
Can Vitamin C Improve Proliferation and Viability of Smokers’ Gingival Fibroblasts on Collagen Membranes? An In Vitro Study

Department of Periodontics and Community Dentistry, College of Dentistry King Saud University, Riyadh 12372, Saudi Arabia
Appl. Sci. 2023, 13(19), 10828; https://doi.org/10.3390/app131910828
Submission received: 7 September 2023
/
Revised: 25 September 2023
/
Accepted: 28 September 2023
/
Published: 29 September 2023
(This article belongs to the Special Issue Advanced Materials and Technology in Dental, Oral and Maxillofacial Health)
Abstract
:Periodontal regeneration using a barrier membrane can be affected by several factors, including patient-related factors (such as smoking habits), surgical techniques, and type of barrier membrane. Smoking exposure has a negative impact on the periodontium due to its direct inhibition of gingival fibroblast function. Vitamin C is widely recognized as an antioxidant that can be used to mitigate the detrimental impact of smoking products on periodontal cells. This study aimed to investigate whether vitamin C could improve the proliferation and viability of gingival fibroblasts extracted from smoking and non-smoking donors and then cultured on non-crosslinked (CopiOs Pericardium) and crosslinked (BioMend) collagen membranes. To address this aim, human gingival fibroblasts were extracted from healthy periodontium of smoker patients (Group 1) and non-smoker patients (Group 2). The cells were cultivated and subsequently subcultured in a growth medium supplemented with the required nutrients. Subsequently, the medium at passage six was supplemented with vitamin C, i.e., at the start of the experiment. An evaluation of cell proliferation and viability was carried out using cell migration assays and AlamarBlue® assays for cells grown on BioMend and CopiOs Pericardium collagen membranes. Assessment of the morphology and attachment of gingival fibroblasts to the experimental collagen membranes was conducted using scanning electron microscopy (SEM). The viability and proliferation assessments of hGFs from the migration assay were evaluated using AlamarBlue®. The results exhibited significant fluorescent intensity of gingival fibroblasts on both membrane groups (BioMend and CopiOs Pericardium) in the smoker group compared to the non-smoker group (p < 0.05), which was interpreted to be the result of hGF metabolic activity and the exclusion of any cytotoxic effects, particularly from vitamin C addition. Vitamin C positively affected cells from the smoker group with statistically significant results in the BioMend group (Wilcoxon signed-rank test of p value < 0.05; p = 0.028). SEM images revealed the crosslinking pattern of the BioMend membrane and the non-crosslinked natural tissue structure of the CopiOs Pericardium membrane, which did not change regardless of whether the cultured smoker or non-smoker hGFs were treated with vitamin C. Small numbers of attached hGFs in membrane matrices in all samples, mainly in the peripheries, were observed. It can be concluded that the addition of vitamin C to collagen membranes in vitro seems to combat the adverse effects of smoking products on gingival fibroblasts.
1. Introduction
Periodontitis is a pathological condition characterized by inflammation arising from the intricate interaction between the bacterial microbiota and the human immune response, which is frequently influenced by behavioral variables [1]. The aim of periodontal therapy is to control periodontal tissue inflammation, while the ideal goal is to regenerate the periodontal tissue that has been lost as a consequence of destruction caused by periodontitis or traumatic injury [2]. The biological concept of potentially regenerating various tissue components as a part of the healing process following periodontal surgery was introduced early in the 1980s [3].
Clinical application of guided periodontal tissue regeneration is based on the principle of using a physical barrier membrane to shield the affected area from undesirable tissue ingrowth, while guiding the repopulation of periodontal and bone cells [2,4]. Not all regenerative procedures are associated with the same level of clinical efficacy. Several factors, including patient and surgical factors, influence clinical outcomes [2].
At least 20% of etiological factors for periodontal tissue destruction can be attributed to tobacco use [5]. Therefore, smoking is recognized as a risk factor in the periodontitis grading system [6,7]. The direct suppression of normal fibroblast function may be responsible for a variety of underlying effects of tobacco products on periodontal tissues [8].
On the other hand, the surgical factor with a critical effect on the outcome of the tissue regeneration procedure involves the proper selection of the barrier membrane [9]. Bioabsorbable membranes comprising type I bovine or porcine collagen or poly(hydroxy acids), such as poly(lactic acid) (PLA), poly(glycolic acid) (PGA), and their co-polymers, are predominantly utilized in periodontal regeneration [10]. Biocompatibility with periodontal cells (particularly gingival fibroblasts) plays an important role if the membrane is exposed to the oral environment, which presents many challenges during the regeneration process [11]. BioMend®, made from glutaraldehyde-crosslinked bovine type I collagen, is one of the most commonly used collagen membranes [12]. Another commonly used, but non-crosslinked, bioabsorbable membrane is CopiOs® Pericardium, which is composed of pericardium-derived collagen types I and III. Different strategies to promote regeneration of periodontal defects have been developed. Expanding the functions of these membranes as not only barriers but also delivery devices for various agents, such as anti-oxidants, is a recently introduced approach [13].
The role of antioxidants in overall health, and particularly in the health of oral hard and soft tissues, is well established in the literature [14], and there is evidence that antioxidant supplements are necessary for the successful prevention and treatment of disease, including gingival and periodontal diseases [15,16,17]. Vitamin C, as a water-soluble and potent reducing agent, is an effective antioxidant that has been shown to regulate the procollagen gene’s expression, which impacts both collagen synthesis and fibroblast transformation [18]. It has been demonstrated that vitamin C alters the epigenetic/gene expression profile and extracellular matrix (microenvironment) of human cells [15]. In addition, this vitamin stimulates the osteoblasts’ growth, metabolism, differentiation, and morphogenesis [19]. Vitamin C has been suggested as a supplement capable of reducing the negative effects of toxic compounds in tobacco smoke, as it protects the aqueous components of cells (particularly the cytoplasm) against oxidative reactions and free radicals [20]. Vitamin C, when administered systemically, locally, or both, reverses the negative effects of nicotine and cotinine on human gingival fibroblasts [20,21,22]. Biomaterials containing vitamin C (i.e., microspheres, scaffolds, tissue adhesives, and hydrogels) may aid in the bioengineering and regeneration of soft and hard oral tissues [23] in which Vitamin C assumes a significant function in safeguarding against oxidative stress in diverse tissues, and it represents an exceptional and secure strategy to mitigate the detrimental effects of smoking toxicity [24]. Therefore, incorporating Vitamin C in resorbable collagen membranes may provide an additional advantage for periodontal regeneration, especially in smokers.
The purpose of this study is to investigate if vitamin C can improve the proliferation and viability of gingival fibroblasts extracted from smoking and non-smoking donors and then cultured on non-crosslinked (CopiOs Pericardium) and crosslinked (BioMend) collagen membranes.
2. Materials and Methods
2.1. Ethical Guidelines
The present investigation was carried out in accordance with the protocols of King Saud University (KSU). Ethical approval for the study was obtained from the Ethics Committee of the Institutional Review Board (IRB) at KSU, under Project No. E-18-3071. Additionally, the College of Dentistry Research Center also granted its approval for the study (CDRC No. PR0071). Participants who took part in the study gave their written consent after receiving appropriate explanations of the study and its procedures. The study protocol was carried out at the Stem Cell Unit laboratory, located in the Department of Anatomy at the College of Medicine, King Saud University in Riyadh, Saudi Arabia.
2.2. Human Gingival Tissue Explantation
The gingival connective tissues from two healthy adult males, both under the age of 20, were obtained for analysis. The inclusion criteria encompassed the presence of clinically healthy gingiva that exhibited no signs of inflammation, such as erythema, edema, or bleeding. The exclusion criteria encompassed those with documented systemic disorders and those who had received antibiotic treatment within the preceding month. Gingival samples were taken after the dental surgical procedures that involved the excision of gingival tissues, such as third molar extraction, gingivectomies, or surgical crown lengthening surgery. These procedures were conducted at the College of Dentistry, King Saud University, located in Riyadh, Saudi Arabia. The study was carried out using gingival tissues excised from two human participants who agreed to donate their tissues. The first tissue samples were harvested from a ‘non-smoker’ who did not engage in smoking activities, including the use of cigarettes, hookah, or vaporizers, and were labeled as (N-N). In contrast, the second group of samples (S-S) were harvested from an individual who was a regular cigarette smoker, consuming a minimum of 20 cigarettes per day for a duration of at least 2 years [25]. The gingival tissue samples were handled using aseptic techniques and transferred to the laboratory in 15 mL centrifuge tubes (BD FalconTM, Edison, NJ, USA) filled with fibroblast culture media. The medium was prepared for direct explant culture in a laminar-flow hood.
2.3. Culture of Human Gingival Fibroblasts (hGFs)
The excised tissues underwent a triple rinse using phosphate-buffered saline (PBS; Gibco® Life Technologies, Roskilde, Denmark) supplemented with 10,000 IU/mL penicillin–streptomycin (Pen-Strep; Gibco®, Carlsbad, CA, USA). The specimens were sectioned into 23 mm fragments and placed in the central region of individual wells in Corning® six-well tissue culture plates (Tewksbury, MA, USA). Subsequently, the explants were coated with a small quantity of fibroblast culture medium, approximately 0.5 mL, which consisted of Dulbecco’s modified Eagle’s medium with high glucose (DMEM; Gibco®, BRL, Grand Island, NY, USA). This medium was supplemented with 10% fetal bovine serum (FBS; Gibco®), 1% Pen-Strep (Gibco®), and 1% MEM non-essential amino acids (Invitrogen Gibco®). The purpose of this medium was to facilitate the attachment of cells to the culture plate. Prior to the addition of 1 mL of fresh medium, the tissues were subjected to incubation at a temperature of 37 °C for a duration of 30 min inside a humidified environment consisting of 5% CO2 and 95% oxygen. The culture medium was replaced at 72 h intervals until cellular migration from the tissue explant became apparent.
2.4. Subculture and Expansion of hGFs
The non-adherent cells were eliminated, and afterwards, fresh culture media was supplied until the confluence of migrating cells reached 80–90%. In order to ascertain the attainment of the desired confluence of the cells, an inverted phase-contrast microscope (Carl Zeiss®, Axio Observer A1 inverted microscope, Leica, Berlin, Germany) was employed. The confluent cells adhering to the plastic surface were passaged by treating them with 0.25% trypsin/EDTA (Gibco®) for a duration of 2–3 min at a temperature of 37 °C while periodically swaying the flask. The trypsin/EDTA reagent was neutralized using a full DMEM solution that was double the volume of the reagent. The cell suspensions were thereafter subjected to centrifugation at a speed of 1500 revolutions per minute (rpm) for a duration of 5 min. The supernatant was then removed via aspiration and disposed of. The cell pellets were reconstituted in 5 mL of complete media. Following the process of dilution and division, the cells were allocated into two T-75 flasks. Subsequently, a fresh growth medium was introduced to facilitate the expansion of the cells. The cells were routinely examined using an inverted phase-contrast microscope. The experiments were conducted utilizing cells derived from the sixth passage.
2.5. Experimental Collagen Membrane Groups
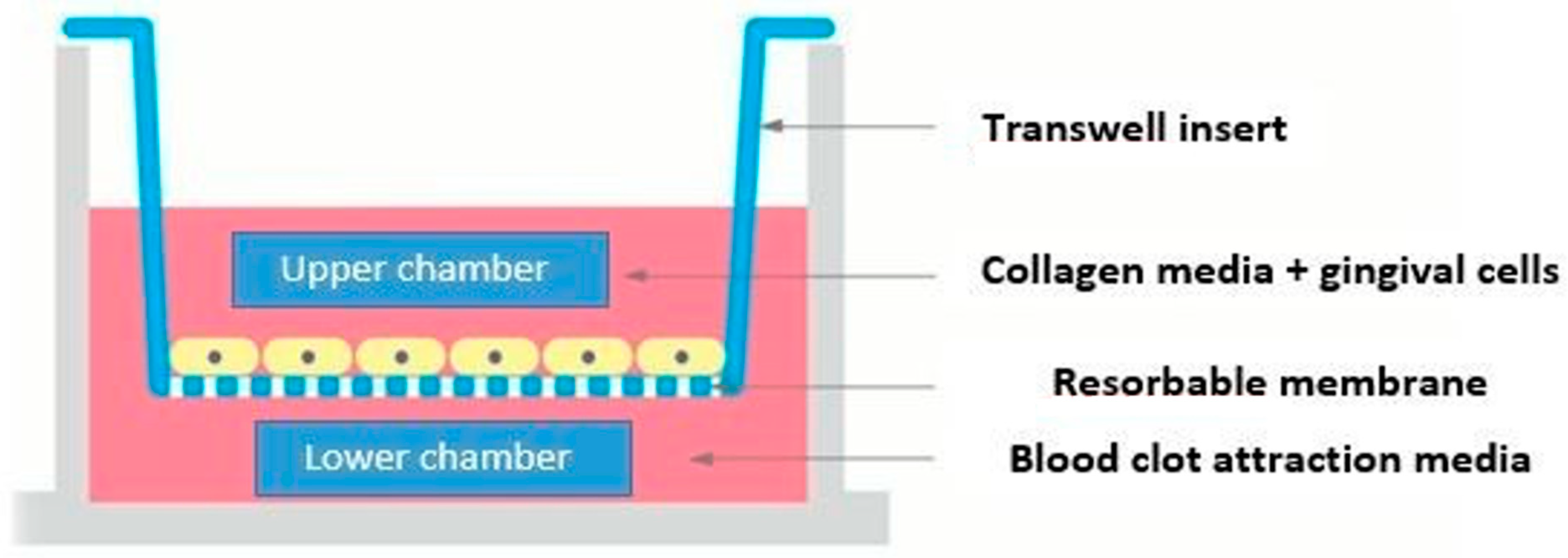
A cell migration assay was performed in polycarbonate 12-transwell chemotaxis plates with cell culture inserts of 8.00 µm pore size PET track-etched membranes (Becton Dickinson Labware, Franklin Lakes, NJ, USA), as illustrated in Figure 1. Bioabsorbable BioMend® collagen membranes (Sulzer Medica, Colla-Tec Inc., Plainsboro, NJ, USA) and CopiOs® Pericardium membranes (Zimmer Biomet Dental, Parsippany-Troy Hills, FL, USA) were placed in the insert according to the experimental groups shown in Table 1. All experiments were performed in triplicate.
The experiment started with cell starvation using cultured hGFs at 90% confluence. After removing the previous medium, cells were washed with PBS. Then, 20 mL of medium with 1% serum (100 mL of DMEM + 1 mL FBS + 1 mL penicillin–streptomycin + 1 mL non-essential amino acids) was added to a T-175 flask and incubated for 24 h. After incubation, cells were washed with PBS before adding 3 mL/flask trypsin (0.25%) and placing them in an incubator for 5 min. The cells that had been incubated with 1% medium were centrifuged for 5 min at 1500 rpm. The cells were counted to seed 3 × 105 cells/cell culture insert. The 12-well size cutter customized in the physical lab of the Dental College, King Saud University, Riyadh, KSA, was used to cut the membranes to fit each insert before seeding cells on the membranes. Vitamin C was then added to the treatment groups. The attraction medium used in the lower chamber of all the groups was the 10% culture medium used for cell culture and subculture. All the plates were incubated for 3 days before proceeding to the next test [21,22,26].
2.6. Assessment of Cell Viability and Proliferation/AlamarBlue® Assay Viability Test
Based on previously published protocols [21,22] AlamarBlue® assay (Thermo Fisher Scientific, Waltham, MA, USA) was employed to evaluate the grown cells derived from the four conditions within the two experimental groups. Cells were transferred to 96-well plates in triplicate and then cultured with AlamarBlue® substrate in the amount of 10% of the sample volume (i.e., 20 μL AlamarBlue® reagent to 200 μL sample/well), followed by a 2–4 h incubation at 37 °C. The absorbance of AlamarBlue® reagent in the fluorescent mode (Ex 530 nm/Em 590 nm) was measured using a spectrophotometer, BioTek Synergy II microplate reader (BioTek Inc., Winooski, VT, USA), and analyzed with Gen5 data analysis software version 3.13 (BioTek®).
2.7. Evaluation of Cell Attachment/Scanning Electron Microscopy (SEM)
SEM analysis was performed on experimental membrane samples to assess the morphology and attachment of hGFs after 3 days. Membranes were prepared using fixation with 2.5% glutaraldehyde for 48 h at −40 °C followed by subsequent dehydration using increasing concentrations of ethanol. Then, the samples were coated via gold sputtering before being viewed using an SEM (JEOL-JSM-6360 LV; JEOL Inc., Peabody, MA, USA).
3. Statistical Analysis
Statistical analysis was performed using SPSS v.21 (IBM, New York, NY, USA). The statistics are presented in terms of means, medians, and standard deviations (SDs). The Kolmogorov–Smirnov and Shapiro–Wilk normality tests were conducted in order to determine the normality of the data distribution, which was not found. Therefore, non-parametric tests were utilized in this study. The Wilcoxon signed-rank test was used for comparisons within the groups before and after treatment with vitamin C, while pair-wise comparisons between study groups were conducted using the Mann–Whitney U test. The experiments were performed in duplicate.
4. Results
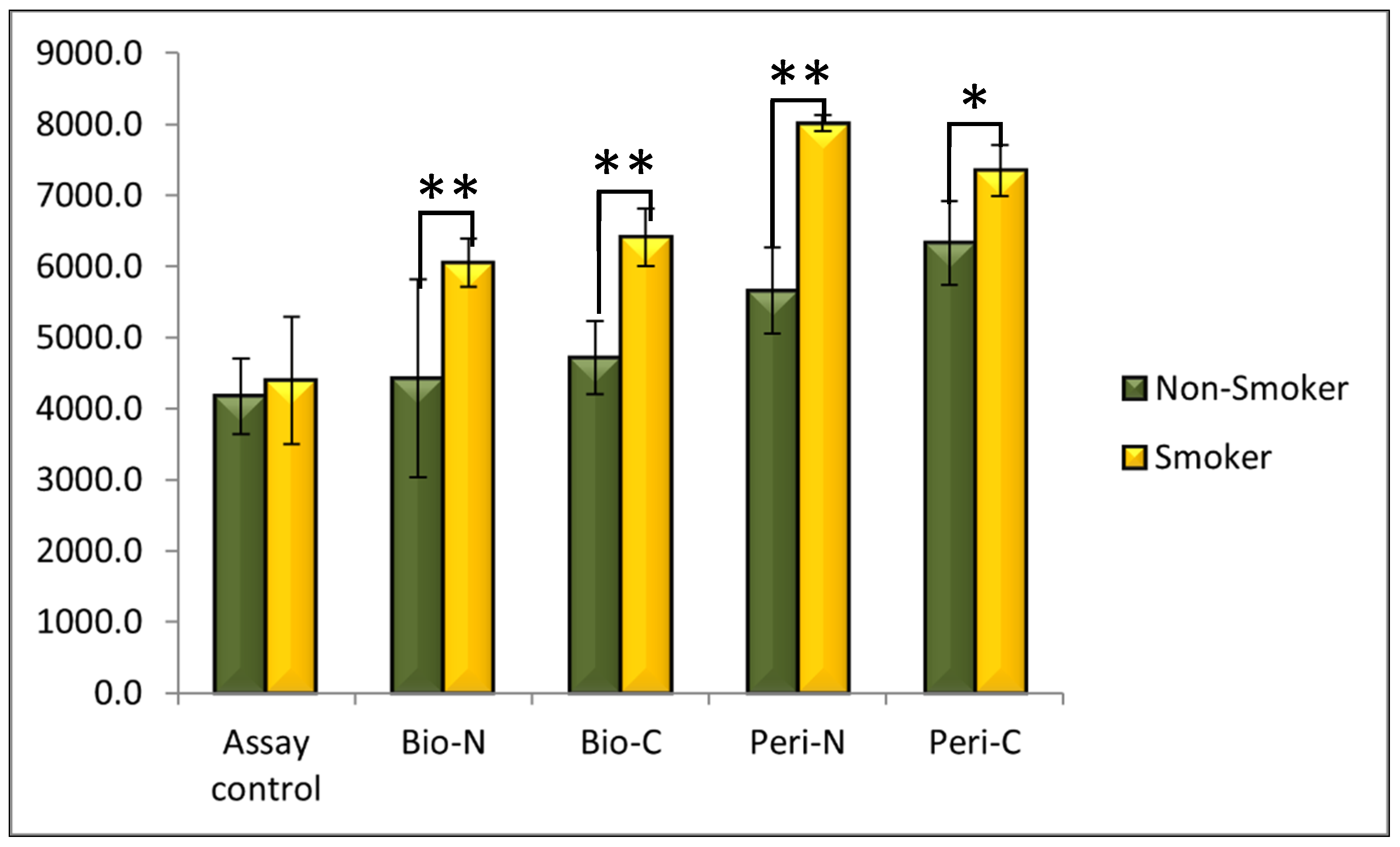
The viability and proliferation assessments of hGFs from the migration assay were evaluated using AlamarBlue®. All membrane groups (BioMend and CopiOs Pericardium) exhibited increased fluorescence intensities (Table 2), with significantly higher results in the smoker group membranes compared to those of the non-smoker group (p < 0.05) (Figure 2). A higher activity was observed in all pericardium membrane models compared to BioMend membranes, regardless of the cell source and treatment induction. The Wilcoxon signed-rank test showed a statistically significant increase in the mean viability of cells cultured on BioMend collagen membranes after treatment with vitamin C (Bio-C) 6411.0 ± 401.1 when compared to the mean before treatment with vitamin C (Bio-N) 6055.2 ± 339.6 (p = 0.028; p value < 0.05) among smokers. However, there was no statistically significant difference among the non-smoker BioMend group after treatment with vitamin C (Bio-C) (p = 0.917).
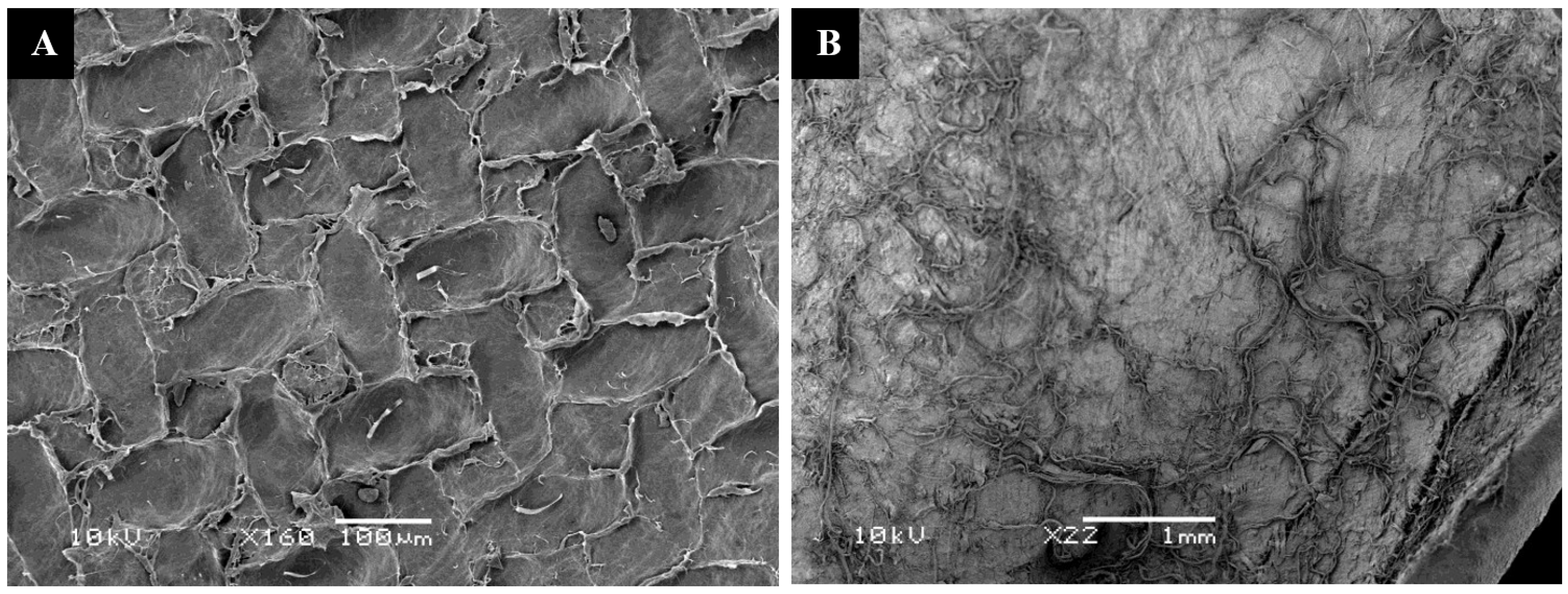
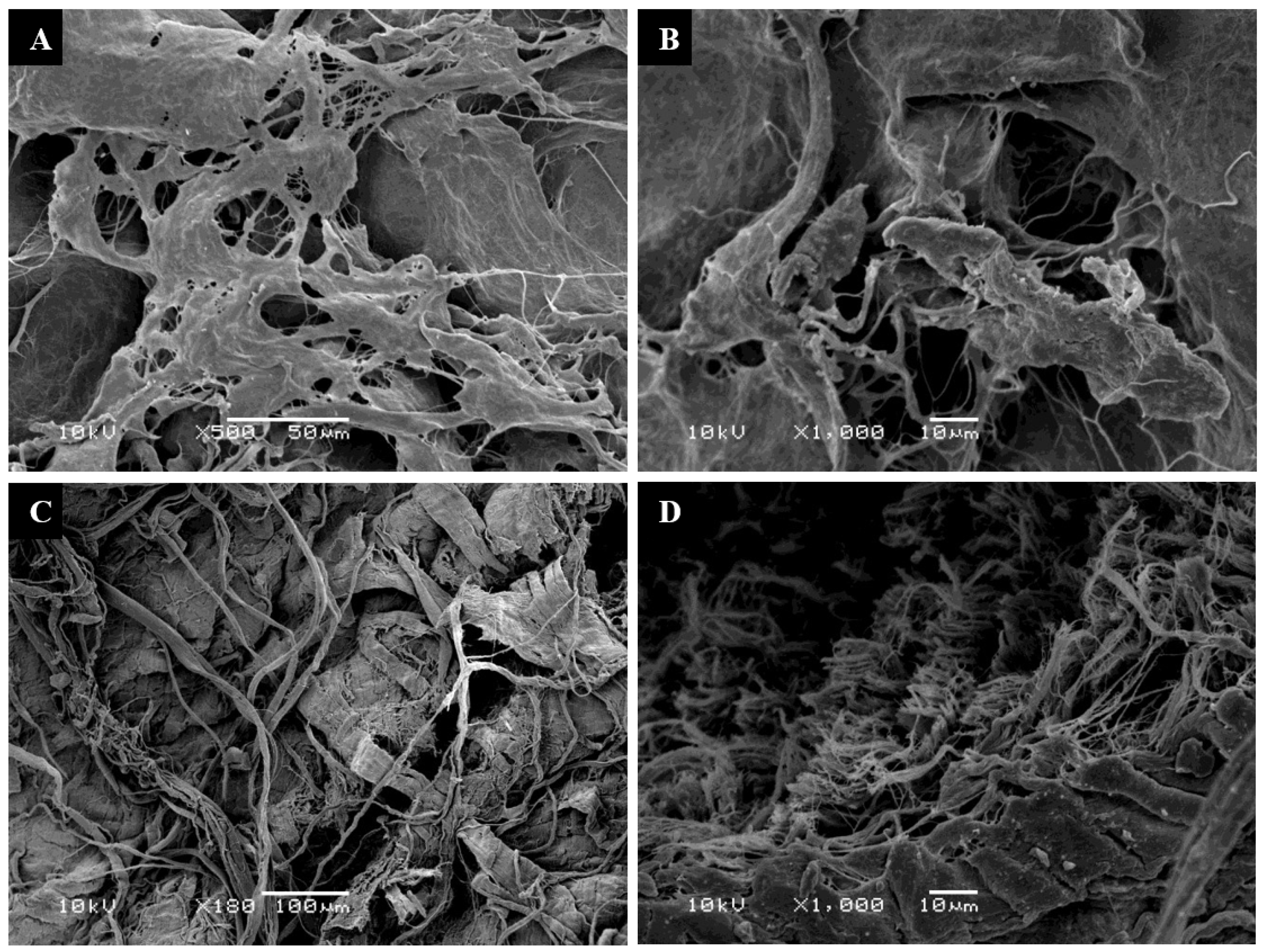
SEM images revealed the crosslinked pattern of the BioMend membrane and the non-crosslinked natural tissue structure of the CopiOs Pericardium membrane (Figure 3A,B). The original microscopy patterns of both membranes’ structures did not change, regardless of whether the cultured smoker or non-smoker hGFs were treated with vitamin C. Small numbers of attached hGFs in membrane matrices of all samples for all models, mainly in the peripheries, were observed. There were no significant differences in the number of attached fibroblasts between samples from smokers and non-smokers after vitamin C treatment. Additionally, SEM analysis of BioMend and pericardium membranes did not demonstrate a marked increase in the number of hGFs on the surface (Figure 4A–D and Figure 5A–D). Although SEM images of pericardium membranes revealed fewer attached hGFs than images of BioMend membranes, the results were not statistically significant. All models showed limited numbers of flat polyhedral cells with long cytoplasmic extensions attached to the membrane surfaces.
5. Discussion
This study aimed to investigate if vitamin C can improve the functional ability of human gingival fibroblasts (hGFs) extracted from smoking and non-smoking donors and then cultured on non-crosslinked (CopiOs) and crosslinked (BioMend) collagen membranes. The findings indicate that vitamin C has the potential to mitigate the detrimental impact of smoking products on gingival fibroblasts when cultivated in vitro on collagen membranes.
Periodontal tissue regeneration using a barrier collagen membrane, called guided tissue regeneration (GTR), is a common clinical periodontal procedure. The principle of GTR is based on using a physical barrier to shield the affected area from undesirable tissue ingrowth, while guiding the repopulation of periodontal and bone cells [2]. Importantly, gingival fibroblasts have a vital role in periodontal regeneration.
According to McGuire et al. [27], the utilization of an appropriate collagen membrane material has the potential to expedite the process of tissue repair by facilitating the attachment and growth of gingival fibroblasts. Collagen membranes are manufactured for clinical applications in two forms: native (non-crosslinked) or chemically processed (crosslinked). The chemical processing involves the introduction of covalent bonds to enhance the strength of collagen fibers [4,9,11,28,29]. Nevertheless, there has been limited research conducted on the impact of crosslinking collagen membranes on the bioactivity of gingival fibroblasts. Therefore, the present in vitro investigation examined the vitality and proliferation of gingival fibroblasts on a native collagen membrane (CopiOs) in comparison to a crosslinked collagen membrane (BioMend). The findings of our study revealed a notable increase in the fluorescence intensity of gingival fibroblasts when exposed to both BioMend and CopiOs collagen membranes. Furthermore, scanning electron microscopy (SEM) pictures revealed that gingival fibroblasts adhered to both membranes, corroborating the findings of the fluorescent test. It can be inferred that crosslinking does not inherently lead to a decrease in the proliferation of gingival fibroblasts.
In the literature, several clinical studies have confirmed the negative role of nicotine, one of the particulate components of tobacco smoke, in periodontal health [30]. Smoking is a risk factor that increases the severity of periodontal tissue destruction and decreases the function of regenerative cells (e.g., gingival fibroblasts) [31]. Cigarettes are comprised of many toxic chemicals, including reactive oxygen species, which have the potential to directly impede the functioning of gingival fibroblasts [31]. In fact, the period of smoking exposure can differently inhibit the growth of hGFs. Papaioannou (1998) found that exposure for more than 9 weeks causes a decrease of 23% in hGFs growth. Therefore, the absence of correlation observed in the vitality of smokers’ human gingival fibroblasts (hGFs) may be attributed to the intracellular impact of nicotine. It can be noted that nicotine acts on lysosomes by lowering the inner pH [32]. Additionally, hGFs appear to be differently sensitive to nicotine. This can be due to their high rate of replication or to the lower metabolic activity. In our in vitro work, gingival fibroblasts from smokers have different growth properties compared to fibroblasts from non-smokers, independent of the collagen membrane.
Vitamin C is acknowledged as an antioxidant supplement that can combat the adverse effects of smoking products on periodontal cells [33,34]. Our results showed that hGFs exhibited significant fluorescent intensities when seeded on a collagen membrane and before or after the addition of vitamin C. Furthermore, this can be interpreted as the result of hGFs’ metabolic activity integrity and the exclusion of any cytotoxic effects, particularly from vitamin C addition.
When comparing smokers to non-smokers before and after treatment with vitamin C, the Mann–Whitney U test showed that cells from smokers had statistically significantly higher results on both collagen membranes. However, the addition of vitamin C was markedly greater in smoker hGFs with the BioMend membrane compared to non-smokers’ cells, which indicated the positive effect of vitamin C addition on the efficacy of the membrane in the smoker environment. The current findings illustrate the promising potential of using collagen membranes as carriers for vitamin C.
The current study focused on the in vitro behavior of hGFs extracted from healthy gingiva of smoker patients compared to non-smokers, and then seeded on two types of collagen membranes (i.e., BioMend and CopiOs). In terms of hGF attachment to the membranes, SEM analysis revealed that both membranes’ topographies supported cell adhesion. The limited number of flat polyhedral cells with long cytoplasmic extensions attached to the membrane surfaces may have been caused by the short incubation duration, which was 3 days in this experiment; another reason may be that cells were lost in the process of preparation and fixation. Similar results were observed in another experiment that involved a crosslinked membrane [35]. The AlamarBlue viability assay was used to assess the viability and proliferation of the cultured cells on the collagen membranes using a migration assay assembly. Resazurin (7-hydroxy-10-oxidophenoxazin-10-ium-3-one) is the active constituent in the AlamarBlue assay. It is stable in culture medium, non-toxic, and water-soluble. It can also permeate cell membranes. Therefore, it is possible to monitor cultured cells in a continuous manner [36]. Cells can change the dye from an oxidized to a reduced state through many enzymes, such as mitochondrial enzymes. The inability of the cells to reduce the dye may signify an impairment of cellular metabolism [36].
This in vitro study has several limitations. The short incubation period limited our assessment of hGF behavior to a single point in time. Cell growth, proliferation, attachment, and adhesion are better understood if we examine them at different time points to reveal their behavior toward different membrane surfaces and to explore the potential effect of vitamin C on these processes. Secondly, the SEM images did not show the attachment of hGF to the membranes. This could be avoided by using Osmium tetroxide in the fixation protocol of SEM. However, we could not follow this protocol for logistical and safety reasons in our laboratory. Another limitation is the use of the Resazurin reduction assay (AlamarBlue®) to assess cell viability and proliferation. The use of another cell viability assay that is more sensitive, less prone to artifacts, and faster, like the ATP assay, would yield more precise results for this study. Lastly, this in vitro study examined one type of cell line, fibroblasts, and evaluated only their migration and proliferation in association with two kinds of membranes. Evaluating other cell types involved in periodontal regeneration and other aspects of their behavior during wound healing like differentiation and interaction with other cells will add better insight to this research.
6. Conclusions
Periodontal regenerative procedures should be compatible with the growth and bioactivity of gingival fibroblasts. Various materials of collagen membranes are available in the periodontal clinic. The results of our study showed the ability of two types of collagen membranes (native (CopiOs Pericardium) and crosslinked (BioMend) membranes), to support gingival fibroblasts’ function. Additionally, the supplementation of vitamin C to collagen membranes in vitro seems to combat the adverse effects of smoking products on gingival fibroblasts.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Ethical Committee of King Saud University (Project No. E-18-3071) and College of Dentistry Research Center (CDRC No. PR0077).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting the study’s findings are available upon request from the author.
Acknowledgments
The author thanks Ruaa Alyami for her valuable assistance and support in this research project.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Page, R.C.; Offenbacher, S.; Schroeder, H.E.; Seymour, G.J.; Kornman, K.S. Advances in the Pathogenesis of Periodontitis: Summary of Developments, Clinical Implications and Future Directions. Periodontology 2000 1997, 14, 216–248. [Google Scholar] [CrossRef] [PubMed]
- Bartold, P.M.; Gronthos, S.; Ivanovski, S.; Fisher, A.; Hutmacher, D.W. Tissue Engineered Periodontal Products. J. Periodontal Res. 2016, 51, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Karring, T.; Nyman, S.; Gottlow, J.; Laurell, L. Development of the Biological Concept of Guided Tissue Regeneration—Animal and Human Studies. Periodontology 2000 1993, 1, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Sbricoli, L.; Guazzo, R.; Annunziata, M.; Gobbato, L.; Bressan, E.; Nastri, L. Selection of Collagen Membranes for Bone Regeneration: A Literature Review. Materials 2020, 13, 786. [Google Scholar] [CrossRef] [PubMed]
- Hujoel, P.P.; del Aguila, M.A.; DeRouen, T.A.; Bergström, J. A Hidden Periodontitis Epidemic during the 20th Century? Community Dent. Oral Epidemiol. 2003, 31, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus Report of Workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. 1), S173–S182. [Google Scholar] [CrossRef]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and Grading of Periodontitis: Framework and Proposal of a New Classification and Case Definition. J. Periodontol. 2018, 89 (Suppl. 1), S159–S172. [Google Scholar] [CrossRef]
- Lallier, T.E.; Moylan, J.T.; Maturin, E. Greater Sensitivity of Oral Fibroblasts to Smoked Versus Smokeless Tobacco. J. Periodontol. 2017, 88, 1356–1365. [Google Scholar] [CrossRef]
- Sehgal, V.; Ruangsawasdi, N.; Kiattavorncharoen, S.; Bencharit, S.; Thanasrisuebwong, P. Occlusive and Proliferative Properties of Different Collagen Membranes—An In Vitro Study. Materials 2023, 16, 1657. [Google Scholar] [CrossRef]
- Stavropoulos, A.; Sculean, A. Current Status of Regenerative Periodontal Treatment. Curr. Oral Health Rep. 2017, 4, 34–43. [Google Scholar] [CrossRef]
- Aprile, P.; Letourneur, D.; Simon-Yarza, T. Membranes for Guided Bone Regeneration: A Road from Bench to Bedside. Adv. Healthc. Mater. 2020, 9, 2000707. [Google Scholar] [CrossRef] [PubMed]
- Rothamel, D.; Schwarz, F.; Sculean, A.; Herten, M.; Scherbaum, W.; Becker, J. Biocompatibility of Various Collagen Membranes in Cultures of Human PDL Fibroblasts and Human Osteoblast-like Cells. Clin. Oral Implants Res. 2004, 15, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Sam, G.; Pillai, B.R.M. Evolution of Barrier Membranes in Periodontal Regeneration—“Are the Third Generation Membranes Really Here?”. J. Clin. Diagn. Res. JCDR 2014, 8, ZE14–ZE17. [Google Scholar] [CrossRef]
- Naidu, K.A. Vitamin C in Human Health and Disease Is Still a Mystery? An Overview. Nutr. J. 2003, 2, 7. [Google Scholar] [CrossRef] [PubMed]
- D’Aniello, C.; Cermola, F.; Patriarca, E.J.; Minchiotti, G. Vitamin C in Stem Cell Biology: Impact on Extracellular Matrix Homeostasis and Epigenetics. Stem Cells Int. 2017, 2017, 8936156. [Google Scholar] [CrossRef] [PubMed]
- San Miguel, S.M.; Opperman, L.A.; Allen, E.P.; Zielinski, J.; Svoboda, K.K.H. Bioactive Antioxidant Mixtures Promote Proliferation and Migration on Human Oral Fibroblasts. Arch. Oral Biol. 2011, 56, 812–822. [Google Scholar] [CrossRef]
- San Miguel, S.M.; Opperman, L.A.; Allen, E.P.; Zielinski, J.; Svoboda, K.K.H. Antioxidants Counteract Nicotine and Promote Migration via RacGTP in Oral Fibroblast Cells. J. Periodontol. 2010, 81, 1675–1690. [Google Scholar] [CrossRef]
- Nishida, M.; Grossi, S.G.; Dunford, R.G.; Ho, A.W.; Trevisan, M.; Genco, R.J. Dietary Vitamin C and the Risk for Periodontal Disease. J. Periodontol. 2000, 71, 1215–1223. [Google Scholar] [CrossRef]
- Takamizawa, S.; Maehata, Y.; Imai, K.; Senoo, H.; Sato, S.; Hata, R.-I. Effects of Ascorbic Acid and Ascorbic Acid 2-Phosphate, a Long-Acting Vitamin C Derivative, on the Proliferation and Differentiation of Human Osteoblast-like Cells. Cell Biol. Int. 2004, 28, 255–265. [Google Scholar] [CrossRef]
- Tatsumi, M.; Yanagita, M.; Yamashita, M.; Hasegawa, S.; Ikegami, K.; Kitamura, M.; Murakami, S. Long-Term Exposure to Cigarette Smoke Influences Characteristics in Human Gingival Fibroblasts. J. Periodontal Res. 2021, 56, 951–963. [Google Scholar] [CrossRef]
- Alyami, R.; Al Jasser, R.; Alshehri, F.A.; Alshibani, N.; Bin Hamdan, S.; Alyami, R.A.; Niazy, A.A. Vitamin C Influences Antioxidative, Anti-Inflammatory and Wound Healing Markers in Smokers’ Gingival Fibroblasts in Vitro. Saudi Dent. J. 2023, 35, 337–344. [Google Scholar] [CrossRef] [PubMed]
- Alyami, R.; Alshehri, F.A.; Al Jasser, R.; Shaheen, S.; Mahmood, A.; Elsafadi, M.A. Vitamin C Stimulates RNA Expression of Human Gingival Fibroblasts Proliferation and Adhesion in Cigarette Smokers: An in Vitro Study. Saudi Dent. J. 2022, 34, 298–305. [Google Scholar] [CrossRef] [PubMed]
- Torshabi, M.; Rezaei Esfahrood, Z.; Jamshidi, M.; Mansuri Torshizi, A.; Sotoudeh, S. Efficacy of Vitamins E and C for Reversing the Cytotoxic Effects of Nicotine and Cotinine. Eur. J. Oral Sci. 2017, 125, 426–437. [Google Scholar] [CrossRef] [PubMed]
- Akbari, A.; Jelodar, G.; Nazifi, S.; Sajedianfard, J. An Overview of the Characteristics and Function of Vitamin C in Various Tissues: Relying on Its Antioxidant Function. Zahedan J. Res. Med. Sci. 2016, 18, e4037. [Google Scholar] [CrossRef]
- Kaldahl, W.B.; Johnson, G.K.; Patil, K.D.; Kalkwarf, K.L. Levels of Cigarette Consumption and Response to Periodontal Therapy. J. Periodontol. 1996, 67, 675–681. [Google Scholar] [CrossRef]
- Hakeem, L.; Al-Kindi, M.; AlMuraikhi, N.; BinHamdan, S.; Al-Zahrani, A. Evaluation of the Regenerative Potential of Decellularized Skeletal Muscle Seeded with Mesenchymal Stromal Cells in Critical-Sized Bone Defect of Rat Models. Saudi Dent. J. 2021, 33, 248–255. [Google Scholar] [CrossRef]
- McGuire, M.K.; Scheyer, E.T.; Nevins, M.L.; Neiva, R.; Cochran, D.L.; Mellonig, J.T.; Giannobile, W.V.; Bates, D. Living Cellular Construct for Increasing the Width of Keratinized Gingiva: Results from a Randomized, within-Patient, Controlled Trial. J. Periodontol. 2011, 82, 1414–1423. [Google Scholar] [CrossRef]
- Minabe, M.; Kodama, T.; Kogou, T.; Tamura, T.; Hori, T.; Watanabe, Y.; Miyata, T. Different Cross-Linked Types of Collagen Implanted in Rat Palatal Gingiva. J. Periodontol. 1989, 60, 35–43. [Google Scholar] [CrossRef]
- Capella-Monsonís, H.; Zeugolis, D.I. Decellularized Xenografts in Regenerative Medicine: From Processing to Clinical Application. Xenotransplantation 2021, 28, e12683. [Google Scholar] [CrossRef]
- Wong, L.S.; Martins-Green, M. Firsthand Cigarette Smoke Alters Fibroblast Migration and Survival: Implications for Impaired Healing. Wound Repair Regen. Off. Publ. Wound Heal. Soc. Eur. Tissue Repair Soc. 2004, 12, 471–484. [Google Scholar] [CrossRef]
- Sawhney, A.; Ralli, M.; Dhar, S.; Gupta, B.; Ghodke, S.S.; Purao, S. Role of Smoking and Its Impact on Periodontium. J. Int. Clin. Dent. Res. Organ. 2021, 13, 3–9. [Google Scholar] [CrossRef]
- Tipton, D.A.; Dabbous, M.K.H. Effects of Nicotine on Proliferation and Extracellular Matrix Production of Human Gingival Fibroblasts In Vitro. J. Periodontol. 1995, 66, 1056–1064. [Google Scholar] [CrossRef]
- Møller, P.; Viscovich, M.; Lykkesfeldt, J.; Loft, S.; Jensen, A.; Poulsen, H.E. Vitamin C Supplementation Decreases Oxidative DNA Damage in Mononuclear Blood Cells of Smokers. Eur. J. Nutr. 2004, 43, 267–274. [Google Scholar] [CrossRef]
- Falsafi, P.; Nasrabadi, E.T.; Nasrabadi, H.T.; Khiyavi, R.K.; Eslami, H. Comparison of Total Antioxidant Capacity and Vitamin C in Smokers and Non-Smokers. Biomed. Pharmacol. J. 2016, 9, 299–304. [Google Scholar] [CrossRef]
- Talebi Ardakani, M.R.; Hajizadeh, F.; Yadegari, Z. Comparison of Attachment and Proliferation of Human Gingival Fibroblasts on Different Collagen Membranes. Ann. Maxillofac. Surg. 2018, 8, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Rampersad, S.N. Multiple Applications of Alamar Blue as an Indicator of Metabolic Function and Cellular Health in Cell Viability Bioassays. Sensors 2012, 12, 12347–12360. [Google Scholar] [CrossRef]
Figure 1.
Illustration of gingival fibroblast cells and collagen –membrane migration assay.

Figure 2.
Absorption rate of experimental smoking and non-smoking groups before and after treatment with vitamin C as measured by fluorescent rate (y-axis). Mann–Whitney U test was used for independent group comparisons. Bio = BioMend crosslinked membrane; Peri = CopiOs Pericardium native membrane; N = without vitamin C treatment; C = with vitamin C treatment.; * p-value < 0.05; ** p-value < 0.005.
Figure 2.
Absorption rate of experimental smoking and non-smoking groups before and after treatment with vitamin C as measured by fluorescent rate (y-axis). Mann–Whitney U test was used for independent group comparisons. Bio = BioMend crosslinked membrane; Peri = CopiOs Pericardium native membrane; N = without vitamin C treatment; C = with vitamin C treatment.; * p-value < 0.05; ** p-value < 0.005.

Figure 3.
Scanning electron microscopy (SEM) of non-smoker hGFs on different membranes before treatment with vitamin C. (A) Representative SEM image of BioMend membrane cultured with untreated non-smoker hGFs (magnification ×160 at 100 µm scale). (B) Representative SEM image of CopiOs Pericardium membrane cultured with untreated non-smoker hGFs (magnification ×22 at 1 mm scale).
Figure 3.
Scanning electron microscopy (SEM) of non-smoker hGFs on different membranes before treatment with vitamin C. (A) Representative SEM image of BioMend membrane cultured with untreated non-smoker hGFs (magnification ×160 at 100 µm scale). (B) Representative SEM image of CopiOs Pericardium membrane cultured with untreated non-smoker hGFs (magnification ×22 at 1 mm scale).

Figure 4.
Scanning electron microscopy images showing the structure of two membranes cultured with non-smoker hGFs treated vs. not treated with vitamin C. (A) Representative SEM image of a BioMend membrane cultured with non-smoker hGFs not treated with vitamin C (Bio N-N; magnification ×500 at 50 µm). (B) Representative SEM image of a BioMend membrane cultured with non-smoker hGFs treated with vitamin C (Bio N-C; magnification ×1000 at 10 µm scale). (C) Scanning electron microscopy image of a CopiOs Pericardium membrane cultured with non-smoker hGFs not treated with vitamin C (Peri N-N; magnification ×180 at 100 µm scale). (D) Scanning electron microscopy image of a CopiOs Pericardium membrane cultured with non-smoker hGFs treated with vitamin C (Peri N-C; magnification ×1000 at 10 µm scale).
Figure 4.
Scanning electron microscopy images showing the structure of two membranes cultured with non-smoker hGFs treated vs. not treated with vitamin C. (A) Representative SEM image of a BioMend membrane cultured with non-smoker hGFs not treated with vitamin C (Bio N-N; magnification ×500 at 50 µm). (B) Representative SEM image of a BioMend membrane cultured with non-smoker hGFs treated with vitamin C (Bio N-C; magnification ×1000 at 10 µm scale). (C) Scanning electron microscopy image of a CopiOs Pericardium membrane cultured with non-smoker hGFs not treated with vitamin C (Peri N-N; magnification ×180 at 100 µm scale). (D) Scanning electron microscopy image of a CopiOs Pericardium membrane cultured with non-smoker hGFs treated with vitamin C (Peri N-C; magnification ×1000 at 10 µm scale).

Figure 5.
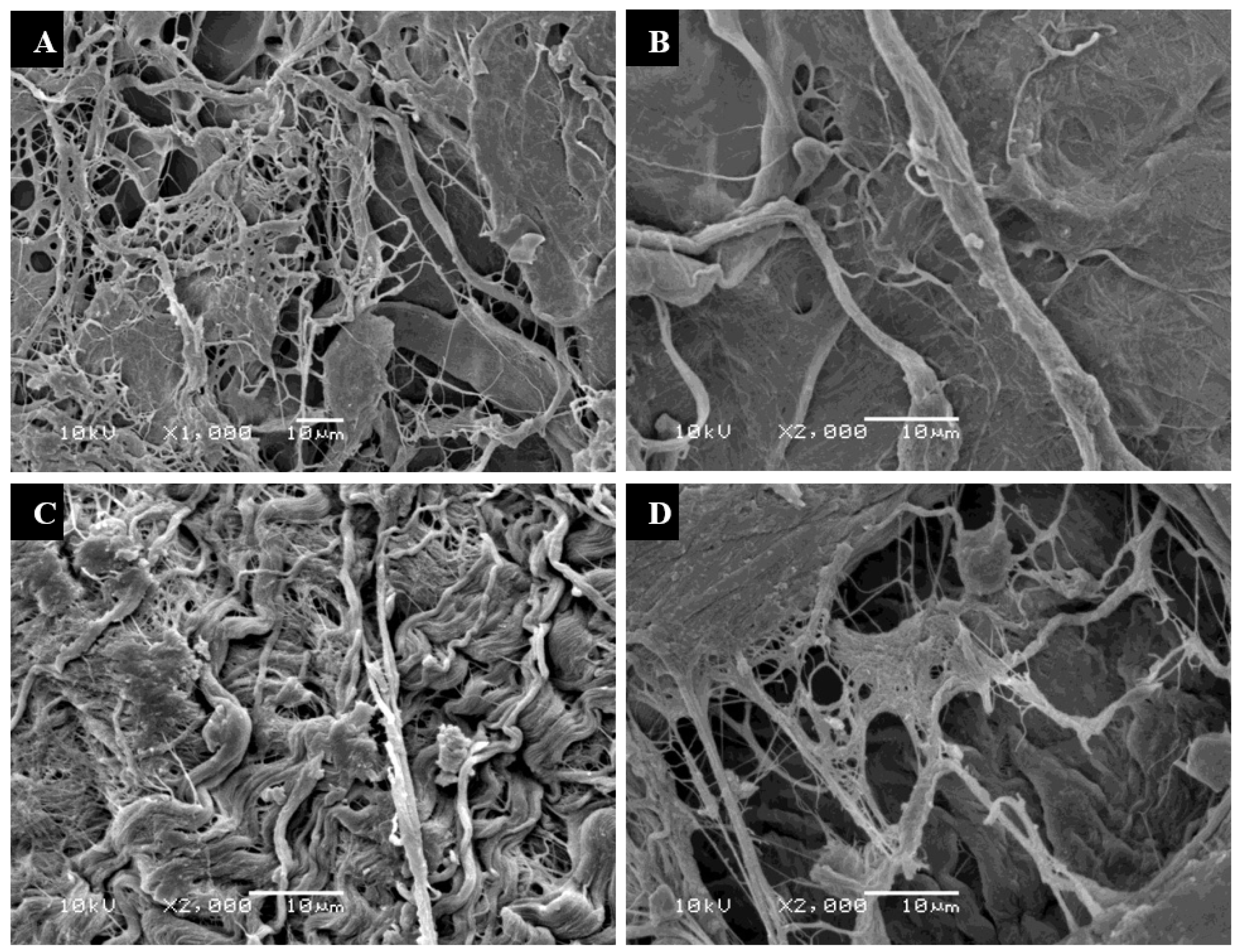
Scanning electron microscopy images showing the structure of two membranes cultured with smoker hGFs treated vs. not treated with vitamin C. (A) Representative SEM image of a BioMend membrane cultured with smoker hGFs not treated with vitamin C (Bio-S-N; magnification ×1000 at 10 µm scale). (B) Representative SEM image of a BioMend membrane cultured with smoker hGFs treated with vitamin C (Bio-S-C; magnification ×2000 at 10 µm scale). (C) Representative SEM image of a CopiOs Pericardium membrane cultured with smoker hGFs not treated with vitamin C (Peri-S-N; magnification ×2000 at 10 µm scale). (D) Representative SEM image of a CopiOs Pericardium membrane cultured with smoker hGFs treated with vitamin C (Peri-S-C; magnification ×2000 at 10 µm scale).
Figure 5.
Scanning electron microscopy images showing the structure of two membranes cultured with smoker hGFs treated vs. not treated with vitamin C. (A) Representative SEM image of a BioMend membrane cultured with smoker hGFs not treated with vitamin C (Bio-S-N; magnification ×1000 at 10 µm scale). (B) Representative SEM image of a BioMend membrane cultured with smoker hGFs treated with vitamin C (Bio-S-C; magnification ×2000 at 10 µm scale). (C) Representative SEM image of a CopiOs Pericardium membrane cultured with smoker hGFs not treated with vitamin C (Peri-S-N; magnification ×2000 at 10 µm scale). (D) Representative SEM image of a CopiOs Pericardium membrane cultured with smoker hGFs treated with vitamin C (Peri-S-C; magnification ×2000 at 10 µm scale).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Experimental collagen membrane groups.
| Non-Smoker (N) Groups | Smoker (S) Groups |
|---|---|
| BioMend membrane without vitamin C (Bio-N-N) | BioMend membrane without vitamin C (Bio-S-N) |
| BioMend membrane with vitamin C (Bio-N-C) | BioMend membrane with vitamin C (Bio-S-C) |
| Pericardium membrane without vitamin C (Peri-N-N) | Pericardium membrane without vitamin C (Peri-S-N) |
| Pericardium membrane with vitamin C (Peri-N-C) | Pericardium membrane with vitamin C (Peri-S-C) |
Table 2.
Comparison of native (BioMend) and crosslinked (CopiOs) membranes before and after treatment with vitamin C. * Using Wilcoxon signed-rank test, statistical significance (p-value) set at 0.05; Bio = BioMend crosslinked membrane; Peri = CopiOs Pericardium membrane; N = without vitamin C treatment; C = with vitamin C treatment.
Table 2.
Comparison of native (BioMend) and crosslinked (CopiOs) membranes before and after treatment with vitamin C. * Using Wilcoxon signed-rank test, statistical significance (p-value) set at 0.05; Bio = BioMend crosslinked membrane; Peri = CopiOs Pericardium membrane; N = without vitamin C treatment; C = with vitamin C treatment.
| Group | n | Mean ± (SD) | p-Value * | |
|---|---|---|---|---|
| Non-smokers | Assay control | 6 | 4173.5 ± (532.8) | - |
| Bio-N-N | 6 | 4422.5 ± (1394.1) | 0.917 | |
| Bio-N-C | 6 | 4719.8 ± (515.6) | ||
| Peri-N-N | 6 | 5659.0 ± (600.4) | 0.028 | |
| Peri-N-C | 6 | 6329.8 ± (593.0) | ||
| Smokers | Assay control | 6 | 4399.5 ± (896.4) | - |
| Bio-S-N | 6 | 6055.2 ± (339.6) | 0.028 | |
| Bio-S-C | 6 | 6411.0 ± (401.1) | ||
| Peri-S-N | 6 | 8012.8 ± (112.9) | 0.028 | |
| Peri-S-C | 6 | 7349.0 ± (360.7) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Alshehri, F.A. Can Vitamin C Improve Proliferation and Viability of Smokers’ Gingival Fibroblasts on Collagen Membranes? An In Vitro Study. Appl. Sci. 2023, 13, 10828. https://doi.org/10.3390/app131910828
AMA Style
Alshehri FA. Can Vitamin C Improve Proliferation and Viability of Smokers’ Gingival Fibroblasts on Collagen Membranes? An In Vitro Study. Applied Sciences. 2023; 13(19):10828. https://doi.org/10.3390/app131910828
Chicago/Turabian StyleAlshehri, Fahad Ali. 2023. "Can Vitamin C Improve Proliferation and Viability of Smokers’ Gingival Fibroblasts on Collagen Membranes? An In Vitro Study" Applied Sciences 13, no. 19: 10828. https://doi.org/10.3390/app131910828
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.