
The Effect of Sleep Disorder Diagnosis on Mortality in End-Stage Renal Disease Patients
 , , and
, , and
Abstract
:Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Population
2.2. Exclusions
2.3. Main Independent Variables
2.4. Outcome Variabl
2.5. Demographic and Other Risk Factors
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bello, A.K.; Alrukhaimi, M.; Ashuntantang, G.E.; Basnet, S.; Rotter, R.C.; Douthat, W.G.; Kazancioglu, R.; Kottgen, A.; Nangaku, M.; Powe, N.R.; et al. Complications of chronic kidney disease: Current state, knowledge gaps, and strategy for action. Kidney Int. Suppl. 2017, 7, 122–129. [Google Scholar] [CrossRef] [PubMed]
- Couser, W.G.; Remuzzi, G.; Mendis, S.; Tonelli, M. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 2011, 80, 1258–1270. [Google Scholar] [CrossRef] [PubMed]
- Kent, S.; Schlackow, I.; Lozano-Kuhne, J.; Reith, C.; Emberson, J.; Haynes, R.; Gray, A.; Cass, A.; Baigent, C.; Landray, M.J.; et al. What is the impact of chronic kidney disease stage and cardiovascular disease on the annual cost of hospital care in moderate-to-severe kidney disease? BMC Nephrol. 2015, 16, 65. [Google Scholar] [CrossRef] [PubMed]
- Saran, R.; Robinson, B.; Abbott, K.C.; Agodoa, L.Y.C.; Bhave, N.; Bragg-Gresham, J.; Balkrishnan, R.; Dietrich, X.; Eckard, A.; Eggers, P.W.; et al. US Renal Data System 2017 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2018, 71, A7. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef]
- Zoccali, C.; Mallamaci, F.; Tripepi, G. Traditional and emerging cardiovascular risk factors in end-stage renal disease. Kidney Int. Suppl. 2003, 63, S105–S110. [Google Scholar] [CrossRef]
- Lin, C.H.; Lurie, R.C.; Lyons, O.D. Sleep Apnea and Chronic Kidney Disease: A State-of-the-Art Review. Chest 2020, 157, 673–685. [Google Scholar] [CrossRef]
- Chen, W.C.; Lim, P.S.; Wu, W.C.; Chiu, H.C.; Chen, C.H.; Kuo, H.Y.; Tsai, T.W.; Chien, P.I.; Su, Y.J.; Su, Y.L.; et al. Sleep behavior disorders in a large cohort of chinese (Taiwanese) patients maintained by long-term hemodialysis. Am. J. Kidney Dis. 2006, 48, 277–284. [Google Scholar] [CrossRef]
- Mahowald, M.W.; Bornemann, M.A. Sleep and ESRD: A wake-up call. Am. J. Kidney Dis. 2006, 48, 332–334. [Google Scholar] [CrossRef]
- Cukor, D.; Unruh, M.; McCurry, S.M.; Mehrotra, R. The challenge of insomnia for patients on haemodialysis. Nat. Rev. Nephrol. 2021, 17, 147–148. [Google Scholar] [CrossRef]
- Eloot, S.; Holvoet, E.; Dequidt, C.; Maertens, S.J.; Vanommeslaeghe, F.; Van Biesen, W. The complexity of sleep disorders in dialysis patients. Clin. Kidney J. 2021, 14, 2029–2036. [Google Scholar] [CrossRef]
- Nicholl, D.D.M.; Ahmed, S.B.; Loewen, A.H.S.; Hemmelgarn, B.R.; Sola, D.Y.; Beecroft, J.M.; Turin, T.C.; Hanly, P.J. Declining kidney function increases the prevalence of sleep apnea and nocturnal hypoxia. Chest 2012, 141, 1422–1430. [Google Scholar] [CrossRef]
- Perl, J.; Unruh, M.L.; Chan, C.T. Sleep disorders in end-stage renal disease: ‘Markers of inadequate dialysis’? Kidney Int. 2006, 70, 1687–1693. [Google Scholar] [CrossRef]
- Kanbay, A.; Buyukoglan, H.; Ozdogan, N.; Kaya, E.; Oymak, F.S.; Gulmez, I.; Demir, R.; Kokturk, O.; Covic, A. Obstructive sleep apnea syndrome is related to the progression of chronic kidney disease. Int. Urol. Nephrol. 2012, 44, 535–539. [Google Scholar] [CrossRef]
- Zoccali, C.; Mallamaci, F.; Tripepi, G. Nocturnal hypoxemia predicts incident cardiovascular complications in dialysis patients. J. Am. Soc. Nephrol. 2002, 13, 729–733. [Google Scholar] [CrossRef]
- Fine, L.G.; Norman, J.T. Chronic hypoxia as a mechanism of progression of chronic kidney diseases: From hypothesis to novel therapeutics. Kidney Int. 2008, 74, 867–872. [Google Scholar] [CrossRef]
- Fine, L.G.; Orphanides, C.; Norman, J.T. Progressive renal disease: The chronic hypoxia hypothesis. Kidney Int. Suppl. 1998, 65, S74–S78. [Google Scholar]
- Tang, S.C.; Lam, B.; Lai, A.S.; Pang, C.B.; Tso, W.K.; Khong, P.L.; Ip, M.S.; Lai, K.N. Improvement in sleep apnea during nocturnal peritoneal dialysis is associated with reduced airway congestion and better uremic clearance. Clin. J. Am. Soc. Nephrol. 2009, 4, 410–418. [Google Scholar] [CrossRef]
- Takaki, J.; Nishi, T.; Nangaku, M.; Shimoyama, H.; Inada, T.; Matsuyama, N.; Kumano, H.; Kuboki, T. Clinical and psychological aspects of restless legs syndrome in uremic patients on hemodialysis. Am. J. Kidney Dis. 2003, 41, 833–839. [Google Scholar] [CrossRef]
- Walker, S.; Fine, A.; Kryger, M.H. Sleep complaints are common in a dialysis unit. Am. J. Kidney Dis. 1995, 26, 751–756. [Google Scholar] [CrossRef]
- Winkelman, J.W.; Shahar, E.; Sharief, I.; Gottlieb, D.J. Association of restless legs syndrome and cardiovascular disease in the Sleep Heart Health Study. Neurology 2008, 70, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Harris, T.J.; Nazir, R.; Khetpal, P.; Peterson, R.A.; Chava, P.; Patel, S.S.; Kimmel, P.L. Pain, sleep disturbance and survival in hemodialysis patients. Nephrol. Dial. Transplant. 2012, 27, 758–765. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M. Prevalence and comorbidity of sleep disorders in general population. Rev. Prat. 2007, 57, 1521–1528. [Google Scholar] [PubMed]
- Sabry, A.A.; Abo-Zenah, H.; Wafa, E.; Mahmoud, K.; El-Dahshan, K.; Hassan, A.; Abbas, T.M.; Saleh Ael, B.; Okasha, K. Sleep disorders in hemodialysis patients. Saudi J. Kidney Dis. Transplant. 2010, 21, 300–305. [Google Scholar]
- Merlino, G.; Piani, A.; Dolso, P.; Adorati, M.; Cancelli, I.; Valente, M.; Gigli, G.L. Sleep disorders in patients with end-stage renal disease undergoing dialysis therapy. Nephrol. Dial. Transplant. 2006, 21, 184–190. [Google Scholar] [CrossRef]
- Johnson, D.A.; Guo, N.; Rueschman, M.; Wang, R.; Wilson, J.G.; Redline, S. Prevalence and correlates of obstructive sleep apnea among African Americans: The Jackson Heart Sleep Study. Sleep 2018, 41, zsy154. [Google Scholar] [CrossRef]
- Jean-Louis, G.; von Gizycki, H.; Zizi, F.; Dharawat, A.; Lazar, J.M.; Brown, C.D. Evaluation of sleep apnea in a sample of black patients. J. Clin. Sleep Med. 2008, 4, 421–425. [Google Scholar] [CrossRef]
- Chen, X.; Wang, R.; Zee, P.; Lutsey, P.L.; Javaheri, S.; Alcantara, C.; Jackson, C.L.; Williams, M.A.; Redline, S. Racial/Ethnic Differences in Sleep Disturbances: The Multi-Ethnic Study of Atherosclerosis (MESA). Sleep 2015, 38, 877–888. [Google Scholar] [CrossRef]
- Jhamb, M.; Ran, X.; Abdalla, H.; Roumelioti, M.E.; Hou, S.; Davis, H.; Patel, S.R.; Yabes, J.; Unruh, M. Association of Sleep Apnea with Mortality in Patients with Advanced Kidney Disease. Clin. J. Am. Soc. Nephrol. 2020, 15, 182–190. [Google Scholar] [CrossRef]
- Puthenpura, M.M.; Hansrivijit, P.; Ghahramani, N.; Thongprayoon, C.; Cheungpasitporn, W. Chronic kidney disease and concomitant sleep apnea are associated with increased overall mortality: A meta-analysis. Int. Urol. Nephrol. 2020, 52, 2337–2343. [Google Scholar] [CrossRef]
- Argekar, P.; Griffin, V.; Litaker, D.; Rahman, M. Sleep apnea in hemodialysis patients: Risk factors and effect on survival. Hemodial. Int. 2007, 11, 435–441. [Google Scholar] [CrossRef]
- Al Wakeel, J.S.; Mitwalli, A.H.; Al Mohaya, S.; Abu-Aisha, H.; Tarif, N.; Malik, G.H.; Hammad, D. Morbidity and mortality in ESRD patients on dialysis. Saudi J. Kidney Dis. Transplant. 2002, 13, 473–477. [Google Scholar]
- Irwin, M. Effects of sleep and sleep loss on immunity and cytokines. Brain Behav. Immun. 2002, 16, 503–512. [Google Scholar] [CrossRef]
- Elagizi, A.; Kachur, S.; Lavie, C.J.; Carbone, S.; Pandey, A.; Ortega, F.B.; Milani, R.V. An Overview and Update on Obesity and the Obesity Paradox in Cardiovascular Diseases. Prog. Cardiovasc. Dis. 2018, 61, 142–150. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Overall | Hypersomnolence | Insomnia | RLS | OSA/CSA | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Dx N = 4, 561 (0.5%) | No Dx N = 975,581 (99.5%) | Dx N = 67,812 (6.9%) | No Dx N = 912,330 (93.1%) | Dx N = 27,261 (2.8%) | No Dx N = 952,881 (97.2%) | Dx N = 123,220 (12.6%) | No Dx N = 856,922 (87.4%) | |||
| Person Years Follow-Up—mean (SD) | 2.3 (2.0) | 2.7 (2.4) | 2.1 (20) | 2.6 (2.4) | 2.2 (1.9) | 2.7 (2.4) | 1.6 (1.8) | 2.6 (2.4) | ||
| Age—mean (SD) | 64.9 (14.3) | 61.1 (13.5) | 64.9 (14.3) | 63.5 (14.4) | 65 (14.3) | 63.4 (13.8) | 64.9 (14.4) | 62.6 (12.6) | 65.2 (14.5) | |
| Race— n (%) | Black | 277,164 (28.3) | 1383 (30.3) | 275,781 (28.3) | 17,192 (25.4) | 259,972 (28.5) | 3679 (13.5) | 273,485 (28.7) | 34,087 (27.7) | 243,077 (28.4) |
| Other | 53,772 (5.5) | 123 (2.7) | 53,649 (5.5) | 3128 (4.6) | 50,644 (5.6) | 958 (3.5) | 52,814 (5.5) | 3804 (3.1) | 49,968 (5.8) | |
| White | 649,206 (66.2) | 3055 (67.0) | 646,151 (66.2) | 47,492 (70.0.) | 601,714 (66.0) | 22,624 (83.0) | 626,582 (65.8) | 85,329 (69.3) | 563,877 (65.8) | |
| Sex— n (%) | Female | 427,690 (43.6) | 2045 (44.8) | 425,645 (43.6) | 31,842 (47.0) | 395,848 (43.4) | 14,275 (52.4) | 413,415 (43.4) | 50,140 (40.7) | 377,550 (44.1) |
| Male | 552,452 (56.4) | 2516 (55.2) | 549,936 (56.4) | 35,970 (53.0) | 516,482 (56.6) | 12,986 (47.6) | 539,466 (56.6) | 73,080 (59.3) | 479,372 (55.9) | |
| Ethnicity— n (%) | Hispanic | 141,527 (14.4) | 468 (10.3) | 141,059 (14.5) | 9560 (14.1) | 131,967 (14.5) | 2496 (9.2) | 139,031 (14.6) | 12,939 (10.5) | 128,588 (15.0) |
| Non-Hispanic | 838,615 (85.6) | 4093 (89.7) | 834,522 (85.5) | 58,252 (85.9) | 780,363 (85.5) | 24,765 (90.8) | 813,850 (85.4) | 110,281 (89.5) | 728,334 (85.0) | |
| Access Type—n (%) | Catheter | 803,615 (82.0) | 3547 (77.8) | 800,068 (82.0.) | 54,869 (80.9) | 748,746 (82.1) | 21,044 (77.2) | 782,571 (82.1) | 98,986 (80.3) | 704,629 (82.2) |
| Graft | 32,785 (3.3) | 183 (4.0) | 32,602 (3.3) | 2607 (3.8) | 30,178 (3.3) | 1025 (3.8) | 31,760 (3.3) | 4145 (3.4) | 28,640 (3.3) | |
| AVF | 143,742 (14.7) | 831 (18.2) | 142,911 (14.7) | 10,336 (15.2) | 133,406 (14.6) | 5192 (19.1) | 138,550 (14.5) | 20,089 (16.3) | 123,653 (14.4) | |
| Dialysis Modality—n (%) | Hemodia-lysis | 979,124 (99.9) | 4553 (99.8) | 974,571 (99.9) | 67,714 (99.9) | 911,410 (99.9) | 27,219 (99.9) | 951,905 (99.9) | 123,069 (99.9) | 856,055 (99.9) |
| Peritoneal | 1018 (0.1) | NR * | NR * | 98 (0.1) | 920 (0.1) | 42 (0.2) | 976 (0.1) | 151 (0.1) | 867 (0.1) | |
| CCI—mean (SD) | 7.0 (3.9) | 9.5 (2.8) | 7.0 (3.9) | 9.5 (2.9) | 6.8 (3.9) | 9.2 (2.7) | 7.0 (3.9) | 9.2 (2.7) | 6.7 (3.9) | |
| Variable | Level | Mortality | Simple CPH | Final CPH | |||
|---|---|---|---|---|---|---|---|
| Died N = 671,568 (68.5%) | Alive N = 308,574 (31.5%) | HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Time to Death/ Follow-Up—mean (SD) | 2.4 (2.3) | 3.4 (2.7) | |||||
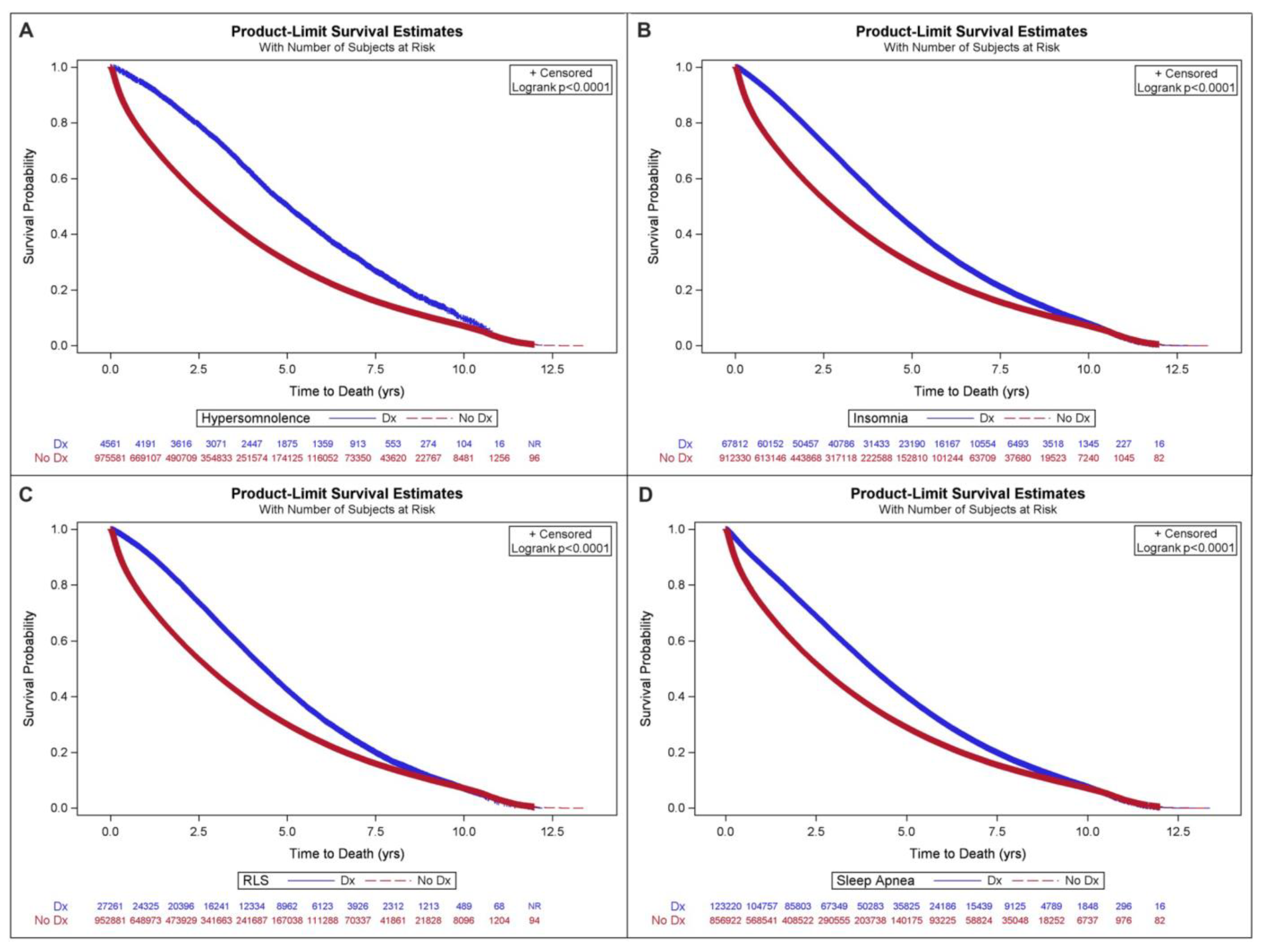
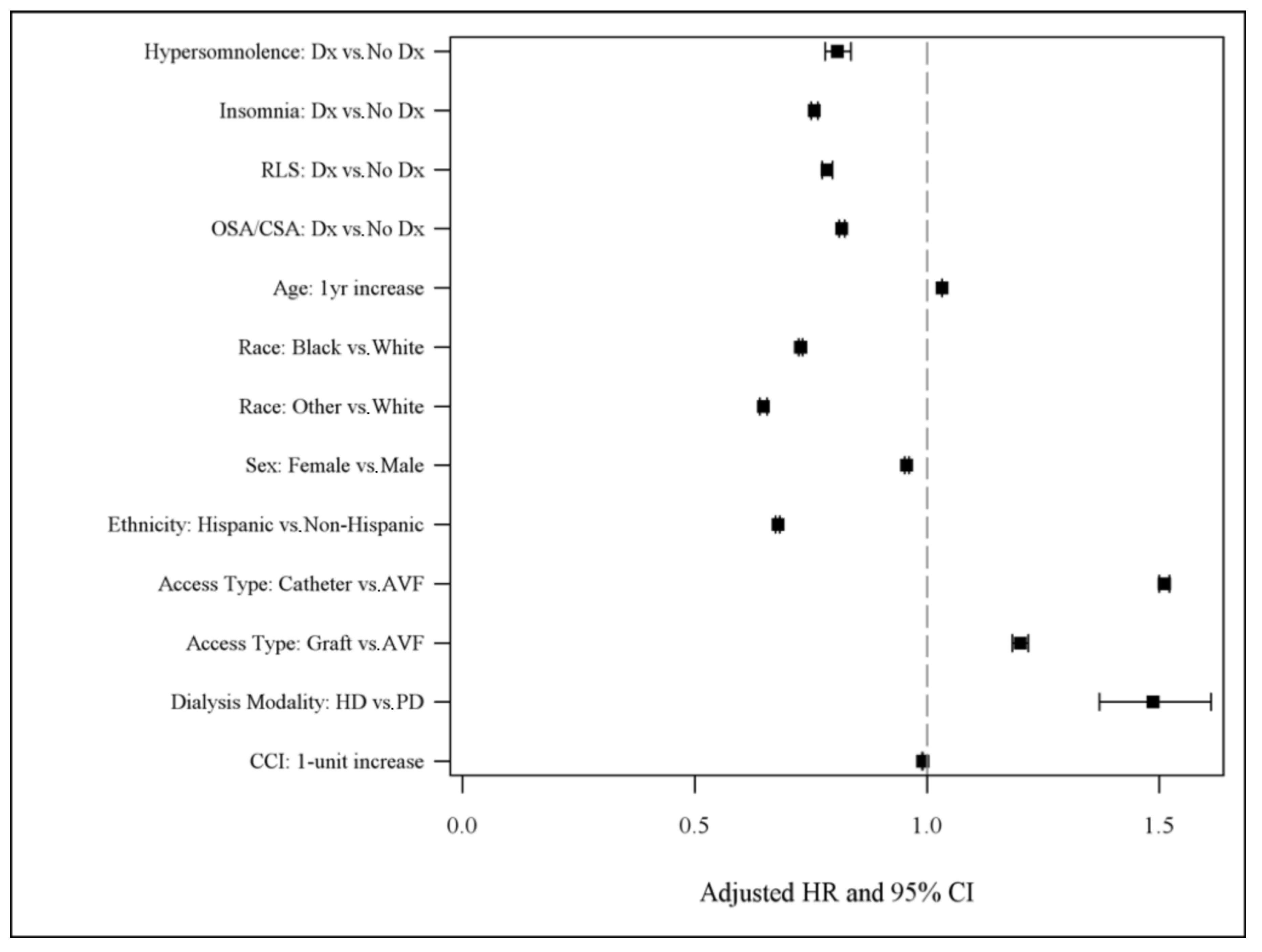
| Hypersomnolence—n (%) | Diagnosis | 3225 (70.7) | 1336 (29.3) | 0.64 (0.61–0.65) | <0.0001 | 0.81 (0.78–0.84) | <0.0001 |
| No Diagnosis | 668,343 (68.5) | 307,238 (31.5) | 1.00 | 1.00 | |||
| Insomnia—n (%) | Diagnosis | 50,691 (74.8) | 17,121 (25.3) | 0.71 (0.81–0.72) | <0.0001 | 0.76 (0.75–0.76) | <0.0001 |
| No Diagnosis | 620,877 (68.1) | 291,453 (32) | 1.00 | 1.00 | |||
| RLS—n (%) | Diagnosis | 20,015 (73.4) | 7246 (26.6) | 0.73 (0.73–0.74) | <0.0001 | 0.79 (0.77–0.80) | <0.0001 |
| No Diagnosis | 651,553 (68.4) | 301,328 (31.6) | 1.00 | 1.00 | |||
| OSA/CSA—n (%) | Diagnosis | 87,877 (71.3) | 35,343 (28.7) | 0.74 (0.73–0.74) | <0.0001 | 0.82 (0.81–0.82) | <0.0001 |
| No Diagnosis | 583,691 (68.1) | 273,231 (31.9) | 1.00 | 1.00 | |||
| Age—mean (SD) | 67.9 (13.3) | 58.3 (14.3) | 1.03 (0.1034–1.034) | <0.0001 | 1.032 (1.032–1.032) | <0.0001 | |
| Race—n (%) | Black | 167,741 (60.5) | 109,423 (39.5) | 0.67 (0.66–0.67) | <0.0001 | 0.73 (0.72–0.73) | <0.0001 |
| Other | 31,452 (58.5) | 22,320 (41.5) | 0.67 (0.66–0.68) | 0.65 (0.64–0.66) | |||
| White | 472,375 (72.8) | 176,831 (27.2) | 1.00 | 1.00 | |||
| Sex—n (%) | Female | 295,485 (69.1) | 132,205 (30.9) | 0.99 (0.98–0.99) | 0.0005 | 0.96 (0.95–0.96) | <0.0001 |
| Male | 376,083 (68.1) | 176,369 (31.9) | 1.00 | 1.00 | |||
| Ethnicity—n (%) | Hispanic | 82,676 (58.4) | 58,851 (41.6) | 0.72 (0.71–0.72) | <0.0001 | 0.68 (0.67–0.68) | <0.0001 |
| Non-Hispanic | 588,892 (70.2) | 249,723 (29.8) | 1.00 | 1.00 | |||
| Access Type – n (%) | Catheter | 562,837 (70.0) | 240,778 (30.0) | 1.37 (1.36–1.38) | <0.0001 | 1.51 (1.50–1.52) | <0.0001 |
| Graft | 22,785 (69.5) | 10,000 (30.5) | 1.16 (1.14–1.17) | 1.20 (1.18–1.22) | |||
| AVF | 85,946 (59.8) | 57,796 (40.2) | 1.00 | 1.00 | |||
| Dialysis Modality—n (%) | Hemodialysis | 670,986 (68.5) | 308,138 (31.5) | 1.57 (1.45–1.71) | <0.0001 | 1.49 (1.37–1.61) | <0.0001 |
| Peritoneal | 582 (57.2) | 436 (42.8) | 1.00 | 1.00 | |||
| CCI—mean (SD) | 7.7 (3.8) | 5.4 (3.7) | 1.008 (1.008–1.009) | <0.0001 | 0.990 (0.989–0.991) | <0.0001 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mixson, A.; Waller, J.L.; Bollag, W.B.; Taskar, V.; Baer, S.L.; Padala, S.; Healy, W.J. The Effect of Sleep Disorder Diagnosis on Mortality in End-Stage Renal Disease Patients. Appl. Sci. 2023, 13, 5354. https://doi.org/10.3390/app13095354
Mixson A, Waller JL, Bollag WB, Taskar V, Baer SL, Padala S, Healy WJ. The Effect of Sleep Disorder Diagnosis on Mortality in End-Stage Renal Disease Patients. Applied Sciences. 2023; 13(9):5354. https://doi.org/10.3390/app13095354
Chicago/Turabian StyleMixson, Andrew, Jennifer L. Waller, Wendy B. Bollag, Varsha Taskar, Stephanie L. Baer, Sandeep Padala, and William J. Healy. 2023. "The Effect of Sleep Disorder Diagnosis on Mortality in End-Stage Renal Disease Patients" Applied Sciences 13, no. 9: 5354. https://doi.org/10.3390/app13095354