
Motor Imagery and Paired Associative Stimulation in Poststroke Rehabilitation: Dissociating Motor and Electrophysiological Effects
 ,
,
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
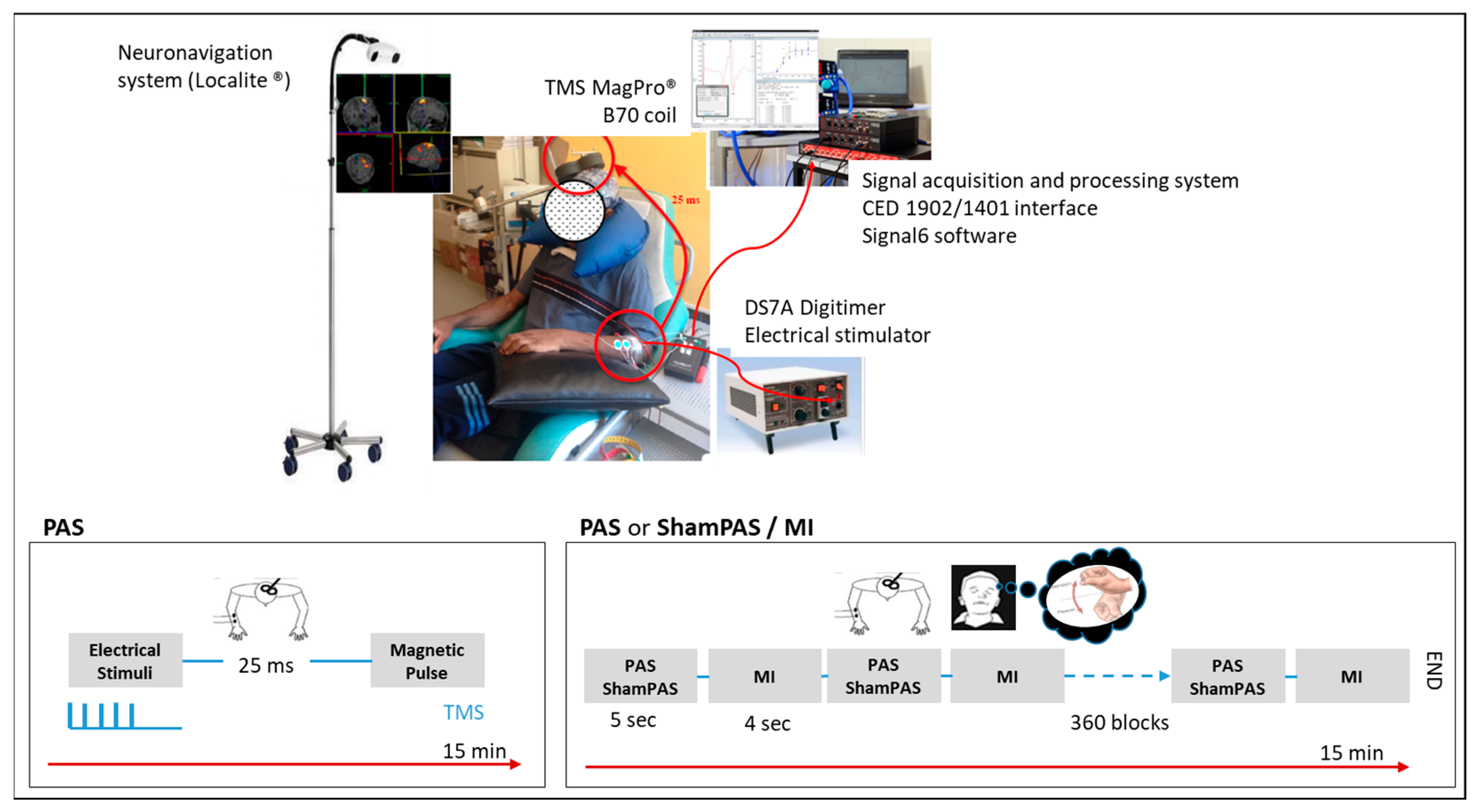
2.3. Experimental Interventions (Figure 1)
2.3.1. TMS Stimulation
2.3.2. Peripheral Electrical Stimulation (ES)
2.3.3. PAS Intervention
2.3.4. PAS/MI Intervention
2.3.5. ShamPAS/MI Intervention
2.4. Study Outcomes
2.4.1. Motor Imagery Outcomes
2.4.2. Electrophysiological Outcomes
2.4.3. Hand Motor Function Outcomes
2.5. Randomization
2.6. Sample Size
2.7. Statistical Analysis
3. Results
3.1. Participants
3.2. Checking for Preliminary Assumptions
3.3. Motor Imagery Outcomes
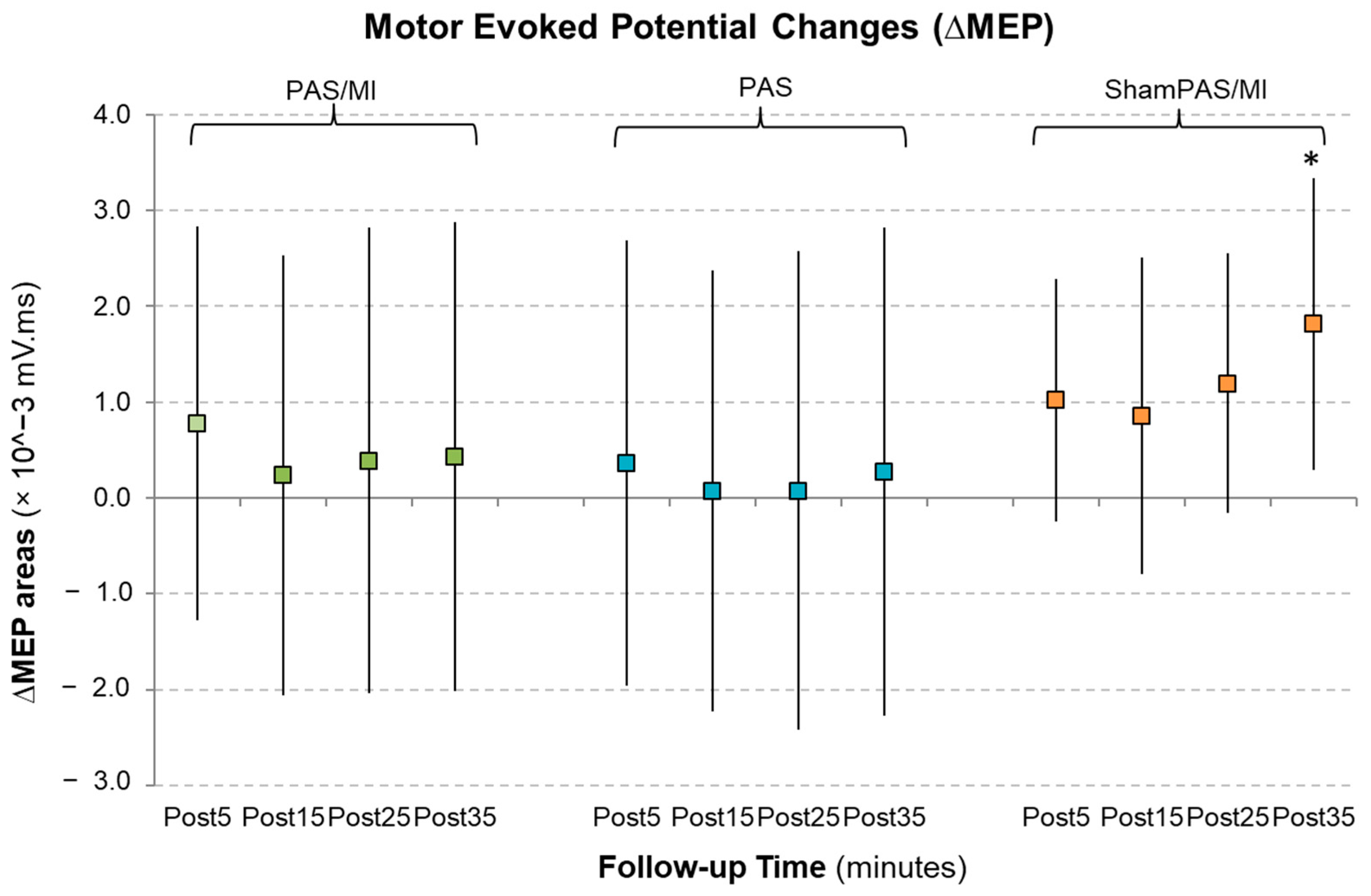
3.4. Corticospinal Excitability Outcomes
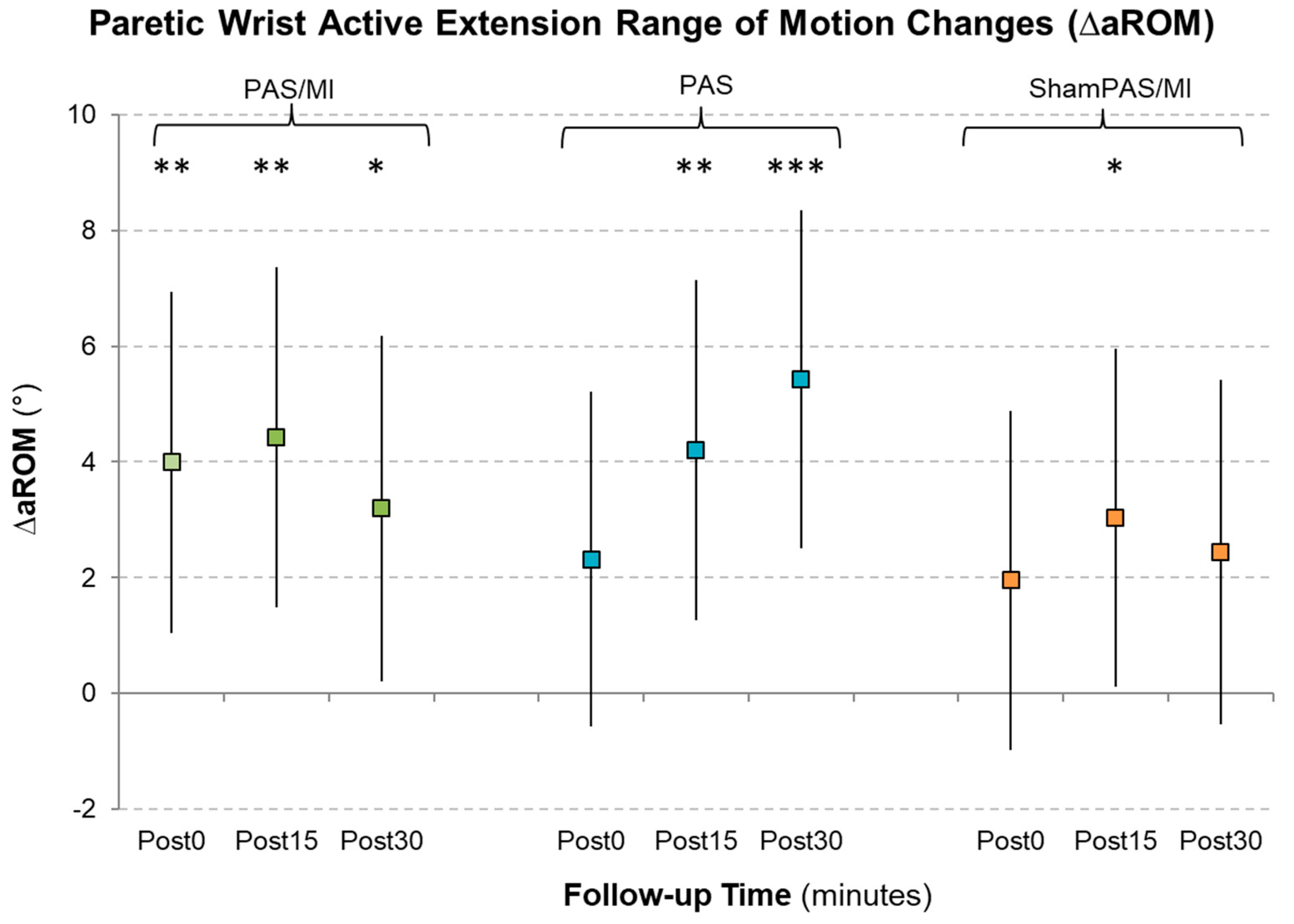
3.5. Hand Motor Function Outcomes
4. Discussion
4.1. Preliminary Assumptions about MI Ability and Performance
4.2. General Results
4.3. Corticospinal Excitability Effects
4.4. Hand Motor Function Effects
4.5. Dissociation of Electrophysiological and Motor Effects
4.6. Limitations and Future Perspectives
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hendricks, H.T.; van Limbeek, J.; Geurts, A.C.; Zwarts, M.J. Motor recovery after stroke: A systematic review of the literature. Arch. Phys. Med. Rehabil. 2002, 83, 1629–1637. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, H.S.; Nakayama, H.; Raaschou, H.O.; Vive-Larsen, J.; Støier, M.; Olsen, T.S. Outcome and time course of recovery in stroke. Part II: Time course of recovery. The Copenhagen Stroke Study. Arch. Phys. Med. Rehabil. 1995, 76, 406–412. [Google Scholar] [CrossRef] [PubMed]
- Kamper, D.; Harvey, R.; Suresh, S.; Rymer, W. Relative contributions of neural mechanisms versus muscle mechanics in promoting finger extension deficits following stroke. Muscle Nerve 2003, 28, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Hatem, S.M.; Saussez, G.; della Faille, M.; Prist, V.; Zhang, X.; Dispa, D.; Bleyenheuft, Y. Rehabilitation of motor function after stroke: A multiple systematic review focused on techniques to stimulate upper extremity recovery. Front. Hum. Neurosci. 2016, 10, 442. [Google Scholar] [CrossRef]
- Kubis, N. Non-invasive brain stimulation to enhance post-stroke recovery. Front. Neural Circuits 2016, 10, 56. [Google Scholar] [CrossRef]
- Stefan, K.; Kunesch, E.; Cohen, L.G.; Benecke, R.; Classen, J. Induction of plasticity in the human motor cortex by paired associative stimulation. Brain 2000, 123 Pt 3, 572–584. [Google Scholar] [CrossRef] [PubMed]
- Ridding, M.C.; Taylor, J.L. Mechanisms of motor-evoked potential facilitation following prolonged dual peripheral and central stimulation in humans. J. Physiol. 2001, 537, 623–631. [Google Scholar] [CrossRef]
- Castel-Lacanal, E.; Gerdelat-Mas, A.; Marque, P.; Loubinoux, I.; Simonetta-Moreau, M. Induction of cortical plastic changes in wrist muscles by paired associative stimulation in healthy subjects and post-stroke patients. Exp. Brain Res. 2007, 180, 113–122. [Google Scholar] [CrossRef]
- Castel-Lacanal, E.; Marque, P.; Tardy, J.; De Boissezon, X.; Guiraud, V.; Chollet, F.; Loubinoux, I.; Simonetta-Moreau, M. Induction of Cortical Plastic Changes in Wrist Muscles by Paired Associative Stimulation in the Recovery Phase of Stroke Patients. Neurorehabil. Neural Repair 2009, 23, 366–372. [Google Scholar] [CrossRef]
- Palmer, J.A.; Wolf, S.L.; Borich, M.R. Paired associative stimulation modulates corticomotor excitability in chronic stroke: A preliminary investigation. Restor. Neurol. Neurosci. 2018, 36, 183–194. [Google Scholar] [CrossRef]
- Versace, V.; Langthaler, P.B.; Höller, Y.; Frey, V.N.; Brigo, F.; Sebastianelli, L.; Saltuari, L.; Nardone, R. Abnormal cortical neuroplasticity induced by paired associative stimulation after traumatic spinal cord injury: A preliminary study. Neurosci. Lett. 2017, 664, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Bunday, K.L.; Urbin, M.; Perez, M.A. Potentiating paired corticospinal-motoneuronal plasticity after spinal cord injury. Brain Stimul. 2018, 11, 1083–1092. [Google Scholar] [CrossRef] [PubMed]
- Bunday, K.L.; Perez, M.A. Motor recovery after spinal cord injury enhanced by strengthening corticospinal synaptic transmission. Curr. Biol. 2012, 22, 2355–2361. [Google Scholar] [CrossRef] [PubMed]
- Tolmacheva, A.; Savolainen, S.; Kirveskari, E.; Brandstack, N.; Mäkelä, J.P.; Shulga, A. Paired associative stimulation improves hand function after non-traumatic spinal cord injury: A case series. Clin. Neurophysiol. Pract. 2019, 4, 178–183. [Google Scholar] [CrossRef] [PubMed]
- Jo, H.J.; Perez, M.A. Corticospinal-motor neuronal plasticity promotes exercise-mediated recovery in humans with spinal cord injury. Brain 2020, 143, 1368–1382. [Google Scholar] [CrossRef]
- Guo, T.-C.; Hu, Y.; Zhang, X.-Y.; Tian, J.; Lu, Y.-S. Paired associative stimulation improves synaptic plasticity and functional outcomes after cerebral ischemia. Neural Regen. Res. 2019, 14, 1968–1976. [Google Scholar] [CrossRef]
- Sui, Y.-F.; Tong, L.-Q.; Zhang, X.-Y.; Song, Z.-H.; Guo, T.-C. Effects of paired associated stimulation with different stimulation position on motor cortex excitability and upper limb motor function in patients with cerebral infarction. J. Clin. Neurosci. 2021, 90, 363–369. [Google Scholar] [CrossRef]
- Tarri, M.; Brihmat, N.; Gasq, D.; Lepage, B.; Loubinoux, I.; De Boissezon, X.; Marque, P.; Castel-Lacanal, E. Five-day course of paired associative stimulation fails to improve motor function in stroke patients. Ann. Phys. Rehabil. Med. 2018, 61, 78–84. [Google Scholar] [CrossRef]
- Fathi, D.; Ueki, Y.; Mima, T.; Koganemaru, S.; Nagamine, T.; Tawfik, A.; Fukuyama, H. Effects of aging on the human motor cortical plasticity studied by paired associative stimulation. Clin. Neurophysiol. 2010, 121, 90–93. [Google Scholar] [CrossRef]
- Malouin, F.; Jackson, P.L.; Richards, C.L. Towards the integration of mental practice in rehabilitation programs. A critical review. Front. Hum. Neurosci. 2013, 7, 576. [Google Scholar] [CrossRef]
- Kim, Y.K.; Park, E.; Lee, A.; Im, C.-H.; Kim, Y.-H. Changes in network connectivity during motor imagery and execution. PLoS ONE 2018, 13, e0190715. [Google Scholar] [CrossRef] [PubMed]
- Szameitat, A.J.; Shen, S.; Conforto, A.; Sterr, A. Cortical activation during executed, imagined, observed, and passive wrist movements in healthy volunteers and stroke patients. Neuroimage 2012, 62, 266–280. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Byblow, W.; Steyvers, M.; Levin, O.; Swinnen, S.P. Kinesthetic, but not visual, motor imagery modulates corticomotor excitability. Exp. Brain Res. 2006, 168, 157–164. [Google Scholar] [CrossRef]
- Kaneko, F.; Hayami, T.; Aoyama, T.; Kizuka, T. Motor imagery and electrical stimulation reproduce corticospinal excitability at levels similar to voluntary muscle contraction. J. Neuroeng. Rehabil. 2014, 11, 94. [Google Scholar] [CrossRef]
- Ziegler, L.; Schulte, R.; Gharabaghi, A. Combined endogenous and exogenous disinhibition of intracortical circuits augments plasticity induction in the human motor cortex. Brain Stimul. 2019, 12, 1027–1040. [Google Scholar] [CrossRef] [PubMed]
- Brihmat, N.; Tarri, M.; Gasq, D.; Marque, P.; Castel-Lacanal, E.; Loubinoux, I. Cross-modal Functional Connectivity of the Premotor Cortex reflects Residual Motor Output after Stroke. Brain Connect. 2020, 10, 236–249. [Google Scholar] [CrossRef]
- Wasserman, E.M. Risk and safety of repetitive transcranial magnetic stimulation: Report and suggested guidelines from the International Workshop on the Safety of Repetitive Transcranial Magnetic Stimulation, June 5–7, 1996. Electroenchaphalogr. Clin. Neurophysiol. 1998, 108, 1–16. [Google Scholar] [CrossRef]
- Malouin, F.; Richards, C.L.; Durand, A.; Doyon, J. Reliability of Mental Chronometry for Assessing Motor Imagery Ability After Stroke. Arch. Phys. Med. Rehabil. 2008, 89, 311–319. [Google Scholar] [CrossRef]
- Malouin, F.; Richards, C.L.; Jackson, P.; LaFleur, M.F.; Durand, A.; Doyon, J. The Kinesthetic and Visual Imagery Questionnaire (KVIQ) for assessing motor imagery in persons with physical disabilities: A reliability and construct validity study. J. Neurol. Phys. Ther. 2007, 31, 20–29. [Google Scholar] [CrossRef]
- Sattler, V.; Dickler, M.; Michaud, M.; Simonetta-Moreau, M. Interhemispheric inhibition in human wrist muscles. Exp. Brain Res. 2012, 221, 449–458. [Google Scholar] [CrossRef]
- Vickers, A.J. The use of percentage change from baseline as an outcome in a controlled trial is statistically inefficient: A simulation study. BMC Med. Res. Methodol. 2001, 1, 6. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.-S.; Wang, X.-J.; Gong, L.-K. The Construction of a Williams Design and Randomization in Cross-Over Clinical Trials Using SAS. J. Stat. Softw. 2009, 29, 1–10. [Google Scholar] [CrossRef]
- Talelli, P.; Greenwood, R.; Rothwell, J. Exploring Theta Burst Stimulation as an intervention to improve motor recovery in chronic stroke. Clin. Neurophysiol. 2007, 118, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Stefan, K.; Kunesch, E.; Benecke, R.; Cohen, L.G.; Classen, J. Mechanisms of enhancement of human motor cortex excitability induced by interventional paired associative stimulation. J. Physiol. 2002, 543, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.; Byblow, W.; Ward, S. An update on predicting motor recovery after stroke. Ann. Phys. Rehabil. Med. 2014, 57, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Foysal, K.M.R.; Baker, S.N. Induction of plasticity in the human motor system by motor imagery and transcranial magnetic stimulation. J. Physiol. 2020, 598, 2385–2396. [Google Scholar] [CrossRef]
- de Vries, S.; Tepper, M.; Otten, B.; Mulder, T. Recovery of motor imagery ability in stroke patients. Rehabil. Res. Pract. 2011, 2011, 283840. [Google Scholar] [CrossRef]
- Collet, C.; Guillot, A.; Lebon, F.; MacIntyre, T.; Moran, A. Measuring motor imagery using psychometric, behavioral, and psychophysiological tools. Exerc. Sport Sci. Rev. 2011, 39, 85–92. [Google Scholar] [CrossRef]
- Siebner, H.R.; Lang, N.; Rizzo, V.; Nitsche, M.A.; Paulus, W.; Lemon, R.N.; Rothwell, J.C. Preconditioning of Low-Frequency Repetitive Transcranial Magnetic Stimulation with Transcranial Direct Current Stimulation: Evidence for Homeostatic Plasticity in the Human Motor Cortex. J. Neurosci. 2004, 24, 3379–3385. [Google Scholar] [CrossRef]
- Stefan, K.; Wycislo, M.; Gentner, R.; Schramm, A.; Naumann, M.; Reiners, K.; Classen, J. Temporary Occlusion of Associative Motor Cortical Plasticity by Prior Dynamic Motor Training. Cereb. Cortex 2006, 16, 376–385. [Google Scholar] [CrossRef]
- Avanzino, L.; Gueugneau, N.; Bisio, A.; Ruggeri, P.; Papaxanthis, C.; Bove, M. Motor cortical plasticity induced by motor learning through mental practice. Front. Behav. Neurosci. 2015, 9, 105. [Google Scholar] [CrossRef] [PubMed]
- Ruffino, C.; Papaxanthis, C.; Lebon, F. Neural plasticity during motor learning with motor imagery practice: Review and perspectives. Neuroscience 2017, 341, 61–78. [Google Scholar] [CrossRef]
- Li, F.; Zhang, T.; Li, B.-J.; Zhang, W.; Zhao, J.; Song, L.-P. Motor imagery training induces changes in brain neural networks in stroke patients. Neural Regen. Res. 2018, 13, 1771–1781. [Google Scholar] [CrossRef]
- Mrachacz-Kersting, N.; Voigt, M.; Stevenson, A.; Aliakbaryhosseinabadi, S.; Jiang, N.; Dremstrup, K.; Farina, D. The effect of type of afferent feedback timed with motor imagery on the induction of cortical plasticity. Brain Res. 2017, 1674, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Kasai, T.; Kawai, S.; Kawanishi, M.; Yahagi, S. Evidence for facilitation of motor evoked potentials (MEPs) induced by motor imagery. Brain Res. 1997, 744, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Foysal, K.M.R.; Baker, S.N. A hierarchy of corticospinal plasticity in human hand and forearm muscles. J. Physiol. 2019, 597, 2729–2739. [Google Scholar] [CrossRef]
- Guerra, A.; Lopez-Alonso, V.; Cheeran, B.; Suppa, A. Variability in non-invasive brain stimulation studies: Reasons and results. Neurosci. Lett. 2017, 719, 133330. [Google Scholar] [CrossRef]
- Sale, M.V.; Ridding, M.C.; Nordstrom, M.A. Factors influencing the magnitude and reproducibility of corticomotor excitability changes induced by paired associative stimulation. Exp. Brain Res. 2007, 181, 615–626. [Google Scholar] [CrossRef]
- Fratello, F.; Veniero, D.; Curcio, G.; Ferrara, M.; Marzano, C.; Moroni, F.; Pellicciari, M.C.; Bertini, M.; Rossini, P.; De Gennaro, L. Modulation of corticospinal excitability by paired associative stimulation: Reproducibility of effects and intraindividual reliability. Clin. Neurophysiol. 2006, 117, 2667–2674. [Google Scholar] [CrossRef]
- Saimpont, A.; Mercier, C.; Malouin, F.; Guillot, A.; Collet, C.; Doyon, J.; Jackson, P.L. Anodal transcranial direct current stimulation enhances the effects of motor imagery training in a finger tapping task. Eur. J. Neurosci. 2016, 43, 113–119. [Google Scholar] [CrossRef]
- Jo, H.J.; Perez, M.A. Changes in motor-evoked potential latency during grasping after tetraplegia. J. Neurophysiol. 2019, 122, 1675–1684. [Google Scholar] [CrossRef]
- Pascual-Leone, A.; Nguyet, D.; Cohen, L.G.; Brasil-Neto, J.P.; Cammarota, A.; Hallett, M. Modulation of muscle responses evoked by transcranial magnetic stimulation during the acquisition of new fine motor skills. J. Neurophysiol. 1995, 74, 1037–1045. [Google Scholar] [CrossRef]
- Goldsworthy, M.R.; Hordacre, B.; Rothwell, J.C.; Ridding, M.C. Effects of rTMS on the brain: Is there value in variability? Cortex 2021, 139, 43–59. [Google Scholar] [CrossRef] [PubMed]
- Pitcher, J.B.; Ogston, K.M.; Miles, T.S. Age and sex differences in human motor cortex input–output characteristics. J. Physiol. 2003, 546 Pt 2, 605–613. [Google Scholar] [CrossRef]
- Lemon, R.N. Descending Pathways in Motor Control. Annu. Rev. Neurosci. 2008, 31, 195–218. [Google Scholar] [CrossRef]
- Welniarz, Q.; Dusart, I.; Roze, E. The corticospinal tract: Evolution, development, and human disorders. Dev. Neurobiol. 2016, 77, 810–829. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Byblow, W.D.; Ackerley, S.J.; Smith, M.C.; Borges, V.M.; Barber, P.A. PREP2: A biomarker-based algorithm for predicting upper limb function after stroke. Ann. Clin. Transl. Neurol. 2017, 4, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Birchenall, J.; Térémetz, M.; Roca, P.; Lamy, J.-C.; Oppenheim, C.; Maier, M.A.; Mas, J.-L.; Lamy, C.; Baron, J.-C.; Lindberg, P.G. Individual recovery profiles of manual dexterity, and relation to corticospinal lesion load and excitability after stroke—A longitudinal pilot study. Neurophysiol. Clin. 2018, 49, 149–164. [Google Scholar] [CrossRef]
- Choudhury, S.; Shobhana, A.; Singh, R.; Sen, D.; Anand, S.S.; Shubham, S.; Baker, M.; Kumar, H.; Baker, S.N. The Relationship Between Enhanced Reticulospinal Outflow and Upper Limb Function in Chronic Stroke Patients. Neurorehabil. Neural Repair 2019, 33, 375–383. [Google Scholar] [CrossRef]
- Lindenberg, R.; Renga, V.; Zhu, L.L.; Betzler, F.; Alsop, D.; Schlaug, G. Structural integrity of corticospinal motor fibers predicts motor impairment in chronic stroke. Neurology 2010, 74, 280–287. [Google Scholar] [CrossRef]
- Schulz, R.; Park, C.-H.; Boudrias, M.-H.; Gerloff, C.; Hummel, F.C.; Ward, N. Assessing the Integrity of Corticospinal Pathways From Primary and Secondary Cortical Motor Areas After Stroke. Stroke 2012, 43, 2248–2251. [Google Scholar] [CrossRef] [PubMed]
- Schulz, R.; Park, E.; Lee, J.; Chang, W.H.; Lee, A.; Kim, Y.-H.; Hummel, F.C. Synergistic but independent: The role of corticospinal and alternate motor fibers for residual motor output after stroke. NeuroImage Clin. 2017, 15, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Bestmann, S.; Krakauer, J.W. The uses and interpretations of the motor-evoked potential for understanding behaviour. Exp. Brain Res. 2015, 233, 679–689. [Google Scholar] [CrossRef] [PubMed]
- López-Alonso, V.; Cheeran, B.; Río-Rodríguez, D.; Fernández-Del-Olmo, M. Inter-individual variability in response to non-invasive brain stimulation paradigms. Brain Stimul. 2014, 7, 372–380. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean | SD (Range) |
|---|---|---|
| Age (years) | 53.1 | 13.2 [27–74] |
| Time since stroke (months) | 9.7 | 20.9 [1–105] |
| UEFMS | ||
| UEFMSA (/36) | 17 | 6.9 [4–28] |
| UEFMSB (/10) | 3 | 2.8 [0–7] |
| Total (/66) | 27.4 | 13.3 [7–49] |
| KVIQ | ||
| VIQ (/85) | 65.1 | 12 [40–85] |
| KIQ (/85) | 53.6 | 14.1 [23–85] |
| Total (/170) | 118.8 | 22.7 [80–170] |
| Paretic wrist aROM (°) | 42.8 | 22.1 [0–78] |
| Number (n) | Percentage (%) | |
| Lesion Locations | ||
| Cortical | 11 | 45.8 |
| Subcortical | 10 | 41.7 |
| Brainstem | 3 | 12.5 |
| Stroke Types | ||
| Ischemic | 19 | 79.2 |
| Hemorrhagic | 5 | 20.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brihmat, N.; Castel-Lacanal, E.; Tarri, M.; Lepage, B.; Montane, E.; Cormier, C.; de Boissezon, X.; Gasq, D.; Loubinoux, I.; Marque, P. Motor Imagery and Paired Associative Stimulation in Poststroke Rehabilitation: Dissociating Motor and Electrophysiological Effects. Appl. Sci. 2023, 13, 6063. https://doi.org/10.3390/app13106063
Brihmat N, Castel-Lacanal E, Tarri M, Lepage B, Montane E, Cormier C, de Boissezon X, Gasq D, Loubinoux I, Marque P. Motor Imagery and Paired Associative Stimulation in Poststroke Rehabilitation: Dissociating Motor and Electrophysiological Effects. Applied Sciences. 2023; 13(10):6063. https://doi.org/10.3390/app13106063
Chicago/Turabian StyleBrihmat, Nabila, Evelyne Castel-Lacanal, Mohamed Tarri, Benoit Lepage, Emmeline Montane, Camile Cormier, Xavier de Boissezon, David Gasq, Isabelle Loubinoux, and Philippe Marque. 2023. "Motor Imagery and Paired Associative Stimulation in Poststroke Rehabilitation: Dissociating Motor and Electrophysiological Effects" Applied Sciences 13, no. 10: 6063. https://doi.org/10.3390/app13106063