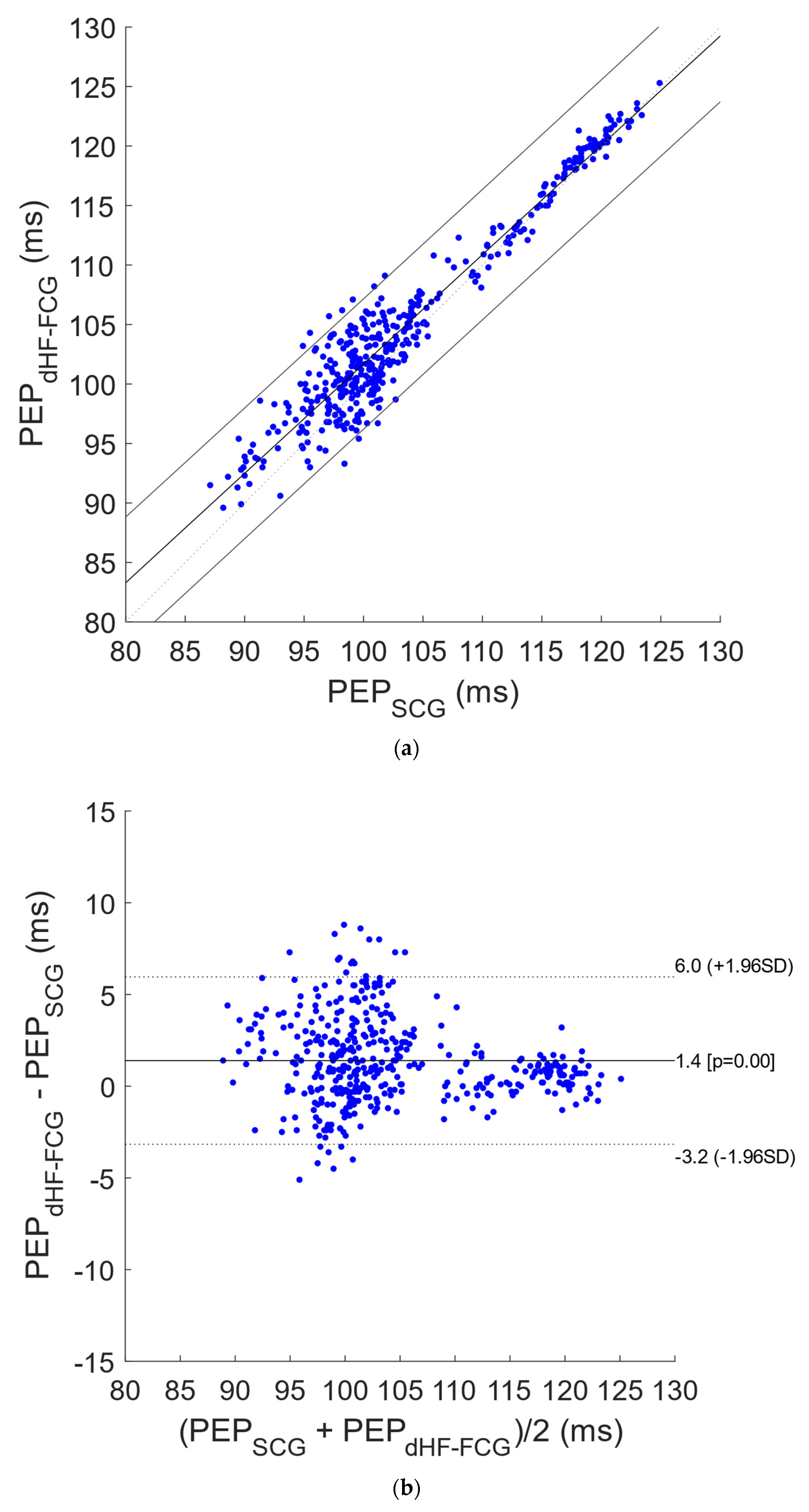
2.4. Statistical Analyses on Pre-Ejection Period Estimates
3. Results
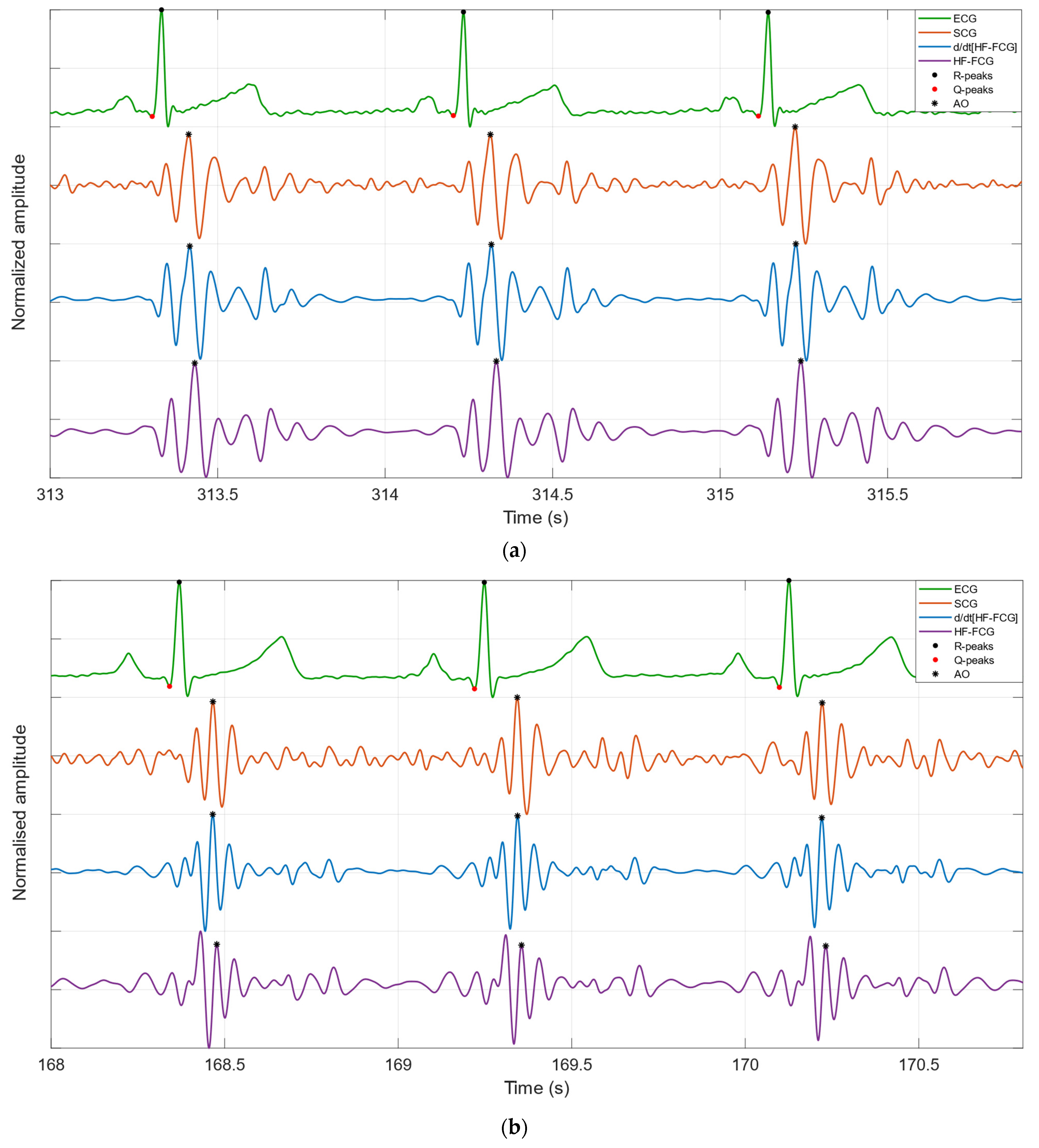
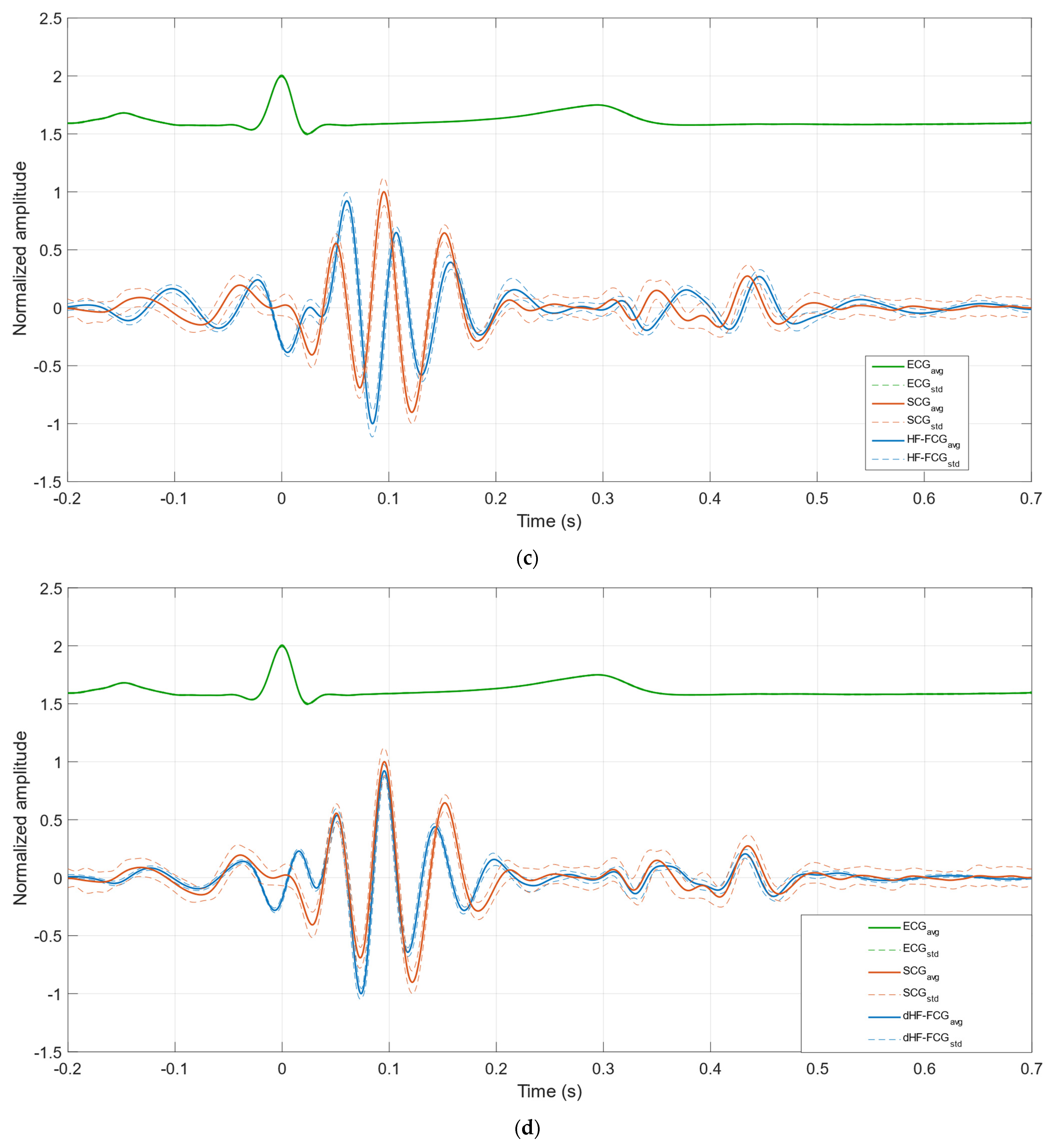
3.1. Morphological Comparison between FCG and SCG Signals
3.2. Statistical Analyses on Pre-Ejection Period Estimates
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviation
| Abbreviation | Definition |
| AC | aortic valve closure |
| AO | aortic valve opening |
| AS | peak of atrial systole |
| BCG | ballistocardiography |
| dHF-FCG | first derivative of HF-FCG |
| ECG | electrocardiogram |
| FCG | forcecardiography |
| FRG | forcerespirogram |
| GCG | gyrocardiography |
| HF-FCG | high-frequency component of FCG signal |
| HS-FCG | heart sounds component of FCG signal |
| IC | isotonic contraction |
| IM | isovolumic movement |
| KCG | kinocardiography |
| LF-FCG | low-frequency component of FCG signal |
| MC | mitral valve closure |
| MEMS | microelectromechanical systems |
| MO | mitral valve opening |
| PCG | phonocardiography |
| PEP | pre-ejection period |
| RE | peak of rapid systolic ejection |
| RF | peak of rapid systolic filling |
| SCG | seismocardiography |
References
- Zanetti, J.; Salerno, D. Seismocardiography: A new technique for recording cardiac vibrations. Concept, method, and initial observations. J. Cardiovasc. Technol. 1990, 9, 111–118. [Google Scholar]
- Inan, O.T.; Migeotte, P.F.; Park, K.S.; Etemadi, M.; Tavakolian, K.; Casanella, R.; Zanetti, J.; Tank, J.; Funtova, I.; Prisk, G.K.; et al. Ballistocardiography and Seismocardiography: A Review of Recent Advances. IEEE J. Biomed. Health Inform. 2015, 19, 1414–1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taebi, A.; Solar, B.E.; Bomar, A.J.; Sandler, R.H.; Mansy, H.A. Recent Advances in Seismocardiography. Vibration 2019, 2, 64–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gordon, J.W. On certain molar movements of the human body produced by the circulation of blood. J. Anat. Physiol. 1877, 11, 533. [Google Scholar] [PubMed]
- Starr, I. The relation of the ballistocardiogram to cardiac function. Am. J. Cardiol. 1958, 2, 737–747. [Google Scholar] [CrossRef]
- Sadek, I.; Biswas, J.; Abdulrazak, B. Ballistocardiogram signal processing: A review. Health Inf. Sci. Syst. 2019, 7, 10. [Google Scholar] [CrossRef]
- Jafari Tadi, M.; Lehtonen, E.; Saraste, A.; Tuominen, J.; Koskinen, J.; Teräs, M.; Airaksinen, J.; Pänkäälä, M.; Koivisto, T. Gyrocardiography: A New Non-invasive Monitoring Method for the Assessment of Cardiac Mechanics and the Estimation of Hemodynamic Variables. Sci. Rep. 2017, 7, 6823. [Google Scholar] [CrossRef]
- Sieciński, S.; Kostka, P.S.; Tkacz, E.J. Gyrocardiography: A Review of the Definition, History, Waveform Description, and Applications. Sensors 2020, 20, 6675. [Google Scholar] [CrossRef]
- Hossein, A.; Mirica, D.C.; Rabineau, J.; Del Rio, J.I.; Morra, S.; Gorlier, D.; Nonclercq, A.; van de Borne, P.; Migeotte, P.F. Accurate Detection of Dobutamine-induced Haemodynamic Changes by Kino-Cardiography: A Randomised Double-Blind Placebo-Controlled Validation Study. Sci. Rep. 2019, 9, 10479. [Google Scholar] [CrossRef] [Green Version]
- Hossein, A.; Rabineau, J.; Gorlier, D.; Del Rio, J.I.J.; van de Borne, P.; Migeotte, P.-F.; Nonclercq, A. Kinocardiography Derived from Ballistocardiography and Seismocardiography Shows High Repeatability in Healthy Subjects. Sensors 2021, 21, 815. [Google Scholar] [CrossRef]
- Crow, R.S.; Hannan, P.; Jacobs, D.; Hedquist, L.; Salerno, D.M. Relationship between Seismocardiogram and Echocardiogram for Events in the Cardiac Cycle. Am. J. Noninvasive Cardiol. 1994, 8, 39–46. [Google Scholar] [CrossRef]
- Lin, W.; Chou, W.; Chang, P.; Chou, C.; Wen, M.; Ho, M.; Lee, M. Identification of Location Specific Feature Points in a Cardiac Cycle Using a Novel Seismocardiogram Spectrum System. IEEE J. Biomed. Health Inform. 2018, 22, 442–449. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, K.; Schmidt, S.E.; Jensen, A.S.; Søgaard, P.; Struijk, J.J. Definition of Fiducial Points in the Normal Seismocardiogram. Sci. Rep. 2018, 8, 15455. [Google Scholar] [CrossRef] [Green Version]
- Dehkordi, P.; Khosrow-Khavar, F.; Di Rienzo, M.; Inan, O.T.; Schmidt, S.E.; Blaber, A.P.; Sørensen, K.; Zakeri, V.; Lombardi, P.; Shandhi, M.M.H.; et al. Comparison of Different Methods for Estimating Cardiac Timings: A Comprehensive Multimodal Echocardiography Investigation. Front. Physiol. 2019, 10, 1057. [Google Scholar] [CrossRef] [PubMed]
- Gurev, V.; Tavakolian, K.; Constantino, J.; Kaminska, B.; Blaber, A.P.; Trayanova, N.A. Mechanisms Underlying Isovolumic Contraction and Ejection Peaks in Seismocardiogram Morphology. J. Med. Biol. Eng. 2012, 32, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Tadi, M.; Koivisto, T.; Pankaala, M.; Paasio, A.; Knuutila, T.; Teras, M.; Hanninen, P. A new algorithm for segmentation of cardiac quiescent phases and cardiac time intervals using seismocardiography. In Proceedings of the Sixth International Conference on Graphic and Image Processing (ICGIP 2014), Beijing, China, 24–26 October 2015; p. 94432. [Google Scholar] [CrossRef]
- Ashouri, H.; Inan, O.T. Automatic detection of seismocardiogram sensor misplacement for robust pre-ejection period estimation in unsupervised settings. IEEE Sens. J. 2017, 17, 3805–3813. [Google Scholar] [CrossRef] [PubMed]
- Zia, J.S.; Kimball, J.; Hersek, S.; Shandhi, M.; Semiz, B.; Inan, O.T. Unified Framework for Quality Indexing and Classification of Seismocardiogram Signals. IEEE J. Biomed. Health Inform. 2019, 24, 1080–1092. [Google Scholar] [CrossRef]
- Zia, J.S.; Kimball, J.; Hersek, S.; Inan, O.T. Modeling Consistent Dynamics of Cardiogenic Vibrations in Low-Dimensional Subspace. IEEE J. Biomed. Health Inform. 2020, 24, 1887–1898. [Google Scholar] [CrossRef]
- Zia, J.S.; Kimball, J.; Rozell, C.J.; Inan, O.T. Harnessing the Manifold Structure of Cardiomechanical Signals for Physiological Monitoring during Hemorrhage. IEEE Transac. Biomed. Eng. 2020, 68, 1759–1767. [Google Scholar] [CrossRef]
- Andreozzi, E.; Fratini, A.; Esposito, D.; Naik, G.; Polley, C.; Gargiulo, G.D.; Bifulco, P. Forcecardiography: A Novel Technique to Measure Heart Mechanical Vibrations onto the Chest Wall. Sensors 2020, 20, 3885. [Google Scholar] [CrossRef]
- Andreozzi, E.; Centracchio, J.; Punzo, V.; Esposito, D.; Polley, C.; Gargiulo, G.D.; Bifulco, P. Respiration Monitoring via Forcecardiography Sensors. Sensors 2021, 21, 3996. [Google Scholar] [CrossRef] [PubMed]
- Andreozzi, E.; Gargiulo, G.D.; Esposito, D.; Bifulco, P. A Novel Broadband Forcecardiography Sensor for Simultaneous Monitoring of Respiration, Infrasonic Cardiac Vibrations and Heart Sounds. Front. Physiol. 2021, 12, 725716. [Google Scholar] [CrossRef] [PubMed]
- Esposito, D.; Andreozzi, E.; Fratini, A.; Gargiulo, G.D.; Savino, S.; Niola, V.; Bifulco, P. A Piezoresistive Sensor to Measure Muscle Contraction and Mechanomyography. Sensors 2018, 18, 2553. [Google Scholar] [CrossRef] [Green Version]
- Esposito, D.; Andreozzi, E.; Gargiulo, G.D.; Fratini, A.; D’Addio, G.; Naik, G.R.; Bifulco, P. A Piezoresistive Array Armband With Reduced Number of Sensors for Hand Gesture Recognition. Front. Neurorobotics 2020, 13, 114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savitzky, A.; Golay, M.J.E. Smoothing and Differentiation of Data by Simplified Least Squares Procedures. Anal. Chem. 1964, 36, 1627–1639. [Google Scholar] [CrossRef]
- Sedghamiz, H. BioSigKit: A Matlab Toolbox and Interface for Analysis of BioSignals. J. Open Source Softw. 2018, 3, 671. [Google Scholar] [CrossRef]
- Ran, K. Bland-Altman and Correlation Plot, MATLAB Central File Exchange. 2020. Available online: https://www.mathworks.com/matlabcentral/fileexchange/45049-bland-altman-and-correlation-plot (accessed on 28 May 2020).
- Su, H.-M.; Lin, T.-H.; Hsu, P.-C.; Chu, C.-Y.; Lee, W.-H.; Chen, S.-C.; Lee, C.-S.; Voon, W.-C.; Lai, W.-T.; Sheu, S.-H. A Comparison between Brachial and Echocardiographic Systolic Time Intervals. PLoS ONE 2013, 8, e55840. [Google Scholar] [CrossRef] [Green Version]
- Noda, K.; Endo, H.; Kadosaka, T.; Nakata, T.; Watanabe, T.; Terui, Y.; Kajitani, S.; Monnma, Y.; Sato, K.; Kanazawa, M.; et al. Comparison of the measured pre-ejection periods and left ventricular ejection times between Echocardiography and impedance cardiography for optimizing cardiac resynchronization therapy. J. Arrhythmia 2017, 33, 130–133. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | HF-FCG vs. SCG | dHF-FCG vs. SCG | ||
|---|---|---|---|---|
| NCC | Lag (ms) | NCC | Lag (ms) | |
| #1 | 0.8333 | 18.6 | 0.9107 | 1.2 |
| #2 | 0.7764 | 14.7 | 0.8988 | −2.2 |
| #3 | 0.7773 | 10.7 | 0.7998 | −1.2 |
| Subject | Heartbeats in ECG | Missed AO in SCG | Missed AO in dHF-FCG | |||
|---|---|---|---|---|---|---|
| Apnea | Quiet Breathing | Apnea | Quiet Breathing | Apnea | Quiet Breathing | |
| #1 | 112 | 200 | 0 | 0 | 0 | 0 |
| #2 | 54 | 118 | 0 | 0 | 0 | 0 |
| #3 | 61 | 106 | 0 | 1 | 0 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Centracchio, J.; Andreozzi, E.; Esposito, D.; Gargiulo, G.D.; Bifulco, P. Detection of Aortic Valve Opening and Estimation of Pre-Ejection Period in Forcecardiography Recordings. Bioengineering 2022, 9, 89. https://doi.org/10.3390/bioengineering9030089
Centracchio J, Andreozzi E, Esposito D, Gargiulo GD, Bifulco P. Detection of Aortic Valve Opening and Estimation of Pre-Ejection Period in Forcecardiography Recordings. Bioengineering. 2022; 9(3):89. https://doi.org/10.3390/bioengineering9030089
Chicago/Turabian StyleCentracchio, Jessica, Emilio Andreozzi, Daniele Esposito, Gaetano Dario Gargiulo, and Paolo Bifulco. 2022. "Detection of Aortic Valve Opening and Estimation of Pre-Ejection Period in Forcecardiography Recordings" Bioengineering 9, no. 3: 89. https://doi.org/10.3390/bioengineering9030089