
Optical Coherence Tomography as a Biomarker in the Differential Diagnosis between Parkinson’s Disease and Atypical Parkinsonian Syndromes: A Narrative Review

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
2.4. Data Analysis
3. Results
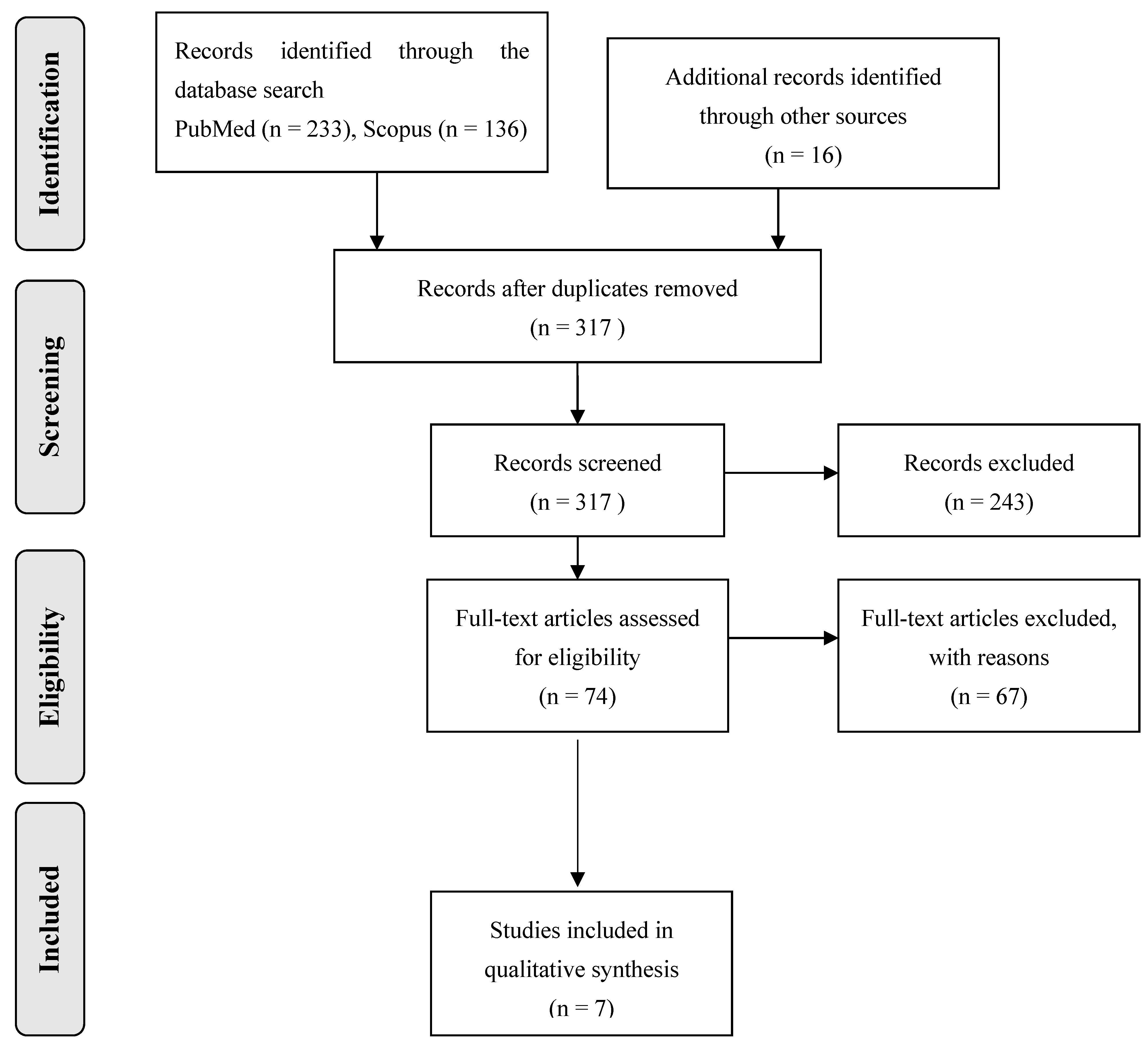
3.1. Database Searches
3.2. Study Characteristics
4. Literature Review Sections
4.1. Exploring Retinal Findings in Patients with Typical (PD) and Atypical Parkinsonism (PSP, MSA, CBS)
4.2. Investigating Retinal Parameters among Patients with PD versus PSP
4.3. Examining Retinal Changes in a Setting of Dementia Associated with the Presence of Lewy Bodies or Parkinson’s Disease
5. Discussion
6. Conclusions
Funding
Conflicts of Interest
References
- Williams, D.R.; Litvan, I. Parkinsonian syndromes. Contin. Lifelong Learn. Neurol. 2013, 19, 1189–1212. [Google Scholar] [CrossRef]
- Keener, A.M.; Bordelon, Y.M. Parkinsonism. Semin. Neurol. 2016, 36, 330–334. [Google Scholar] [CrossRef]
- Shin, H.W.; Hong, S.W.; Youn, Y.C. Clinical Aspects of the Differential Diagnosis of Parkinson’s Disease and Parkinsonism. J. Clin. Neurol. 2022, 18, 259–270. [Google Scholar] [CrossRef]
- McFarland, N.R. Diagnostic Approach to Atypical Parkinsonian Syndromes. Continuum 2016, 22, 1117–1142. [Google Scholar] [CrossRef]
- Levin, J.; Kurz, A.; Arzberger, T.; Giese, A.; Hoglinger, G.U. The Differential Diagnosis and Treatment of Atypical Parkinsonism. Dtsch. Arztebl. Int. 2016, 113, 61–69. [Google Scholar] [CrossRef]
- Marino, B.L.B.; de Souza, L.R.; Sousa, K.P.A.; Ferreira, J.V.; Padilha, E.C.; da Silva, C.H.T.P.; Taft, C.A.; Hage-Melim, L.I.S. Parkinson’s Disease: A Review from Pathophysiology to Treatment. Mini Rev. Med. Chem. 2020, 20, 754–767. [Google Scholar] [CrossRef] [PubMed]
- Tysnes, O.B.; Storstein, A. Epidemiology of Parkinson’s disease. J. Neural Transm. 2017, 124, 901–905. [Google Scholar] [CrossRef]
- Vertes, A.C.; Beato, M.R.; Sonne, J.; Khan Suheb, M.Z. Parkinson-Plus Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK585113/ (accessed on 4 February 2024).
- Albrecht, P.; Müller, A.K.; Südmeyer, M.; Ferrea, S. Optical coherence tomography in parkinsonian syndromes. PLoS ONE 2012, 7, e34891. [Google Scholar] [CrossRef]
- Hess, C.W.; Okun, M.S. Diagnosing parkinson disease. Continuum (Minneap. Minn.) 2016, 22, 1047–1063. [Google Scholar] [CrossRef]
- GBD 2016 Parkinson’s Disease Collaborators. Global, regional, and national burden of Parkinson’s disease, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018, 17, 939–953. [Google Scholar] [CrossRef] [PubMed]
- Pula, J.H.; Kim, J.; Nichols, J. Visual aspects of neurologic protein misfolding disorders. Curr. Opin. Ophthalmol. 2009, 20, 482–489. [Google Scholar] [CrossRef]
- Bak, T.H.; Caine, D.; Hearn, V.C.; Hodges, J.R. Visuospatial functions in atypical parkinsonian syndromes. J. Neurol. Neurosurg. Psychiatry 2006, 77, 454–456. [Google Scholar] [CrossRef]
- Archibald, N.K.; Clarke, M.P.; Mosimann, U.P.; Burn, D.J. The retina in Parkinson’s disease. Brain 2009, 132, 1128–1145. [Google Scholar] [CrossRef]
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical coherence tomography. Science 1991, 254, 1178–1181. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liu, S.; Lou, S.; Zhang, W.; Cai, H.; Chen, X. Application of optical coherence tomography in clinical diagnosis. J. Xray Sci. Technol. 2019, 27, 995–1006. [Google Scholar] [CrossRef] [PubMed]
- Galetta, K.M.; Calabresi, P.A.; Frohman, E.M.; Balcer, L.J. Optical coherence tomography (OCT): Imaging the visual pathway as a model for neurodegeneration. Neurother. J. Am. Soc. Exp. Neurother. 2011, 8, 117–132. [Google Scholar] [CrossRef] [PubMed]
- Harnois, C.; Di Paolo, T. Decreased dopamine in the retinas of patients with Parkinson’s disease. Investig. Ophthalmol. Vis. Sci. 1990, 31, 2473–2475. [Google Scholar]
- Schneider, M.; Müller, H.P.; Lauda, F.; Tumani, H.; Ludolph, A.C.; Kassubek, J.; Pinkhardt, E.H. Retinal single-layer analysis in Parkinsonian syndromes: An optical coherence tomography study. J. Neural Transm. 2014, 121, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Li, S.; Zheng, B.; Hu, L.; Liu, H.; Wang, Z.; Wang, Z.; Chen, H.; Su, W. Retinal Structure Abnormalities in Parkinson’s Disease and Atypical Parkinsonism. Biomolecules 2023, 13, 218. [Google Scholar] [CrossRef] [PubMed]
- Alkabie, S.; Lange, A.; Manogaran, P.; Stoessl, A.J.; Costello, F.; Barton, J.J.S. Optical coherence tomography of patients with Parkinson’s disease and progressive supranuclear palsy. Clin. Neurol. Neurosurg. 2020, 189, 105635. [Google Scholar] [CrossRef]
- Gulmez Sevim, D.; Unlu, M.; Gultekin, M.; Karaca, C.; Mirza, M.; Mirza, G.E. Evaluation of Retinal Changes in Progressive Supranuclear Palsy and Parkinson Disease. J. Neuroophthalmol. 2018, 38, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Rebolleda, G.; Sanchez Sanchez, C.; Martinez Castrillo, J.C.; Gonzalez Lopez, J.J.; Oblanca Llamazares, N.; Muñoz-Negrete, F.J. Optical coherence tomography to distinguish Parkinson disease versus supranuclear progressive palsy. Acta Ophthalmol. 2016, 94, S256. [Google Scholar] [CrossRef]
- Moreno-Ramos, T.; Benito-León, J.; Villarejo, A.; Bermejo-Pareja, F. Retinal nerve fiber layer thinning in dementia associated with Parkinson’s disease, dementia with Lewy bodies, and Alzheimer’s disease. J. Alzheimers Dis. 2013, 34, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Inzelberg, R.; Ramirez, J.A.; Nisipeanu, P.; Ophir, A. Retinal nerve fiber layer thinning in Parkinson disease. Vis. Res. 2004, 44, 2793–2797. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Wang, Y.; Wang, N.; Zhang, R. Retina thickness in atypical parkinsonism: A systematic review and meta-analysis. J. Neurol. 2022, 269, 1272–1281. [Google Scholar] [CrossRef]
- Miller, N.; Drachman, D.A. The optic nerve: A window into diseases of the brain? Neurology. 2006, 67, 1742–1743. [Google Scholar] [CrossRef] [PubMed]
- London, A.; Benhar, I.; Schwartz, M. The retina as a window to the brain-from eye research to CNS disorders. Nat. Rev. Neurol. 2013, 9, 44–53. [Google Scholar] [CrossRef]
- Lim, J.K.; Li, Q.X.; He, Z.; Vingrys, A.J.; Wong, V.H.; Currier, N.; Mullen, J.; Bui, B.V.; Nguyen, C.T. The eye as a biomarker for Alzheimer’s disease. Front. Neurosci. 2016, 10, 536. [Google Scholar] [CrossRef]
- Martinez-Lapiscina, E.H.; Sanchez-Dalmau, B.; Fraga-Pumar, E.; Ortiz-Perez, S.; Tercero-Uribe, A.I.; Torres-Torres, R.; Villoslada, P. The visual pathway as a model to understand brain damage in multiple sclerosis. Mult. Scler. 2014, 20, 1678–1685. [Google Scholar] [CrossRef]
- Gupta, S.; Zivadinov, R.; Ramanathan, M.; Weinstock-Guttman, B. Optical coherence tomography and neurodegeneration: Are eyes the windows to the brain? Expert Rev. Neurother. 2016, 16, 765–775. [Google Scholar] [CrossRef]
- Garcia-Martin, E.; Satue, M.; Fuertes, I.; Otin, S.; Alarcia, R.; Herrero, R.; Bambo, M.P.; Fernandez, J.; Pablo, L.E. Ability and reproducibility of Fourier-domain optical coherence tomography to detect retinal nerve fiber layer atrophy in Parkinson’s disease. Ophthalmology 2012, 119, 2161–2167. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Kuroiwa, Y.; Kamitani, T.; Li, M.; Takahashi, T.; Suzuki, Y.; Shimamura, M.; Hasegawa, O. Visual event-related potentials in progressive supranuclear palsy, corticobasal degeneration, striatonigral degeneration, and Parkinson’s disease. J. Neurol. 2000, 247, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, C.; Cestari, D.M.; Rizzo, J.F., 3rd. The use of fourth generation optical coherence tomography in multiple sclerosis: A review. Semin. Ophthalmol. 2012, 27, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Bodis-Wollner, I.; Miri, S.; Glazman, S. Venturing into the no-man’s land of the retina in Parkinson’s disease. Mov. Disord. Off. J. Mov. Disord. Soc. 2014, 29, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Ahn, J.; Kim, T.W.; Jeon, B.S. Optical coherence tomography in Parkinson’s disease: Is the retina a biomarker? J. Park. Dis. 2014, 4, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.; Lee, J.Y.; Kim, T.W.; Yoon, E.J.; Oh, S.; Kim, Y.K.; Kim, J.M.; Woo, S.J.; Kim, K.W.; Jeon, B. Retinal thinning associates with nigral dopaminergic loss in de novo Parkinson disease. Neurology 2018, 91, e1003–e1012. [Google Scholar] [CrossRef] [PubMed]
- Oertel, F.C.; Zimmermann, H.; Paul, F.; Brandt, A.U. Optical coherence tomography in neuromyelitis optica spectrum disorders: Potential advantages for individualized monitoring of progression and therapy. EPMA J. 2017, 9, 21–33. [Google Scholar] [CrossRef]
- Balcer, L.J.; Balk, L.J.; Brandt, A.U.; Calabresi, P.A.; Martinez-Lapiscina, E.H.; Nolan, R.C.; Paul, F.; Petzold, A.; Saidha, S. The international multiple sclerosis visual system consortium: Advancing visual system research in multiple sclerosis. J. Neuroophthalmol. 2018, 38, 494–501. [Google Scholar] [CrossRef]
- Coppola, G.; Di Renzo, A.; Ziccardi, L.; Martelli, F.; Fadda, A.; Manni, G.; Barboni, P.; Pierelli, F.; Sadun, A.A.; Parisi, V. Optical coherence tomography in Alzheimer’s disease: A meta-analysis. PLoS ONE 2015, 10, e0134750. [Google Scholar] [CrossRef]
- Ratchford, J.N.; Quigg, M.E.; Conger, A.; Frohman, T.; Frohman, E.; Balcer, L.J.; Calabresi, P.A.; Kerr, D.A. Optical coherence tomography helps differentiate neuromyelitis optica and MS optic neuropathies. Neurology 2009, 73, 302–308. [Google Scholar] [CrossRef]
- Mailankody, P.; Lenka, A.; Pal, P.K. The role of Optical Coherence Tomography in Parkinsonism: A critical review. J. Neurol. Sci. 2019, 403, 67–74. [Google Scholar] [CrossRef]
- Cipollini, V.; Abdolrahimzadeh, S.; Troili, F.; De Carolis, A.; Calafiore, S.; Scuderi, L.; Giubilei, F.; Scuderi, G. Neurocognitive Assessment and Retinal Thickness Alterations in Alzheimer Disease: Is There a Correlation? J. Neuro-Ophthalmol. Off. J. N. Am. Neuro-Ophthalmol. Soc. 2020, 40, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Di Pippo, M.; d’Agostino, S.; Ruggeri, F.; Carrozzi, C.; Fasciolo, D.; Abdolrahimzadeh, S. Parkinson’s Disease: What Can Retinal Imaging Tell Us? J. Integr. Neurosci. 2024, 23, 23. [Google Scholar] [CrossRef] [PubMed]
- Picillo, M.; Salerno, G.; Tepedino, M.F.; Abate, F.; Cuoco, S.; Gioia, M.; Coppola, A.; Erro, R.; Pellecchia, M.T.; Rosa, N.; et al. Retinal thinning in progressive supranuclear palsy: Differences with healthy controls and correlation with clinical variables. Neurol. Sci. 2022, 43, 4803–4809. [Google Scholar] [CrossRef] [PubMed]
- Woo, K.A.; Shin, J.Y.; Kim, H.; Ahn, J.; Jeon, B.; Lee, J.Y. Peripapillary retinal nerve fiber layer thinning in patients with progressive supranuclear palsy. J. Neurol. 2022, 269, 3216–3225. [Google Scholar] [CrossRef] [PubMed]
- Stemplewitz, B.; Kromer, R.; Vettorazzi, E.; Hidding, U.; Frings, A.; Buhmann, C. Retinal degeneration in progressive supranuclear palsy measured by optical coherence tomography and scanning laser polarimetry. Sci. Rep. 2017, 7, 5357. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wang, H.; Wang, B.; Li, W.; Ye, P.; Xu, W.; Liu, P.; Chen, X.; Cen, Z.; Ouyang, Z.; et al. Retinal Thinning as a Marker of Disease Severity in Progressive Supranuclear Palsy. J. Mov. Disord. 2024, 17, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Fischer, M.D.; Synofzik, M.; Heidlauf, R.; Schicks, J.; Srulijes, K.; Kernstock, C.; Berg, D.; Schols, L.; Schiefer, U. Retinal nerve fiber layer loss in multiple system atrophy. Mov. Disord. Off. J. Mov. Disord. Soc. 2011, 26, 914–916. [Google Scholar] [CrossRef]
- Pula, J.H.; Towle, V.L.; Staszak, V.M.; Cao, D.; Bernard, J.T.; Gomez, C.M. Retinal nerve fibre layer and macular thinning in spinocerebellar ataxia and cerebellar multisystem atrophy. Neuroophthalmology 2011, 35, 108–114. [Google Scholar] [CrossRef]
- Fischer, M.D.; Synofzik, M.; Kernstock, C.; Dietzsch, J.; Heidlauf, R.; Schicks, J.; Srulijes, K.; Wiethoff, S.; Menn, O.; Berg, D.; et al. Decreased retinal sensitivity and loss of retinal nerve fibers in multiple system atrophy. Graefes Arch. Clin. Exp. Ophthalmol. 2013, 251, 235–241. [Google Scholar] [CrossRef]
- Mendoza-Santiesteban, C.E.; Palma, J.A.; Martinez, J.; NorcliffeKaufmann, L.; Hedges, T.R., 3rd; Kaufmann, H. Progressive retinal structure abnormalities in multiple system atrophy. Mov. Disord. Off. J. Mov. Disord. Soc. 2015, 30, 1944–1953. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Santiesteban, C.; Palma, J.A.; Ortuño-Lizaran, I.; Cuenca, N.; Kaufmann, H. Pathologic confirmation of retinal ganglion cell loss in multiple system atrophy. Neurology 2017, 88, 2233–2235. [Google Scholar] [CrossRef]
- Ahn, J.; Lee, J.Y.; Kim, T.W. Retinal thinning correlates with clinical severity in multiple system atrophy. J. Neurol. 2016, 263, 2039–2047. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Santiesteban, C.E.; Gabilondo, I.; Palma, J.A.; Norcliffe-Kaufmann, L.; Kaufmann, H. The Retina in Multiple System Atrophy: Systematic Review and Meta-Analysis. Front. Neurol. 2017, 8, 206. [Google Scholar] [CrossRef]
- Cetin, E.N.; Bir, L.S.; Sarac, G.; Yaldızkaya, F.; Yaylalı, V. Optic Disc and Retinal Nerve Fibre Layer Changes in Parkinson’s Disease. Neuro-Ophthalmology 2013, 37, 20–23. [Google Scholar] [CrossRef]
- Stemplewitz, B.; Keserü, M.; Bittersohl, D.; Buhmann, C.; Skevas, C.; Richard, G.; Hassenstein, A. Scanning laser polarimetry and spectral domain optical coherence tomography for the detection of retinal changes in Parkinson’s disease. Acta Ophthalmol. 2015, 93, e672–e677. [Google Scholar] [CrossRef]
- Hajee, M.E.; March, W.F.; Lazzaro, D.R.; Wolintz, A.H.; Shrier, E.M.; Glazman, S.; Bodis-Wollner, I.G. Inner retinal layer thinning in Parkinson disease. Arch. Ophthalmol. 2009, 127, 737–741. [Google Scholar] [CrossRef]
- Altintaş, O.; Işeri, P.; Ozkan, B.; Cağlar, Y. Correlation between retinal morphological and functional findings and clinical severity in Parkinson’s disease. Doc. Ophthalmol. 2008, 116, 137–146. [Google Scholar] [CrossRef]
- Moschos, M.M.; Tagaris, G.; Markopoulos, I.; Margetis, I.; Tsapakis, S.; Kanakis, M.; Koutsandrea, C. Morphologic changes and functional retinal impairment in patients with Parkinson disease without visual loss. Eur. J. Ophthalmol. 2011, 21, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Kirbas, S.; Turkyilmaz, K.; Tufekci, A.; Durmus, M. Retinal nerve fiber layer thickness in Parkinson disease. J. Neuroophthalmol. 2013, 33, 62–65. [Google Scholar] [CrossRef] [PubMed]
- La Morgia, C.; Barboni, P.; Rizzo, G.; Carbonelli, M.; Savini, G.; Scaglione, C.; Capellari, S.; Bonazza, S.; Giannoccaro, M.P.; Calandra-Buonaura, G.; et al. Loss of temporal retinal nerve fibers in Parkinson’s disease: A mitochondrial pattern? Eur. J. Neurol. 2013, 20, 198–201. [Google Scholar] [CrossRef] [PubMed]
- Rohani, M.; Langroodi, A.S.; Ghourchian, S.; Falavarjani, K.G.; SoUdi, R.; Shahidi, G. Retinal nerve changes in patients with tremor dominant and akinetic rigid Parkinson’s disease. Neurol. Sci. 2013, 34, 689–693. [Google Scholar] [CrossRef]
- Jimenez, B.; Ascaso, F.J.; Cristóbal, J.A.; López del Val, J. Development of a prediction formula of Parkinson disease severity by optical coherence tomography. Mov. Disord. 2014, 29, 68–74. [Google Scholar] [CrossRef]
- Garcia-Martin, E.; Satue, M.; Otin, S.; Fuertes, I.; Alarcia, R.; Larrosa, J.M.; Polo, V.; Pablo, L.E. Retina measurements for diagnosis of Parkinson disease. Retina 2014, 34, 971–980. [Google Scholar] [CrossRef] [PubMed]
- Satue, M.; Garcia-Martin, E.; Fuertes, I.; Otin, S.; Alarcia, R.; Herrero, R.; Bambo, M.P.; Pablo, L.E.; Fernandez, F.J. Use of Fourier-domain OCT to detect retinal nerve fiber layer degeneration in Parkinson’s disease patients. Eye 2013, 27, 507–514. [Google Scholar] [CrossRef]
- Yu, J.G.; Feng, Y.F.; Xiang, Y.; Huang, J.H.; Savini, G.; Parisi, V.; Yang, W.J.; Fu, X.A. Retinal nerve fiber layer thickness changes in Parkinson disease: A meta-analysis. PLoS ONE 2014, 9, e85718. [Google Scholar] [CrossRef]
- Aydin, T.S.; Umit, D.; Nur, O.M.; Fatih, U.; Asena, K.; Nefise, O.Y.; Serpil, Y. Optical coherence tomography findings in Parkinson’s disease. Kaohsiung J. Med. Sci. 2018, 34, 166–171. [Google Scholar] [CrossRef]
- Huang, L.; Zhang, D.; Ji, J.; Wang, Y.; Zhang, R. Central retina changes in Parkinson’s disease: A systematic review and meta-analysis. J. Neurol. 2021, 268, 4646–4654. [Google Scholar] [CrossRef]
- Schrier, E.M.; Adam, C.R.; Spund, B.; Glazman, S.; BodisWollner, I. Interocular asymmetry of foveal thickness in Parkinson’s disease. J. Ophthalmo. 2012, 2012, 728457. [Google Scholar] [CrossRef]
- Aaker, G.D.; Myung, J.S.; Ehrlich, J.R.; Mohammed, M.; Henchcliffe, C.; Kiss, S. Detection of retinal changes in Parkinson’s disease with spectral-domain optical coherence tomography. Clin. Ophthalmol. 2010, 4, 1427–1432. [Google Scholar] [CrossRef]
- Lee, Y.W.; Lim, M.N.; Lee, J.Y.; Yoo, Y. Central retina thickness measured with spectral-domain optical coherence tomography in Parkinson disease: A meta-analysis. Medicine 2023, 102, e35354. [Google Scholar] [CrossRef]
- Satue, M.; Obis, J.; Rodrigo, M.J.; Otin, S.; Fuertes, M.I.; Vilades, E.; Gracia, H.; Ara, J.R.; Alarcia, R.; Polo, V.; et al. Optical Coherence Tomography as a Biomarker for Diagnosis, Progression, and Prognosis of Neurodegenerative Diseases. J. Ophthalmol. 2016, 2016, 8503859. [Google Scholar] [CrossRef] [PubMed]
- Tsironi, E.E.; Dastiridou, A.; Katsanos, A.; Dardiotis, E.; Veliki, S.; Patramani, G.; Zacharaki, F.; Ralli, S.; Hadjigeorgiou, G.M. Perimetric and retinal nerve fiber layer findings in patients with Parkinson’s disease. BMC Ophthalmol. 2012, 12, 54. [Google Scholar] [CrossRef] [PubMed]
- Cubo, E.; López Peña, M.J.; Diez-Feijo Varela, E.; Pérez Gil, O.; Garcia Gutierrez, P.; Araus González, E.; Prieto Tedejo, R.; Mariscal Pérez, N.; Armesto, D. Lack of association of morphologic and functional retinal changes with motor and non-motor symptoms severity in Parkinson’s disease. J. Neural Transm. 2014, 121, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Archibald, N.K.; Clarke, M.P.; Mosimann, U.P.; Burn, D.J. Retinal thickness in Parkinson’s disease. Park. Relat. Disord. 2011, 17, 431–436. [Google Scholar] [CrossRef]
- Messina, D.; Cerasa, A.; Condino, F.; Arabia, G.; Novellino, F.; Nicoletti, G.; Salsone, M.; Morelli, M.; Lanza, P.L.; Quattrone, A. Patterns of brain atrophy in Parkinson’s disease, progressive supranuclear palsy and multiple system atrophy. Park. Relat. Disord. 2011, 17, 172–176. [Google Scholar] [CrossRef]
- Satue, M.; Rodrigo, M.J.; Obis, J.; Vilades, E.; Gracia, H.; Otin, S.; Fuertes, M.I.; Alarcia, R.; Crespo, J.A.; Polo, V.; et al. Evaluation of progressive visual dysfunction and retinal degeneration in patients with Parkinson’s disease. Investig. Ophthalmol. Vis. Sci. 2017, 58, 1151–1157. [Google Scholar] [CrossRef]


{kind=link}
| Authors, Year of Publication | Number of Participants | Type of Implemented OCT | Assessed Retinal Parameters | Cutoff Values; (Specificity); [Sensitivity] | Main Results |
|---|---|---|---|---|---|
| Albrecht et al., 2012 [9] | 35 healthy controls 84 patients - 40 PD - 19 MSA - 10 CBS - 15 PSP | Spectral domain optical coherence tomography with manual segmentation | pRNFL, paramacular thickness and volume, thickness of all retinal layers | ONL/OPL ratio cutoff of 3.1 for differentiation between PSP and PD (96%); [59%], combined ONL/OPL ratio with INL cutoff of 46 mm (96%); [70%] | The mean total macular thickness and volume of patients with PSP were found to be significantly reduced compared with patients with PD, while the ONL/OPL ratio combined with INL changes within group with PSP may serve as a diagnostic marker |
| Schneider et al., 2013 [19] | 41 healthy controls 93 patients - 65 PD - 16 PSP - 12 MSA | Spectral domain OCT with a semiautomatic algorithm | RNFL, GCL + IPL, INL, OPL, ONL, WRT | ONL/OPL ratio cutoff of 5.03 for discrimination between PSP and MSA (88%); [91%] | Retinal parameters of patients with PD were not significantly different that those of healthy individuals, while opposite changes of ONL/OPL ratios were reported between patients’ groups with PSP and MSA |
| Ma et al., 2023 [20] | 14 healthy controls 52 patients - 24 PD - 19 MSA - 9 PSP | Spectral domain OCT | pRNFL thickness, macular thickness and volume | N/A | Specific patterns of retina alterations were reported among patients with PD and atypical Parkinsonism with a macular thinning in patients with PD and MSA and a higher peripapillary RNFL thickness in patients with PSP |
| Alkabie et al., 2019 [21] | 12 healthy controls 23 patients - 12 PD - 11 PSP | Spectral domain OCT | RNFL thickness, macular volume | RNFL thickness cutoff of 93 μm in patients with disease duration of ≥3 years for distinguishing between patients with PD and PSP (~70%), [~70%] | A significant reduction in mean RNFL thickness was observed in eyes from patients with PSP as compared with those of patients with PD with a disease duration of at least 3 years |
| Sevim et al., 2018 [22] | 33 healthy controls 39 patients - 29 PD - 10 PSP | Spectral domain OCT with automatic segmentation | pRNFL thickness, thickness and volume of retinal layers at the macula (mRNFL, GCL, IPL, INL, OPL, ONL, PRs, RPE) | N/A | A significant thinning of both pRNFL and GCL, IPL, INL was reported among patients with PSP when compared with a group with PD. Regarding levodopa use, a decreased ONL/OPL ratio and pRNFL thinning were observed among levodopa non-users compared with levodopa users |
| Rebolleda et al., 2016 [23] | 53 patients - 38 PD - 15 PSP | Spectral domain OCT | pRNFL, macular thickness, GCA | Minimum GCIPL thickness cut-off value of 69 μm for differentiating PSP from PD (91.7%), [72.7%] | A thicker mean average RNFL and a higher mean macular volume was found among patients with PD than those patients of group with PSP |
| Moreno-Ramos et al., 2013 [24] | 10 healthy controls 30 patients - 10 AD - 10 LBD - 10 PD | OCT | RNFL thickness | N/A | A greater reduction in RNFL thickness was observed in patients with Lewy body dementia compared with the group with PD dementia, with a significant positive correlation between disease severity and retinal parameters |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karatzetzou, S.; Parisis, D.; Ioannidis, S.; Afrantou, T.; Ioannidis, P. Optical Coherence Tomography as a Biomarker in the Differential Diagnosis between Parkinson’s Disease and Atypical Parkinsonian Syndromes: A Narrative Review. Appl. Sci. 2024, 14, 2491. https://doi.org/10.3390/app14062491
Karatzetzou S, Parisis D, Ioannidis S, Afrantou T, Ioannidis P. Optical Coherence Tomography as a Biomarker in the Differential Diagnosis between Parkinson’s Disease and Atypical Parkinsonian Syndromes: A Narrative Review. Applied Sciences. 2024; 14(6):2491. https://doi.org/10.3390/app14062491
Chicago/Turabian StyleKaratzetzou, Stella, Dimitrios Parisis, Serafeim Ioannidis, Theodora Afrantou, and Panagiotis Ioannidis. 2024. "Optical Coherence Tomography as a Biomarker in the Differential Diagnosis between Parkinson’s Disease and Atypical Parkinsonian Syndromes: A Narrative Review" Applied Sciences 14, no. 6: 2491. https://doi.org/10.3390/app14062491