
Bruxism Influence on Volume and Interleukin-1β Concentration of Gingival Crevicular Fluid: A Preliminary Study

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Study Protocol
2.3. Gingival Crevicular Fluid Samples
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fatima, T.; Khurshid, Z.; Rehman, A.; Imran, E.; Srivastava, K.C.; Shrivastava, D. Gingival Crevicular Fluid (GCF): A Diagnostic Tool for the Detection of Periodontal Health and Diseases. Molecules 2021, 26, 1208. [Google Scholar] [CrossRef] [PubMed]
- Gilowski, Ł.; Płocica, I.; Wiench, R.; Kalamarz, I.; Krzemiński, T.F. The Application of Periotron 8000 in Diagnosis and Studies of Periodontal Diseases. Dent. Med. Probl. 2004, 41, 107–111. [Google Scholar]
- Perozini, C.; Chibebe, P.C.A.; Leao, M.V.P.; da Silva Queiroz, C.; Pallos, D. Gingival Crevicular Fluid Biochemical Markers in Periodontal Disease: A Cross-Sectional Study. Quintessence Int. 2010, 41, 877–883. [Google Scholar] [PubMed]
- Heboyan, A.; Manrikyan, M.; Zafar, M.S.; Rokaya, D.; Nushikyan, R.; Vardanyan, I.; Vardanyan, A.; Khurshid, Z. Bacteriological Evaluation of Gingival Crevicular Fluid in Teeth Restored Using Fixed Dental Prostheses: An In Vivo Study. Int. J. Mol. Sci. 2021, 22, 5463. [Google Scholar] [CrossRef] [PubMed]
- De Aguiar, M.C.S.; Perinetti, G.; Capelli, J. The Gingival Crevicular Fluid as a Source of Biomarkers to Enhance Efficiency of Orthodontic and Functional Treatment of Growing Patients. BioMed Res. Int. 2017, 2017, 3257235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nijakowski, K.; Surdacka, A. Salivary Biomarkers for Diagnosis of Inflammatory Bowel Diseases: A Systematic Review. Int. J. Mol. Sci. 2020, 21, 7477. [Google Scholar] [CrossRef] [PubMed]
- Gamonal, J.; Acevedo, A.; Bascones, A.; Jorge, O.; Silva, A. Levels of Interleukin-1 Beta, -8, and -10 and RANTES in Gingival Crevicular Fluid and Cell Populations in Adult Periodontitis Patients and the Effect of Periodontal Treatment. J. Periodontol. 2000, 71, 1535–1545. [Google Scholar] [CrossRef] [Green Version]
- Romano, F.; Del Buono, W.; Bianco, L.; Arena, M.; Mariani, G.M.; Di Scipio, F.; Berta, G.N.; Aimetti, M. Gingival Crevicular Fluid Cytokines in Moderate and Deep Sites of Stage III Periodontitis Patients in Different Rates of Clinical Progression. Biomedicines 2020, 8, 515. [Google Scholar] [CrossRef]
- McDevitt, M.J.; Russell, C.M.; Schmid, M.J.; Reinhardt, R.A. Impact of Increased Occlusal Contact, Interleukin-1 Genotype, and Periodontitis Severity on Gingival Crevicular Fluid IL-1beta Levels. J. Periodontol. 2003, 74, 1302–1307. [Google Scholar] [CrossRef]
- Da Silva, F.R.P.; Vasconcelos, A.C.C.G.; de Carvalho França, L.F.; Di Lenardo, D.; Nascimento, H.M.S.; Vasconcelos, D.F.P. Association between the Rs1143634 Polymorphism in Interleukin-1B and Chronic Periodontitis: Results from a Meta-Analysis Composed by 54 Case/Control Studies. Gene 2018, 668, 97–106. [Google Scholar] [CrossRef]
- Daneshmand, H.; Wade, A.B. Correlation between Gingival Fluid Measurements and Macroscopic and Microscopic Characteristics of Gingival Tissue. J. Periodontal Res. 1976, 11, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Hyun, Y.-C.; Lee, Y.-J. Gingival Crevicular Fluid Measure on Individual Tooth by Use of Periotron 8000. Int. J. Clin. Prev. Dent. 2009, 5, 031–037. [Google Scholar]
- Attar, N.B.; Banodkar, A.B.; Gaikwad, R.P.; Patil, C.L.; Simon, S. Evaluation of Gingival Crevicular Fluid Volume in Relation to Clinical Periodontal Status with Periotron 8000. Int. J. Appl. Dent. Sci. 2018, 4, 68–71. [Google Scholar]
- Nijakowski, K.; Surdacka, A. Diagnostics of Gingival Crevicular Fluid Using the Periotron 8000. In Biofizyka a Medycyna. T. 8.; Wydawnictwo Naukowe Uniwersytetu Medycznego im. K. Marcinkowskiego w Poznaniu: Poznań, Poland, 2019; pp. 170–180. [Google Scholar]
- Urbaniak, M.; Wiench, R.; Gilowski, Ł.; Płocica, I.; Krzemiński, T.F. The Amount of Gingival Crevicular Fluid in the Different Phases of the Menstrual Cycle. Dent. Med. Probl. 2012, 49, 523–528. [Google Scholar]
- Drummond, S.; Canavarro, C.; Perinetti, G.; Teles, R.; Capelli, J. The Monitoring of Gingival Crevicular Fluid Volume during Orthodontic Treatment: A Longitudinal Randomized Split-Mouth Study. Eur. J. Orthod. 2012, 34, 109–113. [Google Scholar] [CrossRef] [Green Version]
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; De Laat, A.; De Leeuw, R.; et al. International Consensus on the Assessment of Bruxism: Report of a Work in Progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef]
- Manfredini, D.; Ahlberg, J.; Lobbezoo, F. Bruxism Definition: Past, Present, and Future—What Should a Prosthodontist Know? J. Prosthet. Dent. 2021, in press. [Google Scholar] [CrossRef]
- Flueraşu, M.I.; Bocşan, I.C.; Țig, I.-A.; Iacob, S.M.; Popa, D.; Buduru, S. The Epidemiology of Bruxism in Relation to Psychological Factors. Int. J. Environ. Res. Public Health 2022, 19, 691. [Google Scholar] [CrossRef]
- Wieckiewicz, M.; Bogunia-Kubik, K.; Mazur, G.; Danel, D.; Smardz, J.; Wojakowska, A.; Poreba, R.; Dratwa, M.; Chaszczewska-Markowska, M.; Winocur, E.; et al. Genetic Basis of Sleep Bruxism and Sleep Apnea-Response to a Medical Puzzle. Sci. Rep. 2020, 10, 7497. [Google Scholar] [CrossRef]
- Maciejewska-Szaniec, Z.; Kaczmarek-Ryś, M.; Hryhorowicz, S.; Przystańska, A.; Gredes, T.; Maciejewska, B.; Hoppe-Gołębiewska, J.; Słomski, R.; Pławski, A.; Czajka-Jakubowska, A. Polymorphic Variants in Genes Related to Stress Coping Are Associated with the Awake Bruxism. BMC Oral Health 2021, 21, 496. [Google Scholar] [CrossRef]
- Vavrina, J.; Vavrina, J. Bruxism: Classification, Diagnostics and Treatment. Praxis 2020, 109, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Ahlberg, J.; Aarab, G.; Bracci, A.; Durham, J.; Ettlin, D.; Gallo, L.M.; Koutris, M.; Wetselaar, P.; Svensson, P.; et al. Towards a Standardized Tool for the Assessment of Bruxism (STAB)-Overview and General Remarks of a Multidimensional Bruxism Evaluation System. J. Oral Rehabil. 2020, 47, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Manfredini, D.; Lobbezoo, F. Sleep Bruxism and Temporomandibular Disorders: A Scoping Review of the Literature. J. Dent. 2021, 111, 103711. [Google Scholar] [CrossRef] [PubMed]
- Michalek-Zrabkowska, M.; Wieckiewicz, M.; Smardz, J.; Gac, P.; Poreba, R.; Wojakowska, A.; Mazur, G.; Martynowicz, H. Determination of Inflammatory Markers, Hormonal Disturbances, and Sleepiness Associated with Sleep Bruxism Among Adults. Nat. Sci. Sleep 2020, 12, 969–979. [Google Scholar] [CrossRef]
- Michalek-Zrabkowska, M.; Wieckiewicz, M.; Macek, P.; Gac, P.; Smardz, J.; Wojakowska, A.; Poreba, R.; Mazur, G.; Martynowicz, H. The Relationship between Simple Snoring and Sleep Bruxism: A Polysomnographic Study. Int. J. Environ. Res. Public Health 2020, 17, 8960. [Google Scholar] [CrossRef]
- Lobbezoo, F.; Ahlberg, J.; Glaros, A.G.; Kato, T.; Koyano, K.; Lavigne, G.J.; de Leeuw, R.; Manfredini, D.; Svensson, P.; Winocur, E. Bruxism Defined and Graded: An International Consensus. J. Oral Rehabil. 2013, 40, 2–4. [Google Scholar] [CrossRef]
- Smith, B.G.; Knight, J.K. An Index for Measuring the Wear of Teeth. Br. Dent. J. 1984, 156, 435–438. [Google Scholar] [CrossRef]
- Thymi, M.; Visscher, C.M.; Yoshida-Kohno, E.; Crielaard, W.; Wismeijer, D.; Lobbezoo, F. Associations between Sleep Bruxism and (Peri-) Implant Complications: A Prospective Cohort Study. BDJ Open 2017, 3, 17003. [Google Scholar] [CrossRef] [Green Version]
- Mohammadi, H.; Roochi, M.M.; Sadeghi, M.; Garajei, A.; Heidar, H.; Meybodi, A.A.; Dallband, M.; Mostafavi, S.; Mostafavi, M.; Salehi, M.; et al. Association between Interleukin-1 Polymorphisms and Susceptibility to Dental Peri-Implant Disease: A Meta-Analysis. Pathogens 2021, 10, 1600. [Google Scholar] [CrossRef]
- Alassy, H.; Parachuru, P.; Wolff, L. Peri-Implantitis Diagnosis and Prognosis Using Biomarkers in Peri-Implant Crevicular Fluid: A Narrative Review. Diagnostics 2019, 9, E214. [Google Scholar] [CrossRef] [Green Version]
- Nogueira-Filho, G.; Pesun, I.; Isaak-Ploegman, C.; Wijegunasinghe, M.; Wierzbicki, T.; McCulloch, C.A. Longitudinal Comparison of Cytokines in Peri-Implant Fluid and Gingival Crevicular Fluid in Healthy Mouths. J. Periodontol. 2014, 85, 1582–1588. [Google Scholar] [CrossRef] [PubMed]
- Yaghobee, S.; Khorsand, A.; Paknejad, M. Comparison of Interleukin-1β Levels in Gingival Crevicular Fluid and Peri-Implant Crevicular Fluid and Its Relationship with Clinical Indexes. J. Dent. 2013, 10, 1–9. [Google Scholar]
- BinShabaib, M.; ALHarthi, S.S.; Akram, Z.; Khan, J.; Rahman, I.; Romanos, G.E.; Javed, F. Clinical Periodontal Status and Gingival Crevicular Fluid Cytokine Profile among Cigarette-Smokers, Electronic-Cigarette Users and Never-Smokers. Arch. Oral Biol. 2019, 102, 212–217. [Google Scholar] [CrossRef] [PubMed]
- Slawik, S.; Staufenbiel, I.; Schilke, R.; Nicksch, S.; Weinspach, K.; Stiesch, M.; Eberhard, J. Probiotics Affect the Clinical Inflammatory Parameters of Experimental Gingivitis in Humans. Eur. J. Clin. Nutr. 2011, 65, 857–863. [Google Scholar] [CrossRef]
- Grieve, W.G.; Johnson, G.K.; Moore, R.N.; Reinhardt, R.A.; DuBois, L.M. Prostaglandin E (PGE) and Interleukin-1 Beta (IL-1 Beta) Levels in Gingival Crevicular Fluid during Human Orthodontic Tooth Movement. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Const. Soc. Am. Board Orthod. 1994, 105, 369–374. [Google Scholar] [CrossRef]
- Tzannetou, S.; Efstratiadis, S.; Nicolay, O.; Grbic, J.; Lamster, I. Comparison of Levels of Inflammatory Mediators IL-1beta and BetaG in Gingival Crevicular Fluid from Molars, Premolars, and Incisors during Rapid Palatal Expansion. Am. J. Orthod. Dentofac. Orthop. Off. Publ. Am. Assoc. Orthod. Const. Soc. Am. Board Orthod. 2008, 133, 699–707. [Google Scholar] [CrossRef]
- Kalemaj, Z.; Buti, J.; Deregibus, A.; Canuto, R.M.; Maggiora, M.; Debernardi, C.L. Aligning Effectiveness, Secretion of Interleukin 1β and Pain Control During Fixed Orthodontic Treatment with Self-Ligating Appliances and Supplemental Vibrational Appliances. A Randomized Controlled Clinical Trial. J. Biomed. 2017, 2, 25–33. [Google Scholar] [CrossRef] [Green Version]
- Castroflorio, T.; Gamerro, E.F.; Caviglia, G.P.; Deregibus, A. Biochemical Markers of Bone Metabolism during Early Orthodontic Tooth Movement with Aligners. Angle Orthod. 2017, 87, 74–81. [Google Scholar] [CrossRef] [Green Version]
- Arif, R.; Dennison, J.B.; Garcia, D.; Yaman, P. Gingival Health of Porcelain Laminate Veneered Teeth: A Retrospective Assessment. Oper. Dent. 2019, 44, 452–458. [Google Scholar] [CrossRef]
- Abdullah Al-Abdaly, M.M.A. Evaluation of Gingival Crevicular Fluid Volume by (Periotron 8000) ® in Yemeni Qat Chewing Samples. J. Dent. Res. Rev. 2016, 3, 51–53. [Google Scholar] [CrossRef]
- Gunpinar, S.; Alptekin, N.O.; Dundar, N. Gingival Crevicular Fluid Levels of Monocyte Chemoattractant Protein-1 in Patients with Aggressive Periodontitis. Oral Dis. 2017, 23, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, L.; De Biasi, M.; Lorenzon, M.G.; Frattini, C.; Angerame, D. Volumetric Analysis of Gingival Crevicular Fluid and Peri-Implant Sulcus Fluid in Healthy and Diseased Sites: A Cross-Sectional Split-Mouth Pilot Study. Open Dent. J. 2016, 10, 131–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ata-Ali, J.; Flichy-Fernandez, A.J.; Alegre-Domingo, T.; Candel-Marti, M.E.; Penarrocha, D.; Balaguer-Martinez, J.; Penarrocha, M.A. Analysis of the Peri-Implant Microbiota in 90 Dental Implants and Its Relationship to Crevicular Fluid Volume. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e944–e947. [Google Scholar] [CrossRef] [Green Version]
- Bilgin Çetin, M.; Sezgin, Y.; Maraş, E.; Cebeci, İ.A. Association of Probable Bruxism with Periodontal Status: A Cross-Sectional Study in Patients Seeking Periodontal Care. J. Periodontal Res. 2021, 56, 370–378. [Google Scholar] [CrossRef] [PubMed]
- Botelho, J.; Machado, V.; Proença, L.; Rua, J.; Martins, L.; Alves, R.; Cavacas, M.A.; Manfredini, D.; Mendes, J.J. Relationship between Self-Reported Bruxism and Periodontal Status: Findings from a Cross-Sectional Study. J. Periodontol. 2019, 91, 1049–1056. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Bruxists M [Q1–Q3] | Non-Bruxists M [Q1–Q3] |
|---|---|---|
| Approximal plaque index [%] | 23.1 [16.7–26.9] | 15.4 [10.0–23.1] |
| Plaque index | 0.21 [0.13–0.21] | 0.08 [0.00–0.25] |
| Sulcus bleeding index [%] | 0.0 [0.0–3.8] | 0.0 [0.0–3.8] |
| Gingival index | 0.13 [0.13–0.21] | 0.08 [0.04–0.17] |
| Periodontal probing depth [mm] | 1.15 [1.02–1.29] | 1.35 [1.04–1.73] |
| TWI | Bruxists M [Q1–Q3] | Non-Bruxists M [Q1–Q3] | p-Value |
|---|---|---|---|
| 16 | 1.0 [1.0–2.0] | 0.0 [0.0–1.0] | 0.013 * |
| 11 | 1.0 [1.0–2.0] | 1.0 [0.0–1.0] | 0.058 |
| 24 | 1.0 [1.0–2.0] | 0.0 [0.0–0.0] | 0.010 * |
| 36 | 1.0 [1.0–2.0] | 1.0 [0.0–1.0] | 0.018 * |
| 31 | 2.0 [1.0–2.0] | 1.0 [1.0–2.0] | 0.098 |
| 44 | 2.0 [1.0–2.0] | 0.0 [0.0–1.0] | 0.003 * |
| Total | 1.5 [1.2–1.5] | 0.5 [0.2–0.8] | <0.001 * |
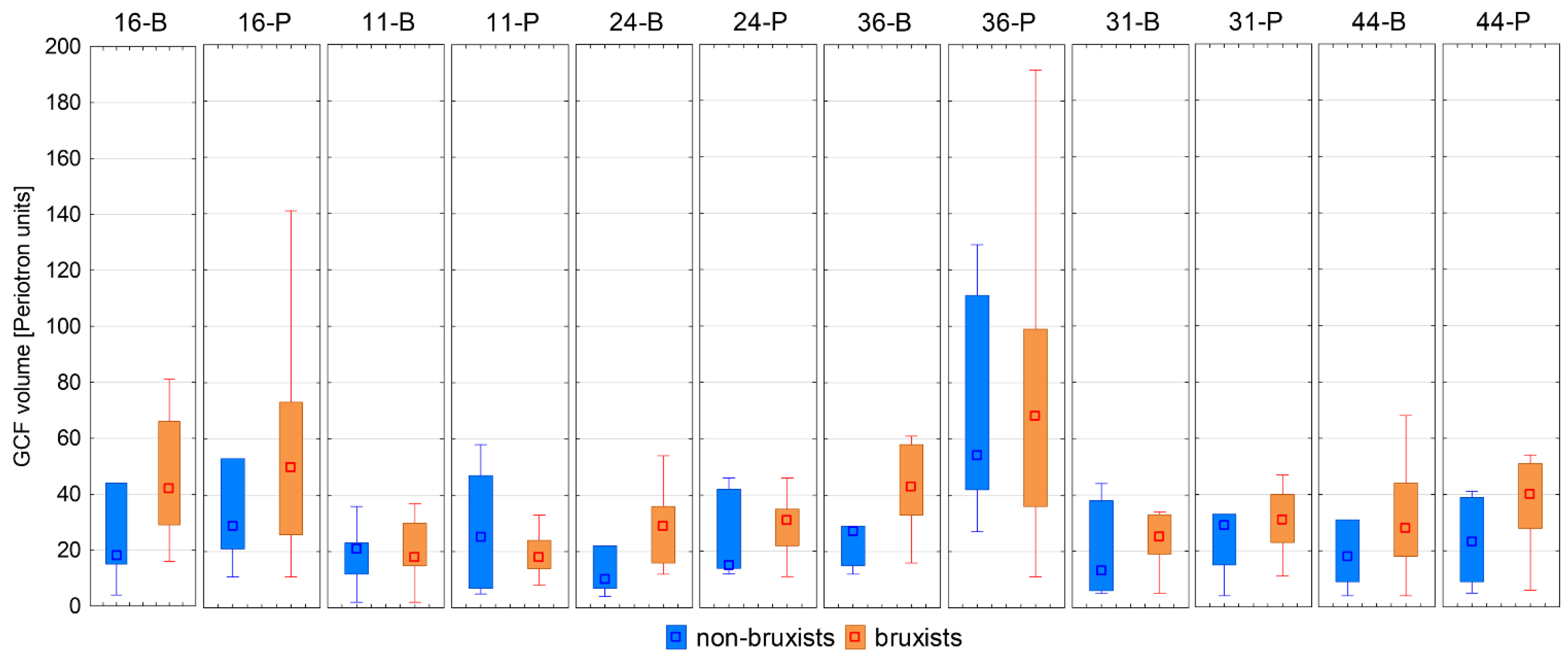
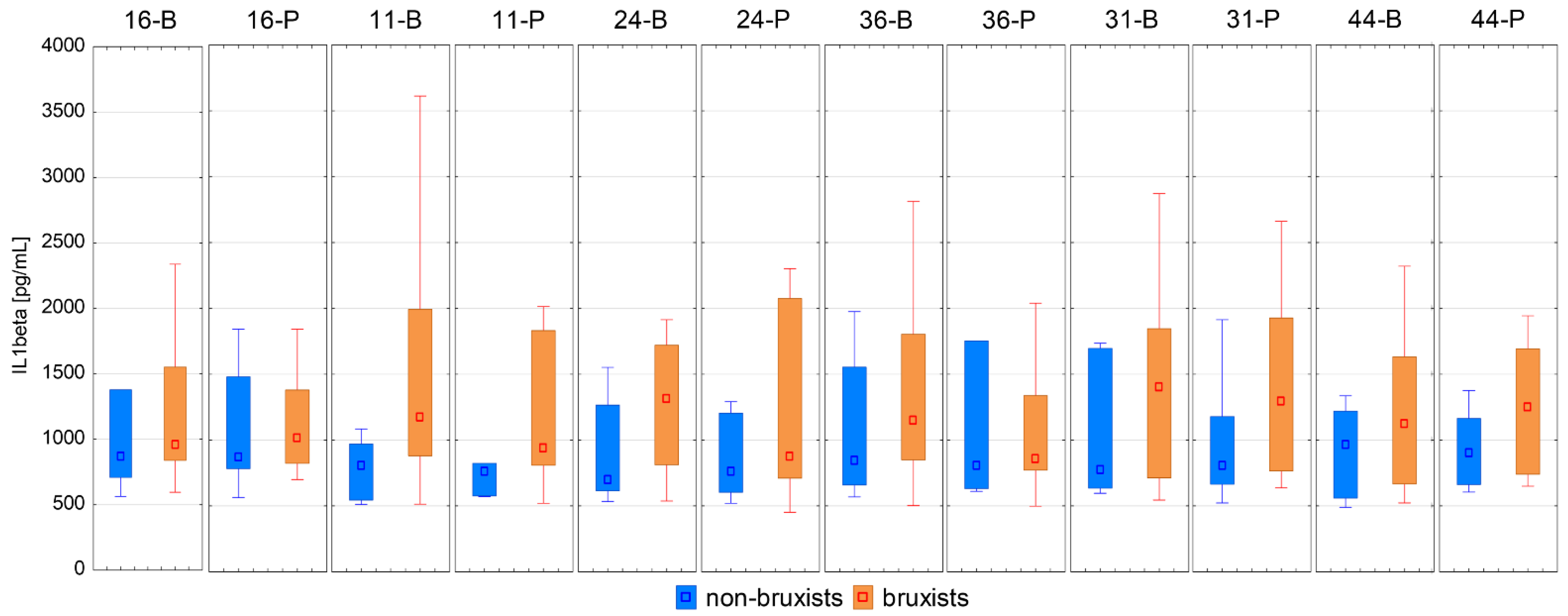
| GCF Volume [Periotron Units] | IL-1β [pg/mL] | |||||
|---|---|---|---|---|---|---|
| Bruxists M [Q1–Q3] | Non-Bruxists M [Q1–Q3] | p-Value | Bruxists M [Q1–Q3] | Non-Bruxists M [Q1–Q3] | p-Value | |
| 16-B | 42 [29–66] | 18 [15–44] | 0.165 | 960.6 [839.4–1551.3] | 870.0 [708.3–1377.2] | 0.526 |
| 16-P | 50 [26–73] | 29 [21–53] | 0.405 | 1011.8 [823.7–1379.4] | 866.5 [783.9–1479.4] | 0.663 |
| 11-B | 18 [15–30] | 21 [12–23] | 0.937 | 1175.6 [880.9–1993.9] | 808.9 [545.7–970.2] | 0.062 |
| 11-P | 18 [14–24] | 25 [7–47] | 0.382 | 937.6 [808.9–1830.2] | 758.6 [575.1–823.7] | 0.048 * |
| 24-B | 29 [16–36] | 10 [7–22] | 0.062 | 1314.7 [811.8–1719.5] | 700.5 [614.7–1265.3] | 0.113 |
| 24-P | 31 [22–35] | 15 [14–42] | 0.142 | 873.6 [710.3–2074.1] | 761.0 [604.4–1203.2] | 0.428 |
| 36-B | 43 [33–58] | 27 [15–29] | 0.026 * | 1150.8 [849.3–1803.8] | 846.0 [658.4–1553.2] | 0.383 |
| 36-P | 68 [36–99] | 54 [42–111] | 0.843 | 856.0 [771.0–1337.8] | 808.9 [631.1–1753.3] | 0.663 |
| 31-B | 25 [19–33] | 13 [6–38] | 0.321 | 1404.7 [712.3–1846.4] | 773.5 [635.4–1696.1] | 0.303 |
| 31-P | 31 [23–40] | 29 [15–33] | 0.362 | 1294.9 [765.9–1926.1] | 806.0 [664.9–1178.8] | 0.235 |
| 44-B | 28 [18–44] | 18 [9–31] | 0.204 | 1120.8 [666.5–1632.2] | 965.4 [560.4–1220.2] | 0.267 |
| 44-P | 40 [28–51] | 23 [9–39] | 0.074 | 1250.9 [740.0–1691.5] | 900.0 [663.2–1162.9] | 0.154 |
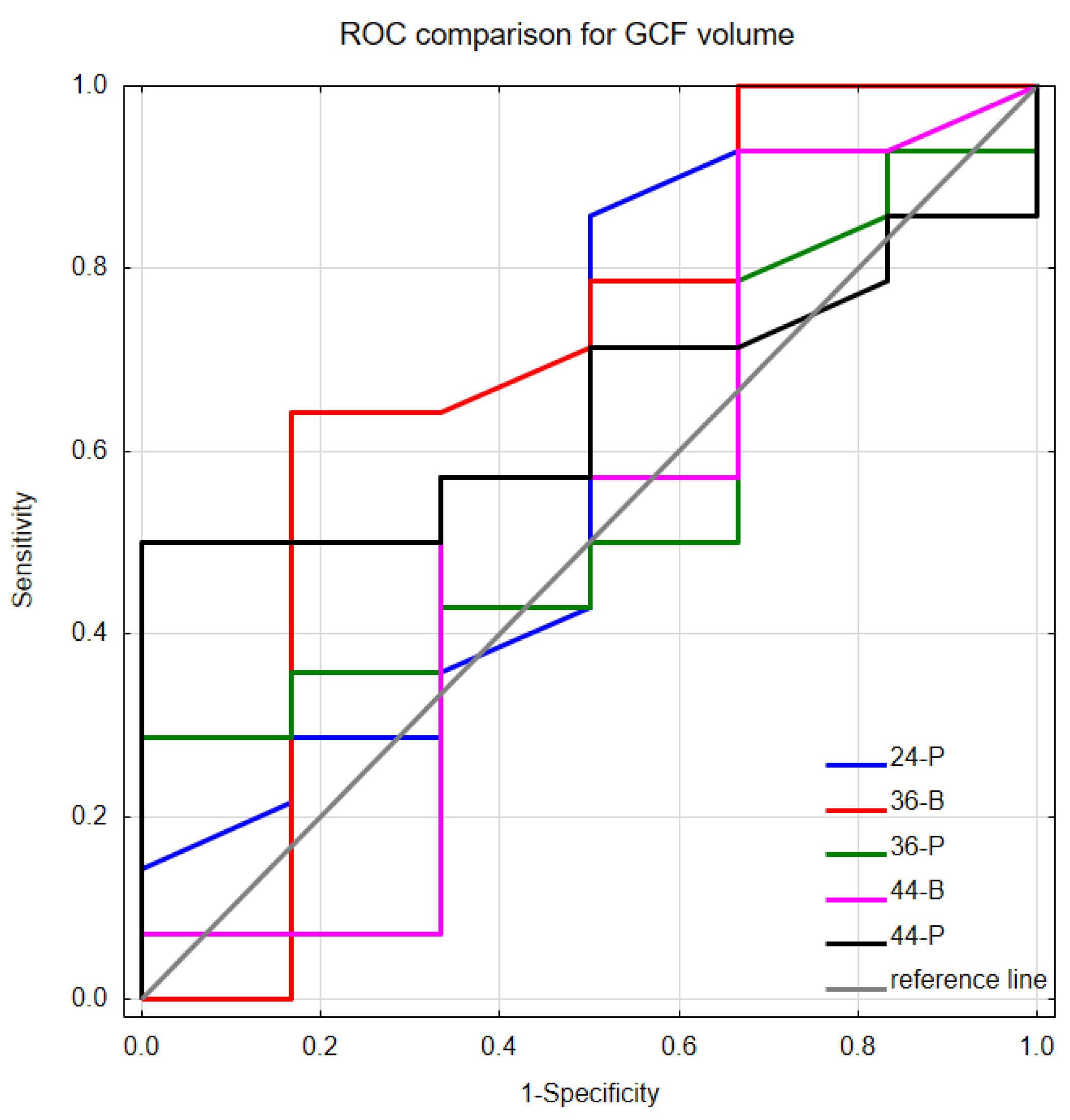
| Stimulant | AUC | SE | p-Value |
|---|---|---|---|
| 16-B | 0.458 | 0.157 | 0.791 |
| 16-P | 0.488 | 0.150 | 0.937 |
| 11-B | 0.357 | 0.134 | 0.287 |
| 11-P | 0.327 | 0.146 | 0.236 |
| 24-B | 0.381 | 0.160 | 0.458 |
| 24-P | 0.601 | 0.151 | 0.504 |
| 36-B | 0.685 | 0.151 | 0.221 |
| 36-P | 0.554 | 0.137 | 0.695 |
| 31-B | 0.476 | 0.148 | 0.873 |
| 31-P | 0.500 | 0.151 | >0.999 |
| 44-B | 0.530 | 0.161 | 0.854 |
| 44-P | 0.649 | 0.121 | 0.219 |
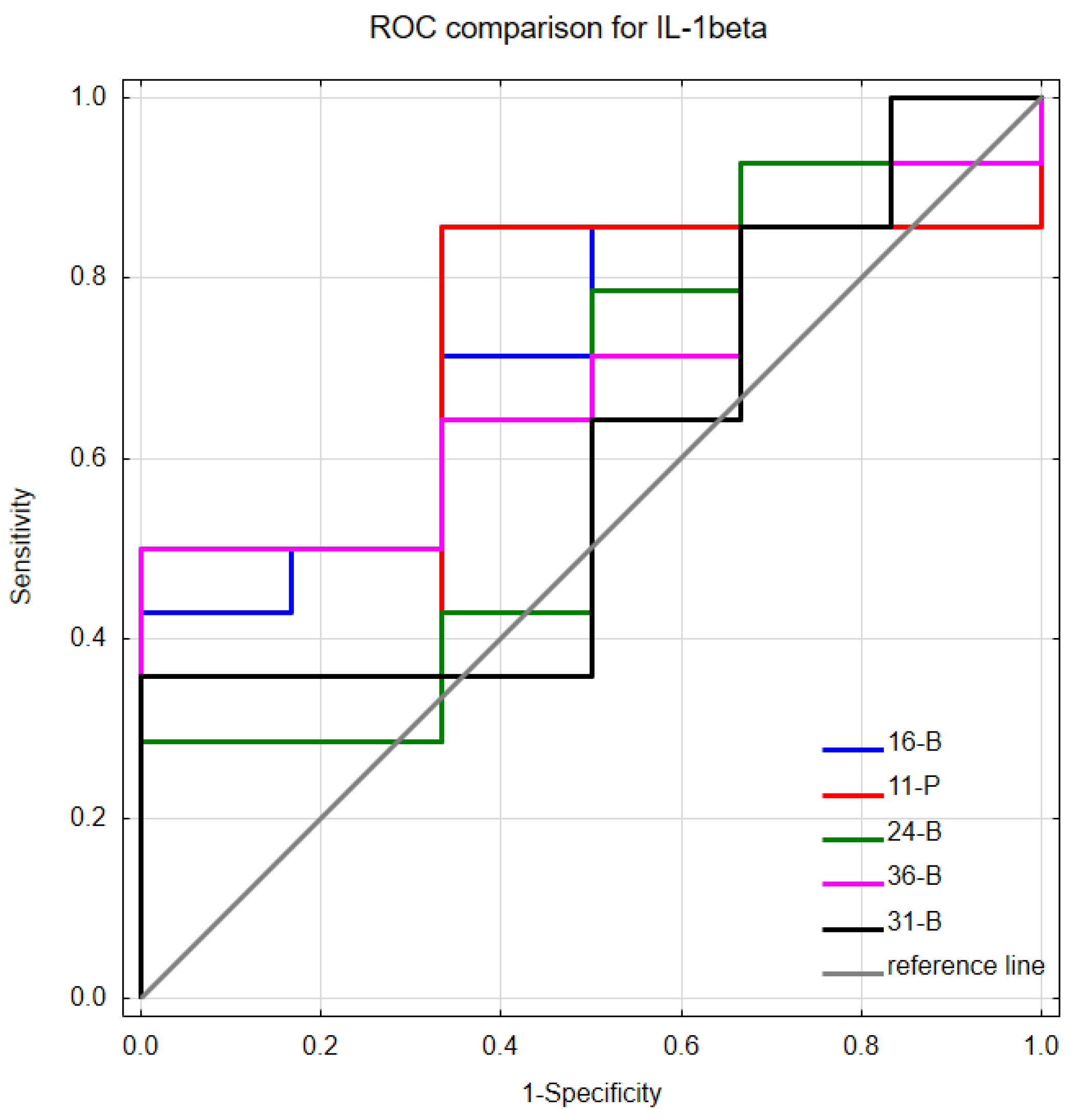
| Stimulant | AUC | SE | p-Value |
|---|---|---|---|
| 16-B | 0.714 | 0.118 | 0.070 |
| 16-P | 0.440 | 0.160 | 0.710 |
| 11-B | 0.583 | 0.129 | 0.519 |
| 11-P | 0.667 | 0.140 | 0.233 |
| 24-B | 0.607 | 0.142 | 0.452 |
| 24-P | 0.571 | 0.156 | 0.648 |
| 36-B | 0.690 | 0.118 | 0.107 |
| 36-P | 0.548 | 0.158 | 0.763 |
| 31-B | 0.595 | 0.139 | 0.494 |
| 31-P | 0.571 | 0.148 | 0.629 |
| 44-B | 0.560 | 0.139 | 0.668 |
| 44-P | 0.571 | 0.142 | 0.615 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nijakowski, K.; Ortarzewska, M.; Morawska, A.; Brożek, A.; Nowicki, M.; Formanowicz, D.; Surdacka, A. Bruxism Influence on Volume and Interleukin-1β Concentration of Gingival Crevicular Fluid: A Preliminary Study. Appl. Sci. 2022, 12, 2089. https://doi.org/10.3390/app12042089
Nijakowski K, Ortarzewska M, Morawska A, Brożek A, Nowicki M, Formanowicz D, Surdacka A. Bruxism Influence on Volume and Interleukin-1β Concentration of Gingival Crevicular Fluid: A Preliminary Study. Applied Sciences. 2022; 12(4):2089. https://doi.org/10.3390/app12042089
Chicago/Turabian StyleNijakowski, Kacper, Martyna Ortarzewska, Alicja Morawska, Alicja Brożek, Marcin Nowicki, Dorota Formanowicz, and Anna Surdacka. 2022. "Bruxism Influence on Volume and Interleukin-1β Concentration of Gingival Crevicular Fluid: A Preliminary Study" Applied Sciences 12, no. 4: 2089. https://doi.org/10.3390/app12042089