

Development and Validation of a Prediction Model for Differentiation of Benign and Malignant Fat-Poor Renal Tumors Using CT Radiomics
 , , , and
, , , and
Abstract
:1. Introduction
2. Methods
2.1. Patients
2.2. Radiomics Workflow
2.3. Radiomics Feature Extraction and Feature Selection
2.4. Ethic Statement, Statistics, and Machine Learning
3. Results
3.1. Demographic Characteristics of the Patients
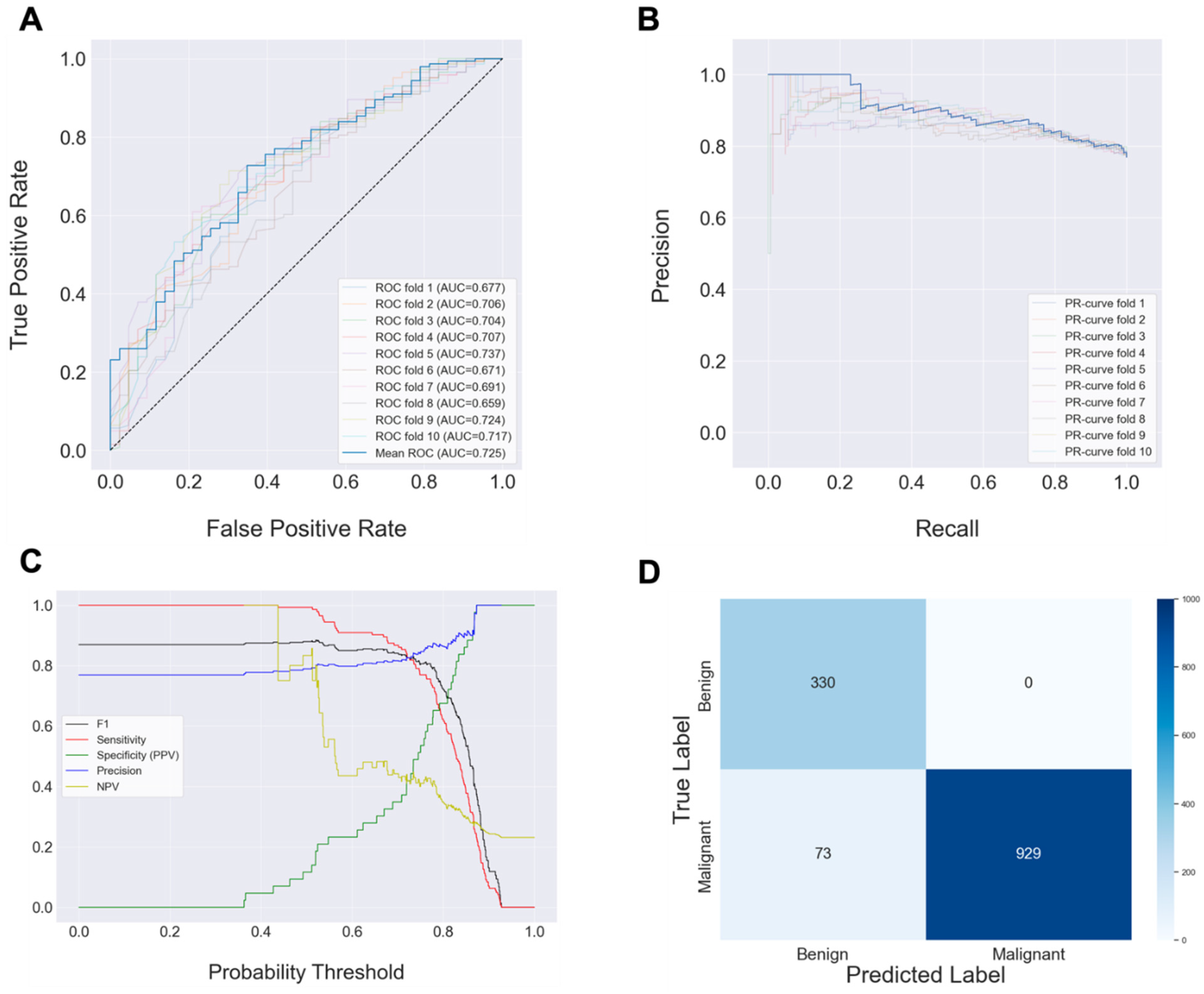
3.2. Multi-Phase CT Radiomic Features-Based Machine Learning Model
3.3. Single-Phase CT Radiomic Feature-Based Machine Learning Model
4. Discussion
5. Conclusions
6. Code Availability
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Ljungberg, B.; Bensalah, K.; Canfield, S.; Dabestani, S.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; Lam, T.; Marconi, L.; Merseburger, A.S.; et al. EAU guidelines on renal cell carcinoma: 2014 update. Eur. Urol. 2015, 67, 913–924. [Google Scholar] [CrossRef] [PubMed]
- Donat, S.M.; Diaz, M.; Bishoff, J.T.; Coleman, J.A.; Dahm, P.; Derweesh, I.H.; Herrell, S.D., 3rd; Hilton, S.; Jonasch, E.; Lin, D.W.; et al. Follow-up for Clinically Localized Renal Neoplasms: AUA Guideline. J. Urol. 2013, 190, 407–416. [Google Scholar] [CrossRef] [PubMed]
- Capitanio, U.; Bensalah, K.; Bex, A.; Boorjian, S.A.; Bray, F.; Coleman, J.; Gore, J.L.; Sun, M.; Wood, C.; Russo, P. Epidemiology of Renal Cell Carcinoma. Eur. Urol. 2019, 75, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Luciano, R.L.; Moeckel, G.W. Update on the Native Kidney Biopsy: Core Curriculum 2019. Am. J. Kidney Dis. 2019, 73, 404–415. [Google Scholar] [CrossRef] [PubMed]
- Flum, A.S.; Hamoui, N.; Said, M.A.; Yang, X.J.; Casalino, D.D.; McGuire, B.B.; Perry, K.T.; Nadler, R.B. Update on the Diagnosis and Management of Renal Angiomyolipoma. J. Urol. 2016, 195, 834–846. [Google Scholar] [CrossRef] [PubMed]
- Lubner, M.G. Radiomics and Artificial Intelligence for Renal Mass Characterization. Radiol. Clin. N. Am. 2020, 58, 995–1008. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Hong, S.H. Use of artificial intelligence to characterize renal tumors. Investig. Clin. Urol. 2022, 63, 123–125. [Google Scholar] [CrossRef] [PubMed]
- Uhm, K.H.; Jung, S.W.; Choi, M.H.; Shin, H.K.; Yoo, J.I.; Oh, S.W.; Kim, J.Y.; Kim, H.G.; Lee, Y.J.; Youn, S.Y.; et al. Deep learning for end-to-end kidney cancer diagnosis on multi-phase abdominal computed tomography. NPJ Precis. Oncol. 2021, 5, 54. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Guestrin, C. Xgboost: A scalable tree boosting system. In Proceedings of the 22nd Acm Sigkdd International Conference on Knowledge Discovery and Data Mining, San Francisco, CA, USA, 13–17 August 2016; pp. 785–794. [Google Scholar]
- Akiba, T.; Sano, S.; Yanase, T.; Ohta, T.; Koyama, M. Optuna: A Next-generation Hyperparameter Optimization Framework. In Proceedings of the 25th ACM SIGKDD International Conference on Knowledge Discovery & Data Mining, Anchorage, AK, USA, 4–8 August 2019; Association for Computing Machinery: New York, NY, USA, 2019; pp. 2623–2631. [Google Scholar]
- Lemaître, G.; Nogueira, F.; Aridas, C.K. Imbalanced-learn: A python toolbox to tackle the curse of imbalanced datasets in machine learning. J. Mach. Learn. Res. 2017, 18, 559–563. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Van Griethuysen, J.J.; Fedorov, A.; Parmar, C.; Hosny, A.; Aucoin, N.; Narayan, V.; Beets-Tan, R.G.; Fillion-Robin, J.-C.; Pieper, S.; Aerts, H.J. Computational radiomics system to decode the radiographic phenotype. Cancer Res. 2017, 77, e104–e107. [Google Scholar] [CrossRef] [PubMed]
- Klontzas, M.E.; Gatti, A.A.; Tejani, A.S.; Kahn, C.E., Jr. AI Reporting Guidelines: How to Select the Best One for Your Research. Radiol. Artif. Intell. 2023, 5, e230055. [Google Scholar] [CrossRef] [PubMed]
- Moor, M.; Banerjee, O.; Abad, Z.S.H.; Krumholz, H.M.; Leskovec, J.; Topol, E.J.; Rajpurkar, P. Foundation models for generalist medical artificial intelligence. Nature 2023, 616, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Chambon, P.; Bluethgen, C.; Langlotz, C.P.; Chaudhari, A. Adapting pretrained vision-language foundational models to medical imaging domains. arXiv 2022, arXiv:2210.04133. [Google Scholar]
- Qin, Z.; Yi, H.; Lao, Q.; Li, K. Medical image understanding with pretrained vision language models: A comprehensive study. arXiv 2022, arXiv:2209.15517. [Google Scholar]
- Kirillov, A.; Mintun, E.; Ravi, N.; Mao, H.; Rolland, C.; Gustafson, L.; Xiao, T.; Whitehead, S.; Berg, A.C.; Lo, W.-Y. Segment anything. arXiv 2023, arXiv:2304.02643. [Google Scholar]
- Radford, A.; Kim, J.W.; Hallacy, C.; Ramesh, A.; Goh, G.; Agarwal, S.; Sastry, G.; Askell, A.; Mishkin, P.; Clark, J. Learning transferable visual models from natural language supervision. In Proceedings of the International Conference on Machine Learning: PMLR, Virtual, 18–24 July 2021; pp. 8748–8763. [Google Scholar]
- Nie, P.; Yang, G.; Wang, Y.; Xu, Y.; Yan, L.; Zhang, M.; Zhao, L.; Wang, N.; Zhao, X.; Li, X.; et al. A CT-based deep learning radiomics nomogram outperforms the existing prognostic models for outcome prediction in clear cell renal cell carcinoma: A multicenter study. Eur. Radiol. 2023. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Gong, M.; Zhou, D.; Yuan, R.; Kong, J.; Jiang, F.; Zhang, L.; Chen, W.; Li, Y. A CT-based radiomics nomogram for differentiation of benign and malignant small renal masses (≤4 cm). Transl. Oncol. 2023, 29, 101627. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; He, X.; Shao, W.; Bian, J.; Terry, R. Classification of Benign and Malignant Renal Tumors Based on CT Scans and Clinical Data Using Machine Learning Methods. Informatics 2023, 10, 55. [Google Scholar] [CrossRef]
- Klontzas, M.E.; Koltsakis, E.; Kalarakis, G.; Trpkov, K.; Papathomas, T.; Sun, N.; Walch, A.; Karantanas, A.H.; Tzortzakakis, A. A pilot radiometabolomics integration study for the characterization of renal oncocytic neoplasia. Sci. Rep. 2023, 13, 12594. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Training Dataset | Test Dataset | p Value | |
|---|---|---|---|
| Gender | 396 | 103 | 0.412 |
| Male (%) | 222 (56.3%) | 63 (61.2%) | |
| Female (%) | 174 (43.7%) | 40 (38.8%) | |
| Age (years, range) | 57.0 (22, 83) | 54.0 (27, 79) | 0.708 |
| Cancer size (cm, range) | 3.573 (0.7, 17.5) | 3.291 (1.0, 9.4) | 0.294 |
| Renal tumor | 0.9 | ||
| Benign (%) | 99 (25%) | 27 (26.2%) | |
| Malignant (%) | 297 (75%) | 76 (73.8%) |
| AU-ROC | AU-PRC | ACC | ||||
|---|---|---|---|---|---|---|
| Linear SVM | ||||||
| Rbf SVM | ||||||
| XGBoost | ||||||
| Random Forest | ||||||
| Probability Threshold | F1 Score | Precision | Sensitivity | Specificity (PPV) | NPV | |
| Linear SVM | 0.7555 | |||||
| Rbf SVM | 0.8044 | |||||
| XGBoost | 0.715 | |||||
| Random Forest | 0.79 | |||||
| AU-ROC | AU-PRC | |||||||
|---|---|---|---|---|---|---|---|---|
| CT Phase | Arterial | Delayed | Non-Contrast | Portal | Arterial | Delayed | Non-Contrast | Portal |
| Sample Size (Train/Test) | 236/82 | 252/88 | 318/101 | 360/81 | 236/82 | 252/88 | 318/101 | 360/81 |
| Linear SVM | ||||||||
| Rbf SVM | ||||||||
| XGBoost | ||||||||
| Random Forest | ||||||||
| ACC | F1 Score | |||||||
| CT Phase | Arterial | Delayed | Non-Contrast | Portal | Arterial | Delayed | Non-Contrast | Portal |
| Sample Size (Train/Test) | 236/82 | 252/88 | 318/101 | 360/81 | 236/82 | 252/88 | 318/101 | 360/81 |
| Linear SVM | ||||||||
| Rbf SVM | ||||||||
| XGBoost | ||||||||
| Random Forest | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bang, S.; Wang, H.-H.; Kim, H.; Choi, M.H.; Cha, J.; Choi, Y.; Hong, S.-H. Development and Validation of a Prediction Model for Differentiation of Benign and Malignant Fat-Poor Renal Tumors Using CT Radiomics. Appl. Sci. 2023, 13, 11345. https://doi.org/10.3390/app132011345
Bang S, Wang H-H, Kim H, Choi MH, Cha J, Choi Y, Hong S-H. Development and Validation of a Prediction Model for Differentiation of Benign and Malignant Fat-Poor Renal Tumors Using CT Radiomics. Applied Sciences. 2023; 13(20):11345. https://doi.org/10.3390/app132011345
Chicago/Turabian StyleBang, Seokhwan, Hee-Hwan Wang, Hokun Kim, Moon Hyung Choi, Jiook Cha, Yeongjin Choi, and Sung-Hoo Hong. 2023. "Development and Validation of a Prediction Model for Differentiation of Benign and Malignant Fat-Poor Renal Tumors Using CT Radiomics" Applied Sciences 13, no. 20: 11345. https://doi.org/10.3390/app132011345