B Cell Subsets in Colombian Adults with Predominantly Antibody Deficiencies, Bronchiectasis or Recurrent Pneumonia


Abstract
:Highlights
- Flow cytometry evaluation of B cells subsets in peripheral blood successfully recognizes subjects predominantly with antibodies deficiencies.
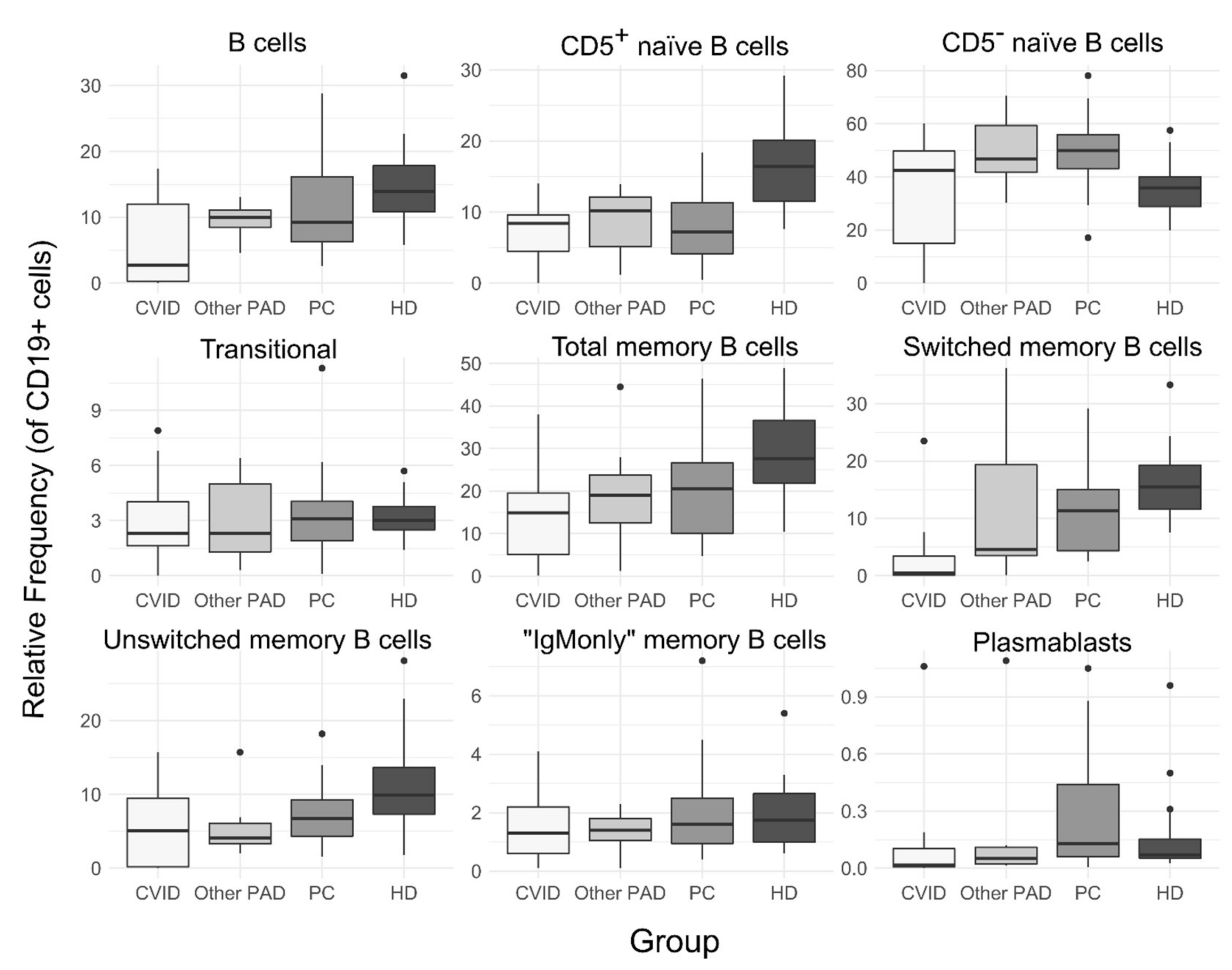
- Memory B cell populations (especially switched memory B cells) are decreased in subjects predominantly with antibodies deficiencies.
- CD8+ T cells and NK cells are affected in subjects with common variable immunodeficiency.
- Patients with non-cystic fibrosis bronchiectasis or recurrent pneumonia exhibit a reduction in naive B cells.
Abstract
1. Introduction
Clinical Rationale for the Study
2. Methods
2.1. Study Subjects
2.2. Isolation of Peripheral Blood Mononuclear Cells (PBMC) and Leucocytes Evaluation
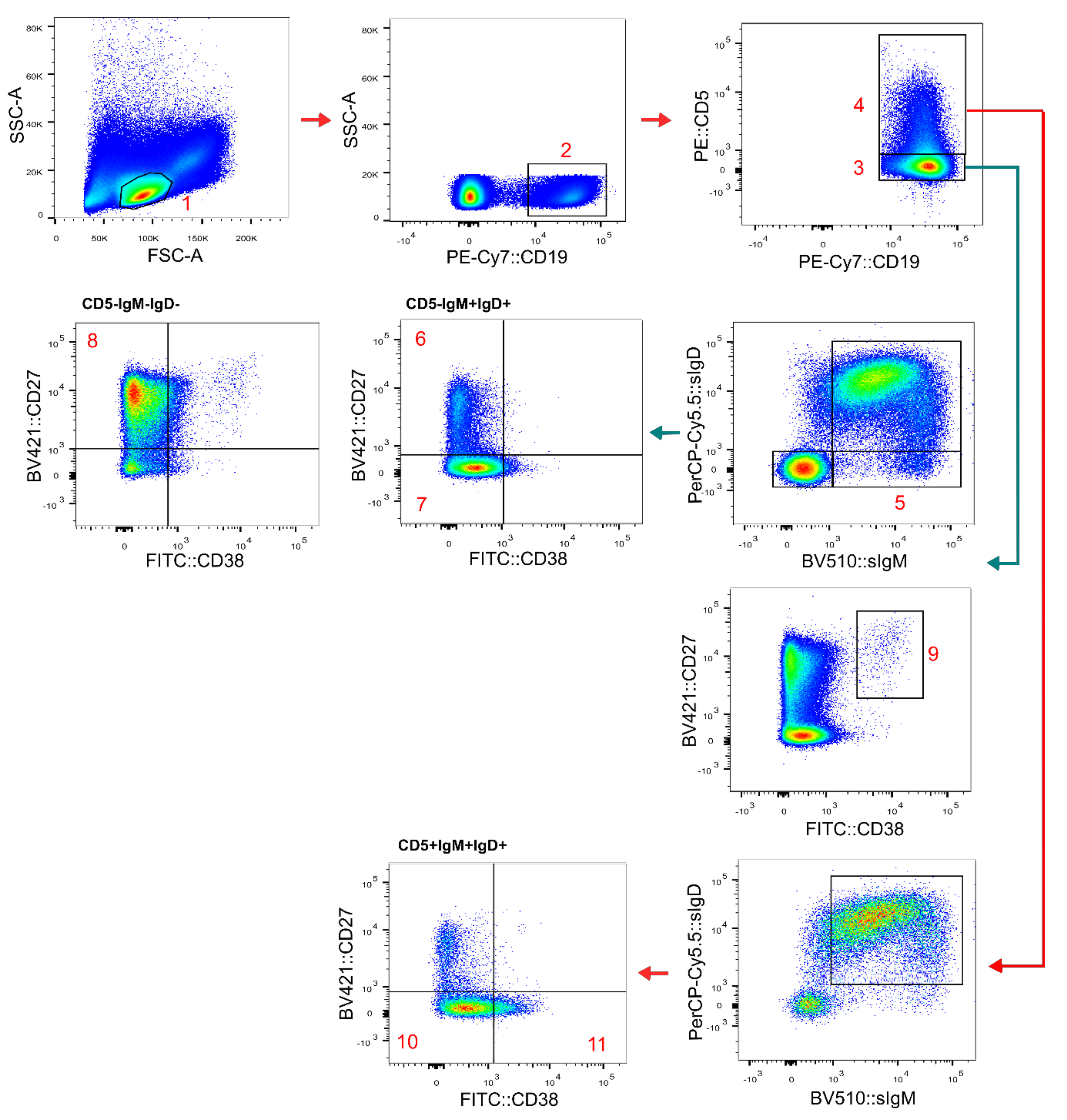
2.3. Flow Cytometric Analysis
2.4. Statistical Analysis
3. Results
3.1. Subjects Characteristics
3.2. Peripheral Blood Lymphocyte Populations
3.3. B Cell Subsets
3.4. Alteration of B Cell Subsets Frequencies and Classification of PAD Participants
4. Discussion
Clinical Implications/Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Modell, V.; Orange, J.S.; Quinn, J.; Modell, F. Global report on primary immunodeficiencies: 2018 update from the Jeffrey Modell Centers Network on disease classification, regional trends, treatment modalities, and physician reported outcomes. Immunol. Res. 2018, 66, 367–380. [Google Scholar] [CrossRef]
- Bousfiha, A.; Jeddane, L.; Picard, C.; Al-Herz, W.; Ailal, F.; Chatila, T.; Cunningham-Rundles, C.; Etzioni, A.; Franco, J.L.; Holland, S.M.; et al. Human Inborn Errors of Immunity: 2019 Update of the IUIS Phenotypical Classification. J. Clin. Immunol. 2020, 40, 66–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tangye, S.G.; Al-Herz, W.; Bousfiha, A.; Chatila, T.; Cunningham-rundles, C. Human Inborn Errors of Immunity: 2019 Update on the Classification from the International Union of Immunological Societies Expert Committee. J. Clin. Immunol. 2020, 40, 24–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durandy, A.; Kracker, S.; Fischer, A. Primary antibody deficiencies. Nat. Rev. Immunol. 2013, 13, 519–533. [Google Scholar] [CrossRef] [PubMed]
- Baumann, U.; Routes, J.M.; Soler-Palacín, P.; Jolles, S. The lung in primary immunodeficiencies: New concepts in infection and inflammation. Front. Immunol. 2018, 9, 1837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramzi, N.; Jamee, M.; Bakhtiyari, M.; Rafiemanesh, H.; Zainaldain, H.; Tavakol, M.; Rezaei, A.; Kalvandi, M.; Zian, Z.; Mohammadi, H.; et al. Bronchiectasis in common variable immunodeficiency: A systematic review and meta-analysis. Pediatr. Pulmonol. 2020, 55, 292–299. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.D.; Chang, A.B.; Chotirmall, S.H.; Dhar, R.; McShane, P.J. Bronchiectasis. Nat. Rev. Dis. Prim. 2018, 4, 45. [Google Scholar]
- ESID Registry Working Party. ESID Registry—Working Definitions for Clinical Diagnosis of IEI. 2019, pp. 1–33. Available online: https://esid.org/Working-Parties/Registry-Working-Party/Diagnosis-criteria (accessed on 10 January 2022).
- Al Kindi, M.; Mundy, J.; Sullivan, T.; Smith, W.; Kette, F.; Smith, A.; Heddle, R.; Hissaria, P. Utility of peripheral blood B cell subsets analysis in common variable immunodeficiency. Clin. Exp. Immunol. 2012, 167, 275–281. [Google Scholar] [CrossRef]
- Warnatz, K.; Denz, A.; Dräger, R.; Braun, M.; Groth, C.; Wolff-Vorbeck, G.; Eibel, H.; Schlesier, M.; Peter, H.H. Severe deficiency of switched memory B cells (CD27+IgM-IgD-) in subgroups of patients with common variable immunodeficiency: A new approach to classify a heterogeneous disease. Blood 2002, 99, 1544–1551. [Google Scholar] [CrossRef] [Green Version]
- Piqueras, B.; Lavenu-Bombled, C.; Galicier, L.; Bergeron-Van Der Cruyssen, F.; Mouthon, L.; Chevret, S.; Debré, P.; Schmitt, C.; Oksenhendler, E. Common variable immunodeficiency patient classification based on impaired B cell memory differentiation correlates with clinical aspects. J. Clin. Immunol. 2003, 23, 385–400. [Google Scholar] [CrossRef]
- Wehr, C.; Kivioja, T.; Schmitt, C.; Ferry, B.; Witte, T.; Eren, E.; Vlkova, M.; Hernandez-Gonzalez, M.; Detkova, D.; Bos, P.R.; et al. The EUROclass trial: Defining subgroups in common variable immunodeficiency. Blood 2008, 111, 77–85. [Google Scholar] [CrossRef]
- Driessen, G.J.; Van Zelm, M.C.; Van Hagen, P.M.; Hartwig, N.G.; Trip, M.; Warris, A.; De Vries, E.; Barendregt, B.H.; Pico, I.; Hop, W.; et al. B-cell replication history and somatic hypermutation status identify distinct pathophysiologic backgrounds in common variable immunodeficiency. Blood 2011, 118, 6814–6823. [Google Scholar] [CrossRef]
- Vélez, A.C.; Castaño, D.M.; Gómez, R.D.; Orrego, J.C.; Moncada, M.; Franco, J.L. Inmunodeficiencia común variable: Caracterización clínica e inmunológica de pacientese identificación de subgrupos homogéneoscon base en la tipificación de subpoblaciones de linfocitos B. Biomédica 2015, 35, 101–116. [Google Scholar] [CrossRef] [Green Version]
- Pasteur, M.C.; Bilton, D.; Hill, A.T. British thoracic society guideline for non-CF bronchiectasis. Thorax 2010, 65, i1–i58. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, K.A.; Beierle, E.A.; Faro, A.; Eskin, T.A.; Flotte, T.R. Recurrent pneumonia in children: A case report and approach to diagnosis. Clin. Pediatr. 2006, 45, 15–22. [Google Scholar] [CrossRef]
- Van Dongen, J.J.M.; Van Der Burg, M.; Kalina, T.; Perez-Andres, M.; Mejstrikova, E.; Vlkova, M.; Lopez-Granados, E.; Wentink, M.; Kienzler, A.-K.; Philippé, J.; et al. EuroFlow-Based Flowcytometric Diagnostic Screening and Classification of Primary Immunodeficiencies of the Lymphoid System. Front. Immunol. 2019, 10, 1271. [Google Scholar] [CrossRef] [Green Version]
- Bateman, E.A.L.; Ayers, L.; Sadler, R.; Lucas, M.; Roberts, C.; Woods, A.; Packwood, K.; Burden, J.; Harrison, D.; Kaenzig, N.; et al. T cell phenotypes in patients with common variable immunodeficiency disorders: Associations with clinical phenotypes in comparison with other groups with recurrent infections. Clin. Exp. Immunol. 2012, 170, 202–211. [Google Scholar] [CrossRef]
- Wong, G.K.; Huissoon, A.P. T-cell abnormalities in common variable immunodeficiency: The hidden defect. J. Clin. Pathol. 2016, 69, 672–676. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Kuchen, S.; Fischer, R.; Chang, S.; Lipsky, P.E. Identification and Characterization of a Human CD5 + Pre-Naive B Cell Population. J. Immunol. 2009, 182, 4116–4126. [Google Scholar] [CrossRef] [Green Version]
- Sanz, I.; Wei, C.; Jenks, S.A.; Cashman, K.S.; Tipton, C.; Woodruff, M.C.; Hom, J.; Lee, F.E.H. Challenges and opportunities for consistent classification of human b cell and plasma cell populations. Front. Immunol. 2019, 10, 2458. [Google Scholar] [CrossRef] [Green Version]
- Isnardi, I.; Ng, Y.S.; Menard, L.; Meyers, G.; Saadoun, D.; Srdanovic, I.; Samuels, J.; Berman, J.; Buckner, J.H.; Cunningham-Rundles, C.; et al. Complement receptor 2/CD21- human naive B cells contain mostly autoreactive unresponsive clones. Blood 2010, 115, 5026–5036. [Google Scholar] [CrossRef] [Green Version]
- Celiksoy, M.H.; Yildiran, A. A comparison of B cell subsets in primary immune deficiencies that progress with antibody deficiency and age-matched healthy children. Allergol. Immunopathol. 2016, 44, 331–340. [Google Scholar] [CrossRef]
- Carsetti, R.; Rosado, M.M.; Donnanno, S.; Guazzi, V.; Soresina, A.; Meini, A.; Plebani, A.; Aiuti, F.; Quinti, I. The loss of IgM memory B cells correlates with clinical disease in common variable immunodeficiency. J. Allergy Clin. Immunol. 2005, 115, 412–417. [Google Scholar] [CrossRef]
- Stuchlý, J.; Kanderová, V.; Vlková, M.; Heřmanová, I.; Slámová, L.; Pelák, O.; Taraldsrud, E.; Jílek, D.; Králíčková, P.; Fevang, B.; et al. Common Variable Immunodeficiency patients with a phenotypic profile of immunosenescence present with thrombocytopenia. Sci. Rep. 2017, 7, 39710. [Google Scholar]
- King, P.T.; Hutchinson, P.; Holmes, P.W.; Freezer, N.J.; Bennett-Wood, V.; Robins-Browne, R.; Holdsworth, S.R. Assessing immune function in adult bronchiectasis. Clin. Exp. Immunol. 2006, 144, 440–446. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | CVID | Other PAD | PC | HD |
|---|---|---|---|---|
| n | 9 | 7 | 20 | 20 |
| Age, n (%) | ||||
| 15–29 | 4 (44) | 1 (14) | 6 (30) | 7 (35) |
| 30–39 | 4 (44) | 1 (14) | 5 (25) | 6 (30) |
| 40–50 | 0 | 2 (29) | 2 (10) | 5 (25) |
| >50 | 1 (11) | 3 (43) | 7 (35) | 2 (10) |
| Gender, n (%) | ||||
| Male | 7 (78) | 1 (14) | 9 (45) | 8 (40) |
| Female | 2 (22) | 6 (86) | 11 (55) | 12 (60) |
| Ethnicity, n (%) | ||||
| Mestizo | 7 (78) | 5 (71) | 15 (75) | 17 (85) |
| Black | 2 (22) | 2 (29) | 4 (20) | 1 (5) |
| Indigenous | 0 | 0 | 1(5) | 0 |
| White | 0 | 0 | 0 | 2 (10) |
| Bronchiectasis, n (%) | 0 | 1 (14) | 6 (30) | - |
| Recurrent pneumonia, n (%) | 3 (33) | 3 (43) | 7 (35) | - |
| Bronchiectasis and Recurrent pneumonia, n (%) | 6 (67) | 3 (43) | 7 (35) | - |
| Exposure to biomass, n (%) | ||||
| Yes | 1 (11) | 2 (29) | 4 (20) | - |
| No | 8 (89) | 5 (71) | 16 (80) | - |
| Exposure to wood smoke, n (%) | ||||
| Yes | 0 | 1 (14) | 7 (35) | - |
| No | 9 (100) | 6 (86) | 13 (65) | - |
| Exposure to tobacco smoke, n (%) | ||||
| Yes | 3 (33) | 3 (43) | 6 (30) | - |
| No | 6 (67) | 4 (57) | 14 (70) | - |
| Group | Age (Years) | Dx Delay (Years) | Pneumonia Episodes | Ig Treatment | Other Manifestations Diagnosed | CD4:CD8 | B Cells | Total Memory B Cells | SM B Cells | UsM B Cells | Naive CD5-B Cells | Transitional B Cells | EUROclass | Driessen et al. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PAD | ||||||||||||||
| CVID-1 | 56 | 11 | 3 | Yes | Skin abscesses | 0.4 | <1 * | 0.5 * | 0.1 * | 0.21 * | 15 * | 42 ~ | B- | - |
| CVID-2 | 30 | 2 | >5 | Yes | Viral Hepatitis | 0.6 | 12 (430.8) | 8 (34.4) | 1.3 (5.7) * | 9.5 (40.8) *† | 58.9 (253.7) | 3.1 (13.1) | smB+21norm | NA |
| CVID-3 | 31 | 14 | >10 | No | sinusitis | 8 | <1 (2.9) *† | 38 (1.1) † | 23.5 (0.7) † | 1.1 (0) *† | 29.7 (0.9) † | 2.2 (0.1) † | B- | Pattern 1 |
| CVID-4 | 37 | 6 | 3 | Yes | - | 0.5 | 3.5 (90.2) * | 15.7 (14.2) † | 0.11 (0.1) *† | 15.7 (14.2) | 49.7 (44.8) | 6.8 (6.1) | smB-Trnorm smB-21lo | Pattern 4 |
| CVID-5 | 23 | 6 | >3 | Yes | Otitis, sinusitis | 0.3 | 2.7 (77.5) *† | 19.5 (15.1) † | 3.4 (2.7) *† | 12.1 (9.4) † | 49.5 (38.4) | 2.1 (1.6) | smB+21norm | Pattern 3 |
| CVID-6 | 24 | 11 | 2 | Yes | Diarrhea, ITP, AD, Sjögren syndrome | 0.8 | 17.4 (819.5) | 5.09 (41.7) * | 0.5 (4.2) *† | 6.7 (54.7) | 42.4 (347.5) | 7.9 (64.3) ~ | smB-Trnorm smB-21lo | NA |
| CVID-7 | 16 | 6 | 6 | Yes | - | 1.4 | <1 (0.2) *† | 35.8 (0.1) † | 0 (0) *† | 0 (0) *† | 2.6 (0) *† | 0 (0) *† | B- | Pattern 1 |
| CVID-8 | 36 | 9 | >10 | Yes | Kernicterus, Hypoacousis, otitis, asthma, gastritis, AD | 1.9 | 14 (380.8) | 14.9 (56.7) | 7.6 (28.8) | 5.1 (19.5) | 60.1 (228.9) | 2.4 (9.1) | smB+21norm | Pattern 5 |
| CVID-9 | 21 | 2 | >5 | Yes | Sinusitis, nephrotic syndrome, gastroesophageal reflux | 0.8 | <1 (4.3) *† | 0.1 (0) *† | 0.05 (0) *† | 0 (0) *† | 0 (0) *† | 0.2 (0) *† | B- | Pattern 1 |
| SIgAD-1 | 34 | 17 | >10 | Yes | Esophageal candidiasis | 1.1 | 9.3 (189.8) | 1.18 (2.2) *† | 0.09 (0.2) *† | 2.8 (5.2) *† | 59.6 (59.6) | 6 (11.4) | smB-Trnorm smB-21norm | Pattern 3 |
| SIgAD-2 | 63 | 28 | >10 | No | Gastritis, asthma | 2.1 | 13.1 (305.2) | 19.6 (59.8) | 14.2 (43.3) | 4.1 (12.4) ~ | 46.8 (46.8) | 4 (12.2) | smB+21norm | Pattern 5 |
| SIgAD-3 | 50 | 5 | 0 | No | Gastritis, asthma | 0.8 | 11.3 (340.1) | 8.6 (29.4) *† | 3.8 (13) *† | 2 (6.8) *† | 70.6 (70.6) ~ | 1.4 (4.7) | smB+21norm | Pattern 3 |
| SIgAD-4 | 48 | 15 | 3 | No | Gastritis, asthma, sinusitis | 1.9 | 10.9 (170) | 19 (32.3)† | 3.2 (5.4) *† | 15.7 (26.7) | 59.1 (59.1) | 1.2 (2) † | smB+21norm | Pattern 1 |
| SIgMD-1 | 64 | 28 | 4 | No | Asthma, hypothyroidism | 4.7 | 10 (214) | 27.9 (59.7) | 24.5 (52.4) | 5.3 (11.3) ~~ | 40.3 (86.2) | 2.3 (5) *† | smB+21norm | NA |
| SIgMD-2 | 64 | 57 | 4 | No | Asthma | 1.9 | 4.6 (176.3) * | 44.5 (78.5) ~ | 36.2 (63.8) ~ | 3.8 (6.6) ~ | 30.2 (53.2) † | 0.3 (0.6) *† | smB+21norm | NA |
| UAD | 15 | 13 | >15 | No | Asthma, sinusitis, AD, absent corpus callosum | 2.3 | 7.6 (175.7) | 16.4 (28.8) † | 4.6 (8) *† | 6.9 (12.1) † | 43.1 (75.7) | 6.4 (11.3) | smB+21norm | Pattern 3 |
| HD | 36 (28–42) | - | - | - | - | 2.1 | 14 (290) | 27.7 (72.2) | 15.5 (43) | 9.9 (21.7) | 35.9 (102.2) | 3 (7.2) | - | - |
| PC | 39 (29–54) | - | 4 (3–10) | No | - | 1.8 | 9.2 (242) | 20.5 (24.9) | 11.3 (16.7) | 6.7 (13.7) | 50 (109) | 3 (9) | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giraldo-Ocampo, S.; Bonelo, A.; Zea-Vera, A.F. B Cell Subsets in Colombian Adults with Predominantly Antibody Deficiencies, Bronchiectasis or Recurrent Pneumonia. Adv. Respir. Med. 2022, 90, 254-266. https://doi.org/10.3390/arm90040035
Giraldo-Ocampo S, Bonelo A, Zea-Vera AF. B Cell Subsets in Colombian Adults with Predominantly Antibody Deficiencies, Bronchiectasis or Recurrent Pneumonia. Advances in Respiratory Medicine. 2022; 90(4):254-266. https://doi.org/10.3390/arm90040035
Chicago/Turabian StyleGiraldo-Ocampo, Sebastian, Anilza Bonelo, and Andres F. Zea-Vera. 2022. "B Cell Subsets in Colombian Adults with Predominantly Antibody Deficiencies, Bronchiectasis or Recurrent Pneumonia" Advances in Respiratory Medicine 90, no. 4: 254-266. https://doi.org/10.3390/arm90040035