
Feasibility of an Application-Based Outpatient Rehabilitation Program for Stroke Survivors: Acceptability and Preliminary Results for Patient-Reported Outcomes
 , , and
, , and
Abstract
:1. Background
2. Methods
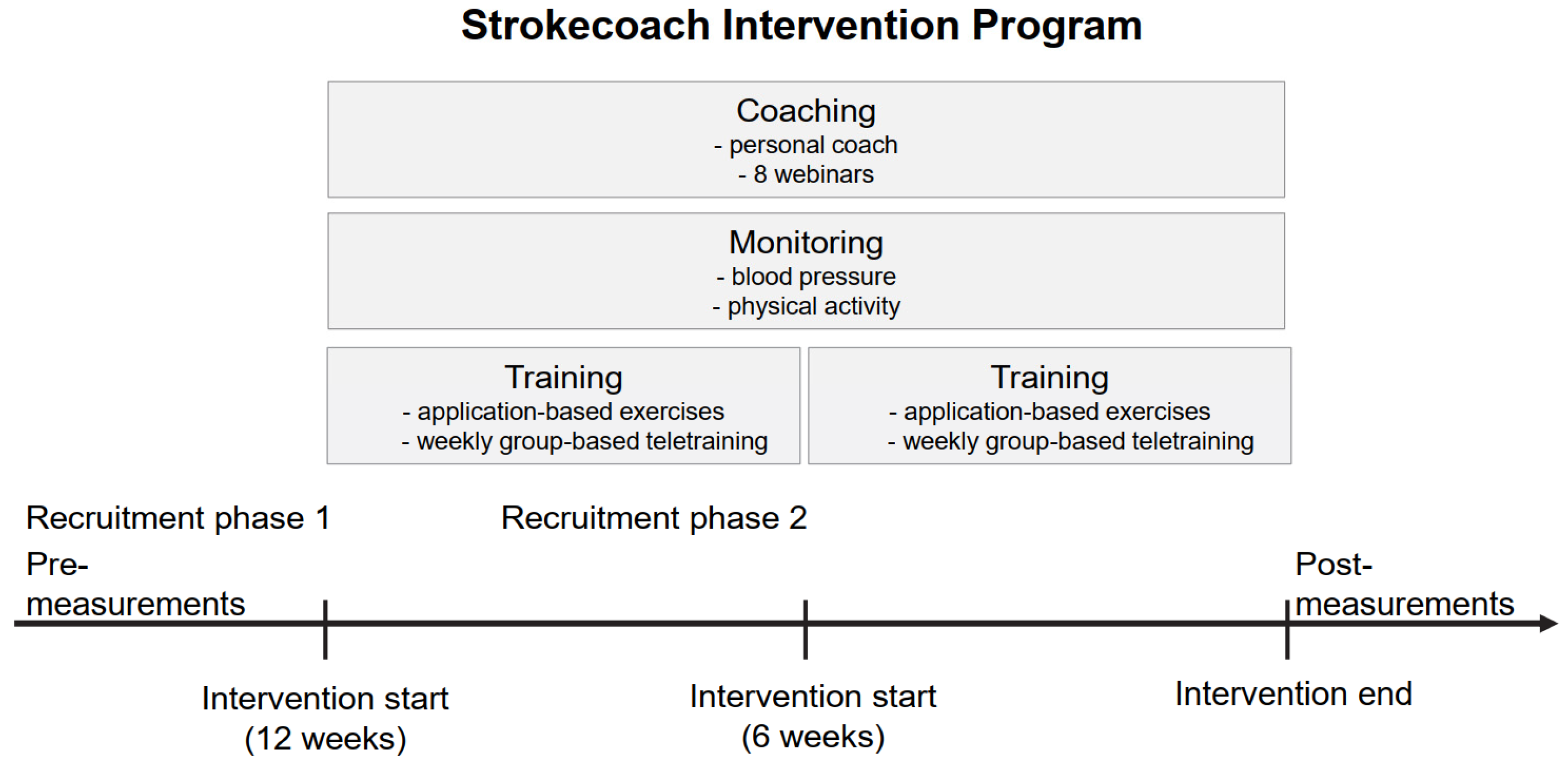
2.1. Study Design
2.2. Participants and Setting of the SIP
2.3. Participant Recruitment of the SIP
2.4. The Strokecoach Intervention Program

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1. Brief name |
|
| 2. Why Describe |
|
| 3. What Materials |
|
| 4. Procedures |
|
| 5. Who provided |
|
| 6. How |
|
| 7. Where |
|
| 8. When and how much |
|
| 9. Tailoring |
|
| 10. Modifications |
|
| 11. How well: planned |
|
| 12. Actual: |
|
2.5. Outcome Measures
- ▪
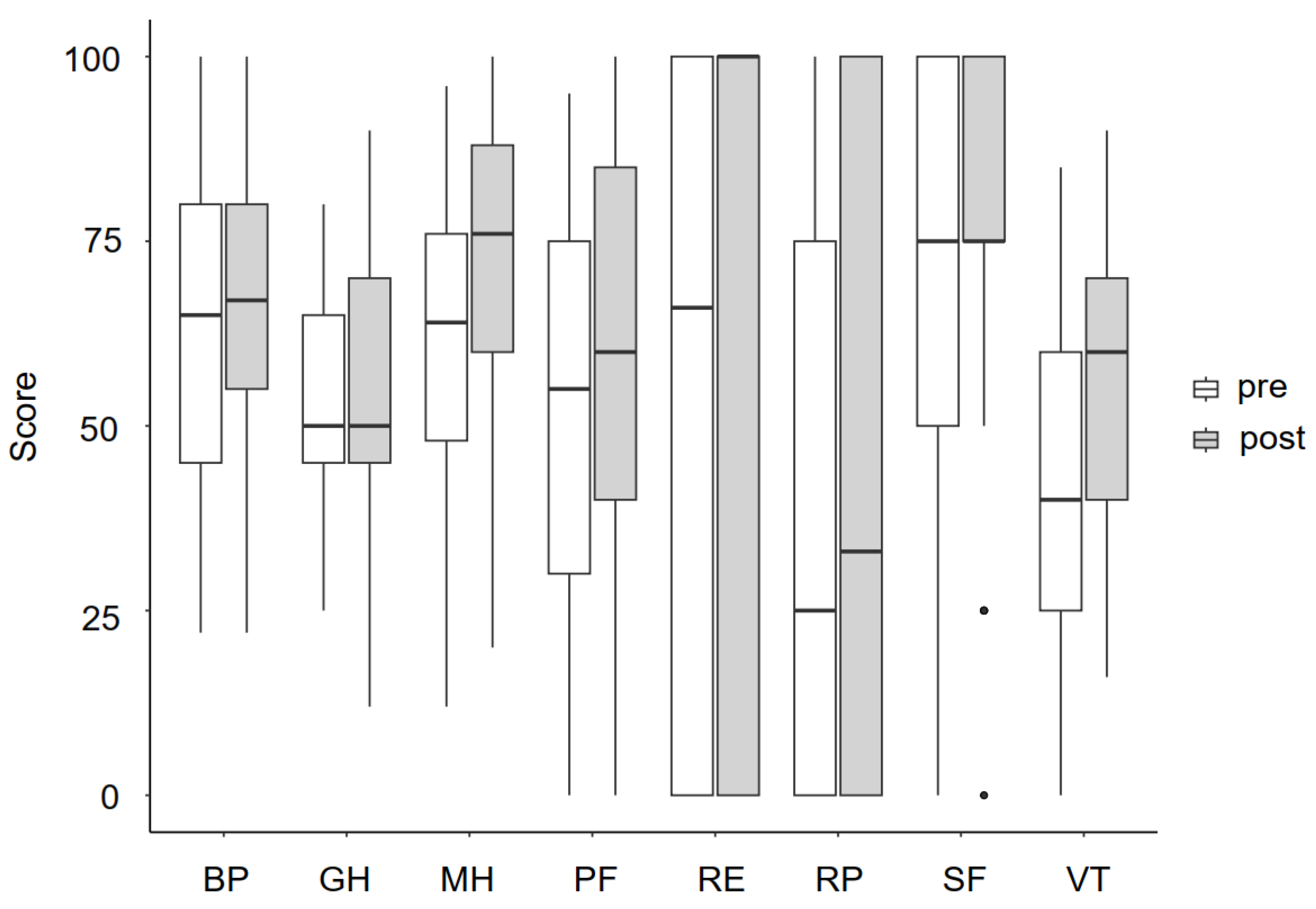
- Health-related quality of life was determined using the German version of the 36-item Short Form Survey (SF-36). The SF-36 consists of eight subscales: physical functioning, role limitations due to physical health, role limitations due to emotional problems, energy/fatigue, mental health, social functioning, pain, and general health. Each consists of different questions and the score ranges from 0 to 100, with higher values representing better health-related quality of life [39].
- ▪
- ▪
- The 4-Metre Walking test was used to measure habitual gait speed. Although assessments of walking speed are common, different protocols are used [43]. In our study, patients were instructed to measure the time for walking a distance of 4 m. They started from a resting position and repeated the test four times, as previously described for people with COPD [41]. The mean was calculated.
- ▪
- Muscle strength was evaluated by self-performed exercises based on the Medical Research Council Scale [44]. Participants rated their performance for shoulder flexion, elbow flexion, wrist extension, hip flexion, knee extension and foot dorsiflexion bilaterally on a 6-point rating scale.
- ▪
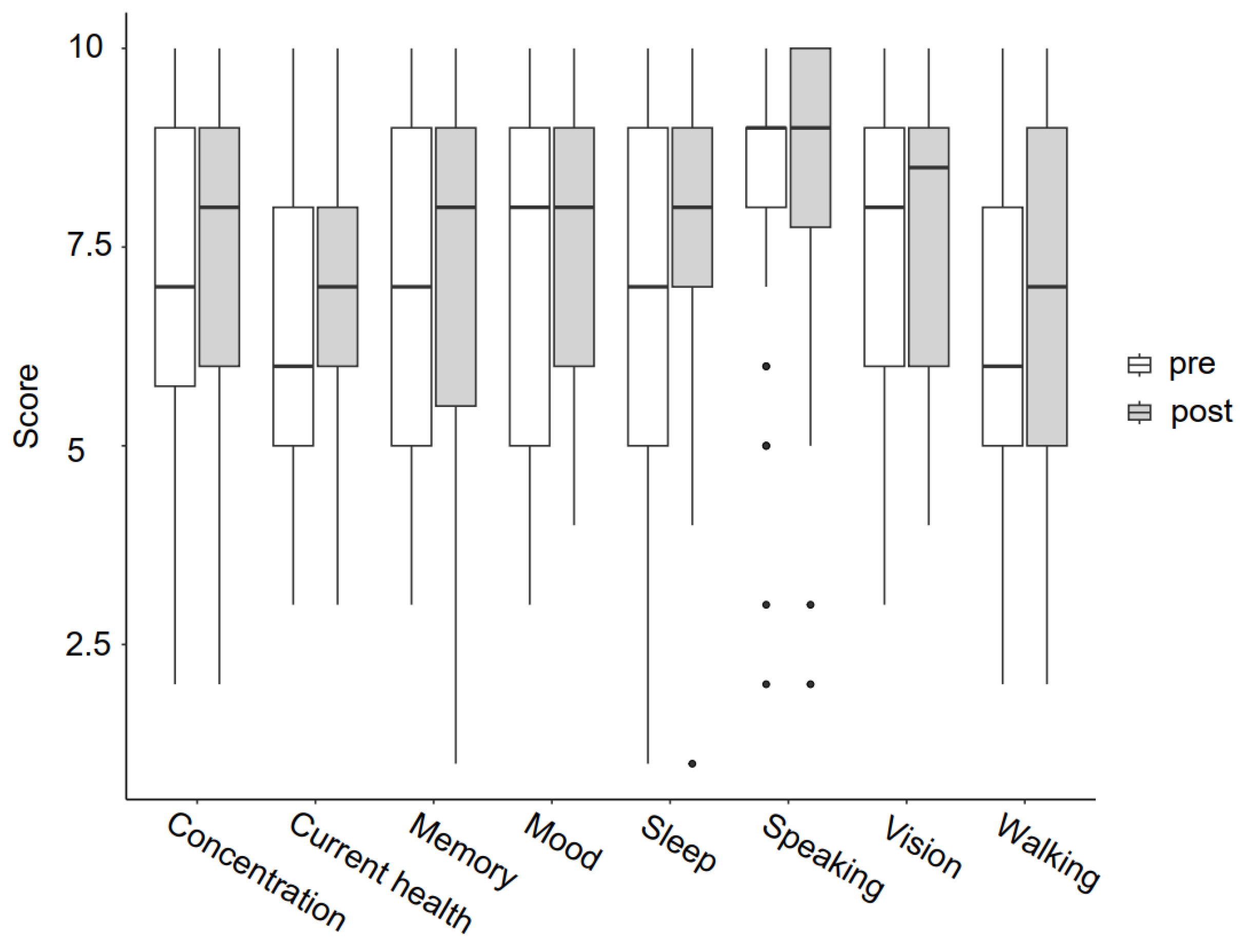
- General health questions included the self-rating of capabilities walking, speaking, vision, memory, concentration, mood, sleep and current health on a 10-point visual analogue scale with verbalized endpoints (very bad to very good).
- ▪
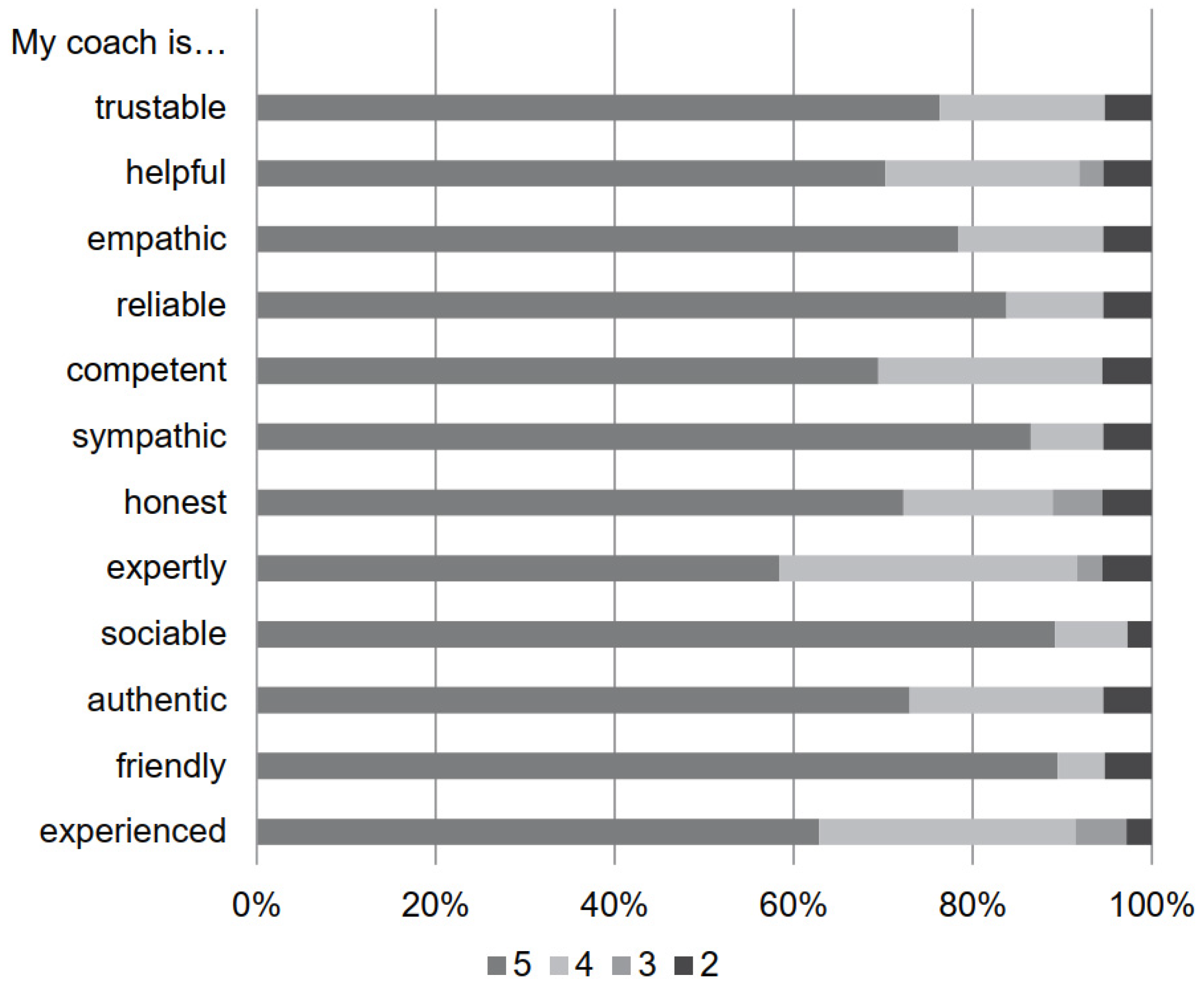
- For the evaluation of coaching aspects, online questionnaires were sent. Webinar attendance was evaluated dichotomously. The questions about their webinar experience were rated on a visual analogue scale (from “not at all useful” to “very useful”). Based on the Counselor Rating Form–Short Version (CRF-S) [45], the coach was rated on different items (friendly, experienced, authentic, sociable, competent, honest, sympathetic, reliable, empathic, helpful, expertly, trustworthy) with 0 = not at all to 5 = very much.
2.6. Data Analysis and Statistics
3. Results
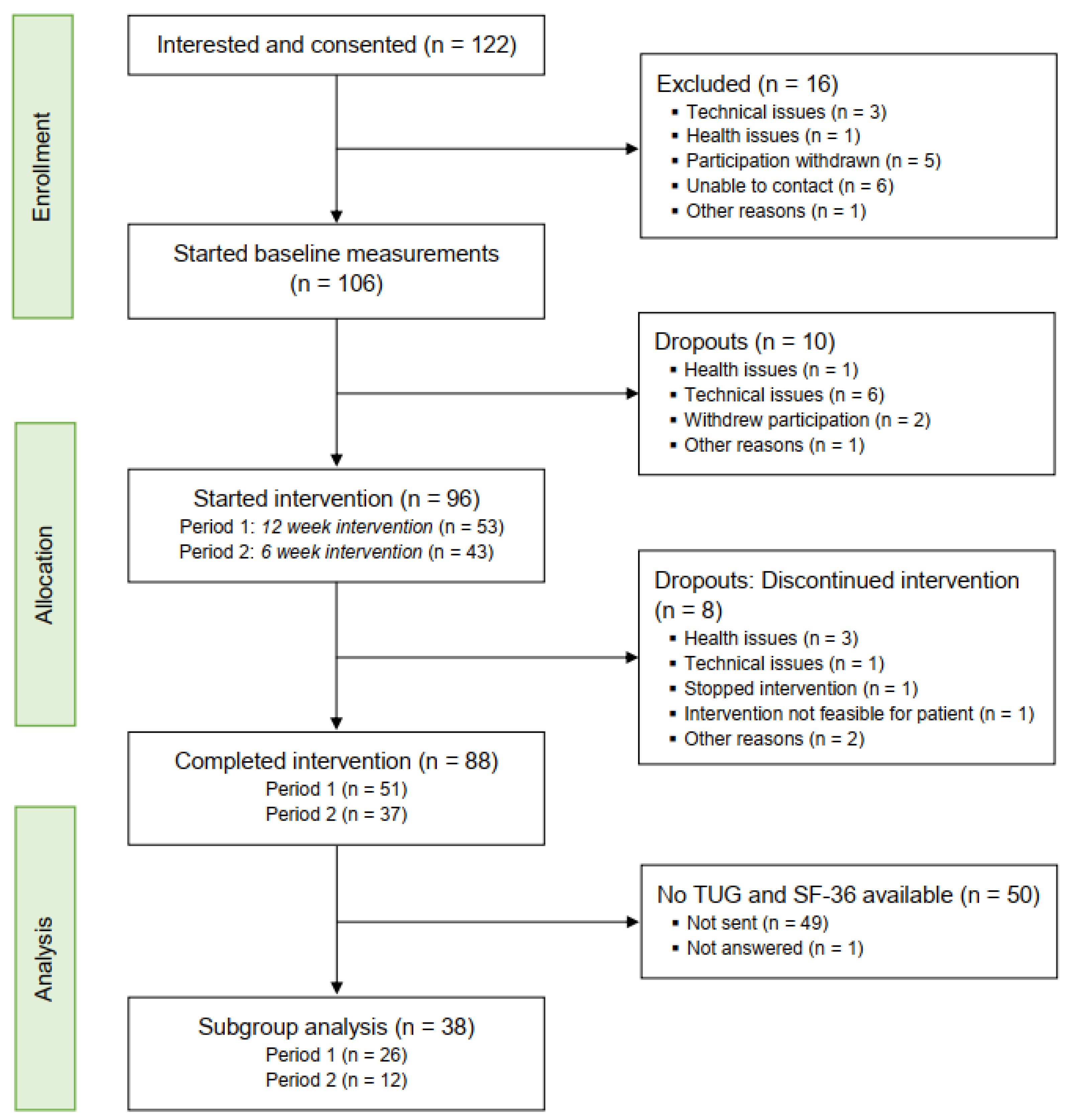
3.1. Feasiblity of the Stroke Intervention Program
3.2. Acceptability of Using the Strokecoach Intervention
3.3. Patient-Reported Outcome Measures and Performance-Based Measures
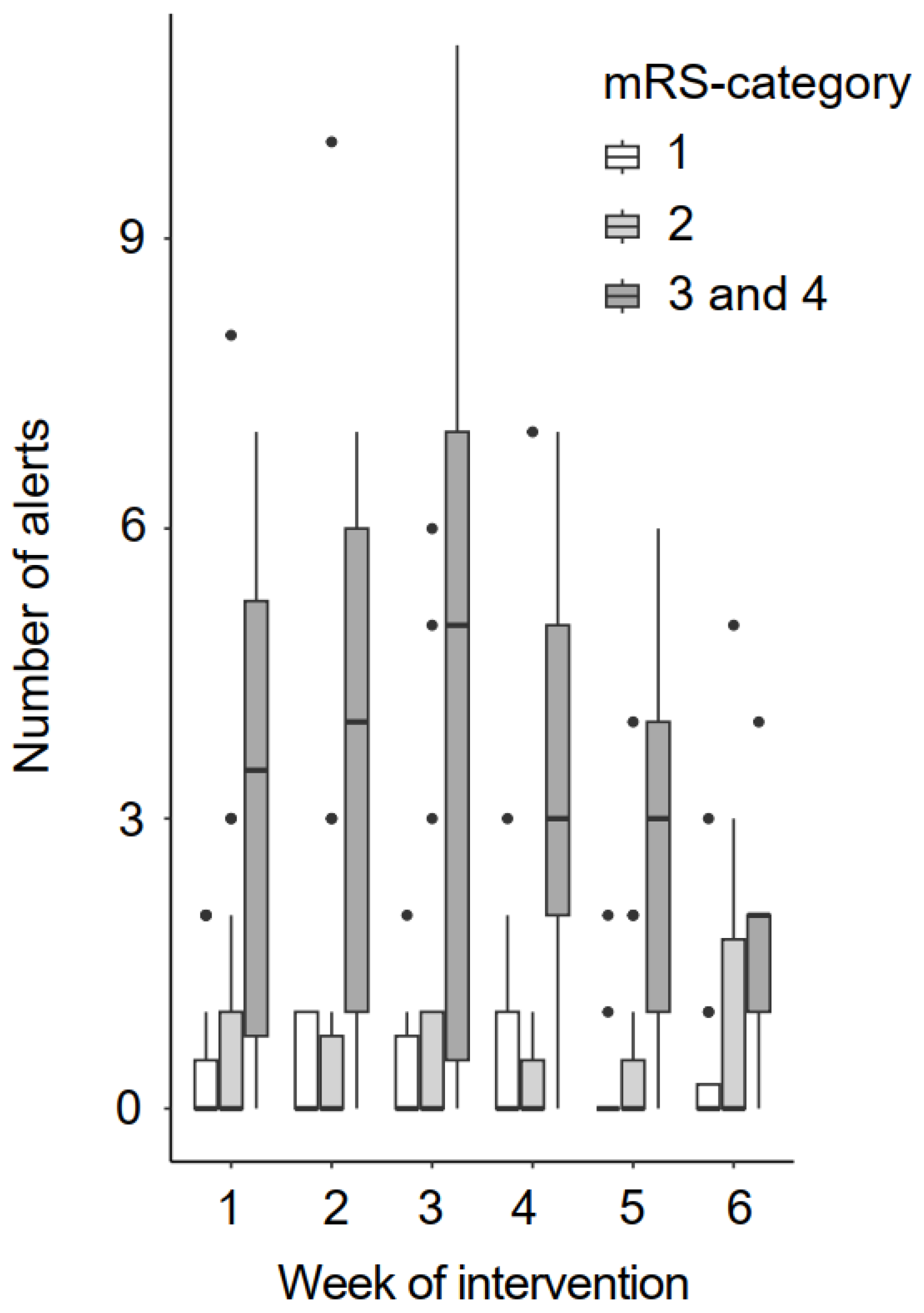
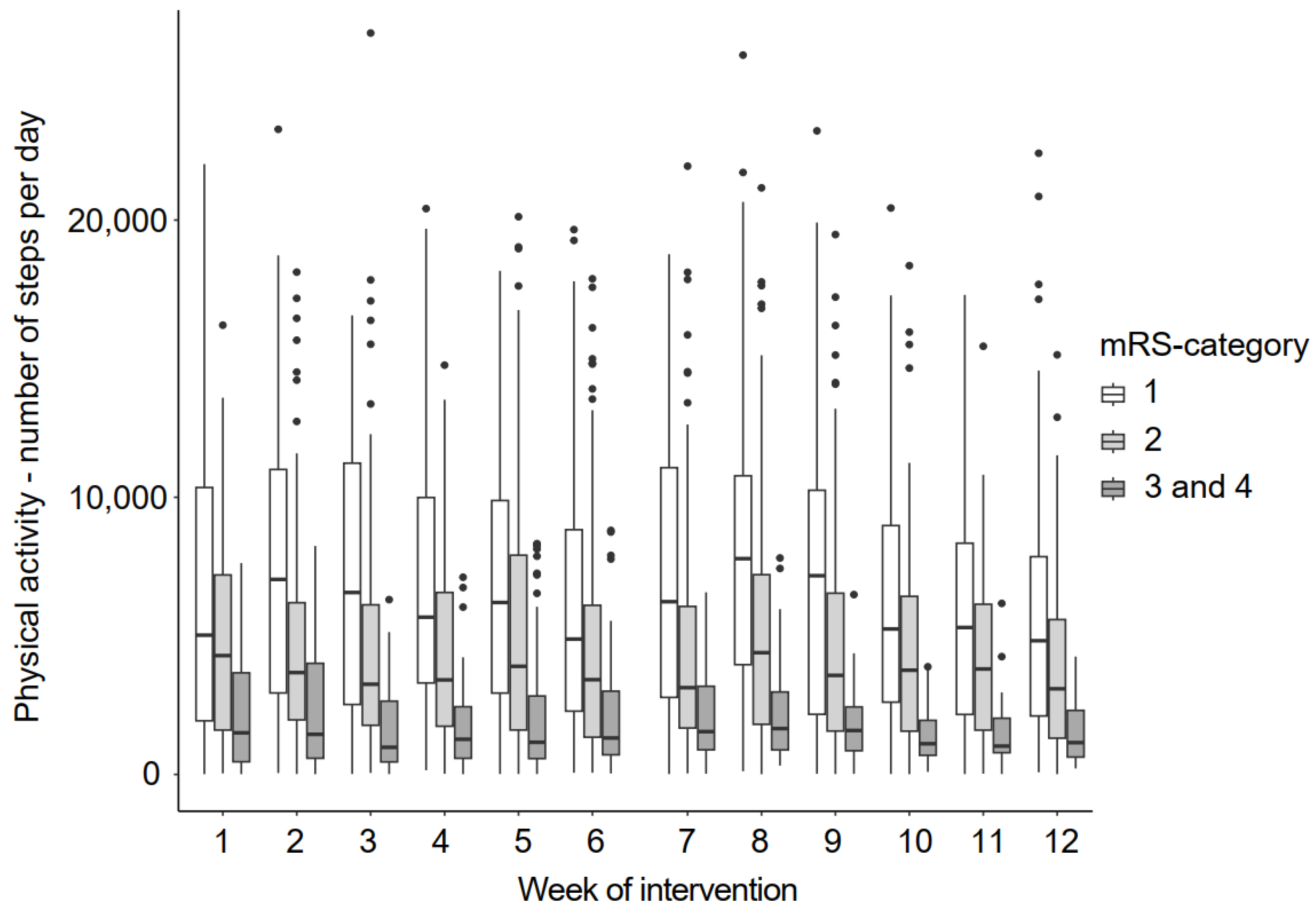
3.4. Physiological Parameters and Physical Activity Patterns
4. Discussion
4.1. Strengths and Limitations
4.2. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| SD | Standard deviation |
| SIP | Strokecoach Intervention Program |
| TUG | Timed Up and Go |
References
- Katan, M.; Luft, A. Global burden of stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [CrossRef]
- Krishnamurthi, R.V.; Ikeda, T.; Feigin, V.L. Global, Regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: A systematic analysis of the global burden of disease study 2017. Neuroepidemiology 2020, 54, 171–179. [Google Scholar] [CrossRef]
- Donkor, E.S. Stroke in the 21(st) century: A snapshot of the burden, epidemiology, and quality of life. Stroke Res. Treat. 2018, 2018, 3238165. [Google Scholar]
- Lopez-Espuela, F.; Zamorano, J.D.P.; Ramírez-Moreno, J.M.; Jiménez-Caballero, P.E.; Portilla-Cuenca, J.C.; Lavado-García, J.M.; Casado-Naranjo, I. Determinants of quality of life in stroke survivors after 6 months, from a comprehensive stroke unit. Biol. Res. Nurs. 2015, 17, 461–468. [Google Scholar] [CrossRef]
- Schindel, D.; Schneider, A.; Grittner, U.; Jöbges, M.; Schenk, L. Quality of life after stroke rehabilitation discharge: A 12-month longitudinal study. Disabil. Rehabil. 2019, 43, 2332–2341. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.J.; Chin, S.L.; Rangarajan, S.; Xavier, D.; Liu, L.; Zhang, H.; Rao-Melacini, P.; Zhang, X.; Pais, P.; Agapay, S.; et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): A case-control study. Lancet 2016, 388, 761–775. [Google Scholar] [CrossRef] [PubMed]
- Boehme, A.K.; Esenwa, C.; Elkind, M.S. Stroke risk factors, genetics, and prevention. Circ. Res. 2017, 120, 472–495. [Google Scholar] [CrossRef]
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Guilbert, J.J. The world health report 2002—Reducing risks, promoting healthy life. Educ. Health (Abingdon) 2003, 16, 230. [Google Scholar] [PubMed]
- Katsanos, A.H.; Filippatou, A.; Manios, E.; Deftereos, S.; Parissis, J.; Frogoudaki, A.; Vrettou, A.R.; Ikonomidis, I.; Pikilidou, M.; Kargiotis, O.; et al. Blood pressure reduction and secondary stroke prevention: A systematic review and metaregression analysis of randomized clinical trials. Hypertension 2017, 69, 171–179. [Google Scholar] [CrossRef]
- Lawes, C.M.M.; Bennett, D.A.; Feigin, V.L.; Rodgers, A. Blood pressure and stroke: An overview of published reviews. Stroke 2004, 35, 1024. [Google Scholar] [CrossRef]
- MacMahon, S.; Peto, R.; Collins, R.; Godwin, J.; Cutler, J.; Sorlie, P.; Abbott, R.; Neaton, J.; Dyer, A.; Stamler, J. Blood pressure, stroke, and coronary heart disease *1Part 1, prolonged differences in blood pressure: Prospective observational studies corrected for the regression dilution bias. Lancet 1990, 335, 765–774. [Google Scholar] [CrossRef]
- Howard, V.J.; McDonnell, M.N. Physical activity in primary stroke prevention: Just do it! Stroke 2015, 46, 1735–1739. [Google Scholar] [CrossRef] [PubMed]
- Prior, P.L.; Suskin, N. Exercise for stroke prevention. Stroke Vasc. Neurol. 2018, 3, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Reinholdsson, M.; Palstam, A.; Sunnerhagen, K.S. Prestroke physical activity could influence acute stroke severity (part of PAPSIGOT). Neurology 2018, 91, e146–e1467. [Google Scholar] [CrossRef] [PubMed]
- Calugi, S.; Taricco, M.; Rucci, P.; Fugazzaro, S.; Stuart, M.; Dallolio, L.; Pillastrini, P.; Fantini, M.P. Effectiveness of adaptive physical activity combined with therapeutic patient education in stroke survivors at twelve months: A non-randomized parallel group study. Eur. J. Phys. Rehabil. Med. 2015, 52, 72–80. [Google Scholar] [PubMed]
- Towfighi, A.; Hill, V.A. Modifiable risk factors for stroke and strategies for stroke prevention. Semin. Neurol. 2017, 37, 237–258. [Google Scholar] [CrossRef] [PubMed]
- Grau-Pellicer, M.; Chamarro-Lusar, A.; Medina-Casanovas, J.; Ferrer, B.-C.S. Walking speed as a predictor of community mobility and quality of life after stroke. Top. Stroke Rehabil. 2019, 26, 349–358. [Google Scholar] [CrossRef]
- Gordon, N.F.; Gulanick, M.; Costa, F.; Fletcher, G.; Franklin, B.A.; Roth, E.J.; Shephard, T.; American Heart Association Council on Clinical Cardiology; Subcommittee on Exercise; Cardiac Rehabilitation; et al. Physical activity and exercise recommendations for stroke survivors: An American Heart Association scientific statement from the Council on Clinical Cardiology, Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention; the Council on Cardiovascular Nursing; the Council on Nutrition, Physical Activity, and Metabolism; and the Stroke Council. Circulation 2004, 109, 2031–2041. [Google Scholar]
- Field, M.J.; Gebruers, N.; Sundaram, T.S.; Nicholson, S.; Mead, G. Physical activity after stroke: A systematic review and meta-analysis. ISRN Stroke 2013, 2013, 464176. [Google Scholar] [CrossRef]
- Yan, M.; Filieri, R.; Raguseo, E.; Gorton, M. Mobile apps for healthy living: Factors influencing continuance intention for health apps. Technol. Forecast. Soc. Chang. 2021, 166, 120644. [Google Scholar] [CrossRef]
- Ganesan, B.; Fong, K.N.K.; Meena, S.K.; Prasad, P.; Tong, R.K.Y. Impact of COVID-19 pandemic lockdown on occupational therapy practice and use of telerehabilitation—A cross sectional study. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 3614–3622. [Google Scholar]
- Hohberg, V.; Fuchs, R.; Gerber, M.; Künzler, D.; Paganini, S.; Faude, O. Blended care interventions to promote physical activity: A systematic review of randomized controlled trials. Sports Med. Open 2022, 8, 100. [Google Scholar] [CrossRef]
- Sheehy, L.; Taillon-Hobson, A.; Sveistrup, H.; Bilodeau, M.; Yang, C.; Welch, V.; Hossain, A.; Finestone, H. Home-based virtual reality training after discharge from hospital-based stroke rehabilitation: A parallel randomized feasibility trial. Trials 2019, 20, 333. [Google Scholar] [CrossRef]
- Chen, Y.; Abel, K.T.; Janecek, J.T.; Chen, Y.; Zheng, K.; Cramer, S.C. Home-based technologies for stroke rehabilitation: A systematic review. Int. J. Med. Inform. 2019, 123, 11–22. [Google Scholar] [CrossRef]
- Marsden, D.L.; Dunn, A.; Callister, R.; McElduff, P.; Levi, C.R.; Spratt, N.J. A home- and community-based physical activity program can improve the cardiorespiratory fitness and walking capacity of stroke survivors. J. Stroke Cerebrovasc. Dis. 2016, 25, 2386–2398. [Google Scholar] [CrossRef]
- Han, D.S.; Chuang, P.W.; Chiu, E.C. Effect of home-based reablement program on improving activities of daily living for patients with stroke: A pilot study. Medicine 2020, 99, e23512. [Google Scholar] [CrossRef] [PubMed]
- Brouns, B.; Meesters, J.J.L.; de Kloet, A.J.; Vlieland, T.P.M.V.; Houdijk, S.; Arwert, H.J.; van Bodegom-Vos, L. What works and why in the implementation of eRehabilitation after stroke—A process evaluation. Disabil. Rehabil. Assist. Technol. 2022, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Dutt, S. Importance of patient adherence and compliance in the present day. J. Bacteriol. Mycol. 2017, 4, 150–152. [Google Scholar] [CrossRef]
- Dayapoglu, N.; Tan, M. Quality of life in stroke patients. Neurol. India 2010, 58, 697–701. [Google Scholar] [PubMed]
- Morris, J.; Oliver, T.; Kroll, T.; MacGillivray, S. The importance of psychological and social factors in influencing the uptake and maintenance of physical activity after stroke: A structured review of the empirical literature. Stroke Res. Treat. 2011, 2012, 195249. [Google Scholar] [CrossRef]
- Lawless, M.T.; Tieu, M.; Feo, R.; Kitson, A.L. Theories of self-care and self-management of long-term conditions by community-dwelling older adults: A systematic review and meta-ethnography. Soc. Sci. Med. 2021, 287, 114393. [Google Scholar] [CrossRef] [PubMed]
- Strokelab, B.V. Strokecoach. [1.0.3]. 2021. Available online: https://apps.apple.com/de/app/strokecoach/id1567573365 (accessed on 21 November 2023).
- Strokecoach. Strokecoach Training Videos. 2023. Available online: https://www.youtube.com/channel/UCgMd30gcflLAO0UJnfWx51A (accessed on 22 November 2023).
- van Swieten, J.C.; Koudstaal, P.J.; Visser, M.C.; Schouten, H.J.; van Gijn, J. Interobserver agreement for the assessment of handicap in stroke patients. Stroke 1988, 19, 604–607. [Google Scholar] [CrossRef]
- Mancia, G.; De Backer, G.; Dominiczak, A.; Cifkova, R.; Fagard, R.; Germano, G.; Grassi, G.; Heagerty, A.M.; Kjeldsen, S.E.; Laurent, S.; et al. 2007 Guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur. Heart J. 2007, 28, 1462–1536. [Google Scholar] [CrossRef]
- European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension. J. Hypertens. 2003, 21, 1011–1053. [CrossRef]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Morfeld, M.; Kirchberger, I.; Bullinger, M. SF-36 Fragebogen zum Gesundheitszustand: Deutsche Version des Short Form-36 Health Survey, in SF-36 Fragebogen zum Gesundheitszustand: Deutsche Version des Short Form-36 Health Survey; Hogrefe-Verlag: Göttingen, Germany, 2011; pp. 1–221. [Google Scholar]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Kon, S.S.; Patel, M.S.; Canavan, J.L.; Clark, A.L.; Jones, S.E.; Nolan, C.M.; Cullinan, P.; Polkey, M.I.; Man, W.D.-C. Reliability and validity of 4-metre gait speed in COPD. Eur. Respir. J. 2012, 42, 333–340. [Google Scholar] [CrossRef]
- Hafsteinsdóttir, T.B.; Rensink, M.; Schuurmans, M. Clinimetric properties of the timed up and go test for patients with stroke: A systematic review. Top. Stroke Rehabil. 2014, 21, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Graham, J.E.; Ostir, G.V.; Fisher, S.R.; Ottenbacher, K.J. Assessing walking speed in clinical research: A systematic review. J. Eval. Clin. Pract. 2008, 14, 552–562. [Google Scholar] [CrossRef]
- Council, M.R. Aids to the Examination of the Peripheral Nervous System (Memorandum No. 45); Her Majesty’s Stationery Office: London, UK, 1976. [Google Scholar]
- Corrigan, J.D.; Schmidt, L.D. Development and validation of revisions in the Counselor Rating Form. J. Couns. Psychol. 1983, 30, 64–75. [Google Scholar] [CrossRef]
- Boehme, C.; Toell, T.; Lang, W.; Knoflach, M.; Kiechl, S. Longer term patient management following stroke: A systematic review. Int. J. Stroke 2021, 16, 917–926. [Google Scholar] [CrossRef]
- Sarfo, F.S.; Ulasavets, U.; Opare-Sem, O.K.; Ovbiagele, B. Tele-rehabilitation after stroke: An updated systematic review of the literature. J. Stroke Cerebrovasc. Dis. 2018, 27, 2306–2318. [Google Scholar] [CrossRef]
- Laver, K.E.; Adey-Wakeling, Z.; Crotty, M.; Lannin, N.A.; George, S.; Sherrington, C. Telerehabilitation services for stroke. Cochrane Database Syst. Rev. 2020, 1, Cd010255. [Google Scholar] [CrossRef]
- Burgos, P.I.; Lara, O.; Lavado, A.; Rojas-Sepúlveda, I.; Delgado, C.; Bravo, E.; Kamisato, C.; Torres, J.; Castañeda, V.; Cerda, M. Exergames and Telerehabilitation on Smartphones to Improve Balance in Stroke Patients. Brain Sci. 2020, 10, 773. [Google Scholar] [CrossRef]
- Lambert, C.M.; Olulana, O.; Bailey-Davis, L.; Abedi, V.; Zand, R. “Lessons Learned” Preventing Recurrent Ischemic Strokes through Secondary Prevention Programs: A Systematic Review. J. Clin. Med. 2021, 10, 4209. [Google Scholar] [CrossRef] [PubMed]
- Gallanagh, S.; Quinn, T.J.; Alexander, J.; Walters, M.R. Physical Activity in the Prevention and Treatment of Stroke. ISRN Neurol. 2011, 2011, 953818. [Google Scholar] [CrossRef]
- Tudor-Locke, C.; Craig, C.L.; Aoyagi, Y.; Bell, R.C.; Croteau, K.A.; De Bourdeaudhuij, I.; Ewald, B.; Gardner, A.W.; Hatano, Y.; Lutes, L.D.; et al. How many steps/day are enough? For older adults and special populations. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 80. [Google Scholar] [CrossRef] [PubMed]
- Kono, Y.; Kawajiri, H.; Kamisaka, K.; Kamiya, K.; Akao, K.; Asai, C.; Inuzuka, K.; Yamada, S. Predictive impact of daily physical activity on new vascular events in patients with mild ischemic stroke. Int. J. Stroke 2014, 10, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Salbach, N.M.; O’Brien, K.; Brooks, D.; Irvin, E.; Martino, R.; Takhar, P.; Chan, S.; Howe, J.-A. Speed and Distance Requirements for Community Ambulation: A Systematic Review. Arch. Phys. Med. Rehabil. 2014, 95, 117–128.e11. [Google Scholar] [CrossRef] [PubMed]
- Kloek, C.; van Tilburg, M.; Staal, J.; Veenhof, C.; Bossen, D. Development and proof of concept of a blended physiotherapeutic intervention for patients with non-specific low back pain. Physiotherapy 2019, 105, 483–491. [Google Scholar] [CrossRef] [PubMed]
- Bossen, D.; Kloek, C.; Snippe, H.W.; Dekker, J.; de Bakker, D.; Veenhof, C. A blended intervention for patients with knee and hip osteoarthritis in the physical therapy practice: Development and a pilot study. JMIR Res. Protoc. 2016, 5, e32. [Google Scholar] [CrossRef] [PubMed]
- White, C.L.; Pergola, P.E.; Szychowski, J.M.; Talbert, R.; Cervantes-Arriaga, A.; Clark, H.D.; Del Brutto, O.H.; Godoy, I.E.; Hill, M.D.; Pelegrí, A.; et al. Blood pressure after recent stroke: Baseline findings from the secondary prevention of small subcortical strokes trial. Am. J. Hypertens. 2013, 26, 1114–1122. [Google Scholar] [CrossRef] [PubMed]
- Langhorne, P.; Bernhardt, J.; Kwakkel, G. Stroke rehabilitation. Lancet 2011, 377, 1693–1702. [Google Scholar] [CrossRef] [PubMed]
- Cheraghifard, M.; Sarlak, N.; Taghizadeh, G.; Azad, A.; Fallah, S.; Akbarfahimi, M. Minimal and robust clinically important difference of three fatigue measures in chronic stroke survivors. Top. Stroke Rehabil. 2022, 30, 522–531. [Google Scholar] [CrossRef]
- Maggio, M.; Ceda, G.P.; Ticinesi, A.; De Vita, F.; Gelmini, G.; Costantino, C.; Meschi, T.; Kressig, R.W.; Cesari, M.; Fabi, M.; et al. Instrumental and Non-Instrumental Evaluation of 4-Meter Walking Speed in Older Individuals. PLoS ONE 2016, 11, e0153583. [Google Scholar] [CrossRef]
- Miller, A.; Collier, Z.; Reisman, D.S. Beyond steps per day: Other measures of real-world walking after stroke related to cardiovascular risk. J. Neuroeng. Rehabil. 2022, 19, 111. [Google Scholar] [CrossRef]
- Smith, E.; Cunningham, C.; Greene, B.R.; Persson, U.M.; Blake, C. Detecting subtle mobility changes among older adults: The Quantitative Timed Up and Go test. Aging Clin. Exp. Res. 2020, 33, 2157–2164. [Google Scholar] [CrossRef] [PubMed]







| Objectives | Endpoints | Measures and Approaches |
|---|---|---|
| Feasibility of the Strokecoach Intervention Program (study methods) | Recruitment |
|
| Retention and dropout |
| |
| To explore the acceptability of using the Strokecoach intervention consisting of Training, Coaching and Monitoring | User engagement |
|
| Acceptability and satisfaction of coaching aspects (webinars, personal coach) |
| |
| Acceptability of monitoring |
| |
| To provide preliminary evidence for patient-reported outcome measures and performance-based measures in a home-based setting. | Health-related quality of life |
|
| General health |
| |
| Functional mobility |
| |
| Walking speed |
| |
| Muscle function/strength |
| |
| To explore physiological parameters and physical activity patterns | Blood pressure |
|
| Daily physical activity during intervention period |
|
| Sex (% female) | 54.2% |
| Age (in years) Mean (SD) | 54.8 (13.1) missing n = 44 |
| Type of stroke | ischemic: 52.5% haemorrhagic: 21.3% not known: 13.8% TIA: 3.8% missing n = 16 |
| Time since stroke (in years) Mean (SD) | 6.1 (6.6) missing n = 18 |
| Affected body side (subjectively) | left 50.7% right 40.0% both 5.3% missing n = 21 |
| Recurrent stroke prior to participation (% yes) | 35.0% missing n = 16 |
| Total | ||
|---|---|---|
| n = 38 | ||
| Sex, female (%) | 57.9% | |
| Age in years, M (SD) missing n = 15 | 49.9 (11.6) | |
| Stroke subtype (%) | ischemic | 57.9% |
| haemorrhagic | 15.8% | |
| Not known | 15.8% | |
| TIA | 2.6% | |
| other | 7.9% | |
| Time since stroke (in years), M (SD) | 6.4 (6.9) | |
| Subjectively affected body side missing n = 1 | Left: 43.2%, right: 54.1%, no affected side: 2.7% | |
| Recurrent stroke (% yes) | 31.6% | |
| mRS score Md [IQR] | 2 [1] | |
| intervention duration, in days M ± SD (Range) | 92.6 ± 5.1 (61; 141) | |
| function arm [1–10], Md [IQR] | 8.5 [4.0] | |
| strength arm [1–10], Md [IQR] | 6.0 [4.0] | |
| pain arm [1–10], Md [IQR] | 7.0 [3.0] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bindschedler, A.; Ziller, C.; Gerber, E.-Y.; Behrendt, F.; Crüts, B.; Parmar, K.; Gerth, H.U.; Gäumann, S.; Dierkes, W.; Schuster-Amft, C.; et al. Feasibility of an Application-Based Outpatient Rehabilitation Program for Stroke Survivors: Acceptability and Preliminary Results for Patient-Reported Outcomes. Bioengineering 2024, 11, 135. https://doi.org/10.3390/bioengineering11020135
Bindschedler A, Ziller C, Gerber E-Y, Behrendt F, Crüts B, Parmar K, Gerth HU, Gäumann S, Dierkes W, Schuster-Amft C, et al. Feasibility of an Application-Based Outpatient Rehabilitation Program for Stroke Survivors: Acceptability and Preliminary Results for Patient-Reported Outcomes. Bioengineering. 2024; 11(2):135. https://doi.org/10.3390/bioengineering11020135
Chicago/Turabian StyleBindschedler, Annina, Carina Ziller, Eve-Yaël Gerber, Frank Behrendt, Björn Crüts, Katrin Parmar, Hans Ulrich Gerth, Szabina Gäumann, Wiebke Dierkes, Corina Schuster-Amft, and et al. 2024. "Feasibility of an Application-Based Outpatient Rehabilitation Program for Stroke Survivors: Acceptability and Preliminary Results for Patient-Reported Outcomes" Bioengineering 11, no. 2: 135. https://doi.org/10.3390/bioengineering11020135