

A Meta-Analysis on Dual Protocols for Chronic Stroke Motor Recovery: Robotic Training and tDCS

1
Division of Sport Science, Health Promotion Center, Sport Science Institute, Incheon National University, Incheon 22012, Republic of Korea
2
Department of Applied Physiology and Kinesiology, University of Florida, Gainesville, FL 32611, USA
*
Author to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Appl. Sci. 2023, 13(3), 1992; https://doi.org/10.3390/app13031992
Submission received: 24 November 2022
/
Revised: 9 January 2023
/
Accepted: 30 January 2023
/
Published: 3 February 2023
(This article belongs to the Special Issue New Trends in Biosciences III)
Abstract
:Two popular chronic stroke rehabilitation protocols are robotic-assisted movements and transcranial direct current stimulation (tDCS). Separately, both protocols have produced encouraging motor recovery improvements. An intriguing question remains: what happens to motor recovery when both protocols are administered together? Do the two protocols together produce additive dual effects? This systematic review and meta-analysis investigated the dual effect of combining robotic training and tDCS. We investigated the potential effects of tDCS protocols in addition to robotic-training programs on motor recovery of the upper and lower extremities post-stroke. A systematic literature search identified 20 qualified studies that used robotic training combined with tDCS protocols for upper limb (i.e., 15 studies) and lower limb (i.e., 5 studies) post-stroke rehabilitation. Individuals in the subacute and chronic stages of recovery were investigated. The 20 included studies compared additive effects of the combined protocols with robotic training sham control groups. Further, we estimated short-term and long-term treatment effects of the combined protocols. The random-effects model meta-analyses failed to find any significant short-term and long-term motor improvements in the upper extremities after the combined treatments. However, robotic-assisted movements combined with tDCS protocols revealed significant moderate transient and sustained improvements in functions of the lower limbs post-stroke. These meta-analytic findings suggest clinical implications concerning coupled top-down and bottom-up training protocols (i.e., robotic training and tDCS combined), which will allow us to make progress toward post-stroke motor recovery.
1. Introduction
Stroke is the leading cause of motor impairments worldwide [1]. Unfortunately, many individuals post-stroke continue to struggle with executing movements, as dysfunctional motor actions in both the upper and lower extremities adversely affect activities of daily living [2,3]. Thus, overcoming these motor problems has become the focus of multiple stroke researchers and therapists as they seek answers to efficacy, effectiveness, intensity, duration, and unilateral/bilateral treatment protocols. Importantly, stroke rehabilitation programs that have a sound basis in neurophysiological and motor learning theories are helping to overcome motor impairments [4,5,6].
Convincing neural plasticity evidence shows that individuals post-stroke are able to improve motor deficits while re-acquiring their capability to will goal-directed movements [7,8,9]. Triggering neural plasticity in the damaged motor cortex regions involves the problem of volition [10,11]. That is, activating appropriate brain areas for the purpose of initiating, controlling, and stopping motor actions requires that we learn and control our movements on command. Moreover, facilitating neural plasticity across targeted brain areas may be accomplished by administering rehabilitation focused on (a) a top-down protocol: brain stimulation affecting the central nervous system; (b) a bottom-up protocol: functional electrical stimulation or specific movements influencing the peripheral nervous system; or (c) combining the two novel stroke treatment protocols [12,13].
Two promising post-stroke treatment protocols are transcranial direct stimulation (tDCS) and robotic-assisted movements [14,15]. Non-invasive brain stimulation protocols such as tDCS have become popular treatments for post-stroke motor rehabilitation [16,17]. Many tDCS studies have focused on stimulating the primary motor cortex (M1), which is located in the dorsal region of the frontal lobe and is related to controlling the motor system [14,16]. Attaching tDCS surface electrodes to the M1 region of the ipsilesional hemisphere and applying a weak electrical current (0.5–2 mA) to the area continuously for 10–30 min routinely induces changes in cortical excitability that may persist for nearly 60 min [18,19]. Presumably, anodal stimulation increases cortical excitability whereas cathodal stimulation decreases excitability [20]. Frequently, when tDCS is provided before or during (i.e., offline or online) traditional stroke rehabilitation programs, motor actions are re-acquired more quickly in comparison to tDCS alone [21,22]. This favorable evidence is reported with fixed and variable stimulation techniques as well as various stimulation intensities. Moreover, these positive effects on motor recovery were found in both the upper and lower extremities during two retention tests: immediate (1 week after treatment) and delayed (24 weeks after treatment). Thus, the potential short-term and long-term benefits of tDCS on individuals post-stroke may address each of the three common stroke stages (i.e., acute, subacute, and chronic) [14,23]. Granted, some researchers argue that standardizing tDCS electrode placement, stimulation intensity, and treatment duration would be ideal for stroke patients and rehabilitation therapists [24,25]. Regardless, diverse tDCS and stroke motor recovery studies continue to report beneficial effects.
A second stroke rehabilitation protocol that has recently become popular is robotic-assisted movement [26,27]. Essentially, impaired limbs are moved through a range of movements programmed for specific joints. Robot assistance has been applied to both upper and lower extremities with encouraging results [28,29]. One critical advantage of this rehabilitation protocol is that a high number of repetitions can be completed in every training session [30]. Increasing the number of assisted movements and the consistency in the motor actions generally produce improved paretic limb performances as well as an increased range of functional motions [30,31,32]. Taken together, the accumulated quantitative data from several prior meta-analysis studies indicated that robot-assisted therapy effectively improved motor control capabilities, muscle strength, and gait/balance functions post-stroke [29,33,34]. Further, some researchers suggested that robotic-assisted movements combined with additional rehabilitation protocols (e.g., physiotherapy or body-weight support training) may increase motor improvements beyond the effects of robotic training alone [29,35].
Given the elusive nature of effective and efficient stroke motor recovery protocols, researchers have begun combining two novel approaches for the purpose of optimizing rehabilitation effects on paretic limbs [36,37]. Indeed, providing tDCS before or during robotic treatments has high learning potential for recovering treated motor actions. Augmenting robotic training with tDCS appears to activate favorable movement action re-acquisition conditions in the primary motor cortex and the supplementary motor area [38,39]. That is, priming the motor system while performing an extended set of repetitive robotic-assisted movements has been embraced in the rehabilitation arena. Indeed, prior studies have reported that tDCS priming facilitated motor improvements in individuals post-stroke when this technique was employed with high intensity and task-specific motor training designed to activate neuroplasticity and motor learning [40,41].
However, two recent systematic review and meta-analysis studies reported insufficient evidence regarding the beneficial combined effects of tDCS and robotic training on stroke motor rehabilitation [42,43]. Importantly, these findings were limited to functional recovery of the upper extremities, with a relatively small number of analyzed studies. A third meta-analysis study followed different inclusion criteria and found slightly expanded potential effects of robotic-assisted movements combined with tDCS by demonstrating moderate positive effects in the lower extremities post-stroke [44]. Moreover, these three sets of meta-analytic findings predominantly focused on transient performance effects (i.e., short-term retention) of the combined training protocols.
Considering the conflicting findings and limited number of comparisons in the previous meta-analyses, a convincing answer to the question regarding the additive effects of combining robotic-assisted movements and tDCS as stroke rehabilitation protocols is missing. Further, determining whether functional recovery of the upper and lower limbs improves after delayed retention testing is still unknown. Thus, combining two effective individual rehabilitation protocols and simultaneously administering both of them is a novel approach to minimizing long-term motor dysfunctions post-stroke [45,46]. Given the increased number of publications reporting the separate effects of tDCS and robotic training, a question arises concerning the additive effect of dual protocols. Thus, our purpose was to conduct a systematic review and meta-analysis to determine the overall effects of the two augmented protocols [36,47] on post-stroke motor recovery in the upper and lower extremities.
2. Materials and Methods
2.1. Review Inclusion Criteria
Primary sources and peer-reviewed articles that examined the effects of tDCS combined with robotic training on either upper or lower motor functions in patients with stroke were eligible for inclusion in this systematic review and meta-analysis. Qualifying studies were selected according to the PICO criteria [48] shown in Table 1.
2.2. Search Strategy and Study Selection
The Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines [49,50] served as the basis for this study. Our search of the literature identified potential studies that investigated the effects of robotic training combined with tDCS protocols on motor functions of upper and lower extremities post-stroke. We searched the literature from 1 September 2022 to 15 November 2022, and the publication date of the potential articles was not limited. Keyword inputs based on Boolean logic for searching included: (stroke OR brain infarction OR cerebrovascular disease) AND (tDCS OR transcranial direct current stimulation) AND (robot OR robotic OR robot-assisted). We used constant keyword inputs and the same search procedure for three search engines: (1) PubMed, (2) Web of Science, and (3) Cochrane Database of Systematic Reviews. We considered all types of publications (e.g., journal articles, conference abstracts, dissertations) for this meta-analysis.
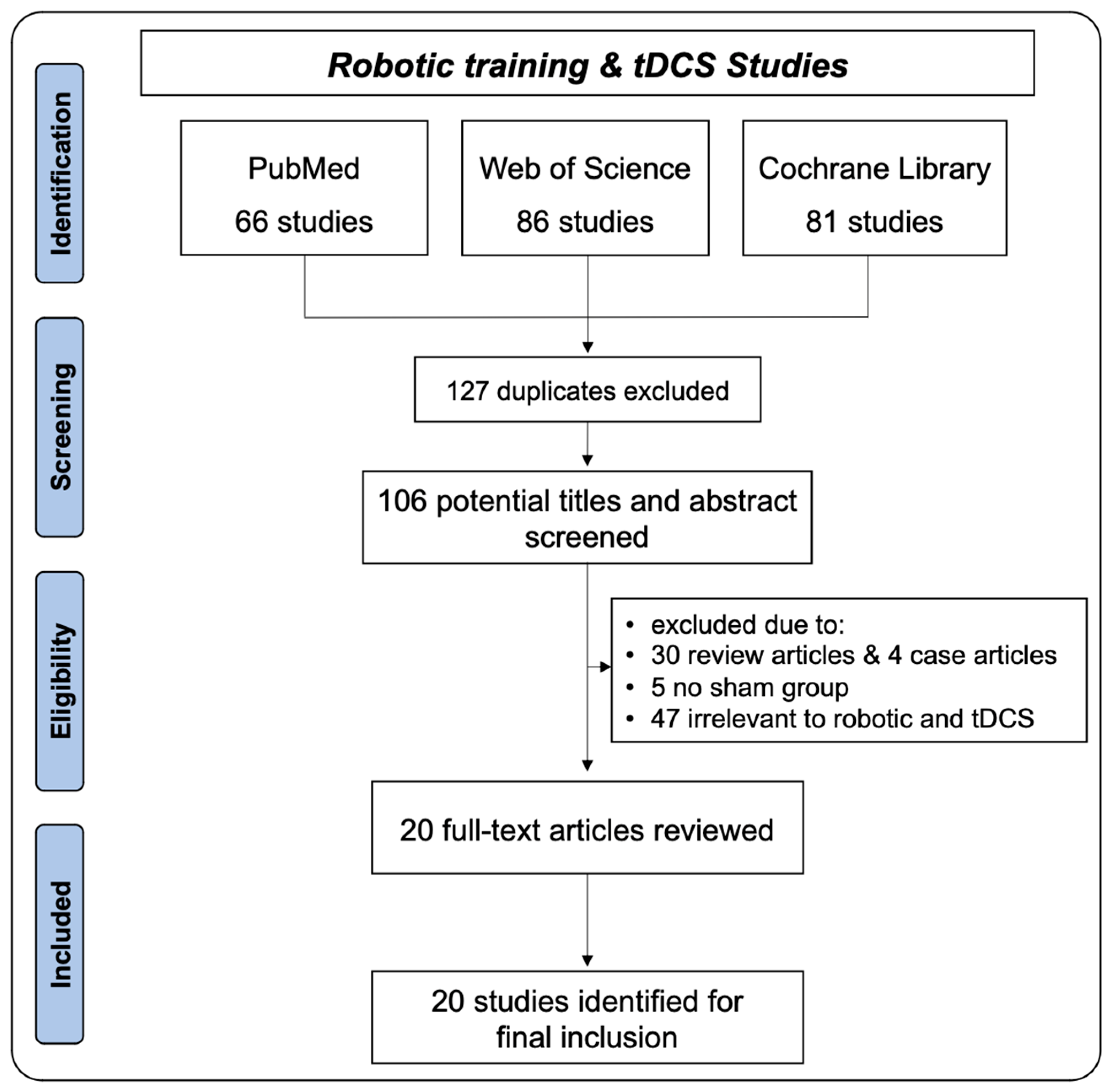
Initially, we identified 233 potential studies with 66 articles from PubMed, 86 from Web of Science, and 81 from the Cochrane Database of Systematic Reviews. After removing 127 duplicate studies, we closely read 106 articles. Based on the PICO criteria, we excluded 86 studies (i.e., 30 review articles, 4 case study articles, 5 studies with no sham control group, and 47 studies irrelevant to the current topic). Thus, 20 studies qualified for inclusion in our meta-analysis [37,45,46,47,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66]. The specific study identification procedures are shown in our PRISMA flow chart (Figure 1).
2.3. Types of Studies Included
Fifteen studies examined changes in the upper limb motor functions of patients with stroke after combined protocols of tDCS and robotic training (Table 2). In addition, five included studies reported altered lower limb functions in individuals post-stroke after undergoing the two combined protocols. The twenty total qualifying studies consisted of fifteen RCT studies, three crossover design studies, and two non-RCT studies.
2.4. Types of Participants
The 20 qualifying studies focused on the effects of robotic training combined with tDCS protocols on motor functions in 574 patients with stroke (range of mean time since stroke onset = 0.8–152.5 months). Fourteen studies investigated chronic stroke and six studies focused on individuals in the post-stroke subacute phase (i.e., four subacute studies and two subacute and chronic studies). Table 2 displays the demographic information of all of the participants.
2.5. Types of Interventions and Control
The 15 included studies that focused on rehabilitating the upper extremities post-stroke used two robotic-training protocols: (a) motor imagery brain–computer interface (MI-BCI) (six studies) and (b) robot-assisted therapies (nine studies) (e.g., robotic devices on the wrists and arms). Nine out of the fifteen upper limb studies used unilateral tDCS protocols (i.e., anodal tDCS on the ipsilesional hand area within the M1), whereas six studies applied bilateral tDCS protocols (i.e., anodal tDCS on ipsilesional hand area within the M1 and cathodal tDCS on contralesional hand area within the M1). In total, 12 studies administered multiple sessions of robotic training combined with tDCS protocols (e.g., 10–36 sessions), and only 3 studies used a single session of the combined rehabilitation protocols.
Concerning the robotic devices, fourteen studies applied end-effector type devices and only one study used an exoskeleton-type device. Moreover, five specific types of joint movements were initiated during the robotic training: (a) unilateral finger: one study, (b) unilateral hand and wrist: four studies, (c) unilateral shoulder and elbow: seven studies, (d) unilateral whole arm: two studies, and (e) bilateral wrists and hands: one study.
The comparison control groups in the upper limb rehabilitation studies varied by two types: (a) nine studies provided robotic training with a sham tDCS condition; and (b) six studies administered only robotic training. All of the control groups experienced the same number of robotic training sessions as the combined-protocols treatment groups (Table S1).
Post-stroke rehabilitation for the lower limbs consisted of robot-assisted gait training (four studies) and robotic gait orthosis on the impaired lower extremities (one study). Using anodal tDCS, four studies stimulated the leg area within the M1, located close to the midline, whereas one study used unilateral anodal tDCS on the ipsilesional hand area within the M1. These studies administered multiple sessions of the combined training protocols (e.g., 10–20 sessions). In addition, for lower limb rehabilitation, two studies with end-effector, two studies with exoskeleton, and one study with end-effector/exoskeleton robot device characteristics were included. Note that each of the five studies trained bilateral whole leg movements. For the controls, during lower limb rehabilitation periods, three studies provided robotic training with sham tDCS condition whereas two studies administered only robotic training. All studies used the same number of training sessions and robotic training protocols as the combined protocol treatment groups (Table S1). Table 3 shows the specific details of the tDCS intervention protocols.
2.6. Outcome Measures
We determined the short-term and long-term effects of robotic training combined with tDCS protocols on the motor capabilities of both the upper and lower extremities of individuals post-stroke. The short-term effects were considered transient performance changes in motor functions and were evaluated by immediate post-testing administered less than 24 h after the final treatment session. In contrast, the long-term effects represented relatively sustained changes in motor functions evaluated by delayed post-testing administered more than 2 weeks after the final combined tDCS and robotic intervention session.
Fifteen out of the twenty qualified studies reported primary outcome measures on motor function recovery of the upper limbs. Specific details on the primary upper limb motor function outcome measures from each study were evaluated by: (a) Fugl-Meyer assessment on upper extremity (FMA-UE): 12 studies; (b) straightness during a reaching task: one study; (c) movement aiming task: one study; and (d) average performance during a 3D reaching task: one study.
We identified 20 total short-term effect comparisons from the 15 included studies, (a) single comparisons from 12 studies and (b) multiple comparisons from 3 studies, based on different tDCS timings (i.e., before, during, and after), montages (i.e., anodal and cathodal stimulation), and bimanual tasks (speed/accuracy trade-off, coordination, and force). Nine out of the fifteen included studies reported ten long-term effect comparisons, (a) single comparison from eight studies and (b) two comparisons from one study, based on different tDCS montages (i.e., anodal and cathodal stimulation).
Five out of the twenty qualified studies revealed changes in the lower limb motor functions after the combined tDCS and robotic training protocols. The primary lower limb motor function outcome measures were: (a) 10 m walk test (10 MWT): two studies; (b) 6 min walk test (6 MWT): two studies; and (c) functional ambulation category (FAC): one study. The lower limb studies reported five short-term effect comparisons and four long-term effect comparisons.
Given that one study administered retention tests in two different periods (i.e., two and four weeks after the final intervention session), selecting one of two different time points may cause either overestimated or underestimated meta-analytic findings. To minimize the issue of multiple comparisons [49], we statistically combined two effect sizes into one comparison via a procedure that used the mean of the selected outcomes.
2.7. Methodological Quality
Three researchers (RK, ZD, and NK) independently conducted methodological quality assessments on the 20 qualified studies using the Physiotherapy Evidence Database (PEDro) rating scale [67]. The PEDro scale for estimating study quality included a checklist of 11 items scored yes or no regarding group allocation, blinding, attrition, statistical analyses, and data variability. A fourth researcher (JHC) additionally graded and confirmed final scores when any discrepancies in rating scores across the three researchers appeared. The range of PEDro scores from the 20 studies was 7 to 11 (mean PEDro score = 9.15). Based on previous studies [68,69], these findings indicate a relatively high methodological quality in this meta-analysis: (1) excellent: 9–10, (2) good: 6–8, (3) fair: 4–5, and (4) poor: below 4. Table 4 shows specific details on all PEDro scores of each domain.
2.8. Data Extraction
Based on the recommendations of classical meta-analysis procedures by Borenstein and colleagues, we performed data extraction [49]. To calculate individual effect size for each qualified study that used either RCT or non-RCT design, we extracted one of three data formats: (a) mean and SD values between treatment and control groups, (b) mean values between treatment and control groups with p-values indicating between-group differences, and (c) sample size values between treatment and control groups with p-value indicating between-group differences. For studies that used a crossover design, we extracted a sample size value between paired groups (i.e., treatment and control conditions) with p-values indicating within-group differences. Specific data formats for the included studies are shown in Table S2.
2.9. Data Synthesis
We conducted all meta-analysis procedures using the Comprehensive Meta-Analysis software (ver. 3.3, Englewood, NJ, USA). To quantify overall and individual effect sizes, we calculated the standardized mean difference (SMD) with 95% confidence intervals (CIs) [49]. The meta-analysis on upper limb motor function included 20 short-term effect comparisons and 10 long-term effect comparisons, whereas the analysis on lower limb motor function used 5 short-term effect comparisons and 4 long-term effect comparisons. Positive SMD values indicated greater positive effects on motor improvements in the augmented active tDCS and robotic training protocol groups than in the sham control groups. We conducted random-effects meta-analysis models to account for different participants, interventions, outcome measures, or statistical methods used in the individual included studies [49]. The level of heterogeneity was estimated by Higgins and Green’s I2 [70]. Publication bias was assessed by two approaches: (a) comparing original and revised funnel plots after the trim-and-fill technique [71] and (b) Egger’s regression test [72]. Finally, we performed two moderator variable analyses to determine whether treatment effects were different, according to (a) study designs: randomized controlled trials (RCT) versus crossover versus non-RCT; or (b) recovery phase post-stroke: subacute versus chronic versus subacute and chronic.
3. Results
3.1. Upper Limb Motor Functions: Short-Term Effects
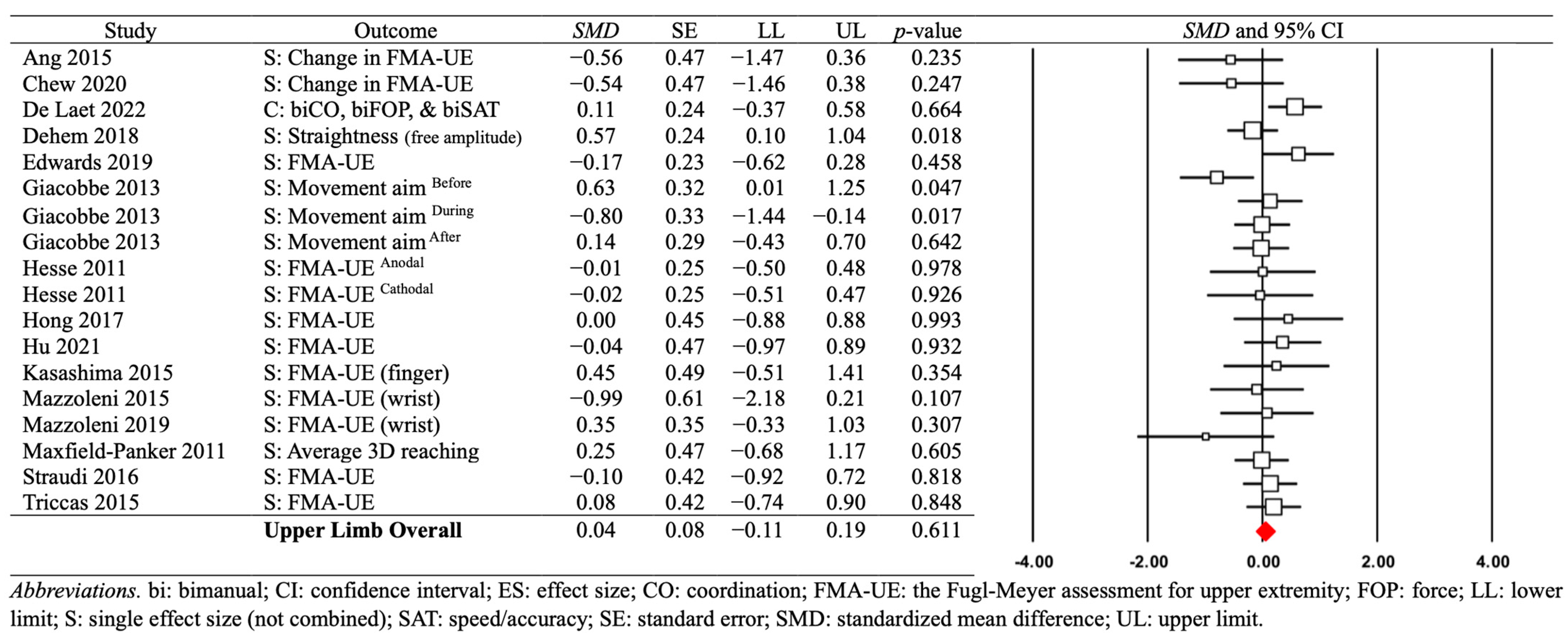
A random-effects model meta-analysis on the 20 comparisons revealed no significant short-term effects of combined tDCS and robotic training protocols on motor capabilities of the upper limbs post-stroke: SMD = 0.041; SE = 0.082; variance = 0.007; 95% CI = −0.120–0.202; Z = 0.504; p = 0.614 (see Figure 2). Heterogeneity tests indicated a relatively low variability across the individual effect sizes: (a) Q-value = 24.082 with p = 0.193; and (b) I2 = 21.104%. Further, the publication bias assessments showed minimal asymmetry levels of individual effect sizes: (a) a revised funnel plot with four imputed values after applying the trim and fill technique (see Figure S1) and (b) Egger’s regression test: β0 = −1.095 and p = 0.220. These findings indicate that robot training combined with tDCS showed no significant transient effects on the rehabilitation of the upper limbs post-stroke.
3.2. Moderator Variable Analysis: Study Designs and Recovery Phase
The first moderator variable analysis showed no significant short-term effects across different study designs: (a) 12 RCT comparisons from 11 studies (SMD = −0.079; SE = 0.102; variance = 0.010; 95% CI = −0.279–0.121; Z = −0.773; p = 0.439); (b) 7 crossover comparisons from 3 studies (SMD = 0.141; SE = 0.155; variance = 0.024; 95% CI = −0.162–0.444; Z = 0.912; p = 0.362); and (c) 1 non-RCT comparison from one study (SMD = 0.454; SE = 0.489; variance = 0.239; 95% CI = −0.506–1.413; Z = 0.927; p = 0.354). These findings indicate that different study designs did not change the transient effects of robotic training combined with tDCS protocols on upper limb rehabilitation post-stroke.
The second moderator variable analysis revealed no significant short-term effects across different post-stroke recovery phases: (a) 4 subacute comparisons from 3 studies (SMD = −0.011; SE = 0.174; variance = 0.030; 95% CI = −0.351–0.330; Z = −0.061; p = 0.951); (b) 14 chronic comparisons from 10 studies (SMD = 0.055; SE = 0.108; variance = 0.012; 95% CI = −0.156–0.266; Z = 0.511; p = 0.609); and (c) 2 subacute and chronic comparisons from 2 studies (SMD = −0.008; SE = 0.295; variance = 0.087; 95% CI = −0.587–0.571; Z = −0.028; p = 0.978). These analyses failed to identify transient motor effects after the augmented combined protocols regardless of the post-stroke recovery phase.
3.3. Upper Limb Motor Functions: Long-Term Effects
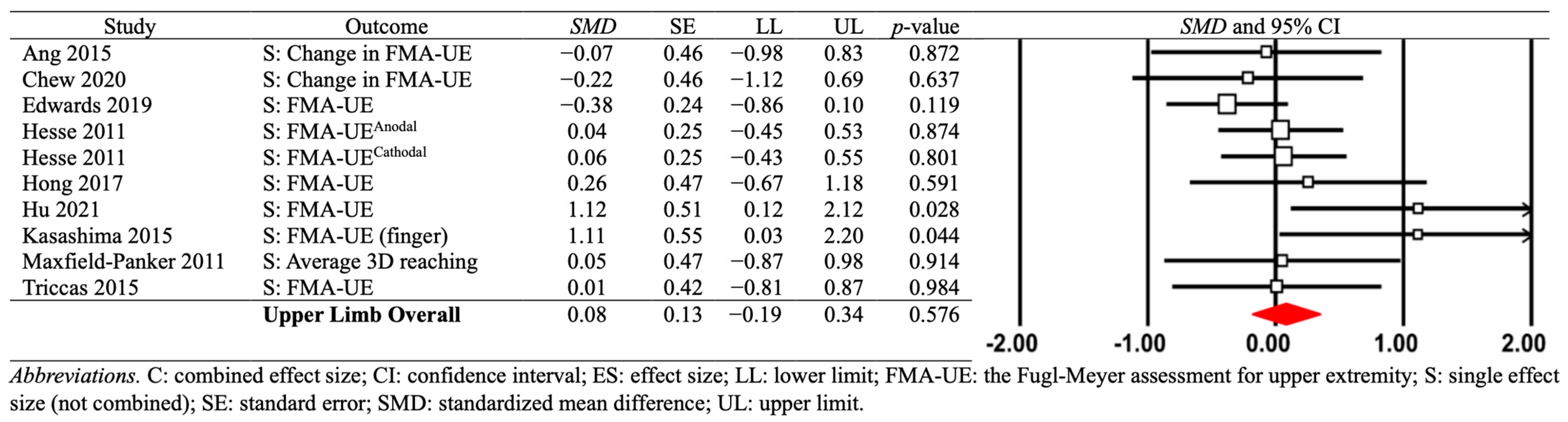
For the long-term effects of combined robotic training and tDCS protocols, the analysis of the 10 comparisons from 9 studies showed no significant effect size: SMD = −0.075; SE = 0.134; variance = 0.018; 95% CI = −0.188–0.338; Z = −0.559; p = 0.576; Figure 3. In addition, the heterogeneity levels across the individual effect sizes were minor: (a) Q-value = 11.808 with p = 0.224 and (b) I2 = 23.782%. Two publication bias tests additionally revealed minimal asymmetry levels of individual effect sizes: (a) a revised funnel plot with three imputed values after executing the trim and fill technique (Figure S2); and (b) Egger’s regression test: β0 = 2.010 and p = 0.075. These findings indicate that the combined tDCS and robotic training protocols showed no significant sustained effects on upper limb rehabilitation post-stroke.
3.4. Moderator Variable Analysis: Study Designs and Recovery Phase
The first moderator variable analysis showed no significant long-term effects across different study designs: (a) nine RCT comparisons from eight studies (SMD = −0.006; SE = 0.114; variance = 0.013; 95% CI = −0.229–0.218; Z = −0.051; p = 0.960); and (b) one non-RCT comparison from one study (SMD = 1.113; SE = 0.553; variance = 0.305; 95% CI = 0.030–2.197; Z = 2.015; p = 0.044). These findings indicate that different study designs did not change the sustained effects of tDCS combined with robotic training on the upper limbs post-stroke.
The second moderator variable analysis revealed no significant long-term effects across different post-stroke recovery phases: (a) two subacute comparisons from one study (SMD = 0.051; SE = 0.177; variance = 0.031; 95% CI = −0.295–0.398; Z = 0.290; p = 0.772); (b) seven chronic comparisons from seven studies (SMD = 0.174; SE = 0.230; variance = 0.053; 95% CI = −0.277–0.625; Z = 0.755; p = 0.450); and (c) one subacute and chronic comparison from one study (SMD = 0.008; SE = 0.417; variance = 0.174; 95% CI = −0.810–0.826; Z = 0.020; p = 0.984). These findings indicate that sustained effects on upper limb rehabilitation were not altered by different post-stroke recovery phases.
3.5. Lower Limb Motor Functions: Short-Term Effects
A random-effects model meta-analysis on the five comparisons from five studies revealed significant positive short-term effects of combined tDCS and robotic training protocols on lower limb recovery post-stroke: SMD = 0.693; SE = 0.237; variance = 0.056; 95% CI = 0.228–1.157; Z = 2.924; p = 0.003; (see Figure 4). These findings included a relatively small degree of heterogeneity: (a) Q-value = 4.789 with p = 0.310 and (b) I2 = 16.472%. Moreover, the publication bias assessments indicated minimal levels of asymmetry for the individual effect sizes: (a) a revised funnel plot with two imputed values after conducting the trim and fill technique (Figure S3) and (b) Egger’s regression test: β0 = 3.625 and p = 0.130. Importantly, these findings revealed that the combined robot-assisted movements and tDCS protocols significantly improved the motor capabilities of the lower extremities post-stroke.
3.6. Moderator Variable Analysis: Study Designs and Recovery Phase
The first moderator variable analysis showed significant short-term effects for RCT studies: (a) four RCT comparisons from four studies (SMD = 0.910; SE = 0.255; variance = 0.065; 95% CI = 0.411–1.409; Z = 3.574; p < 0.001) and (b) one non-RCT comparison from one study (SMD = 0.100; SE = 0.393; Variance = 0.155; 95% CI = −0.671–0.872; Z = 0.255; p = 0.798). These RCT findings indicate that significant positive transient effects were found after the combined protocols on the lower limbs post-stroke.
The second moderator variable analysis revealed significant short-term effects for chronic stroke patients: (a) four chronic comparisons from four studies (SMD = 0.910; SE = 0.255; variance = 0.065; 95% CI = 0.411–1.409; Z = 3.574; p < 0.001) and (b) one subacute comparison from one study (SMD = 0.100; SE = 0.393; variance = 0.155; 95% CI = −0.671–0.872; Z = 0.255; p = 0.798). These findings revealed significant positive transient effects on the lower limbs after the combined protocols in the chronic stage of stroke recovery.
3.7. Lower Limb Motor Functions: Long-Term Effects
For the long-term effects of combined robotic-training and tDCS protocols, the analysis on the four comparisons from four studies showed a significant effect size: SMD = 0.692; SE = 0.258; variance = 0.067; 95% CI = 0.186–1.198; Z = 2.678; p = 0.007; Figure 5. The levels of heterogeneity across the individual effect sizes were relatively minimal: (a) Q-value = 2.715 with p = 0.438 and (b) I2 = 0.000%. Moreover, two publication bias tests reported minor asymmetry levels in individual effect sizes: (a) a revised funnel plot with one imputed value after performing the trim and fill technique (Figure S4); and (b) Egger’s regression test: β0 = 2.652 and p = 0.400. In addition, given that all four comparisons from four studies used RCT design and recruited chronic stroke patients, moderator variable analyses were not necessary. Taken together, these findings indicate that robotic training combined with tDCS protocols showed significant positive transient and sustained effects on lower limb rehabilitation post-stroke as compared with those individuals in the control groups (i.e., robotic training only).
4. Discussion
The current systematic review and meta-analysis investigated the potential effects of robotic training programs in addition to tDCS protocols on motor recovery of the upper and lower extremities post-stroke. In contrast, analysis of the studies focused on the lower extremities revealed significant motor improvement findings for both moderate transient and sustained learning. Positive short-term and long-term motor effects were found for the augmented robotic training and tDCS protocols. These significant overall gait improvements were confirmed for individuals in the chronic stage of stroke recovery.
The meta-analytic findings on the upper extremity studies showed insufficient evidence regarding treatment effects of tDCS in addition to robotic-training programs. This is consistent with two recent review studies [42,43]. Specifically, the systematic review results on the eight individual studies performed by Simonetti and colleagues argued that robotic training coupled with tDCS protocols led to similar clinical improvements in upper limb functions post-stroke as compared with the robotic training protocol only [43]. Similarly, a meta-analysis reported no significant additional effects (mean difference = 0.15 with p-value = 0.93) of non-invasive brain stimulation (NIBS) protocols, including tDCS (i.e., six studies) and continuous theta burst stimulation (i.e., one study), combined with robotic training on upper limb motor recovery in patients with stroke [42]. Reis and colleagues suggested the possibility that the association of NIBS and robotic training may reveal long-term motor improvements in the upper limbs rather than short-term effects. However, our meta-analytic findings confirmed that the sustained effects estimated at 2–12 weeks after administering the final tDCS intervention were not significantly positive.
Moreover, the potential treatment effects of robotic training protocols on paretic arm recovery were controversial. Several meta-analysis studies argued that functional improvements in the upper extremities post-stroke (e.g., motor functions, muscle tone, and activities of daily living) were comparable between robotic training protocols and dose-matched conventional rehabilitation programs [27,34,73,74,75]. Despite some meta-analytic findings that reported significant improvements in motor control and strength of the paretic arms, the magnitude of motor recovery evidence was relatively small (e.g., two points of FMA arm score and Hedges’ g = 0.25) [34,76] and insignificant in the random-effects model [75]. Some studies suggested that quantifying kinematic and kinetic outcome measures may effectively detect changes in upper limb functions and motor learning after robotic training protocols for certain patients with stroke [34,77]. Patients, at three months post-stroke, may adapt their motor actions and prefer compensatory behaviors for daily living instead of the behavioral restitution of neurological impairments that would indicate true recovery [78,79]. Thus, clinical measurements are presumably insensitive for differentiating exactly what to learn (i.e., behavioral restitution) from the use of compensation strategies, and this limitation may potentially influence insignificant motor improvements of the paretic arms after robotic training combined with tDCS protocols. In fact, two individual studies in the current meta-analysis reported positive trends in functional improvement for patients with chronic stroke, as indicated by kinematic outcome measures on paretic arms (e.g., aim and straightness during upper limb reaching movements) [55,58]. The future studies need to confirm whether tDCS protocols in addition to robotic training improve kinematic and kinetic variables on paretic arms.
To advance motor recovery of the upper limbs post-stroke, administering bilateral robot-assisted rehabilitation programs coupled with bilateral tDCS protocols may be beneficial. Previous stroke rehabilitation studies have raised the possibility that functional improvements in the paretic arms may be better facilitated after bilateral treatments with robot devices such as an end-effector and exoskeleton systems as compared with unilateral robotic training protocols [80,81,82]. Potentially, bimanual movements may increase interlimb coupling, contributing to motor recovery of the paretic arms. This would be due to rebalanced inter-hemispheric inhibitions between hemispheres and greater involvement of both the contralateral pathway from the ipsilesional hemisphere as well as the ipsilateral pathway from the contralesional hemisphere to the affected upper limb [6,81,83]. Similarly, bilateral tDCS protocols such as anodal tDCS on the primary motor area (M1) of the ipsilesional hemisphere, and cathodal tDCS on the M1 of contralesional hemisphere, may enhance paretic arm functions via modulating and balancing cortical excitation and inhibition between hemispheres [84]. Nevertheless, nearly all of the included studies in this meta-analysis used unimanual robotic training protocols with active tDCS to stimulate the affected unilateral hemisphere. Taken together, these findings demonstrate that robotic training combined with tDCS protocols for advancing upper limb rehabilitation may target both sides of the central and peripheral nervous system.
For the five lower limb rehabilitation studies, robotic training combined with tDCS protocols revealed greater positive effects on gait functions post-stroke than those observed for robotic training only. These additional treatment effects were observed in the post-test conducted directly after the final intervention from the five comparisons, as well as in follow-up tests from the four comparisons. These meta-analytic findings support the proposition that non-invasive brain stimulation techniques administered with task-specific physical interventions may facilitate progress toward motor recovery in patients with stroke [14]. Recent meta-analysis studies indicated a possibility that applying specific tDCS montages (e.g., bi-hemispheric stimulation) can improve mobility, lower limb muscle strength, and gait functions estimated by clinical measurements in patients with stroke [85,86]. Presumably, stimulating motor cortical regions in both the affected and unaffected hemispheres may influence and trigger corticospinal and brainstem–spinal descending pathways, contributing to modulating the spinal central pattern generators [87,88,89]. Moreover, robot-assisted gait training can allow both ambulatory and non-ambulatory patients with stroke to perform intensive, repetitive, and complex walking practices, with more body weight support for patients and convenient administration for clinicians [90]. Thus, combining the top-down and bottom-up rehabilitation approaches may effectively increase neural plasticity and functional recovery across the central and peripheral nervous systems post-stroke. However, given that the number of included studies seems to be rather sparse, more studies will be necessary for validating potential treatment effects of tDCS protocols combined with robotic training on functional recovery of the lower limbs post-stroke.
Despite the potential additive effects of tDCS protocols with robotic training on post-stroke motor recovery, these findings should be cautiously interpreted. First, given that the qualified studies in this meta-analysis included no acute stroke patients, the current meta-analytic findings might be limited to subacute or chronic stroke patients. Although our moderator variable analyses additionally identified positive functional improvements in the lower limbs for chronic stroke patients, these results were obtained from only four studies. Thus, adding more studies in a future meta-analysis is necessary to validate the current findings. Further, more studies should examine appropriate timing of stimulation relative to providing robotic training, which may increase the efficacy of combining the tDCS and robotic training protocols for upper and lower limb motor recovery post-stroke. Although the superior treatment effects between offline (i.e., tDCS before motor training) and online (i.e., tDCS during motor training) tDCS protocols are still controversial in the literature, some studies have suggested that online tDCS protocols effectively facilitate motor learning network activation in the brain, contributing to better motor learning performances [91,92]. A recent animal study additionally proposed that online tDCS may enhance Hebbian plasticity improving motor learning capabilities, as they observed two crucial properties of Hebbian plasticity, including synaptic specificity and associativity, in vitro [19]. Finally, increasing the focal intensity of stimulation, such as by using high-definition tDCS (HD-tDCS) in addition to robotic training, may be an alternative to elevate motor improvement in patients with stroke, as HD-tDCS may show more long-lasting after-effects that would presumably boost physical practice effects [93,94].
5. Conclusions
The current systematic review and meta-analysis revealed the potential additional treatment effects of robotic-assisted movements coupled with tDCS protocols post-stroke. Specifically, we found transient and sustained motor improvements in gait functions post-stroke after individuals participated in rehabilitation sessions with coupled robotic training and tDCS protocols. Helping stroke survivors to re-acquire walking capabilities is impactful for the two augmented treatment protocols. Even though significant motor improvements were absent in the upper extremities, the overall findings suggest clinical implications of considering coupled top-down and bottom-up rehabilitation protocols. The additive effects of executing two augmented rehabilitation protocols as dual treatment interventions for the lower extremities warrants further investigation.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/app13031992/s1, Figure S1: Funnel plots including 20 comparisons about short-term effects of combined robotic training and tDCS protocols on the upper limbs for publication bias assessments; Figure S2: Funnel plots including 10 comparisons about long-term effects of combined robotic training and tDCS protocols on the upper limbs for publication bias assessments; Figure S3: Funnel plots including five comparisons of short-term effects of combined robotic training and tDCS protocols on lower limbs for publication bias assessments; Figure S4: Funnel plots including four comparisons of long-term effects of combined robotic training and tDCS protocols on lower limbs for publication bias assessments. Table S1: Intervention protocols for control; Table S2: Specific data format and meta-analytic calculation data.
Author Contributions
Conceptualization, N.K., R.-K.K. and J.H.C.; methodology, N.K., R.-K.K., Z.D. and J.H.C.; software, N.K. and R.-K.K.; validation, N.K., R.-K.K., Z.D. and J.H.C.; writing—original draft preparation, N.K., R.-K.K., Z.D. and J.H.C.; writing—review and editing, N.K., R.-K.K., Z.D. and J.H.C.; supervision, N.K. and J.H.C.; project administration, N.K. and J.H.C.; funding acquisition, N.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Incheon National University Research Grant in 2021 (2021-0072).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N. Heart disease and stroke statistics—2021 update: A report from the American Heart Association. Circulation 2021, 143, 254–743. [Google Scholar] [CrossRef]
- Arene, N.; Hidler, J. Understanding motor impairment in the paretic lower limb after a stroke: A review of the literature. Top. Stroke Rehabil. 2009, 16, 346–356. [Google Scholar] [CrossRef]
- Kim, R.K.; Kang, N. Bimanual coordination functions between paretic and nonparetic arms: A systematic review and meta-analysis. J. Stroke Cerebrovasc. Dis. 2020, 29, 104544. [Google Scholar] [CrossRef] [PubMed]
- Kantak, S.; Jax, S.; Wittenberg, G. Bimanual coordination: A missing piece of arm rehabilitation after stroke. Restor. Neurol. Neurosci. 2017, 35, 347–364. [Google Scholar] [CrossRef] [PubMed]
- van Delden, A.E.; Beek, P.J.; Roerdink, M.; Kwakkel, G.; Peper, C.E. Unilateral and bilateral upper-limb training interventions after stroke have similar effects on bimanual coupling strength. Neurorehabil. Neural Repair. 2015, 29, 255–267. [Google Scholar] [CrossRef]
- Cauraugh, J.H.; Summers, J.J. Neural plasticity and bilateral movements: A rehabilitation approach for chronic stroke. Prog. Neurobiol. 2005, 75, 309–320. [Google Scholar] [CrossRef]
- Kleim, J.A.; Jones, T.A. Principles of experience-dependent neural plasticity: Implications for rehabilitation after brain damage. J. Speech Lang. Hear. Res. 2008, 51, S225–S239. [Google Scholar] [CrossRef]
- Schaechter, J.D. Motor rehabilitation and brain plasticity after hemiparetic stroke. Prog. Neurobiol. 2004, 73, 61–72. [Google Scholar] [CrossRef]
- Cramer, S.C. Treatments to Promote Neural Repair after Stroke. J. Stroke 2018, 20, 57–70. [Google Scholar] [CrossRef]
- Ebbesen, C.L.; Brecht, M. Motor cortex—To act or not to act? Nat. Rev. Neurosci. 2017, 18, 694–705. [Google Scholar] [CrossRef]
- Kimble, G.A.; Perlmuter, L.C. The problem of volition. Psychol. Rev. 1970, 77, 361–384. [Google Scholar] [CrossRef] [PubMed]
- Belda-Lois, J.M.; Mena-del Horno, S.; Bermejo-Bosch, I.; Moreno, J.C.; Pons, J.L.; Farina, D.; Iosa, M.; Molinari, M.; Tamburella, F.; Ramos, A.; et al. Rehabilitation of gait after stroke: A review towards a top-down approach. J. Neuroeng. Rehabil. 2011, 8, 66. [Google Scholar] [CrossRef]
- Biasiucci, A.; Leeb, R.; Iturrate, I.; Perdikis, S.; Al-Khodairy, A.; Corbet, T.; Schnider, A.; Schmidlin, T.; Zhang, H.; Bassolino, M.; et al. Brain-actuated functional electrical stimulation elicits lasting arm motor recovery after stroke. Nat. Commun. 2018, 9, 2421. [Google Scholar] [CrossRef] [PubMed]
- Kang, N.; Summers, J.J.; Cauraugh, J.H. Transcranial direct current stimulation facilitates motor learning post-stroke: A systematic review and meta-analysis. J. Neurol. Neurosurg. Psychiatry 2016, 87, 345–355. [Google Scholar] [CrossRef]
- Masiero, S.; Celia, A.; Rosati, G.; Armani, M. Robotic-assisted rehabilitation of the upper limb after acute stroke. Arch. Phys. Med. Rehabil. 2007, 88, 142–149. [Google Scholar] [CrossRef]
- Marquez, J.; van Vliet, P.; McElduff, P.; Lagopoulos, J.; Parsons, M. Transcranial direct current stimulation (tDCS): Does it have merit in stroke rehabilitation? A systematic review. Int. J. Stroke 2015, 10, 306–316. [Google Scholar] [CrossRef] [PubMed]
- Kang, N.; Summers, J.J.; Cauraugh, J.H. Non-invasive brain stimulation improves paretic limb force production: A systematic review and meta-analysis. Brain Stimul. 2016, 9, 662–670. [Google Scholar] [CrossRef]
- Au-Yeung, S.S.; Wang, J.; Chen, Y.; Chua, E. Transcranial direct current stimulation to primary motor area improves hand dexterity and selective attention in chronic stroke. Am. J. Phys. Med. Rehabil. 2014, 93, 1057–1064. [Google Scholar] [CrossRef]
- Kronberg, G.; Rahman, A.; Sharma, M.; Bikson, M.; Parra, L.C. Direct current stimulation boosts hebbian plasticity in vitro. Brain Stimul. 2020, 13, 287–301. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527, 633–639. [Google Scholar] [CrossRef]
- Lindenberg, R.; Renga, V.; Zhu, L.; Nair, D.; Schlaug, G. Bihemispheric brain stimulation facilitates motor recovery in chronic stroke patients. Neurology 2010, 75, 2176–2184. [Google Scholar] [CrossRef]
- Wu, D.; Qian, L.; Zorowitz, R.D.; Zhang, L.; Qu, Y.; Yuan, Y. Effects on decreasing upper-limb poststroke muscle tone using transcranial direct current stimulation: A randomized sham-controlled study. Arch. Phys. Med. Rehabil. 2013, 94, 1–8. [Google Scholar] [CrossRef]
- Bornheim, S.; Croisier, J.L.; Maquet, P.; Kaux, J.F. Transcranial direct current stimulation associated with physical-therapy in acute stroke patients—A randomized, triple blind, sham-controlled study. Brain Stimul. 2020, 13, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.; Bachmann, C.; Lee, J.S.; Gregoriou, E.; Ward, N.; Bestmann, S. Dose-controlled tDCS reduces electric field intensity variability at a cortical target site. Brain Stimul. 2020, 13, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Bestmann, S.; Ward, N. Are current flow models for transcranial electrical stimulation fit for purpose? Brain Stimul. 2017, 10, 865–866. [Google Scholar] [CrossRef]
- Krebs, H.I.; Palazzolo, J.J.; Dipietro, L.; Ferraro, M.; Krol, J.; Rannekleiv, K.; Volpe, B.T.; Hogan, N. Rehabilitation robotics: Performance-based progressive robot-assisted therapy. Auton. Robot. 2003, 15, 7–20. [Google Scholar] [CrossRef]
- Kwakkel, G.; Kollen, B.J.; Krebs, H.I. Effects of robot-assisted therapy on upper limb recovery after stroke: A systematic review. Neural Repair. 2008, 22, 111–121. [Google Scholar] [CrossRef]
- Fasoli, S.E.; Krebs, H.I.; Stein, J.; Frontera, W.R.; Hogan, N. Effects of robotic therapy on motor impairment and recovery in chronic stroke. Arch. Phys. Med. Rehabil. 2003, 84, 477–482. [Google Scholar] [CrossRef]
- Moucheboeuf, G.; Griffier, R.; Gasq, D.; Glize, B.; Bouyer, L.; Dehail, P.; Cassoudesalle, H. Effects of robotic gait training after stroke: A meta-analysis. Ann. Phys. Rehabil. Med. 2020, 63, 518–534. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Pohl, M.; Platz, T.; Kugler, J.; Elsner, B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2018, 6. [Google Scholar] [CrossRef]
- Lum, P.S.; Burgar, C.G.; Shor, P.C.; Majmundar, M.; Van der Loos, M. Robot-assisted movement training compared with conventional therapy techniques for the rehabilitation of upper-limb motor function after stroke. Arch. Phys. Med. Rehabil. 2002, 83, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, I.; Sajin, A.; Fisher, I.; Neeb, M.; Shochina, M.; Katz-Leurer, M.; Meiner, Z. The effectiveness of locomotor therapy using robotic-assisted gait training in subacute stroke patients: A randomized controlled trial. PM&R 2009, 1, 516–523. [Google Scholar] [CrossRef]
- Baronchelli, F.; Zucchella, C.; Serrao, M.; Intiso, D.; Bartolo, M. The effect of robotic assisted gait training with lokomat® on balance control after stroke: Systematic review and meta-analysis. Front. Neurol. 2021, 12, 661815. [Google Scholar] [CrossRef]
- Veerbeek, J.M.; Langbroek-Amersfoort, A.C.; van Wegen, E.E.; Meskers, C.G.; Kwakkel, G. Effects of robot-assisted therapy for the upper limb after stroke. Neurorehabil. Neural Repair. 2017, 31, 107–121. [Google Scholar] [CrossRef]
- Hesse, S.; Schattat, N.; Mehrholz, J.; Werner, C. Evidence of end-effector based gait machines in gait rehabilitation after CNS lesion. Neurorehabilitation 2013, 33, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Ochi, M.; Saeki, S.; Oda, T.; Matsushima, Y.; Hachisuka, K. Effects of anodal and cathodal transcranial direct current stimulation combined with robotic therapy on severely affected arms in chronic stroke patients. J. Rehabil. Med. 2013, 45, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Picelli, A.; Chemello, E.; Castellazzi, P.; Roncari, L.; Waldner, A.; Saltuari, L.; Smania, N. Combined effects of transcranial direct current stimulation (tDCS) and transcutaneous spinal direct current stimulation (tsDCS) on robot-assisted gait training in patients with chronic stroke: A pilot, double blind, randomized controlled trial. Restor. Neurol. Neurosci. 2015, 33, 357–368. [Google Scholar] [CrossRef]
- Manji, A.; Amimoto, K.; Matsuda, T.; Wada, Y.; Inaba, A.; Ko, S. Effects of transcranial direct current stimulation over the supplementary motor area body weight-supported treadmill gait training in hemiparetic patients after stroke. Neurosci. Lett. 2018, 662, 302–305. [Google Scholar] [CrossRef]
- Zimerman, M.; Heise, K.F.; Hoppe, J.; Cohen, L.G.; Gerloff, C.; Hummel, F.C. Modulation of training by single-session transcranial direct current stimulation to the intact motor cortex enhances motor skill acquisition of the paretic hand. Stroke 2012, 43, 2185–2191. [Google Scholar] [CrossRef] [PubMed]
- Turner, D.L.; Ramos-Murguialday, A.; Birbaumer, N.; Hoffmann, U.; Luft, A. Neurophysiology of robot-mediated training and therapy: A perspective for future use in clinical populations. Front. Neurol. 2013, 4, 184. [Google Scholar] [CrossRef] [Green Version]
- Wessel, M.J.; Zimerman, M.; Hummel, F.C. Non-invasive brain stimulation: An interventional tool for enhancing behavioral training after stroke. Front. Hum. Neurosci. 2015, 9, 265. [Google Scholar] [CrossRef]
- Reis, S.B.; Bernardo, W.M.; Oshiro, C.A.; Krebs, H.I.; Conforto, A.B. Effects of robotic therapy associated with noninvasive brain stimulation on upper-limb rehabilitation after stroke: Systematic review and meta-analysis of randomized clinical trials. Neurorehabil. Neural Repair. 2021, 35, 256–266. [Google Scholar] [CrossRef]
- Simonetti, D.; Zollo, L.; Milighetti, S.; Miccinilli, S.; Bravi, M.; Ranieri, F.; Magrone, G.; Guglielmelli, E.; Di Lazzaro, V.; Sterzi, S. Literature review on the effects of tDCS coupled with robotic therapy in post stroke upper limb rehabilitation. Front. Hum. Neurosci. 2017, 11. [Google Scholar] [CrossRef] [PubMed]
- Comino-Suárez, N.; Moreno, J.C.; Gómez-Soriano, J.; Megía-García, Á.; Serrano-Muñoz, D.; Taylor, J.; Alcobendas-Maestro, M.; Gil-Agudo, Á.; Del-Ama, A.J.; Avendaño-Coy, J. Transcranial direct current stimulation combined with robotic therapy for upper and lower limb function after stroke: A systematic review and meta-analysis of randomized control trials. J. Neuroeng. Rehabil. 2021, 18, 148. [Google Scholar] [CrossRef] [PubMed]
- Kasashima-Shindo, Y.; Fujiwara, T.; Ushiba, J.; Matsushika, Y.; Kamatani, D.; Oto, M.; Ono, T.; Nishimoto, A.; Shindo, K.; Kawakami, M.; et al. Brain-computer interface training combined with transcranial direct current stimulation in patients with chronic severe hemiparesis: Proof of concept study. J. Rehabil. Med. 2015, 47, 318–324. [Google Scholar] [CrossRef]
- Triccas, L.T.; Burridge, J.H.; Hughes, A.; Verheyden, G.; Desikan, M.; Rothwell, J. A double-blinded randomised controlled trial exploring the effect of anodal transcranial direct current stimulation and uni-lateral robot therapy for the impaired upper limb in sub-acute and chronic stroke. Neurorehabilitation 2015, 37, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Leon, D.; Cortes, M.; Elder, J.; Kumru, H.; Laxe, S.; Edwards, D.J.; Tormos, J.M.; Bernabeu, M.; Pascual-Leone, A. tDCS does not enhance the effects of robot-assisted gait training in patients with subacute stroke. Restor. Neurol. Neurosci. 2017, 35, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Cumpston, M.S.; McKenzie, J.E.; Welch, V.A.; Brennan, S.E. Strengthening systematic reviews in public health: Guidance in the Cochrane Handbook for Systematic Reviews of Interventions, 2nd edition. J. Public Health 2022, 44, e588–e592. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: Chichester, UK, 2009. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef]
- Ang, K.K.; Guan, C.; Phua, K.S.; Wang, C.; Zhao, L.; Teo, W.P.; Chen, C.; Ng, Y.S.; Chew, E. Facilitating effects of transcranial direct current stimulation on motor imagery brain-computer interface with robotic feedback for stroke rehabilitation. Arch. Phys. Med. Rehabil. 2015, 96, S79–S87. [Google Scholar] [CrossRef]
- Chew, E.; Teo, W.P.; Tang, N.; Ang, K.K.; Ng, Y.S.; Zhou, J.H.; Teh, I.; Phua, K.S.; Zhao, L.; Guan, C. Using transcranial direct current stimulation to augment the effect of motor imagery-assisted brain-computer interface training in chronic stroke patients-cortical reorganization considerations. Front. Neurol. 2020, 11, 948. [Google Scholar] [CrossRef]
- Danzl, M.M.; Chelette, K.C.; Lee, K.; Lykins, D.; Sawaki, L. Brain stimulation paired with novel locomotor training with robotic gait orthosis in chronic stroke: A feasibility study. Neurorehabilitation 2013, 33, 67–76. [Google Scholar] [CrossRef]
- De Laet, C.; Herman, B.; Riga, A.; Bihin, B.; Regnier, M.; Leeuwerck, M.; Raymackers, J.M.; Vandermeeren, Y. Bimanual motor skill learning after stroke: Combining robotics and anodal tDCS over the undamaged hemisphere: An exploratory study. Front. Neurol. 2022, 13, 882225. [Google Scholar] [CrossRef] [PubMed]
- Dehem, S.; Gilliaux, M.; Lejeune, T.; Delaunois, E.; Mbonda, P.; Vandermeeren, Y.; Detrembleur, C.; Stoquart, G. Effectiveness of a single session of dual-transcranial direct current stimulation in combination with upper limb robotic-assisted rehabilitation in chronic stroke patients: A randomized, double-blind, cross-over study. Int. J. Rehabil. Res. 2018, 41, 138–145. [Google Scholar] [CrossRef]
- Edwards, D.J.; Cortes, M.; Rykman-Peltz, A.; Chang, J.; Elder, J.; Thickbroom, G.; Mariman, J.J.; Gerber, L.M.; Oromendia, C.; Krebs, H.I. Clinical improvement with intensive robot-assisted arm training in chronic stroke is unchanged by supplementary tDCS. Restor. Neurol. Neurosci. 2019, 37, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Geroin, C.; Picelli, A.; Munari, D.; Waldner, A.; Tomelleri, C.; Smania, N. Combined transcranial direct current stimulation and robot-assisted gait training in patients with chronic stroke: A preliminary comparison. Clin. Rehabil. 2011, 25, 537–548. [Google Scholar] [CrossRef]
- Giacobbe, V.; Krebs, H.I.; Volpe, B.T.; Pascual-Leone, A.; Rykman, A.; Zeiarati, G.; Fregni, F.; Dipietro, L.; Thickbroom, G.W.; Edwards, D.J. Transcranial direct current stimulation (tDCS) and robotic practice in chronic stroke: The dimension of timing. Neurorehabilitation 2013, 33, 49–56. [Google Scholar] [CrossRef]
- Hesse, S.; Waldner, A.; Mehrholz, J.; Tomelleri, C.; Pohl, M.; Werner, C. Combined transcranial direct current stimulation and robot-assisted arm training in subacute stroke patients: An exploratory, randomized multicenter trial. Neurorehabil. Neural Repair. 2011, 25, 838–846. [Google Scholar] [CrossRef]
- Hong, X.; Lu, Z.K.; Teh, I.; Nasrallah, F.A.; Teo, W.P.; Ang, K.K.; Phua, K.S.; Guan, C.; Chew, E.; Chuang, K.H. Brain plasticity following MI-BCI training combined with tDCS in a randomized trial in chronic subcortical stroke subjects: A preliminary study. Sci. Rep. 2017, 7, 9222. [Google Scholar] [CrossRef] [PubMed]
- Maxfield-Panker, S.N. The Effects of Robotic Training and Cortical Stimulation on Reaching Skill after Chronic Stroke. Ph.D. Thesis, Georgetown University, Washington, DC, USA, 2011. [Google Scholar]
- Mazzoleni, S.; Dario, P.; Posteraro, F.; Iardella, L. Effects of combined transcranial direct current stimulation and wrist robot-assisted therapy in subacute stroke patients: Preliminary results. In Proceedings of the 2015 IEEE International Conference on Rehabilitation Robotics (ICORR), Singapore, 11–14 August 2015; pp. 217–222. [Google Scholar]
- Mazzoleni, S.; Tran, V.D.; Dario, P.; Posteraro, F. Effects of transcranial direct current stimulation (tDCS) combined with wrist robot-assisted rehabilitation on motor recovery in subacute stroke patients: A randomized controlled trial. IEEE Trans. Neural Syst. Rehabil. Eng 2019, 27, 1458–1466. [Google Scholar] [CrossRef]
- Seo, H.G.; Lee, W.H.; Lee, S.H.; Yi, Y.; Kim, K.D.; Oh, B.M. Robotic-assisted gait training combined with transcranial direct current stimulation in chronic stroke patients: A pilot double-blind, randomized controlled trial. Restor. Neurol. Neurosci. 2017, 35, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Straudi, S.; Fregni, F.; Martinuzzi, C.; Pavarelli, C.; Salvioli, S.; Basaglia, N. tDCS and robotics on upper limb stroke rehabilitation: Effect modification by stroke duration and type of stroke. BioMed Res. Int. 2016, 2016, 5068127. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.; Cheng, H.-J.; Ji, F.; Chong, J.S.X.; Lu, Z.; Huang, W.; Ang, K.K.; Phua, K.S.; Chuang, K.-H.; Jiang, X.; et al. Brain functional changes in stroke following rehabilitation using brain-computer interface-assisted motor imagery with and without tDCS: A pilot study. Front. Hum. Neurosci. 2021, 15, 692304. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Bastani, A.; Jaberzadeh, S. Does anodal transcranial direct current stimulation enhance excitability of the motor cortex and motor function in healthy individuals and subjects with stroke: A systematic review and meta-analysis. Clin. Neurophysiol. 2012, 123, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Foley, N.C.; Teasell, R.W.; Bhogal, S.K.; Speechley, M.R. Stroke rehabilitation evidence-based review: Methodology. Top. Stroke Rehabil. 2003, 10, 1–7. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot–based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Mehrholz, J.; Pollock, A.; Pohl, M.; Kugler, J.; Elsner, B. Systematic review with network meta-analysis of randomized controlled trials of robotic-assisted arm training for improving activities of daily living and upper limb function after stroke. J. Neuroeng. Rehabil. 2020, 17, 83. [Google Scholar] [CrossRef] [PubMed]
- Chien, W.T.; Chong, Y.Y.; Tse, M.K.; Chien, C.W.; Cheng, H.Y. Robot-assisted therapy for upper-limb rehabilitation in subacute stroke patients: A systematic review and meta-analysis. Brain Behav. 2020, 10, e01742. [Google Scholar] [CrossRef]
- Bertani, R.; Melegari, C.; De Cola, M.C.; Bramanti, A.; Bramanti, P.; Calabro, R.S. Effects of robot-assisted upper limb rehabilitation in stroke patients: A systematic review with meta-analysis. Neurol. Sci. 2017, 38, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Cheng, H.; Zhang, J.; Yang, S.; Cai, S. Robot-assisted therapy for upper extremity motor impairment after stroke: A systematic review and meta-analysis. Phys. Ther. 2021, 101, pzab010. [Google Scholar] [CrossRef]
- Krebs, H.I.; Krams, M.; Agrafiotis, D.K.; DiBernardo, A.; Chavez, J.C.; Littman, G.S.; Yang, E.; Byttebier, G.; Dipietro, L.; Rykman, A.; et al. Robotic measurement of arm movements after stroke establishes biomarkers of motor recovery. Stroke 2014, 45, 200–204. [Google Scholar] [CrossRef]
- van Kordelaar, J.; van Wegen, E.E.; Nijland, R.H.; Daffertshofer, A.; Kwakkel, G. Understanding adaptive motor control of the paretic upper limb early poststroke: The EXPLICIT-stroke program. Neurorehabil. Neural Repair 2013, 27, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, J.; Hayward, K.S.; Kwakkel, G.; Ward, N.S.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; Boyd, L.A.; Carmichael, S.T.; Corbett, D.; et al. Agreed definitions and a shared vision for new standards in stroke recovery research: The stroke recovery and rehabilitation roundtable taskforce. Neurorehabil. Neural Repair. 2017, 31, 793–799. [Google Scholar] [CrossRef] [PubMed]
- Simkins, M.; Kim, H.; Abrams, G.; Byl, N.; Rosen, J. Robotic unilateral and bilateral upper-limb movement training for stroke survivors afflicted by chronic hemiparesis. In Proceedings of the 2013 IEEE 13th International Conference on Rehabilitation Robotics (ICORR), Seattle, WA, USA, 24–26 June 2013; Volume 2013, p. 6650506. [Google Scholar] [CrossRef]
- Hung, C.S.; Lin, K.C.; Chang, W.Y.; Huang, W.C.; Chang, Y.J.; Chen, C.L.; Grace Yao, K.; Lee, Y.Y. Unilateral vs bilateral hybrid approaches for upper limb rehabilitation in chronic stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2019, 100, 2225–2232. [Google Scholar] [CrossRef]
- Miao, Q.; Zhang, M.; Wang, Y.; Xie, S.Q. Design and interaction control of a new bilateral upper-limb rehabilitation device. J. Healthc. Eng. 2017, 2017, 7640325. [Google Scholar] [CrossRef]
- Tazoe, T.; Sasada, S.; Sakamoto, M.; Komiyama, T. Modulation of interhemispheric interactions across symmetric and asymmetric bimanual force regulations. Eur. J. Neurosci. 2013, 37, 96–104. [Google Scholar] [CrossRef]
- Santos Ferreira, I.; Teixeira Costa, B.; Lima Ramos, C.; Lucena, P.; Thibaut, A.; Fregni, F. Searching for the optimal tDCS target for motor rehabilitation. J. Neuroeng. Rehabil. 2019, 16, 90. [Google Scholar] [CrossRef]
- Tien, H.H.; Liu, W.Y.; Chen, Y.L.; Wu, Y.C.; Lien, H.Y. Transcranial direct current stimulation for improving ambulation after stroke: A systematic review and meta-analysis. Int. J. Rehabil. Res. 2020, 43, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Fan, J.; Yang, J.; He, C.; Li, S. Effects of transcranial direct current stimulation on walking ability after stroke: A systematic review and meta-analysis. Restor. Neurol. Neurosci. 2018, 36, 59–71. [Google Scholar] [CrossRef]
- Naro, A.; Billeri, L.; Manuli, A.; Balletta, T.; Cannavo, A.; Portaro, S.; Lauria, P.; Ciappina, F.; Calabro, R.S. Breaking the ice to improve motor outcomes in patients with chronic stroke: A retrospective clinical study on neuromodulation plus robotics. Neurol. Sci. 2020, 42, 2785–2793. [Google Scholar] [CrossRef]
- Gunduz, A.; Rothwell, J.; Vidal, J.; Kumru, H. Non-invasive brain stimulation to promote motor and functional recovery following spinal cord injury. Neural Regen. Res. 2017, 12, 1933–1938. [Google Scholar] [CrossRef] [PubMed]
- Nitsche, M.A. Beyond the target area: Remote effects of non-invasive brain stimulation in humans. J. Physiol. 2011, 589, 3053–3054. [Google Scholar] [CrossRef]
- Morone, G.; Paolucci, S.; Cherubini, A.; De Angelis, D.; Venturiero, V.; Coiro, P.; Iosa, M. Robot-assisted gait training for stroke patients: Current state of the art and perspectives of robotics. Neuropsychiatr. Dis. Treat. 2017, 13, 1303–1311. [Google Scholar] [CrossRef] [PubMed]
- Liebrand, M.; Karabanov, A.; Antonenko, D.; Floel, A.; Siebner, H.R.; Classen, J.; Kramer, U.M.; Tzvi, E. Beneficial effects of cerebellar tDCS on motor learning are associated with altered putamen-cerebellar connectivity: A simultaneous tDCS-fMRI study. Neuroimage 2020, 223, 117363. [Google Scholar] [CrossRef]
- Amadi, U.; Allman, C.; Johansen-Berg, H.; Stagg, C.J. The homeostatic interaction between anodal transcranial direct current stimulation and motor learning in humans is related to GABA(A) activity. Brain Stimul. 2015, 8, 898–905. [Google Scholar] [CrossRef]
- Kuo, H.I.; Bikson, M.; Datta, A.; Minhas, P.; Paulus, W.; Kuo, M.F.; Nitsche, M.A. Comparing cortical plasticity induced by conventional and high-definition 4 x 1 ring tDCS: A neurophysiological study. Brain Stimul. 2013, 6, 644–648. [Google Scholar] [CrossRef]
- Elsner, B.; Kugler, J.; Mehrholz, J. Transcranial direct current stimulation (tDCS) for upper limb rehabilitation after stroke: Future directions. J. Neuroeng. Rehabil. 2018, 15, 106. [Google Scholar] [CrossRef]
Figure 1.
Flow chart for study identification procedure.

Figure 2.
Short-term effects of combining the protocols of robot training and tDCS on upper limb functions. The synthesized data derived from a random-effects model show no significant positive transient effects on upper motor rehabilitation. Note that the red diamond indicates overall effect size and squares denote individual effect sizes with 95% CI. More positive values indicate more treatment effects after the combined protocols [45,46,51,52,54,55,56,58,59,60,61,62,63,65,66].
Figure 2.
Short-term effects of combining the protocols of robot training and tDCS on upper limb functions. The synthesized data derived from a random-effects model show no significant positive transient effects on upper motor rehabilitation. Note that the red diamond indicates overall effect size and squares denote individual effect sizes with 95% CI. More positive values indicate more treatment effects after the combined protocols [45,46,51,52,54,55,56,58,59,60,61,62,63,65,66].

Figure 3.
Long-term effects of robotic training combined with tDCS on upper limb function. The synthesized data derived from a random-effects model show no significant positive sustained effects on upper motor rehabilitation. Note that the red diamond indicates overall effect size and squares denote individual effect sizes with 95% CI. More positive values indicate more treatment effects after the combined protocols [45,46,51,52,56,59,60,61,66].
Figure 3.
Long-term effects of robotic training combined with tDCS on upper limb function. The synthesized data derived from a random-effects model show no significant positive sustained effects on upper motor rehabilitation. Note that the red diamond indicates overall effect size and squares denote individual effect sizes with 95% CI. More positive values indicate more treatment effects after the combined protocols [45,46,51,52,56,59,60,61,66].

Figure 4.
Short-term effects of robotic training combined with tDCS on motor function in the lower extremities. The synthesized data derived from a random-effects model show significant positive transient effects after lower motor rehabilitation. Note that the red diamond indicates overall effect size and squares denote individual effect sizes with 95% CI. More positive values indicate more treatment effects after the combined protocols [37,47,53,57,64].
Figure 4.
Short-term effects of robotic training combined with tDCS on motor function in the lower extremities. The synthesized data derived from a random-effects model show significant positive transient effects after lower motor rehabilitation. Note that the red diamond indicates overall effect size and squares denote individual effect sizes with 95% CI. More positive values indicate more treatment effects after the combined protocols [37,47,53,57,64].

Figure 5.
Long-term effects of robotic training combined with tDCS on lower limb functions. The synthesized data derived from a random-effects model show significant positive sustained effects on lower motor rehabilitation. Note that the red diamond indicates overall effect size and squares denote individual effect sizes with 95% CI. More positive values indicate more treatment effects after the combined protocols [37,53,57,64].
Figure 5.
Long-term effects of robotic training combined with tDCS on lower limb functions. The synthesized data derived from a random-effects model show significant positive sustained effects on lower motor rehabilitation. Note that the red diamond indicates overall effect size and squares denote individual effect sizes with 95% CI. More positive values indicate more treatment effects after the combined protocols [37,53,57,64].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
PICO criteria for inclusion and exclusion.
| Contents | |
|---|---|
| P (Population) | Patients with stroke without restriction on age and demographic variables |
| I (Intervention) | Combined protocols including tDCS and robotic training |
| C (Comparator) | Patients with stroke with robotic training combined with either sham tDCS or no tDCS condition |
| O (Outcome) | Quantitative changes in either upper or lower limb motor functions |
Table 2.
Participant characteristics.
| Study | Study Design | Total (N) | Age (yrs) | Gender | TSO (Month) | Stroke Type | Affected Hemisphere | Motor Impairment Level | Recovery Stage |
|---|---|---|---|---|---|---|---|---|---|
| Upper Limb Rehabilitation | |||||||||
| Ang 2015 [51] | RCT | 19 | 54.1 ± 10.6 | 5 F, 14 M | 9.6–55.2 | 6 H, 13 I | 11 R, 8 L | FMA-UE = 34.0 ± 7.9 | Chronic |
| Chew 2020 [52] | RCT | 19 | 54.2 ± 10.7 | 5 F, 14 M | 32.3 ± 20.1 | 6 H, 13 I | 11 R, 8 L | FMA-UE = 34.0 ± 7.9 | Chronic |
| De Laet 2022 [54] | COVR | 17 | 60.0 ± 13.0 | 9 F, 8 M | 6–35 | NA | NA | FMA-UE = 54.4 ± 14.6 | Chronic |
| Dehem 2018 [55] | COVR | 21 | 60.5 ± 9.5 | 6 F, 15 M | 38.6 ± 57.0 | 6 H, 15 I | NA | SIAS = 57.6 ± 10.5 | Chronic |
| Edwards 2019 [56] | RCT | 82 | 67.8 (42–90) | 32 F, 50 M | 42.4 (4.9–223.7) | NA | NA | FMA-UE = 25.4 ± 16.2 | Chronic |
| Giacobbe 2013 [58] | COVR | 12 | 64.4 ± 11.6 | 6 F, 6 M | 46.5 ± 21.1 | NA | 7 R, 5 L | FMA-UE = 38.3 ± 16.8 | Chronic |
| Hesse 2011 [59] | RCT | 96 | 18–79 | 37 F, 59 M | 0.9–1.0 | NA | 45 R, 51 L | FMA-UE = 7.8–8.2 | Subacute |
| Hong 2017 [60] | RCT | 18 | 54.1 ± 10.8 | 5 F, 13 M | 33.6 ± 19.8 | NA | NA | FMA-UE = 34.7 ± 7.8 | Chronic |
| Hu 2021 [66] | RCT | 18 | 54.1 ± 10.6 | 5 F, 14 M | 34.6 ± 19.9 | 6 H, 12 I | 10 R 8 L | FMA-UE = 35.3 ± 8.0 (real), 33.7 ± 8.1 (sham) | Chronic |
| Kasashima 2015 [45] | N-RCT | 18 | 48.0–53.5 | 5 F, 13 M | 46.2–56.4 | 9 H, 9 I | 11 R, 7 L | FMA-UE = 38.3 ± 16.8 | Chronic |
| Mazzoleni 2015 [62] | RCT | 12 | 75.9 ± 7.0 | 10 F, 2 M | 0.9 | NA | 8 R, 4 L | FMA-UE = 28.0 ± 20.9 (real), 41.8 ± 14.5 (sham) | Subacute |
| Mazzoleni 2019 [63] | RCT | 39 | 67.5–68.74 | 24 F, 15 M | 0.8 | NA | 22 R, 17 L | FMA-UE = 34.1–34.2 | Subacute |
| Maxfield- Panker 2011 [61] | RCT | 18 | 59.8 ± 13.5 | 6 F, 12 M | 13–133 | NA | 8 L, 10 R | FMA-UE = 19.2 | Chronic |
| Straudi 2016 [65] | RCT | 23 | 58.2 ± 14.4 | 11 F, 12 M | 14.7 ± 13.1 | 4 H, 19 I | 8 R, 15 L | FMA-UE = 22.8 ± 14.9 | S & C |
| Triccas 2015 [46] | RCT | 23 | 63.4 ± 12.0 | 9 F, 14 M | 2–90 | 5 H, 18 I | NA | FMA-UE = 32.3 ± 16.6 | S & C |
| Lower Limb Rehabilitation | |||||||||
| Danzl 2013 [53] | RCT | 8 | 67.8 ± 12.6 | 4 F, 4 M | 33.5 ± 22.9 | 2 H, 6 I | 8 L | 10-MWT = 65.6–117.4 s | Chronic |
| Geroin 2011 [57] | RCT | 30 | 62.7 ± 6.4 | 7 F, 23 M | 26.4 ± 5.5 | NA | NA | 6-MWT = 156.1–162.9 m | Chronic |
| Leon 2017 [47] | N-RCT | 50 | 48.7 ± 11.2 | 15 F, 35 M | 1.9 ± 1.1 | 21 H, 29 I | 26 R, 24 L | FAC = 0.5–0.8 | Subacute |
| Picelli 2015 [37] | RCT | 30 | 62.5 | 8 F, 22 M | 56.4 | NA | NA | 6-MWT = 181.1–182.5 m | Chronic |
| Seo 2017 [64] | RCT | 21 | 62.0 ± 8.7 | 5 F, 16 M | 75.5–152.5 | 5 H, 16 I | 13 R, 8 L | FAC = 3.5–3.6 | Chronic |
Abbreviations. 6-MWT: 6 min walk test; 10-MWT: 10 m walk test; B: blind; C: chronic; COVR: crossover; F: female; FAC: functional ambulatory category; FMA-UE: the Fugl-Meyer Assessment for Upper Extremity; H: hemorrhagic; I: ischemic; L: left; M: male; N: no; NA: not available; R: right; RCT: randomized controlled trials; S: subacute; SIAS: stroke impairment assessment set; TSO: time since stroke onset.
Table 3.
Specific parameters for robotic training and stimulation.
| Study | Robotic Training | Joints | Support Type | Retention Period (Weeks) | tDCS Timing | Session | tDCS Targeted Areas | Parameter (Intensity, Duration, Size) |
|---|---|---|---|---|---|---|---|---|
| Upper Limb Rehabilitation | ||||||||
| Ang 2015 [51] | MI-BCI /MIT-Manus | Uni: S/E | E-E | 2 | B | 10 | Bi: A: iM1 (hand), C: cM1 (hand) | 1 mA, 20 min, NA |
| Chew 2020 [52] | MI-BCI /MIT-Manus | Uni: S/E | E-E | 4 | B | 10 | Bi: A: iM1 (hand), C: cM1 (hand) | 1 mA, 20 min, 35 cm2 |
| De Laet 2022 [54] | REAplan robot | Uni: S/E | E-E | 1 | B | 1 | Uni: A: cM1 (hand) C: cEyebrow | 1 mA, 30 min, 34 cm2 |
| Dehem 2018 [55] | REAplan robot | Uni: S/E | E-E | NA | D | 1 | Bi: A: iM1 (hand), C: cM1 (hand) | 1 mA, 20 min, 35 cm2 |
| Edwards 2019 [56] | MIT-Manus | Uni: WA | E-E | 24 | B | 36 | Uni: A: iM1 (hand), C: CSA | 2 mA, 20 min, 35 cm2 |
| Giacobbe 2013 [58] | InMotion3 wrist robot | Uni: W/H | E-E | NA | B, D, AF | 1 | Uni: A: iM1 (hand), C: CSA | 2 mA, 20 min, NA |
| Hesse 2011 [59] | Bi-Manu Track | Bi: W/H | E-E | 12 | D | 30 | Uni: A: iM1 (hand), C: CO Uni: A: CO, C: iM1 (hand) | 2 mA, 20 min, 35 cm2 |
| Hong 2017 [60] | MI-BCI /MIT-Manus | Uni: S/E | E-E | 4 | B | 10 | Bi: A: iM1 (hand), C: cM1 (hand) | 1 mA, 20 min, 35 cm2 |
| Hu 2021 [66] | MI-BCI /MIT-Manus | Uni: S/E | E-E | 2 | AF | 10 | Bi: A: iM1 (hand), C: cM1 (hand) | 1 mA, 20 min, NA |
| Kasashima 2015 [45] | MI-BCI /Motor-driven orthosis | Uni: F | E-E | 12 | B | 30 | Uni: A: iM1 (hand), C: CSA | 1 mA, 10 min, 35 cm2 |
| Mazzoleni 2015 [62] | InMotion3 wrist robot | Uni: W/H | E-E | NA | D | 16 | Uni: A: iM1 (hand), C: CO | 2 mA, 20 min, 35 cm2 |
| Mazzoleni 2019 [63] | InMotion3 wrist robot | Uni: W/H | E-E | NA | D | 30 | Uni: A: iM1 (hand), C: CO | 2 mA, 20 min, 35 cm2 |
| Maxfield- Panker 2011 [61] | ReoGo robotic device | Uni: S/E | E-E | 12 | D | 22 | Uni: A: iM1 (hand), C: CSA | 1 mA, 20 min, 35 cm2 |
| Straudi 2016 [65] | ReoGo robotic device | Uni: S/E | E-E | NA | D | 10 | Bi: A: iM1 (hand), C: cM1 (hand) | 1 mA, 30 min, 35 cm2 |
| Triccas 2015 [46] | Armeo® Spring arm robot | Uni: WA | Ekso | 12 | D | 18 | Uni: A: iM1 (hand), C: CSA | 1 mA, 20 min, 35 cm2 |
| Lower Limb Rehabilitation | ||||||||
| Danzl 2013 [53] | Lokomat | Bi: WL | Ekso | 4 | B | 12 | Bi: A: iM1 (leg), C: CSA | 2 mA, 20 min, 25 cm2 |
| Geroin 2011 [57] | Gait Trainer GT1 | Bi: WL | E-E | 2 | D | 10 | Bi: A: iM1 (leg), C: CO | 1.5 mA, 7 min, 35 cm2 |
| Leon 2017 [47] | Gait Trainer or Lokomat | Bi: WL | E-E or Ekso | NA | D | 20 | Bi: A: iM1 (leg), C: CSA | 2 mA, 20 min, 35 cm2 |
| Picelli 2015 [37] | G-EO System Evolution | Bi: WL | E-E | 2&4 | D | 10 | Uni: A: iM1 (hand), C: CO | 2 mA, 20 min, 35 cm2 |
| Seo 2017 [64] | Walkbot_ S-WALKBOT | Bi: WL | Ekso | 4 | B | 10 | Bi: A: iM1 (leg), C: CO | 2 mA, 20 min, 35 cm2 |
Abbreviations. A: anodal electrode; AF: after; B: before; C: cathodal electrode; c: contralateral; CO: contralateral orbit; CSA: contralateral supraorbital area; D: during; Ekso: exoskeleton; E-E: end-effector; F: finger; i: ipsilateral; MI-BCI: motor imagery brain–computer interface; NA: not available; S/E: shoulder/elbow; tDCS: transcranial direct current stimulation; WA: whole arm; WL: whole leg; W/H: wrist/hand.
Table 4.
Methodological quality assessment using PEDro Score.
| Upper Limb Rehabilitation Criteria | Ang 2015 [51] | Chew 2020 [52] | De Laet 2022 [54] | Dehem 2018 [55] | Edwards 2019 [56] | Giacobbe 2013 [58] | Hesse 2011 [59] | |
| 1. eligibility criteria were specified | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| 2. subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| 3. allocation was concealed | 0 | 1 | 1 | 0 | 1 | 0 | 1 | |
| 4. the groups were similar at baseline regarding the most important prognostic indicators | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| 5. there was blinding of all subjects | 1 | 1 | 1 | 1 | 1 | 0 | 1 | |
| 6. there was blinding of all therapists who administered the therapy | 0 | 1 | 0 | 0 | 1 | 0 | 1 | |
| 7. there was blinding of all assessors who measured at least one key outcome | 0 | 1 | 1 | 1 | 1 | 0 | 1 | |
| 8. measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups | 1 | 1 | 1 | 1 | 0 | 1 | 1 | |
| 9. all subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome were analyzed by “intention to treat” | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| 10. the results of between-group statistical comparisons are reported for at least one key outcome | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| 11. the study provides both point measures and measures of variability for at least one key outcome | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| Total | 8 | 11 | 10 | 9 | 10 | 7 | 11 | |
| Upper Limb Rehabilitation Criteria | Hong 2017 [60] | Hu 2021 [66] | Kasashima 2015 [45] | Mazzoleni 2015 [62] | Mazzoleni 2019 [63] | Maxfield-Panker 2011 [61] | Straudi 2016 [65] | Triccas2015 [46] |
| 1. eligibility criteria were specified | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 2. subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received) | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 |
| 3. allocation was concealed | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 |
| 4. the groups were similar at baseline regarding the most important prognostic indicators | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 5. there was blinding of all subjects | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| 6. there was blinding of all therapists who administered the therapy | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 7. there was blinding of all assessors who measured at least one key outcome | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 |
| 8. measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 9. all subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome were analyzed by “intention to treat” | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 10. the results of between-group statistical comparisons are reported for at least one key outcome | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 11. the study provides both point measures and measures of variability for at least one key outcome | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Total | 10 | 7 | 8 | 10 | 8 | 9 | 9 | 10 |
Lower Limb Rehabilitation | Danzl 2013 [53] | Geroin 2011 [57] | Leon 2017 [47] | Picelli 2015 [37] | Seo 2017 [64] | |||
| Criteria | ||||||||
| 1. eligibility criteria were specified | 1 | 1 | 1 | 1 | 1 | |||
| 2. subjects were randomly allocated to groups (in a crossover study, subjects were randomly allocated an order in which treatments were received) | 1 | 1 | 0 | 1 | 1 | |||
| 3. allocation was concealed | 0 | 1 | 0 | 1 | 1 | |||
| 4. the groups were similar at baseline regarding the most important prognostic indicators | 1 | 1 | 1 | 1 | 1 | |||
| 5. there was blinding of all subjects | 1 | 0 | 1 | 1 | 1 | |||
| 6. there was blinding of all therapists who administered the therapy | 1 | 0 | 0 | 0 | 1 | |||
| 7. there was blinding of all assessors who measured at least one key outcome | 1 | 1 | 0 | 1 | 1 | |||
| 8. measures of at least one key outcome were obtained from more than 85% of the subjects initially allocated to groups | 0 | 1 | 1 | 1 | 1 | |||
| 9. all subjects for whom outcome measures were available received the treatment or control condition as allocated or, where this was not the case, data for at least one key outcome were analyzed by “intention to treat” | 1 | 1 | 1 | 1 | 1 | |||
| 10. the results of between-group statistical comparisons are reported for at least one key outcome | 1 | 1 | 1 | 1 | 1 | |||
| 11. the study provides both point measures and measures of variability for at least one key outcome | 1 | 1 | 1 | 1 | 1 | |||
| Total | 9 | 9 | 7 | 10 | 11 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kim, R.-K.; Kang, N.; Desai, Z.; Cauraugh, J.H. A Meta-Analysis on Dual Protocols for Chronic Stroke Motor Recovery: Robotic Training and tDCS. Appl. Sci. 2023, 13, 1992. https://doi.org/10.3390/app13031992
AMA Style
Kim R-K, Kang N, Desai Z, Cauraugh JH. A Meta-Analysis on Dual Protocols for Chronic Stroke Motor Recovery: Robotic Training and tDCS. Applied Sciences. 2023; 13(3):1992. https://doi.org/10.3390/app13031992
Chicago/Turabian StyleKim, Rye-Kyeong, Nyeonju Kang, Zeel Desai, and James H. Cauraugh. 2023. "A Meta-Analysis on Dual Protocols for Chronic Stroke Motor Recovery: Robotic Training and tDCS" Applied Sciences 13, no. 3: 1992. https://doi.org/10.3390/app13031992
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.