
Caraway Oil as a Multimodal Therapy for Neuropathic Pain: Investigating the Mechanisms of Action in Rats with Chronic Constriction Injury



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
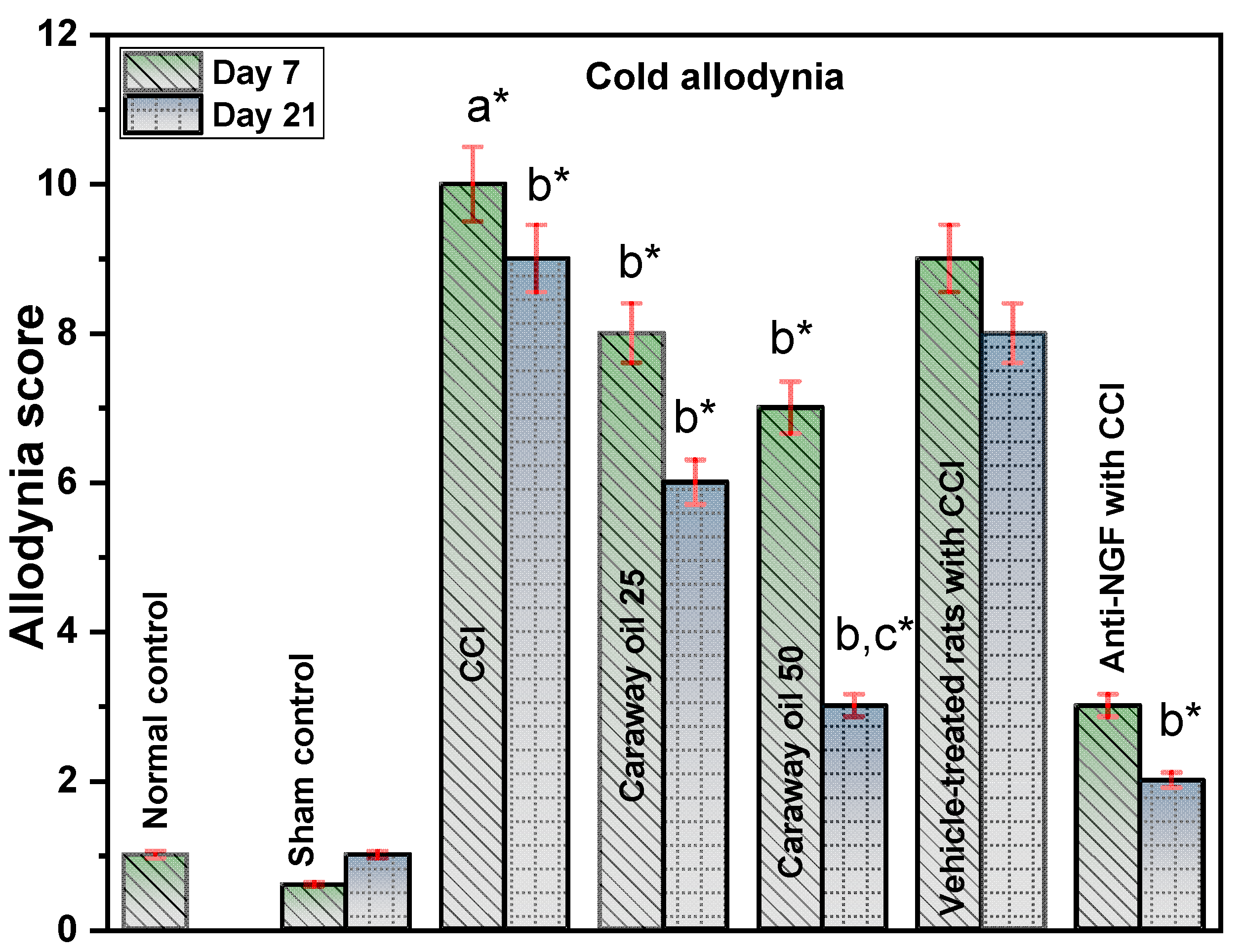
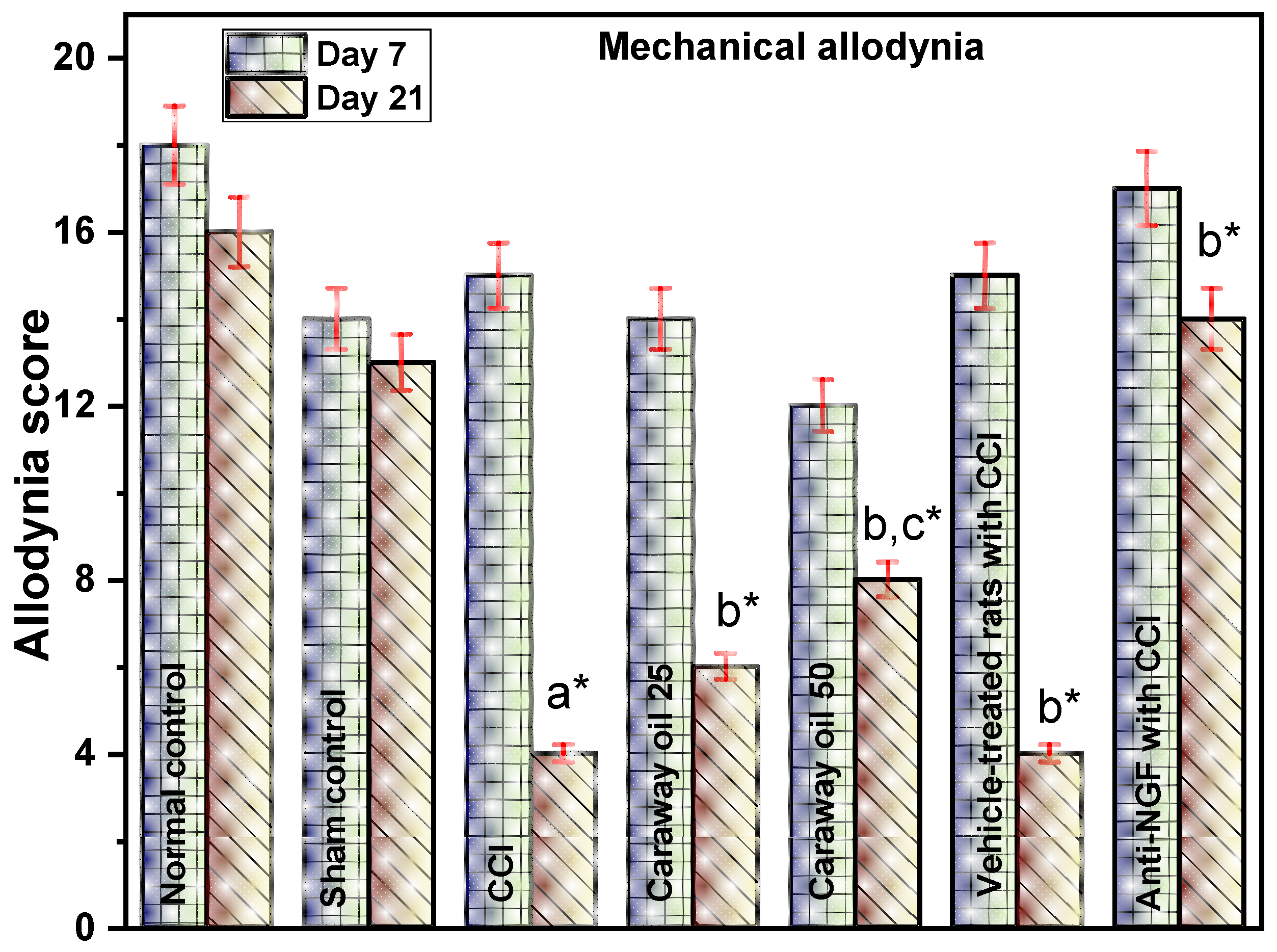
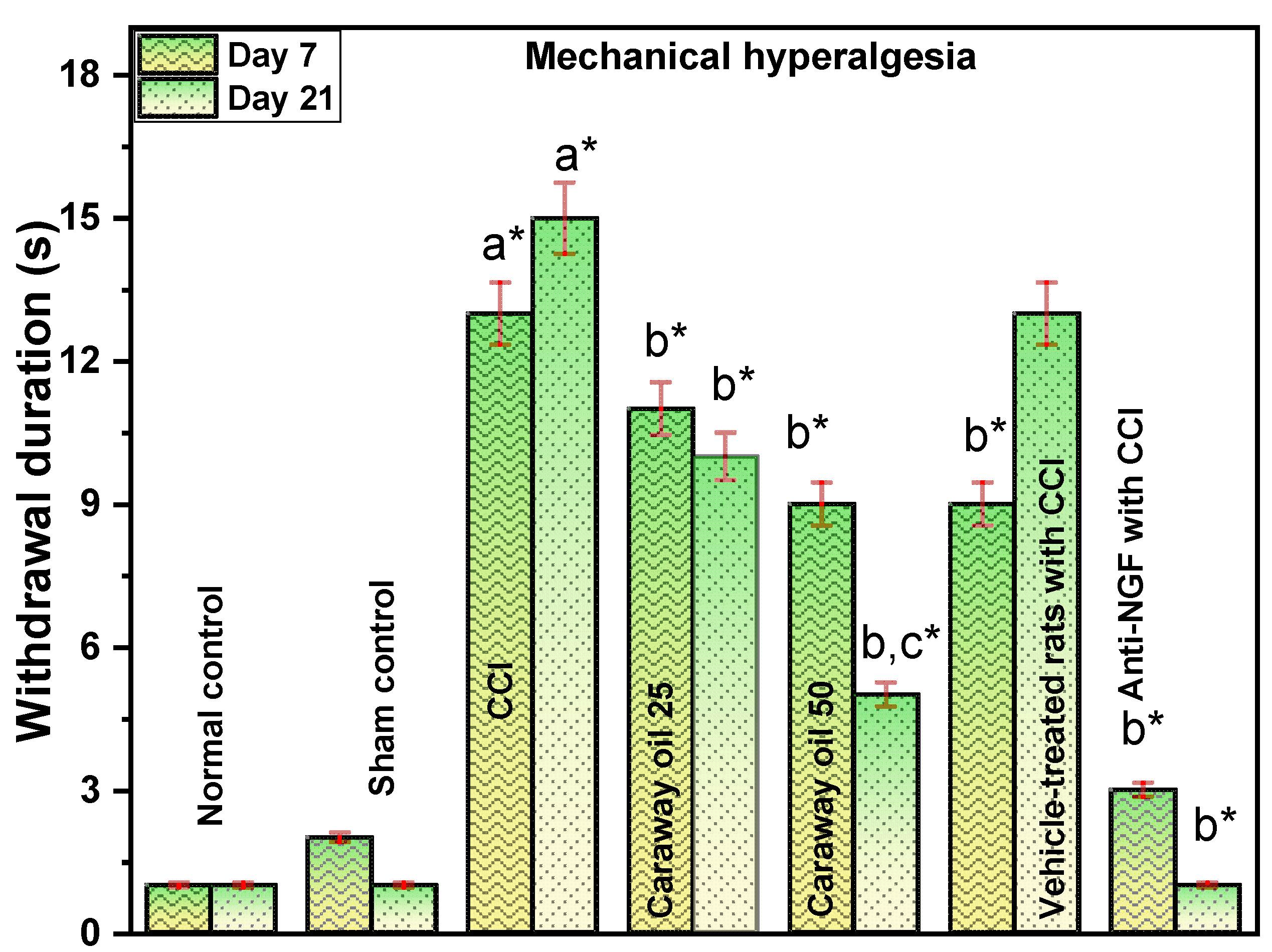
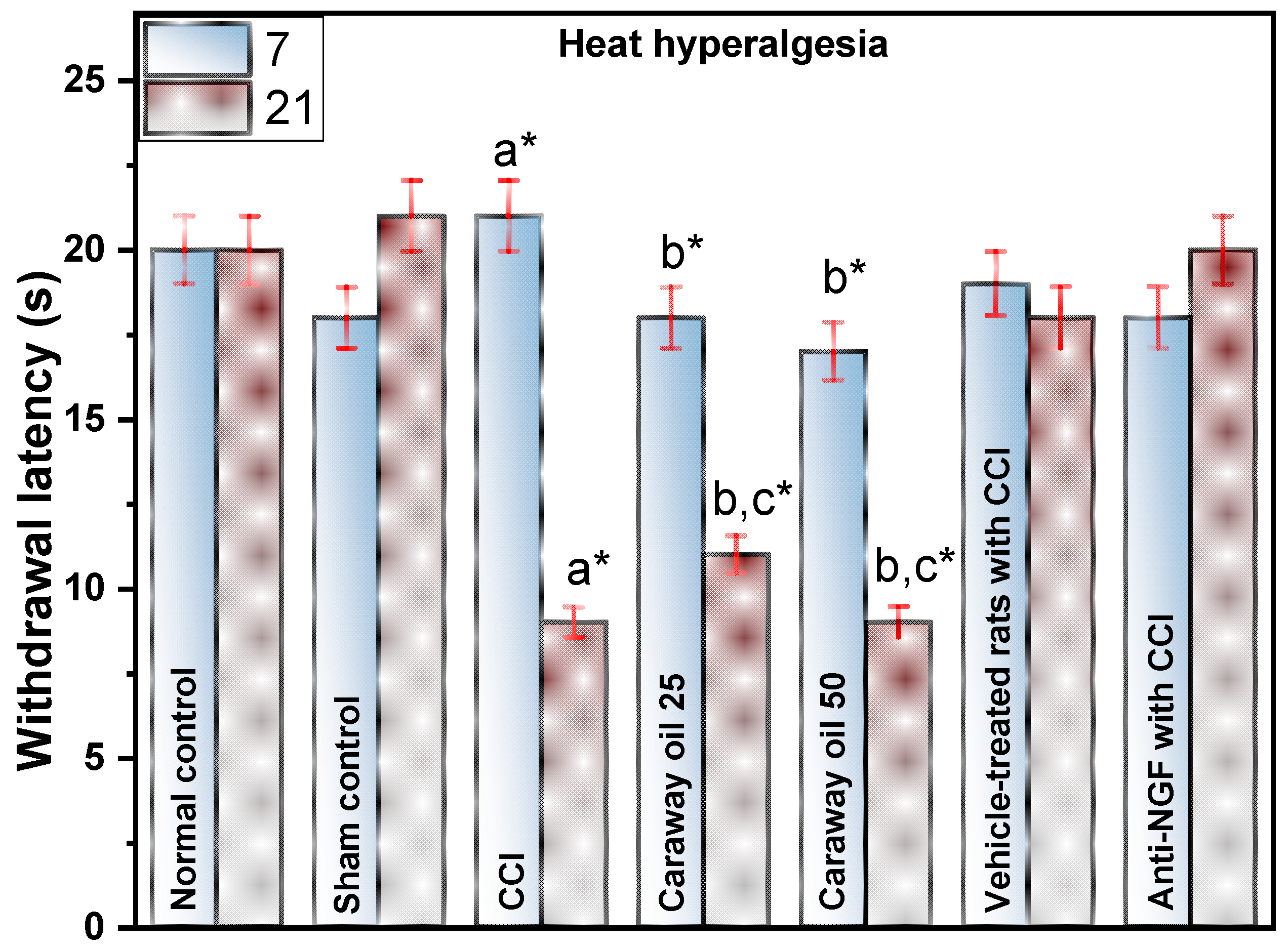
2.1. Effect of Caraway Oil on Hyperalgesia and Allodynia in CCI-Induced Neuropathic Pain
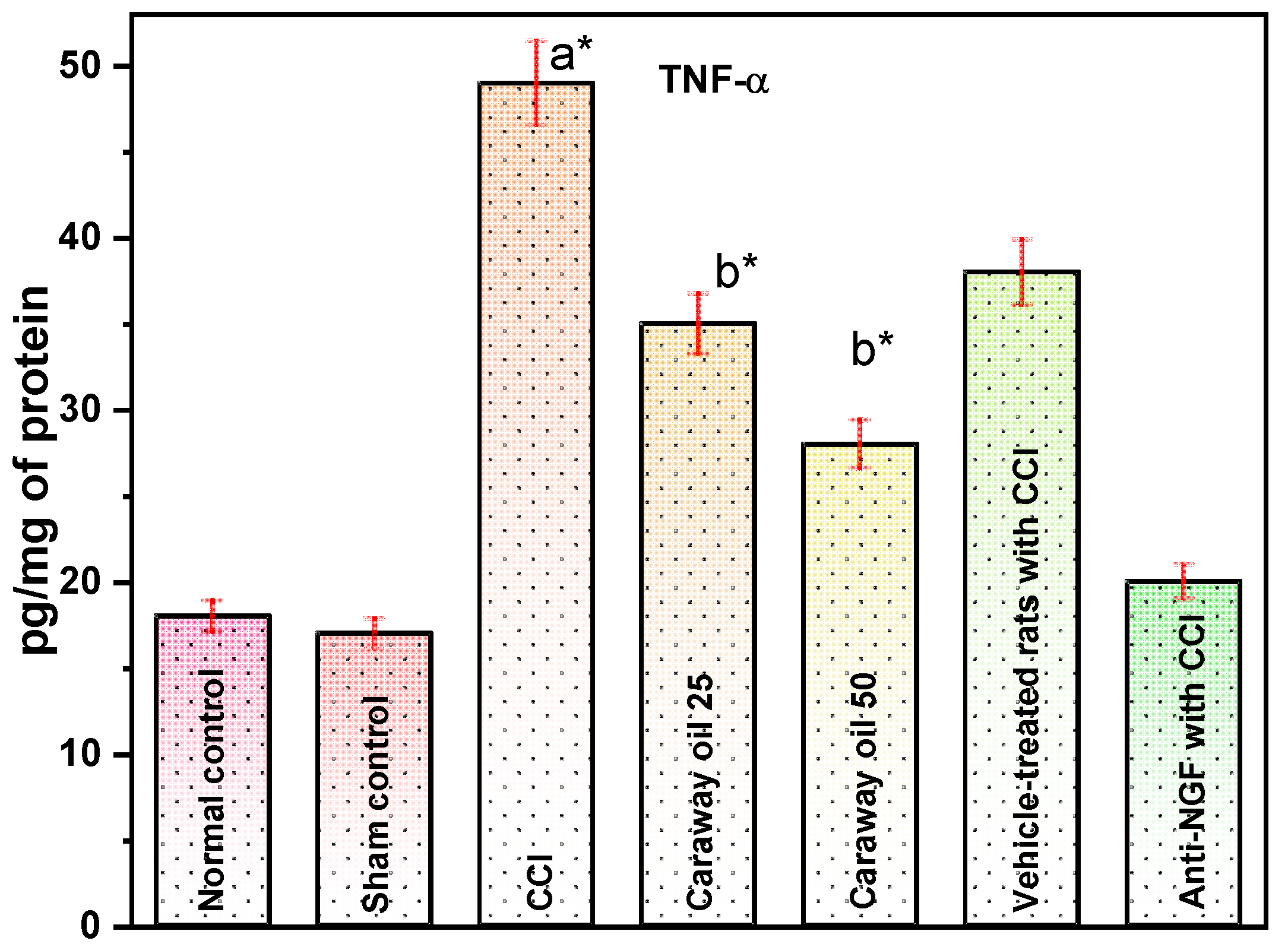
2.2. Effect of Caraway Oil on TNF-α and Total Protein Content in CCI-Induced Neuropathic Pain
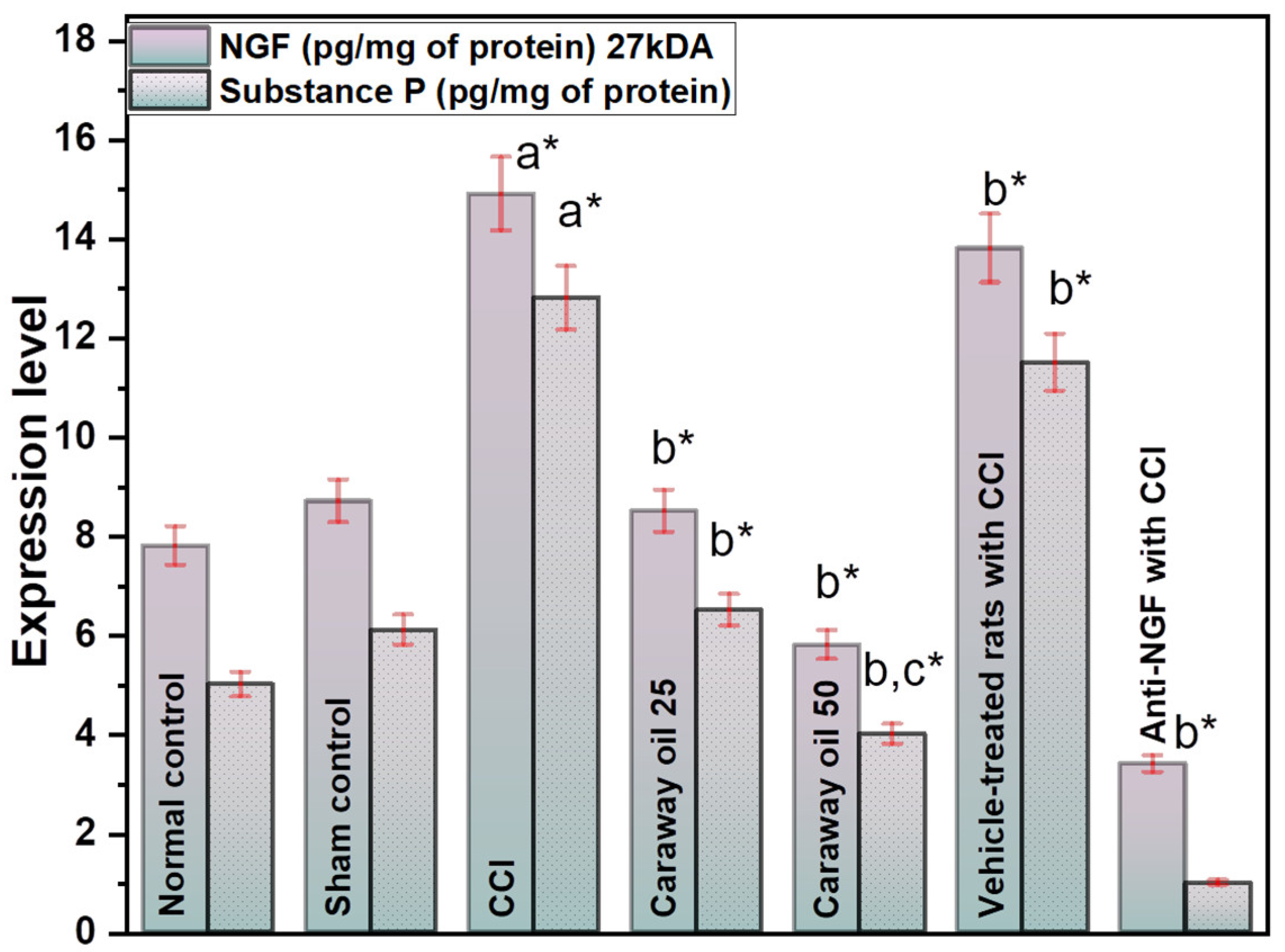
2.3. Effect of Caraway Oil on NGF and Substance P in CCI-Induced Neuropathic Pain
3. Discussion
4. Materials and Methods
4.1. Chemicals
4.2. Experimental Animals
4.3. Induction of Neuropathy by CCI
4.4. Behavioural Studies
4.4.1. Determination of Paw Cold Allodynia (Acetone Sprinkling Test)
4.4.2. Determination of Mechanical Hyperalgesia (Pinprick Test)
4.4.3. Determination of Paw Heat Hyperalgesia (Hot Plate Test)
4.4.4. Determination of Mechanical Allodynia by Von Frey Hair Test
4.5. Biochemical Estimations
4.5.1. Estimation of TNF-α
4.5.2. Estimation of NGF and Substance P
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Descalzi, G.; Mitsi, V.; Purushothaman, I.; Gaspari, S.; Avrampou, K.; Loh, Y.H.E.; Shen, L.; Zachariou, V. Neuropathic pain promotes adaptive changes in gene expression in brain networks involved in stress and depression. Sci. Signal. 2017, 10, eaaj1549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohno, K.; Shirasaka, R.; Yoshihara, K.; Mikuriya, S.; Tanaka, K.; Takanami, K.; Inoue, K.; Sakamoto, H.; Ohkawa, Y.; Masuda, T.; et al. A spinal microglia population involved in remitting and relapsing neuropathic pain. Science 2022, 376, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.H.; Yarnitsky, D.; Freeman, R.; Truini, A.; Attal, N.; Finnerup, N.B.; et al. Neuropathic pain. Nat. Rev. Dis. Prim. 2017, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Foudah, A.I.; Alqarni, M.H.; Devi, S.; Singh, A.; Alam, A.; Alam, P.; Singh, S. Analgesic Action of Catechin on Chronic Constriction Injury–Induced Neuropathic Pain in Sprague–Dawley Rats. Front. Pharmacol. 2022, 13, 895079. [Google Scholar] [CrossRef]
- Gould, H.J.; Gould, T.N.; England, J.D.; Paul, D.; Liu, Z.P.; Levinson, S.R. A possible role for nerve growth factor in the augmentation of sodium channels in models of chronic pain. Brain Res. 2000, 854, 19–29. [Google Scholar] [CrossRef]
- Singh, R.; Rao, H.K.; Singh, T.G. Neuropathic pain in diabetes mellitus: Challenges and future trends. Obes. Med. 2020, 18, 100215. [Google Scholar] [CrossRef]
- Wild, K.D.; Bian, D.; Zhu, D.; Davis, J.; Bannon, A.W.; Zhang, T.J.; Louis, J.C. Antibodies to nerve growth factor reverse established tactile allodynia in rodent models of neuropathic pain without tolerance. J. Pharmacol. Exp. Ther. 2007, 322, 282–287. [Google Scholar] [CrossRef]
- Aloe, L.; Rocco, M.L.; Bianchi, P.; Manni, L. Nerve growth factor: From the early discoveries to the potential clinical use. J. Transl. Med. 2012, 10, 239. [Google Scholar] [CrossRef] [Green Version]
- Watson, J.J.; Allen, S.J.; Dawbarn, D. Targeting Nerve Growth Factor in Pain. BioDrugs 2008, 22, 239. [Google Scholar] [CrossRef]
- Ruiz, G.; Ceballos, D.; Baños, J.E. Behavioral and histological effects of endoneurial administration of nerve growth factor: Possible implications in neuropathic pain. Brain Res. 2004, 1011, 1–6. [Google Scholar] [CrossRef]
- McKelvey, L.; Shorten, G.D.; O’Keeffe, G.W. Nerve growth factor-mediated regulation of pain signalling and proposed new intervention strategies in clinical pain management. J. Neurochem. 2013, 124, 276–289. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.J.; Roth, J.; Ondreka, N.; Kramer, M.; Rummel, C. A potential role for substance p and interleukin-6 in the cerebrospinal fluid of cavalier king charles spaniels with neuropathic pain. J. Vet. Intern. Med. 2013, 27, 530–535. [Google Scholar] [CrossRef] [PubMed]
- Meert, T.F.; Vissers, K.; Geenen, F.; Kontinen, V.K. Functional role of exogenous administration of substance P in chronic constriction injury model of neuropathic pain in gerbils. Pharmacol. Biochem. Behav. 2003, 76, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Colangelo, A.M.; Bianco, M.R.; Vitagliano, L.; Cavaliere, C.; Cirillo, G.; De Gioia, L.; Diana, D.; Colombo, D.; Redaelli, C.; Zaccaro, L.; et al. A new nerve growth factor-mimetic peptide active on neuropathic pain in rats. J. Neurosci. 2008, 28, 2698–2709. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Yang, K.; Zhang, F.; Liu, W.; Wang, Y.; Yu, C.; Wang, J.; Zhang, K.; Zhang, C.; Nenadic, G.; et al. Identification of herbal categories active in pain disorder subtypes by machine learning help reveal novel molecular mechanisms of algesia. Pharmacol. Res. 2020, 156, 104797. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Li, T.; Chen, X.; Zhang, K.; Li, M.; Yao, W.; Zhang, C.; Wan, L. A network-based analysis and experimental validation of traditional Chinese medicine Yuanhu Zhitong Formula in treating neuropathic pain. J. Ethnopharmacol. 2021, 274, 114037. [Google Scholar] [CrossRef]
- Baron, R. Mechanisms of disease: Neuropathic pain—A clinical perspective. Nat. Clin. Pract. Neurol. 2006, 2, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Ji, B.U.; Lee, J.E.; Park, M.Y.; Kim, S.; Kim, S.T.; Koo, S. Inhibitory Effects of Scolopendra Pharmacopuncture on the Development and Maintenance of Neuropathic Pain in Rats: Possible Involvement of Spinal Glial Cells. JAMS J. Acupunct. Meridian. Stud. 2015, 8, 236–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biozid, S.; Alam, M.N.; Abeden, J. Evaluation of Neuropharmacological Effects of Different Chemical Extracts of Flemingia Stricta (Roxb.) Leaves. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Lizarazo, C.I.; Lampi, A.M.; Mäkelä, P.S.A. Can foliar-applied nutrients improve caraway (Carum carvi L.) seed oil composition? Ind. Crops Prod. 2021, 170, 113793. [Google Scholar] [CrossRef]
- Mahboubi, M. Caraway as Important Medicinal Plants in Management of Diseases. Nat. Prod. Bioprospect. 2019, 9, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Goerg, K.J.; Spilker, T. Effect of peppermint oil and caraway oil on gastrointestinal motility in healthy volunteers: A pharmacodynamic study using simultaneous determination of gastric and gall-bladder emptying and orocaecal transit time. Aliment. Pharmacol. Ther. 2003, 17, 445–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, M.S.; Khan, A.U.; Al Kury, L.T.; Shah, F.A. Computational and Pharmacological Evaluation of Carveol for Antidiabetic Potential. Front. Pharmacol. 2020, 11, 919. [Google Scholar] [CrossRef]
- Brenesel, M.D.; Pilija, V.; Popović, T.; Arsić, A.; Milić, M.; Kojić, D.; Milić, N.; Mišan, A. Antihyperlipidemic, antioxidant and weightlowering effects of “vitalplant”. Open Life Sci. 2015, 10, 291–298. [Google Scholar] [CrossRef] [Green Version]
- Grafu, I.A.; Badea, G.; Balaci, T. Synthesis of anticancer vegetable-based lipid nanocarriers. UPB Sci. Bull. Ser. B Chem. Mater. Sci 2015, 77, 247–254. [Google Scholar]
- Shahrajabian, M.H.; Sun, W.; Khoshkharam, M.; Cheng, Q. Caraway, Chinese Chives and Cassia As Functional Foods With Considering Nutrients And Health Benefits. Carpathian J. Food Sci. Technol. 2021, 13, 101–119. [Google Scholar] [CrossRef]
- Gniewosz, M.; Kraśniewska, K.; Woreta, M.; Kosakowska, O. Antimicrobial activity of a pullulan-caraway essential oil coating on reduction of food microorganisms and quality in fresh baby carrot. J. Food Sci. 2013, 78, M1242–M1248. [Google Scholar] [CrossRef]
- Sultan, M.T.; Butt, M.S.; Akhtar, S.; Ahmad, A.N.; Rauf, M.; Saddique, M.S.; Naz, A. Antioxidant and antimicrobial potential of dried cumin (Cuminum cyminum L.), caraway (Carum carvi L.) and turmeric powder (Curcuma longa L.). J. Food Agric. Environ. 2014, 12, 71–76. [Google Scholar]
- Hromiš, N.M.; Lazić, V.L.; Markov, S.L.; Vaštag, Ž.G.; Popović, S.Z.; Šuput, D.Z.; Džinić, N.R. Improvement of antioxidant and antimicrobial activity of chitosan film with caraway and oregano essential oils. Acta Period. Technol. 2014, 45, 33–43. [Google Scholar] [CrossRef]
- Eid, A.M.; Elmarzugi, N.A.; Abu Ayyash, L.M.; Sawafta, M.N.; Daana, H.I. A Review on the Cosmeceutical and External Applications of Nigella sativa. J. Trop. Med. 2017, 2017, 7092514. [Google Scholar] [CrossRef] [Green Version]
- Lacatusu, I.; Badea, G.; Popescu, M.; Bordei, N.; Istrati, D.; Moldovan, L.; Seciu, A.M.; Panteli, M.I.; Rasit, I.; Badea, N. Marigold extract, azelaic acid and black caraway oil into lipid nanocarriers provides a strong anti-inflammatory effect in vivo. Ind. Crops Prod. 2017, 109, 141–150. [Google Scholar] [CrossRef]
- Saini, R.K.; Song, M.H.; Yu, J.W.; Shang, X.; Keum, Y.S. Phytosterol profiling of apiaceae family seeds spices using GC-MS. Foods 2021, 10, 2378. [Google Scholar] [CrossRef] [PubMed]
- Sachan, N.K.; Pushkar, S.; Sachan, A.K.; Ghosh, S.K. Thermal stability and drug-excipient compatibility studies of peppermint and caraway oils for formulation of chewable tablets. Asian J. Chem. 2013, 25, 5930–5934. [Google Scholar] [CrossRef]
- Abo-El Seoud, M.A.; Sarhan, M.M.; Omar, A.E.; Helal, M.M. Biocides formulation of essential oils having antimicrobial activity. Arch. Phytopathol. Plant Prot. 2005, 38, 175–184. [Google Scholar] [CrossRef]
- Kukkar, A.; Singh, N.; Jaggi, A.S. Attenuation of neuropathic pain by sodium butyrate in an experimental model of chronic constriction injury in rats. J. Formos. Med. Assoc. 2014, 113, 921–928. [Google Scholar] [CrossRef] [Green Version]
- Li, J.; Lv, L.; Zhang, J.; Xu, L.; Zeng, E.; Zhang, Z.; Wang, F.; Tang, X. A Combination of Peppermint Oil and Caraway Oil for the Treatment of Functional Dyspepsia: A Systematic Review and Meta-Analysis. Evid. Based Complement. Altern. Med. 2019, 2019, 7654947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komirishetty, P.; Areti, A.; Sistla, R.; Kumar, A. Morin Mitigates Chronic Constriction Injury (CCI)-Induced Peripheral Neuropathy by Inhibiting Oxidative Stress Induced PARP Over-Activation and Neuroinflammation. Neurochem. Res. 2016, 41, 2029–2042. [Google Scholar] [CrossRef]
- Minnone, G.; De Benedetti, F.; Bracci-Laudiero, L. NGF and Its Receptors in the Regulation of Inflammatory Response. Int. J. Mol. Sci 2017, 18, 51028. [Google Scholar] [CrossRef] [Green Version]
- Keshavarz, A.; Minaiyan, M.; Ghannadi, A.; Mahzouni, P. Effects of Carum carvi L. (Caraway) extract and essential oil on TNBS-induced colitis in rats. Res. Pharm. Sci. 2013, 8, 1–8. [Google Scholar]
- Hökfelt, T.; Pernow, B.; Wahren, J. Substance P: A pioneer amongst neuropeptides. J. Intern. Med. 2001, 249, 27–40. [Google Scholar] [CrossRef]
- Krause, J.E.; DiMaggio, D.A.; McCarson, K.E. Alterations in neurokinin 1 receptor gene expression in models of pain and inflammation. Proc. Can. J. Physiol. Pharmacol. 1995, 73, 854–859. [Google Scholar] [CrossRef]
- De Vry, J.; Kuhl, E.; Franken-Kunkel, P.; Eckel, G. Pharmacological characterization of the chronic constriction injury model of neuropathic pain. Eur. J. Pharmacol. 2004, 491, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Flatters, S.J.L.; Bennett, G.J. Ethosuximide reverses paclitaxel- and vincristine-induced painful peripheral neuropathy. Pain 2004, 109, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Erichsen, H.K.; Blackburn-Munro, G. Pharmacological characterisation of the spared nerve injury model of neuropathic pain. Pain 2002, 98, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Nomura, E.C.O.; Rodrigues, M.R.A.; Da Silva, C.F.; Hamm, L.A.; Nascimento, A.M.; De Souza, L.M.; Cipriani, T.R.; Baggio, C.H.; De Paula Werner, M.F. Antinociceptive effects of ethanolic extract from the flowers of Acmella oleracea (L.) R.K. Jansen in mice. J. Ethnopharmacol. 2013, 150, 583–589. [Google Scholar] [CrossRef]
- Hijazi, M.A.; El-Mallah, A.; Aboul-Ela, M.; Ellakany, A. Evaluation of Analgesic Activity of Papaver libanoticum Extract in Mice: Involvement of Opioids Receptors. Evid. Based Complement. Alternat. Med. 2017, 2017, 8935085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaplan, S.R.; Bach, F.W.; Pogrel, J.W.; Chung, J.M.; Yaksh, T.L. Quantitative assessment of tactile allodynia in the rat paw. J. Neurosci. Methods 1994, 53, 55–63. [Google Scholar] [CrossRef]
- Lowry, O.; Schagger, H.; Cramer, W.A.; Vonjagow, G. Protein measurement with the folin phenol reagent. Anal. Biochem. 1994, 217, 265–275. [Google Scholar] [CrossRef]
- Singh, T.G. Comparison of efficacy and safety of pregabalin and duloxetine in patients with diabetic neuropathic pain: A double-blind clinical study. Int. J. Green Pharm 2019, 13, 398–403. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alkholifi, F.K.; Devi, S.; Alam, A.; Kamal, M.; Yusufoglu, H.S. Caraway Oil as a Multimodal Therapy for Neuropathic Pain: Investigating the Mechanisms of Action in Rats with Chronic Constriction Injury. Appl. Sci. 2023, 13, 2989. https://doi.org/10.3390/app13052989
Alkholifi FK, Devi S, Alam A, Kamal M, Yusufoglu HS. Caraway Oil as a Multimodal Therapy for Neuropathic Pain: Investigating the Mechanisms of Action in Rats with Chronic Constriction Injury. Applied Sciences. 2023; 13(5):2989. https://doi.org/10.3390/app13052989
Chicago/Turabian StyleAlkholifi, Faisal K., Sushma Devi, Aftab Alam, Mehnaz Kamal, and Hasan S. Yusufoglu. 2023. "Caraway Oil as a Multimodal Therapy for Neuropathic Pain: Investigating the Mechanisms of Action in Rats with Chronic Constriction Injury" Applied Sciences 13, no. 5: 2989. https://doi.org/10.3390/app13052989