

Salivary Interleukin-6, Interleukin-1β, and C-Reactive Protein as a Diagnostic Tool for Plaque-Induced Gingivitis in Children
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
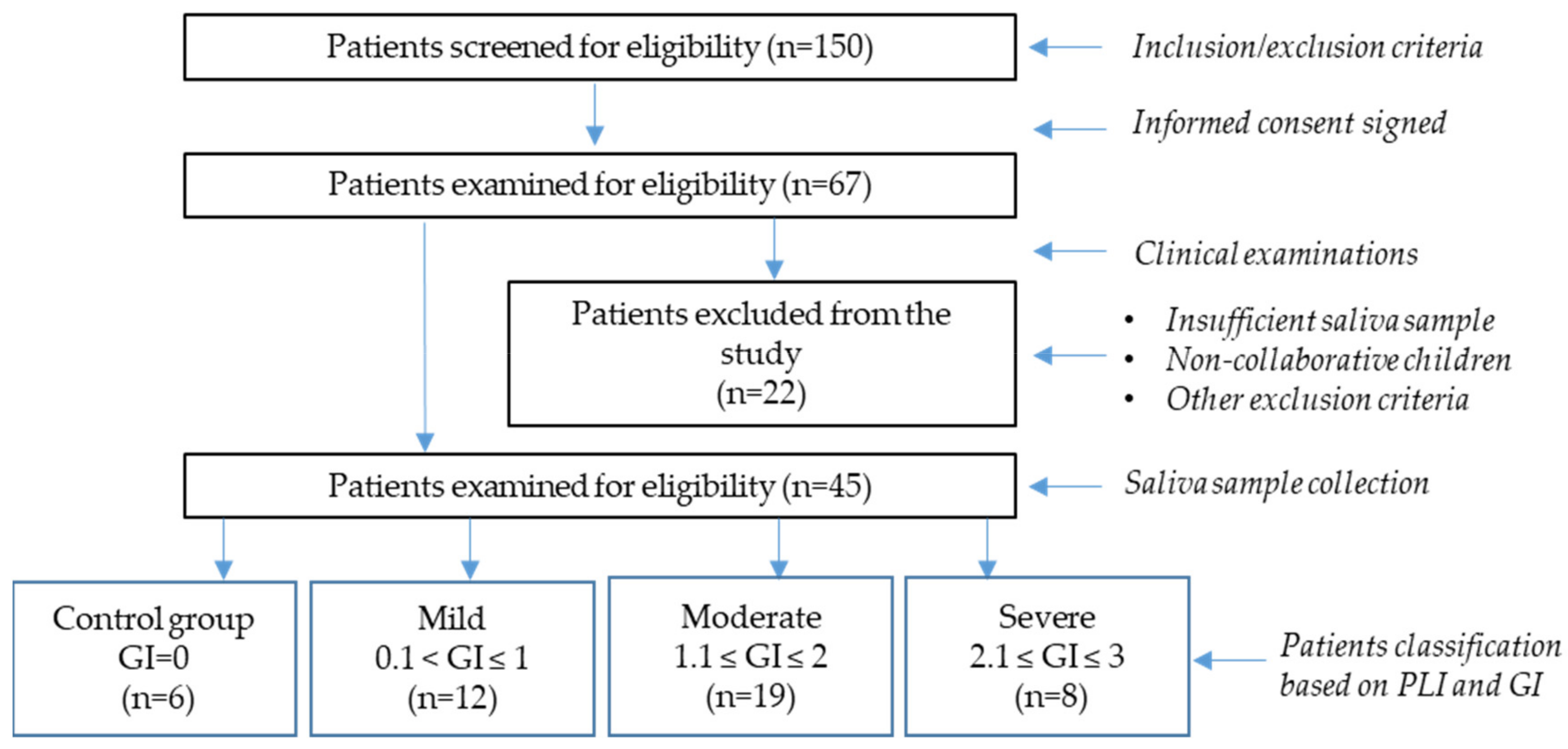
2.1. Study Design
- Informed consent signed by the parent or guardian of each participant;
- Age between 4–14 years;
- No acute or chronic disease reported;
- No medicine intake, including homeopathic remedies;
- No known allergic reactions.
- Children who are not collaborative during the examination and/or sample collection procedures;
- Children with reported acute or chronic disease at the time of examination;
- Children taking any treatment (anti-inflammatory, antibiotics, anti-allergy drugs, or homeopathic remedies);
- Children with established allergic reactions;
- Children displaying an open bite and mouth breathing;
2.2. Sample Size Calculation
2.3. Salivary Sample Collection and Analysis
2.4. Statistical Analysis
3. Results
3.1. Clinical Indicators for Plaque-Induced Gingivitis
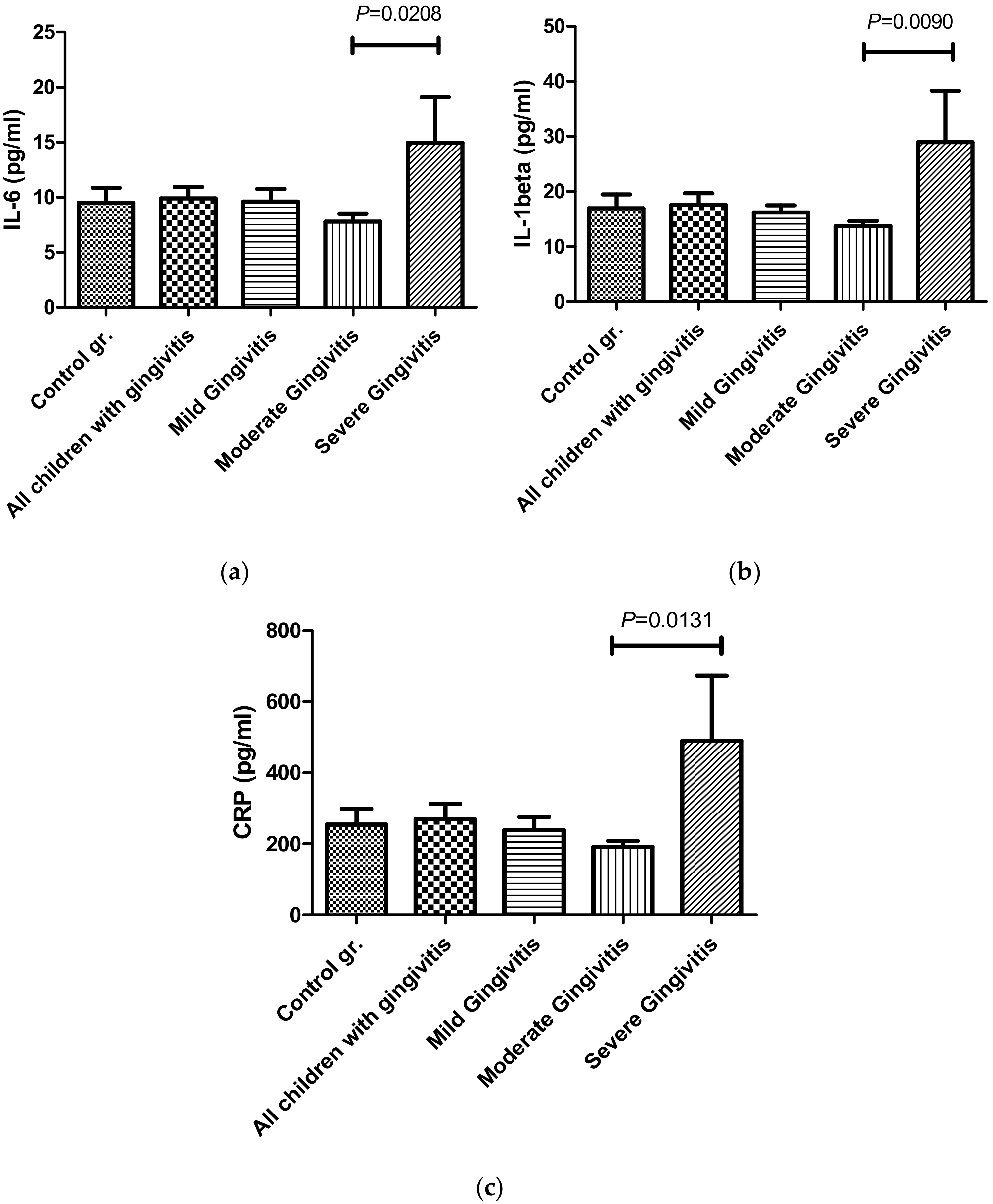
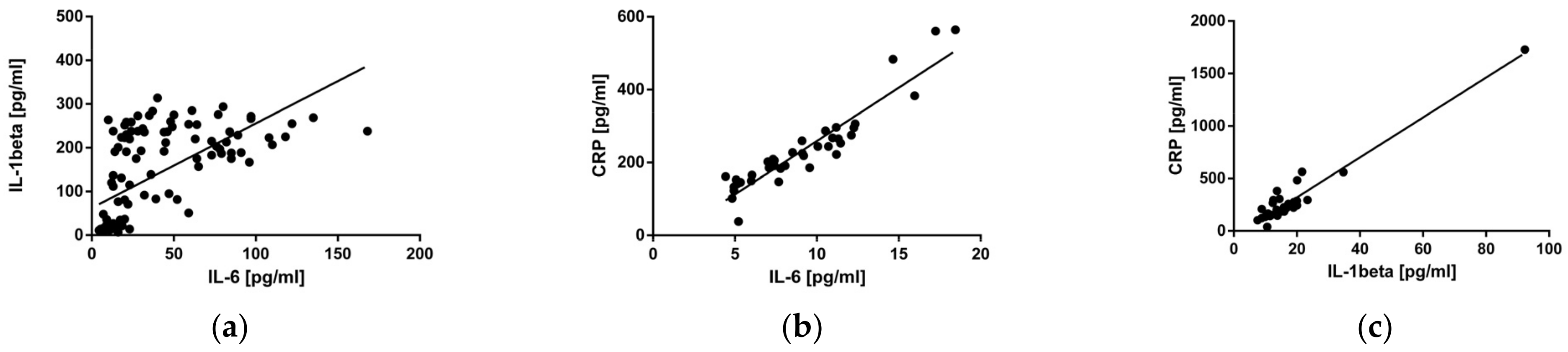
3.2. Salivary Levels of IL-6, IL-1β, and CRP in Children with Different Degrees of Plaque-Induced Gingivitis
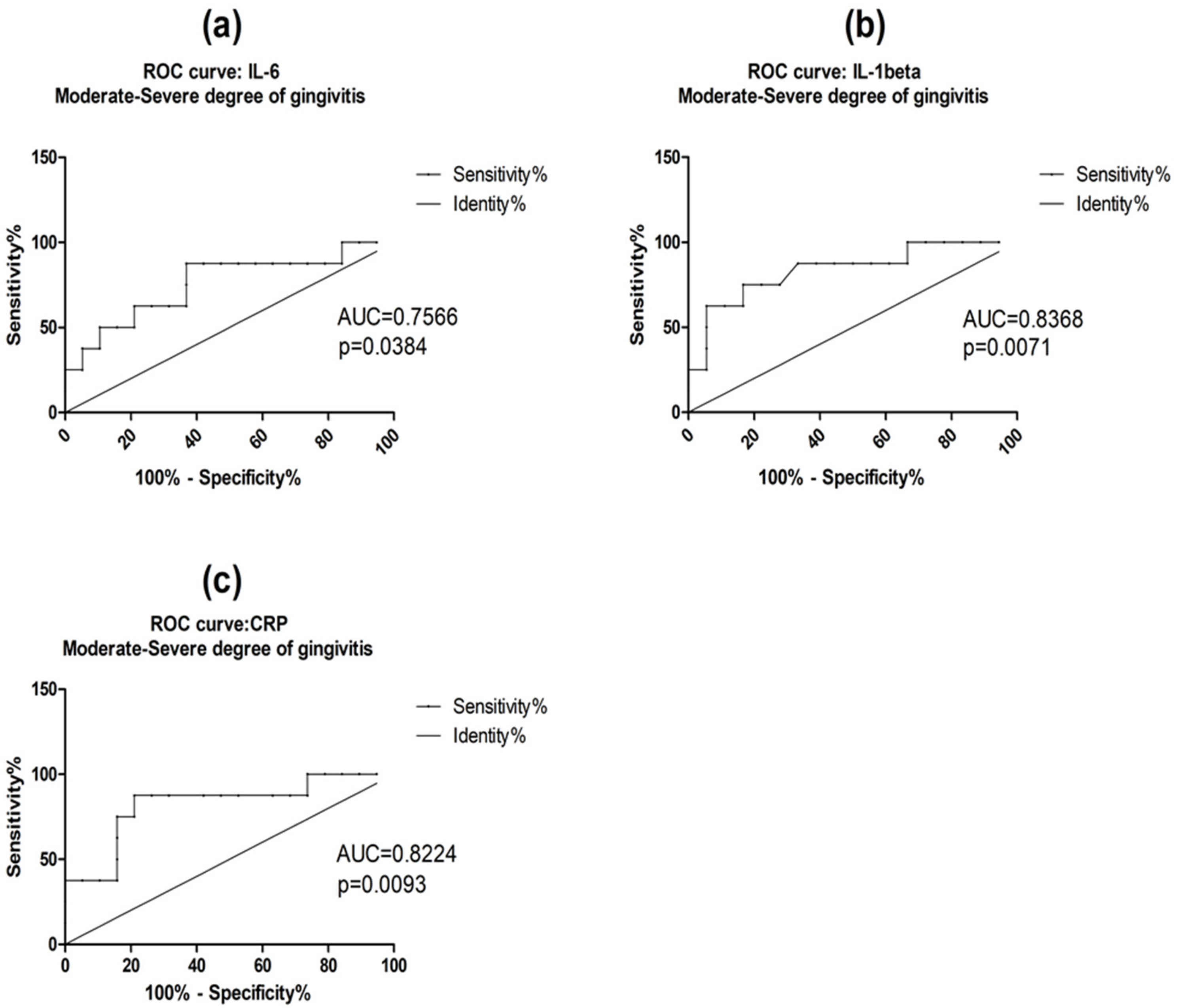
3.3. Diagnostic Accuracy of Salivary IL-6, IL-1β, and CRP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bimstein, E.; Huja, P.E.; Ebersole, J.L. The potential lifespan impact of gingivitis and periodontitis in children. J. Clin. Pediatr. Dent. 2013, 38, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Modéer, T.; Wondimu, B. Periodontal diseases in children and adolescents. Rev. Dent. Clin. N. Am. 2000, 44, 633–658. [Google Scholar] [CrossRef]
- Murakami, S.; Mealey, B.L.; Mariotti, A.; Chapple, I.L.C. Dental plaque-induced gingival conditions. J. Periodontol. 2018, 89, 17–27. [Google Scholar] [CrossRef]
- Ahmadi-Motamayel, F.; Goodarzi, M.T.; Mahdavinezhad, A.; Jamshidi, Z.; Darvishi, M. Salivary and serum antioxidant and oxidative stress markers in dental caries. Caries Res. 2018, 52, 565–569. [Google Scholar] [CrossRef]
- Kaczor-Urbanowicz, K.E.; Trivedi, H.M.; Lima, P.O.; Camargo, P.M.; Giannobile, W.V.; Grogan, T.R.; Gleber-Netto, F.O.; Whiteman, Y.; Li, F.; Lee, H.J.; et al. Salivary exRNA biomarkers to detect gingivitis and monitor disease regression. J. Clin. Periodontol. 2018, 45, 806–817. [Google Scholar] [CrossRef]
- Jenkins, W.M.; Papapanou, P.N. Epidemiology of periodontal disease in children and adolescents. Periodontol. 2000 2001, 26, 16–32. [Google Scholar] [CrossRef]
- Singh, A.K. Prevalence of gingivitis and periodontitis among schools children in Lucknow region of Uttar Pradesh, India. IOSR J. Dent. Med. Sci. 2014, 13, 21–23. [Google Scholar] [CrossRef]
- Bossnjak, A.; Curilovic, Z.; Vuccicevic-Boras, V.; Plancak, D.; Jorgic-Srdjak, K.; Relja, T.; Bozic, D.; Varnica, H. Prevalence of gingivitis in 6- to 11-year-old Croatian children. Eur. J. Med. Res. 2003, 8, 313–317. [Google Scholar]
- Leous, P.; Palianskaya, L.; Leous, L. Oral hygiene and gingival inflammation in 6–8-year-olds from a junior school in Minsk who participated in a supervised oral hygiene programme. Oral Health Dent. Manag. 2009, 7, 27–30. [Google Scholar]
- Burt, B. Research, Science and Therapy Committee of the American Academy of Periodontology. Position paper: Epidemiology of periodontal diseases. J. Periodontol. 2005, 76, 1406–1419. [Google Scholar] [CrossRef]
- Dye, B.A. Global periodontal disease epidemiology. Periodontol. 2000 2012, 58, 10–25. [Google Scholar] [CrossRef] [PubMed]
- Yaghobee, S.; Khorsand, A.; Rasouli Ghohroudi, A.A.; Sanjari, K.; Kadkhodazadeh, M. Assessment of interleukin-1beta and interleukin-6 in the crevicular fluid around healthy implants, implants with peri-implantitis, and healthy teeth: A cross-sectional study. J. Korean Assoc. Oral Maxillofac. Surg. 2014, 40, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Amar, S.; Oyaisu, K.; Li, L.; Van Dyke, T. Moesin: A potential LPS receptor on human monocytes. J. Endotoxin. Res. 2001, 7, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Polizzi, A.; Santonocito, S.; Alibrandi, A.; Williams, R.C. Periodontitis activates the NLRP3 inflammasome in serum and saliva. J. Periodontol. 2022, 93, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Gorska, R.; Gregorek, H.; Kowalski, J.; Laskus-Perendyk, A.; Syczewska, M.; Madaliński, K. Relationship between clinical parameters and cytokine profiles in inflamed gingival tissue and serum samples from patients with chronic periodontitis. J. Clin. Periodontol. 2003, 30, 1046–1052. [Google Scholar] [CrossRef]
- Aurer, A.; Jorgić-Srdjak, K.; Plancak, D.; Stavljenić-Rukavina, A.; Aurer-Kozelj, J. Proinflammatory factors in saliva as possible markers for periodontal disease. Coll. Antropol. 2005, 29, 435–439. [Google Scholar]
- Shojaee, M.; Fereydooni Golpasha, M.; Maliji, G.; Bijani, A.; Aghajanpour Mir, S.M.; Mousavi Kani, S.N. Creactive protein levels in patients with periodontal disease and normal subjects. Int. J. Mol. Cell Med. 2013, 2, 151–155. [Google Scholar]
- Belstrøm, D.; Damgaard, C.; Könönen, E.; Gürsoy, M.; Holmstrup, P.; Gürsoy, U.K. Salivary cytokine levels in early gingival inflammation. J. Oral Microbiol. 2017, 9, 1364101. [Google Scholar] [CrossRef]
- Boronat-Catalá, M.; Catalá-Pizarro, M.; Bagán Sebastián, J.V. Salivary and crevicular fluid interleukins in gingivitis. J. Clin. Exp. Dent. 2014, 2, e175–e179. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kim, K.R.; Kim, H.N. The potential impact of salivary IL-1 on the diagnosis of periodontal disease: A pilot study. Healthcare 2021, 9, 729. [Google Scholar] [CrossRef]
- Rebelo, M.A.; Queiroz, A.C. Gingival Indices: State of Art. In Gingival Diseases—Their Aetiology, Prevention and Treatment; Panagakos, F., Davies, R., Eds.; IntechOpen: Rijeka, Croatia, 2011; pp. 41–54. [Google Scholar] [CrossRef]
- El-Patal, M.A.; Khalil, M.A.; Shipl, W.; Barakat, I.; Youssef, E.M.I.; El Attar, S.; Fathi, A.; Abdallah, A.A. Detection of soluble urokinase type plasminogen activator receptors in children with gingivitis and normal subjects. BMC Oral Health. 2022, 22, 436. [Google Scholar] [CrossRef] [PubMed]
- Nahm, F.S. Receiver operating characteristic curve: Overview and practical use for clinicians. Korean J. Anesthesiol. 2022, 75, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Taylor, J.J.; Preshaw, P.M.; Donaldson, P.T. Cytokine gene polymorphism and immunoregulation in periodontal disease. Periodontol. 2000 2004, 35, 158–182. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Ghaname, C.B.; Braun, T.M.; Sugai, J.V.; Teles, R.P.; Loesche, W.J.; Kornman, K.S.; Giannobile, W.V.; Kinney, J.S. Bacterial and salivary biomarkers predict the gingival inflammatory profile. J. Periodontol. 2012, 83, 79–89. [Google Scholar] [CrossRef]
- Syndergaard, B.; Al-Sabbagh, M.; Kryscio, R.J.; Xi, J.; Ding, X.; Ebersole, J.L.; Miller, C.S. Salivary biomarkers associated with gingivitis and response to therapy. J. Periodontol. 2014, 85, e295–e303. [Google Scholar] [CrossRef]
- Naruishi, K.; Nagata, T. Biological effects of interleukin-6 on Gingival Fibroblasts: Cytokine regulation in periodontitis. J. Cell Physiol. 2018, 233, 6393–6400. [Google Scholar] [CrossRef]
- Volanakis, J.E. Human C-reactive protein: Expression, structure, and function. Mol. Immunol. 2001, 38, 189–197. [Google Scholar] [CrossRef]
- Marsh, P.D.; Moter, A.; Devine, D.A. Dental plaque biofilms: Communities, conflict and control. Periodontol. 2000 2011, 55, 16–35. [Google Scholar] [CrossRef]
- Marsh, P.D. Are dental diseases examples of ecological catastrophes? Microbiology 2003, 149, 279–294. [Google Scholar] [CrossRef]
- Cekici, A.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontol. 2000 2014, 64, 57–80. [Google Scholar] [CrossRef]
- Rathee, M.; Jain, P. Gingivitis; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Garaicoa-Pazmino, C.; Fretwurst, T.; Squarize, C.H.; Berglundh, T.; Giannobile, W.V.; Larsson, L.; Castilho, R.M. Characterization of macrophage polarization in periodontal disease. J. Clin. Periodontol. 2019, 46, 830–839. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Zhao, L.; Huang, X.; Ma, C.; Wang, Y.; Zhang, J.; Xuan, D. Enhanced activity of the macrophage m1/m2 phenotypes and phenotypic switch to m1 in periodontal infection. J. Periodontol. 2016, 87, 1092–1102. [Google Scholar] [CrossRef] [PubMed]
- Martinez, F.O.; Gordon, S. The M1 and M2 paradigm of macrophage activation: Time for reassessment. F1000Prime Rep. 2014, 6, 13. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Sinha, M.; Datta, S.; Abas, M.; Chaffee, S.; Sen, C.K.; Roy, S. Monocyte and macrophage plasticity in tissue repair and regeneration. Am. J. Pathol. 2015, 185, 2596–2606. [Google Scholar] [CrossRef] [PubMed]
- Garlet, G.P.; Giannobile, W.V. Macrophages: The bridge between inflammation resolution and tissue repair? J. Dent. Res. 2018, 97, 1079–1081. [Google Scholar] [CrossRef] [PubMed]
- Young, D.P.; Kushner, I.; Samols, D. Binding of C/EBPbeta to the C-reactive protein (CRP) promoter in Hep3B cells is associated with transcription of CRP mRNA. J. Immunol. 2008, 181, 2420–2427. [Google Scholar] [CrossRef]
- Kida, Y.; Kobayashi, M.; Suzuki, T.; Takeshita, A.; Okamatsu, Y.; Hanazawa, S.; Hasegawa, K. Interleukin-1 stimulates cytokines, prostaglandin E2 and matrix metalloproteinase-1 production via activation of MAPK/AP-1 and NF-kappaB in human gingival fibroblasts. Cytokine 2005, 29, 159–168. [Google Scholar] [CrossRef]
- Sawada, S.; Chosa, N.; Ishisaki, A.; Naruishi, K. Enhancement of gingival inflammation induced by synergism of IL-1β and IL-6. Biomed. Res. 2013, 34, 31–40. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Indicators | Control Group n = 6 | Mild-Degree n = 12 | Moderate-Degree n = 18 | Severe-Degree n = 8 | p Value t-Test |
|---|---|---|---|---|---|
| PLI | 0.74 ± 0.25 | 1.2 ± 0.12 | 1.64 ± 0.29 | 1.98 ± 0.21 | p < 0.05 |
| GI | 0 ± 0 | 0.75 ± 0.24 | 1.38 ± 0.17 | 2.19 ± 0.09 | p < 0.05 |
| Mild–Moderate Degree of Gingivitis AUC (95% CI) | p-Value | Mild–Severe Degree of Gingivitis AUC (95% CI) | p-Value | Moderate–Severe Degree of Gingivitis AUC (95% CI) | p-Value | |
|---|---|---|---|---|---|---|
| IL-6 | 0.6250 | 0.2478 | 0.6354 | 0.3159 | 0.7566 | 0.0384 |
| IL-1β | 0.6620 | 0.1385 | 0.6979 | 0.1427 | 0.8368 | 0.0071 |
| CRP | 0.6272 | 0.2396 | 0.6719 | 0.2031 | 0.8224 | 0.0093 |
| Cut-Off | AUC (95% CI) | Youden Index | Sensitivity% | Specificity% | p-Value | |
|---|---|---|---|---|---|---|
| IL-6 | 8.385 pg/mL | 0.7566 | 0.5066 | 87.50 | 63.16 | 0.0384 |
| IL-1β | 16.99 pg/mL | 0.8368 | 0.5833 | 75.00 | 83.33 | 0.0071 |
| CRP | 223.8 pg/mL | 0.8224 | 0.6645 | 87.50 | 78.95 | 0.0093 |
| Control Group—Mild Degree of Gingivitis AUC (95% CI) | p-Value | Control Group—Moderate Degree of Gingivitis AUC (95% CI) | p-Value | Control Group—Severe Degree of Gingivitis AUC (95% CI) | p-Value | |
|---|---|---|---|---|---|---|
| IL-6 | 0.5139 | 0.9254 | 0.6711 | 0.2148 | 0.7083 | 0.1968 |
| IL-1β | 0.5139 | 0.9254 | 0.6435 | 0.3015 | 0.7083 | 0.1968 |
| CRP | 0.5139 | 0.9254 | 0.6667 | 0.2267 | 0.7083 | 0.1968 |
| Cut-Off | AUC (95% CI) | Youden Index | Sensitivity% | Specificity% | p-Value | |
|---|---|---|---|---|---|---|
| IL-6 | 8.576 pg/mL | 0.7083 | 0.5417 | 87.50 | 66.67 | 0.1968 |
| IL-1β | 16.62 pg/ml | 0.7083 | 0.5833 | 75.00 | 83.33 | 0.1968 |
| CRP | 218.4 pg/ml | 0.7083 | 0.5417 | 87.50 | 66.67 | 0.1968 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salim, A.; Angelova, S.; Roussev, B.; Sokrateva, T.; Kiselova-Kaneva, Y.; Peev, S.; Ivanova, D. Salivary Interleukin-6, Interleukin-1β, and C-Reactive Protein as a Diagnostic Tool for Plaque-Induced Gingivitis in Children. Appl. Sci. 2023, 13, 5046. https://doi.org/10.3390/app13085046
Salim A, Angelova S, Roussev B, Sokrateva T, Kiselova-Kaneva Y, Peev S, Ivanova D. Salivary Interleukin-6, Interleukin-1β, and C-Reactive Protein as a Diagnostic Tool for Plaque-Induced Gingivitis in Children. Applied Sciences. 2023; 13(8):5046. https://doi.org/10.3390/app13085046
Chicago/Turabian StyleSalim, Ayshe, Sirma Angelova, Bogdan Roussev, Todorka Sokrateva, Yoana Kiselova-Kaneva, Stefan Peev, and Diana Ivanova. 2023. "Salivary Interleukin-6, Interleukin-1β, and C-Reactive Protein as a Diagnostic Tool for Plaque-Induced Gingivitis in Children" Applied Sciences 13, no. 8: 5046. https://doi.org/10.3390/app13085046