
The Influence of the Menstrual Cycle and Oral Contraceptives on Knee Laxity or Anterior Cruciate Ligament Injury Risk: A Systematic Review
 , ,
, , 
Abstract
:1. Introduction
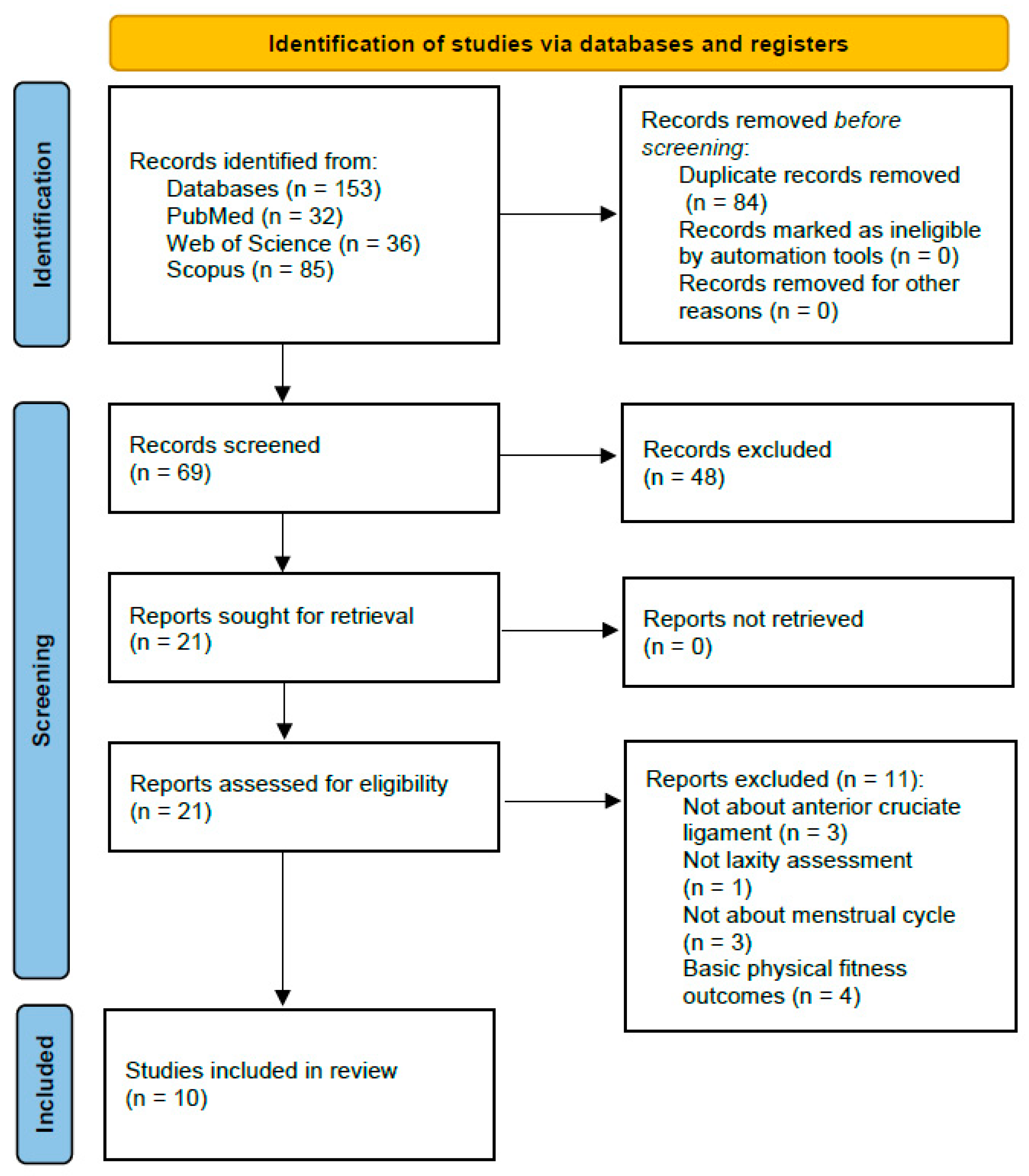
2. Methods
2.1. Study Design
2.2. Data Source
2.3. Inclusion/Exclusion Criteria
2.4. Data Extraction and Data Synthesis
2.5. Risk of Bias Assessment
3. Results
3.1. ACL Tears
3.2. Knee Laxity
3.3. Hormones
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Datson, N.; Drust, B.; Weston, M.; Jarman, I.H.; Lisboa, P.; Gregson, W. Match Physical Performance of Elite Female Soccer Players During International Competition. J. Strength Cond. Res. 2017, 31, 2379–2387. [Google Scholar] [CrossRef] [PubMed]
- Datson, N.; Hulton, A.; Andersson, H.; Lewis, T.; Weston, M.; Drust, B.; Gregson, W. Applied physiology of female soccer: An update. Sport. Med. 2014, 44, 1225–1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gebert, A.; Gerber, M.; Pühse, U.; Gassmann, P.; Stamm, H.; Lamprecht, M. Costs resulting from nonprofessional soccer injuries in Switzerland: A detailed analysis. J. Sport Health Sci. 2020, 9, 240–247. [Google Scholar] [CrossRef]
- Mufty, S.; Bollars, P.; Vanlommel, L.; Van Crombrugge, K.; Corten, K.; Bellemans, J. Injuries in male versus female soccer players: Epidemiology of a nationwide study. Acta Orthop. Belg. 2015, 81, 289–295. [Google Scholar] [PubMed]
- Roos, K.G.; Wasserman, E.B.; Dalton, S.L.; Gray, A.; Djoko, A.; Dompier, T.P.; Kerr, Z.Y. Epidemiology of 3825 injuries sustained in six seasons of National Collegiate Athletic Association men’s and women’s soccer (2009/2010–2014/2015). Br. J. Sports Med. 2017, 51, 1029–1034. [Google Scholar] [CrossRef] [PubMed]
- Somerson, J.S.; Isby, I.J.; Hagen, M.S.; Kweon, C.Y.; Gee, A.O. The Menstrual Cycle May Affect Anterior Knee Laxity and the Rate of Anterior Cruciate Ligament Rupture: A Systematic Review and Meta-Analysis. JBJS Rev. 2019, 7, e2. [Google Scholar] [CrossRef]
- Larruskain, J.; Lekue, J.A.; Diaz, N.; Odriozola, A.; Gil, S.M. A comparison of injuries in elite male and female football players: A five-season prospective study. Scand. J. Med. Sci. Sports 2018, 28, 237–245. [Google Scholar] [CrossRef]
- Lin, C.Y.; Casey, E.; Herman, D.C.; Katz, N.; Tenforde, A.S. Sex Differences in Common Sports Injuries. PM&R 2018, 10, 1073–1082. [Google Scholar]
- Shafiei, S.E.; Peyvandi, S.; Kariminasab, M.H.; Azar, M.S.; Daneshpoor, S.M.M.; Khalilian, A.; Aghajantabar, Z. Knee Laxity Variations in the Menstrual Cycle in Female Athletes Referred to the Orthopedic Clinic. Asian J. Sports Med. 2016, 7, e30199. [Google Scholar] [CrossRef] [Green Version]
- Lovering, R.M.; Romani, W.A. Effect of testosterone on the female anterior cruciate ligament. Am. J. Physiol. Integr. Comp. Physiol. 2005, 289, R15–R22. [Google Scholar] [CrossRef] [Green Version]
- Gosselin, M. Menstrual Cycle: Signs and Symptoms, Psychological/Behavioral Changes and Abnormalities: Signs and Symptoms, Psychological/Behavioral Changes and Abnormalities; Nova Science Publishers Incorporated: Hauppauge, NY, USA, 2013. [Google Scholar]
- Maruyama, S.; Yamazaki, T.; Sato, Y.; Suzuki, Y.; Shimizu, S.; Ikezu, M.; Kaneko, F.; Matsuzawa, K.; Hirabayashi, R.; Edama, M. Relationship Between Anterior Knee Laxity and General Joint Laxity During the Menstrual Cycle. Orthop. J. Sports Med. 2021, 9, 2325967121993045. [Google Scholar] [CrossRef] [PubMed]
- Knudtson, J.; McLaughlin, J.E. Endocrinologie de la Reproduction Féminine; MSD Manuals: Rahway, NJ, USA, 2019. [Google Scholar]
- Samuelson, K.; Balk, E.M.; Sevetson, E.L.; Fleming, B.C. Limited Evidence Suggests a Protective Association Between Oral Contraceptive Pill Use and Anterior Cruciate Ligament Injuries in Females: A Systematic Review. Sports Health A Multidiscip. Approach 2017, 9, 498–510. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.-D.; Shultz, S.J. Sex Differences in Clinical Measures of Lower Extremity Alignment. J. Orthop. Sports Phys. Ther. 2007, 37, 389–398. [Google Scholar] [CrossRef]
- Shultz, S.J.; Sander, T.C.; Kirk, S.E.; Perrin, D.H. Sex differences in knee joint laxity change across the female menstrual cycle. J. Sports Med. Phys. Fitness 2005, 45, 594–603. [Google Scholar]
- Beynnon, B.D.; Bernstein, I.M.; Belisle, A.; Brattbakk, B.; Devanny, P.; Risinger, R.; Durant, D. The Effect of Estradiol and Progesterone on Knee and Ankle Joint Laxity. Am. J. Sports Med. 2005, 33, 1298–1304. [Google Scholar] [CrossRef] [PubMed]
- Shultz, S.J.; Nguyen, A.-D.; Schutz, R.J. Differences in Lower Extremity Anatomical and Postural Characteristics in Males and Females Between Maturation Groups. J. Orthop. Sports Phys. Ther. 2008, 38, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.H.; Al-Shaikh, R.; Panossian, V.; Yang, R.S.; Nelson, S.D.; Soleiman, N.; Finerman, G.A.M.; Lane, J.M. Primary immunolocalization of estrogen and progesterone target cells in the human anterior cruciate ligament. J. Orthop. Res. 1996, 14, 526–533. [Google Scholar] [CrossRef]
- Yu, W.D.; Panossian, V.; Hatch, J.D.; Liu, S.H.; A Finerman, G. Combined Effects of Estrogen and Progesterone on the Anterior Cruciate Ligament. Clin. Orthop. Relat. Res. 2001, 383, 268–281. [Google Scholar] [CrossRef]
- Karageanes, S.J.; Blackburn, K.; Vangelos, Z.A. The association of the menstrual cycle with the laxity of the anterior cruciate ligament in adolescent female athletes. Clin. J. Sport Med. 2000, 10, 162–168. [Google Scholar] [CrossRef]
- Schmitz, R.J.; Shultz, S.J. Anterior knee stiffness changes in laxity “responders” versus “nonresponders” across the menstrual cycle. J. Athl. Train. 2013, 48, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Faryniarz, D.A.; Bhargava, M.; Lajam, C.; Attia, E.T.; Hannafin, J.A. Quantitation of estrogen receptors and relaxin binding in human anterior cruciate ligament fibroblasts. Vitr. Cell. Dev. Biol. Anim. 2006, 42, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Herzberg, S.D.; Motu’apuaka, M.L.; Lambert, W.; Fu, R.; Brady, J.; Guise, J.-M. The Effect of Menstrual Cycle and Contraceptives on ACL Injuries and Laxity: A Systematic Review and Meta-analysis. Orthop. J. Sport. Med. 2017, 5, 2325967117718781. [Google Scholar] [CrossRef] [PubMed]
- DeFroda, S.F.; Bokshan, S.L.; Worobey, S.; Ready, L.; Daniels, A.H.; Owens, B.D. Oral contraceptives provide protection against anterior cruciate ligament tears: A national database study of 165,748 female patients. Phys. Sportsmed. 2019, 47, 416–420. [Google Scholar] [CrossRef] [PubMed]
- Gray, A.M.; Gugala, Z.; Baillargeon, J.G. Effects of Oral Contraceptive Use on Anterior Cruciate Ligament Injury Epidemiology. Med. Sci. Sports Exerc. 2016, 48, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Herzog, M.M.; Young, J.C.; Lund, J.L.; Pate, V.; Mack, C.D.; Marshall, S.W. Oral contraceptive use and anterior cruciate ligament injury: Comparison of active comparator new user cohort and case-control study designs. Inj. Epidemiol. 2020, 7, 53. [Google Scholar] [CrossRef]
- Khowailed, I.A.; Petrofsky, J.; Lohman, E.; Daher, N.; Mohamed, O. 17β-Estradiol Induced Effects on Anterior Cruciate Ligament Laxness and Neuromuscular Activation Patterns in Female Runners. J. Womens Health 2015, 24, 670–680. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.; Petrofsky, J.S.; Yim, J. Do Oral Contraceptives Alter Knee Ligament Damage with Heavy Exercise? Tohoku J. Exp. Med. 2015, 237, 51–56. [Google Scholar] [CrossRef] [Green Version]
- Nose-Ogura, S.; Yoshino, O.; Yamada-Nomoto, K.; Nakamura, M.; Harada, M.; Dohi, M.; Okuwaki, T.; Osuga, Y.; Kawahara, T.; Saito, S. Oral contraceptive therapy reduces serum relaxin-2 in elite female athletes. J. Obstet. Gynaecol. Res. 2017, 43, 530–535. [Google Scholar] [CrossRef]
- Shagawa, M.; Maruyama, S.; Sekine, C.; Yokota, H.; Hirabayashi, R.; Hirata, A.; Yokoyama, M.; Edama, M. Comparison of anterior knee laxity, stiffness, genu recurvatum, and general joint laxity in the late follicular phase and the ovulatory phase of the menstrual cycle. BMC Musculoskelet. Disord. 2021, 22, 886. [Google Scholar] [CrossRef]
- Stijak, L.; Kadija, M.; Djulejić, V.; Aksić, M.; Petronijević, N.; Marković, B.; Radonjić, V.; Bumbaširević, M.; Filipović, B. The influence of sex hormones on anterior cruciate ligament rupture: Female study. Knee Surg. Sport. Traumatol. Arthrosc. 2015, 23, 2742–2749. [Google Scholar] [CrossRef]
- Law, M.; Stewart, D.; Pollock, N.; Letts, L.; Bosch, J.; Westmorland, M. Guidelines for Critical Review Form—Quantitative Studies; McMaster University Occupational Therapy Evidence-Based Practice Research Group: Hamilton, ON, Canada, 1998. [Google Scholar]
- Bisciotti, G.N.; Chamari, K.; Cena, E.; Bisciotti, A.; Corsini, A.; Volpi, P. Anterior cruciate ligament injury risk factors in football. J. Sports Med. Phys. Fitness 2019, 59, 1724–1738. [Google Scholar] [CrossRef] [PubMed]
- Sung, E.-S.; Kim, J.-H. The influence of ovulation on postural stability (Biodex Balance System) in young female. J. Exerc. Rehabil. 2018, 14, 638–642. [Google Scholar] [CrossRef] [PubMed]
- Noyola-Martínez, N.; Halhali, A.; Barrera, D. Steroid hormones and pregnancy. Gynecol. Endocrinol. 2019, 35, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Hackney, A. Sex Hormones, Exercise and Women, 1st ed.; Springer: Cham, Switzerland, 2017; pp. 113–138. [Google Scholar]
- Orio, F.; Muscogiuri, G.; Ascione, A.; Marciano, F.; Volpe, A.; La Sala, G.; Savastano, S.; Colao, A.; Palomba, S. Effects of physical exercise on the female reproductive system. Minerva Endocrinol. 2013, 38, 305–319. [Google Scholar]
- Reynolds, T.A.; Makhanova, A.; Marcinkowska, U.M.; Jasienska, G.; McNulty, J.K.; Eckel, L.A.; Nikonova, L.; Maner, J.K. Progesterone and women’s anxiety across the menstrual cycle. Horm. Behav. 2018, 102, 34–40. [Google Scholar] [CrossRef]
- Nillni, Y.I.; Toufexis, D.J.; Rohan, K.J. Anxiety sensitivity, the menstrual cycle, and panic disorder: A putative neuroendocrine and psychological interaction. Clin. Psychol. Rev. 2011, 31, 1183–1191. [Google Scholar] [CrossRef]


{kind=link}
| Authors | Year | Objective | Type of Study | Participants | Age | Specificity | Study Quality |
|---|---|---|---|---|---|---|---|
| DeFroda et al. [25] | 2019 | To examine the effects of OC usage on ACL tear and subsequent reconstruction | Case-controls | 82,874 | 15–49 years | Database | E |
| Gray et al. [26] | 2016 | To determine if women undergoing anterior cruciate ligament surgical reconstruction were less likely to use oral contraceptives than a matched noninjured population | Case-controls | 12,819 | 15–39 years | Database | E |
| Herzog et al. [27] | 2020 | Quantifying the association between OC use and ACL injury | Cohort | 2,992,084 | 13–45 years | Database | A |
| Khowailed et al. [28] | 2015 | Investigating the effects of 17ᵝ-estradiol across phases of the menstrual cycle on neuromuscular control patterns of ACL laxity during running | transverse | 12 | 25.6 ± 3.7 years | Runners | E |
| Lee et al. [29] | 2015 | To study the difference in ACL laxity after squat exercise in healthy women between OC users and non-OC users. | Cohort | 40 | 25.2 ± 2.2 years | Low to moderate PA | E |
| Maruyama et al. [12] | 2021 | To determine the relationship between knee joint looseness, stiffness, and general joint looseness in relation to the menstrual cycle | transverse | 15 | 21 ± 0.2 years | female students Low to moderate PA | E |
| Nose-Ogura et al. [30] | 2017 | To study the concentration of relaxin-2 during the menstrual cycle in athletes without and with OC. | transverse | 106 | 22 ± 3 years | athletes | E |
| Shafiei et al. [9] | 2016 | Comparing knee laxity changes in the menstrual cycle in female athletes | transverse | 40 | 25.5 ± 5.12 years | athletes | A |
| Shagawa et al. [31] | 2021 | To examine changes in AKL, stiffness, GR and GJL during the late follicular phase and ovulation | transverse | 15 | 21 ± 0.3 years | E | E |
| Stijak et al. [32] | 2015 | To determine the difference in testosterone, 17ᵝ estradiol and progesterone concentrations between patients with and without ACL tear, and the possible effect of these hormones on generalized joint laxity | Case-controls | 24 | 16–37 years | athletes | E |
| Authors | Variables Studied | Method of Measurement of Variables | ACL Tear | Contraceptive Method | Hormones Studied | Results | |
|---|---|---|---|---|---|---|---|
| DeFroda et al. 2019 [25] | ACL injury | Follow-up over time | Case: surgical reconstruction of ACL with OC Controls: surgical reconstruction of ACL without OC | 569 ACL reconstruction patients in the non-OC group, and 465 patients in the OC group. | / | OC users: 18% decrease in the risk of ACL tear requiring reconstruction OC users 15–19 age group: 63% reduction in tears | |
| Gray et al. 2016 [26] | ACL injury | Follow-up over time | Case: surgical reconstruction of the ACL | 12,819 OC | / | 15–19 age group with ACL repair surgery: not use OC 1.22 times > controls (12 months prior to injury) (p < 0.0001) 25–39 age group: use OC 1.1 to 1.16 times > controls OC users: 18% fewer ACL injuries than non-users (15–19 age group) | |
| Herzog et al. 2020 [27] | ACL injury | Follow-up over time | 3571 at OC 1620 at IUD | OC (exposed) IUD (unexposed) | / | No difference in the risk of ACL injury in OCs and IUDs | |
| Khowailed et al. 2015 [28] | Knee laxity [estradiol] Neuromuscular control | KT-2000 Cobas e602 blood test (Roche/Hitachi) → EMG | No | No | Estradiol | ↑ ATT: ovulation (5.75 ± 0.47) (p < 0.01) ↓ ATT: follicular (4.18 ± 0.27) (p < 0.01) [17ᵝ estradiol] ↓ menstruation (34.14 ± 15.47 pg/mL) [17ᵝ estradiol] ↑ ovulation (207.74 ± 53.42 pg/mL) [17ᵝ estradiol]ovulation > [17ᵝ estradiol]follicular (p < 0.01) | |
| Lee et al. 2015 [29] | ACL laxity Pain | KT-2000 EVA | No | 25 with normal cycle 15 with OC | / | Decreased ACL laxity (OC users) compared to non-OC users before and after strenuous exercise Pain after exercise (OC) > pain after exercise (non-OC) | |
| Maruyama et al. 2021 [12] | AKL Stiffness GJL GR | KS-measurement Δ force/Δ displacement University of Tokyo joint laxity test Item 4 of the GJL test, goniometer | No | No | / | GR | No GR |
| AKL (89N and 133N) Ovulatory phase > early follicular phase | No difference in AKL between phases | ||||||
| AKL: GR (ovulation) > no GR GJL: No differences between GR and non-GR AKL, stiffness, GJL: No difference between phases | |||||||
| Nose-Ogura et al. 2017 [30] | [relaxin-2] [sex hormones] | Immunoassay (quantikin Human relaxin-2) CLIA kit | No | 16 with OC 77 eumenorhea 13 amenorrhea | relaxin-2 sex hormones | [relaxin-2]luteal > [relaxin-2]follicular, ovulatory in eumhenorrea [relaxin-2] at eumennorhee > [relaxin-2] at OC luteal phase: [relaxin-2] > 6.0 pg/mL in 36.8% of FDR cases. ACL injury correlation between relaxin-2 and progesterone in CM phases except luteal phase | |
| Shafiei et al. 2016 [9] | Knee laxity (ACL) [sex hormones] | Lachman Front drawer ELISA and DEMEDITEC kit | No | No | [estrogen] [progesterone] | No difference for ACL laxity nor hormonal levels. No relationship between menstrual cycle phases and knee laxity | |
| Shagawa et al. 2021 [31] | AKL stiffness GJL GR [estradiol] | KS-measurement Δ force/Δ displacement University of Tokyo joint laxity test Item 4 of the GJL test, goniometer Saliva sample Ovulation kit (+T° control: thermometer) | No | No | Estradiol | [oestradiol] ovulatory > late follicular [oestradiol] (p = 0.018) No differences between AKL or rigidity of the follicular phase and the ovulatory phase GR and GJL ↑ during ovulatory phase > follicular phase Changes in [estradiol] during the cycle can affect changes in GR and GJL | |
| Stijak et al. 2015 [32] | GJL [sex hormones] | Laxity score (Beighton, Solomon, Soskolne) sample → enzyme immunoassay Salimetrics | Yes contactless (case) No (control) | No | [17ᵝ estradiol] [progesterone] [testosterone] | Significant differences in [17ᵝ estradiol], [progesterone], and [testosterone] between the two groups Lower [hormones] in women with ACL tears | |
| Criteria | T | % | QM | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Article | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | |||
| Shagawa et al., (2021) [31] | 1 | 1 | 1 (c) | 1 | 0 | 1 | 1 | 1 | N/A | 1 | 1 | 1 | 1 | 1 | 1 | 13/14 | 93% | E |
| Maruyama et al., (2021) [12] | 1 | 1 | 1 (c) | 1 | 0 | 1 | 1 | 1 | N/A | 1 | 1 | 1 | 1 | 1 | 1 | 13/14 | 93% | E |
| Herzog et al., (2020) [27] | 1 | 1 | 1 (a) | 0 | 0 | 1 | 1 | 0 | N/A | 0 | 0 | 1 | 1 | 0 | 1 | 8/14 | 57% | A |
| DeFroda et al., (2019) [25] | 1 | 1 | 1 (b) | 0 | 0 | 1 | 1 | 0 | N/A | 0 | 1 | 1 | 1 | 0 | 1 | 9/14 | 64% | A |
| Nose-Ogura et al., (2017) [30] | 1 | 1 | 1 (c) | 1 | 0 | 1 | 1 | 1 | N/A | 1 | 1 | 1 | 1 | 1 | 1 | 13/14 | 93% | E |
| Gray et al., (2016) [26] | 1 | 1 | 1 (b) | 1 | 1 | 1 | 1 | 0 | N/A | 0 | 1 | 1 | 1 | 0 | 1 | 11/14 | 79% | H |
| Shafiei et al., (2016) [9] | 1 | 1 | 1 (c) | 1 | 0 | 1 | 1 | 0 | N/A | 0 | 1 | 1 | 0 | 0 | 0 | 8/14 | 57% | A |
| Lee et al., (2015) [29] | 1 | 1 | 1 (a) | 1 | 0 | 1 | 1 | 1 | N/A | 1 | 1 | 1 | 1 | 0 | 1 | 12/14 | 86% | E |
| Stijak et al., (2015) [32] | 1 | 1 | 1 (b) | 1 | 0 | 1 | 1 | 1 | N/A | 1 | 1 | 1 | 1 | 0 | 1 | 12/14 | 86% | E |
| Khowailed et al., (2015) [28] | 1 | 1 | 1 (c) | 1 | 1 | 1 | 1 | 1 | N/A | 1 | 1 | 1 | 1 | 0 | 1 | 13/14 | 93% | E |
| Total | 8 | 8 | 8 | 7 | 1 | 8 | 8 | 6 | / | 6 | 7 | 8 | 7 | 3 | 7 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moriceau, J.; Fevre, A.; Domínguez-Balmaseda, D.; González-de-la-Flor, Á.; Simón-Areces, J.; García-Pérez-de-Sevilla, G. The Influence of the Menstrual Cycle and Oral Contraceptives on Knee Laxity or Anterior Cruciate Ligament Injury Risk: A Systematic Review. Appl. Sci. 2022, 12, 12627. https://doi.org/10.3390/app122412627
Moriceau J, Fevre A, Domínguez-Balmaseda D, González-de-la-Flor Á, Simón-Areces J, García-Pérez-de-Sevilla G. The Influence of the Menstrual Cycle and Oral Contraceptives on Knee Laxity or Anterior Cruciate Ligament Injury Risk: A Systematic Review. Applied Sciences. 2022; 12(24):12627. https://doi.org/10.3390/app122412627
Chicago/Turabian StyleMoriceau, Juliette, Amandine Fevre, Diego Domínguez-Balmaseda, Ángel González-de-la-Flor, Julia Simón-Areces, and Guillermo García-Pérez-de-Sevilla. 2022. "The Influence of the Menstrual Cycle and Oral Contraceptives on Knee Laxity or Anterior Cruciate Ligament Injury Risk: A Systematic Review" Applied Sciences 12, no. 24: 12627. https://doi.org/10.3390/app122412627