
Quantitative Electroencephalographic Analysis in Women with Migraine during the Luteal Phase
 and
and
Abstract
:1. Introduction
2. Material and Methods
2.1. Subjects
Inclusion Criteria for All Participants
2.2. EEG Session
2.3. Recordings
3. Data Analysis
3.1. EEG Spectral Power Analysis
3.2. Statistical Analysis
4. Results
4.1. Topographical Analysis
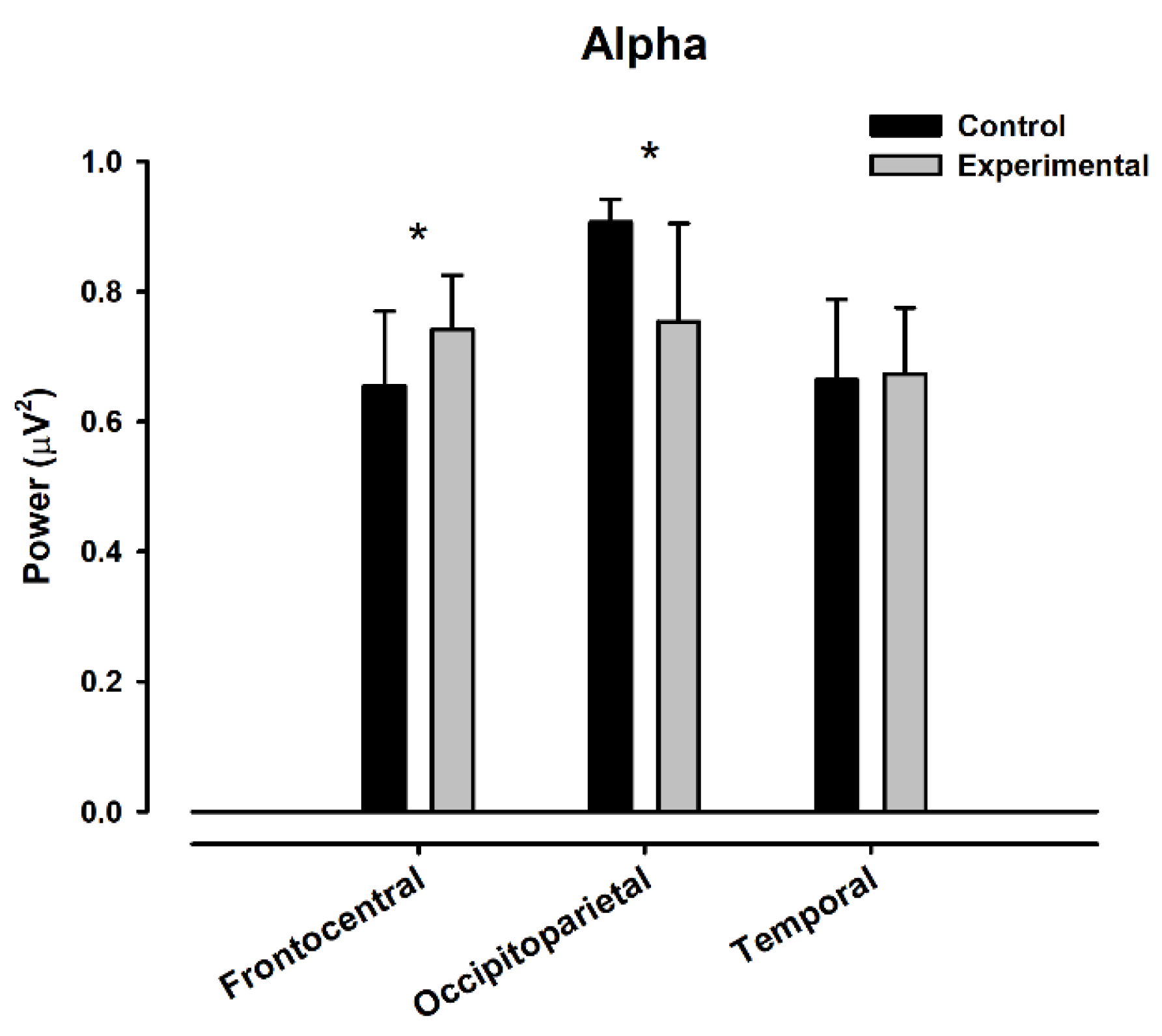
4.2. Alpha
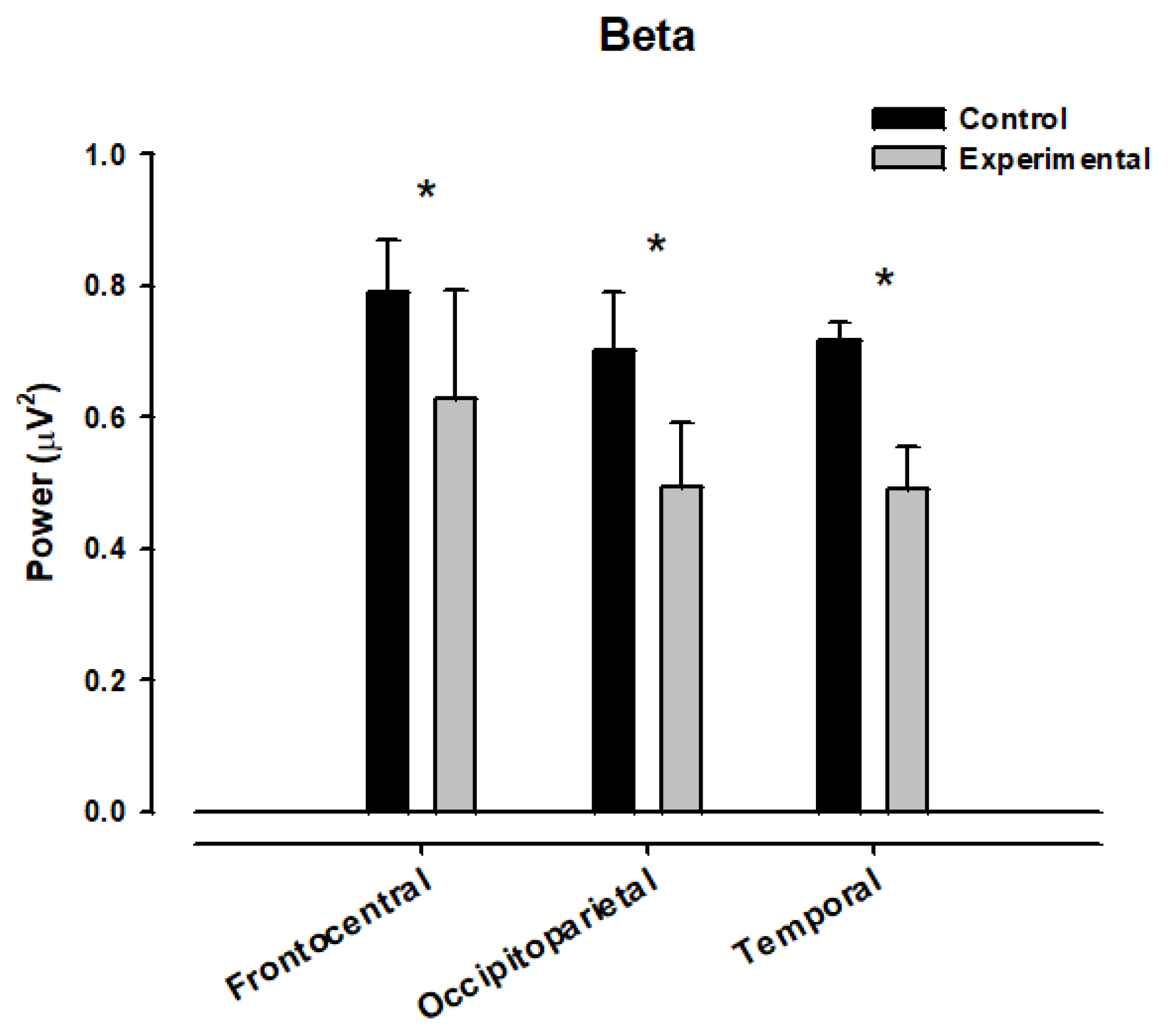
4.3. Beta
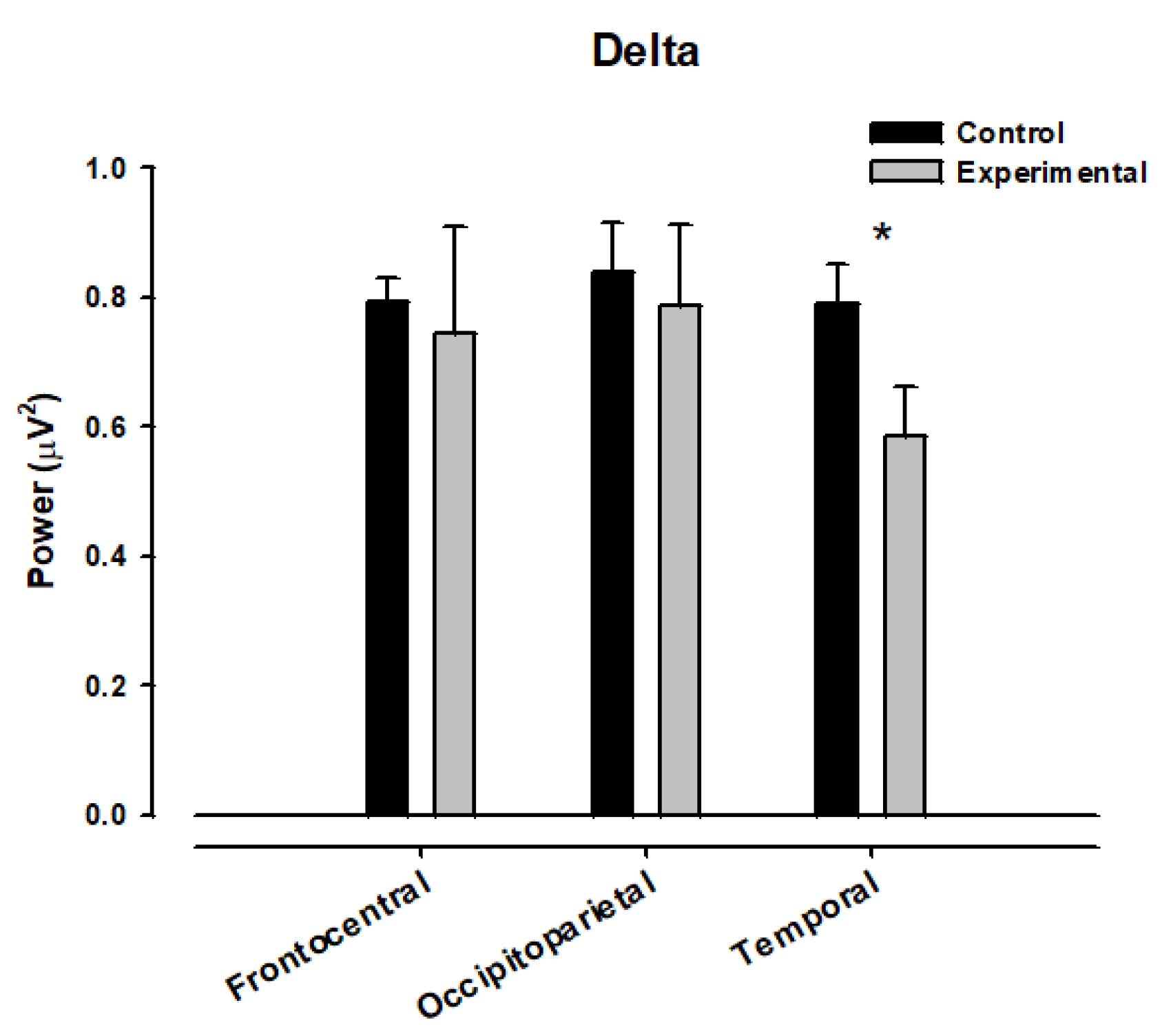
4.4. Delta
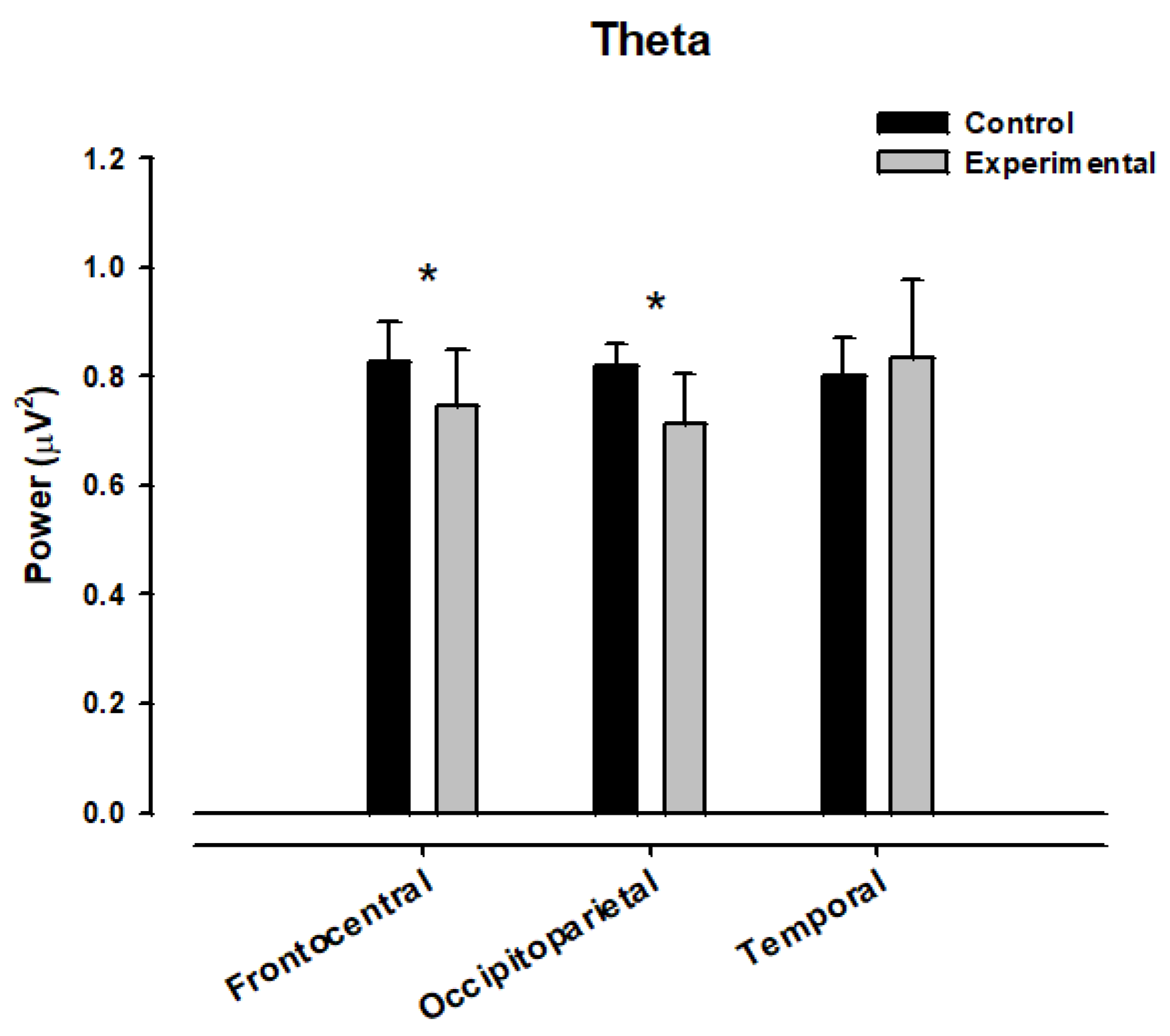
4.5. Theta
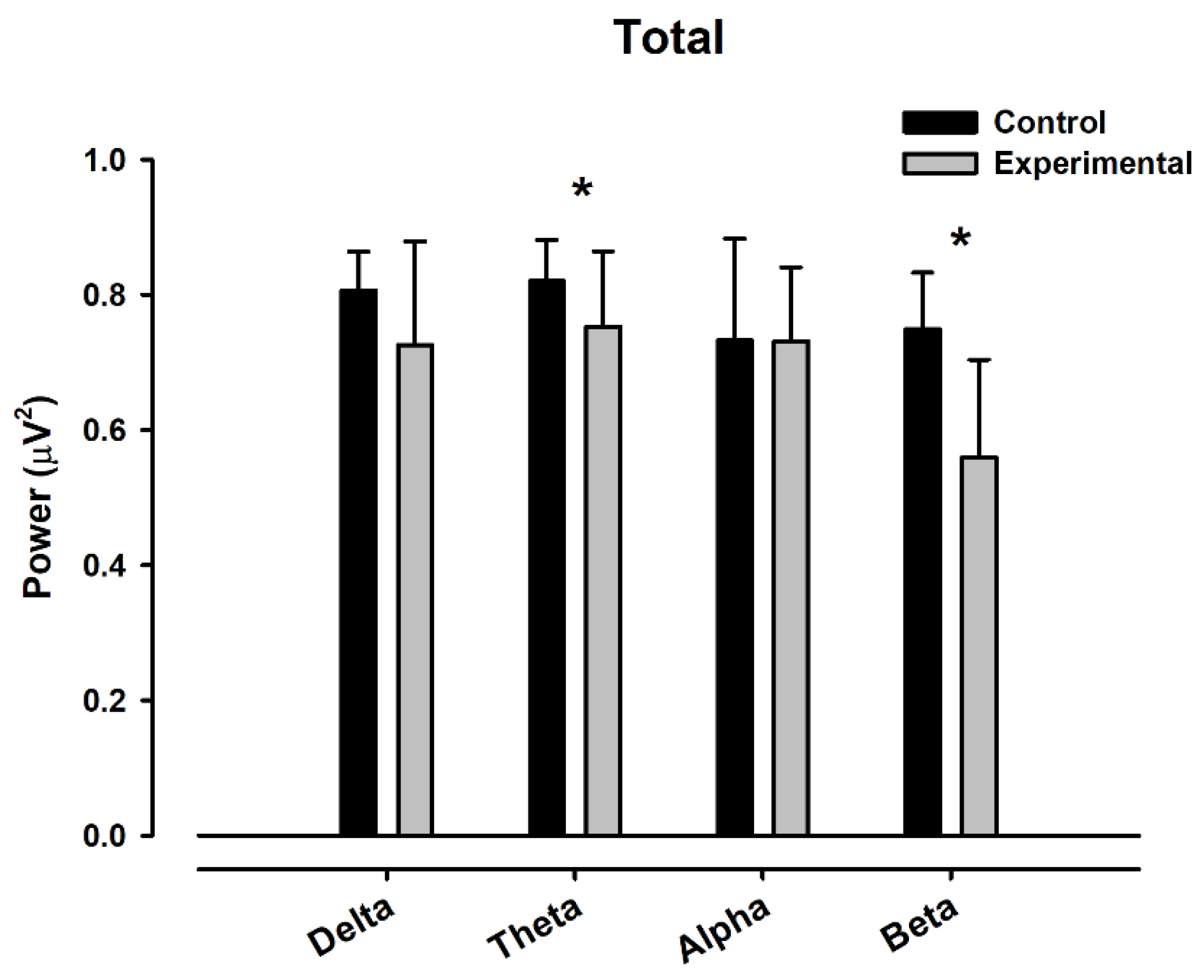
4.6. Grand Average Band Analysis
4.7. Independent Channel Analysis
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, J.H.; Suh, S.I.; Seol, H.Y.; Oh, K.; Seo, W.K.; Yu, S.W.; Park, K.W.; Koh, S.B. Regional grey matter changes in patients with migraine: A voxel-based morphometry study. Cephalalgia 2008, 28, 598–604. [Google Scholar] [CrossRef]
- Salomone, S.; Caraci, F.; Capasso, A. Migraine: An Overview. Open Neurol. J. 2009, 3, 64–71. [Google Scholar] [CrossRef]
- Lipton, R.B.; Bigal, M.E.; Scher, A.I.; Stewart, W.F. The global burden of migraine. J. Headache Pain 2003, 4 (Suppl. S1), s3. [Google Scholar] [CrossRef]
- Mannix, L.K. Menstrual-related pain conditions: Dysmenorrhea and migraine. J. Women’s Health 2008, 17, 879–891. [Google Scholar] [CrossRef] [PubMed]
- Spierings, E.L. Pathogenesis of the migraine attack. Clin. J. Pain 2003, 19, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Bigal, M.E.; Lipton, R.B.; Stewart, W.F. The epidemiology and impact of migraine. Curr. Neurol. Neurosci. Rep. 2004, 4, 98–104. [Google Scholar] [CrossRef]
- Bigal, M.E.; Liberman, J.N.; Lipton, R.B. Obesity and migraine: A population study. Neurology 2006, 66, 545–550. [Google Scholar] [CrossRef] [PubMed]
- Kelman, L. Migraine changes with age: IMPACT on migraine classification. Headache J. Head Face Pain 2006, 46, 1161–1171. [Google Scholar] [CrossRef]
- Di Clemente, L.; Coppola, G.; Magis, D.; Fumal, A.; De Pasqua, V.; Di Piero, V. Interictal habituation deficit of the nociceptive blink reflex: An endophenotypic marker for presymptomatic migraine? Brain 2007, 130, 765–770. [Google Scholar] [CrossRef]
- Capuano, A.; De Corato, A.; Lisi, L.; Tringali, G.; Navarra, P.; Russo, C.D. Proinflammatory-activated trigeminal satellite cells promote neuronal sensitization: Relevance for migraine pathology. Molecular Pain. 2009, 5, 1744–8069. [Google Scholar] [CrossRef] [PubMed]
- Granella, F.; Sances, G.; Allais, G.; Nappi, R.E.; Tirelli, A.; Benedetto, C.; Brundu, B.; Facchinetti, F.; Nappi, G. Characteristics of menstrual and nonmenstrual attacks in women with menstrually related migraine referred to headache centres. Cephalalgia 2004, 24, 707–771. [Google Scholar] [CrossRef]
- MacGregor, E.A.; Frith, A.; Ellis, J.; Aspinall, L.; Hackshaw, A. Incidence of migraine relative to menstrual cycle phases of rising and falling estrogen. Neurology 2006, 67, 2154–2158. [Google Scholar] [CrossRef]
- Pinkerman, B.; Holroyd, K. Menstrual and nonmenstrual migraines differ in women with menstrually-related migraine. Cephalalgia 2010, 30, 1187–1194. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.; Patel, S. Menstrual migraine: An updated review on hormonal causes, prophylaxis and treatment. Expert Opin. Pharmacother. 2014, 15, 2063–2070. [Google Scholar] [CrossRef] [PubMed]
- Pavlović, J.M.; Allshouse, A.A.; Santoro, N.F.; Crawford, S.L.; Thurston, R.C.; Neal-Perry, G.S.; Lipton, R.B.; Derby, C.A. Sex hormones in women with and without migraine: Evidence of migraine-specific hormone profiles. Neurology 2016, 87, 49–56. [Google Scholar] [CrossRef]
- Nappi, R.E.; Tiranini, L.; Sacco, S.; De Matteis, E.; De Icco, R.; Tassorelli, C. Role of Estrogens in Menstrual Migraine. Cells 2022, 11, 1355. [Google Scholar] [CrossRef] [PubMed]
- Vetvik, K.G.; MacGregor, E.A. Menstrual migraine: A distinct disorder needing greater recognition. Lancet Neurol. 2021, 20, 304–315. [Google Scholar] [CrossRef]
- Rosenberg, J.; Alter, M.; Byrne, T. Practice parameter: The electroencephalogram in the evaluation of headache. Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 1995, 45, 1411–1413. [Google Scholar]
- Golla, M.D.; Winter, A.L. Analysis of cerebral response to flickering in patients complaining of an episodic headache. Electroencephalogr. Clin. Neurophysiol. 1959, 11, 539–549. [Google Scholar] [CrossRef]
- Walser, H.; Isler, H. Frontal Intermittent Rhythmic Delta Activity, Impairment of Consciousness and Migraine. Headache J. Head Face Pain 1981, 22, 74–80. [Google Scholar] [CrossRef]
- Schoenen, J.; Jamart, B.; Delwaide, P.J. Cartographie electroencephalographique dans les migraines en periodes critique et intercritique. Electroencephalogr. Neurophysiol. Clinic. 1987, 17, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Nyrke, T.; Kangasniemi, P.; Lang, H. Alpha Rhythm in Classical Migraine (Migraine with Aura): Abnormalities in the Headache-Free Interval. Cephalalgia 1990, 10, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Bjork, M.H.; Stovner, L.J.; Nilsen, B.M.; Stjern, M.; Hagen, K.; Sand, T. The occipital alpha rhythm related to the “migraine cycle” and headache burden: A blinded, controlled longitudinal study. Clin. Neurophysiol. 2009, 120, 464–471. [Google Scholar] [CrossRef]
- O’Hare, L.; Menchinelli, F.; Durrant, S.J. Resting-state alpha-band oscillations in migraine. Perception 2018, 47, 379–396. [Google Scholar] [CrossRef]
- Silberstein, S.D. The role of sex hormones in headache. Neurology 1992, 42, 37–42. [Google Scholar]
- Becker, D.; Creutzfeldt, O.; Schwibbe, M.; Wuttke, W. Changes in physiological, eeg and psychological parameters in women during the spontaneous menstrual cycle and following oral contraceptives. Psychoneuroendocrinology 1982, 7, 75–90. [Google Scholar] [CrossRef]
- Solis-Ortiz, S.; Ramos, J.; Arce, C.; Guevara, M.A.; Corsi-Cabrera, M. EEG oscillations during menstrual cycle. Int. J. Neurosci. 1994, 76, 279–292. [Google Scholar] [CrossRef]
- Baehr, E.; Rosenfeld, P.; Miller, L.; Baehr, R. Premenstrual dysphoric disorder and changes in frontal alpha asymmetry. Int. J. Psychophysiol. 2004, 52, 159–167. [Google Scholar] [CrossRef]
- Haraguchi, R.; Hoshi, H.; Ichikawa, S.; Hanyu, M.; Nakamura, K.; Fukasawa, K.; Poza, J.; Rodríguez-González, V.; Gómez, C.; Shigihara, Y. The Menstrual Cycle Alters Resting-State Cortical Activity: A Magnetoencephalography Study. Front. Hum. Neurosci. 2021, 15, 652789. [Google Scholar] [CrossRef]
- Pletzer, B.; Harris, T.A.; Scheuringer, A.; Hidalgo-Lopez, E. The cycling brain: Menstrual cycle-related fluctuations in hippocampal and frontostriatal activation and connectivity during cognitive tasks. Neuropsychopharmacology 2019, 44, 1867–1875. [Google Scholar] [CrossRef]
- Hidalgo-Lopez, E.; Pletzer, B. Fronto-striatal changes along the menstrual cycle during working memory: Effect of sex hormones on activation and connectivity patterns. Psychoneuroendocrinology 2021, 125, 105108. [Google Scholar] [CrossRef]
- Geschwind, N.; Behan, P. Left-handedness: Association with immune disease, migraine, and developmental learning disorder. Proc. Natl. Acad. Sci. USA 1982, 79, 5097–5100. [Google Scholar] [CrossRef]
- General Assembly of the World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Coll. Dent. 2014, 81, 14–18. [Google Scholar]
- Olesen, J. International classification of headache disorders. Lancet Neurol. 2018, 14, 396–397. [Google Scholar] [CrossRef]
- MacGregor, E.A. Oestrogen and attacks of migraine with and without aura. Lancet Neurol. 2004, 3, 354–361. [Google Scholar] [CrossRef]
- Allais, G.; Gabellari, I.C.; Burzio, C.; Rolando, S.; De Lorenzo, C.; Mana, O.; Benedetto, C. Premenstrual syndrome and migraine. Neurol. Sci. 2012, 33, 111–115. [Google Scholar] [CrossRef]
- Jonkman, E.J.; Lelieveld, M.H.J. EEG computer analysis in patients with migraine. Electroencephalogr. Clin. Neurophysiol. 1981, 52, 652–655. [Google Scholar] [CrossRef]
- Polich, J.; Ehlers, C.L.; Dalessio, D.J. Pattern shift visual evoked responses and EEG in migraine. Headache J. Head Face Pain 1986, 26, 451–456. [Google Scholar] [CrossRef]
- Drake, M.E.; Du Bois, C.; Huber, S.J.; Pakanis, A.; Denio, L.S. EEG spectral analysis and time domain descriptors in headache. Headache 1988, 28, 201–203. [Google Scholar] [CrossRef]
- Hughes, J.R.; Robbins, L.D. Brain mapping in migraine. Clin. Electroencephalogr. 1990, 21, 14–24. [Google Scholar] [CrossRef]
- Parain, D.; Samson-Dollfus, D. Electroencephalograms in basilar artery migraine. Electroencephalogr. Clin. Neurophysiol. 1984, 58, 392–399. [Google Scholar] [CrossRef]
- Walker, J.E. QEEG-guided neurofeedback for recurrent migraine headaches. Clin. EEG Neurosci. 2011, 42, 59–61. [Google Scholar] [CrossRef]
- Jensen, M.P. A neuropsychological model of pain: Research and clinical implications. J. Pain 2010, 11, 2–12. [Google Scholar] [CrossRef]
- Knyazev, G.G. EEG delta oscillations as a correlate of basic homeostatic and motivational processes. Neurosci. Biobehav. Rev. 2012, 36, 677–695. [Google Scholar] [CrossRef]
- Xie, J.; Lu, Y.; Li, J.; Zhang, W. Alpha neural oscillation of females in the luteal phase is sensitive to high risk during sequential risk decisions. Behav. Brain Res. 2021, 413, 113427. [Google Scholar] [CrossRef]
- Coppola, G.; Pierelli, F.; Schoenen, J. Is the cerebral cortex hyperexcitable or hyperresponsive in migraine? Cephalalgia 2007, 27, 1429–1439. [Google Scholar] [CrossRef]
- Borsook, D.; Maleki, N.; Becerra, L.; McEwen, B. Understanding Migraine through the Lens of Maladaptive Stress Responses: A Model Disease of Allostatic Load. Neuron 2012, 73, 219–234. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Pain Place L (Left), R (Right) | Symptoms |
|---|---|---|
| 1 | Frontal L | Dizziness |
| 2 | Fronto-Parietal R | Blurred vision |
| 3 | Frontal R | None |
| 4 | Frontal L–R | None |
| 5 | Frontal L | Dizziness |
| 6 | Frontal L-R | Dizziness |
| 7 | Frontal L-R | None |
| 8 | Frontal L | Dizziness |
| 9 | Frontal R | Dizziness |
| 10 | Frontal L | Dizziness, blurred vision |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pelayo-González, H.J.; Reyes-Meza, V.; Méndez-Balbuena, I.; Méndez-Díaz, O.; Trenado, C.; Ruge, D.; García-Aguilar, G.; López-Cortés, V.A. Quantitative Electroencephalographic Analysis in Women with Migraine during the Luteal Phase. Appl. Sci. 2023, 13, 7443. https://doi.org/10.3390/app13137443
Pelayo-González HJ, Reyes-Meza V, Méndez-Balbuena I, Méndez-Díaz O, Trenado C, Ruge D, García-Aguilar G, López-Cortés VA. Quantitative Electroencephalographic Analysis in Women with Migraine during the Luteal Phase. Applied Sciences. 2023; 13(13):7443. https://doi.org/10.3390/app13137443
Chicago/Turabian StylePelayo-González, Héctor Juan, Verónica Reyes-Meza, Ignacio Méndez-Balbuena, Oscar Méndez-Díaz, Carlos Trenado, Diane Ruge, Gregorio García-Aguilar, and Vicente Arturo López-Cortés. 2023. "Quantitative Electroencephalographic Analysis in Women with Migraine during the Luteal Phase" Applied Sciences 13, no. 13: 7443. https://doi.org/10.3390/app13137443