
Light and Affordable Vision System for Mouth Opening–Closing Movement Deviation Assessment in Women with Mild Temporomandibular Joint Disorder
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
- -
- Age below 20 or above 55 years;
- -
- Males;
- -
- Rheumatic, neoplastic, and central nervous system diseases;
- -
- Lack of more than 5 teeth (excluding third molars);
- -
- Neuralgia of cranial nerves;
- -
- Previous injuries to the skull, jaw, or cervical spine;
- -
- Previous surgical treatment of the skull or jaw;
- -
- Joint disc blockage without reduction;
- -
- Angle’s Class III malocclusion;
- -
- Open bite.
2.1. Clinical Examination
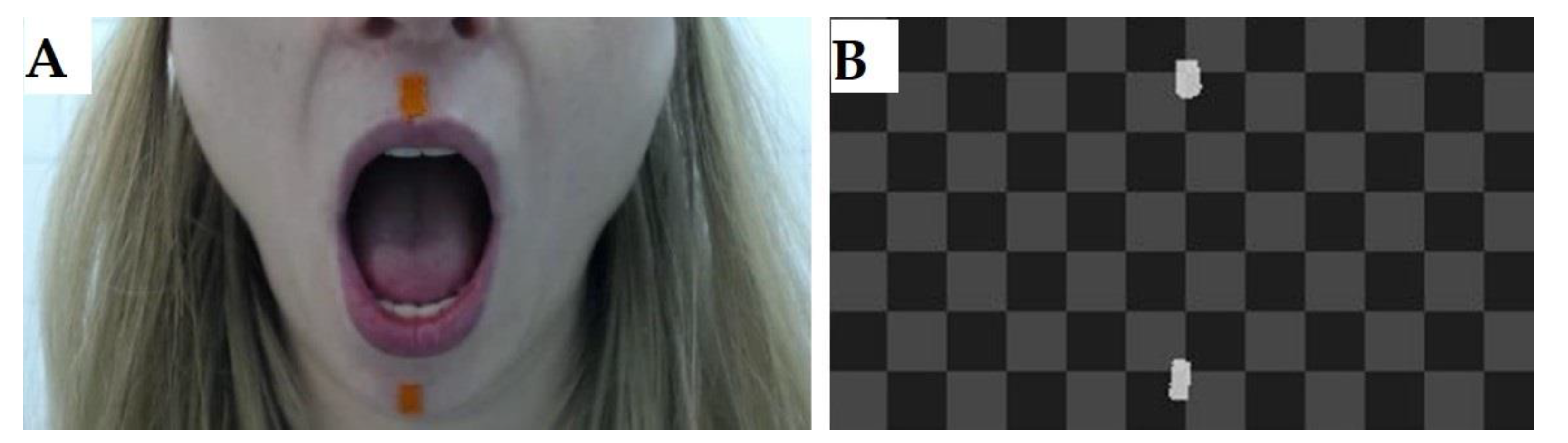
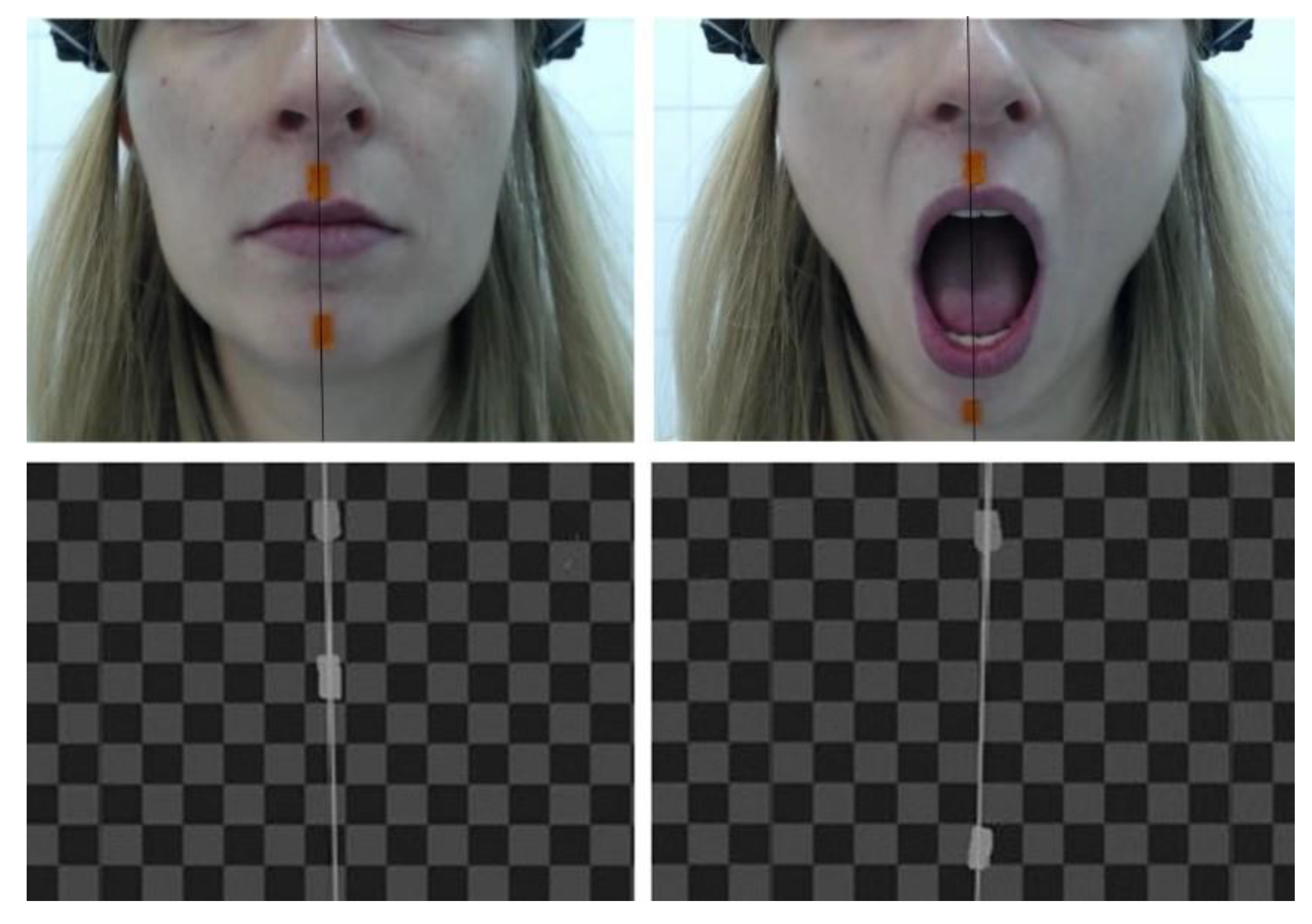
2.2. Camera Recording
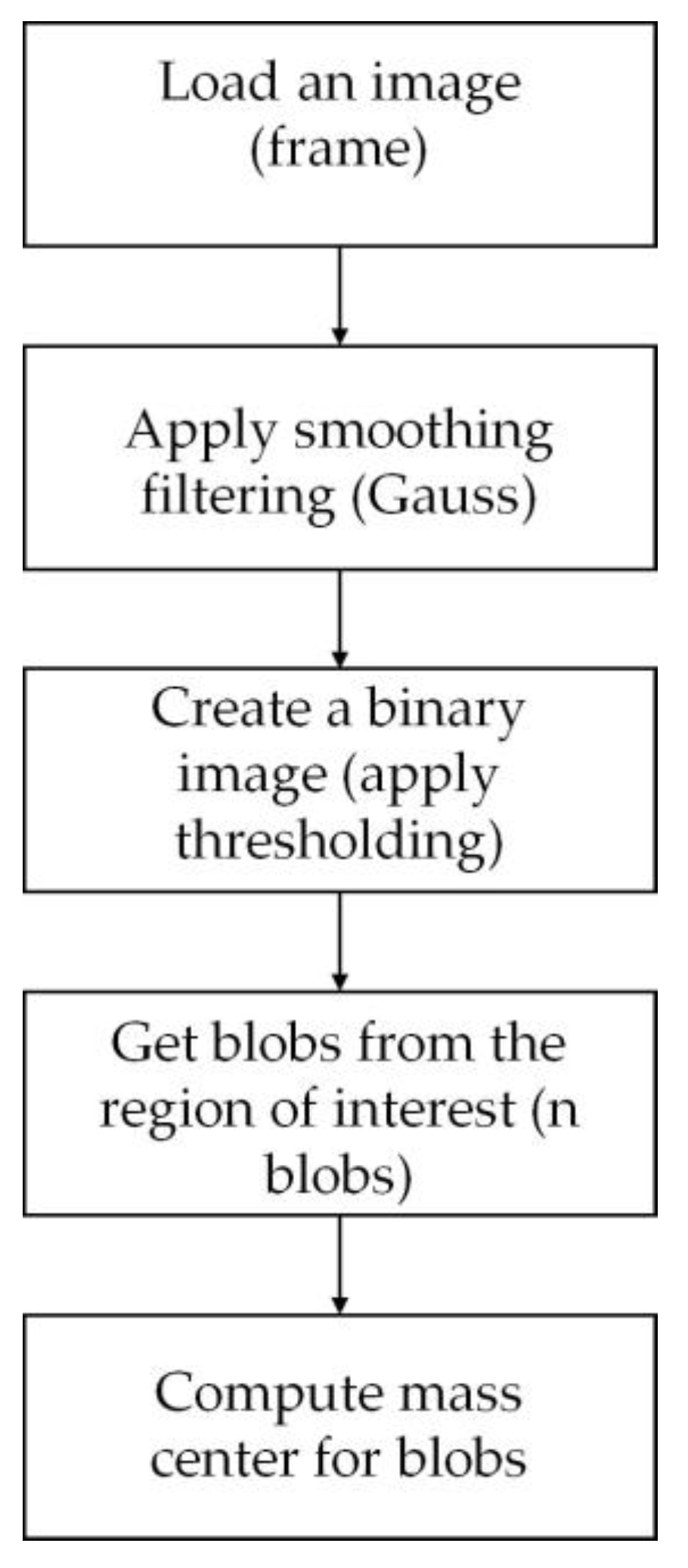
Stages of Image Analysis: Software
3. Results
3.1. Statistics
3.2. Clicking in Temporomandibular Joints
3.3. Oral Parafunctions
3.4. Mandibular Deviation Parameters
4. Discussion
Limitation
5. Conclusions
- In women with mild TMD, a lack of coordination between the right and left joints can be observed;
- In women with mild TMD, a displaced disc is reduced in the early stage of mouth opening, so it does not affect the range of maximum lateral deviations;
- The proposed vision system method for assessing the quality of mandibular opening and closing movements appears to be an interesting tool for evaluating the coordination between the left and right temporomandibular joints;
- With easy and fast attachment, the proposed method lends itself to population-based diagnostic studies and may be successfully used even by individuals with no advanced knowledge of the masticatory apparatus;
- The proposed device may have applications in physiotherapy; however, it is not sufficient for use in dental or surgical treatments.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Valesan, L.F.; Da-Cas, C.D.; Réus, J.C.; Denardin, A.C.S.; Garanhani, R.R.; Bonotto, D.; Januzzi, E.; de Souza, B.D.M. Prevalence of temporomandibular joint disorders: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Seo, H.; Jung, B.; Yeo, J.; Kim, K.-W.; Cho, J.-H.; Lee, Y.J.; Ha, I.-H. Healthcare utilisation and costs for temporomandibular disorders: A descriptive, cross-sectional study. BMJ Open 2020, 10, e036768. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Steinkeler, A. Epidemiology, Diagnosis, and Treatment of Temporomandibular Disorders. Dent. Clin. N. Am. 2013, 57, 465–479. [Google Scholar] [CrossRef]
- Alona, E.-P.; Ilana, E. One year into the COVID-19 pandemic—Temporomandibular disorders and bruxism: What we have learned and what we can do to improve our manner of treatment. Dent. Med. Probl. 2021, 58, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Saccomanno, S.; Saran, S.; De Luca, M.; Mastrapasqua, R.F.; Raffaelli, L.; Levrini, L. The Influence of SARS-CoV-2 Pandemic on TMJ Disorders, OSAS and BMI. Int. J. Environ. Res. Public Health 2022, 19, 7154. [Google Scholar] [CrossRef]
- Haddad, C.; Sayegh, S.M.; El Zoghbi, A.; Lawand, G.; Nasr, L. The Prevalence and Predicting Factors of Temporomandibular Disorders in COVID-19 Infection: A Cross-Sectional Study. Cureus 2022, 14, e28167. [Google Scholar] [CrossRef]
- Bicaj, T.; Shala, K.; Krasniqi, T.P.; Ahmedi, E.; Dula, L.; Lila-Krasniqi, Z. Frequency of Symptoms of Temporomandibular Disorders among Prishtina Dental Students. Open Access Maced. J. Med. Sci. 2017, 5, 781–784. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, M.S.; Saag, M.; Jagomägi, T.; Nguyen, Q.H.; Voog-Oras, Ü. The impact of occlusal support on temporomandibular disorders: A literature review. Proc. Singap. Healthc. 2022, 31, 20101058211023780. [Google Scholar] [CrossRef]
- Berni, K.C.D.S.; Filho, A.V.D.; Pires, P.; Rodrigues-Bigaton, D. Accuracy of the surface electromyography RMS processing for the diagnosis of myogenous temporomandibular disorder. J. Electromyogr. Kinesiol. 2015, 25, 596–602. [Google Scholar] [CrossRef]
- Boening, K.; Wieckiewicz, M.; Paradowska-Stolarz, A.; Wiland, P.; Shiau, Y.-Y. Temporomandibular Disorders and Oral Parafunctions: Mechanism, Diagnostics, and Therapy. BioMed Res. Int. 2015, 2015, 354759. [Google Scholar] [CrossRef]
- Wright, E.F.; North, S.L. Management and Treatment of Temporomandibular Disorders: A Clinical Perspective. J. Man. Manip. Ther. 2009, 17, 247–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saran, S.; Saccomanno, S.; Petricca, M.T.; Carganico, A.; Bocchieri, S.; Mastrapasqua, R.F.; Caramaschi, E.; Levrini, L. Physiotherapists and Osteopaths’ Attitudes: Training in Management of Temporomandibular Disorders. Dent. J. 2022, 10, 210. [Google Scholar] [CrossRef] [PubMed]
- Crăciun, M.D.; Geman, O.; Leuciuc, F.V.; Holubiac, I.; Gheorghiţă, D.; Filip, F. Effectiveness of Physiotherapy in the Treatment of Temporomandibular Joint Dysfunction and the Relationship with Cervical Spine. Biomedicines 2022, 10, 2962. [Google Scholar] [CrossRef]
- SedkyAdly, M.; Youssif, A.A.; Eldin, A.S. Recording and Measuring of Jaw Movements using a Computer Vision System. Int. J. Comput. Appl. 2013, 81, 38–43. [Google Scholar] [CrossRef]
- Furtado, D.A.; Pereira, A.A.; Andrade, A.d.O.; BellomoJunior, D.P.; da Silva, M.R. A specialized motion capture system for real-time analysis of mandibular movements using infrared cameras. Biomed. Eng. Online 2013, 12, 17. [Google Scholar] [CrossRef] [Green Version]
- Rahman, F.; Femiano, F.; Louis, P.J.; Kau, C.H. An Evaluation of Jaw Tracking Movements in Patients with Total Joint Replacements versus a Control Group. Medicina 2022, 58, 738. [Google Scholar] [CrossRef]
- Duxbury, A.J.; McEwan, C.G.; Rothwell, P.S. A digital optoelectronic method for recording mandibular movement in association with oral electromyograms and temporomandibular joint noises. Med. Biol. Eng. Comput. 1974, 12, 707–711. [Google Scholar] [CrossRef]
- Fang, J.-J.; Kuo, T.-H. Modelling of mandibular movement. Comput. Biol. Med. 2008, 38, 1152–1162. [Google Scholar] [CrossRef] [PubMed]
- Von Piekartz, H.; Lüdtke, K. Effect of Treatment of Temporomandibular Disorders (TMD) in Patients with Cervicogenic Headache: A Single-Blind, Randomized Controlled Study. J. Craniomandib. Sleep Pract. 2011, 29, 43–56. [Google Scholar] [CrossRef]
- Małgorzata, P.; Małgorzata, K.-M.; Karolina, C.; Gala, A. Diagnostic of Temporomandibular Disorders and Other Facial Pain Conditions—Narrative Review and Personal Experience. Medicina 2020, 56, 472. [Google Scholar] [CrossRef]
- Andrade, R.M.; Guimarães, L.R.; Ribeiro, A.P.; Marques, A.P.; Crivello, O.; de Carvalho, B.K.G.; João, S.M.A. Reliability in Mandibular Movement Evaluation Using Photogrammetry in Patients with Temporomandibular Disorders. J. Manip. Physiol. Ther. 2019, 42, 267–275. [Google Scholar] [CrossRef]
- Helkimo, M. Studies on Function and Dysfunction of the Masticatory System. II. Index for Anamnestic and Clinical Dysfunction and Occlusal State. Sven Tandlak Tidskr. 1974, 67, 101–121. [Google Scholar]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef] [PubMed]
- Litko, M.; Szkutnik, J.; Berger, M.; Bakalczuk, M.; Różyło-Kalinowska, I. Range and pattern of mandibular opening in patients with anterior displacement of temporomandibular disc without reduction. J. Pre-Clin. Clin. Res. 2018, 12, 59–62. [Google Scholar] [CrossRef]
- Poluha, R.L.; Canales, G.D.L.T.; Costa, Y.M.; Grossmann, E.; Bonjardim, L.R.; Conti, P.C.R. Temporomandibular joint disc displacement with reduction: A review of mechanisms and clinical presentation. J. Appl. Oral Sci. 2019, 27, e20180433. [Google Scholar] [CrossRef]
- de Bont, L.G.; Stegenga, B. Pathology of temporomandibular joint internal derangement and osteoarthrosis. Int. J. Oral Maxillofac. Surg. 1993, 22, 71–74. [Google Scholar] [CrossRef]
- Al-Ani, Z. Temporomandibular Joint Osteoarthrosis: A Review of Clinical Aspects and Management. Prim. Dent. J. 2021, 10, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Bae, Y.; Park, Y. The Effect of Relaxation Exercises for the Masticator Muscles on Temporomandibular Joint Dysfunction (TMD). J. Phys. Ther. Sci. 2013, 25, 583–586. [Google Scholar] [CrossRef] [Green Version]
- Winocur-Arias, O.; Winocur, E.; Shalev-Antsel, T.; Reiter, S.; Shifra, L.; Emodi-Perlman, A.; Friedman-Rubin, P. Painful Temporomandibular Disorders, Bruxism and Oral Parafunctions before and during the COVID-19 Pandemic Era: A Sex Comparison among Dental Patients. J. Clin. Med. 2022, 11, 589. [Google Scholar] [CrossRef]
- Eraslan, R.; Ozturk, T. Comparison of the Relationship between Temporomandibular Disorder and Oral Habits or Quality of Life in Dentistry Students in Different Years of Education. Chin. J. Dent. Res. 2022, 25, 223–232. [Google Scholar] [CrossRef]
- Fernandes, G.; Franco-Micheloni, A.L.; Siqueira, J.T.T.; Gonçalves, D.; Camparis, C.M. Parafunctional habits are associated cumulatively to painful temporomandibular disorders in adolescents. Braz. Oral Res. 2016, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobbezoo, F.; Koyano, K.; Paesani, D.A.; Manfredini, D. Chapter 145—Sleep Bruxism: Diagnostic Considerations. In Principles and Practice of Sleep Medicine, 6th ed.; Kryger, M., Roth, T., Dement, W.C., Eds.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 1427–1434.e4. ISBN 978-0-323-24288-2. [Google Scholar]
- Baba, K.; Akishige, S.; Yaka, T.; Ai, M. Influence of alteration of occlusal relationship on activity of jaw closing muscles and mandibular movement during submaximal clenching. J. Oral Rehabil. 2000, 27, 793–801. [Google Scholar] [CrossRef] [PubMed]
- Kau, C.H.; He, S.; Liao, L.; Kinderknecht, K.; Ow, A.; Saleh, T.A. The use of a dynamic real-time jaw tracking device and cone beam computed tomography simulation. Ann. Maxillofac. Surg. 2016, 6, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Yuan, F.; Sui, H.; Li, Z.; Yang, H.; Lu, P.; Wang, Y.; Sun, Y. A Method of Three-Dimensional Recording of Mandibular Movement Based on Two-Dimensional Image Feature Extraction. PLoS ONE 2015, 10, e0137507. [Google Scholar] [CrossRef]
- Zhao, T.; Yang, H.; Sui, H.; Salvi, S.S.; Wang, Y.; Sun, Y. Accuracy of a Real-Time, Computerized, Binocular, Three-Dimensional Trajectory-Tracking Device for Recording Functional Mandibular Movements. PLoS ONE 2016, 11, e0163934. [Google Scholar] [CrossRef] [Green Version]
- Mostashiri, N.; Dhupia, J.S.; Verl, A.W.; Xu, W. A Novel Spatial Mandibular Motion-Capture System Based on Planar Fiducial Markers. IEEE Sens. J. 2018, 18, 10096–10104. [Google Scholar] [CrossRef]
- Pinheiro, A.P.; Andrade, A.O.; Pereira, A.A.; Bellomo, D. A computational method for recording and analysis of mandibular movements. J. Appl. Oral Sci. 2008, 16, 321–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Cunha, D.V.; Degan, V.V.; Filho, M.V.; Bellomo, D.P.; Silva, M.R.; Furtado, D.A.; Andrade, A.O.; Milagre, S.T.; Pereira, A.A. Real-time three-dimensional jaw tracking in temporomandibular disorders. J. Oral Rehabil. 2017, 44, 580–588. [Google Scholar] [CrossRef]
- Bapelle, M.; Dubromez, J.; Savoldelli, C.; Tillier, Y.; Ehrmann, E. Modjaw® device: Analysis of mandibular kinematics recorded for a group of asymptomatic subjects. J. Craniomandib. Sleep Pract. 2021, 1–7. [Google Scholar] [CrossRef]
- Jakubowska, S.; Szerszeń, M.P.; Kostrzewa-Janicka, J. Jaw motion tracking systems—Literature review. Prosthodontics 2023, 73, 18–28. [Google Scholar] [CrossRef]
- Linsen, S.S.; Stark, H.; Samai, A. The influence of different registration techniques on condyle displacement and electromyographic activity in stomatognathically healthy subjects: A prospective study. J. Prosthet. Dent. 2012, 107, 47–54. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | No. | Mean ± SD | Median | Min–Max | p-Value |
|---|---|---|---|---|---|
| Experimental | 25 | 40.0 ± 7.4 | 42 | 24–53 | 0.813 |
| Control | 25 | 33.9 ± 7.5 | 33 | 23–46 |
| Opening with Clicking | Answer | Experimental N = 25 | Control N = 25 | p-Value |
|---|---|---|---|---|
| Right side | yes | 6 | 0 | 0.03 |
| no | 19 | 25 | 0.4 | |
| Left side | yes | 9 | 0 | 0.004 |
| no | 16 | 25 | 0.4 |
| Parafunction Type | Answer | Experimental N = 25 | Control N = 25 |
|---|---|---|---|
| teeth clenching | yes | 24 | 0 |
| no | 1 | 25 | |
| teeth grinding | yes | 12 | 0 |
| no | 13 | 25 | |
| Asymmetrical non-occlusal | yes | 25 | 0 |
| no | 0 | 25 |
| Parameter | Group | No. | Mean ± SD | Median | Min–Max | p-Value |
|---|---|---|---|---|---|---|
| MAX | Experimental | 25 | 2.08 ± 0.80 | 2.01 | 0.80–4.01 | 0.113 * |
| Control | 25 | 1.74 ± 0.67 | 1.69 | 0.62–3.17 | ||
| MSE | Experimental | 25 | 52.89 ± 55.77 | 26.84 | 4.49–254.58 | 0.007 ** |
| Control | 25 | 28.16 ± 36.01 | 12.37 | 1.67–148.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goślińska, J.; Wareńczak-Pawlicka, A.; Gośliński, J.; Owczarek, P.; Lisiński, P. Light and Affordable Vision System for Mouth Opening–Closing Movement Deviation Assessment in Women with Mild Temporomandibular Joint Disorder. Appl. Sci. 2023, 13, 8224. https://doi.org/10.3390/app13148224
Goślińska J, Wareńczak-Pawlicka A, Gośliński J, Owczarek P, Lisiński P. Light and Affordable Vision System for Mouth Opening–Closing Movement Deviation Assessment in Women with Mild Temporomandibular Joint Disorder. Applied Sciences. 2023; 13(14):8224. https://doi.org/10.3390/app13148224
Chicago/Turabian StyleGoślińska, Jagoda, Agnieszka Wareńczak-Pawlicka, Jarosław Gośliński, Piotr Owczarek, and Przemysław Lisiński. 2023. "Light and Affordable Vision System for Mouth Opening–Closing Movement Deviation Assessment in Women with Mild Temporomandibular Joint Disorder" Applied Sciences 13, no. 14: 8224. https://doi.org/10.3390/app13148224