

Combined Effect of Prenatal Mosquito Coil Smoke Exposure and Early Postnatal Nutritional Status on Obesity among Preschoolers

Abstract
:1. Introduction
2. Materials and Methods
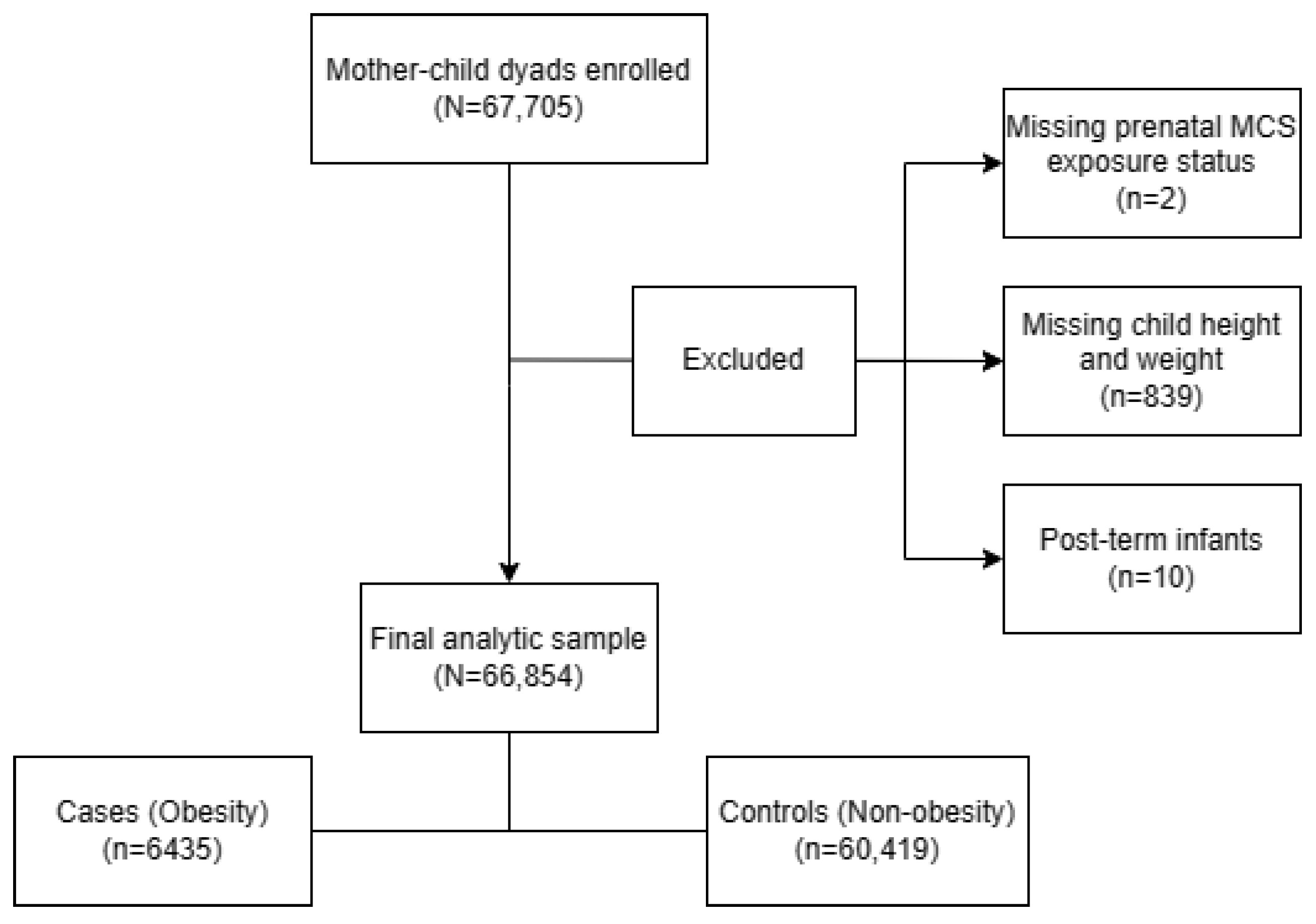
2.1. Study Population
2.2. Data Collection
2.3. Prenatal MCS Exposure Measurement
2.4. Early Postnatal Nutritional Status Measurement
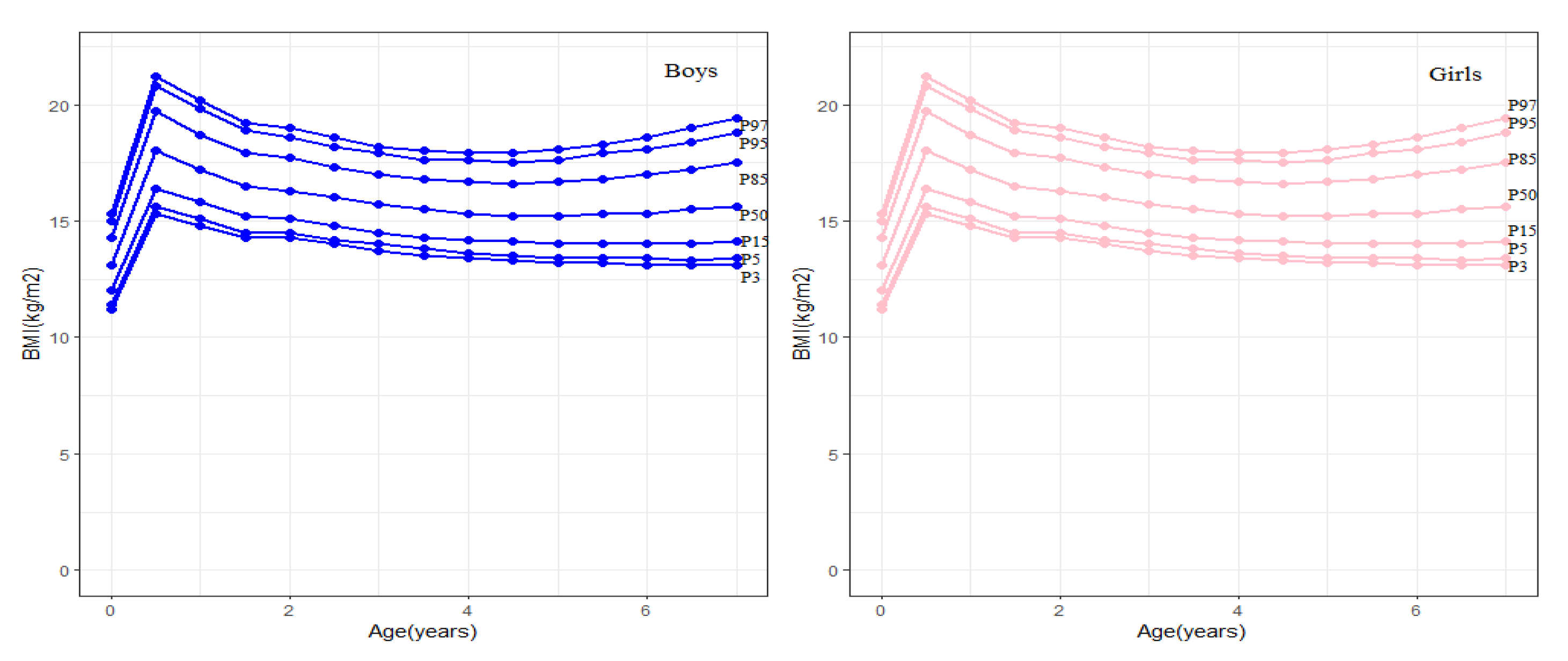
2.5. Measurement and Definition of Obesity
2.6. Potential Confounding Variables
2.7. Statistical Analyses
3. Results
3.1. Population Characteristics
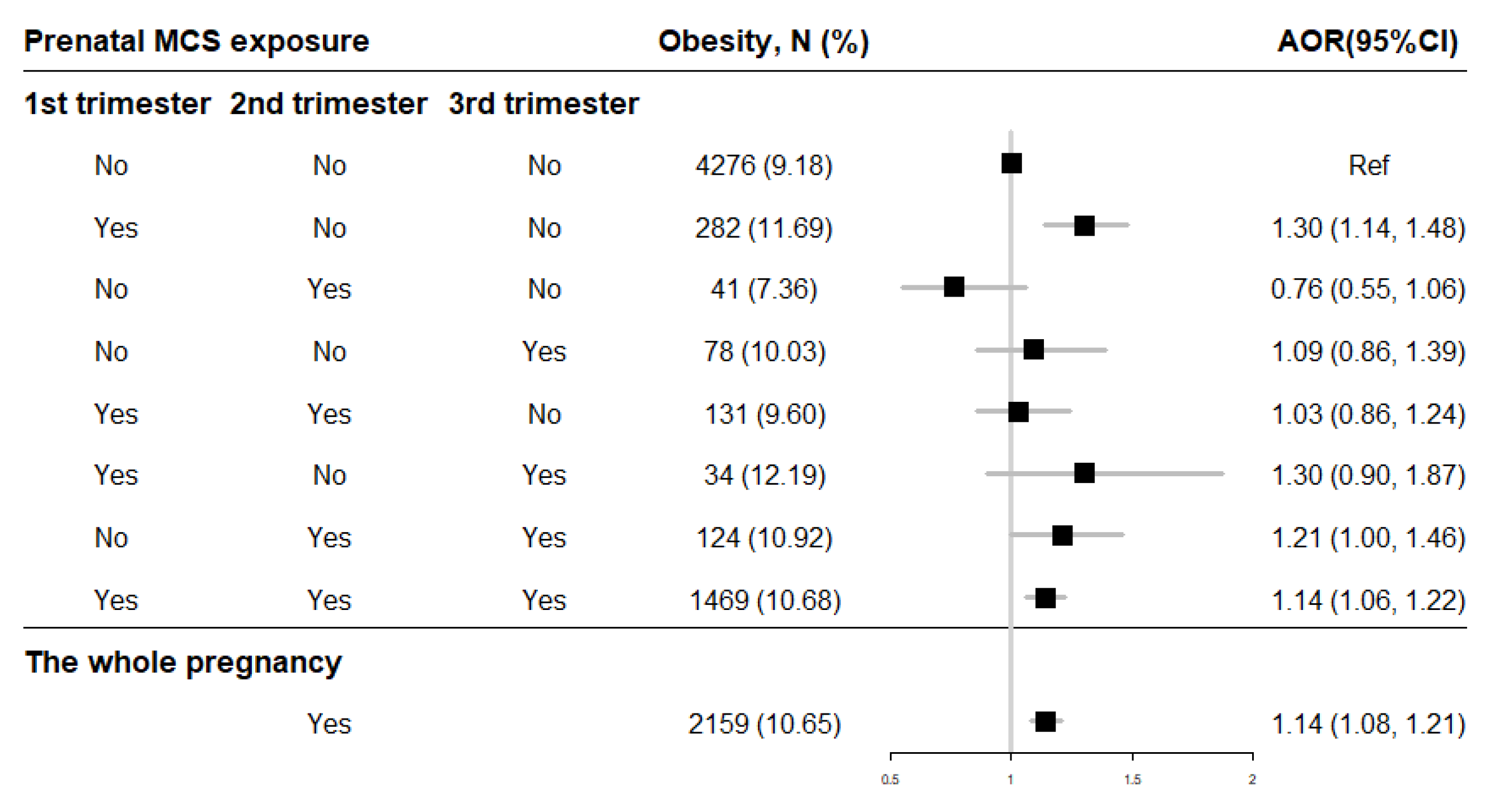
3.2. Association between Prenatal MCS Exposure and Obesity
3.3. Association between Early Postnatal Child Nutritional Status and Obesity among Preschoolers
3.4. Combination Effect of Prenatal MCS Exposure and Early Postnatal Child Nutritional Status on Obesity among Preschoolers
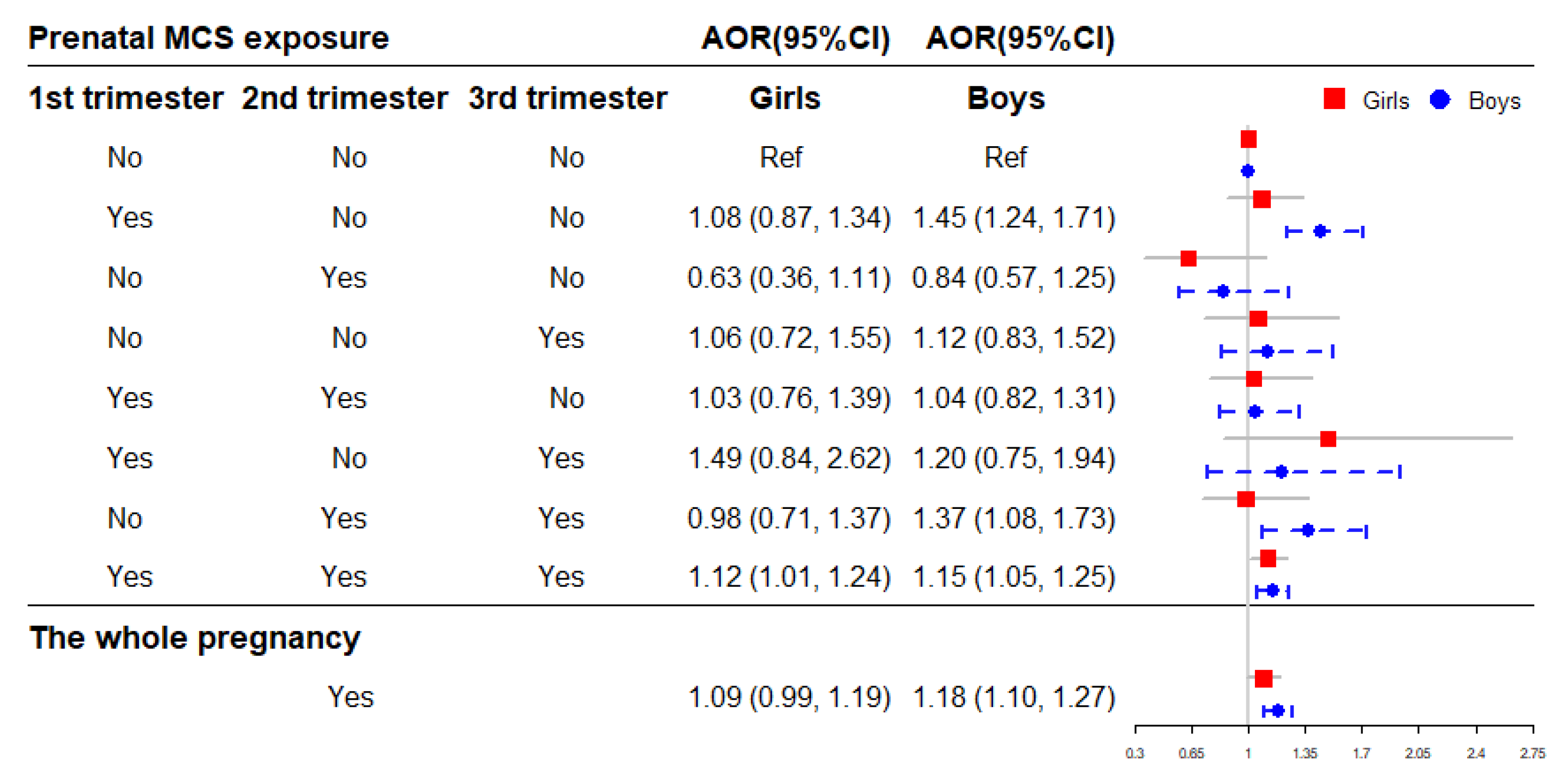
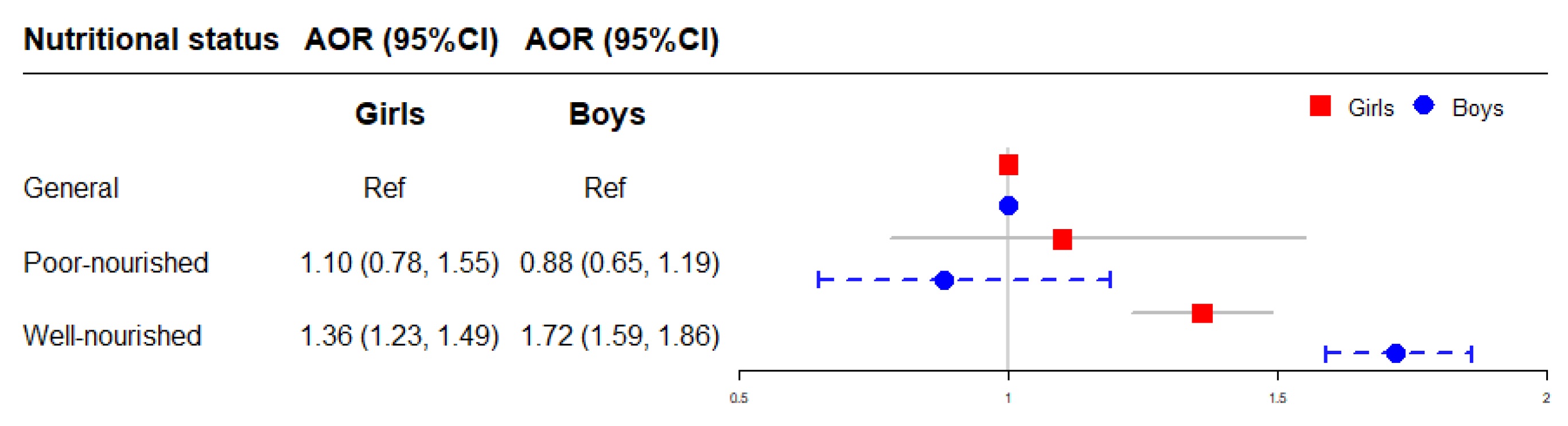
3.5. Stratified Analyses by Sex
3.6. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO. Obesity and Overweight: Fact Sheet. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 9 June 2021).
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 1289 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Pan, X.F.; Wang, L.; Pan, A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021, 9, 373–392. [Google Scholar] [CrossRef]
- Carli, M.M.; Sabo, R.T.; Sun, S.S. Childhood waist growth curves and adult diabetes. J. Dev. Orig. Health Dis. 2021, 13, 656–662. [Google Scholar] [CrossRef]
- Brady, T.M. Obesity-Related Hypertension in Children. Front. Pediatr. 2017, 5, 197. [Google Scholar] [CrossRef] [Green Version]
- Faienza, M.F.; Urbano, F.; Lassandro, G.; Valente, F.; D’Amato, G.; Portincasa, P.; Giordano, P. The Cardiovascular Disease (CVD) Risk Continuum from Prenatal Life to Adulthood: A Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 8282. [Google Scholar] [CrossRef]
- Weihe, P.; Spielmann, J.; Kielstein, H.; Henning-Klusmann, J.; Weihrauch-Blüher, S. Childhood Obesity and Cancer Risk in Adulthood. Curr. Obes. Rep. 2020, 9, 204–212. [Google Scholar] [CrossRef]
- Lindberg, L.; Danielsson, P.; Persson, M.; Marcus, C.; Hagman, E. Association of childhood obesity with risk of early all-cause and cause-specific mortality: A Swedish prospective cohort study. PLoS Med. 2020, 17, e1003078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Cesare, M.; Sorić, M.; Bovet, P.; Miranda, J.J.; Bhutta, Z.; Stevens, G.A.; Laxmaiah, A.; Kengne, A.P.; Bentham, J. The epidemiological burden of obesity in childhood: A worldwide epidemic requiring urgent action. BMC Med. 2019, 17, 212. [Google Scholar] [CrossRef] [Green Version]
- Barker, D.J. The origins of the developmental origins theory. J. Intern. Med. 2007, 261, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Lynch, F.; Lewis, S.; Macciocca, I.; Craig, J.M. Epigenetics and DOHaD: How translation to predictive testing will require a better public understanding. J. Dev. Orig. Health Dis. 2022, 13, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, K.M.; Lillycrop, K.A.; Burdge, G.C.; Gluckman, P.D.; Hanson, M.A. Epigenetic mechanisms and the mismatch concept of the developmental origins of health and disease. Pediatr. Res. 2007, 61, 5r–10r. [Google Scholar] [CrossRef] [PubMed]
- Kwon, E.J.; Kim, Y.J. What is fetal programming?: A lifetime health is under the control of in utero health. Obstet. Gynecol. Sci. 2017, 60, 506–519. [Google Scholar] [CrossRef]
- Wells, J.C. The thrifty phenotype: An adaptation in growth or metabolism? Am. J. Hum. Biol. Off. J. Hum. Biol. Counc. 2011, 23, 65–75. [Google Scholar] [CrossRef]
- Belkacemi, L.; Nelson, D.M.; Desai, M.; Ross, M.G. Maternal undernutrition influences placental-fetal development. Biol. Reprod. 2010, 83, 325–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, G.J.; Jauniaux, E. What is the placenta? Am. J. Obstet. Gynecol. 2015, 213, S6.E1–S6.E4. [Google Scholar] [CrossRef] [Green Version]
- Hu, P.; Fan, L.; Ding, P.; He, Y.H.; Xie, C.; Niu, Z.; Tian, F.Y.; Yuan, S.; Jia, D.; Chen, W.Q. Association between prenatal exposure to cooking oil fumes and full-term low birth weight is mediated by placental weight. Environ. Res. 2018, 167, 622–631. [Google Scholar] [CrossRef]
- Hu, P.; Wang, C.; Ding, P.; He, Y.H.; Xie, C.; Tian, F.Y.; Yuan, S.; Jia, D.; Chen, W.Q. Placental weight mediates association between prenatal exposure to cooking oil fumes and preterm birth. J. Matern. Fetal Neonatal Med. 2021, 35, 7248–7258. [Google Scholar] [CrossRef]
- Yuan, Z.P.; Yang, M.; Liang, L.; Fu, J.F.; Xiong, F.; Liu, G.L.; Gong, C.X.; Luo, F.H.; Chen, S.K.; Zhang, D.D.; et al. Possible role of birth weight on general and central obesity in Chinese children and adolescents: A cross-sectional study. Ann. Epidemiol. 2015, 25, 748–752. [Google Scholar] [CrossRef] [PubMed]
- Vasylyeva, T.L.; Barche, A.; Chennasamudram, S.P.; Sheehan, C.; Singh, R.; Okogbo, M.E. Obesity in prematurely born children and adolescents: Follow up in pediatric clinic. Nutr. J. 2013, 12, 150. [Google Scholar] [CrossRef] [Green Version]
- Rahmalia, A.; Giorgis-Allemand, L.; Lepeule, J.; Philippat, C.; Galineau, J.; Hulin, A.; Charles, M.A.; Slama, R. Pregnancy exposure to atmospheric pollutants and placental weight: An approach relying on a dispersion model. Environ. Int. 2012, 48, 47–55. [Google Scholar] [CrossRef]
- Ouidir, M.; Tekola-Ayele, F.; Canty, T.; Grantz, K.L.; Sciscione, A.; Tong, D.; Jones, R.R.; Sundaram, R.; Williams, A.; Stevens, D.; et al. Acute ambient air pollution exposure and placental Doppler results in the NICHD fetal growth studies—Singleton cohort. Environ. Res. 2021, 202, 111728. [Google Scholar] [CrossRef] [PubMed]
- De Bont, J.; Hughes, R.; Tilling, K.; Díaz, Y.; de Castro, M.; Cirach, M.; Fossati, S.; Nieuwenhuijsen, M.; Duarte-Salles, T.; Vrijheid, M. Early life exposure to air pollution, green spaces and built environment, and body mass index growth trajectories during the first 5 years of life: A large longitudinal study. Environ. Pollut. 2020, 266, 115266. [Google Scholar] [CrossRef]
- Patterson, W.B.; Glasson, J.; Naik, N.; Jones, R.B.; Berger, P.K.; Plows, J.F.; Minor, H.A.; Lurmann, F.; Goran, M.I.; Alderete, T.L. Prenatal exposure to ambient air pollutants and early infant growth and adiposity in the Southern California Mother’s Milk Study. Environ. Health A Glob. Access. Sci. Source 2021, 20, 67. [Google Scholar] [CrossRef]
- Bloemsma, L.D.; Dabelea, D.; Thomas, D.S.K.; Peel, J.L.; Adgate, J.L.; Allshouse, W.B.; Martenies, S.E.; Magzamen, S.; Starling, A.P. Prenatal exposure to ambient air pollution and traffic and indicators of adiposity in early childhood: The Healthy Start study. Int. J. Obes. 2022, 46, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Qureshi, R.; Jadotte, Y.; Zha, P.; Porter, S.A.; Holly, C.; Salmond, S.; Watkins, E.A. The association between prenatal exposure to environmental tobacco smoke and childhood obesity: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 1643–1662. [Google Scholar] [CrossRef]
- Shi, X.; Zheng, Y.; Cui, H.; Zhang, Y.; Jiang, M. Exposure to outdoor and indoor air pollution and risk of overweight and obesity across different life periods: A review. Ecotoxicol. Environ. Saf. 2022, 242, 113893. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zheng, X.; Stevanovic, S.; Xiang, Z.; Liu, J.; Shi, H.; Liu, J.; Yu, M.; Zhu, C. Characterizing pollutant emissions from mosquito repellents incenses and implications in risk assessment of human health. Chemosphere 2018, 191, 962–970. [Google Scholar] [CrossRef]
- Li, H.; Lydy, M.J.; You, J. Pyrethroids in indoor air during application of various mosquito repellents: Occurrence, dissipation and potential exposure risk. Chemosphere 2016, 144, 2427–2435. [Google Scholar] [CrossRef]
- Elehinafe, F.B.; Okedere, O.B.; Adesanmi, A.J.; Jimoh, E.M. Assessment of Indoor Levels of Carbon Monoxide Emission from Smoldering Mosquito Coils Used in Nigeria. Environ. Health Insights 2022, 16, 1–6. [Google Scholar] [CrossRef]
- Salvi, D.; Limaye, S.; Muralidharan, V.; Londhe, J.; Madas, S.; Juvekar, S.; Biswal, S.; Salvi, S. Indoor Particulate Matter < 2.5 μm in Mean Aerodynamic Diameter and Carbon Monoxide Levels during the Burning of Mosquito Coils and Their Association with Respiratory Health. Chest 2016, 149, 459–466. [Google Scholar] [CrossRef]
- Dubey, J.; Banerjee, A.; Meena, R.K.; Kumari, K.M.; Lakhani, A. Characterization of polycyclic aromatic hydrocarbons in emissions of different mosquito coils. Bull. Environ. Contam. Toxicol. 2014, 92, 650–654. [Google Scholar] [CrossRef]
- Lu, F.; Li, S.; Shen, B.; Zhang, J.; Liu, L.; Shen, X.; Zhao, R. The emission characteristic of VOCs and the toxicity of BTEX from different mosquito-repellent incenses. J. Hazard. Mater. 2020, 384, 121428. [Google Scholar] [CrossRef]
- Yang, J.H.; Strodl, E.; Wu, C.A.; Yin, X.N.; Wen, G.M.; Sun, D.L.; Xian, D.X.; Chen, J.Y.; Chen, Y.J.; Chen, J.; et al. Association between prenatal exposure to indoor air pollution and autistic-like behaviors among preschool children. Indoor Air 2022, 32, e12953. [Google Scholar] [CrossRef]
- Fang, X.Y.; Strodl, E.; Liu, B.Q.; Liu, L.; Yin, X.N.; Wen, G.M.; Sun, D.L.; Xian, D.X.; Jiang, H.; Jing, J.; et al. Association between prenatal exposure to household inhalants exposure and ADHD-like behaviors at around 3 years of age: Findings from Shenzhen Longhua Child Cohort Study. Environ. Res. 2019, 177, 108612. [Google Scholar] [CrossRef]
- Hisada, A.; Yoshinaga, J.; Zhang, J.; Kato, T.; Shiraishi, H.; Shimodaira, K.; Okai, T.; Ariki, N.; Komine, Y.; Shirakawa, M.; et al. Maternal Exposure to Pyrethroid Insecticides during Pregnancy and Infant Development at 18 Months of Age. Int. J. Environ. Res. Public Health 2017, 14, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Ji, C.Y.; Zong, X.N.; Zhang, Y.Q. Body mass index growth curves for Chinese children and adolescents aged 0 to 18 years. Chin. J. Pediatr. 2009, 47, 493–498. [Google Scholar]
- Abrego Del Castillo, K.Y.; Dennis, C.L.; Wamithi, S.; Briollais, L.; McGowan, P.O.; Dol, J.; Lye, S.J. Maternal BMI, breastfeeding and perinatal factors that influence early childhood growth trajectories: A scoping review. J. Dev. Orig. Health Dis. 2022, 13, 541–549. [Google Scholar] [CrossRef]
- Hemmingsson, E. Early Childhood Obesity Risk Factors: Socioeconomic Adversity, Family Dysfunction, Offspring Distress, and Junk Food Self-Medication. Curr. Obes. Rep. 2018, 7, 204–209. [Google Scholar] [CrossRef] [Green Version]
- Heindel, J.J.; Howard, S.; Agay-Shay, K.; Arrebola, J.P.; Audouze, K.; Babin, P.J.; Barouki, R.; Bansal, A.; Blanc, E.; Cave, M.C.; et al. Obesity II: Establishing causal links between chemical exposures and obesity. Biochem. Pharmacol. 2022, 199, 115015. [Google Scholar] [CrossRef] [PubMed]
- Sirkka, O.; Fleischmann, M.; Abrahamse-Berkeveld, M.; Halberstadt, J.; Olthof, M.R.; Seidell, J.C.; Corpeleijn, E. Dietary Patterns in Early Childhood and the Risk of Childhood Overweight: The GECKO Drenthe Birth Cohort. Nutrients 2021, 13, 2046. [Google Scholar] [CrossRef]
- Mahumud, R.A.; Sahle, B.W.; Owusu-Addo, E.; Chen, W.; Morton, R.L.; Renzaho, A.M.N. Association of dietary intake, physical activity, and sedentary behaviours with overweight and obesity among 282,213 adolescents in 89 low and middle income to high-income countries. Int. J. Obes. 2021, 45, 2404–2418. [Google Scholar] [CrossRef]
- Woo Baidal, J.A.; Locks, L.M.; Cheng, E.R.; Blake-Lamb, T.L.; Perkins, M.E.; Taveras, E.M. Risk Factors for Childhood Obesity in the First 1000 Days: A Systematic Review. Am. J. Prev. Med. 2016, 50, 761–779. [Google Scholar] [CrossRef] [PubMed]
- Rundle, A.; Hoepner, L.; Hassoun, A.; Oberfield, S.; Freyer, G.; Holmes, D.; Reyes, M.; Quinn, J.; Camann, D.; Perera, F.; et al. Association of childhood obesity with maternal exposure to ambient air polycyclic aromatic hydrocarbons during pregnancy. Am. J. Epidemiol. 2012, 175, 1163–1172. [Google Scholar] [CrossRef] [Green Version]
- Chiu, Y.M.; Hsu, H.L.; Wilson, A.; Coull, B.A.; Pendo, M.P.; Baccarelli, A.; Kloog, I.; Schwartz, J.; Wright, R.O.; Taveras, E.M.; et al. Prenatal particulate air pollution exposure and body composition in urban preschool children: Examining sensitive windows and sex-specific associations. Environ. Res. 2017, 158, 798–805. [Google Scholar] [CrossRef]
- Dattilo, A.M.; Birch, L.; Krebs, N.F.; Lake, A.; Taveras, E.M.; Saavedra, J.M. Need for early interventions in the prevention of pediatric overweight: A review and upcoming directions. J. Obes. 2012, 2012, 123023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flynn, A.C.; Thompson, J.M.D.; Dalrymple, K.V.; Wall, C.; Begum, S.; Pallippadan Johny, J.; Cutfield, W.S.; North, R.; McCowan, L.M.E.; Godfrey, K.M.; et al. Childhood dietary patterns and body composition at age 6 years: The Children of SCOPE study. Br. J. Nutr. 2020, 124, 217–224. [Google Scholar] [CrossRef]
- Samaranayake, D.; Lanerolle, P.; Waidyatilaka, I.; de Lanerolle-Dias, M.; Hills, A.P.; Wickremasinghe, A.R.; Wickramasinghe, V.P. Association between early weight gain and later adiposity in Sri Lankan adolescents. J. Dev. Orig. Health Dis. 2021, 12, 250–259. [Google Scholar] [CrossRef]
- Larqué, E.; Labayen, I.; Flodmark, C.E.; Lissau, I.; Czernin, S.; Moreno, L.A.; Pietrobelli, A.; Widhalm, K. From conception to infancy—Early risk factors for childhood obesity. Nat. Rev. Endocrinol. 2019, 15, 456–478. [Google Scholar] [CrossRef]
- Wang, G.; DiBari, J.; Bind, E.; Steffens, A.M.; Mukherjee, J.; Bartell, T.R.; Bellinger, D.C.; Hong, X.; Ji, Y.; Wang, M.C.; et al. In utero exposure to mercury and childhood overweight or obesity: Counteracting effect of maternal folate status. BMC Med. 2019, 17, 216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zulkifli, S.; Mohd Nor, N.S.; Sheikh Abdul Kadir, S.H.; Mohd Ranai, N.; Mohd Kornain, N.K.; Wan Mohd Zain, W.N.I.; Abdul Aziz, M. Prenatal Bisphenol a Exposure and Postnatal Trans Fat Diet Alter Small Intestinal Morphology and Its Global DNA Methylation in Male Sprague-Dawley Rats, Leading to Obesity Development. Nutrients 2022, 14, 2382. [Google Scholar] [CrossRef]
- Barbero, A.; Astiz, S.; Ovilo, C.; Lopez-Bote, C.J.; Perez-Solana, M.L.; Ayuso, M.; Garcia-Real, I.; Gonzalez-Bulnes, A. Prenatal programming of obesity in a swine model of leptin resistance: Modulatory effects of controlled postnatal nutrition and exercise. J. Dev. Orig. Health Dis. 2014, 5, 248–258. [Google Scholar] [CrossRef]
- Hales, C.N.; Barker, D.J. The thrifty phenotype hypothesis. Br. Med. Bull. 2001, 60, 5–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gluckman, P.D.; Hanson, M.A.; Low, F.M. Evolutionary and developmental mismatches are consequences of adaptive developmental plasticity in humans and have implications for later disease risk. Philos. Trans. R. Soc. Lond. Ser. B Biol. Sci. 2019, 374, 20180109. [Google Scholar] [CrossRef] [Green Version]
- Xie, P.; Zhao, C.; Huang, W.; Yong, T.; Chung, A.C.K.; He, K.; Chen, X.; Cai, Z. Prenatal exposure to ambient fine particulate matter induces dysregulations of lipid metabolism in adipose tissue in male offspring. Sci. Total Environ. 2019, 657, 1389–1397. [Google Scholar] [CrossRef]
- Chen, M.; Wang, X.; Hu, Z.; Zhou, H.; Xu, Y.; Qiu, L.; Qin, X.; Zhang, Y.; Ying, Z. Programming of mouse obesity by maternal exposure to concentrated ambient fine particles. Part. Fibre Toxicol. 2017, 14, 20. [Google Scholar] [CrossRef]
- Wells, J.C. Sexual dimorphism of body composition. Best Pract. Res. Clin. Endocrinol. Metab. 2007, 21, 415–430. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisle, F. Gender differences in food choice: The contribution of health beliefs and dieting. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total, N = 66,854 | Obesity, n | Prevalence (%) | p |
|---|---|---|---|---|
| Child gender | <0.001 | |||
| Male | 35,656 | 3980 | 11.16 | |
| Female | 31,198 | 2455 | 7.87 | |
| Child age (years) | 0.008 | |||
| ≤3 | 3926 | 320 | 8.15 | |
| 3–4 | 21,231 | 2034 | 9.58 | |
| 4–5 | 24,280 | 2402 | 9.89 | |
| >5 | 17,417 | 1679 | 9.64 | |
| Child birth weight (g) | <0.001 | |||
| <2500 | 3668 | 378 | 10.31 | |
| 2500–4000 | 60,842 | 5729 | 9.42 | |
| >4000 | 2344 | 328 | 13.99 | |
| Preterm birth | <0.001 | |||
| No | 61,484 | 5804 | 9.44 | |
| Yes | 5370 | 631 | 11.75 | |
| Maternal age at conception (years) | 0.470 | |||
| <35 | 58,735 | 5635 | 9.59 | |
| ≥35 | 8119 | 800 | 9.85 | |
| Maternal pre-pregnancy BMI (kg/m2) | <0.001 | |||
| <18.5 | 13,289 | 974 | 7.33 | |
| 18.5–23.9 | 45,518 | 4299 | 9.44 | |
| ≥24 | 8047 | 1162 | 14.44 | |
| Maternal weight gain during pregnancy (kg) | <0.001 | |||
| <5 | 3236 | 419 | 12.95 | |
| 5–10 | 22,308 | 2203 | 9.88 | |
| 10–15 | 26,278 | 2231 | 8.49 | |
| 15–20 | 11,413 | 1154 | 10.11 | |
| ≥20 | 3619 | 428 | 11.83 | |
| Maternal education level | <0.001 | |||
| Middle school or below | 9888 | 1083 | 10.95 | |
| High school | 13,503 | 1364 | 10.10 | |
| College or above | 43,463 | 3988 | 9.18 | |
| Paternal education level | <0.001 | |||
| Middle school or below | 8866 | 997 | 11.25 | |
| High school | 13,666 | 1396 | 10.22 | |
| College or above | 44,322 | 4042 | 9.12 | |
| Marital status | <0.001 | |||
| Married | 65,131 | 6203 | 9.52 | |
| Not married | 1723 | 232 | 13.46 | |
| Household income (RMB/month) | <0.001 | |||
| <10,000 | 10,102 | 1124 | 11.13 | |
| 10,000–20,000 | 23,067 | 2220 | 9.62 | |
| 20,001–30,000 | 14,478 | 1335 | 9.22 | |
| >30,000 | 19,207 | 1756 | 9.14 | |
| Mosquito coil smoke (MCS) exposure | <0.001 | |||
| No | 46,573 | 4276 | 9.18 | |
| Yes | 20,281 | 2159 | 10.65 | |
| Environmental tobacco smoke (ETS) exposure | 0.108 | |||
| No | 55,616 | 5307 | 9.54 | |
| Yes | 11,238 | 1128 | 10.04 | |
| Incense smoke exposure | <0.001 | |||
| No | 60,531 | 5730 | 9.47 | |
| Yes | 6323 | 705 | 11.15 | |
| Cooking fuel type | 0.002 | |||
| Electricity | 6262 | 577 | 9.21 | |
| Liquefied petroleum gas or natural gas | 59,050 | 5670 | 9.60 | |
| Coal | 1542 | 188 | 12.19 | |
| Heavy metal exposure | 0.829 | |||
| No | 66,334 | 6383 | 9.62 | |
| Yes | 520 | 52 | 10.00 | |
| Benzene exposure | 0.290 | |||
| No | 66,379 | 6382 | 9.61 | |
| Yes | 475 | 53 | 11.16 | |
| Feeding pattern | 0.015 | |||
| Breastfeeding | 38,676 | 3759 | 9.72 | |
| Bottle feeding | 6832 | 707 | 10.35 | |
| Mixed feeding | 21,346 | 1969 | 9.22 | |
| Child nutritional status | <0.001 | |||
| Poor-nourished | 1055 | 88 | 8.34 | |
| General | 21,130 | 1601 | 7.58 | |
| Well-nourished | 44,669 | 4746 | 10.62 | |
| Child physical activity frequency (days/week) | <0.001 | |||
| 7 | 28,833 | 2565 | 8.90 | |
| 4–6 | 17,520 | 1604 | 9.16 | |
| 2–3 | 16,140 | 1701 | 10.54 | |
| 1 | 4033 | 497 | 12.32 | |
| 0 | 328 | 68 | 20.73 | |
| Child sleep duration (hours/day) | <0.001 | |||
| <9 | 2309 | 347 | 15.03 | |
| 9–16 | 59,565 | 5593 | 9.39 | |
| >16 | 4980 | 495 | 9.94 |
| Frequency of Prenatal MCS Exposure | Total, N= 66,854 | Obesity, n (%) | OR (95%CI) | AOR (95% CI) a |
|---|---|---|---|---|
| 1st trimester | ||||
| 0 time/week | 49,044 | 4519 (9.21) | 1.00 | 1.00 |
| 1 time/week | 12,813 | 1365 (10.65) | 1.17 (1.10, 1.25) *** | 1.14 (1.06, 1.21) *** |
| ≥2 times/week | 4997 | 551 (11.03) | 1.22 (1.11, 1.34) *** | 1.18 (1.08, 1.31) ** |
| 2nd trimester | ||||
| 0 time/week | 50,042 | 4670 (9.33) | 1.00 | 1.00 |
| 1 time/week | 12,147 | 1254 (10.32) | 1.12 (1.05, 1.19) ** | 1.07 (1.00, 1.15) * |
| ≥2 times/week | 4665 | 511 (10.95) | 1.20 (1.09, 1.32) *** | 1.17 (1.06, 1.29) ** |
| 3rd trimester | ||||
| 0 time/week | 50,907 | 4730 (9.29) | 1.00 | 1.00 |
| 1 time/week | 11,542 | 1214 (10.52) | 1.15 (1.07, 1.23) *** | 1.10 (1.03, 1.18) ** |
| ≥2 times/week | 4405 | 491 (11.15) | 1.22 (1.11, 1.35) *** | 1.20 (1.08, 1.32) ** |
| Postnatal Nutritional Status | Total, N = 66,854 | Obesity, n (%) | OR (95%CI) | AOR (95% CI) a |
|---|---|---|---|---|
| General | 21,130 | 1601 (7.58) | 1.00 | 1.00 |
| Poor-nourished | 1055 | 88 (8.34) | 1.11 (0.89, 1.39) | 0.96 (0.77, 1.21) |
| Well-nourished | 44,669 | 4746 (10.62) | 1.45 (1.37, 1.54) *** | 1.56 (1.47, 1.66) *** |
| Prenatal MCS Exposure | Postnatal Nutritional Status | Total, N = 66,854 | Obesity, n (%) | AOR (95% CI) a | IOR (95% CI) a | RERI (95% CI) a | AP (95% CI) a |
|---|---|---|---|---|---|---|---|
| No | General | 13,339 | 910 (6.82) | 1.00 | |||
| No | Poor-nourished | 604 | 48 (7.95) | 1.04 (0.77, 1.42) | |||
| No | Well-nourished | 32,630 | 3318 (10.17) | 1.62 (1.50, 1.75) *** | |||
| Yes | General | 7791 | 691 (8.87) | 1.22 (1.10, 1.36) *** | |||
| Yes | Poor-nourished | 451 | 40 (8.87) | 1.06 (0.76, 1.49) | |||
| Yes | Well-nourished | 12,039 | 1428 (11.86) | 1.81 (1.65, 1.97) *** | 1.80 (1.65, 1.98) *** | −0.03 (−0.20, 0.13) | −0.02 (−0.11, 0.07) |
| Group | Prenatal MCS Exposure | Postnatal Nutritional Status | Total, N | Obesity, n (%) | AOR (95% CI) a | IOR (95% CI) a | RERI (95% CI) a | AP (95% CI) a |
|---|---|---|---|---|---|---|---|---|
| Boys | ||||||||
| No | General | 7103 | 524 (7.38) | 1.00 | ||||
| No | Poor-nourished | 334 | 24 (7.19) | 0.89 (0.58, 1.36) | ||||
| No | Well-nourished | 17,323 | 2078 (12.00) | 1.78 (1.61, 1.97) *** | ||||
| Yes | General | 4241 | 416 (9.81) | 1.26 (1.10, 1.45) ** | ||||
| Yes | Poor-nourished | 259 | 24 (9.27) | 1.08 (0.70, 1.67) | ||||
| Yes | Well-nourished | 6396 | 914 (14.29) | 2.05 (1.83, 2.30) *** | 2.05 (1.83, 2.30) *** | 0.01 (−0.22, 0.23) | 0.01 (−0.11, 0.11) | |
| Girls | ||||||||
| No | General | 6236 | 386 (6.19) | 1.00 | ||||
| No | Poor-nourished | 270 | 24 (8.89) | 1.26 (0.81, 1.95) | ||||
| No | Well-nourished | 15,307 | 1240 (8.10) | 1.41 (1.25, 1.59) *** | ||||
| Yes | General | 3550 | 275 (7.75) | 1.17 (0.99, 1.38) | ||||
| Yes | Poor-nourished | 192 | 16 (8.33) | 1.07 (0.63, 1.82) | ||||
| Yes | Well-nourished | 5643 | 514 (9.11) | 1.49 (1.30, 1.72) *** | 1.49 (1.30, 1.72) *** | −0.08 (−0.33, 0.16) | −0.06 (−0.22, 0.11) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, Y.; Strodl, E.; Lu, Q.; Liu, X.-C.; Hu, B.-J.; Chen, W.-Q. Combined Effect of Prenatal Mosquito Coil Smoke Exposure and Early Postnatal Nutritional Status on Obesity among Preschoolers. Atmosphere 2023, 14, 1004. https://doi.org/10.3390/atmos14061004
Liang Y, Strodl E, Lu Q, Liu X-C, Hu B-J, Chen W-Q. Combined Effect of Prenatal Mosquito Coil Smoke Exposure and Early Postnatal Nutritional Status on Obesity among Preschoolers. Atmosphere. 2023; 14(6):1004. https://doi.org/10.3390/atmos14061004
Chicago/Turabian StyleLiang, Yang, Esben Strodl, Qing Lu, Xin-Chen Liu, Bing-Jie Hu, and Wei-Qing Chen. 2023. "Combined Effect of Prenatal Mosquito Coil Smoke Exposure and Early Postnatal Nutritional Status on Obesity among Preschoolers" Atmosphere 14, no. 6: 1004. https://doi.org/10.3390/atmos14061004