
Damage to Oral Mucosae Induced by Weekend Alcohol Consumption: The Role of Gender and Alcohol Concentration

 , , , , ,
, , , , ,  and
and 
Abstract
:1. Introduction
1.1. Oral Cavity
1.2. Alcohol Effects on Oral Cavity
2. Materials and Methods
2.1. Experimental Design
- (a)
- Control female rats to which only water and food ad libitum were administered without ethanol.
- (b)
- Female rats to which 40% ethanol with ad libitum consumption was administered to the drink container, 2 days a week for 3 months.
- (c)
- Female rats to which 5% ethanol with ad libitum consumption was administered to the drink container, 2 days a week for 3 months.
- (d)
- Control male rats to which only water and food ad libitum were administered without ethanol.
- (e)
- Male rats to which 40% ethanol was administered with ad libitum consumption, 2 days a week for 3 months.
- (f)
- Male rats to which 5% ethanol was administered with ad libitum consumption, 2 days a week for 3 months.
2.2. Microscopic Analysis
3. Results
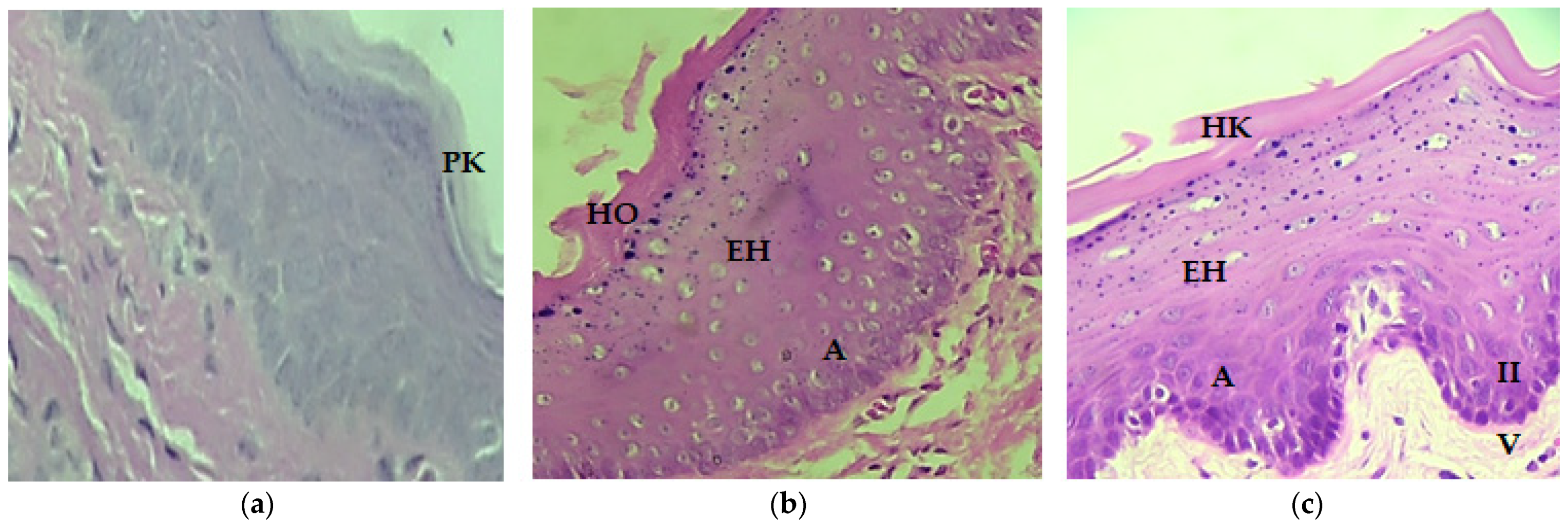
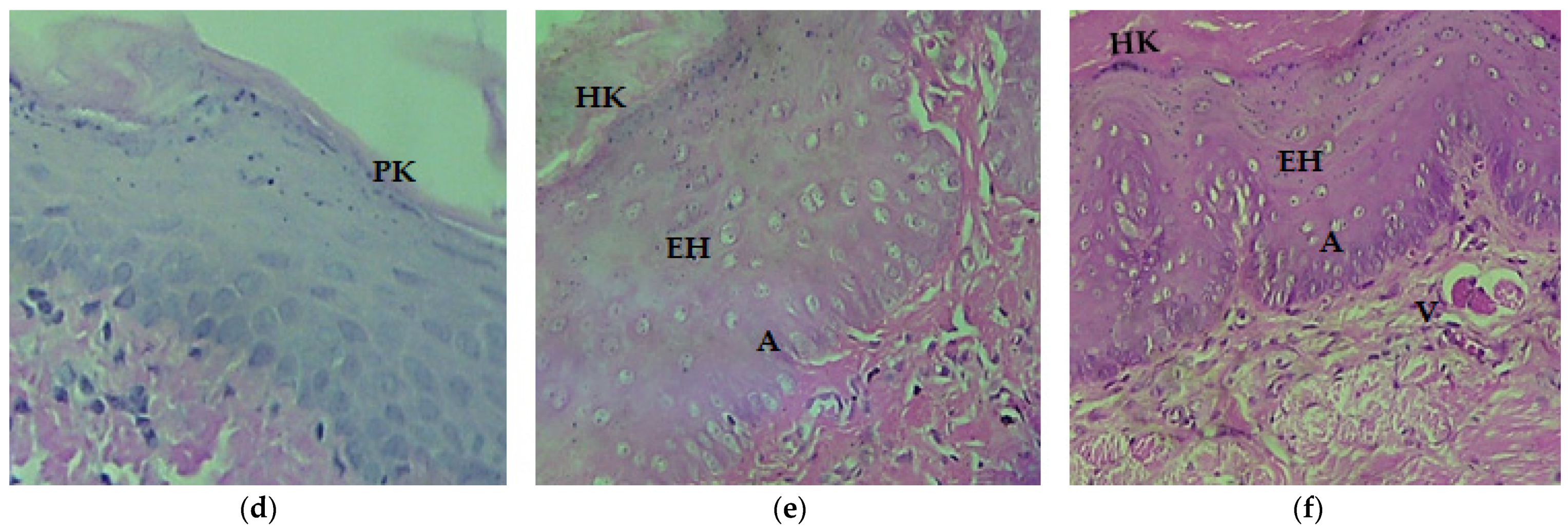
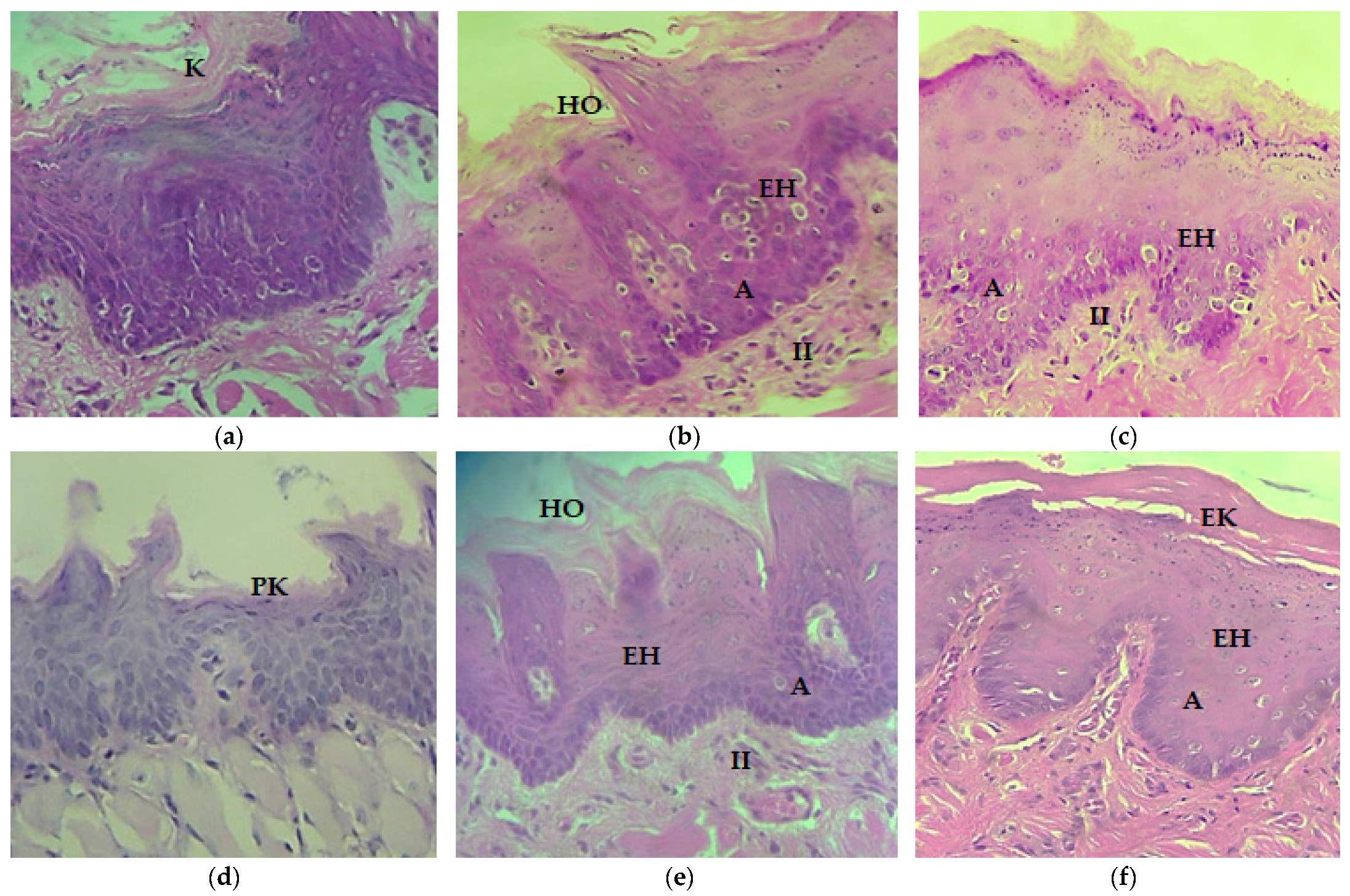
Histological Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Conflicts of Interest
References
- WHO. Global Status Report on Alcohol and Health 2018; License: CC BY-NC-SA 3.0 IGO; World Health Organization: Geneva, Switzerland, 2018; p. 450.
- De Souza, D.P.; Areco, K.N.; da Silveira Filho, D.X. Alcohol and alcoholism among Brazilian adolescent public-school students. Rev. Saúde Pública 2005, 39, 585–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjet, C.; Borges, G.; Méndez, E.; Casanova, L.; Medina-Mora, M.E. Adolescent alcohol use and alcohol use disorders in Mexico City. Drug Alcohol Depend. 2014, 136, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Aguirre, A.A.; Alonso Castillo, M.M.; Zanetti, A.C. Alcohol consumption and self esteem in adolescents. Rev. Lat.-Am. Enferm. 2010, 18, 634–640. [Google Scholar] [CrossRef] [Green Version]
- González-Bautista, E.; Zavala-Arciniega, L.; Rivera-Rivera, L.; Leyva-López, A.; Natera-Rey, G.; Reynales-Shigematsu, L.M. Social factors associated with tobacco and alcohol consumption in Mexican adolescents from populations under 100,000 inhabitants. Salud Publica Mex. 2019, 61, 764–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoes, L.; Dok, R.; Verstrepen, K.J.; Nuyts, S. Ethanol-Induced Cell Damage Can Result in the Development of Oral Tumors. Cancers 2021, 13, 3846. [Google Scholar] [CrossRef]
- Room, R.; Babor, T.; Rehm, J. Alcohol and public health. Lancet 2005, 365, 519–530. [Google Scholar] [CrossRef]
- Griswold, M.G.; Fullman, N.; Hawley, C.; Arian, N.; Zimsen, S.R.M.; Tymeson, H.D.; Venkateswaran, V.; Tapp, A.D.; Forouzanfar, M.H.; Salama, J.S.; et al. Alcohol use and burden for 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018, 392, 1015–1035. [Google Scholar] [CrossRef] [Green Version]
- INPRFM. Encuesta Nacional de Consumo de Drogas, Alcohol y Tabaco 2016–2017: Reporte de Alcohol; Instituto Nacional de Psiquiatría Ramón de la Fuente Muñíz, Instituto Nacional de Salud Pública, Comisión Contra las Adicciones, Secretaría de Salud: Ciudad de México, Mexico, 2017. [Google Scholar]
- Jovanovic, A.; Schulten, E.A.; Kostense, P.J.; Snow, G.B.; van der Waal, I. Tobacco and alcohol related to the anatomical site of oral squamous cell carcinoma. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 1993, 22, 459–462. [Google Scholar] [CrossRef]
- Carrard, V.C.; Pires, A.S.; Mendez, M.; Pasquali, M.A.; Badauy, C.M.; Lauxen, I.S.; Moreira, J.C.; Sant’Ana Filho, M. Exploring the mechanisms of alcohol-related damage in oral mucosa—Is oxidative stress associated with the increase in cell proliferation in rat tongue epithelium? Pharm. Biol. 2013, 51, 160–169. [Google Scholar] [CrossRef]
- Bagnardi, V.; Blangiardo, M.; La Vecchia, C.; Corrao, G. A meta-analysis of alcohol drinking and cancer risk. Br. J. Cancer 2001, 85, 1700–1705. [Google Scholar] [CrossRef]
- Moreno-López, L.A.; Esparza-Gómez, G.C.; González-Navarro, A.; Cerero-Lapiedra, R.; González-Hernández, M.J.; Domínguez-Rojas, V. Risk of oral cancer associated with tobacco smoking, alcohol consumption and oral hygiene: A case-control study in Madrid, Spain. Oral Oncol. 2000, 36, 170–174. [Google Scholar] [CrossRef]
- Fioretti, F.; Bosetti, C.; Tavani, A.; Franceschi, S.; La Vecchia, C. Risk factors for oral and pharyngeal cancer in never smokers. Oral Oncol. 1999, 35, 375–378. [Google Scholar] [CrossRef]
- Goldstein, B.Y.; Chang, S.C.; Hashibe, M.; La Vecchia, C.; Zhang, Z.F. Alcohol consumption and cancers of the oral cavity and pharynx from 1988 to 2009: An update. Eur. J. Cancer Prev. Off. J. Eur. Cancer Prev. Organ. (ECP) 2010, 19, 431–465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wight, A.J.; Ogden, G.R. Possible mechanisms by which alcohol may influence the development of oral cancer—A review. Oral Oncol. 1998, 34, 441–447. [Google Scholar] [CrossRef]
- Carrard, V.C.; Filho, M.S.; Rados, P.V.; Chaves, A.C.; Lauxen Ida, S. Quantification of silver-staining nucleolar organizer region in epithelial cells of tongue of mice after exposure to, or intake of, alcohol. Alcohol 2004, 34, 233–238. [Google Scholar] [CrossRef]
- Mandel, L.; Hamele-Bena, D. Alcoholic parotid sialadenosis. J. Am. Dent. Assoc. (1939) 1997, 128, 1411–1415. [Google Scholar] [CrossRef]
- Khairnar, M.R.; Wadgave, U.; Khairnar, S.M. Effect of Alcoholism on Oral Health: A Review. J. Alcohol Drug Depend. 2017, 5, 1–4. [Google Scholar] [CrossRef]
- Guggenheimer, J.; Close, J.M.; Eghtesad, B. Sialadenosis in patients with advanced liver disease. Head Neck Pathol. 2009, 3, 100–105. [Google Scholar] [CrossRef] [Green Version]
- Chilla, R. Sialadenosis of the salivary glands of the head. Studies on the physiology and pathophysiology of parotid secretion. Adv. Oto-Rhino-Laryngol. 1981, 26, 1–38. [Google Scholar]
- Dunkley, R.P.; Carson, R.M. Dental requirements of the hospitalized alcoholic patient. J. Am. Dent. Assoc. (1939) 1968, 76, 800–803. [Google Scholar] [CrossRef]
- Niquille, M.; Burnand, B.; Magnenat, P.; Paccaud, F.; Yersin, B. Dental disease among alcoholic individuals: A comparative study of hospitalized patients. J. Gen. Intern. Med. 1993, 8, 470–475. [Google Scholar] [CrossRef]
- Shepherd, S. Alcohol consumption a risk factor for periodontal disease. Evid.-Based Dent. 2011, 12, 76. [Google Scholar] [CrossRef] [Green Version]
- Himmerich, H.; Anghelescu, I.; Klawe, C.; Szegedi, A. Vitamin B12 and hepatic enzyme serum levels correlate in male alcohol-dependent patients. Alcohol Alcohol. 2001, 36, 26–28. [Google Scholar] [CrossRef] [PubMed]
- Stornetta, A.; Guidolin, V.; Balbo, S. Alcohol-Derived Acetaldehyde Exposure in the Oral Cavity. Cancers 2018, 10, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figuero Ruiz, E.; Carretero Peláez, M.A.; Cerero Lapiedra, R.; Esparza Gómez, G.; Moreno López, L.A. Effects of the consumption of alcohol in the oral cavity: Relationship with oral cancer. Med. Oral Organo Of. Soc. Esp. Med. Oral Acad. Iberoam. Patol. Med. Bucal 2004, 9, 14–23. [Google Scholar]
- Ogden, G.R.; Wight, A.J. Aetiology of oral cancer: Alcohol. Br. J. Oral Maxillofac. Surg. 1998, 36, 247–251. [Google Scholar] [CrossRef]
- Reidy, J.; McHugh, E.; Stassen, L.F. A review of the relationship between alcohol and oral cancer. Surg. J. R. Coll. Surg. Edinb. Irel. 2011, 9, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Seitz, H.K.; Matsuzaki, S.; Yokoyama, A.; Homann, N.; Väkeväinen, S.; Wang, X.D. Alcohol and cancer. Alcohol. Clin. Exp. Res. 2001, 25, 137S–143S. [Google Scholar] [CrossRef]
- Valentine, J.A.; Scott, J.; West, C.R.; St Hill, C.A. A histological analysis of the early effects of alcohol and tobacco usage on human lingual epithelium. J. Oral Pathol. 1985, 14, 654–665. [Google Scholar] [CrossRef]
- Mascrès, C.; Ming-Wen, F.; Joly, J.G. Morphologic changes of the esophageal mucosa in the rat after chronic alcohol ingestion. Exp. Pathol. 1984, 25, 147–153. [Google Scholar] [CrossRef]
- Maier, H.; Weidauer, H.; Zöller, J.; Seitz, H.K.; Flentje, M.; Mall, G.; Born, I.A. Effect of chronic alcohol consumption on the morphology of the oral mucosa. Alcohol. Clin. Exp. Res. 1994, 18, 387–391. [Google Scholar] [CrossRef] [PubMed]
- Born, I.A.; Zöller, J.; Weidauer, H.; Maier, H. Effects of chronic alcohol drinking on mouth mucosa. A morphometric study. Laryngo-Rhino-Otol. 1996, 75, 754–758. [Google Scholar] [CrossRef] [PubMed]
- Maier, H.; Tisch, M.; Schneeberg, E.; Born, A. An association of chronic alcohol consumption with morphological alterations of the laryngeal mucosa in rats. Eur. Arch. Oto-Rhino-Laryngol. Off. J. Eur. Fed. Oto-Rhino-Laryngol. Soc. (EUFOS) Affil. Ger. Soc. Oto-Rhino-Laryngol.-Head Neck Surg. 1999, 256, 247–249. [Google Scholar] [CrossRef] [PubMed]
- Müller, P.; Hepke, B.; Meldau, U.; Raabe, G. Tissue damage in the rabbit oral mucosa by acute and chronic direct toxic action of different alcohol concentrations. Exp. Pathol. 1983, 24, 171–181. [Google Scholar] [CrossRef]
- Howie, N.M.; Trigkas, T.K.; Cruchley, A.T.; Wertz, P.W.; Squier, C.A.; Williams, D.M. Short-term exposure to alcohol increases the permeability of human oral mucosa. Oral Dis. 2001, 7, 349–354. [Google Scholar] [CrossRef]
- Squier, C.A.; Kremer, M.J.; Wertz, P.W. Effect of ethanol on lipid metabolism and epithelial permeability barrier of skin and oral mucosa in the rat. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 2003, 32, 595–599. [Google Scholar] [CrossRef]
- Feng, L.; Wang, L. Effects of alcohol on the morphological and structural changes in oral mucosa. Pak. J. Med. Sci. 2013, 29, 1046–1049. [Google Scholar] [CrossRef]
- Srinivasamurthy, B.C.; Balamurugesan, K.; Sathishkumar, N.; Prakash, M.; Bhat, R.V. Cytomorphometric Study of Changes in Buccal Mucosal Cells in Alcoholics. Adv. Biomed. Res. 2020, 9, 48. [Google Scholar] [CrossRef]
- Paquot, N. The metabolism of alcohol. Rev. Med. Liege 2019, 74, 265–267. [Google Scholar]
- Homann, N.; Jousimies-Somer, H.; Jokelainen, K.; Heine, R.; Salaspuro, M. High acetaldehyde levels in saliva after ethanol consumption: Methodological aspects and pathogenetic implications. Carcinogenesis 1997, 18, 1739–1743. [Google Scholar] [CrossRef] [PubMed]
- Homann, N.; Tillonen, J.; Rintamäki, H.; Salaspuro, M.; Lindqvist, C.; Meurman, J.H. Poor dental status increases acetaldehyde production from ethanol in saliva: A possible link to increased oral cancer risk among heavy drinkers. Oral Oncol. 2001, 37, 153–158. [Google Scholar] [CrossRef]
- Homann, N.; Tillonen, J.; Meurman, J.H.; Rintamäki, H.; Lindqvist, C.; Rautio, M.; Jousimies-Somer, H.; Salaspuro, M. Increased salivary acetaldehyde levels in heavy drinkers and smokers: A microbiological approach to oral cavity cancer. Carcinogenesis 2000, 21, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Abdelaziz, M.S.; Osman, T.E. Detection of Cytomorphological Changes in Oral Mucosa among Alcoholics and Cigarette Smokers. Oman Med. J. 2011, 26, 349–352. [Google Scholar] [CrossRef] [PubMed]
- Radoï, L.; Paget-Bailly, S.; Cyr, D.; Papadopoulos, A.; Guida, F.; Schmaus, A.; Cénée, S.; Menvielle, G.; Carton, M.; Lapôtre-Ledoux, B.; et al. Tobacco smoking, alcohol drinking and risk of oral cavity cancer by subsite: Results of a French population-based case-control study, the ICARE study. Eur. J. Cancer Prev. Off. J. Eur. Cancer Prev. Organ. (ECP) 2013, 22, 268–276. [Google Scholar] [CrossRef]
- Scott, J.; Valentine, J.A.; St Hill, C.A.; Balasooriya, B.A. A quantitative histological analysis of the effects of age and sex on human lingual epithelium. J. Biol. Buccale 1983, 11, 303–315. [Google Scholar]
- Reis, S.R.; do Espírito Santo, A.R.; Andrade, M.G.; Sadigursky, M. Cytologic alterations in the oral mucosa after chronic exposure to ethanol. Braz. Oral Res. 2006, 20, 97–102. [Google Scholar] [CrossRef] [Green Version]
- Morales-González, J.A.; Sernas-Morales, M.L.; Morales-González, Á.; González-López, L.L.; Madrigal-Santillán, E.O.; Vargas-Mendoza, N.; Fregoso-Aguilar, T.A.; Anguiano-Robledo, L.; Madrigal-Bujaidar, E.; Álvarez-González, I.; et al. Morphological and biochemical effects of weekend alcohol consumption in rats: Role of concentration and gender. World J. Hepatol. 2018, 10, 297–307. [Google Scholar] [CrossRef]
- Waszkiewicz, N.; Zalewska, A.; Szajda, S.D.; Szulc, A.; Kępka, A.; Minarowska, A.; Wojewódzka-Żelezniakowicz, M.; Konarzewska, B.; Chojnowska, S.; Supronowicz, Z.B.; et al. The effect of chronic alcohol intoxication and smoking on the activity of oral peroxidase. Folia Histochem. Cytobiol. 2012, 50, 450–455. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group | Parakeratinized | Keratinized | Ortokeratinized | Hyperorthokeratinized |
|---|---|---|---|---|
| Female control | + | 0 | 0 | 0 |
| Female 40% | + | +++ | 0 | + |
| Female 5% | 0 | +++ | +++ | 0 |
| Male control | + | 0 | 0 | 0 |
| Male 40% | 0 | +++ | + | 0 |
| Male 5% | 0 | ++ | 0 | + |
| Group | Epithelial Hyperplasia | Acanthosis | Chronic Inflammatory Infiltrate (Monocuclear Inflammatory Cells) | Vascularization |
|---|---|---|---|---|
| female control | 0 | 0 | 0 | 0 |
| female 40% | +/++/+++ | ++/+++/+ | 0/+ | ++/+ |
| female 5% | +++/++ | +++/++ | +/++ | ++/+ |
| male control | 0 | 0 | 0 | 0 |
| male 40% | ++/+ | ++/+ | +/0 | +/++ |
| male 5% | +++ | +++/++ | 0 | ++/+ |
| Group | Parakeratinized | Keratinized | Ortokeratinized | Hyperortokeratinized |
|---|---|---|---|---|
| Female control | 0 | + | 0 | 0 |
| Female 40% | 0 | +++ | + | ++ |
| Female 5% | ++ | ++ | 0 | ++ |
| Male control | + | 0 | 0 | 0 |
| Male 40% | + | +++ | + | 0 |
| Male, 5% | 0 | +++ | + | 0 |
| Group | Epithelial Hyperplasia | Acanthosis | Chronic Inflammatory Infiltrate (Mononuclear Inflammatory Cells) | Vascularization |
|---|---|---|---|---|
| Female control | 0 | 0 | 0 | + |
| Female 40% | ++/+++/+ | ++/+++/+ | +/0 | ++/+++ |
| Female 5% | +++ | ++/+++ | +/0 | ++/+ |
| Male control | 0 | 0 | 0 | + |
| Male 40% | ++/+++/+ | +/++ | +/0 | ++/+ |
| Male 5% | +++/++ | ++ | 0 | ++/+++ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González-López, L.L.; Morales-González, Á.; Sosa-Gómez, A.; Madrigal-Santillán, E.O.; Anguiano-Robledo, L.; Madrigal-Bujaidar, E.; Álvarez-González, I.; Delgado-Olivares, L.; Valadez-Vega, C.; Esquivel-Chirino, C.; et al. Damage to Oral Mucosae Induced by Weekend Alcohol Consumption: The Role of Gender and Alcohol Concentration. Appl. Sci. 2022, 12, 3464. https://doi.org/10.3390/app12073464
González-López LL, Morales-González Á, Sosa-Gómez A, Madrigal-Santillán EO, Anguiano-Robledo L, Madrigal-Bujaidar E, Álvarez-González I, Delgado-Olivares L, Valadez-Vega C, Esquivel-Chirino C, et al. Damage to Oral Mucosae Induced by Weekend Alcohol Consumption: The Role of Gender and Alcohol Concentration. Applied Sciences. 2022; 12(7):3464. https://doi.org/10.3390/app12073464
Chicago/Turabian StyleGonzález-López, Laura Ligia, Ángel Morales-González, Alejandra Sosa-Gómez, Eduardo Osiris Madrigal-Santillán, Liliana Anguiano-Robledo, Eduardo Madrigal-Bujaidar, Isela Álvarez-González, Luis Delgado-Olivares, Carmen Valadez-Vega, César Esquivel-Chirino, and et al. 2022. "Damage to Oral Mucosae Induced by Weekend Alcohol Consumption: The Role of Gender and Alcohol Concentration" Applied Sciences 12, no. 7: 3464. https://doi.org/10.3390/app12073464